 Rakshya Sharma
Rakshya Sharma Hari Prasad Kaphle
Hari Prasad Kaphle- School of Health and Allied Sciences, Pokhara University, Pokhara, Nepal
Introduction: Intimate partner violence during pregnancy (IPVDP) is increasingly being recognized as a significant problem in the developing world due to its adverse health consequences on both pregnant women and children. The objective of the study is to measure the magnitude of intimate partner violence during pregnancy and the factors associated with IPVDP.
Methods: A community-based cross-sectional study was conducted among 263 married women in their extended postpartum period between October 2019 and March 2020 in Putalibajar municipality, Nepal. A face-to-face interview was conducted and data were collected using an interview schedule. A Chi-square test and logistic regression analysis were performed to examine the association between IPVDP and the independent variables.
Results: Among the 263 women interviewed, 30% experienced IPV during pregnancy, the most common type of violence was controlling behavior (20.2%) followed by emotional (18.6%), sexual (10.6%), economic (6.1%), and physical violence (5.3%). It was observed that IPV was more likely to occur among women whose husbands consumed alcohol (AOR = 3.171; CI 95%: 1.588–9.167), women whose husbands consumed tobacco (AOR =3.815; CI 95%: 2.157–7.265), women who sometimes received family support during pregnancy (AOR =2.948; CI 95%: 1.115–7.793) and women who did not decide on marriage timing (AOR =2.777; CI 95%: 1.331–5.792).
Conclusion: Three out of ten pregnant women experienced IPVDP. To prevent violence, and ensure women’s empowerment, formulating strict laws and discouraging the element of a violent milieu is important.
Introduction
Intimate partner violence (IPV) is defined as any act of physical, sexual, or psychological controlling actions or economic violence that takes place between intimate partners. It is regarded as global public health and human rights issue (García-Moreno et al., 2005). Globally, 30% of women experience violence by their intimate partner (García-Moreno et al., 2013). In recent years, intimate partner violence during pregnancy (IPVDP) is increasingly being recognized as a significant problem in the world due to its prevalence and its adverse health consequences on both pregnant women and children. The World Health Organization (WHO) estimated that, globally, the proportion of ever-pregnant women who reported violence during pregnancy varied from 1 to 28%. Physical violence exceeded 5% in 11 out of 15 settings where one-half of the women reported being punched or kicked in the abdomen and the majority (90%) of abuse was perpetrated by the biological father of the child she was carrying (García-Moreno et al., 2005).
Women experiencing violence during pregnancy are less likely to receive prenatal care and may experience adverse health outcomes such as poor nutrition, miscarriage, premature labor, trauma, placenta abruption, low birth weight (LBW), stillbirth, UTI, Chronic Pelvic infection, depression, and maternal death (García-Moreno et al., 2005; Nejatizade et al., 2017; Regmi et al., 2017). Nepal is a diverse ecological, ethnic, cultural, and multi-language society but is predominantly a Hindu country where it has its own cultural practices, norms, and values regarding men and women. In the context of Nepal, the key structural factors that make women vulnerable to IPV are economic dependency on men, cultural obligations, early marriage, giving birth to a girl, dowry practices, and lower social position which constructs and reinforces male dominance in society (Office of the Prime Minister and Council of Ministers, 2012; Deuba et al., 2016; Gurung and Acharya, 2016).
According to the Nepal Demographic Health Survey (NDHS) 2016, 26% of ever-married women have ever experienced physical, sexual, or emotional violence at the hands of their husbands. Of the 6% of women who have ever been pregnant and experienced physical violence during pregnancy, the majority of them experienced violence that was perpetrated by their current husbands (Ministry of Health Nepal, 2016). Studies conducted in Nepal showed a significant prevalence of IPVDP, 28.9% in Dhanusha and 53.2% in Kathmandu (Regmi et al., 2017; Singh et al., 2018). The aim of the study was to identify the magnitude of IPVDP and the factors associated with IPVDP.
Methodology
Study design and population
A community-based cross-sectional analytical study was carried out among 263 married women aged 15 to 49 years who had at least one child aged 12 months and younger in Putalibajar municipality, Gandaki Province, Nepal from October 2019 to March 2020. The sample size was calculated by using the finite population formula:
A sample size of 263 was determined based on a 28.9% prevalence of IPVDP from a previous study conducted in Dhanusha, Nepal, with a 10% non-response rate and an estimated population of children aged 0–11 months in 2075/76 (2018/2019) of Putalibajar municipality (N) of 954 (Singh et al., 2018). Married women aged 15 to 49 years who had at least one child aged 12 months or younger were eligible for the study but mothers who were temporary residents, who refused to participate, who had no contact with their husband during the period of pregnancy, who could not answer, and who did not understand the Nepali language were excluded. A multi-stage random sampling technique was followed where 4 out of 14 wards were selected using a simple random technique; participants from each selected ward were determined proportionately based on the sample population. Finally, a systematic random sampling technique was carried out to select individual study participants where the sampling interval (K) was determined by dividing the total population size by the sample size.
Data collection and quality control
A face-to-face interview was carried out using an interview schedule to gather the information. To ensure the validity of the study, a tool was developed by using a standard questionnaire on IPVDP from the instrument of the WHO multi-country study questionnaire (García-Moreno et al., 2005). The Cronbach’s alpha values for the physical and psychological IPV scales of the WHO multi-country study questionnaire were 0.78 and 0.75, respectively, in a study conducted in Bangladesh (Islam et al., 2017). Reliability was ensured by pretesting the tool among 10% of the estimated sample size. The tool was developed in both English and Nepali language.
Variables
The interview schedule included questions about socio-demographic characteristics such as family type, ethnicity, religion, the main occupation of the family, the woman’s age, education, and involvement in an income-generating activity. The participants also provided information about their partner’s characteristics such as age, education, involvement in an income-generating activity, substance use, gambling, presence of polygamy, and partner’s preference for the specific sex of their child. Obstetric and reproductive characteristics such as age at marriage, type of marriage, the decision on marriage timing, duration of the marriage, gravida, previous history of miscarriage or induced abortion, number of living children, pregnancy intention, family support, and timing of 1st antenatal care (ANC) visit.
The dependent variable (IPVDP) was measured through a structured questionnaire regarding physical, sexual, emotional, and economic violence and controlling behavior from the instrument of the WHO multi-country study (García-Moreno et al., 2005). Participants answered yes or no whether they have experienced each of five forms of IPV.
Data analysis
Data entry was done using EPI-DATA and data analysis was done using SPSS. Descriptive statistics were used to describe the study population, which included means, ranges, frequencies, and percentages. The first step in the analysis was to find out the association between IPVDP and independent variables using the chi-square test. Variables that were significant in the chi-square test with a value of p < 0.05 were further analyzed by using bivariate and multivariate logistic regression to assess the strength of the association.
Ethical consideration
The study was given ethical approval by the Nepal Health Research Council (NHRC). The 2001 guidelines of Ethical and Safety Recommendations for Research on Domestic Violence against Women by the WHO were followed (World Health Organization, 2001). The participants were fully informed about the nature and benefits of the research and full informed consent was taken prior to the conduction of the interview. The participants were informed about the rights of women under the law regardless of their experience of violence. If a woman needed help, contact was made with support institutions or police stations only after the woman’s consent had been obtained.
Results
Socio-demographic characteristics
Out of 263 participants, more than half of the respondents [146 (55.5%)] were between 25 and 34 years old. Of the upper caste group 117(44.5%) belonged to Hindu 228(86.7%). The mean age of the participants was 27 years (SD ± 4.9). Nearly all respondents were literate [256 (97.3%)], and nearly half [125(47.5%)] of the participants belonged to a nuclear family. The majority of the participants’ husbands were aged between 25 and 34 years [168(63.9%)]. The mean age of the participants’ husbands was 30 years old (SD ± 5.4), and ranged from 19 to 51 years. Almost all the participants’ husbands were literate [261(99.2%)] and were involved in any type of income-generating activity [246(93.5%); Table 1].
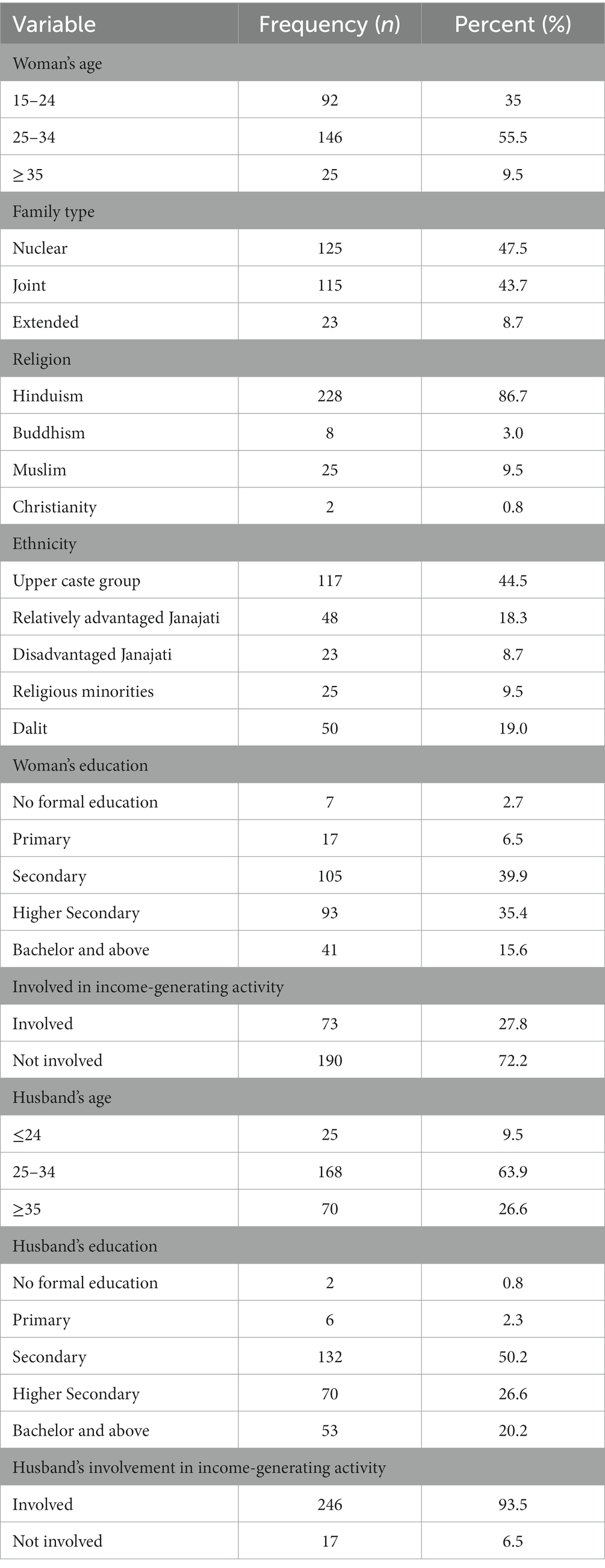
Table 1. Socio-demographic characteristics.
Magnitude of IPVDP
Out of 263 participants, 79 (30%) experienced any kind of IPVDP. The most common type of IPV faced by the participants among the different forms of violence was controlling behavior [53(67.1%)], followed by emotional [49(62.0%)], sexual [28(35.4%)], economic [16(20.3%)], and physical violence [14(17.7%)].
Association between variables and IPVDP
Association between socio-demographic characteristics and IPVDP
Intimate partner violence during pregnancy was significantly associated with family size (p < 0.01), ethnicity (p < 0.01), the main occupation of the family (p < 0.05), and women’s education (p < 0.05; Table 2).
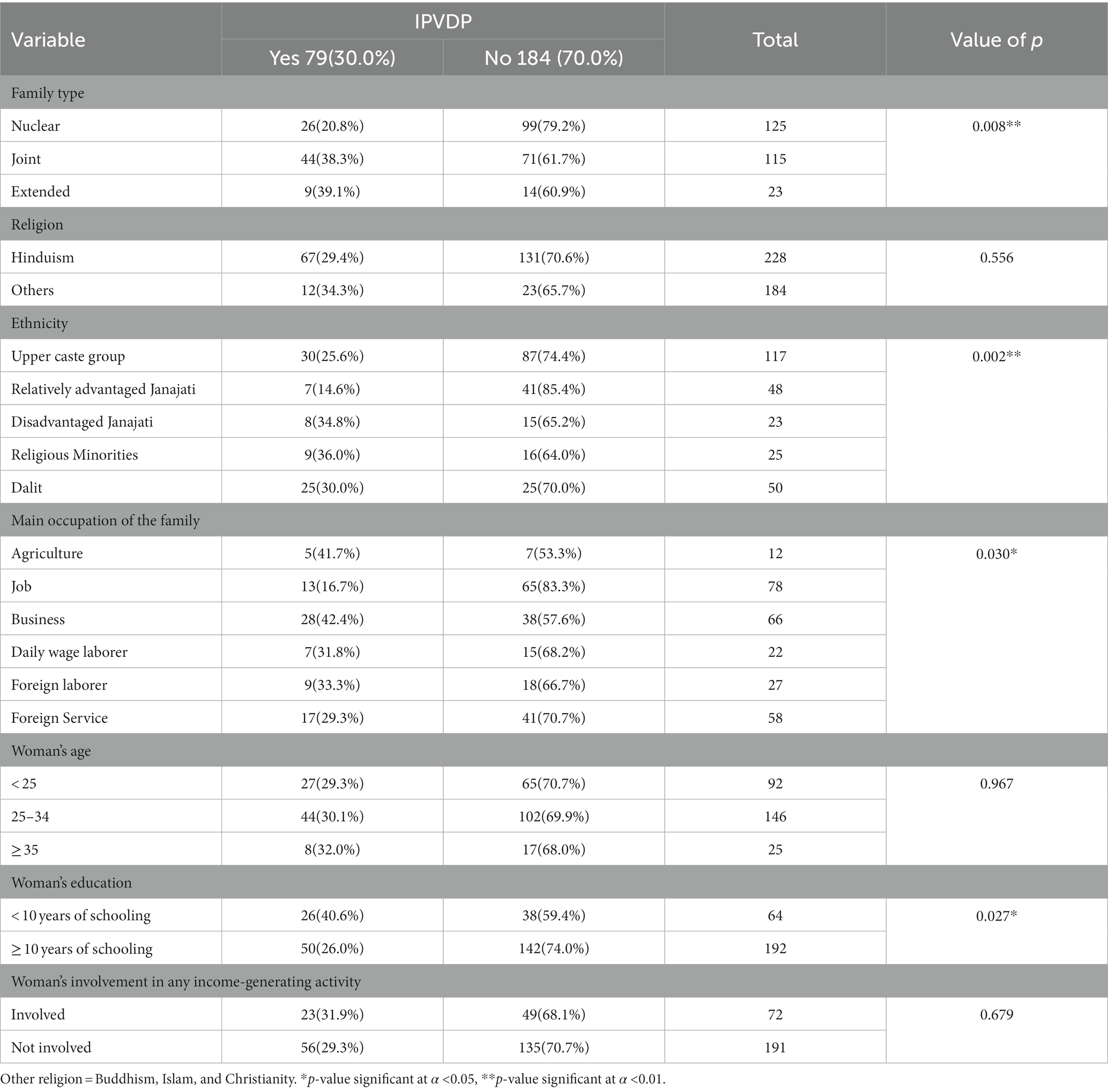
Table 2. Association between socio-demographic characteristics of participants and Intimate partner violence during pregnancy (IPVDP).
Association between the participants’ husband’s characteristics and IPVDP
IPVDP was strongly associated with the husband’s alcohol consumption, frequency of alcohol consumption, and the husband’s tobacco consumption (p < 0.001). Similarly, family support during pregnancy and the husband’s involvement in gambling were also associated with IPVDP (p < 0.01; Table 3).
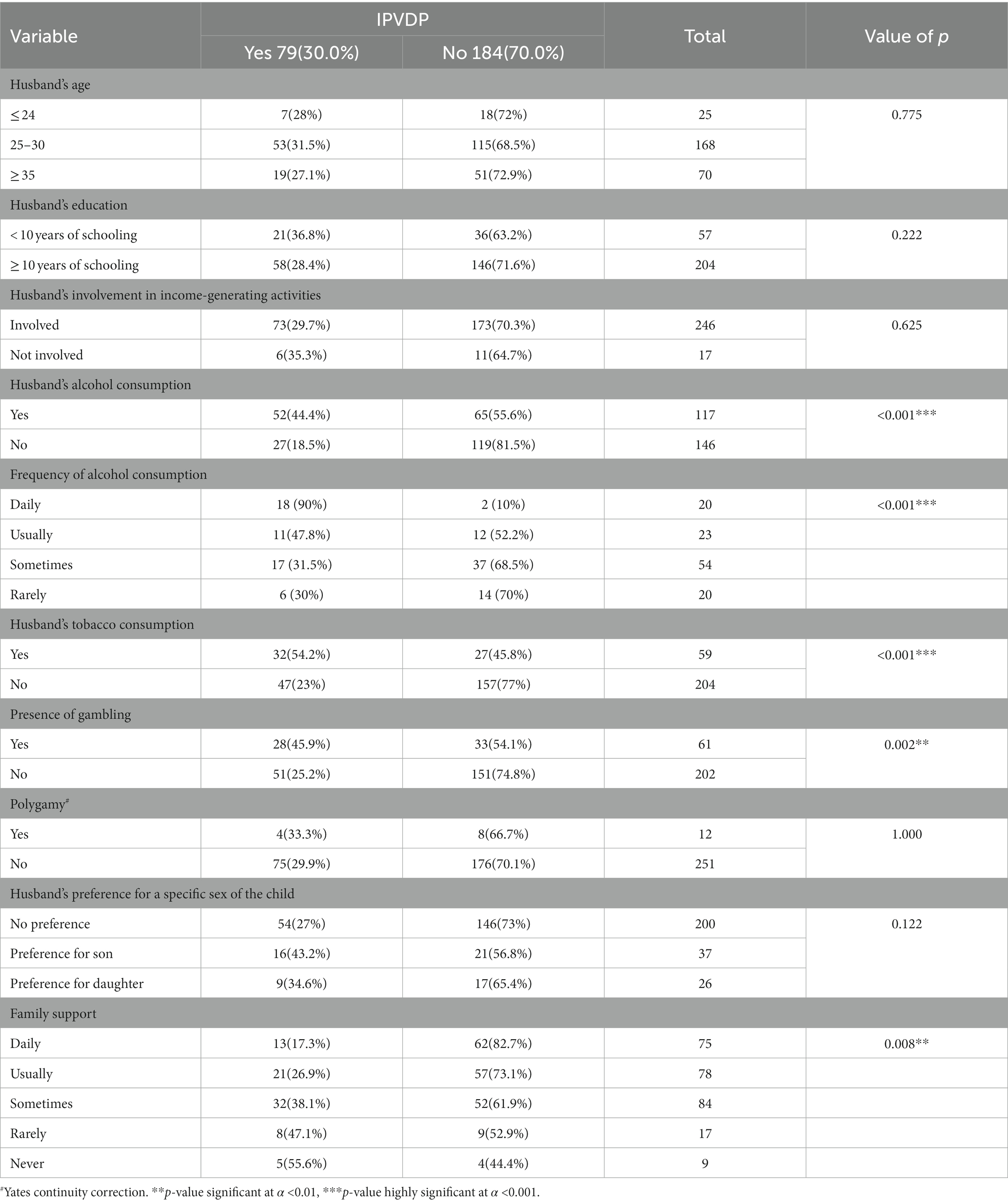
Table 3. Association between participants’ husband’s characteristics and IPVDP.
Association between obstetric and reproductive characteristics and IPVDP
IPVDP was significantly associated with decisions about marriage timing by the participants (p < 0.01) and family support during pregnancy (p < 0.001; Table 4).
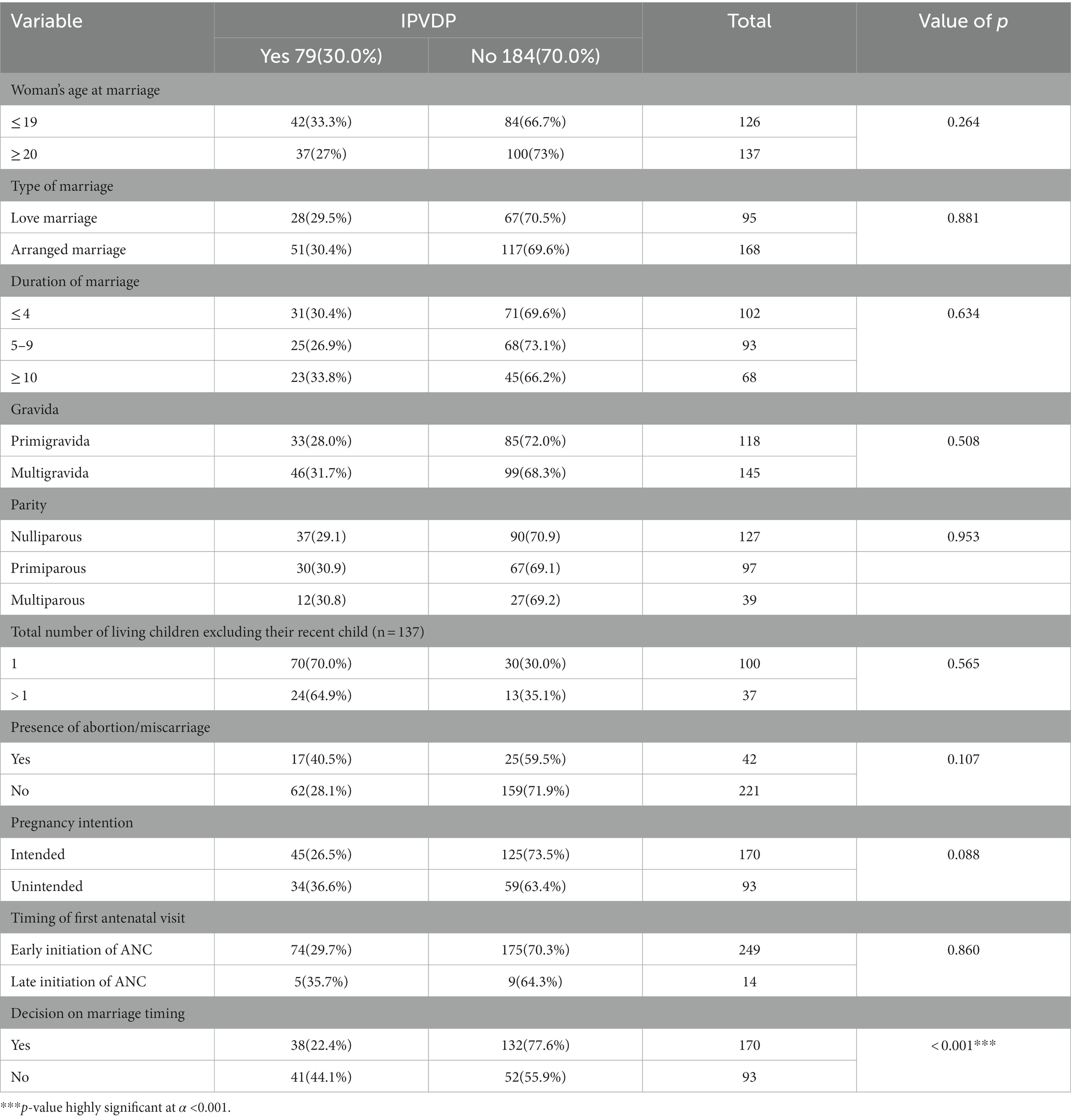
Table 4. Association between IPVDP and obstetric and reproductive characteristics.
Bivariate and multivariate logistic regression analysis between IPVDP and selected variables
In multivariate logistic regression analysis, after adjusting for potential confounding factors, IPV was significantly associated with the husband’s alcohol consumption (AOR = 3.171; CI 95%:1.454 – 6.912), husband’s tobacco consumption (AOR = 3.815; CI 95%:1.588 – 9.167). Similarly, women who reported receiving family support only sometimes during their pregnancy were more likely to experience IPV in comparison to women who received family support on a daily basis (AOR = 2.948; CI 95%:1.115–7.793), and women who did not decide upon their marriage timing (AOR = 2.777; CI 95%:1.331–5.792) were more likely to experience IPVDP (Table 5).
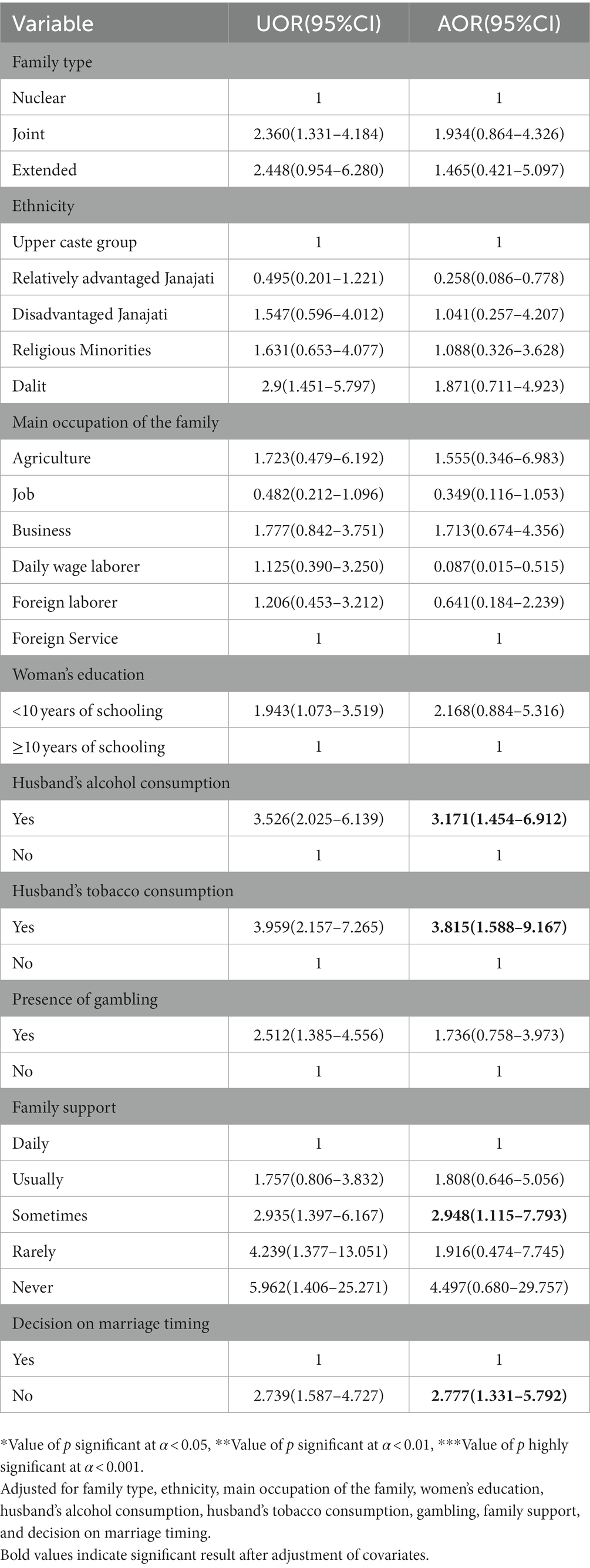
Table 5. Bivariate and multivariate logistic regression analysis between IPVDP and selected variables.
Discussion
The prevalence of IPVDP in this study was 30% among the 263 participants, which is consistent with another study from Dhanusha, Nepal, showing a prevalence of 28.9%. This may be due to the similarities in the population based on the setting (Singh et al., 2018). The prevalence figures of this study were also consistent with the global prevalence of IPVDP estimated by the WHO in a multi-country study (García-Moreno et al., 2005).
However, our prevalence figure is lower than that of other studies conducted in Ethiopia (Abebe Abate et al., 2016), Nigeria (Ezeudu et al., 2019), Vietnam (Hoang et al., 2016), Kenya (Makayoto et al., 2013), Rwanda (Ntaganira et al., 2008), South Korea (Lee and Lee, 2018), and Gambia (Idoko et al., 2015) but higher than the studies conducted in Belgium (Van Parys et al., 2014) Japan (Doi et al., 2019), South Africa (Groves et al., 2012), Guatemala (Johri et al., 2011), and India (Jain et al., 2017). Such a difference may be attributed due to the differences in methodologies, population, and assessments that have been used in the previous research. A strong association was found between alcohol use by the husband and the experience of IPVDP by women. Consistent with our findings, strong links have been found between alcohol use and the occurrence of IPV in many countries such as India (Das et al., 2013), Kenya (Makayoto et al., 2013; Owaka et al., 2017), Rwanda (Ntaganira et al., 2008), Brazil (Teixeira et al., 2015), and Zimbabwe (Shamu et al., 2013).
Our study showed that women whose husbands consumed alcohol were more than three times more likely to experience violence than women whose husbands did not consume alcohol. Studies from other countries showed that women who had partners who drank alcohol were more than two times as likely in Kenya (Makayoto et al., 2013), and four times as likely in Rwanda (Ntaganira et al., 2008), to experience violence. This might be explained due to the low-socio-economic status of the family, societal beliefs, or the impulsive personality of the husband, which accounts for an unhappy and stressful partnership, thus resulting in violence. However, our study does not determine that the increased stress from the use of alcohol leads to IPV or that the abuse of alcohol is a result of the stress of IPV but the association is significant.
Women whose husbands consumed tobacco were more than three times more likely to experience violence than women whose husbands did not consume tobacco. Similar to our finding, a study conducted in Iran showed an association between a smoking partner and psychological violence during pregnancy where women whose partner smoked were more than two times more likely to experience violence during pregnancy (Hajikhani Golchin et al., 2014). However, this study took only one type of violence to show their association while in our study, the association was shown with the experience of any type of violence as a whole.
A significant association was found between family support and IPVDP. Our study revealed that women who never received any assistance from family members in taking care of them during pregnancy or helping with household chores were almost six times more likely to experience violence during pregnancy. Similar literature on this topic was not found in previous studies. However, this variable is very important since pregnancy is a time when women need more care and support from their families. No support during this period might cause quarreling and violence in the family. However, our study does not determine that a lack of care during pregnancy led to the generation of a stressful relationship between the woman and their intimate partner or that the experience of IPV led to a lack of care during pregnancy but there remains a strong association.
Similarly, a strong association was found between the woman’s decision on marriage timing and the experience of IPVDP. Our study showed that women who did not decide upon their marriage timing were more than two times more likely to experience IPVDP.
Conclusion
Our results demonstrate that in Putalibajar municipality, Syangja, three out of ten women experienced IPVDP. Controlling behavior inflicted by the husband was the most common type of violence followed by emotional, sexual, economic, and physical violence. To prevent violence, educating young people about respectful relationships, ensuring women’s empowerment by focusing on higher education opportunities as well as discouraging the element of a violent milieu are important. Appropriate laws prohibiting violence against women and actions regarding screening of IPVDP at antenatal visits with proper management and referral to relevant care are needed.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by IRC, Pokhara University Research Center and ERB, Nepal Health Research Council. The patients/participants provided their written informed consent to participate in this study.
Author contributions
RS and HPK: conceptualization, data curation, formal analysis, methodology, visualization, and writing—review and editing. RS: funding acquisition, investigation, and writing—original draft. HPK: supervision and validation. All authors contributed to the article and approved the submitted version.
Funding
This research has been funded by Nepal Health Research Council with Under Graduate Health Grant.
Acknowledgments
The authors would like to acknowledge the School of Health and Allied Science, Pokhara University for giving this opportunity to conduct research. The authors’ deep gratitude to the Institutional Review Committee, PURC, and all the participants of the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abebe Abate, B., Admassu Wossen, B., and Tilahun, D. T. (2016). Determinants of intimate partner violence during pregnancy among married women in Abay Chomen district, Western Ethiopia: a community based cross sectional study. BMC Womens Health 16:16. doi: 10.1186/s12905-016-0294-6
Das, S., Bapat, U., Shah More, N., Alcock, G., Joshi, W., Pantvaidya, S., et al. (2013). Intimate partner violence against women during and after pregnancy: a cross-sectional study in Mumbai slums. BMC Public Health 13:817. doi: 10.1186/1471-2458-13-817
Deuba, K., Mainali, A., Alvesson, H. M., and Karki, D. K. (2016). Experience of intimate partner violence among young pregnant women in urban slums of Kathmandu Valley, Nepal: a qualitative study. BMC Womens Health 16:11. doi: 10.1186/s12905-016-0293-7
Doi, S., Fujiwara, T., and Isumi, A. (2019). Development of the intimate partner violence during pregnancy instrument (IPVPI). Front. Public Health 7:43. doi: 10.3389/fpubh.2019.00043
Ezeudu, C. C., Akpa, O., Waziri, N. E., Oladimeji, A., Adedire, E., Saude, I., et al. (2019). Prevalence and correlates of intimate partner violence, before and during pregnancy among attendees of maternal and child health services, Enugu, Nigeria: mixed method approach, January 2015. Pan Afr. Med. J. 32:14. doi: 10.11604/pamj.supp.2019.32.1.13287
García-Moreno, C., Jansen, H., Ellsberg, M., Heise, L., and Watts, C.. WHO Multi-country Study on Women’s Health and Domestic Violence Against Women. Geneva: World Health Organization. (2005); 204:1–18.
García-Moreno, C., Pallitto, C., Devries, K., Stöckl, H., Watts, C., and Abrahams, N.. Global and Regional Estimates of Violence Against Women: Prevalence and Health Effects of Intimate Partner Violence and Non-partner Sexual Violence. Geneva: World Health Organization; (2013).
Groves, A. K., Kagee, A., Maman, S., Moodley, D., and Rouse, P. (2012). Associations between intimate partner violence and emotional distress among pregnant women in Durban, South Africa. J. Interpers. Violence 27, 1341–1356. doi: 10.1177/0886260511425247
Gurung, S., and Acharya, J. (2016). Gender-based violence among pregnant women of Syangja District, Nepal. Osong Public Health Res. Perspect. 7, 101–107. doi: 10.1016/j.phrp.2015.11.010
Hajikhani Golchin, N. A., Hamzehgardeshi, Z., Hamzehgardeshi, L., and Shirzad, A. M. (2014). Sociodemographic characteristics of pregnant women exposed to domestic violence during pregnancy in an Iranian setting. Iran Red Crescent Med J 16:e11989. doi: 10.5812/ircmj.11989
Hoang, T. N., Van, T. N., Gammeltoft, T., Nguyen Thi Thuy, H., and Rasch, V. (2016). Association between intimate partner violence during pregnancy and adverse pregnancy outcomes in Vietnam: a prospective cohort study. PLoS One 11:e0162844. doi: 10.1371/journal.pone.0162844
Idoko, P., Ogbe, E., Jallow, O., and Ocheke, A. (2015). Burden of intimate partner violence in the Gambia—a cross sectional study of pregnant women. Reprod. Health 12:34. doi: 10.1186/s12978-015-0023-x
Islam, M. J., Broidy, L., Baird, K., and Mazerolle, P. (2017). Intimate partner violence around the time of pregnancy and postpartum depression: the experience of women of Bangladesh. PLoS One 12:e0176211. doi: 10.1371/journal.pone.0176211
Jain, S., Varshney, K., Vaid, N. B., Guleria, K., Vaid, K., and Sharma, N. (2017). A hospital-based study of intimate partner violence during pregnancy. Int. J. Gynaecol. Obstet. 137, 8–13. doi: 10.1002/ijgo.12086
Johri, M., Morales, R. E., Boivin, J. F., Samayoa, B. E., Hoch, J. S., Grazioso, C. F., et al. (2011). Increased risk of miscarriage among women experiencing physical or sexual intimate partner violence during pregnancy in Guatemala City, Guatemala: cross-sectional study. BMC Pregnancy Childbirth 11:49. doi: 10.1186/1471-2393-11-49
Lee, S., and Lee, E. (2018). Predictors of intimate partner violence among pregnant women. Int. J. Gynaecol. Obstet. 140, 159–163. doi: 10.1002/ijgo.12365
Makayoto, L. A., Omolo, J., Kamweya, A. M., Harder, V. S., and Mutai, J. (2013). Prevalence and associated factors of intimate partner violence among pregnant women attending Kisumu District Hospital, Kenya. Matern. Child Health J. 17, 441–447. doi: 10.1007/s10995-012-1015-x
Ministry of Health Nepal. Nepal Demographic Health Survey. Kathmandu: Ministry of Health, New Era, ICF, (2016).
Nejatizade, A. A., Roozbeh, N., Yabandeh, A. P., Dabiri, F., Kamjoo, A., and Shahi, A. (2017). Prevalence of domestic violence on pregnant women and maternal and neonatal outcomes in Bandar Abbas, Iran. Electron. Physician. 9, 5166–5171. doi: 10.19082/5166
Ntaganira, J., Muula, A. S., Masaisa, F., Dusabeyezu, F., Siziya, S., and Rudatsikira, E. (2008). Intimate partner violence among pregnant women in Rwanda. BMC Womens Health 8:17. doi: 10.1186/1472-6874-8-17
Office of the Prime Minister and Council of Ministers. A Study on Gender-based Violence Conducted in Selected Rural Districts of Nepal. Nepal: Office of the Prime Minister and Council of Ministers, (2012).
Owaka, I. O., Nyanchoka, M. K., and Atieli, H. E. (2017). Intimate partner violence in pregnancy among antenatal attendees at health facilities in west Pokot county, Kenya. Pan Afr. Med. J. 28:229. doi: 10.11604/pamj.2017.28.229.8840
Regmi, M. C., Subedi, L., Shrestha, R., Dixit, B., and Shrestha, N. (2017). Prevalence of domestic violence among the pregnant women attending BPKIHS. Nepal J. Obstet. Gynaecol. 12, 32–35. doi: 10.3126/njog.v12i1.18978
Shamu, S., Abrahams, N., Zarowsky, C., Shefer, T., and Temmerman, M. (2013). Intimate partner violence during pregnancy in Zimbabwe: a cross-sectional study of prevalence, predictors and associations with HIV. Trop. Med. Int. Health 18, 696–711. doi: 10.1111/tmi.12078
Singh, J. K., Evans-Lacko, S., Acharya, D., Kadel, R., and Gautam, S. (2018). Intimate partner violence during pregnancy and use of antenatal care among rural women in southern Terai of Nepal. Women Birth 31, 96–102. doi: 10.1016/j.wombi.2017.07.009
Teixeira, S. V. B., Moura, M. A. V., Silva, L. R., Queiroz, A. B. A., Souza, K. V., and Albuquerque, N. L. (2015). Intimate partner violence against pregnant women: the environment according to Levine's nursing theory. Rev. Esc. Enferm. U.S.P. 49, 882–889. doi: 10.1590/S0080-623420150000600002
Van Parys, A. S., Deschepper, E., Michielsen, K., Temmerman, M., and Verstraelen, H. (2014). Prevalence and evolution of intimate partner violence before and during pregnancy: a cross-sectional study. BMC Pregnancy Childbirth 14:294. doi: 10.1186/1471-2393-14-294
Keywords: intimate partner violence, pregnancy, postpartum woman, factors associated, cross sectional study
Citation: Sharma R and Kaphle HP (2023) Intimate partner violence during pregnancy among married women in Putalibajar municipality, Nepal. Front. Psychol. 14:1158406. doi: 10.3389/fpsyg.2023.1158406
Edited by:
Russell Kabir, Anglia Ruskin University, United KingdomReviewed by:
Sarah Gino, University of Eastern Piedmont, ItalyMichael Amera, Debre Berhan University, Ethiopia
Copyright © 2023 Sharma and Kaphle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hari Prasad Kaphle, aGFyaWthZmxlMDdAZ21haWwuY29t