 Alexandru I. Tiba1*
Alexandru I. Tiba1* Simona Trip1
Simona Trip1 Carmen H. Bora1
Carmen H. Bora1 Marius Drugas1Feliciana Borz1Daiana C. Miclăuş1Laura Voss2Sorin C. Iova3Simona Pop3
Marius Drugas1Feliciana Borz1Daiana C. Miclăuş1Laura Voss2Sorin C. Iova3Simona Pop3- 1Department of Psychology, University of Oradea, Oradea, Romania
- 2Hull York Medical School, Hull, United Kingdom
- 3Faculty of Medicine and Pharmacy, University of Oradea, Oradea, Romania
Primary irrational beliefs, such as demanding about attaining personal goals, are a common trans-diagnostic factor involved in many emotional disorders. Although Bipolar Disorder (BPD) is a severe emotional disorder, little is known about the role of primary irrational beliefs in the risk of BPD. Given that the risk for mania is related to responses to positive rather than adverse events, we developed a measure of irrational beliefs in response to cues of positive events. This is the first study that examines the relationship between positive primary irrational beliefs and the risk of BPD. 119 participants completed an online survey including measures for the risk of BPD, irrational beliefs, positive irrational beliefs, mania-related cognitions, and mood measures (depressive and manic mood). Results revealed significant associations between the risk of BPD and positive primary irrational beliefs, irrational beliefs, positive generalization, and mood. Regression analyses revealed that positive primary irrational beliefs, such as demanding to attain significant goals in response to cues for positive events, uniquely predict the risk for BPD independently of mood, mania-related cognitions and irrational beliefs. These findings encourage the treatment approaches focused on restructuring primary irrational beliefs in response to positive situations to reduce the risk of BPD.
Introduction
Bipolar disorder (BPD) is a highly severe mental disorder (Vigo et al., 2016). Added to its severity, the poor treatment adherence and the limited effectiveness of existing interventions (Ye et al., 2016) complicate its treatment. Several meta-analyses showed that cognitive-behavioral therapies (CBT) are an effective adjunctive treatment for BPD, reducing the relapse rate, depressive symptoms, mania severity, and resulting in an increased psychosocial functioning (Szentagotai and David, 2010; Ye et al., 2016; Chiang et al., 2017; Miklowitz et al., 2021). Yet, some effects are short-lived and controversial (Ye et al., 2016). The need to improve the existing treatments and preventive interventions for BPD has oriented the research efforts on elucidating the psychological mechanisms involved in the risk of developing the disorder. Finding new mechanisms amenable to change by psychotherapy interventions, is a very promising avenue (Szentagotai and David, 2010). Cognitive factors are such examples of treatment targets that can offer a great promise for improving the psychological treatment of BPD. However, research on cognitive processes underlying the risk for BPD yielded mixed results about the types of cognitions involved in the risk of BPD (Yesilyaprak et al., 2019). Recent research has consistently pointed toward dysregulation of goal representations and approach behavioral systems as significant risk factors for BPD (Johnson, 2005; Johnson et al., 2010). Unfortunately, these findings have not consistently informed the existing treatments. A possible answer may come from looking into existing trans-diagnostic cognitive mechanisms involved in emotional disorders for which effective treatment methods have already been tested. Responding with primary irrational beliefs (e.g., absolute demands for attaining personal goals or desires: “I must have what I want”) (Ellis, 1994; Ellis et al., 2010; Dryden, 2019) when adverse events block someone’s goals is one form of goal dysregulation that has been consistently shown as a mechanism for various emotional disorders and dysfunctions (Tiba et al., 2012; Vîslã et al., 2016; David et al., 2019).
Furthermore, there is substantial evidence for the effectiveness of psychotherapy methods (e.g., Rational Emotive Behavior Therapy) in changing irrational beliefs (David et al., 2018, 2019). Lately, both empirical and theoretical studies have linked rigid goals in form of demandingness to dysregulated behavioral activation system (BAS) (Tiba, 2005; Yıldırım and Maltby, 2021), increased activation after goal-attainment (Tiba and Szentagotai, 2005), and exaggerated active coping in response to both adversities (Tiba, 2010; Tiba and Manea, 2018a,b). Being a well-known trans-diagnostic mechanism for emotional disorders (Vîslã et al., 2016) for which we have effective treatment methods (Trip et al., 2010; David et al., 2018, 2019), evidence of the role of primary irrational beliefs in vulnerability to BPD may provide a strong treatment target, spurring the development of better psychological interventions for the treatment or the prevention of BPD.
Unfortunately, to our knowledge, no study has investigated irrational primary beliefs or rigid beliefs in relation to the risk of BPD and mania. One reason for this lack of research is that primary irrational beliefs were measured as responses to negative situations (Macavei and McMahon, 2010). Primary irrational beliefs or rigid beliefs are usually defined referring to the situation in which one person demands that he should meet personal goals and desires when adverse events interfere with his goal attainment (Ellis, 1994). Instead, the risk for manic episodes is related to responses to positive events and not to negative events (Johnson et al., 2000; Gruber et al., 2008). Moreover, dysfunctional responses involved in the risk for mania are mainly related to specific types of positive events, such as goal-attainment related positive events (Johnson et al., 2000). Thus, the types of positive cognition involved in the risk for mania are expected to follow the situation of attaining personal goals. Given the role of positive events as activating events for the risk for mania, the existing measurements of irrational beliefs may not be appropriate to test their involvement in the risk for BPD and the development of episodes of mania.
In the present study, we overcome these shortcomings by measuring irrational beliefs in positive situations. We examined whether primary irrational beliefs (Ellis et al., 2010) about attaining goals in positive situations predict hypomanic personality which is a well-known risk factor of bipolar disorder beyond other cognitive and affective factors such as hypo/manic states, depressive mood, and positive generalizations.
The present study
In the present study, we investigated whether irrational beliefs in positive situations were uniquely related to the risk of hypo/mania measured by the Hypomanic Personality Scale (HPS). We asked participants to measures related to the risk for hypo/mania, HPS and a measure of positive irrational beliefs. Then, we used regression analyses to examine whether positive irrational beliefs have an unique contribution to the hypo/mania risk (measured by HPS) controlling for the contribution of demographic variables (age and sex), depressed and manic mood, and positive hypo/manic thoughts. To develop a measure of positive irrational beliefs, we followed the suggestion of Leahy and Beck (1988), according to which cognitive schemas in mania are the mirror image of cognitive schemas in depression (Leahy and Beck, 1988). Based on this suggestion, we developed positive items mirroring items based on a well-known measure of irrational beliefs. We used comfort, achievement and approval-related items from the General Attitude and Beliefs Scale (GABS scale; DiGiuseppe et al., 1988; Bernard, 1998) and developed by positive correspondence a positive irrational measure. We mirrored four types of irrational appraisals: demandingness (e.g., “It’s essential to be liked by important people, and I will not accept their not liking me”) into positive demandingness (e.g., “When I see important persons like me, I consider being liked by them as a necessity because it is essential to be liked by important persons”), low frustration tolerance (e.g., “I can’t stand not doing well at tasks that are important to me”) into “positive overwhelming” (e.g., “I am overwhelmed by happiness when I do well tasks that are important for me”), awfulizing (e.g., “It’s awful to have hassles in one’s life and it is a catastrophe to be hassled”) in wonderfulizing (e.g., “It is wonderful to have daily uplifts in your life and it is extraordinary when this happens”) and self-depreciation (e.g., “If I do not perform well at tasks that are so important to me, it is because I am a worthless bad person”) into self-appreciation (e.g., “When I succeed in something important I am a good and valuable person”). Each process referred to three content types: achievement, comfort, and social approval. The items we developed by the first author (A.T.). Two psychologists (A.T. and C.B.) have evaluated the mirror correspondence of the items. We analyzed the relationship between positive primary irrational beliefs and hypo/mania risk (HPS) along with other mania and cognitive related measures in the general population.
Materials and methods
Participants
We recruited an online sample of 119 participants for this study. Participants were recruited using social media adverts for undergraduates enrolled at the university and contacting undergraduate students who took part in previous research at university. No incentives to participate were provided. Two participants did not give their consent for participation and were excluded. Additionally, nine subjects who failed at attention check questions were eliminated. One participant was eliminated being below 18 years of age at the enrolment in the study. The final sample consisted of 107 participants (Meanage = 25.11 years, SD = 10.00; 83 females, 24 males) (see Table 1).

Table 1. Sample characteristics and the main variables.
Measures
Depression
Participants completed the Patient Health Questionnaire 2 (PHQ-2; Kroenke et al., 2003). The PHQ-2 is a 2-item self-report measure developed to screen for symptoms of depression. Participants had to endorse how much they had “little interest or pleasure in doing things” (Kroenke et al., 2003) and were “feeling down, depressed or hopeless” (Kroenke et al., 2003) over the previous 2 weeks on a 4 points Likert scale from 0 (not at all) to 3 (nearly every day) (Cronbach α was 0.63).
Irrational beliefs in negative situations
To measure irrational beliefs, we used a variant of the ABS2-short form scale focused on achievement (HABS2-short form; Hyland et al., 2014). HABS2-short form contains 24 items extracted from a 72 items widely used irrational beliefs measure (ABS-2) reflecting four irrational cognitive processes (demandingness, low-frustration tolerance, awfulizing, and self-depreciation) mainly about achievement and comfort (DiGiuseppe et al., 2020). We summed the responses from rational items to calculate the rational subscale score Cronbach α was 0.89) and the responses from irrational items to calculate the irrational subscale score (Cronbach α was 0.80). Given the relevance of the content-specific irrational beliefs for different pathologies (DiGiuseppe et al., 2021), and the suggestion that individuals with manic pathology have dysfunctional responses to achievement related-events (Johnson et al., 2000), we additionally calculated two scores: an irrational achievement score (Cronbach α was 0.74) and a rational achievement scale each containing five items (Cronbach α was 0.85).
Hypomanic personality
The Hypomanic Personality Scale (HPS; Eckblad and Chapman, 1986) is a self-report scale that measures the risk of bipolar disorder. Participants had to endorse 48 items using a true-false response format. Items refer to emotional, behavioral and cognitive tendencies that characterize hypomanic personality (e.g., “I am frequently in such high spirits that I can’t concentrate on any one thing for too long.”; “I often feel excited and happy for no apparent reason” (Cronbach α was good 0.87).
Hypo/mania symptoms
The Altman Self-Rating Scale for Mania (ASRM; Altman et al., 1997) measure the experience of hypo/manic symptoms over the past week. Participants rate their responses on a Likert scale from 1 (e.g., “I do not feel happier or more cheerful than usual”) to 5 (“I feel happier of more cheerful than usual all the time”). The scores were recoded from 0 to 4 to compare the responses to the recommended cut-off of 6 (Altman et al., 1997) (Cronbach α was acceptable 0.74).
Positive hypo/manic thoughts
The Positive Generalization Scale (POG; Eisner et al., 2008) contains 16 items that measure the over-generalization people make from successes (e.g., “When something good happens to me, it makes me expect good things in other parts of my life too”). Participants had to indicate how much they disagree with each item on a Likert type scale from 1 (I disagree a lot) to 4 (I agree a lot) (Cronbach α was good 0.89).
Positive irrational beliefs measure
Thirty-seven positive irrational statements mirroring to four types of irrational appraisals from the General Attitude and Beliefs scale (GABS scale; DiGiuseppe et al., 1988; Bernard, 1998) were included in the analyses: positive demandingness (e.g., “When I see I am about to know I will succeed, for me succeeding becomes a must not just a desire”), positive “overwhelming” (e.g., “It is the greatest happiness to succeed in what is important and I’m overwhelmed by my happiness when I do”), “wonderfulizing” (e.g., “When I perform well in something important, it is wonderful”), and self-valuing (e.g., “When I succeed in something important I am a good and valuable person”). Thus, we mirrored thirty-four items about comfort, achievement, approval and self-worth from GABS scale. Since only one item of demandingness items was negatively formulated, we included the original items and added three new items reflecting demandingness in response to positive situations (see the positive primary irrational statements below). Participants rated how much they agreed with each statement on a Likert type scale from 1 (totally disagree) to 5 (totally agree). The scale was previously tested in a pilot study of fifteen participants, results showing that participants understood the items. Based on participants feedback the items were adjusted to better reflect their experiences in response to positive events. Principal axis factoring with Promax rotation was run to establish the factorial structure of the positive irrational belief items. The Kaiser-Meyer-Olkin test value was 0.915 suggesting that the sample size in this study was sufficient for exploratory factorial analysis. The Bartlett’s Test of Sphericity χ2 = 3394.657, df = 666 was significant, p < 0.001 showing that the matrix of relationships between the items differs from the unit matrix without relations. The scree plot inspection and the Monte Carlo parallel analysis offered a two factor solution: (1) a sociotropy positive irrational beliefs factor (10 items, Cronbach α 0.94) and (2) an autonomy positive beliefs factor (26 items, Cronbach α 0.96). We removed the item eight because it did not load into either of the two factors. We calculated two additional scores: (1) a general score for all the items (the internal consistency coefficient Cronbach α was excellent 0.96), and (2) a positive primary irrational beliefs score (i.e., “When I see I am about to know I will succeed, for me succeeding becomes a must not just a desire”; “When I realize that someone important for me finally appreciates me, being liked and appreciated by that person becomes a necessity for me”; “When I realize that my life finally becomes pleasurable and comfortable, having a pleasant life becomes a necessity for me”; “When I see important persons like me, I consider being liked by them as a necessity because it is essential to be liked by important persons”(Cronbach α was 0.67).
Procedure
Data collection was conducted online from March 15th to June 9th 2022. Participants were recruited by adverts on social media university groups and by sending an online link with an invitation for study. After accessing the link, participants read the study description and the informed consent form. Participants who gave their consent, responded to demographic questions and completed the study measures. HPS, PHQ-2, HABS short form, Altman scale, POG, and the positive irrational beliefs measures were included in the present study. Additional measures were completed, such as Positive events scale, Profile of affective distress (Opris and Macavei, 2007), additional irrational beliefs items, and an emotional regulation rating form all which were subjected to different analyses for a second study. To keep a minimal number of items, PHQ-2 scale was selected for this study. The study received ethical approval from the ethical committee of the Faculty of Socio-Humanistic Studies, University of Oradea (approval no 516/15.03.2022).
Data analysis plan
Data analysis plan first involved data screening and preliminary analyses. We used parametric correlational analyses for analysis of the associations between the variables. Linear regression model was used to analyze the prediction of HPS by positive primary irrational beliefs. Principal axis factoring with Promax rotation was used to analyze the structure of thirty-seven positive irrational beliefs items. The factorial, correlational and regression analyses were carried out using IBM SPSS Statistics for Windows, Version 23.0, IBM Corp., Armonk, NY, USA. Multicollinearity analyses showed that all values of the variance inflation factor (VIF) were below the maximum threshold level of 10 (all VIFs < 2) and all tolerance levels were above the value of 0.5. The visual inspection of the P-P plot and scatterplot suggests a normal distribution of residuals and that the data meet the homoscedasticity assumption. Exploratory analyses investigated moderation roles of positive overgeneralizations and the current mood in the relationships between positive irrational beliefs and bipolar vulnerability. The calculated power based on seven predictors yielded an acceptable power (0.826) using a 107 sample and a medium effect size (Statistics Kingdom, 2017).
Results
Descriptive statistics
The means, standard deviation, minimum, and maximum scores for the main study variables (age, depression level, hypo/mania, bipolar vulnerability, irrational beliefs, and positive generalizations) are described in Table 1. Analyses of skewness and kurtosis suggest data met the assumptions of normality (all coefficients were below the cut-off point <1). The Kolmogorov–Smirnov test normality suggest normal distributions (all ps > 0.01) for hypomanic personality, total positive irrational beliefs score, irrational beliefs, sociotropic positive irrational belief, autonomy-related positive irrational beliefs, and positive overgeneralizations but not for positive primary irrational beliefs, Altman Scale, and PHQ-2 scale (all ps > 0.01). Regarding the level of depression, 50.5% (N = 54) of the sample scored above the PHQ-2 cut-off score of 3 or more, suggesting clinical depression (Kroenke et al., 2003). Regarding hypo/manic symptoms, 44.9% (N = 48) of the sample scored above the ASRM cut-off of 6, suggesting the possibility of hypo/mania (Altman et al., 1997).
Correlation analyses
Spearman correlation coefficients Rho between the non-parametrically distributed variables (Altman scale, positive primary irrational beliefs, PHQ-2) and Pearson coefficients for normally distributed variables (HPS, positive generalizations, total positive irrational beliefs, autonomy-related positive irrational beliefs, sociotropic positive irrational beliefs, and total positive irrational beliefs) are described in Table 2. According to our hypotheses, the Hypomanic Personality Scale scores were positively correlated with the level of depression and hypomania, positive generalizations (marginally p = 0.056), irrational beliefs, and with primary irrational beliefs measured in positive situations. Positive primary irrational beliefs or rigid pursuit of goals in positive situations (positive demandingness) (and all types of positive irrational beliefs) were positively associated with scores on the Hypomanic Personality Scale, but not with state measures of hypo/mania and positive generalizations. Irrational beliefs were positively associated with the risk of hypo/mania, depression, and all types of positive irrational beliefs and negatively related to positive generalizations. Although the risk of hypo/mania was significantly related to general irrational beliefs (p = 0.042), we observed no significant relationships between the risk of mania and achievement-related irrational beliefs (p > 0.05). Furthermore, partial correlation analyses showed that controlling for positive primary irrational beliefs yields the relation between irrational beliefs and the risk of hypo/mania non-significant (r = 0.027, p = 0.787).
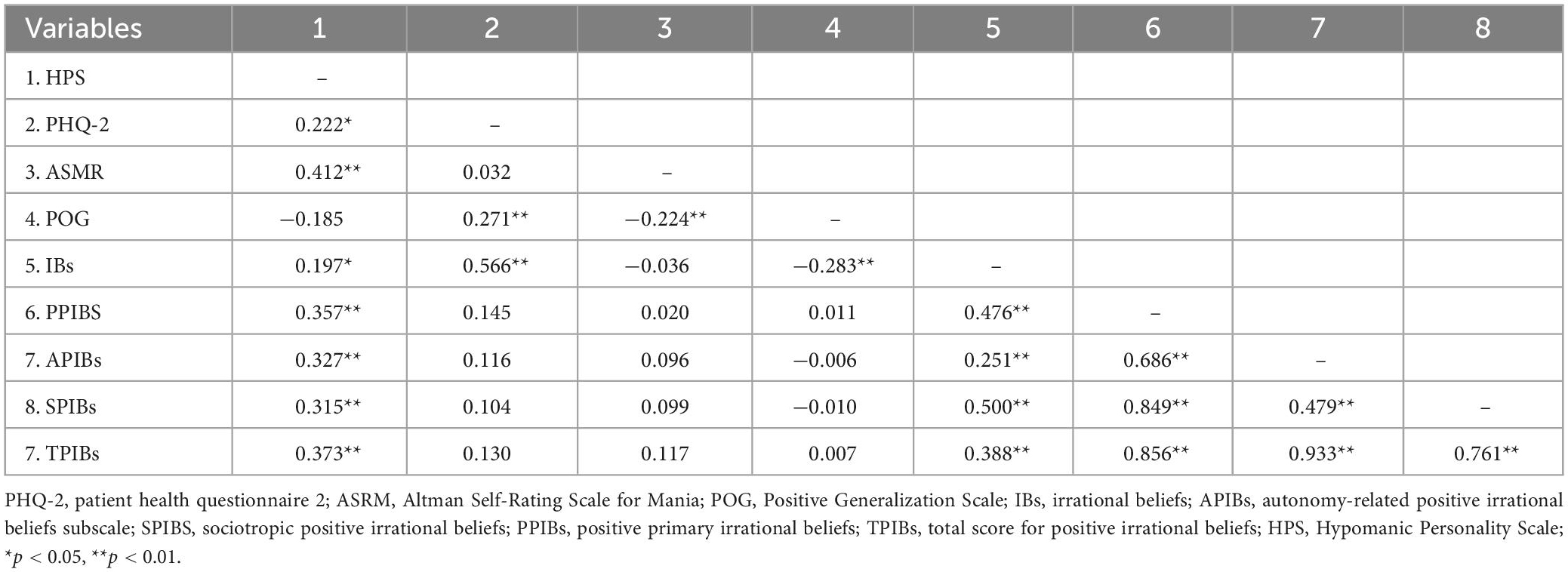
Table 2. Correlation coefficients for the study variables.
Regression analyses
A hierarchical linear regression analysis was used to test the unique contribution of positive primary irrational beliefs to the Hypomanic Personality Scale whilst controlling for participant age, sex, current mood (PHQ-2 and ASRM), positive overgeneralizations, and irrational beliefs. The risk of hypo/mania was significantly related to the general measure of irrational beliefs in negative situations and not to achievement related irrational beliefs. Thus, we used the general irrational beliefs score in the future analyses.
The overall regression model was significant, F(7,98) = 11.686, p < 0.001, and explained 45% of variance in HPS scores. Table 3 details the regression coefficients between the study variables with HPS scores as the outcome.
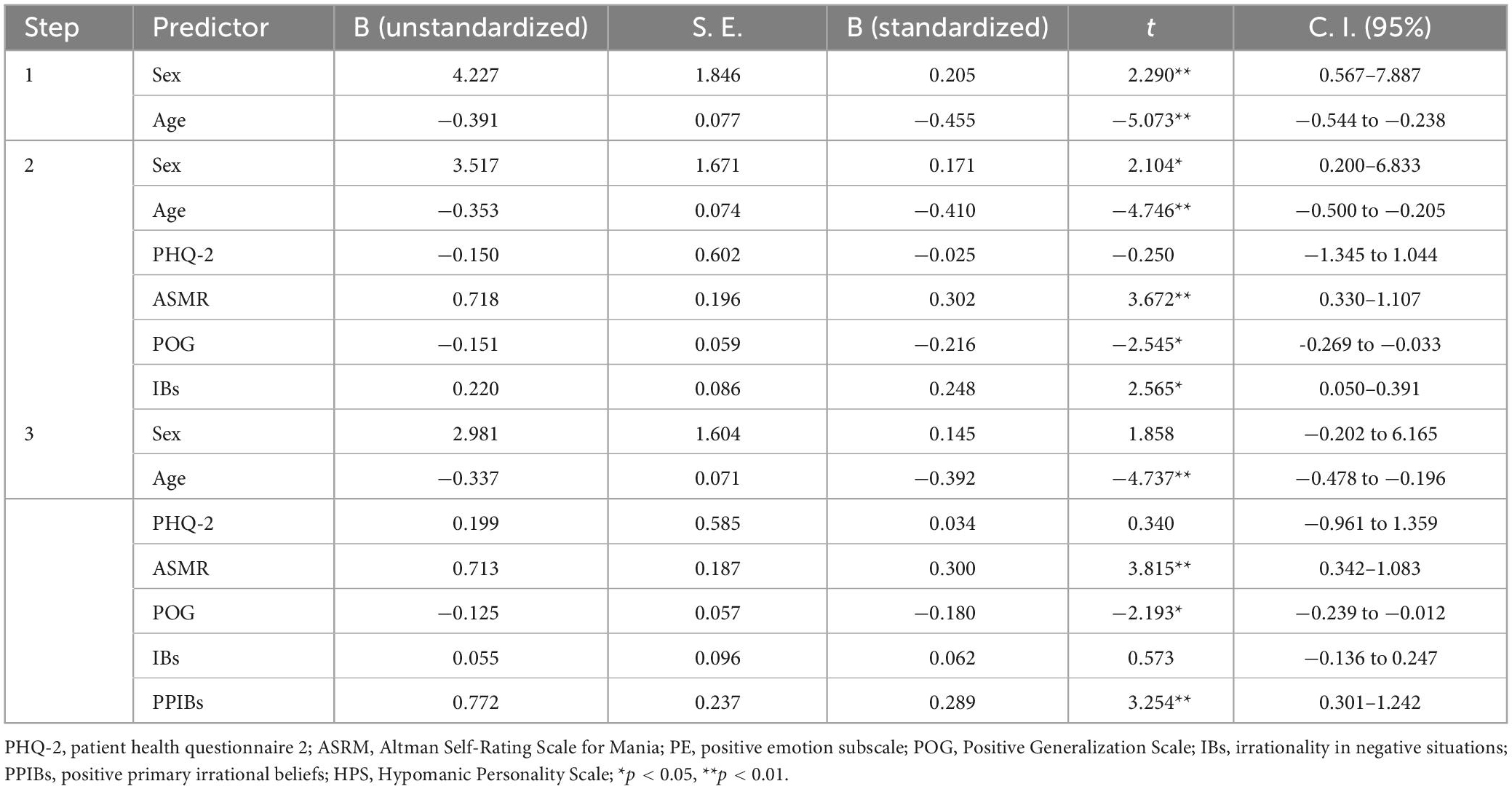
Table 3. Regression analyses of positive primary irrational beliefs predicting hypomanic personality.
In step 1, age and sex variables were entered. In step 2, PHQ-2, ASRM, positive generalizations, and irrationality in negative situations (HABS scale) were added. In step 3, the positive primary irrational beliefs were entered. Adding the ratings for the current mood, positive generation and irrational beliefs in step 2 significantly improved the fit of the model (ΔR2 = 0.187, ΔF(4, 99) = 7.651, p < 0.001), age, current hypomanic mood and positive generalizations significantly predicting the risk for hypomania. Adding positive primary irrational beliefs in step 3 did also significantly improves the fit of the model (ΔR2 = 0.059, ΔF(1, 98) = 10.589, p = 0.002). In the final model, ratings for positive primary irrational beliefs significantly predicted higher the risk for hypomania (β = 0.772, p = 0.002) beyond the current hypomanic mood (β = 0.713, p < 0.001), positive generalizations (β = −0.125, p = 0.031), and irrational beliefs about adverse events (p > 0.05).
As shown in Table 3, positive primary irrational beliefs positively predict HPS scores after controlling for age, participant sex, and current mood symptoms (PHQ-2 and ASRM), positive overgeneralizations and irrational beliefs in response to achievement related negative situations. Positive primary irrational beliefs were a significant positive predictor of HPS scores, showing that increased vulnerability to bipolar disorder is characterized by holding rigid beliefs about the attainment of goals and desires to cues of reaching personal goals.
Ancillary analyses
To check the robustness of the findings, we run the same regression analyses using different measures of positive irrational belief. Results showed that all positive irrational beliefs, such as the global score of positive irrational beliefs (β = 0.083, p = 0.005), sociotropic positive irrational beliefs (β = 0.178, p = 0.030), and autonomy-related positive irrational beliefs (β = 0.097, p = 0.013) predict HPS beyond demographic and mania related variables. Furthermore, we explored potential moderators using the Model 1 of Hayes (2013) PROCESS for SPSS. Thus, we analyzed the moderation of the relationship between positive irrational beliefs and hypomanic personality by potential moderators: positive overgeneralizations and irrational beliefs in negative situations. Similar to previous studies investigating the relationship between dysfunctional dimensions of goals and the hypomanic personality (Dempsey et al., 2020), current mood (hypomanic and depression level) was included as covariate in these analyses. We observed no significant interaction effects between positive overgeneralization (interaction effect p = 0.908) or irrational beliefs in negative situations (interaction effect p = 0.497) and positive primary irrational beliefs in predicting vulnerability for bipolar disorder.
Discussion
This study has investigated whether hypomanic personality, which is a risk factor for bipolar disorder, is associated with primary irrational beliefs (rigid pursuit of goals) in positive situations. Our results demonstrate that the risk of bipolar disorder (hypomanic personality) is associated with irrational beliefs, a well-known trans-diagnostic factor involved in vulnerability for emotional disorders. Especially, we showed that individuals who are more inclined to demand rather than just desire to attain their important goals when cues signal the possibility of goal attainment have higher levels of risk for developing hypo/mania. Although individuals who respond with high levels of irrational beliefs to adverse events have also higher risk of hypo/mania, our results suggest that their increased risk for mania depends on whether they keep responding using irrational demands to positive situations. Current depressed, hypomanic mood, and positive generalizations also characterized vulnerability for bipolar disorder. We found that positive primary irrational beliefs have a unique contribution to bipolar vulnerability beyond mood, positive generalizations, and irrational beliefs related to adversities. To our knowledge, this is the first study to prove that hypomanic personality which is a well-known vulnerability to bipolar disorder is linked to positive primary irrational beliefs. Our results are in line with studies showing a significant goal dysregulation in individuals at risk of bipolar disorder (Johnson et al., 2005; Johnson and Carver, 2006). Previous research showed that individuals with bipolar disorder have higher, perfectionistic, more ambitious goals (Nusslock et al., 2007; Johnson et al., 2012) and goal-striving cognitive style (Francis-Raniere et al., 2006). Moreover, recent research points to significant differences in the drive or how at-risk individuals pursue their goals. For instance, Dempsey et al. (2020) found that the risk of bipolar disorder is associated with higher levels of tenacious pursuit of goals. Both tenacious goal pursuit and positive primary irrational beliefs (e.g., “I must achieve what is important for me”) may be regarded as a form of goal persistence. Thus, it is not surprising that primary irrational beliefs have similar contributions to the risk of psychopathology as tenacious goal pursuit.
Another interpretation of the association between positive irrational beliefs and hypomanic personality is that positive irrational beliefs are cognitive components of hypomanic personality. This interpretation is consistent with the view of primary irrational beliefs as motivational parts of a dysregulated BAS system. Previous research has suggested that primary irrational beliefs (positive demandingness and happiness irrational beliefs) are related to BAS measures (Tiba, 2005; Tiba and Szentagotai, 2005; Yıldırım and Maltby, 2021).Thus, assimilating positive primary irrational beliefs as cognitive components pertaining to the activation of a dysregulated BAS system would explain the association between positive irrational beliefs and the risk of bipolar disorder (Francis-Raniere et al., 2006; Alloy et al., 2009). An oversensitive and dysregulated activity of the BAS has been consistently found in individuals with bipolar disorder (Alloy and Abramson, 2010). Thus, rigidly following goals and desires both in positive and when goals are not met may reflect the activation of BAS. In our study, we did not find a significant relation between the reports of rigidly persisting to attain goals in situations when goals are not met (HABS demandingness) and the risk of hypo/mania. It is possible that irrational beliefs measured by HABS may include persistent avoidance goals that would be related to behavioral inhibition system (BIS) (Tiba, 2005). Yet a visual inspection of the demandingness items from the HABS short form scale do not refer to avoiding aversive situations (e.g., “I should avoid failing at the exam”). Further research should clarify whether rigidly persisting in the pursuit of goals when negative situations block our goals is related or not to the risk of hypo/mania since our results show that general irrational beliefs in negative situations are positively related to the risk of hypo/mania.
Previously, it has been suggested that interventions aiming at reducing tenacious goal pursuit should be added to existing intervention to reduce the risk of bipolar disorder (Nusslock et al., 2009; Dempsey et al., 2020). Our findings suggest that rigid beliefs about attaining goals in response to cues of rewards should also be addressed in order to reduce the risk of developing bipolar disorder. Showing that irrational beliefs are involved in the risk of bipolar disorder brings a major advantage for building interventions for reducing the existing risk for bipolar disorders. There are many studies that consolidate the evidence-base of treatment methods developed for restructuring irrational beliefs (Ellis et al., 2010; David et al., 2018). These methods may be targeted to changing irrational beliefs also in response to positive situations, not only to negative situations. Given that restructuring irrational beliefs may show significant clinical benefits for preventing and reducing depressive episodes (Szentagotai and David, 2010) it may be practical to teach clients to apply similar methods to prevent hypo/manic episodes. However, interventions aiming at changing positive irrational beliefs should undergo empirical clinical tests.
There are several limitations to consider in interpreting the results of the study. The study used validated measures for irrational beliefs and depression. HPS and POG remain to be validated on the Romanian population as the forward and back translations were first made for the present study. Factorial analysis based on current data supported the proposed factorial structure of the scale. We checked for the overlap between measures of HPS and positive irrational beliefs, and found no similar items. Another limitation regards the generalizability of our results to clinical groups. We used a non-clinical sample, with only six participants reporting currently taking medication for affective problems. Similarly, we did not account for family history of depression and bipolar disorder, past depression and other mental illness, or childhood adversity. As these factors could interact with irrational beliefs in determining the risk for bipolar disorder further research should account for them as well. Thus, our conclusions may be interpretable in terms of general population, rather than clinical population. Further research should investigate the role of positive irrational primary beliefs in clinical groups with a diagnosis of bipolar disorder and using longitudinal designs. Similarly, generalizing our results to the male population should be made with caution since 77.6% of our sample was of female participants yet a larger participation of female subjects was expected, since previous studies have typically reported that male sex is associated with non-response to online surveys (Lallukka et al., 2020). Besides these limitations, our results point to primary irrational beliefs in positive situations as a potential route for changing the risk of bipolar disorder and a target for efforts to prevent bipolar disorder.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Faculty of Socio-Humanistic Studies, University of Oradea. The patients/participants provided their written informed consent to participate in this study.
Author contributions
AT designed the study and wrote the protocol. AT, LV, FB, and DM undertook the statistical analysis and wrote the first draft of the manuscript. AT, MD, ST, CB, FB, DM, LV, SI, and SP revised the manuscript. AT, SP, CB, FB, and DM managed the data collection. All authors listed have made a substantial contribution to the work and approved it for publication.
Funding
This research was funded by the University of Oradea, within the Grants Competition “Scientific Research of Excellence Related to Priority Areas with Capitalization through Technology Transfer: INO–TRANSFER–UO,” Project No. 322/2021.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alloy, L. B., Abramson, L. Y., Walshaw, P. D., Gerstein, R. K., Keyser, J. D., Whitehouse, W. G., et al. (2009). Behavioral Approach System (BAS)–relevant cognitive styles and bipolar spectrum disorders: Concurrent and prospective associations. J. Abnorm. Psychol. 118, 459–471. doi: 10.1037/a0016604
Alloy, L. B., and Abramson, L. Y. (2010). The role of the Behavioral Approach System (BAS) in bipolar spectrum disorders. Curr. Dir. Psychol. Sci. 19, 189–194. doi: 10.1177/0963721410370292
Altman, E. G., Hedeker, D., Peterson, J. L., and Davis, J. M. (1997). The altman self-rating mania scale. Biol. Psychiatry 42, 948–955. doi: 10.1016/s0006-3223(96)00548-3
Bernard, M. E. (1998). Validation of the general attitude and belief scale. J. Ration. Emot. Cogn. Behav. Ther. 16, 183–196. doi: 10.1023/a:1024911014579
Chiang, K. J., Tsai, J. C., Liu, D., Lin, C. H., Chiu, H. L., and Chou, K. R. (2017). Efficacy of cognitive-behavioral therapy in patients with bipolar disorder: A meta-analysis of randomized controlled trials. PLoS One 12:e0176849. doi: 10.1371/journal.pone.0176849
David, D. O., DiGiuseppe, R., Dobrean, A., Pǎsǎrelu, C. R., and Balazsi, R. (2019). “The measurement of irrationality and rationality,” in Advances in REBT: Theory, practice, research, measurement prevention and promotion, eds M. E. Bernard and W. Dryden (Cham: Springer), 79–100. doi: 10.1007/978-3-319-93118-0_4
David, D., Cotet, C., Matu, S., Mogoase, C., and Stefan, S. (2018). 50 years of rational-emotive and cognitive-behavioral therapy: A systematic review and meta-analysis. J. Clin. Psychol. 74, 304–318. doi: 10.1002/jclp.22514
Dempsey, R. C., Eardley, K., and Dodd, A. L. (2020). The role of tenacious versus flexible goal pursuit in the vulnerability to bipolar disorder. Curr. Psychol. 41, 2382–2389. doi: 10.1007/s12144-020-00748-7
DiGiuseppe, R., Gorman, B., and Raptis, J. (2020). The factor structure of the attitudes and beliefs scale 2: Implications for rational emotive behavior therapy. J. Ration. Emot. Cogn. Behav. Ther. 38, 111–142. doi: 10.1007/s10942-020-00349-0
DiGiuseppe, R., Gorman, B., Raptis, J., Agiurgioaei-Boie, A., Agiurgioaei, F., Leaf, R., et al. (2021). The development of a short form of an irrational/rational beliefs scale. J. Ration. Emot. Cogn. Behav. Ther. 39, 456–490. doi: 10.1007/s10942-021-00386-3
DiGiuseppe, R., Leaf, R., Exner, T., and Robin, M. W. (1988). “The development of a measure of irrational/rational thinking,” in Poster at the world congress of behavior therapy, Edinburgh.
Dryden, W. (2019). “The distinctive features of rational emotive behavior therapy,” in Advances in REBT, eds M. Bernard and W. Dryden (Cham: Springer). doi: 10.1007/978-3-319-93118-0_2
Eckblad, M., and Chapman, L. J. (1986). Development and validation of a scale for hypomanic personality. J. Abnorm. Psychol. 95, 214–222. doi: 10.1037/0021-843X.95.3.214
Eisner, L. R., Johnson, S. L., and Carver, C. S. (2008). Cognitive responses to failure and success relate uniquely to bipolar depression versus mania. J. Abnorm. Psychol. 117:154. doi: 10.1037/0021-843X.117.1.154
Ellis, A. (1994). Reason and emotion in psychotherapy: Revised and updated. New York, NY: Birch Lane.
Ellis, A., David, D., and Lynn, S. J. (2010). “Rational and irrational beliefs: A historical and conceptual perspective,” in Rational and irrational beliefs: Research, theory, and clinical practice, eds D. David, S. J. Lynn, and A. Ellis (Oxford: Oxford University Press), 3–22.
Francis-Raniere, E. L., Alloy, L. B., and Abramson, L. Y. (2006). Depressive personality styles and bipolar spectrum disorders: Prospective tests of the event congruency hypothesis. Bipolar Disord. 8, 382–399. doi: 10.1111/j.1399-5618.2006.00337.x
Gruber, J., Johnson, S. L., Oveis, C., and Keltner, D. (2008). Risk for mania and positive emotional responding: Too much of a good thing? Emotion (Washington, D.C.) 8, 23–33. doi: 10.1037/1528-3542.8.1.23
Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. New York, NY: Guilford Press.
Hyland, P., Shevlin, M., Adamson, G., and Boduszek, D. (2014). Modeling the structure of the attitudes and belief scale 2 using CFA and bifactor approaches: Toward the development of an abbreviated version. Cogn. Behav. Ther. 43, 60–71. doi: 10.1080/16506073.2013.777467
Johnson, S. L. (2005). Mania and dysregulation in goal pursuit: A review. Clin. Psychol. Rev. 25, 241–262. doi: 10.1016/j.cpr.2004.11.002
Johnson, S. L., and Carver, C. S. (2006). Extreme goal setting and vulnerability to mania among undiagnosed young adults. Cogn. Ther. Res. 30, 377–395. doi: 10.1007/s10608-006-9044-7
Johnson, S. L., Carver, C. S., and Fulford, D. (2010). “Goal dysregulation in the affective disorders” in Emotion Regulation and psychopathology: A transdiagnostic approach to etiology and treatment, eds A. M. Kring and D. M. Sloan (New York, NY: The Guilford Press), 204–228.
Johnson, S. L., Fulford, D., and Carver, C. S. (2012). The double-edged sword of goal engagement: Consequences of goal pursuit in bipolar disorder. Clin. Psychol. Psychother. 19, 352–362. doi: 10.1002/cpp.1801
Johnson, S. L., Ruggero, C. J., and Carver, C. S. (2005). Cognitive, behavioral, and affective responses to reward: links with hypomanic symptoms. J. Soc. Clin. Psychol, 24, 894–906. doi: 10.1521/jscp.2005.24.6.894
Johnson, S. L., Sandrow, D., Meyer, B., Winters, R., Miller, I., Solomon, D., et al. (2000). Increases in manic symptoms after life events involving goal attainment. J. Abnorm. Psychol. 109, 721–727. doi: 10.1037/0021-843X.109.4.721
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2003). The patient health questionnaire-2: Validity of a two-item depression screener. Med. Care 41, 1284–1292. doi: 10.1097/01.MLR.0000093487.78664.3C
Lallukka, T., Pietiläinen, O., Jäppinen, S., Laaksonen, M., Lahti, J., and Rahkonen, O. (2020). Factors associated with health survey response among young employees: A register-based study using online, mailed and telephone interview data collection methods. BMC Public Health 20:184. doi: 10.1186/s12889-020-8241-8
Leahy, R. L., and Beck, A. T. (1988). “Cognitive therapy of depression and mania,” in Depression and mania, eds R. Cancro and R. Georgotas (New York, NY: Elsevier).
Macavei, B., and McMahon, J. (2010). “The assessment of rational and irrational beliefs,” in Rational and irrational beliefs: Research, theory, and clinical practice, eds D. David, S. J. Lynn, and A. Ellis (Oxford: Oxford University Press), 115–147.
Miklowitz, D. J., Efthimiou, O., Furukawa, T. A., Scott, J., McLaren, R., Geddes, J. R., et al. (2021). Adjunctive psychotherapy for bipolar disorder: A systematic review nd component network meta-analysis. JAMA Psychiatry 78, 141–150. doi: 10.1001/jamapsychiatry.2020.2993
Nusslock, R., Abramson, L. Y., Harmon-Jones, E., Alloy, L. B., and Hogan, M. E. (2007). A goal-striving life event and the onset of hypomanic and depressive episodes and symptoms: Perspective from the Behavioral Approach System (BAS) dysregulation theory. J. Abnorm. Psychol. 116, 105–115. doi: 10.1037/0021-843X.116.1.105
Nusslock, R., Abramson, L., Harmon-Jones, E., Alloy, L., and Coan, J. (2009). Psychosocial interventions for bipolar disorder: Perspective from the Behavioral Approach System (BAS) dysregulation theory. Clin. Psychol. Sci. Pract. 16, 449–469. doi: 10.1111/j.1468-2850.2009.01184.x
Opris, D., and Macavei, B. (2007). The profile of emotional distress; norms for the Romanian population. J. Evid. Based Psychother. 7:139. doi: 10.3892/etm.2020.8806
Statistics Kingdom (2017). Statistical power calculator [Internet]. Available online at: http://www.statskingdom.com//33test_power_regression.html (accessed February 23, 2023).
Szentagotai, A., and David, D. (2010). The efficacy of cognitive-behavioral therapy in bipolar disorder: A quantitative meta-analysis. J. Clin. Psychiatry 71, 66–72.
Tiba, A. (2005). Demanding brain; between should and shouldn’t. J. Cogn. Behav. Psychother. 5, 43–53.
Tiba, A. I. (2010). A grounded cognition perspective on irrational beliefs in rational emotive behavior therapy. J. Cogn. Behav. Psychother. 10, 87–99.
Tiba, A. I., and Manea, L. (2018a). The vividness of imagining emotional feelings is attenuated in dysphoria and predicts the experience of positive emotional feelings. J. Clin. Psychol. 74, 2238–2263. doi: 10.1002/jclp.22676
Tiba, A. I., and Manea, L. (2018b). The embodied simulation account of cognition in rational emotive behavior therapy. New Ideas Psychol. 48, 12–20. doi: 10.1016/j.newideapsych.2017.08.003
Tiba, A., and Szentagotai, A. (2005). Positive emotions and irrational beliefs. Dysfunctional positive emotions in healthy individuals. J. Cogn. Behav. Psychother. 5, 53–73.
Tiba, A., Johnson, C., and Vǎdineanu, A. (2012). Cognitive vulnerability and adjustment to having a child with a disability in parents of children with autistic spectrum disorder. J. Cogn. Behav. Psychother. 12, 209–218. doi: 10.1186/s11689-021-09363-4
Trip, S., McMahon, J., Bora, C., and Chipea, F. (2010). The efficiency of a Rational Emotive and Behavioral Education program in diminishing dysfunctional thinking, behaviors and emotions in children. J. Evid. Based Psychother. 10:173.
Vigo, D., Thornicroft, G., and Atun, R. (2016). Estimating the true global burden of mental illness. Lancet Psychiatry 3, 171–178. doi: 10.1016/S2215-0366(15)00505-2
Vîslã, A., Flückiger, C., Grosse Holtforth, M., and David, D. (2016). Irrational beliefs and psychological distress: A meta-analysis. Psychother. Psychosom. 85, 8–15. doi: 10.1159/000441231
Ye, B. Y., Jiang, Z. Y., Li, X., Cao, B., Cao, L. P., Lin, Y., et al. (2016). Effectiveness of cognitive behavioral therapy in treating bipolar disorder: An updated meta-analysis with randomized controlled trials. Psychiatry Clin. Neurosci. 70, 351–361. doi: 10.1111/pcn.12399
Yesilyaprak, N., Batmaz, S., Yildiz, M., Songur, E., and Akpinar Aslan, E. (2019). Automatic thoughts, cognitive distortions, dysfunctional attitudes, core beliefs, and ruminative response styles in unipolar major depressive disorder and bipolar disorder: A comparative study. Psychiatry Clin. Psychopharmacol. 29, 854–863. doi: 10.1080/24750573.2019.1690815
Keywords: irrational beliefs, depression, hypomania, REBT, risk, mania and bipolar disorder
Citation: Tiba AI, Trip S, Bora CH, Drugas M, Borz F, Miclăuş DC, Voss L, Iova SC and Pop S (2023) Positive irrational beliefs are associated with hypomanic personality. Front. Psychol. 14:1053486. doi: 10.3389/fpsyg.2023.1053486
Received: 25 September 2022; Accepted: 06 March 2023;
Published: 20 March 2023.
Edited by:
Huiyuan Huang, Guangzhou University of Chinese Medicine, ChinaReviewed by:
Francisco Welington Lima, Federal University of Piauí, BrazilRavi Philip Rajkumar, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), India
Copyright © 2023 Tiba, Trip, Bora, Drugas, Borz, Miclăuş, Voss, Iova and Pop. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandru I. Tiba, YWxleGFuZHJ1dGliYUBnbWFpbC5jb20=