 Maryse Arcand
Maryse Arcand Alexe Bilodeau-Houle
Alexe Bilodeau-Houle Robert-Paul Juster
Robert-Paul Juster Marie-France Marin
Marie-France Marin- 1Département de Psychiatrie et d'Addictologie, Faculté de Médecine, Université de Montréal, Montréal, QC, Canada
- 2Centre de Recherche de l'Institut Universitaire en Santé Mentale de Montréal, Montréal, QC, Canada
- 3Département de Psychologie, Faculté des Sciences Humaines, Université du Québec à Montréal, Montréal, QC, Canada
Introduction: Stress, depression, and anxiety symptoms have been reported during the pandemic, with important inter-individual differences. Past cross-sectional studies have found that sex and gender roles may contribute to the modulation of one's vulnerability to develop such symptoms. This longitudinal study aimed to examine the interaction of sex and psychological gender roles on stress, depression, and anxiety symptoms in adults during the COVID-19 pandemic.
Methods: Following the confinement measures in March 2020 in Montreal, stress, depression, and anxiety symptoms were assessed every 3 months (from June 2020 to March 2021) with the Depression, Anxiety and Stress Scale among 103 females and 50 males. Femininity and masculinity scores were assessed with the Bem Sex Role Inventory before the pandemic and were added as predictors along with time, sex, and the interactions between these variables using linear mixed models.
Results: We observed similar levels of depressive symptoms between males and females, but higher levels of stress and anxious symptoms in females. No effects of sex and gender roles on depressive symptoms were found. For stress and anxiety, an interaction between time, femininity, and sex was found. At the beginning of the pandemic, females with high femininity had more stress symptoms than males with high femininity, whereas females with low femininity had more anxiety symptoms 1 year after the confinement measures compared to males with low femininity.
Discussion: These findings suggest that sex differences and psychological gender roles contribute to heterogeneous patterns of stress and anxiety symptoms over time in response to the COVID-19 pandemic.
1. Introduction
The health crisis provoked by the COVID-19 pandemic has had significant repercussions on the mental health of individuals worldwide. Indeed, several studies have shown a high prevalence of stress, anxiety, and depressive symptoms in the general population (Luo et al., 2020; Salari et al., 2020; Xiong et al., 2020). These findings have been especially present among females (Findlay et al., 2020; Newby et al., 2020; Özdin and Bayrak Özdin, 2020; Xiong et al., 2020). Meta-analyses of cross-sectional studies reported prevalence rates in these samples of up to 29.6% for stress symptoms, between 14.6% and 48.3% for depressive symptoms, and between 6.3% and 50.9% for anxiety symptoms for people living mainly in Asia, as well as those living in Europe, the Middle East, United States, and Latin America (Luo et al., 2020; Salari et al., 2020; Xiong et al., 2020). In Canada, one study reported a deterioration of mental health in the general population during the first wave of the pandemic, characterized by an increase in anxiety and depressive symptoms (Robillard et al., 2021). The results of the latter study also showed that an increase in perceived stress during the pandemic was associated with an exacerbation of anxiety and depressive symptoms.
Given that most studies have used cross-sectional designs and the heterogeneity of the epidemiological evolution across the globe, the long-term mental health impact of the COVID-19 pandemic and confinement measures have been difficult to pinpoint. While several studies have reported an increase in anxiety and depressive symptoms at the onset of the health crisis relative to pre-pandemic symptoms, one study reported a decrease in symptoms mid-pandemic (Robinson et al., 2021), while another reported maintenance of symptoms (Daly et al., 2020). Although acute stress responses are adaptive and healthy (McEwen, 1998), chronic stress can lead to the dysregulation of the stress system and contribute to the development of psychopathologies such as anxiety and depressive disorders (McGonagle and Kessler, 1990; Staufenbiel et al., 2013). This highlights the need to better understand individual differences in resilience and vulnerability associated with the evolution of psychiatric symptoms over time.
Anxiety and depression are the most common psychopathologies in society and are highly comorbid. Indeed, a global study conducted by Kessler et al. (2015) showed that 45.7% of people who suffered from a depressive disorder in their lifetime had also suffered from one or more anxiety disorders. Sex differences for anxiety and depression are also observed starting from puberty onwards, with a higher vulnerability among females than males (Altemus et al., 2014; Baxter et al., 2014; Remes et al., 2016; Lim et al., 2018). Beyond these sex differences, studies have shown that including psychosocial variables in research (e.g., psychological gender roles) allows for a more profound understanding of these symptoms in individuals (Lengua and Stormshak, 2000; Palapattu et al., 2006).
As a concept distinct from birth-assigned sex, psychological gender roles are defined by the adherence of males and females to socially transmitted stereotypical characteristics associated with femininity and masculinity (Bem, 1981). Indeed, humans are socialized to incorporate personality traits, roles, characteristics, and attitudes that correspond to one's birth-assigned sex (Bem, 1981). Some argue that mental health is strongly modulated by psychological gender roles, as studies have demonstrated the influence of these roles on self-esteem, emotional regulation, psychological adjustment, and coping strategies (Bem, 1981; Jones et al., 2016). Despite criticisms regarding the year in which the instrument was created (Donnelly and Twenge, 2017), the Bem Sex-Role Inventory (Bem, 1974) is one of the most widely used questionnaires to assess psychological feminine and masculine traits (Beere, 1990; Hoffman and Borders, 2001). This instrument was developed to measure typically masculine desirable or instrumental traits, which refers to self-oriented characteristics and the achievement of personal goals (i.e., strong, assertive personality, willingness to take risks, defending one's beliefs). In addition, the instrument was developed to measure typically feminine desirable or expressive traits, which refers to characteristics oriented around connecting with others (i.e., understanding, gentle, warm, sensitive to the needs of others; Bem, 1974).
Rather than being conceptualized as two extremes on one continuum, Bem argued that femininity and masculinity are two independent continuums (Bem, 1974; Spence et al., 1975). In the literature, gender roles have been studied using either categorical or continuous methods. Originally proposed by Bem, the categorical method allows for the creation of groups by considering the level of endorsement of feminine and masculine traits. These groups are defined as follows: feminine (high in femininity), masculine (high in masculinity), androgynous (both high in femininity and high in masculinity), and undifferentiated (both low in femininity and low in masculinity; Bem, 1974). A large body of literature based on this method has shown that an androgynous gender role is associated with better psychological adjustment (Bem, 1974), fewer stress symptoms (Littlefield, 2004), social anxiety (Goodman and Kantor, 1983), and depressive symptoms (Cheng, 2005; Juster et al., 2016; Vafaei et al., 2016). In contrast, undifferentiated gender roles have been associated with poorer mental health (Bem, 1977), higher levels of social anxiety (Goodman and Kantor, 1983), and depression (Flett et al., 2009; Szpitalak and Prochwicz, 2013).
However, as the creation of groups using the categorical method is based on the median of masculinity and femininity of the sample, an individual's gender role is dependent on the study's sample and could easily vary across studies. Consequently, this method significantly impacts the external validity of the research being conducted (Sedney, 1981). Moreover, by classifying individuals as feminine or masculine gender-typed, the use of this method may lead to an under and overestimation of the contribution of the non-dominant and dominant gender roles, respectively (Johnson et al., 2006). Alternatively, the continuous method measures the distinct contributions of femininity and masculinity along continuums without impacting the generalization of the results.
To date, few studies have investigated the impact of categorical gender roles on stress symptoms and no research has explored the impact of gender roles (conceptualized as a continuous method) on stress symptoms specifically. Moreover, past studies exploring this research question were conducted using female-only samples. The latter presents an important limitation for our understanding of the interaction between gender roles and sex differences.
Regarding depressive symptoms, studies have shown that greater identification with masculine traits is associated with lower levels of depression (Feather, 1985; Whitley, 1985; Nezu and Nezu, 1987; Stoppard and Paisley, 1987; Grimmell and Stern, 1992; Thornton and Leo, 1992; Waelde et al., 1994; Bromberger and Matthews, 1996; Lengua and Stormshak, 2000; Gibson et al., 2016; Arcand et al., 2020). For the association between depression and feminine traits, mixed and null results have been reported in the literature (Tinsley et al., 1984; Feather, 1985; Whitley, 1985; Stoppard and Paisley, 1987; Grimmell and Stern, 1992; Waelde et al., 1994; Cheng, 1999; Lengua and Stormshak, 2000; Stoyanova and Hope, 2012; Gibson et al., 2016; Arcand et al., 2020). For anxiety symptoms, studies have reported that masculinity is negatively associated with both anxiety (Nezu and Nezu, 1987; Eisler et al., 1988; Grimmell and Stern, 1992; Kleinplatz et al., 1992; Thornton and Leo, 1992; Stoyanova and Hope, 2012) and social anxiety (Moscovitch et al., 2005; Johnson et al., 2006). On the other hand, femininity has been positively correlated with anxiety symptoms (Palapattu et al., 2006; Blashill and Hughes, 2009; Arcand et al., 2020), social anxiety (Johnson et al., 2006), and phobic reactions (Blashill and Hughes, 2009).
The aforementioned studies have largely examined the global impact of gender roles on symptoms irrespective of birth-assigned sex. However, some studies have investigated whether sex moderates the contribution of psychological gender roles. For depressive symptoms, mixed results have been reported for both femininity and masculinity, with some studies finding associations in females (Lengua and Stormshak, 2000) and males (Szpitalak and Prochwicz, 2013; Gibson et al., 2016), while others found no sex differences at all (Feather, 1985; Waelde et al., 1994; Gibson et al., 2016; Vafaei et al., 2016). For stress and anxiety symptoms, an interaction between sex and gender roles has yet to be found (Nezu and Nezu, 1987; Moscovitch et al., 2005).
Of note, past studies have largely used cross-sectional designs. Indeed, only a few longitudinal studies have examined the effect of gender roles on depressive symptoms. A study by Cheng (1999) conducted on healthy young adults across two time points (with a 6-month interval) found that masculinity was negatively associated with depressive symptoms. These findings suggest that masculinity stably predicts fewer stress symptoms over time (Cheng, 1999). Inversely, in a sample of postmenopausal females, few masculine traits were associated with an increase in depressive symptoms measured 3 years later (Bromberger and Matthews, 1996). As measured across four time points over a 15-year period, only one study has reported no effect of gender roles on depressive symptoms in healthy adults (Wilhlem et al., 1998). To the best of our knowledge, no longitudinal study has explored the effects of gender roles on stress and anxiety symptoms. In addition, studies that have measured the impact of gender roles on symptoms of stress, depression, and anxiety have focused on general symptoms without considering a specific stressor and its temporality. Symptoms of stress, anxiety, and depression have been exacerbated and maintained over time as a result of the COVID-19 pandemic. Furthermore, the entirety of the general population was exposed to the same prolonged stressor (i.e., the pandemic). For this reason, it is important to better understand the effect of gender roles and sex differences to identify the risk factors associated with the development and maintenance of these symptoms.
The goal of our study was to examine the effects of sex and gender roles, as well as the joint effect of sex and gender roles, on stress, depression, and anxiety symptoms during the COVID-19 pandemic. Based on the literature, we formulated the following hypotheses: (1) females will exhibit more symptoms of stress, depression, and anxiety than males at the four time points; (2) higher masculinity will be associated with lower symptoms of stress, anxiety, and depression over the course of a year; (3) femininity will be associated with more anxiety symptoms. Considering the lack of data regarding the effect of gender roles on stress symptoms and mixed results regarding the impact of femininity on depression, we did not formulate a directional hypothesis for the association between gender roles and stress symptoms, nor for the association between femininity and depression. In addition, given the lack of data on sex differences concerning gender roles, no directional hypothesis was formed for the interactions between sex and gender roles.
2. Method and measure
2.1. Sample and study design
Across three different studies conducted in our laboratory, 160 participants between the ages of 19 and 54 years old were recruited via social media and bulletin boards in the Montreal area between July 2017 and March 2020. Upon recruitment, a telephone screening interview was conducted to ensure that participants were physically and mentally healthy and were not taking any medications for mental illnesses. All participants provided their written consent and took part in a laboratory-based experiment involving self-report questionnaires, as well as cognitive and emotional tasks. As a part of their participation in one of these three studies, gender roles were measured in all participants (T0).
The first case of COVID-19 was reported in Quebec in February 2020. In March 2020, all non-essential facilities and services were disrupted (i.e., closure of schools, daycare centers, workplaces, restaurants, and entertainment venues) and a provincial confinement was declared to limit the spread of the virus. Thereafter, the evolution of the confinement measures varied as a function of the epidemiological situation, see Figure 1 for a timeline overview. All participants recruited before the start of the pandemic (n = 160; T0) were re-contacted. In total,159 individuals agreed to take part in the study in May 2020. Gender role data was not available for six participants and thus, they were removed from the current analyses. Therefore, the final sample for the current study included data from 103 females and 50 males. After obtaining consent, sociodemographic data were collected, including measures of self-reported sex (female/male or prefer not to answer). Afterwards, symptoms of stress, depression, and anxiety were measured online at four post-confinement time points: T1 in June 2020 (+3 months), T2 in September 2020 (+6 months), T3 in December 2020 (+9 months), and T4 in March 2021 (+12 months). All self-report data were collected via Qualtrics, a highly secured online platform. For each time point, a personalized URL was sent to each participant by email. From T0, the attrition rate for each time point was as follows: T1 = 2.0 %, T2 = 7.2 %, T3 = 13.7 %, and T4 = 9.8 %. At the end of the study, participants received financial compensation that was proportional to their involvement in the study (ranging from $10 to $50). Ethics approval was obtained from the institutional review board of the CIUSSS-de-l'Est-de-l'Île-de-Montréal. This study was conducted in conformity with the Declaration of Helsinki.
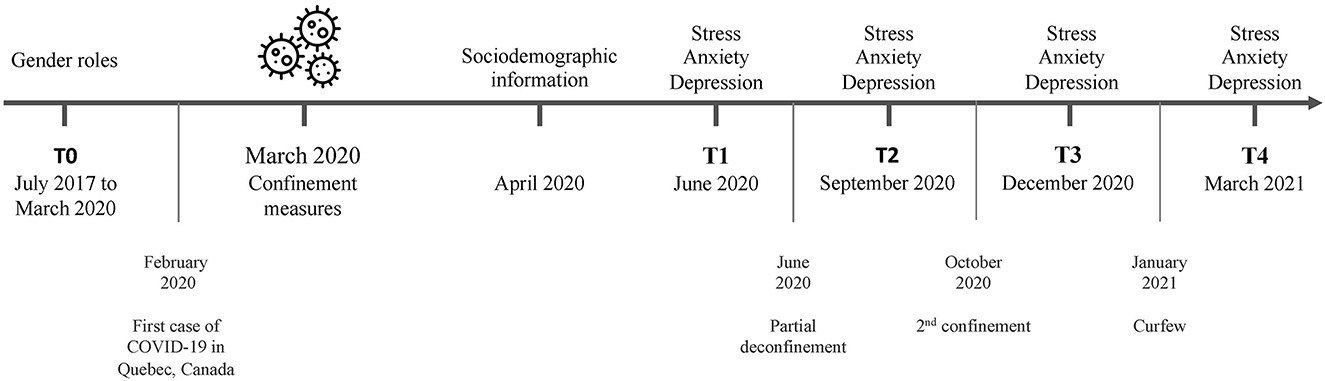
Figure 1. Timeline overview. Symptoms of stress, depression, and anxiety were measured at T1 in June 2020 (+3 months), T2 in September 2020 (+6 months), T3 in December 2020 (+9 months), and T4 in March 2021 (+12 months).
2.2. Measures
2.2.1. Gender roles
The 30-item short form of the Bem Sex-Role Inventory (Bem, 1974) was used to assess psychological gender roles. This questionnaire is composed of subscales focusing on feminine (e.g., “sensitive to the needs of others”) and masculine (e.g., “independent”) stereotyped traits. The questionnaire had 10 items for each of the following traits: feminine, masculine, and neutral traits (the 10 neutral items were not used for the current manuscript). Participants were asked to rate each item using a Likert scale from 1 (never or almost never true) to 7 (always or almost always true), yielding a score between 10 and 70 for each subscale (i.e., femininity and masculinity). In this study, Cronbach's alphas for the masculine and feminine subscales of the French version of the questionnaire are 0.79 and 0.74, respectively.
2.2.2. Depression, anxiety, and stress symptoms
The 21-item Depression, Anxiety, and Stress Scale (DASS-21; Lovibond and Lovibond, 1995) is composed of three subscales which feature seven items evaluating each of the following: depression, anxiety, and stress. Participants had to rate each item using a Likert scale from 0 (does not apply to me at all) to 3 (applies to me entirely or the vast majority of the time). The items evaluating each subscale were summed and multiplied by two, yielding a score between 0 and 42. We used the French version of the questionnaire that was developed by Donald Martin's team from the University of Ottawa (available on the Internet at: French translation of the Donald, 2012). In our sample, we found good internal consistency such that Cronbach's alpha coefficients ranged from 0.8 to 0.83 depending on the subscale.
2.3. Statistical analyses
2.3.1. Preliminary analyses
To determine whether feminine traits, masculine traits, and age differed between males and females, we conducted independent samples t-tests with sex as the between-group variable. Then, we tested if symptoms of stress, depression, and anxiety at the four time points were correlated with potential covariates identified in the literature. Examples of these covariates include status (worker, student), level of education, income, having children, residence type (apartment, house), demographic location (urban, rural), and the number of people living in the household during the COVID-19 pandemic (Arcand et al., 2020; Özdin and Bayrak Özdin, 2020; Vindegaard and Benros, 2020).
2.3.2. Principal analyses
To assess the impact of sex and gender roles, as well as the joint effect of these variables on symptoms of stress, depression, and anxiety, we conducted linear mixed-effects models. Given the longitudinal nature of this study, these analyses allowed us to control for the dependency of the data that may occur when collecting repeated measures. Statistical analyses were performed using RStudio software, version 1.4.1106 for macOS. Distinct models were conducted for stress, depression, and anxiety symptoms. First, to examine the main effects, we entered time, sex, femininity, and masculinity as fixed effects into the model. As symptoms were nested within participants, random intercepts were included. Second, to assess the interaction between sex and gender roles, as well as the interaction between sex and femininity scores/masculinity scores, these interaction terms were added to the model as fixed effects. Residual plots were visually inspected for normality and homoscedasticity and did not reveal any obvious deviations for both statistical assumptions. We used the maximum likelihood estimate with random assumptions for all linear mixed-effects models. This estimate provided unbiased estimates and valid inferences in the case of missing data. Significant interactions were further decomposed using post hoc contrast comparison tests.
3. Results
3.1. Preliminary analyses
Table 1 features sample characteristics according to sex. The independent t-tests revealed no difference between males and females for age [t(151) = 0.423, p = 0.673] and feminine traits [t(139) = −1.202, p = 0.231]. A trend effect was found for masculine traits [t(139) = 1.878, p = 0.062], where males (M = 4.68, SE = 0.11) tended to have more masculine traits than females (M = 4.41, SE = 0.09). The correlation matrix showed no effect of status (worker, student), education level, income, having children, residence type (apartment, house), demographic location (urban, rural), and the number of people living in the household on stress, depression, and anxiety symptoms at all four time points. Therefore, none of these variables were used as covariates in the main analyses.

Table 1. Characteristics of the sample.
3.2. Main analyses for stress
For stress symptoms, the analysis yielded a main effect of sex [F(1, 140) = 12.09, CI95% = 1.67 to 6.23, p = 0.001] and a trend for time [F(1, 386) = 2.99, CI95% = −0.05 to 0.80, p = 0.085]. No main effect of femininity [F(1, 142) = 0.01, CI95% = −1.57 to 1.48, p = 0.95] or masculinity [F(1, 138) = −0.46, CI95% = −1.78 to 0.86, p = 0.48] were found. The time*masculinity interaction reached significance [F(1, 387) = 3.86, CI95% = −1.93 to 0.12, p = 0.050] but post-hoc analyses revealed no significant effect. We also found a time*sex*femininity interaction [F(1, 389) = 3.58, CI95% = −2.54 to 0.06, p = 0.059], see Table 2. To decompose this three-way interaction as a function of femininity, comparisons of means were made with the scores of 3 (low) and 7 (high) on the Bem Sex Role Inventory scale as a function of time (T1 to T4) and sex on femininity scores. These scores were chosen based on the range of scores obtained in our sample (lowest score was 3 and highest score was 7). Post-hoc tests showed that females with high levels of femininity (7) had significantly (p ≤ 0.05) higher stress symptoms than males with high levels of femininity at T1, see Figure 2A.
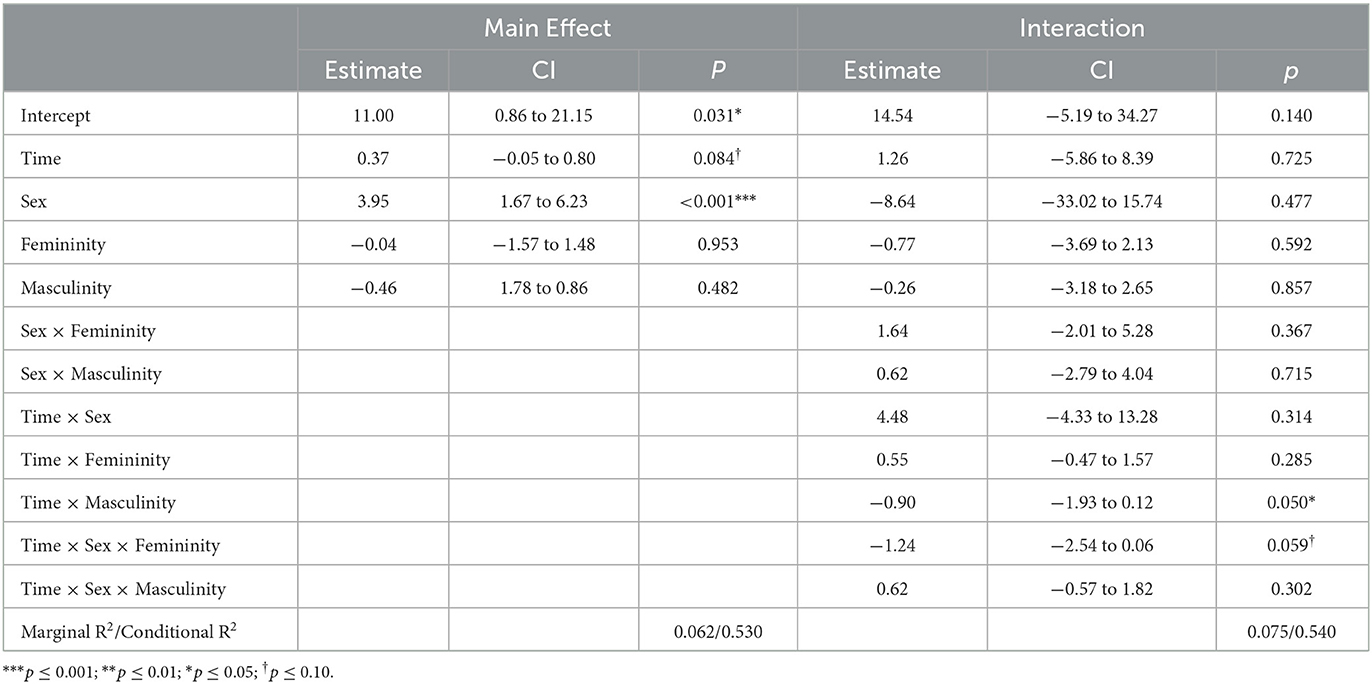
Table 2. Linear mixed model to predict stress symptoms.
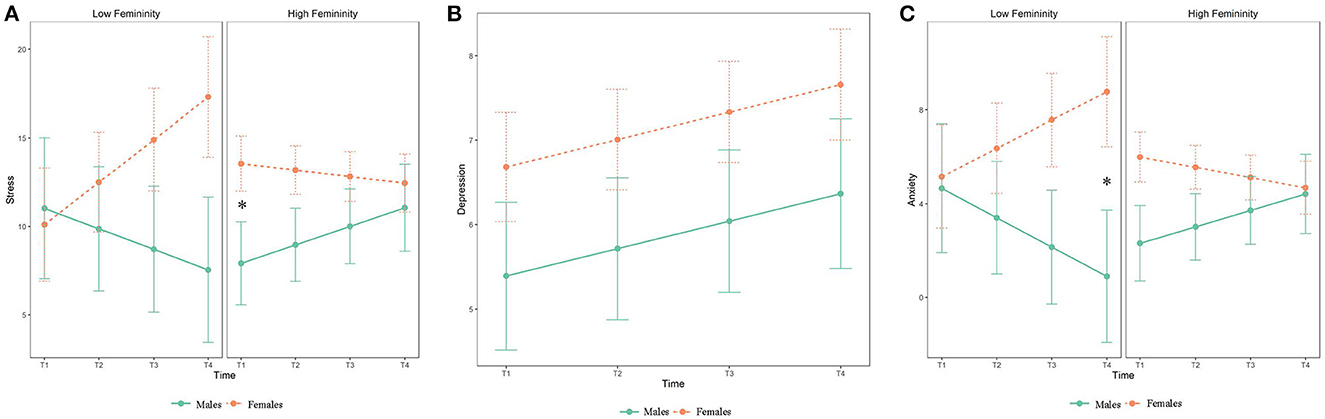
Figure 2. (A, C) Depict the joint effect of sex and gender roles on stress symptoms and anxiety symptoms as a function of time. (B) Depicts depression levels as a function of sex and the different measurement times. Low femininity refers to individuals with scores of 3 (lowest score in our sample) on the Bem Sex Roles Inventory, while high femininity refers to individuals with scores of 7 (highest score in our sample) on the same inventory. Error bars represent standard errors of the mean. Asterisk (*) indicates significant findings (p < 0.05).
3.3. Main analyses for depression
For depressive symptoms, the analysis revealed a trend effect of time [F(1, 384) = 3.11, CI95% = −0.04 to 0.69, p = 0.079] but no effect of sex [F(1, 139) = 1.61, CI95% = −0.75 to 3.33, p = 0.213], femininity [F(1, 141) = 0.21, CI95% = −1.68 to 1.06, p = 0.655], or masculinity [F(1, 137) = 2.61, CI95% = −2.13 to 0.23, p = 0.113]. The analysis did not detect a significant interaction, see Table 3 and Figure 2B.
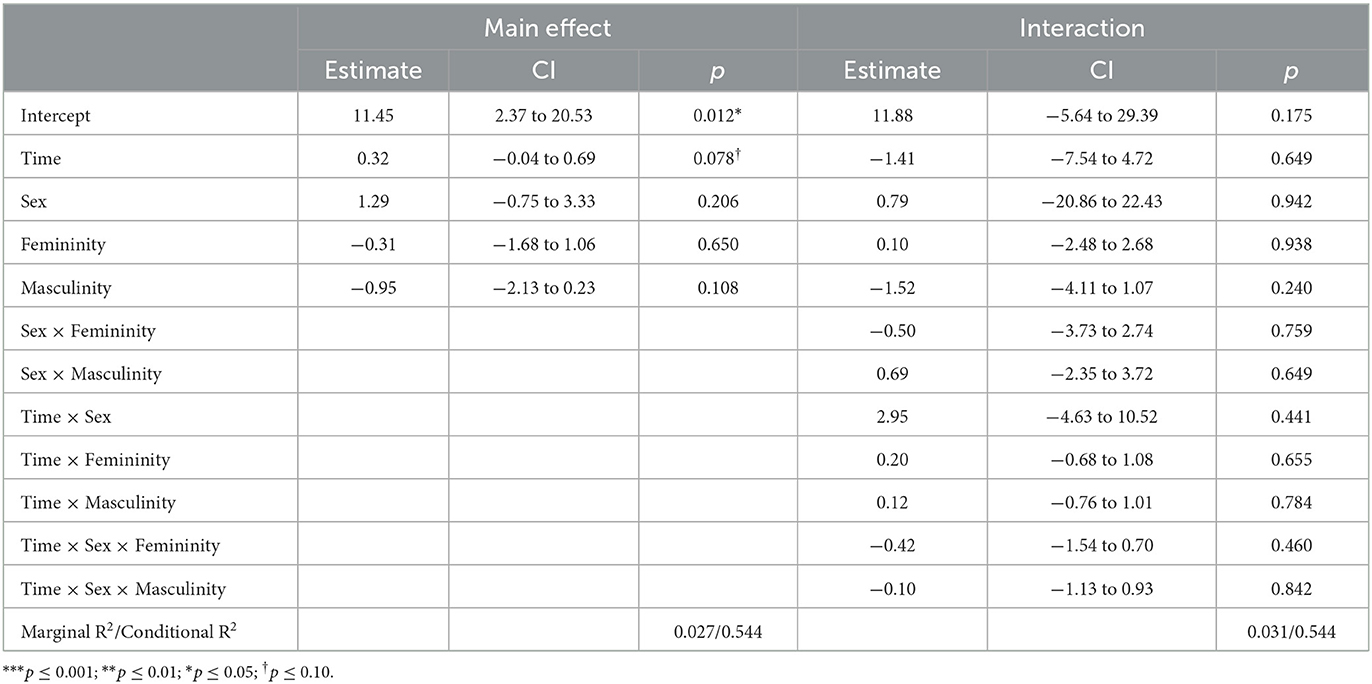
Table 3. Linear mixed model to predict depression symptoms.
3.4. Main analyses for anxiety
For anxiety symptoms, results showed a main effect of sex [F(1, 126) = 12.73, CI95% = 1.21 to 4.32, p = 0.001] but no main effect of time [F(1, 372) = 0.11, CI95% = −1.37 to 12.49, p = 0.745], femininity [F(1, 128) = 0.13, CI95% = −1.23 to 0.85, p = 0.719], or masculinity [F(1, 124) = 0.53, CI95% = −1.23 to 0.57, p = 0.475]. We also found a time*sex*femininity interaction [F(1, 376) = 3.79, CI95% = −1.81 to 0.02, p = 0.052], see Table 4. Similar to the steps performed to decompose the three-way interaction as a function of femininity for stress symptoms, we used scores of 3 (low) and 7 (high) on the Bem Sex Role Inventory scale for anxiety symptoms. Post-hoc tests revealed that females with low levels of femininity had significantly (p ≤ 0.05) higher anxiety symptoms than males with low levels of femininity at T4, see Figure 2C.
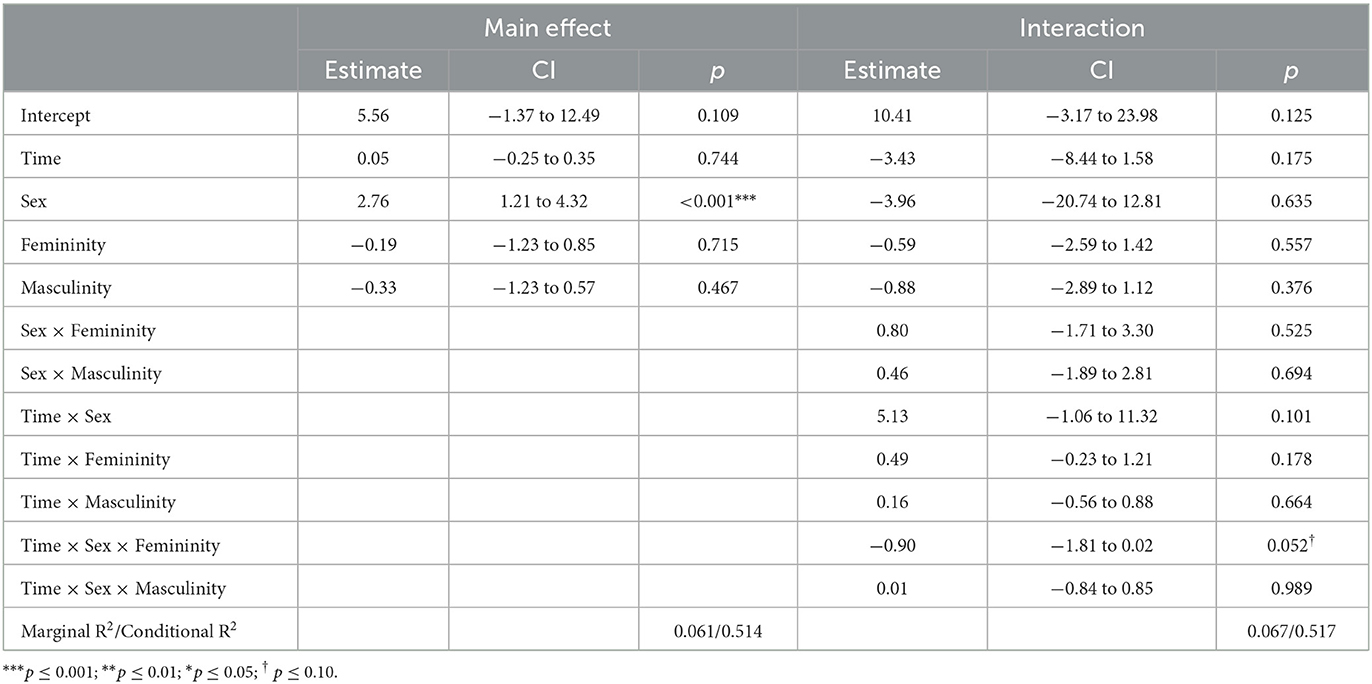
Table 4. Linear mixed model to predict anxiety symptoms.
4. Discussion
The main objective of this study was to examine the effect of sex and gender roles, as well as the interaction of sex and gender roles on symptoms of stress, depression, and anxiety during the COVID-19 pandemic. Over the course of this long-term stressful event, we found that females generally had more symptoms of stress and anxiety than males. We also found an interaction between femininity, sex, and time, such that females with high femininity had more stress symptoms at the beginning of the confinement measures compared to males with high femininity. Additionally, the results showed that females with low femininity had more anxiety symptoms one year after the confinement measures compared to males with low femininity. For depressive symptoms, no effect of gender roles or sex differences was found, nor any sex differences.
Contrary to our hypotheses, we did not find an association between masculine traits and symptoms of stress, anxiety, and depression. This result is surprising as it is inconsistent with previous studies showing that masculinity has a protective effect on mental health (Feather, 1985; Whitley, 1985; Nezu and Nezu, 1987; Stoppard and Paisley, 1987; Eisler et al., 1988; Grimmell and Stern, 1992; Kleinplatz et al., 1992; Thornton and Leo, 1992; Waelde et al., 1994; Bromberger and Matthews, 1996; Lengua and Stormshak, 2000; Stoyanova and Hope, 2012; Gibson et al., 2016; Arcand et al., 2020). One possible explanation for this finding is that the context of the pandemic may have prevented the positive attributes associated with masculinity to be used efficiently. The masculine scale of the questionnaire refers to characteristics of assertiveness and control. However, participants in our study were faced with a situation in which they had little control, had to remain confined to their homes, and had to respect a government-imposed curfew. Together, this may have dampened the expression of masculine traits. This provides insight into our lack of observed beneficial effects of masculinity on psychiatric symptoms. In addition, previous studies have reported that masculinity is associated with the use of active coping strategies and use of less avoidant coping strategies (Nezu and Nezu, 1987; Lengua and Stormshak, 2000). Although coping strategies were not measured in response to the pandemic in this study, individuals with high masculinity likely had coping styles (i.e., active) that could not be deployed as frequently as usual (prior to the pandemic) or that these coping styles did not present the usual beneficial effects. Taken together, our results suggest that masculinity does not appear to have a protective (or fragilizing) effect on psychiatric symptoms in the context of the COVID-19 pandemic. In addition, femininity influenced stress and anxiety symptoms but appeared to be a context-specific effect of the pandemic.
Indeed, our results show that females with more feminine traits were more stressed in the initial stages of the confinement measures compared to males with high feminine traits. The very few studies that have explored the impact of psychological gender roles on stress symptoms have reported a negative association between feminine traits and stress symptoms (Kleinplatz et al., 1992; Littlefield, 2004). However, these studies measured gender roles categorically, which could explain the discrepancy between the literature and results from our study. Sarrasin et al. (2014) reported that femininity was positively associated with threat perception in females, whereas this result was not found in males. Additionally, it has been shown that males tend to perceive stressful situations as challenges compared to females. However, it is unknown whether this effect is moderated by gender roles (Ptacek et al., 1992). In light of these findings, females with high levels of femininity may have interpreted the initial months of the pandemic as more threatening compared to males with high levels of femininity. Our results suggest that in the acute phase of pandemic-related stress, femininity seemed to have helped males and harmed females. To our knowledge, no study has investigated the impact of gender roles on stress symptoms in males. Importantly, some studies have reported that high femininity was negatively associated with mental health outcomes in males (Flett et al., 2009; Szpitalak and Prochwicz, 2013). In the current study, our results suggest that femininity did not increase stress symptoms in males. The typical negative effects of femininity may have been counteracted by the context of the pandemic, which may have been more adaptive for males exhibiting high levels of feminine traits. In fact, the social and economic shutdown triggered by the COVID-19 pandemic and public health measures in Quebec may have required males to suppress their typical masculine behaviors to favor more collectivistic behaviors that protect family and friends. Therefore, males may have appropriated more feminine gendered responsibilities to adapt to the pandemic. These results highlight the importance of contextualizing the use of gender roles, where different contexts could favor or oppose the adoption of given traits by each sex.
Our results also showed that females with few feminine traits were more anxious one year after the pandemic compared to males with few feminine traits. This surprising result is divergent from the existing literature that largely supports a positive association between femininity and anxiety symptoms (Palapattu et al., 2006; Blashill and Hughes, 2009; Arcand et al., 2020). In females, one study reported that femininity was positively associated with social support (Lengua and Stormshak, 2000), where the latter is known to be a protective factor against anxiety symptoms (Munir and Jackson, 1997). Our results align with this finding and suggest that low femininity may be especially harmful to females in the long run. Indeed, we only found an effect at T4, which corresponds to a year after the beginning of the implemented sanitary measures in Quebec. However, these finding warrants replication and is likely to be highly dependent on the contextual nature of the COVID-19 pandemic.
Interestingly, we only found effects for femininity in the current study. This result may be explained by the fact that our sample was more feminine than masculine. In addition, our study had twice as many females as males. For females, this finding is consistent with previous studies (Lengua and Stormshak, 2000; Johnson et al., 2006; Juster et al., 2016; Arcand et al., 2020), though this may be attributable to a sampling bias for males. As mentioned earlier, we re-contacted individuals who participated in our previous laboratory-based experiments to take part in this COVID-19 study. A large portion of our male sample (62%) stemmed from a previous study involving parent-child dyads. Studies have shown that gender roles can be modulated by different roles, worker/student status, and life experiences (Nezu and Nezu, 1987; Fan and Marini, 2000; Bryant, 2003; Kasen et al., 2006; Lemaster et al., 2017; Arcand et al., 2020). Therefore, it is possible that through the nature of their parental responsibilities, fathers exhibit more feminine traits than males without children. A larger sample would allow us to account for parental status in the statistical analyses.
Although we found sex differences for stress and anxiety symptoms, no differences were reported for depressive symptoms. In the literature, several mixed results have been reported. In general, females have higher depressive symptoms than males (Özdin and Bayrak Özdin, 2020; Xiong et al., 2020; Hyland et al., 2021), although a recent study found no sex differences for depressive symptoms (Shevlin et al., 2020). All while controlling for the number of days elapsed between data collection and March 2020, analyses of pre-pandemic depression scores were performed on our sample. Results showed that females were more depressed than males before the pandemic (p = 0.022), suggesting that the lack of sex differences observed in our COVID-19 study was likely due to symptoms of depression in response to the pandemic in males. In Quebec, confinement measures were drastic and resulted in the closure of all non-essential services (e.g., recreation, workplaces, schools). Consequently, individuals were forced to stay at home and limit activities outside of the household. As a result, this had a significant impact on factors that are closely related to depression, such as social connectedness (George et al., 1989).
In this study, we showed that individuals with greater psychological traits associated with femininity were better adapted to the COVID-19 pandemic. This suggests that the effect of gender roles on mental health symptoms is highly context dependent. Thus, some situations may favor individuals who possess more characteristics associated with femininity, while others may favor individuals with greater characteristics associated with masculinity.
This hypothesis supports the theory of androgyny proposed by Bem (1974) who argued that individuals with many feminine and masculine traits are able to better adapt to various situations. Thus, individuals with more rigid psychological gender roles (e.g., a male who identifies predominantly with feminine traits or a male who identifies predominantly with masculine traits) may have more difficulty adapting to situations that require them to display psychological traits that do not belong to their dominant gender role (Bem, 1981). Although these individuals may appear to be highly adapted in some situations, they may be less so in other contexts. Therefore, the development of both feminine and masculine traits should be encouraged in children and adolescents. This would allow youth to develop a larger toolbox that promotes their flexibility to adapt when exposed to different roles and contexts.
4.1. Limitations and future directions
Our results should be interpreted while considering certain limitations. First, every variable in our study stemmed from self-reports, including biological sex. The concept of gender is very broad and encompasses several subcategories including gender identity and gender relations (Johnson and Repta, 2012). As we focused on psychological gender roles in this study, this concept only addresses a portion of the multidimensional aspect of gender (Johnson and Repta, 2012). To adopt a more systemic approach, it would be relevant for future studies to include other aspects of gender (e.g., gender identity) to better understand the influence of the latter (Johnson and Repta, 2012). Further, although participants were all in good health at T0, we did not assess mental or physical health during the COVID-19 pandemic. With that said, studies tend to show that individuals with mental and physical health disorders may be more vulnerable to symptoms of stress, anxiety, and depression within the context of the pandemic (Özdin and Bayrak Özdin, 2020). Therefore, future studies should control for mental and physical health (healthy or disordered) to gain a better understanding of the impact of gender roles on symptom patterns during stressful events. Moreover, social support is known to moderate the relationship between femininity and depression. Given the current sample size and number of predictors in our statistical models, a lack of statistical power prevented us from including social support as a predictor in our model. Nevertheless, future studies should examine the contribution of social support to their findings given its moderating role in the relationship between femininity and mental health. In addition, it has been shown that males with depression tend to exhibit more externalizing symptoms than females (e.g., anger and aggression, substance abuse, and risk-taking; Martin et al., 2013). Therefore, depression scores quantified by the DASS may be underestimated in males. Future studies should utilize tools that are better adapted to the reality of males, such as the Male Depression Risk Scale (Rice et al., 2013). Finally, although we measured depression symptoms before the pandemic, we did not have data for stress and anxiety symptoms. It would be relevant for laboratories with baseline (pre-event) stress, anxiety, and depression data to re-measure these symptoms during a long-term stressful event to better understand the evolution of these symptoms over time.
5. Conclusion
Our findings revealed that females exhibited higher symptoms of stress and anxiety during the COVID-19 pandemic relative to males. Of note, we found that females with higher feminine traits had more stress symptoms at the beginning of the pandemic compared to males with higher feminine traits. However, females with less feminine traits were more anxious one year after the pandemic than males with less femininity. In this study, only feminine traits interacted with biological sex to predict stress and anxiety symptoms. As a result, our study supports the idea that the joint effect of sex and gender provides greater insight into our understanding of stress and anxiety symptoms in adults during a long-term stressful event such as the COVID-19 pandemic.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Institutional Review Board of the CIUSSS-de-l'Est-de-l'Île-de-Montréal. The patients/participants provided their written informed consent to participate in this study.
Author contributions
MA conducted the literature review, participated in the development of the study design, objectives of the article, performed the statistical analyses, and wrote the manuscript. AB-H helped with statistical analyses and created all graphics. R-PJ participated in the development of the study design and objectives of the article and revised the article. M-FM supervised all stages of the project and revised the article. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the Fonds de recherche du Québec—Santé (FRQS), under Grant numbers 251601 and 265447, the Canadian Institutes of Health Research (CIHR) under Grant number 169080, and the Natural Sciences and Engineering Research Council of Canada (NSERC) under the Grant number RGPIN-2018-06082.
Acknowledgments
We would like to thank Charles-Édouard Giguère and Francelyne Jean-Baptiste who helped us with R code for our statistical analyses. As this study is part of a larger research project conducted in M-FM's laboratory, we would like to thank the students of the STEAM Lab who were involved in the development of the research protocol and data collection. We would also like to thank Rebecca Cernik for the linguistic revision and editing of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Altemus, M., Sarvaiya, N., and Neill Epperson, C. (2014). Sex differences in anxiety and depression clinical perspectives. Front. Neuroendocrinol. 35, 320–330. doi: 10.1016/j.yfrne.2014.05.004
Arcand, M., Juster, R.-P., Lupien, S. J., and Marin, M.-F. (2020). Gender roles in relation to symptoms of anxiety and depression among students and workers. Anxiety Stress Coping 33, 661–674. doi: 10.1080/10615806.2020.1774560
Baxter, A. J., Scott, K. M., Ferrari, A. J., Norman, R. E., Vos, T., and Whiteford, H. A. (2014). Challenging the myth of an “epidemic” of common mental disorders: trends in the global prevalence of anxiety and depression between 1990 and 2010. Depression Anxiety 31, 506–516. doi: 10.1002/da.22230
Bem, S. L. (1974). The measurement of psychological androgyny. J. Consult. Clin. Psychol. 42, 155. doi: 10.1037/h0036215
Bem, S. L. (1977). On the utility of alternative procedures for assessing psychological androgyny. J. Consult. Clin. Psychol. 45, 196. doi: 10.1037/0022-006X.45.2.196
Bem, S. L. (1981). Gender schema theory: a cognitive account of sex typing. Psychol. Rev. 88, 354. doi: 10.1037/0033-295X.88.4.354
Blashill, A. J., and Hughes, H. M. (2009). Gender role and gender role conflict: preliminary considerations for psychotherapy with gay men. J. Gay Lesbian Mental Health 13, 170–186. doi: 10.1080/19359700902914300
Bromberger, J. T., and Matthews, K. A. (1996). A “feminine” model of vulnerability to depressive symptoms: a longitudinal investigation of middle-aged women. J. Pers. Soc. Psychol. 70, 591. doi: 10.1037/0022-3514.70.3.591
Bryant, A. N. (2003). Changes in attitudes toward women's roles: predicting gender-role traditionalism among college students. Sex Roles 48, 131–142. doi: 10.1023/A:1022451205292
Cheng, C. (1999). Gender-role differences in susceptibility to the influence of support availability on depression. J. Pers. 67, 440–467. doi: 10.1111/1467-6494.00061
Cheng, C. (2005). Processes underlying gender-role flexibility: do androgynous individuals know more or know how to cope? J. Pers. 73, 645–674. doi: 10.1111/j.1467-6494.2005.00324.x
Daly, M., Sutin, A. R., and Robinson, E. (2020). Longitudinal changes in mental health and the COVID-19 pandemic: evidence from the UK household longitudinal study. Psychol. Med. 52, 2549–2558. doi: 10.31234/osf.io/qd5z7
Donald, M. (2012). French Translation of the DASS [website]. Available online at: http://dass.psy.unsw.edu.au/French/French.htm
Donnelly, K., and Twenge, J. M. (2017). Masculine and feminine traits on the Bem Sex-Role Inventory, 1993–2012: A cross-temporal meta-analysis. Sex Roles 76, 556–565. doi: 10.1007/s11199-016-0625-y
Eisler, R. M., Skidmore, J. R., and Ward, C. H. (1988). Masculine gender-role stress: predictor of anger, anxiety, and health-risk behaviors. J. Pers. Assess. 52, 133–141. doi: 10.1207/s15327752jpa5201_12
Fan, P.-L., and Marini, M. M. (2000). Influences on gender-role attitudes during the transition to adulthood. Soc. Sci. Res. 29, 258–283. doi: 10.1006/ssre.1999.0669
Feather, N. T. (1985). Masculinity, femininity, self-esteem, and subclinical depression. Sex Roles 12, 491–500. doi: 10.1007/BF00288171
Findlay, L. C., Arim, R., and Kohen, D. (2020). Understanding the perceived mental health of Canadians during the COVID-19 pandemic. Health Rep. 31, 22–27. doi: 10.25318/82-003-x202000400003-eng
Flett, G. L., Krames, L., and Vredenburg, K. (2009). Personality traits in clinical depression and remitted depression: an analysis of instrumental-agentic and expressive-communal traits. Curr. Psychol. 28, 240–248. doi: 10.1007/s12144-009-9063-0
George, L. K., Blazer, D. G., Hughes, D. C., and Fowler, N. (1989). Social support and the outcome of major depression. Brit. J. Psychiatry 154, 478–485. doi: 10.1192/bjp.154.4.478
Gibson, P. A., Baker, E. H., and Milner, A. N. (2016). The role of sex, gender, and education on depressive symptoms among young adults in the United States. J. Affect. Disord. 189, 306–313. doi: 10.1016/j.jad.2015.08.067
Goodman, S. H., and Kantor, D. (1983). Influence of sex-role identity on two indices of social anxiety. J. Res. Pers. 17, 443–450. doi: 10.1016/0092-6566(83)90071-5
Grimmell, D., and Stern, G. S. (1992). The relationship between gender role ideals and psychological well-being. Sex Roles 27, 487–497. doi: 10.1007/BF00290005
Hoffman, R. M., and Borders, L. D. (2001). Twenty-five years after the Bem Sex-Role Inventory: A reassessment and new issues regarding classification variability. Meas. Eval. Couns. Dev. 34, 39–55. doi: 10.1080/07481756.2001.120D69021
Hyland, P., Shevlin, M., Murphy, J., McBride, O., Fox, R., Bondjers, K., et al. (2021). A longitudinal assessment of depression and anxiety in the Republic of Ireland during the COVID-19 pandemic. Psychiat. Res. 300, 113905. doi: 10.31234/osf.io/4avt6
Johnson, H. D., McNair, R., Vojick, A., Congdon, D., Monacelli, J., and Lamont, J. (2006). Categorical and continuous measurement of sex-role orientation: differences in associations with young adults'reports of well-being. Soc. Behav. Pers. Int. J. 34, 59–76. doi: 10.2224/sbp.2006.34.1.59
Johnson, J. L., and Repta, R. (2012). “Beyond the binaries,” in Designing and Conducting Gender, Sex and Health Research, eds J. L. Oliffe and L. Greaves (SAGE Publications, Inc.), 17–37.
Jones, K., Mendenhall, S., and Myers, C. A. (2016). The effects of sex and gender role identity on perceived stress and coping among traditional and nontraditional students. J. Am. Coll. Health 64, 205–213. doi: 10.1080/07448481.2015.1117462
Juster, R.-P., Pruessner, J. C., Desrochers, A. B., Bourdon, O., Durand, N., Wan, N., et al. (2016). Sex and gender roles in relation to mental health and allostatic load. Psychosom. Med. 78, 788–804. doi: 10.1097/PSY.0000000000000351
Kasen, S., Chen, H., Sneed, J., Crawford, T., and Cohen, P. (2006). Social role and birth cohort influences on gender-linked personality traits in women: a 20-year longitudinal analysis. J. Pers. Soc. Psychol. 91, 944. doi: 10.1037/0022-3514.91.5.944
Kessler, R. C., Sampson, N. A., Berglund, P., Gruber, M. J., Al-Hamzawi, A., Andrade, L., et al. (2015). Anxious and non-anxious major depressive disorder in the World Health Organization World Mental Health Surveys. Epidemiol. Psychiatr. Sci. 24, 210–226. doi: 10.1017/S2045796015000189
Kleinplatz, P., McCarrey, M., and Kateb, C. (1992). The impact of gender-role identity on women's self-esteem, lifestyle satisfaction and conflict. Can. J. Behav. Sci. 24, 333–347. doi: 10.1037/h0078725
Lemaster, P., Delaney, R., and Strough, J. (2017). Crossover, degendering, or…? a multidimensional approach to life-span gender development. Sex Roles 76, 669–681. doi: 10.1007/s11199-015-0563-0
Lengua, L. J., and Stormshak, E. A. (2000). Gender, gender roles, and personality: gender differences in the prediction of coping and psychological symptoms. Sex Roles 43, 787–820. doi: 10.1023/A:1011096604861
Lim, G. Y., Tam, W. W., Lu, Y., Ho, C. S., Zhang, M. W., and Ho, R. C. (2018). Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci. Rep. 8, 1–10. doi: 10.1038/s41598-018-21243-x
Littlefield, M. B. (2004). Gender role identity and stress in African American women. J. Hum. Behav. Soc. Environ. 8, 93–104. doi: 10.1300/J137v08n04_06
Lovibond, P. F., and Lovibond, S. H. (1995). The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behav. Res. Therapy 33, 335–343. doi: 10.1016/0005-7967(94)00075-U
Luo, M., Guo, L., Yu, M., Jiang, W., and Wang, H. (2020). The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public - A systematic review and meta-analysis. Psychiatry Res. 291, 113190. doi: 10.1016/j.psychres.2020.113190
Martin, L. A., Neighbors, H. W., and Griffith, D. M. (2013). The experience of symptoms of depression in men vs women: analysis of the National Comorbidity Survey Replication. JAMA Psychiat. 70, 1100–1106. doi: 10.1001/jamapsychiatry.2013.1985
McEwen, B. S. (1998). Stress, adaptation, and disease: allostasis and allostatic load. Ann. N. Y. Acad. Sci. 840, 33–44. doi: 10.1111/j.1749-6632.1998.tb09546.x
McGonagle, K. A., and Kessler, R. C. (1990). Chronic stress, acute stress, and depressive symptoms. Am. J. Commun. Psychol. 18, 681–706. doi: 10.1007/BF00931237
Moscovitch, D. A., Hofmann, S. G., and Litz, B. T. (2005). The impact of self-construals on social anxiety: a gender-specific interaction. Pers. Individ. Diff. 38, 659–672. doi: 10.1016/j.paid.2004.05.021
Munir, S. S., and Jackson, D. W. (1997). Social support, need for support, and anxiety among women graduate students. Psychol. Rep. 80, 383–386. doi: 10.2466/pr0.1997.80.2.383
Newby, J. M., O'Moore, K., Tang, S., Christensen, H., and Faasse, K. (2020). Acute mental health responses during the COVID-19 pandemic in Australia. PLoS ONE 15, e0236562. doi: 10.1371/journal.pone.0236562
Nezu, A. M., and Nezu, C. M. (1987). Psychological distress, problem solving, and coping reactions: Sex role differences. Sex Roles 16, 205–214. doi: 10.1007/BF00289650
Özdin, S., and Bayrak Özdin, S. (2020). Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: the importance of gender. Int. J. Soc. Psychiatry 66, 504–511. doi: 10.1177/0020764020927051
Palapattu, A. G., Kingery, J. N., and Ginsburg, G. S. (2006). Gender role orientation and anxiety symptoms among African American Adolescents. J. Abnormal Child Psychol. 34, 423–431. doi: 10.1007/s10802-006-9023-1
Ptacek, J. T., Smith, R. E., and Zanas, J. (1992). Gender, appraisal, and coping: a longitudinal analysis. J. Pers. 60, 747–770. doi: 10.1111/j.1467-6494.1992.tb00272.x
Remes, O., Brayne, C., Linde, R., and van der Lafortune, L. (2016). A systematic review of reviews on the prevalence of anxiety disorders in adult populations. Brain Behav. 6, e00497. doi: 10.1002/brb3.497
Rice, S. M., Fallon, B. J., Aucote, H. M., and Möller-Leimkühler, A. M. (2013). Development and preliminary validation of the male depression risk scale: Furthering the assessment of depression in men. J. Affect. Disord. 151, 950–958. doi: 10.1016/j.jad.2013.08.013
Robillard, R., Daros, A. R., Phillips, J. L., Porteous, M., Saad, M., Pennestri, M.-H., et al. (2021). Emerging new psychiatric symptoms and the worsening of pre-existing mental disorders during the COVID-19 pandemic: a Canadian multisite study. Can. J. Psychiatry 66, 815–826. doi: 10.1177/0706743720986786
Robinson, E., Sutin, A. R., Daly, M., and Jones, A. (2021). A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J. Affect. Disord. 296, 567–576. doi: 10.1101/2021.03.04.21252921
Salari, N., Hosseinian-Far, A., Jalali, R., Vaisi-Raygani, A., Rasoulpoor, S., Mohammadi, M., et al. (2020). Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global. Health 16, 57. doi: 10.1186/s12992-020-00589-w
Sarrasin, O., Mayor, E., and Faniko, K. (2014). Gender traits and cognitive appraisal in young adults: The mediating role of locus of control. Sex Roles 70, 122–133. doi: 10.1007/s11199-013-0336-6
Sedney, M. A. (1981). Comments on median split procedures for scoring androgyny measures. Sex Roles 7, 217–222. doi: 10.1007/BF00287807
Shevlin, M., McBride, O., Murphy, J., Miller, J. G., Hartman, T. K., Levita, L., et al. (2020). Anxiety, depression, traumatic stress and COVID-19-related anxiety in the UK general population during the COVID-19 pandemic. BJPsych Open 6, e125. doi: 10.1192/bjo.2020.109
Spence, J. T., Helmreich, R., and Stapp, J. (1975). Ratings of self and peers on sex role attributes and their relation to self-esteem and conceptions of masculinity and femininity. J. Pers. Soc. Psychol. 32, 29–39. doi: 10.1037/h0076857
Staufenbiel, S. M., Penninx, B. W. J. H., Spijker, A. T., Elzinga, B. M., and van Rossum, E. F. C. (2013). Hair cortisol, stress exposure, and mental health in humans: a systematic review. Psychoneuroendocrinology 38, 1220–1235. doi: 10.1016/j.psyneuen.2012.11.015
Stoppard, J. M., and Paisley, K. J. (1987). Masculinity, femininity, life stress, and depression. Sex Roles 16, 489–496. doi: 10.1007/BF00292483
Stoyanova, M., and Hope, D. A. (2012). Gender, gender roles, and anxiety: Perceived confirmability of self report, behavioral avoidance, and physiological reactivity. J. Anxiety Disord. 26, 206–214. doi: 10.1016/j.janxdis.2011.11.006
Szpitalak, M., and Prochwicz, K. (2013). Psychological gender in clinical depression. Preliminary study. Psychiatria Polska 47, 53–64.
Thornton, B., and Leo, R. (1992). Gender typing, importance of multiple roles, and mental health consequences for women. Sex Roles 27, 307–317. doi: 10.1007/BF00289931
Tinsley, E. G., Sullivan-Guest, S., and McGuire, J. (1984). Feminine sex role and depression in middle-aged women. Sex Roles 11, 25–32. doi: 10.1007/BF00287437
Vafaei, A., Ahmed, T., Freire, A., do, N. F., Zunzunegui, M. V., and Guerra, R. O. (2016). Depression, sex and gender roles in older adult populations: the international mobility in aging study (IMIAS). PLoS ONE 11, e0146867. doi: 10.1371/journal.pone.0146867
Vindegaard, N., and Benros, M. E. (2020). COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 89, 531–542. doi: 10.1016/j.bbi.2020.05.048
Waelde, L. C., Silvern, L., and Hodges, W. F. (1994). Stressful life events: moderators of the relationships of gender and gender roles to self-reported depression and suicidality among college students. Sex Roles 30, 1–22. doi: 10.1007/BF01420737
Whitley, B. E. (1985). Sex-role orientation and psychological well-being: two meta-analyses. Sex Roles 12, 207–225. doi: 10.1007/BF00288048
Wilhlem, K., Parker, G., and Asghari, A. (1998). Sex differences in the experience of depressed mood state over fifteen years. doi: 10.1007/s001270050016
Keywords: stress, anxiety, depression, gender role, sex differences, long-term stressful event
Citation: Arcand M, Bilodeau-Houle A, Juster R-P and Marin M-F (2023) Sex and gender role differences on stress, depression, and anxiety symptoms in response to the COVID-19 pandemic over time. Front. Psychol. 14:1166154. doi: 10.3389/fpsyg.2023.1166154
Received: 14 February 2023; Accepted: 11 April 2023;
Published: 03 May 2023.
Edited by:
Sagrario Gomez-Cantarino, University of Castilla La Mancha, SpainReviewed by:
Maria Angélica De Peres, Federal University of Rio de Janeiro, BrazilFernanda Batista Oliveira Santos, Federal University of Minas Gerais, Brazil
Copyright © 2023 Arcand, Bilodeau-Houle, Juster and Marin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marie-France Marin, bWFyaW4ubWFyaWUtZnJhbmNlQHVxYW0uY2E=