 Xiao Hui Ng
Xiao Hui Ng Jeanie Chu1
Jeanie Chu1 Kinjal Doshi
Kinjal Doshi- 1Department of Health and Wellbeing, National University of Singapore, Singapore, Singapore
- 2INSiGHT Therapeutics and Consulting, Singapore, Singapore
- 3Department of Psychology, National University of Singapore, Singapore, Singapore
Introduction: A diagnosis of a psychological health concern is associated with lower wellbeing and subjective quality of life (sQoL). However, there is limited literature examining whether individuals who suspect they have a psychological health condition (SPHC) experience similar challenges. The primary aim of this study is to investigate the relationship between SPHC, workplace wellbeing, and sQoL, with the goal of informing future workplace wellbeing interventions within a diverse university setting. A secondary aim is to explore whether additional aspects of wellbeing are valued by a multicultural population beyond the five core components defined in Martin Seligman’s Wellbeing Theory: positive emotion, engagement, relationships, meaning, and achievement.
Methods: A 57-item survey was sent to a randomly generated list of 2,000 university staff to request for their participation. It gathered information on their understanding of wellbeing, presence of suspected psychological health conditions, level of distress, workplace psychological wellbeing, and quality of life.
Results: First, individuals with SPHCs reported significantly lower levels of wellbeing and sQoL compared to those who did not suspect having a PHC. Second, workplace wellbeing was found to mediate the relationship between psychological distress and sQoL. Finally, qualitative analysis revealed five additional lay conceptualizations of wellbeing in addition to the five facets identified in PERMA, namely psychological health, physical health, balance, meeting basic needs, and autonomy.
Discussion: That wellbeing mediates the relationship between psychological distress and sQoL suggests that workplace wellbeing interventions may be particularly important in improving sQoL, especially in individuals who experience SPHCs given that they also experience lower sQoL. That five other lay conceptualisations of wellbeing also emerged from the findings suggests that laypeople’s understanding of wellbeing adds a unique cultural and situational lens to the current understanding of this construct. Further implications are discussed.
Introduction
Many studies focus on individuals with diagnosed psychological health concerns (PHCs), examining their prevalence and treatment. However, few studies investigate individuals who suspect they have psychological health conditions (SPHCs) but remain undiagnosed. This area warrants further research, as common PHCs such as depression (Faisal-Cury et al., 2022) and anxiety (Kasper, 2006) are often underdiagnosed or misdiagnosed and, consequently, undertreated, an issue with serious implications. Individuals with SPHCs are more likely to score above the clinical threshold for depression, anxiety, and post-traumatic stress, and to report poorer health-related quality of life and sleep quality compared to those who do not suspect having a PHC (Liu et al., 2020). Furthermore, the treatment gap for SPHC stands at 47% (Islam et al., 2022), which is concerning as longer treatment delays are associated with higher rates of comorbidity of other health conditions and increased mortality (McLaughlin, 2004).
However, beyond clinical recovery or symptomatic alleviation, it is also important to consider personal recovery or the striving toward increased psychological wellbeing (Slade, 2010), especially in individuals who may not have access to clinical services as they are not diagnosed with a psychological condition. While not specific to individuals who have SPHC, Vaingankar et al. (2020) demonstrated that while individuals with diagnosed PHCs generally indicate lower quality of life and poorer health outcomes as compared to individuals without diagnosed PHCs, having increased psychological wellbeing reduces the impact that diagnosed PHCs might have on these areas. This evolving understanding of recovery and wellbeing then raises the question of whether psychological health interventions can be delivered in environments other than traditional settings, such as clinics and hospitals, and by non-clinically trained individuals, if only an understanding of wellbeing can also be reached.
Wellbeing is understood as the experiencing of optimal psychological functioning (Deci and Ryan, 2006), with many attempts to define such positive functioning with a specific value framework (Diener, 1984), one of these being Martin Seligman’s Wellbeing Theory (WBT).
WBT posits that complete wellbeing, or flourishing, consists of five distinct factors, or PERMA, namely:
1. Positive emotion: Experiencing emotions such as hopefulness, happiness, and a sense of peace.
2. Engagement: Having meaningful work that keeps one purposefully occupied.
3. Relationships: Having warm, trusting relationships with others.
4. Meaning: Having a greater goal and sense of purpose in life.
5. Accomplishment: Experiencing a sense of accomplishment (Seligman, 2011).
While the PERMA factors constitute a broader concept of wellbeing, they also serve as distinct paths of striving toward a sense of wellbeing for different individuals (Seligman, 2011). Furthermore, as adults spend a significant portion of their time at work, workplace wellbeing is crucial. Effective workplace wellbeing interventions can reduce psychological distress and offer benefits like improved physical health, job satisfaction, and organizational commitment (Meyers et al., 2012; Kern et al., 2014). However, there are few empirically evaluated wellbeing interventions specifically designed for workplaces (Neumeier et al., 2017). Understanding how employees define and prioritize wellbeing is essential for crafting suitable interventions.
Regarding Quality of Life (QoL), while objective QoL focuses on economic indicators such as wealth and access to healthcare, subjective QoL (sQoL) looks at how an individual assesses their own QoL by their own standards (Cummins, 2000). Furthermore, subjective quality of life (QoL) appears to be more strongly associated with the intensity of distress experienced in relation to a health condition (Andenæs et al., 2004). While the individual concepts of wellbeing and QoL have been well-studied, their relationship is less understood. Research showed that both wellbeing and sQoL significantly contribute to overall QoL (Skevington and Böhnke, 2018). Skevington and Böhnke (2018) proposed an integrated model combining subjective wellbeing and sQoL, incorporating elements like financial resources, physical environment, emotions, and spirituality, which better explains QoL than either factor alone.
Aims
This study first aims to add to the literature on SPHC and workplace wellbeing (WW) in a university work environment by investigating the relationship between SPHCs, WW, and sQoL. Secondly, it aims to explore whether there exist other aspects of wellbeing pertinent to a multicultural workplace that have not yet been identified by current research. Achieving these aims may identify areas of focus for WW interventions to aid in personal recovery beyond symptomatic alleviation, benefiting both individuals and workplaces.
Hypotheses
Based on the aims, the following hypotheses were developed:
H1: Individuals with SPHCs will report lower WW compared to individuals without SPHCs (nSPHC).
H2: Individuals with SPHCs will report lower sQoL compared to individuals who do not experience SPHCs.
H3: WW will mediate the relationship between levels of distress (depression, anxiety, and stress) and sQoL.
To address the final aim, a qualitative component will explore how individuals in a multicultural workplace define wellbeing.
Materials and methods
Procedure
Invitations to respond to an online survey administered using Qualtrics were sent via e-mail to a randomly generated list of 2000 university staff stratified by department. A reminder email was sent 2 weeks after the first email to increase response rates.
Measures
A 57-item questionnaire gathered data on six areas: basic demographic information, understanding of wellbeing, presence of suspected psychological health conditions, level of distress, workplace psychological wellbeing, and quality of life.
Psychological health status
A question on suspected psychological health status was posed to participants. Participants could indicate that they suspected having a psychological health condition (SPHC), had no suspicions of PHC (nSPHC), or preferred not to say (SPNTS).
Understanding of wellbeing
To understand participants’ subjective understanding of wellbeing, an open-ended question was included in the questionnaire asking, “What does wellbeing mean for you personally?”
Subjective quality of life
The single-item Global QoL Scale by Hyland and Sodergren (1996) was included to measure participants’ sQoL. Participants were asked to move a slider from a scale of 0–100 to a point that best describes their QoL. The measure has demonstrated good test–retest reliability (Hyland and Sodergren, 1996).
Depression, anxiety, and stress
The Depression-Anxiety-Stress Scale 21 was used to measure participants’ levels of depression, anxiety, and stress. Each item is scored on a four-point Likert scale. The 21-item self-report measure has three sub-scales designed to measure states of depression, anxiety, and stress and has been found to have strong internal consistency (α range = 0.86–0.96), convergent validity, and discriminant validity in large clinical samples (Brown et al., 1997). Strong internal consistency was observed for all scales (α range = 0.80–0.91), and discriminant validity was noted among various disorders in non-clinical samples (Sinclair et al., 2011).
Workplace wellbeing
The 23-item Workplace PERMA profiler was used to measure subjective wellbeing in a workplace context. The scale was based on Seligman’s WBT (Butler and Kern, 2016) and has five key subscales: Positive Emotion, Engagement, Relationships, Meaning, and Accomplishment. Each subscale has three items scored on a 10-point scale. The sum of the items from the five primary subscales generates an overall workplace wellbeing score. Several studies have validated the profiler, demonstrating strong internal consistency except for the Engagement subscale (α = 0.66), as well as strong convergent and divergent validity (Ryan et al., 2019).
Method of qualitative analysis
Codebook thematic analysis, specifically the Framework Method developed by Ritchie and Spencer (1994), was the selected form of analysis for the qualitative component. The Framework method’s flexibility in integrating both deductive and inductive thematic analysis approaches (Gale et al., 2013) made it an ideal means of analysis in the current study. The current research interest in the PERMA framework makes a deductive approach ideal, as themes can be drawn from the PERMA framework. An inductive approach also allowed for the emergence of new themes beyond the PERMA framework through open coding and refinement.
Results
Demographic information
A total of 214 responses were submitted, with 16 incomplete responses. The 198 completed responses were utilized for quantitative analysis (Table 1: Sociodemographic characteristics of population). Means and standard deviations for utilized measures across sociodemographic characteristics are reported in Table 2, and correlations for utilized measures are reported in Table 3.
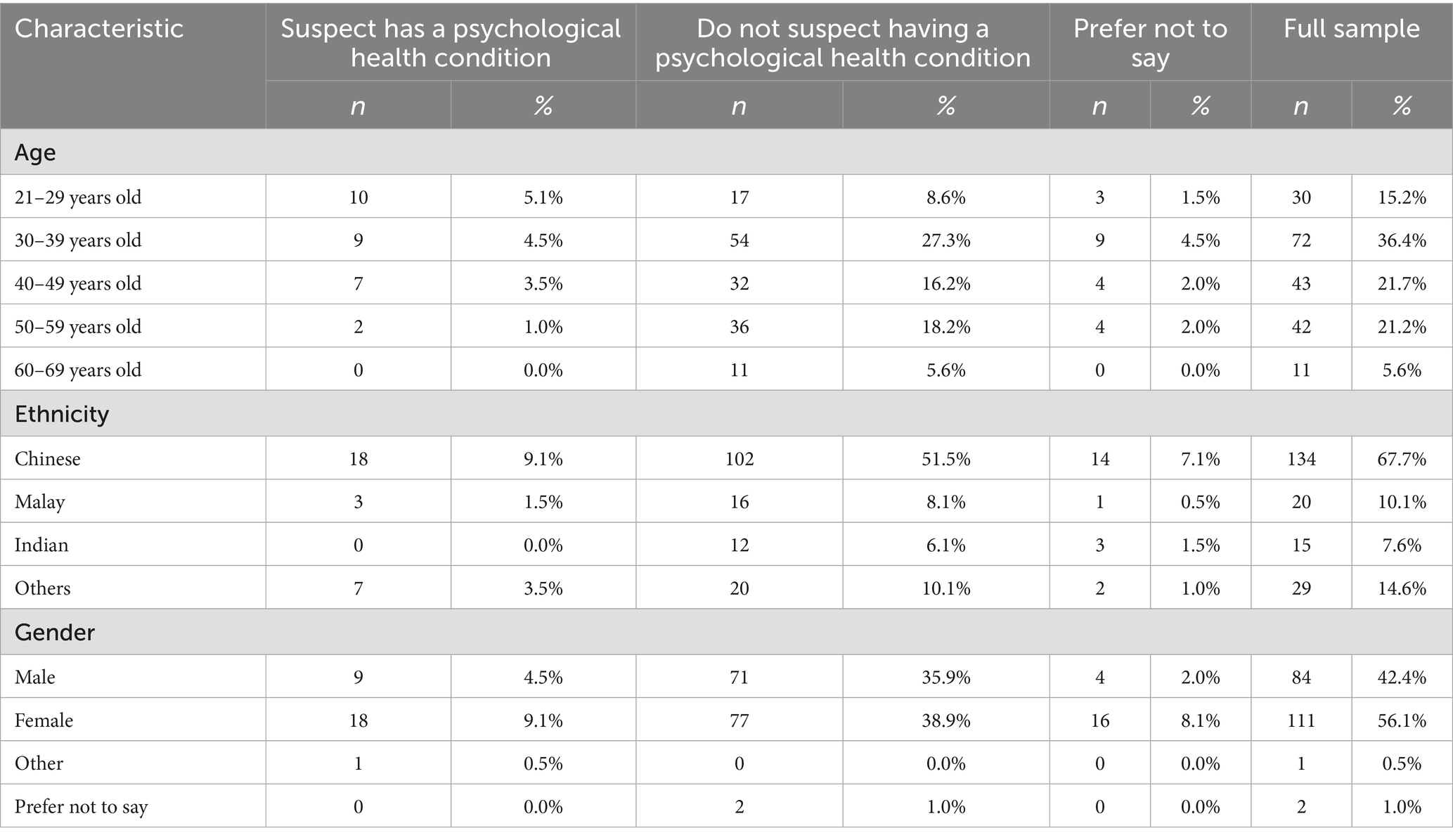
Table 1. Sociodemographic characteristics of population.
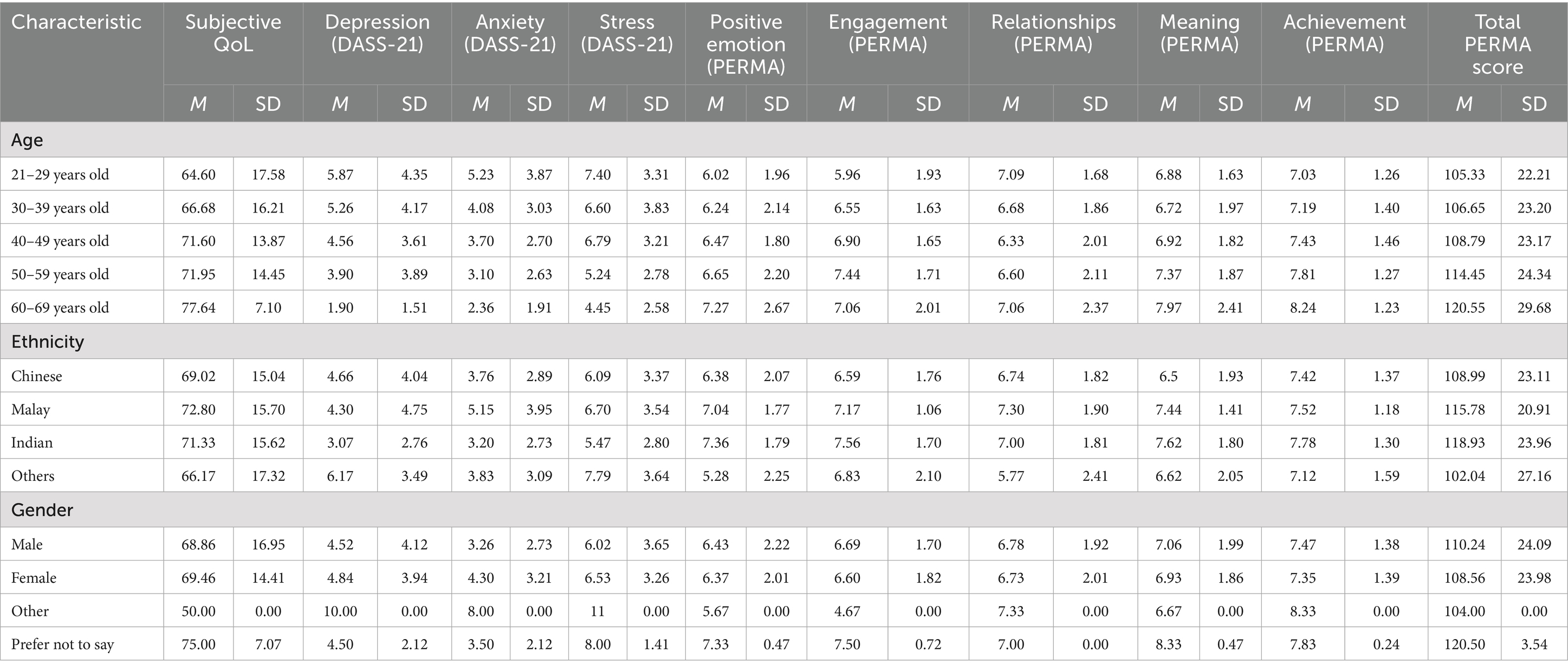
Table 2. Means and standard deviations of measures across sociodemographic characteristics.
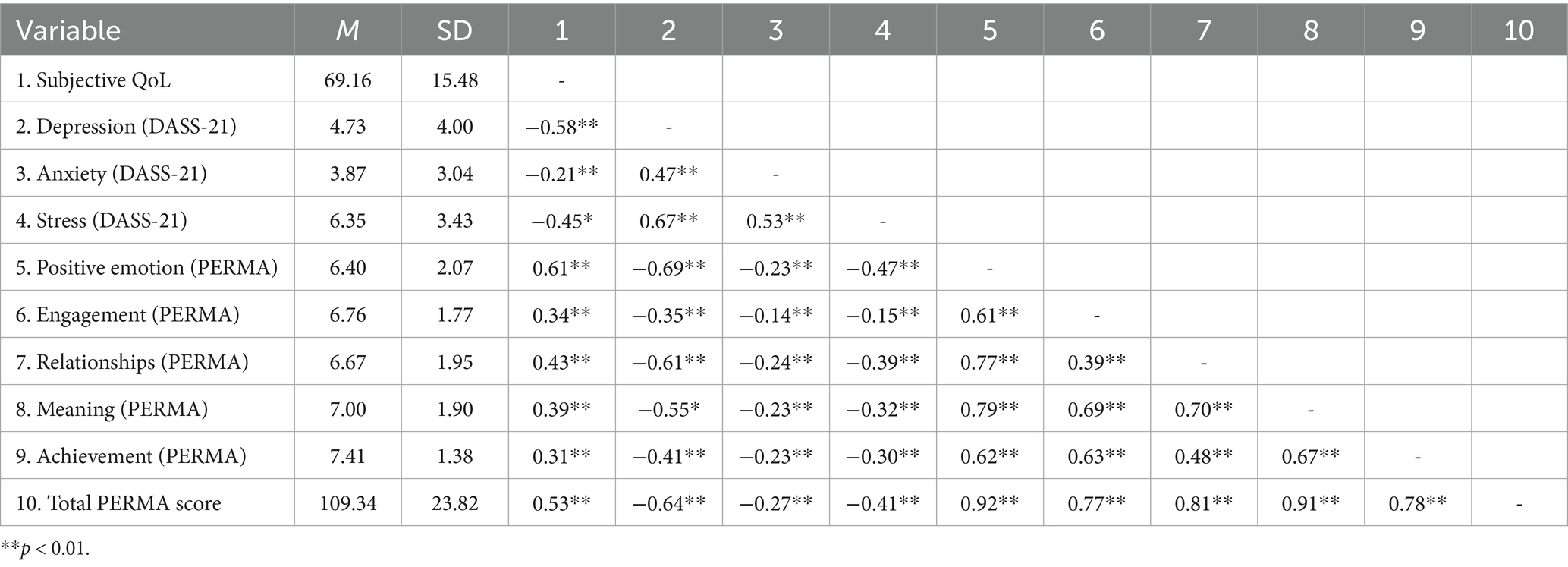
Table 3. Correlations between QoL score, DASS-21 scores, and PERMA scores.
Suspected psychological health conditions
A total of 14.1% of participants reported a suspected PHC (SPHC N = 28), 75.8% had no SPHC (nSPHC N = 150), and 10.1% preferred not to say (SPNTS N = 20).
Suspected psychological health condition and workplace wellbeing
A one-way ANOVA was performed to compare the effect of SPHC on workplace PERMA wellbeing scores with follow-up post-hoc tests using Tukey’s HSD Test for Multiple Comparisons.
Suspected psychological health conditions and wellbeing
There was a significant difference in overall PERMA wellbeing score [F (2, 192) = 10.70, p < 0.01] between the SPHC (M = 3.97, SD = 2.04) and nSPHC (M = 5.71, SD = 2.05) groups, p > 0.01, 95% CI = −32.39, −10.29. These results support H1 that individuals with SPHCs will report lower workplace wellbeing as compared to individuals without SPHCs.
Significant differences were also observed between the SPHC and nSPHC groups at all PERMA sub-facet levels. The nSPHCs group reported higher Positive Emotion, Engagement, Relationships, Meaning, and Achievement than the SPHC group (Table 4: One-way ANOVA; Table 5: Post-hoc tests).
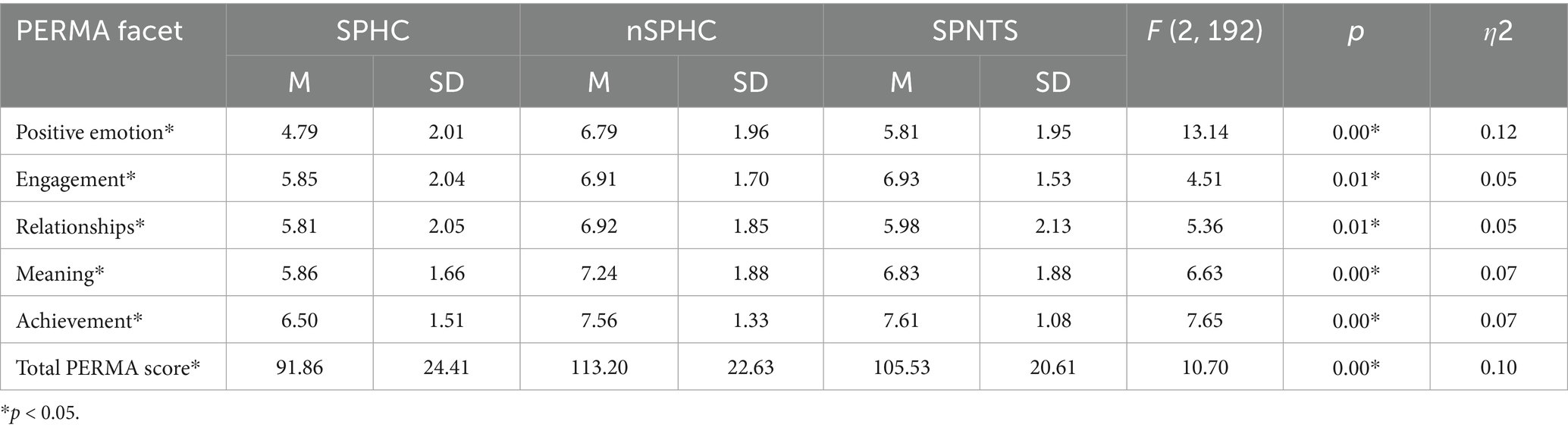
Table 4. One-way ANOVA comparing the presence of suspected psychological health status on workplace wellbeing.
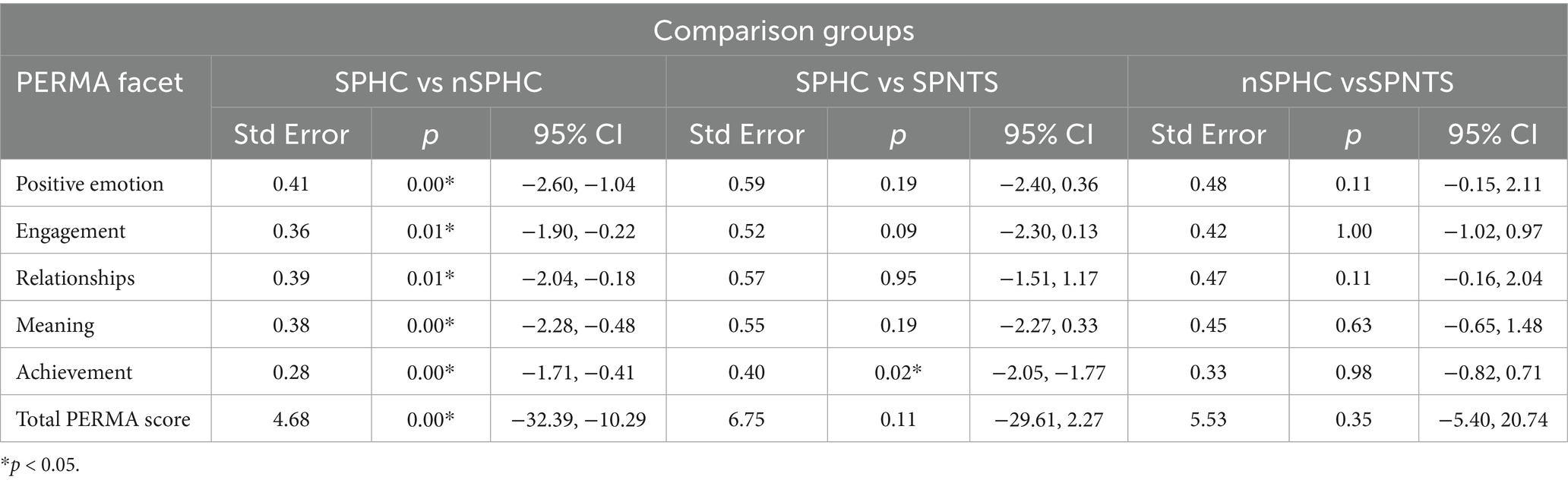
Table 5. Post hoc analysis of suspected psychological health status on workplace wellbeing.
While no difference in overall PERMA scores was noted between SPHC and SPNTS groups, differences at the facet level were noted for achievement [F (2, 192) = 7.65, p < 0.01; SPHC (M = 6.50, SD = 1.51) and SPNTS (M = 7.61, SD = 1.08), p = 0.02, 95% CI = −2.05, −1.77], with the SPNTS group scoring higher than the SPHC group.
No difference in overall PERMA scores was noted between the nSPHC and SPNTS groups [F (2, 192) = 7.52, p = 0.35, 95% CI = −5.40, 20.74].
Suspected psychological health conditions and sQoL
A one-way ANOVA was performed to compare the effect of SPHC on sQoL with follow-up post-hoc tests using Tukey’s HSD Test for Multiple Comparisons.
Suspected psychological health conditions and sQoL
Significant differences were noted in sQoL scores between at least two groups [F (2, 195) = 9.90, p > 0.01], with significant differences between the SPHC (M = 60.11, SD = 15.58) and nSPHC (M = 71.80, SD = 14.66) groups, p > 0.01, 95% CI = −18.90, −4.49, with the nSPHC group demonstrating a higher sQoL score than the SPHC group. These results supported H2, which states that individuals with SPHCs will report lower sQoL compared to individuals without SPHCs (Table 6: One-way ANOVA; Table 7: Post-hoc tests).

Table 6. One-way ANOVA comparing suspected psychological health status effect on sQoL.

Table 7. Post hoc tests for suspected psychological health status effect on sQoL.
There was also a significant difference between the nSPHC and SPNTS groups (M = 62.05, SD = 15.00), p = 0.02, 95% CI = 1.42, 18.08, with SPNTS indicating lower sQoL.
There was no significant difference between the SPHC and SPNTS groups.
Depression, anxiety, and stress levels, workplace wellbeing, and sQoL
SPSS add-on PROCESS Model 4 (Hayes, 2013) was run to assess whether workplace wellbeing PERMA scores mediate the relationship between self-reported depression, anxiety, and stress levels and sQoL.
Mediating effect of workplace wellbeing on the relationship between depression levels and sQoL
There was a significant direct effect of depression level, as measured with the DASS-21, on overall workplace wellbeing, b = −3.81, t = −11.64, p < 0.01 (95% CI = −4.45, −3.16). There was a further direct effect of overall workplace wellbeing on sQoL, b = 0.18, t = 3.62, p < 0.01, (95% CI = 0.08, 0.27), and a direct effect of depression score on sQoL, b = − 1.57, t = −5.48, p < 0.01, (95% CI = −2.14, −1.01).
The total effect model was significant, b = −2.24, t = −9.87, p < 0.01, 95% CI = −2.69, − 1.79. Finally, the indirect effect, b = −0.67, tested using a bootstrapping procedure with 5,000 samples (95% CI = −1.22, −0.22), was statistically significant (Figure 1). These results suggest that PERMA partially mediates the relationship between depression level and sQoL, thus supporting H3.
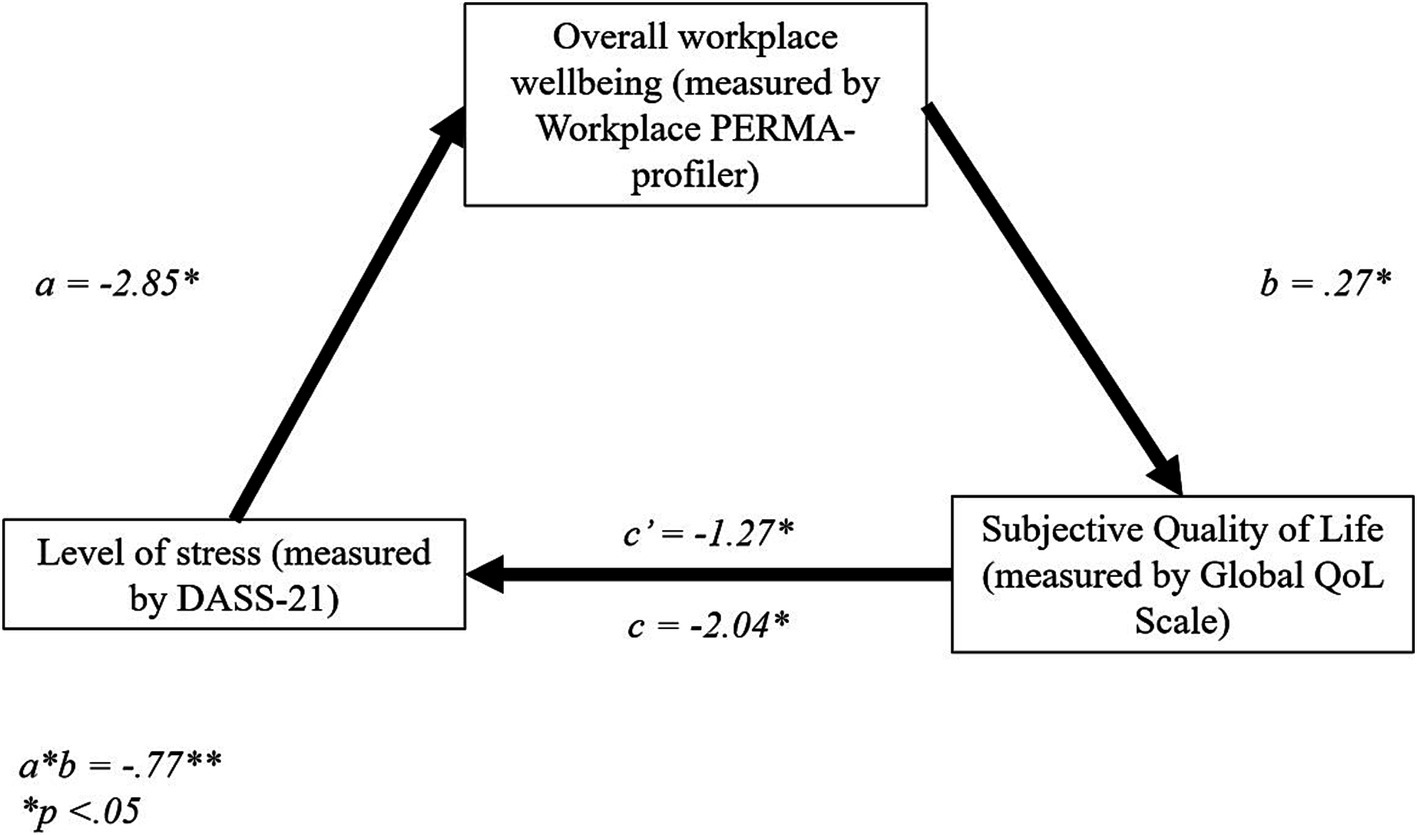
Figure 1. Stanzardised regression coefficients for the relationship between depression and sQoL. *p < 0.05, **p < 0.01.
Mediating effect of workplace wellbeing on the relationship between anxiety levels and sQoL
There was a significant direct effect of anxiety level, as measured with the DASS-21, on overall workplace wellbeing, b = −2.11, t = −3.87, p < 0.01 (95% CI = −3.18, −1.03). There was a further direct effect of overall workplace wellbeing on sQoL, b = 0.33, t = 0.04, p < 0.01, (95% CI = 0.25, 0.41). However, the direct effect of anxiety level on sQoL was not significant, b = −0.42, t = −1.31, p = 0.19, (95% CI = −1.06, 0.22).
The total effect model was significant, b = −1.12, t = −3.12, p < 0.01, 95% CI = −1.83, − 0.41. Finally, the indirect effect, b = −0.70, tested using a bootstrapping procedure with 5,000 samples (95% CI = −1.11, −0.37), was statistically significant (Figure 2). These results suggest that PERMA fully mediates the relationship between anxiety level and sQoL, thus supporting H3.

Figure 2. Standardized regression coefficients for the relationship between anxiety and sQoL. *p < 0.05, **p < 0.01.
Mediating effect of workplace wellbeing on the relationship between stress levels and sQoL
There was a significant direct effect of stress level, as measured with the DASS-21, on overall workplace wellbeing, b = −2.85, t = −6.22, p < 0.01 (95% CI = −3.75, −1.95). There were further direct effects of overall workplace wellbeing on sQoL, b = 0.27, t = 0.04, p < 0.01, (95% CI = 0.19, 0.35), and stress level on sQoL, b = −1.27, t = −4.36, p < 0.01, (95% CI = −1.84, −0.69).
The total effect model was significant, b = −2.04, t = −6.98, p < 0.01, 95% CI = −2.62, −1.46. Finally, the indirect effect, b = −0.77, tested using a bootstrapping procedure with 5,000 samples (95% CI = −1.23, −0.43), was statistically significant (Figure 3). These results suggest that PERMA partially mediates the relationship between stress level and sQoL, thus supporting H3.
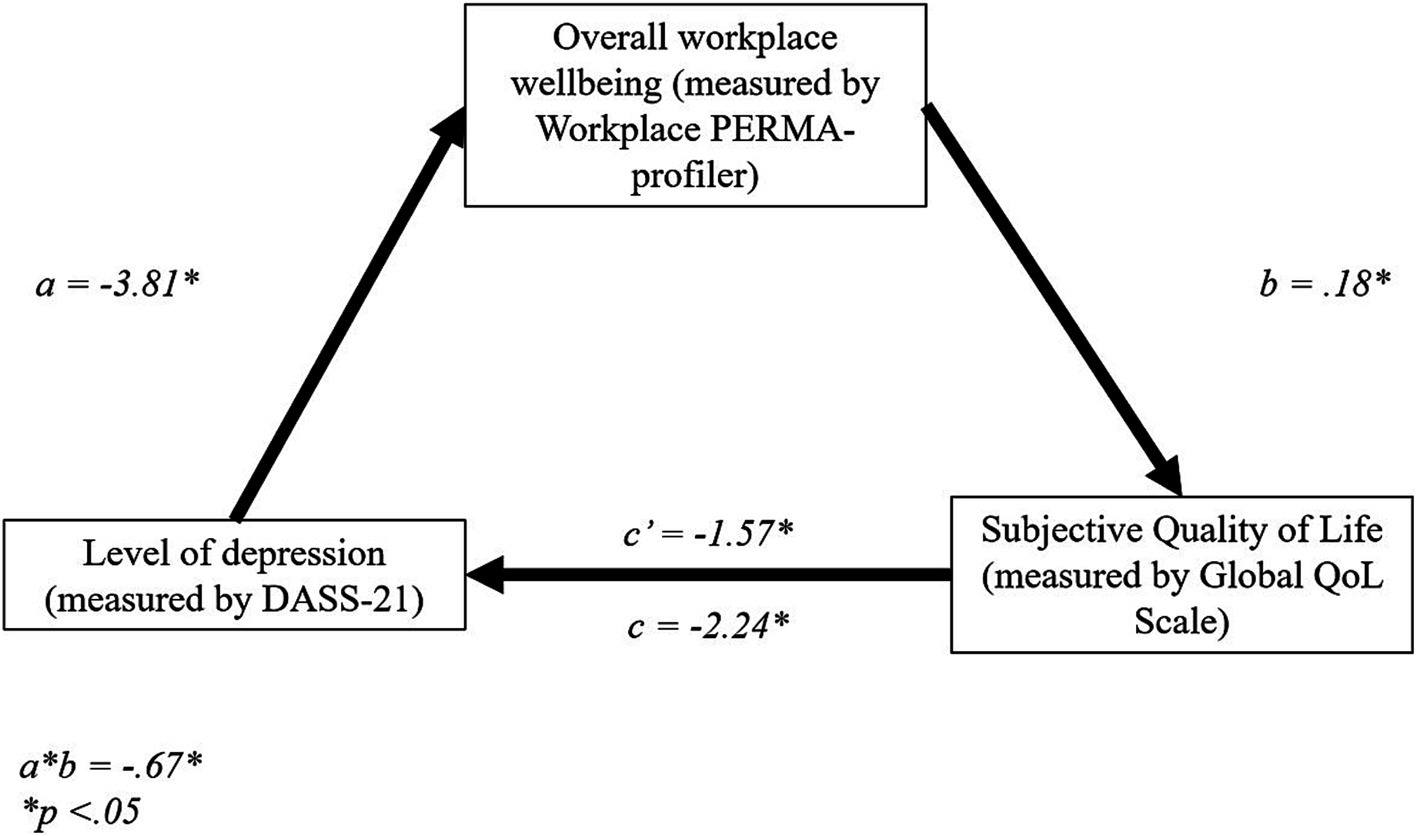
Figure 3. Standardized regression coefficients for the relationship between stress and sQoL. *p < 0.05, **p < 0.01.
Qualitative analysis
This study aimed to explore how individuals within a diverse workplace conceptualize wellbeing. As such, participants were asked to define what wellbeing meant to them. Ritchie and Spencer's (1994) Framework Method, which integrates both inductive and deductive approaches to thematic analysis, was employed to develop themes from participants’ subjective perceptions of what wellbeing means and to determine whether new ideas relating to wellbeing would emerge beyond the PERMA framework. Initial code generation by two researchers yielded 49 individual codes. This was subsequently refined into 10 themes, which, when re-coded, resulted in a 97% inter-rater reliability rate. The remaining data were arbitrated by the third researcher, resulting in 477 statements from 214 responses, which fell into 10 themes (Table 8).
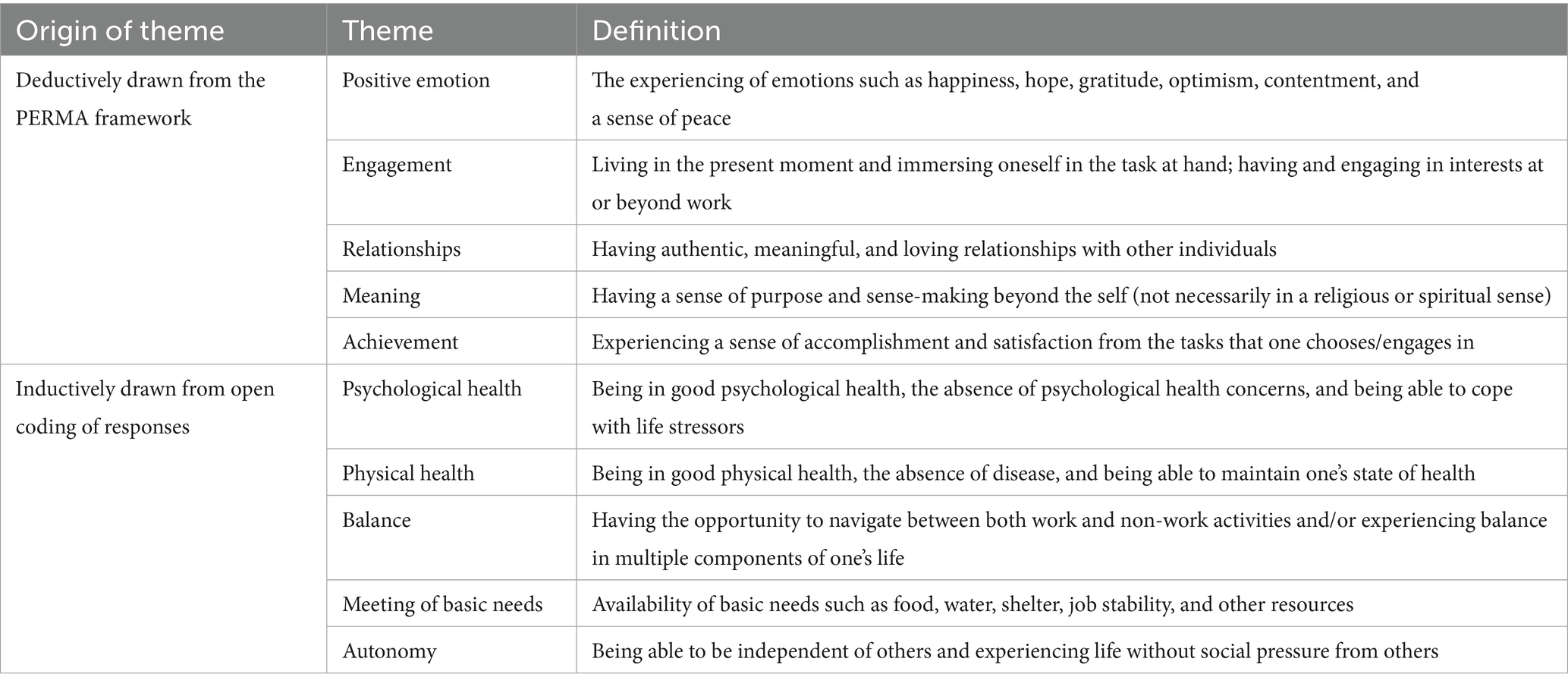
Table 8. Themes identified from qualitative analysis.
The themes are presented below in terms of frequency of appearance, with Psychological Health (N = 104), Physical Health (N = 77), and Positive Emotion (N = 77) being the top three most common responses.
Psychological health
Psychological Health was the most frequently cited theme (N = 107). This theme consists of three distinct components, namely:
1. Being in good psychological health (example response: “(having a) healthy mental state).
2. The absence of poor psychological health (example response: “not always feeling anxious or stressed or in a fight or flight mood”).
3. Being able to cope with stressors and life demands (example response: “able to cope with work demands and stress”).
Physical health
Physical Health and Positive Emotion were in joint second position in terms of frequency in which the themes emerged (N = 77). Physical Health has three broad components, namely:
1. Being in a positive physical state (example response: “(having) high energy”).
2. Being free from physical ailments (example response: “free from sickness”).
3. Having the ability to maintain an optimal state of physical health (example response: “able to rest sufficiently and have a healthy diet”).
Notably, the themes of psychological health and physical health often converged, with many respondents mentioning them simultaneously. Example responses include:
“Being mentally, emotionally, and physically balanced” and “Having a decent quality of life, both physically and mentally.”
Positive emotion
Positive emotion was coded distinctly from Psychological Health, as it focused on the experiencing of desirable emotions and mood states, such as optimism and gratitude, rather than being in an optimal psychological state, the absence of psychological health concerns, or being able to cope with stressors. Example responses include “feeling generally comfortable or at peace with oneself” and “at peace with oneself and the world; get to experience positive emotions like happiness and excitement from time to time.”
Balance
A total of 47 respondents cited having balance as instrumental in helping them experience a sense of wellbeing. Balance consisted of two key components:
1. Being able to achieve equilibrium between work and life (example response: Balance in other components of existence beyond work and personal life).
2. Maintaining balance across multiple life domains beyond just work and personal life (example response: “Having time for rest, being able to spend quality time with loved ones, engaging in meaningful activities, feeling peaceful and having an overall balanced outlook and approach on life”).
Relationships
A total of 39 respondents noted that Relationships contributed to their sense of wellbeing. These respondents noted that they derived wellbeing from having meaningful and authentic relationships with others. Example responses include “(having) support from friends and family and an employer who listens” and “Being able to spend quality time with loved ones.”
Meeting of basic needs
Having basic needs attended to was indicated as a core component of wellbeing for 26 respondents. This entailed having access to food, shelter, jobs, and other resources. Example responses include “to comfortably support the lifestyle that I want for myself and my family financially,” “safe and secure housing, finances, community, employment,” and “having three square meals a day, four if I’m hungry, a bathroom, and a working internet connection.”
Autonomy
A total of 25 respondents noted that having a sense of Autonomy contributed to their sense of wellbeing. In this study, autonomy referred to the freedom to make independent choices without external pressure or imposed values. Example responses include “being able to live according to your personal needs and wishes rather than constraints imposed on you by your environment,” “good locus of control,” and “some extent of freedom of expression and not being tied down by anything.”
Engagement
A total of 21 respondents indicated that Engagement contributed to their wellbeing and highlighted the importance of being able to immerse oneself in one’s chosen activities. Example responses include “being able to work with the flow” and “being fully engaged at work.”
Meaning
A total of 19 respondents indicated that having a sense of meaning, or a sense of purpose and sense-making beyond the self, contributed to their sense of wellbeing. Example responses include “having a meaningful purpose,” “engaging in meaningful activities such as learning and playing,” and “spiritually, he/she is balanced with a good religious belief.”
Achievement
Finally, seven respondents indicated that Achievement, or experiencing a sense of accomplishment in one’s chosen tasks, was important for feeling a sense of wellbeing. Example responses include “thriving at work and in my personal life, achieving goals” and “a certain level of sense of achievement at work.”
Discussion
This study demonstrated that individuals who suspected they had psychological health concerns (SPHC) reported lower workplace wellbeing and subjective quality of life (sQoL) than individuals who did not suspect having PHCs (nSPHC). Individuals who preferred not to say whether they suspected they had PHCs (SPNTS) also reported lower sQoL as compared to individuals who did not suspect they had a PHC (nSPHC). More importantly, the relationships between distress, as measured by the DASS-21, and sQoL were mediated by workplace wellbeing. Specifically, while the relationship between anxiety and sQoL was fully mediated by workplace wellbeing, the relationships between depression and sQoL and stress and sQoL were partially mediated.
Finally, the qualitative analysis indicated that Psychological Health, Physical Health, and Positive Emotion were the top three commonly cited contributors to wellbeing. Further contributors to wellbeing include Balance, Relationships, Meeting basic needs, Autonomy, Engagement, Meaning, and Achievement.
Importance of a multifaceted conceptualization of wellbeing
The present research noted higher overall PERMA scores and individual PERMA facet scores in individuals from the nSPHC group compared to their counterparts from the SPHC group, with no single area being deemed less significant. This has implications on multiple levels. At the individual level, for those who experience SPHC but have yet to be diagnosed, conducting brief assessments and identifying gaps using the PERMA framework can also serve as a means of identifying areas of need and providing customized care. Interventions focusing on PERMA facets may then be helpful as a preventative strategy against psychological health concerns, with previous research showing the effectiveness of holistic PERMA-based interventions in mitigating psychological ill-health in areas such as distress, depression, anxiety, insomnia, and fear of disease progression in liver cancer patients (Guo et al., 2025). Such research suggests that interventions encompassing PERMA elements augment the current predominant symptomatic health management framework by emphasizing psychosocial elements beyond the mere absence of disease, thereby contributing to a more holistic healthcare model. On a broader level, within an organization, these results suggest that integrating PERMA elements and organizational policy may hold value in improving public health and wellbeing at a population level, such as through workplace wellbeing programs and policies.
Suspecting having a psychological health concern
While the current study did not explicitly compare levels of distress in individuals who suspected they had PHCs to individuals who did not suspect having PHCs, the significantly lower PERMA and sQoL levels of SPHC as compared to nSPHC groups converge with previous literature that demonstrated that individuals who suspected that they had psychological health conditions had lower QoL and were more likely to meet clinically significant levels of psychological health symptoms as compared to individuals who did not suspect any psychological health conditions (Liu et al., 2020).
Individuals in the SPHC group experience lower sQoL, suggesting there is a potential impact of their psychological health state on their sQoL. Furthermore, while they have insight and are concerned about their psychological health, they may not have sought a formal diagnosis. Barriers to help-seeking in culturally diverse populations include the cost of treatment, the belief that treatment was unnecessary as the health concern would eventually subside, and fear of discrimination (Subramaniam et al., 2019). In addition to conducting further research into the barriers to help-seeking, interventions such as psychoeducation to increase mental health literacy, destigmatization, and motivational enhancement can be implemented to increase formal help-seeking behavior (Xu et al., 2018). Improving access to affordable psychological healthcare in the workplace and at a societal level is also warranted.
Currently, many companies offer subsidized rates for physical health checkups for their staff. As individuals become more aware of the importance of psychological health, it may also be beneficial to incorporate psychological health screening into employee benefit packages, allowing interested individuals to seek help if needed.
Mediating effect of wellbeing on the relationship between depression, anxiety, and stress levels and sQoL
Previous literature has discussed how general wellbeing is specifically associated with work-related quality of life (QoL) (McFadden et al., 2021), while the current findings contribute to the research on how workplace PERMA mediates the relationship between depression, anxiety, stress levels, and subjective quality of life (sQoL). This adds to the literature that demonstrated PERMA mediates the relationship between depression and QoL (Choi, 2020). The present results provide implications on how potentially increasing workplace wellbeing can help to improve overall sQoL. This would benefit not only individuals but also organizations and the wider community, given that psychological health concerns and related losses in productivity are estimated to cost the global economy USD 2.5 trillion per year (The Lancet Global Health, 2020).
Regarding the differences between depression, anxiety, and stress, while workplace wellbeing only partially mediated the relationship between depression and stress and sQoL, it fully mediated the relationship between anxiety and sQoL. This suggests that workplace wellbeing interventions may be crucial in improving the sQoL of individuals with higher anxiety levels as compared to higher depression and stress levels. Interventions targeted at individuals with higher levels of anxiety may be particularly effective in increasing job productivity, especially given the higher level of anxiety as compared to depression in the workplace (Deady et al., 2021) and how anxiety is associated with increased levels of poorer work functioning and absenteeism (Plaisier et al., 2010). Nevertheless, it remains important to work toward workplace wellbeing for workers in general, as there are high comorbidity rates between anxiety and depression (Groen et al., 2020).
Notably, a study by Weziak-Bialowolska et al. (2020) suggests that there are bidirectional effects between life satisfaction and work satisfaction, with the former having a greater impact on the latter than vice versa. Given the impact of workplace wellbeing on sQoL in the present research, it may be helpful for future studies to consider the combined effect of both non-work and workplace wellbeing on QoL, especially in relation to the amount of time individuals spend in their work life. This may then help inform how wellbeing interventions can be applied in both individual and workplace settings.
The function of non-disclosure
The rates of nondisclosure of suspected psychological health concerns (SPNTS = 10.1%, N = 20) in the present study appears on the higher end as compared to the rate of nondisclosure of other sensitive information, such as sexual activity and household income, ranging from 0.87 to 8.15% in past research (Tourangeau and Yan, 2007).
Respondents may have been cautious about divulging their psychological health status (PHS) for two reasons: first, it may be perceived as a sensitive topic, and second, respondents are concerned that the information they share may be disclosed to third parties (Tourangeau and Yan, 2007).
There were no differences in the sQoL of SPHC individuals and SPNTS individuals. However, both SPNTS and SPHC groups demonstrated significantly lower sQoL as compared to individuals who did not suspect they had psychological health conditions (nSPHC). This suggests that the SPNTS and SPHC groups are more similar to each other compared to the nSPHC group. While there are few studies on non-disclosure of PHS and levels of distress, previous research has demonstrated that non-disclosure of suicide ideation was associated with increased loneliness, poorer health, increased psychological distress, and more frequent suicide ideation (Mérelle et al., 2018). Importantly, Brouwers et al. (2019) suggests that employers can support employees with SPHCs but PNTS in the disclosure process by providing information about how they can disclose their PHC and who they should disclose it to so that individuals with PNTS may seek treatment more easily. Individuals who feel supported and are receiving treatment are also more likely to disclose PHS in the workplace (Reavley et al., 2017). It may prove more beneficial in workplace settings to facilitate ease of access to treatment (e.g., providing subsidized, anonymous therapy services) and foster healthy workplace relationships so that individuals who are hesitant to disclose their PHS would feel more comfortable seeking treatment and receive the support they need.
Qualitative findings
Respondents in the current study were not primed to Seligman’s WBT. While the five PERMA facets did appear as coded responses, five additional themes were identified: Psychological Health, Physical Health, Balance, Meeting of Basic Needs, and Autonomy. These themes may be referred to as lay conceptualizations of wellbeing, or intuitive structures and theories by lay people to define and experience wellbeing, definitions which may differ from how theorists attempt to interpret wellbeing (McMahan et al., 2012). Interestingly, several lay theories proposed by participants in the present study align with additional domains proposed by Seligman’s WBT or the more recent PERMA+4 (Donaldson et al., 2022). These four additional domains are namely:
1. Physical health: Having positive physical health assets such as good genes and physical functioning.
2. Mindset: Having a growth mindset and the ability to overcome setbacks.
3. Work environment: A physical work environment that is suited to the individual’s needs that includes spatiotemporal elements such as sufficient space and natural light and.
4. Economic security: Experiencing financial stability and security in line with the individual’s needs (Donaldson et al., 2022).
The most frequently cited lay theory of wellbeing in the current study, Psychological Health, emphasizes the ability to cope with life stressors as a key component and bears resemblance to the PERMA+4’s proposed addition of Mindset. Psychological Health has previously been cited as a key lay conceptualization of wellbeing (Jarden et al., 2018), and such research, together with the current study, provides support for the proposed addition of this component as a PERMA+4 domain. Future studies may consider further exploring and refining the concept of psychological health and mindset for incorporation into the PERMA.
Physical Health in the present study was defined as being in good physical health, being free from physical ailments, and having the ability to maintain an optimal state of physical functioning. It is inherently similar to the definition of the PERMA+4’s conceptualization of Physical Health. The present study, along with others that also explore lay conceptualizations of wellbeing (Hone et al., 2015; Huang et al., 2022), provides support for incorporating physical health as a PERMA+4 domain.
Economic Security in the PERMA+4 also bears a resemblance to the current study’s theme of Meeting Basic Needs. It is supported by other studies on lay theories of wellbeing, citing the importance of concepts such as financial security (Downey, 2006) and infrastructural and food availability (Joshanloo et al., 2021) to human beings. Given the importance of cultural context in the development of lay theories (Joshanloo et al., 2021), the emergence of this theme may potentially indicate the current state of the world post-COVID, where job insecurity and financial anxiety are on the rise, justifying Economic Security as an additional facet of PERMA+4.
Apart from the similarities to the PERMA+4’s additional domains, the current study also identified other lay theories of wellbeing worthy of further exploration. Importantly, Positive Emotion and Psychological Health were coded as distinct themes, with Positive Emotion referring more to the experiencing of emotions such as happiness and peace, and Psychological Health referring to not just being in good psychological health but also being able to cope with adversity. The ability to cope with adverse experiences, at least in the present study, appears more frequently than the need to experience Positive Emotions. It is telling of the cultural diversity of the current population that these concepts appear as the two most important lay conceptualizations of wellbeing, given how Western-centric cultures tend to favor hedonistic notions of happiness (i.e., experiencing positive emotions) whilst many other cultures view suffering as an inevitable part of life (Joshanloo et al., 2021), possibly explaining here the necessity of being able to cope with challenges as a part of psychological health.
Balance was another frequently cited lay theory, referring not only to navigating between work and non-work activities but also to achieving balance in other areas outside of work and life (e.g., spiritual balance). While work-life balance has been defined as a lay theory in previous research (Hone et al., 2015), deeper notions of balance in non-Western cultures highlight the importance of maintaining a state of equilibrium between both positive and negative aspects while avoiding either extreme (Wong and Liu, 2018). Supporting this point, only one response in the data set defined wellbeing as not needing to work.
Autonomy was the final conceptualization of wellbeing, as derived from participants’ responses. While not part of Seligman’s WBT, autonomy appears as a key part of other wellbeing theories such as Ryff’s (1989) Scales of Psychological Wellbeing, which defines Autonomy as being self-determining and independent, and COMPAS-W, which defines Own-Worth as knowing one’s values and establishing healthy boundaries (Gatt et al., 2014). Autonomy may be a worthy contender for inclusion in the PERMA model in the future.
All in all, the above-derived lay theories of wellbeing demonstrate that, while there are parallels between general perception and theory, laypeople’s understanding of wellbeing adds a unique cultural and situational lens. It would then be important to carefully consider the distinct population in which wellbeing is being measured and craft interventions based on both theory and lay perceptions to cater to the identified population’s unique wellbeing needs.
At the same time, it may be important for researchers to acknowledge that there may never be a PERMA-nent understanding of wellbeing. Rather, wellbeing appears to be a constantly evolving concept, contingent upon time and space. Re-looking at definitions of wellbeing and refining wellbeing interventions may then need to occur periodically, especially in times of global upheaval, such as the COVID-19 pandemic.
Study limitations and future directions
Regarding this study’s limitations, as the research focused on individuals who experienced SPHC, the experiences of individuals with diagnosed PHCs were not explored. There was also no comparison made between how wellbeing is defined by individuals with SPHC and individuals without SPHC. This is a pity, as Connell et al. (2014) suggest that wellbeing may be defined differently for people with and without diagnosed PHC. Future studies may wish to expand on comparisons between individuals with diagnosed PHCs, individuals experiencing SPHCs, and individuals who do not have or suspect having PHCs.
A second limitation in the present research is that demographic factors, such as age, ethnicity, and gender, and how they may manifest differently within the PERMA framework, were not explored. Few studies to date have thoroughly explored these differences, or if explored, findings have been inconsistent. For example, Burke and Minton (2019) observed that Irish male students had higher PERMA scores as compared to their female counterparts. However, Al-Hendawi et al. (2024) note negligible gender differences in PERMA scores. Exploring sociodemographic differences in wellbeing and quality of life, as well as the possible mechanisms behind these observable differences, is worthy of consideration in future research. In addition, research on what specific groups consider lay theories of wellbeing would also be valuable, as the present research has reflected that individuals’ definitions of wellbeing expand beyond current theoretical definitions. Such information would be invaluable in crafting suitable positive psychology interventions for specific groups, which, in turn, could benefit society as a whole.
Third, a missed opportunity in the present study was to further explore which factors might cause individuals to disclose PHC factors that hinder seeking help or diagnosis if they experienced SPHC, and how these areas relate to wellbeing. Doing so can help address issues related to help-seeking and interventions for individuals who experience SPHC.
Finally, future studies may wish to expand on which aspects contribute to a greater sense of wellbeing in various parts of the population (SPHC, no SPHC, SPNTS, diagnosed PHC). This is essential for developing interventions that promote both symptomatic and personal recovery.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by National University of Singapore Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
XN: Formal analysis, Data curation, Conceptualization, Methodology, Investigation, Writing – original draft. JC: Writing – review & editing, Formal analysis, Supervision. KD: Supervision, Writing – review & editing, Formal analysis.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
KD was employed by INSiGHT Therapeutics and Consulting.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Al-Hendawi, M., Alodat, A., Al-Zoubi, S., and Bulut, S. (2024). A PERMA model approach to well-being: a psychometric properties study. BMC Psychol. 12:414. doi: 10.1186/s40359-024-01909-0
Andenæs, R., Kalfoss, M. H., and Wahl, A. (2004). Psychological distress and quality of life in hospitalized patients with chronic obstructive pulmonary disease. J. Adv. Nurs. 46, 523–530. doi: 10.1111/j.1365-2648.2004.03026.x
Brouwers, E. P. M., Joosen, M. C. W., van Zelst, C., and Van Weeghel, J. (2019). To disclose or not to disclose: a multi-stakeholder focus group study on mental health issues in the work environment. J. Occup. Rehabil. 30, 84–92. doi: 10.1007/s10926-019-09848-z
Brown, T. A., Chorpita, B. F., Korotitsch, W., and Barlow, D. H. (1997). Psychometric properties of the depression anxiety stress scales (DASS) in clinical samples. Behav. Res. Ther. 35, 79–89. doi: 10.1016/s0005-7967(96)00068-x
Burke, J., and Minton, S. J. (2019). Well-being in post-primary schools in Ireland: the assessment and contribution of character strengths. Ir. Educ. Stud. 38, 177–192. doi: 10.1080/03323315.2018.1512887
Butler, J., and Kern, M. L. (2016). The PERMA-profiler: a brief multidimensional measure of flourishing. Int. J. Wellbeing 6, 1–48. doi: 10.5502/ijw.v6i3.526
Choi, M. Y. (2020). Mental and physical factors influencing wellbeing among south Korean emergency workers. Int. J. Environ. Res. Public Health 18:70. doi: 10.3390/ijerph18010070
Connell, J., O’Cathain, A., and Brazier, J. (2014). Measuring quality of life in mental health: are we asking the right questions? Soc. Sci. Med. 120, 12–20. doi: 10.1016/j.socscimed.2014.08.026
Cummins, R. A. (2000). Objective and subjective quality of life: an interactive model. Soc. Indic. Res. 52, 55–72. doi: 10.1023/A:1007027822521
Deady, M., Collins, D. a. J., Johnston, D. A., Glozier, N., Calvo, R. A., Christensen, H., et al. (2021). The impact of depression, anxiety and comorbidity on occupational outcomes. Occup. Med. 72, 17–24. doi: 10.1093/occmed/kqab142
Deci, E. L., and Ryan, R. M. (2006). Hedonia, eudaimonia, and well-being: an introduction. J. Happiness Stud. 9, 1–11. doi: 10.1007/s10902-006-9018-1
Diener, E. (1984). Subjective well-being. Psychol. Bull. 95, 542–575. doi: 10.1037/0033-2909.95.3.542
Donaldson, S. I., Van Zyl, L. E., and Donaldson, S. I. (2022). PERMA+4: a framework for work-related wellbeing, performance and positive organizational psychology 2.0. Front. Psychol. 12:7244. doi: 10.3389/fpsyg.2021.817244
Downey, C. A. (2006). Lay theories of Health: multidimensional conceptualizations of what comprises health in young and middle-aged adults. Michigan: University of Michigan.
Faisal-Cury, A., Ziebold, C., De Oliveira Rodrigues, D. M., and Matijasevich, A. (2022). Depression underdiagnosis: prevalence and associated factors. A population-based study. J. Psychiatr. Res. 151, 157–165. doi: 10.1016/j.jpsychires.2022.04.025
Gale, N. K., Heath, G., Cameron, E., Rashid, S., and Redwood, S. (2013). Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 13:117. doi: 10.1186/1471-2288-13-117
Gatt, J. M., Burton, K. L., Schofield, P. R., Bryant, R. A., and Williams, L. M. (2014). The heritability of mental health and wellbeing defined using COMPAS-W, a new composite measure of wellbeing. Psychiatry Res. 219, 204–213. doi: 10.1016/j.psychres.2014.04.033
Groen, R. N., Ryan, O., Wigman, J. T. W., Riese, H., Penninx, B. W. J. H., Giltay, E. J., et al. (2020). Comorbidity between depression and anxiety: assessing the role of bridge mental states in dynamic psychological networks. BMC Med. 18:308. doi: 10.1186/s12916-020-01738-z
Guo, J., Zhang, Y., Yang, F., Zhou, Y., Feng, T., and Deng, X. (2025). The impact of emotional release technique combined with the PERMA model intervention on the fear of disease progression in patients after liver cancer surgery. J. Kunming Med. Univ. 46, 163–169. doi: 10.12259/j.issn.2095-610X.S20250422
Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York: The Guilford Press.
Hone, L. C., Jarden, A., Duncan, S., and Schofield, G. M. (2015). Flourishing in New Zealand workers. Journal of Occupational and Environmental Medicine. 57, 973–983. doi: 10.1097/jom.0000000000000508
Huang, L., Kern, M. L., and Oades, L. G. (2022). Chinese international students’ conceptualizations of wellbeing: a prototype analysis. Front. Psychol. 13:939576. doi: 10.3389/fpsyg.2022.939576
Hyland, M. E., and Sodergren, S. C. (1996). Development of a new type of global quality of life scale, and comparison of performance and preference for 12 global scales. Qual. Life Res. 5, 469–480. doi: 10.1007/bf00540019
Islam, M. I., Yunus, F. M., Isha, S. N., Kabir, E., Khanam, R., and Martiniuk, A. (2022). The gap between perceived mental health needs and actual service utilization in Australian adolescents. Sci. Rep. 12:5430. doi: 10.1038/s41598-022-09352-0
Jarden, R. J., Sandham, M., Siegert, R. J., and Koziol-McLain, J. (2018). Intensive care nurse conceptions of well-being: a prototype analysis. Nurs. Crit. Care 23, 324–331. doi: 10.1111/nicc.12379
Joshanloo, M., Van De Vliert, E., and Jose, P. E. (2021). “Four fundamental distinctions in conceptions of wellbeing across cultures” in The Palgrave handbook of positive education. eds. M. L. Kern and M. L. Wehmeyer (New York: Springer), 675–703.
Kasper, S. (2006). Anxiety disorders: under-diagnosed and insufficiently treated. Int. J. Psychiatry Clin. Pract. 10, 3–9. doi: 10.1080/13651500600552297
Kern, M. L., Waters, L., Adler, A., and White, M. (2014). Assessing employee wellbeing in schools using a multifaceted approach: associations with physical health, life satisfaction, and professional thriving. Psychology 5, 500–513. doi: 10.4236/psych.2014.56060
Liu, C., Stevens, C., Conrad, R., and Hahm, H. (2020). Evidence for elevated psychiatric distress, poor sleep, and quality of life concerns during the COVID-19 pandemic among U.S. young adults with suspected and reported psychiatric diagnoses. Psychiatry Res. 292:113345. doi: 10.1016/j.psychres.2020.113345
McFadden, P., Ross, J., Moriarty, J., Mallett, J., Schroder, H., Ravalier, J., et al. (2021). The role of coping in the wellbeing and work-related quality of life of UK Health and social care workers during COVID-19. Int. J. Environ. Res. Public Health 18:815. doi: 10.3390/ijerph18020815
McLaughlin, C. G. (2004). Delays in treatment for mental disorders and health insurance coverage. Health Serv. Res. 39, 221–224. doi: 10.1111/j.1475-6773.2004.00224.x
McMahan, E. A., Dixon, K. J., and King, L. M. (2012). Evidence of associations between lay conceptions of well-being, conception-congruent behavior, and experienced well-being. J. Happiness Stud. 14, 655–671. doi: 10.1007/s10902-012-9347-1
Mérelle, S., Foppen, E., Gilissen, R., Mokkenstorm, J., Cluitmans, R., and Van Ballegooijen, W. (2018). Characteristics associated with non-disclosure of suicidal ideation in adults. Int. J. Environ. Res. Public Health 15:943. doi: 10.3390/ijerph15050943
Meyers, M. C., Van Woerkom, M., and Bakker, A. B. (2012). The added value of the positive: a literature review of positive psychology interventions in organizations. Eur. J. Work Organ. Psychol. 22, 618–632. doi: 10.1080/1359432x.2012.694689
Neumeier, L. M., Brook, L., Ditchburn, G., and Sckopke, P. (2017). Delivering your daily dose of well-being to the workplace: a randomized controlled trial of an online well-being programme for employees. Eur. J. Work Organ. Psychol. 26, 555–573. doi: 10.1080/1359432x.2017.1320281
Plaisier, I., Beekman, A., De Graaf, R., Smit, J., Van Dyck, R., and Penninx, B. (2010). Work functioning in persons with depressive and anxiety disorders: the role of specific psychopathological characteristics. J. Affect. Disord. 125, 198–206. doi: 10.1016/j.jad.2010.01.072
Reavley, N. J., Morgan, A. J., and Jorm, A. F. (2017). Disclosure of mental health problems: findings from an Australian national survey. Epidemiol. Psychiatr. Sci. 27, 346–356. doi: 10.1017/s204579601600113x
Ritchie, J., and Spencer, L. (1994). “Qualitative data analysis for applied policy research” in Analyzing qualitative data. eds. A. Bryman and R. Burgess (London: Routledge), 173–194.
Ryan, J., Curtis, R., Olds, T., Edney, S., Vandelanotte, C., Plotnikoff, R., et al. (2019). Psychometric properties of the PERMA profiler for measuring wellbeing in Australian adults. PLoS One 14:e0225932. doi: 10.1371/journal.pone.0225932
Ryff, C. D. (1989). Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Pers. Soc. Psychol. 57, 1069–1081. doi: 10.1037/0022-3514.57.6.1069
Seligman, M. E. P. (2011). Flourish: a visionary new understanding of happiness and well-being. New York, NY: Simon and Schuster.
Sinclair, S. J., Siefert, C. J., Slavin-Mulford, J. M., Stein, M. B., Renna, M., and Blais, M. A. (2011). Psychometric evaluation and normative data for the depression, anxiety, and stress Scales-21 (DASS-21) in a nonclinical sample of U.S. adults. Eval. Health Prof. 35, 259–279. doi: 10.1177/0163278711424282
Skevington, S., and Böhnke, J. (2018). How is subjective well-being related to quality of life? Do we need two concepts and both measures? Soc. Sci. Med. 206, 22–30. doi: 10.1016/j.socscimed.2018.04.005
Slade, M. (2010). Mental illness and well-being: the central importance of positive psychology and recovery approaches. BMC Health Serv. Res. 10:26. doi: 10.1186/1472-6963-10-26
Subramaniam, M., Abdin, E., Vaingankar, J. A., Shafie, S., Chua, H. C., Tan, W. M., et al. (2019). Minding the treatment gap: results of the Singapore mental Health study. Soc. Psychiatry Psychiatr. Epidemiol. 55, 1415–1424. doi: 10.1007/s00127-019-01748-0
The Lancet Global Health (2020). Mental health matters. Lancet Glob. Health 8:e1352. doi: 10.1016/s2214-109x(20)30432-0
Tourangeau, R., and Yan, T. (2007). Sensitive questions in surveys. Psychol. Bull. 133, 859–883. doi: 10.1037/0033-2909.133.5.859
Vaingankar, J. A., Chong, S. A., Abdin, E., Kumar, F. D. S., Chua, B. Y., Sambasivam, R., et al. (2020). Understanding the relationships between mental disorders, self-reported health outcomes and positive mental health: findings from a national survey. Health Qual. Life Outcomes 18:55. doi: 10.1186/s12955-020-01308-0
Weziak-Bialowolska, D., Bialowolski, P., Sacco, P. L., VanderWeele, T. J., and McNeely, E. (2020). Well-being in life and well-being at work: which comes first? Evidence from a longitudinal study. Front. Public Health 8:103. doi: 10.3389/fpubh.2020.00103
Wong, Y. J., and Liu, T. (2018). “Dialecticism and mental health: toward a yin-yang vision of well-being” in The psychological and cultural foundations of east Asian cognition: contradiction, change, and holism. eds. J. Spencer-Rodgers and K. Peng (Oxford: Oxford University Press), 547–572.
Keywords: workplace wellbeing, mental health, PERMA, subjective quality of life, multicultural population
Citation: Ng XH, Chu J and Doshi K (2025) A PERMA-nent solution to understanding psychological wellbeing? Exploring the utility of the PERMA model in a university workplace. Front. Psychol. 16:1598910. doi: 10.3389/fpsyg.2025.1598910
Edited by:
Hans Henrik Knoop, Aarhus University, DenmarkReviewed by:
Siaw Leng Chan, Universiti Putra Malaysia Bintulu Sarawak Campus, MalaysiaPrisla Ücker Calvetti, Federal University of Health Sciences of Porto Alegre, Brazil
Copyright © 2025 Ng, Chu and Doshi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiao Hui Ng, eGhuZ0BudXMuZWR1LnNn