 Adelaide Austin1
Adelaide Austin1 Gabriela M. Jiga-Boy1,2
Gabriela M. Jiga-Boy1,2 Sara Rea1
Sara Rea1 Simon A. Newstead1Sian Roderick2,3
Simon A. Newstead1Sian Roderick2,3 Nick J. Davis1R. Marc Clement3
Nick J. Davis1R. Marc Clement3 Frédéric Boy1,2,3*
Frédéric Boy1,2,3*- 1Department of Psychology, College of Human and Health Science, Swansea University, Swansea, Wales
- 2NeuroTherapeutics Limited, Institute of Life Science, Swansea University, Swansea, Wales
- 3Scientia Research Group, School of Medicine, Swansea University, Swansea, Wales
Negative emotional responses to the daily life stresses have cumulative effects which, in turn, impose wide-ranging negative constraints on emotional well being and neurocognitive performance (Kalueff and Nutt, 2007; Nadler et al., 2010; Charles et al., 2013). Crucial cognitive functions such as memory and problem solving, as well more short term emotional responses (e.g., anticipation of- and response to- monetary rewards or losses) are influenced by mood. The negative impact of these behavioral responses is felt at the individual level, but it also imposes major economic burden on modern healthcare systems. Although much research has been undertaken to understand the underlying mechanisms of depressed mood and design efficient treatment pathways, comparatively little was done to characterize mood modulations that remain within the boundaries of a healthy mental functioning. In one placebo-controlled experiment, we applied daily prefrontal transcranial Direct Current Stimulation (tDCS) at five points in time, and found reliable improvements on self-reported mood evaluation. Using a new team of experimenters, we replicated this finding in an independent double-blinded placebo-controlled experiment and showed that stimulation over a shorter period of time (3 days) is sufficient to create detectable mood improvements. Taken together, our data show that repeated bilateral prefrontal tDCS can reduce psychological distress in non-depressed individuals.
Introduction
One function of the dorsolateral prefrontal cortex (DLPFC) is to continuously appraise the emotional content of daily life situations, and to rapidly regulate oriented responses (Lévesque et al., 2003; Banks et al., 2007). The strong negative impact of daily stressors on current mood is well known (Bolger et al., 1989). Over time, the outcomes of this idiosyncratic evaluative and responsive process amass, and impact individuals’ emotional wellbeing and neurocognitive performance (Nadler et al., 2010; Charles et al., 2013). Here, we exploited the modulation of GABA- and glutamate-ergic neurotransmission (Stagg et al., 2009, 2011; Stagg and Nitsche, 2011; Kim et al., 2014) and cortical excitability (Romero Lauro et al., 2014) caused by transcranial Direct Current Stimulation (tDCS) to determine whether negative emotional responses to daily life stresses can be reduced in healthy individuals. tDCS involves placing two macro-electrodes on the scalp, and passing a weak regulated direct current (in the order of the mA) between them. Recent evidence from clinical research shows that repeated prefrontal tDCS in depressed patients produces measurable clinical benefits. Meta-analyses of recent open-label studies and double-blinded trials for the treatment of major depressive disorder (Fregni et al., 2006a,b; Boggio et al., 2008; Loo et al., 2010, 2012; Brunoni et al., 2011a; Dell’Osso et al., 2012), found that active prefrontal tDCS was associated, on average, with a 29.1 ± 4.6% reduction in depressive symptoms; and five of these studies detected long-lasting benefits a month after the last stimulation. In addition, Brunoni et al. (2011b) also found that 1-active tDCS was more effective than sham, 2-tDCS was as effective as Sertraline, a selective serotonin reuptake inhibitor (SSRI) antidepressant and, 3-tDCS and SSRI combined have greater efficacy than each treatment alone. This body of evidence strongly suggests that repeated daily prefrontal tDCS can be an effective tool for improving mood in depressed patient.
However, the present challenge is to understand the neurobiological underpinnings and the psychological mechanisms at play in this effect. Here, we took the original approach of studying how repeated prefrontal tDCS modulated the way non-depressed volunteers self-evaluated the emotional states consequent to life events (stressful or not). This is particularly relevant since one of the leading causal factors in depression onset is the accumulation of negative emotional states resulting from sustained or chronic exposure to stressful life events (Gandiga et al., 2006).
Materials and Methods
Participants
Sixty-six early adult, unmedicated, non-depressed females from Swansea University (mean age: 21.6 ± 2.3 years) participated in the experiments reported here in exchange for payment (£20) or course credit. All participants provided informed consent, were naïve to the purpose of the experiments and had no neuropsychiatric history. Participants were aware that the experimental manipulation repeatedly used tDCS neuromodulation and that they would have to complete several questionnaires, but no further specification was given as to the nature of the hypotheses. The departmental Research Ethics Committee approved all procedures. After completion of experiment 1, two participants voluntarily reported significant events that affected their current mood (passing of a relative, relationship breakup), and their data were discarded.
Bilateral Prefrontal tDCS
A DC stimulator (neuroConn DC stimulator, Ilmenau, Germany) delivered a 1500 mA current to the scalp via 5 × 5 cm rubber-graphite electrodes (current density: 0.06 mA/cm2). Impedance was automatically monitored every 5 s, and tension adjusted accordingly, so as to deliver constant current (within safety limits). In experiment 1 and 2 the anode was centered over the left F3 10–20 position (Figure 1). The cathode was placed over the contralateral F4 position (for similar electrodes placement see Brunoni et al., 2011b; Dell’Osso et al., 2012). Sponges soaked in 0.9% NaCl solution (Sterowash, Steroplast, Manchester, UK) were used to create a conducting medium between the scalp and electrodes. For active stimulation, the current was ramped up over 15 s and was then held at 1500 mA for 12 min, before being ramped down over 15 s. For sham stimulations, the stimulator was automatically switched off after an initial ramp-up (15 s at 0.1 mA s-1), plateau periods (6 s at 1.5 mA), and final ramp-down (15 s at -0.1 mA s-1), to create a realistic placebo control condition (Brunoni et al., 2012) that still generated the short lasting tingling sensations identical to those felt at the beginning of the active tDCS stimulations. Usually, only these very mild sensations are experienced (Gandiga et al., 2006), and when directly asked, most participants do not even perceive a difference between active and sham stimulation (Poreisz et al., 2007). Experiment 1 was single blinded (24 participants randomly allocated to either conditions in a equal proportion), whereas Experiment 2 was a double-blind randomized trial, where neither participants, nor experimenters knew whether the stimulation was active or sham (28 participants in the active condition, 14 in the sham condition).
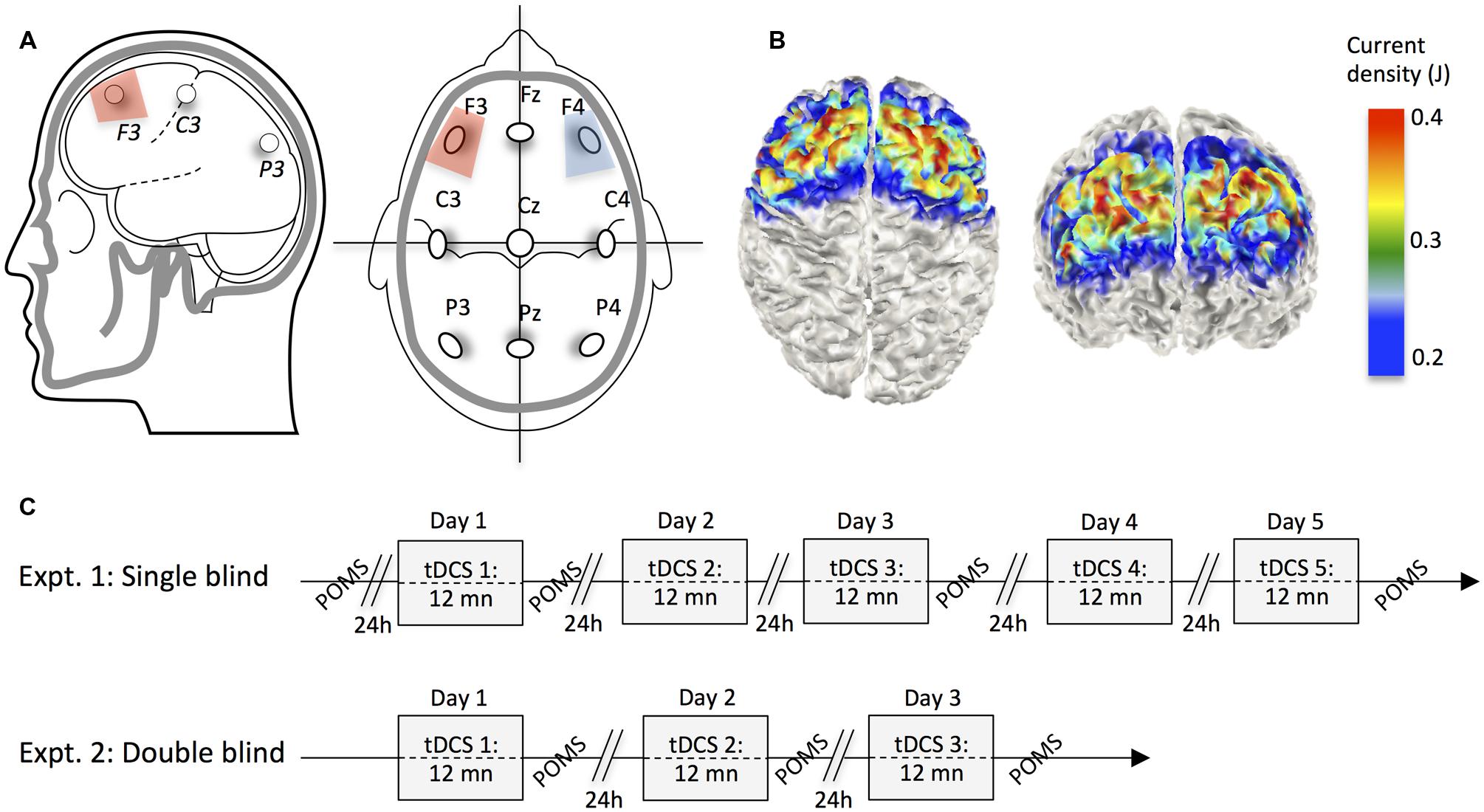
FIGURE 1. (A) Positioning of the stimulating scalp electrodes according to the 10–20 system nomenclature, and in reference to the main cortical fissures. (B) 3D numerical computation of electric fields on the surface of a cortical model for 5 × 5 cm electrodes placed on F3 and F4 head locations (Jung et al., 2013). (C) Timelines of experiments.
Mood Assessment
The Profile of Mood States (Pollock et al., 1979) questionnaire provides a rapid method of assessing transient, fluctuating active mood states. It is an instrument that is particularly well suited to the present research because of its sensitivity to change in affective states. We used the abridged scale – a 24-item questionnaire that measures mood along six dimensions: tension–anxiety, depression–dejection, anger–hostility, vigor-activity, fatigue–inertia, and confusion–bewilderment (Curran et al., 2004). Participants rated how they were currently feeling with respect to 24 words (e.g., Worn-out, Annoyed, Confused, Active, Panicky, and Unhappy) on a scale of 1 (“Not at all”) to 5 (“Extremely”). Scores at each of the factor scores, except for the vigor-activity score, was added together; and then, the vigor-activity score was then subtracted from this total to produce a general composite mood score. In Experiment 1, although participants received tDCS daily over 5 days, we limited the number of post-stimulation mood assessments by only administering the POMS every other day. A baseline measure was taken, on average, 34 min prior to the first stimulation (range 21–44 min). In Experiment 2, where participants were stimulated daily over 3 days, we administered the POMS immediately after every stimulation (Figure 1).
Results
In two experiments, we present converging evidence that series of daily bilateral prefrontal tDCS sessions positively impacted the self-assessment of mood states. In Experiment 1, we first established that, when five 12 mn daily tDCS sessions were administered, scores on the Profile of Mood States scale were improved in the active [F(2,22) = 20.18, p < 1.1e-05, = 0.65; Figure 1A], but not in the sham condition [F(2,22) = 1.03, p < 0.37; Figure 1B]. In the active condition, significant improvements were found between evaluations carried out each other day (all ps < 0.01), whereas no change was noted between sham sessions (all p = NS). This striking dichotomy was independently replicated in Experiment. 2, where tDCS sessions were administered on three consecutive days [active: F(2,54) = 17.31, p < 1.56e-06, = 0.39; Figure 2C; sham: F(2,26) = 1.59, p < 0.22, Figure 2D]. In substantive terms, the reduction in negative mood states in the two active tDCS conditions accounted for 64.7 and 39.1% of the total variations in scores in Experiment 1 and 2, respectively.
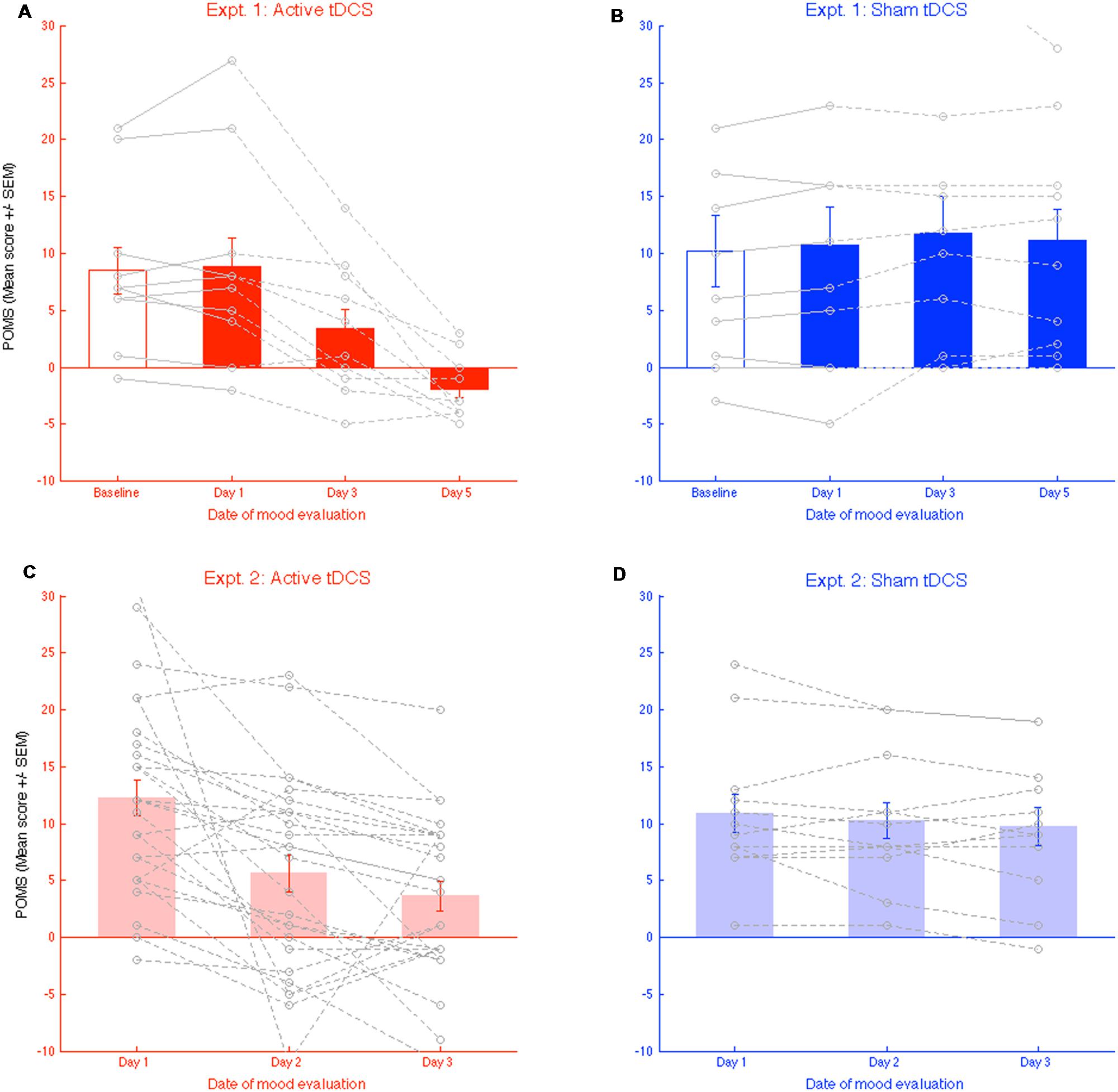
FIGURE 2. (A,B) Evolution of mood states self-evaluation (total score) throughout the 3 days of brain stimulation in the active, and the “sham” conditions. Grey line present individual performances in each condition. (C,D) Similar plots for replication experiment 2. Error bars represent the standard error of the mean (SEM).
The absence of significant mood changes in the sham condition, where participants received series of 36 s 1.5 mA daily stimulations, insured that the observed negative mood reduction was not due to a learning or habituation effect, with participants (consciously or unconsciously) gradually providing less negative ratings during the mood evaluation.
The general tendency toward mood improvement during active tDCS evidenced in the reduction in general composite mood score is logically resulting from improvements in each of the subscales. Although the design of the present research is not adapted to such subsampling of the data, we decided to still present how scores at each of the six subscales in the POMS were modulated by tDCS, without presenting any result of statistical testing (Figure 3). Although the argument is only descriptive, and variability is high, we note that, for all subscales except “vigor,” there is an amelioration tendency (a decrease in scores) in the active tDCS but not in the Sham condition. Interestingly, in Experiment 1, we failed to find significant changes in the mood evaluations made before (labeled “Baseline” in Figure 2) and after the first stimulation [Day 1 active: t(11) = 0.47, p < 0.64, sham: t(11) = 1.28, p < 0.23]. Our current research program explores these aspects, in an adapted research protocol with sufficient statistical power.
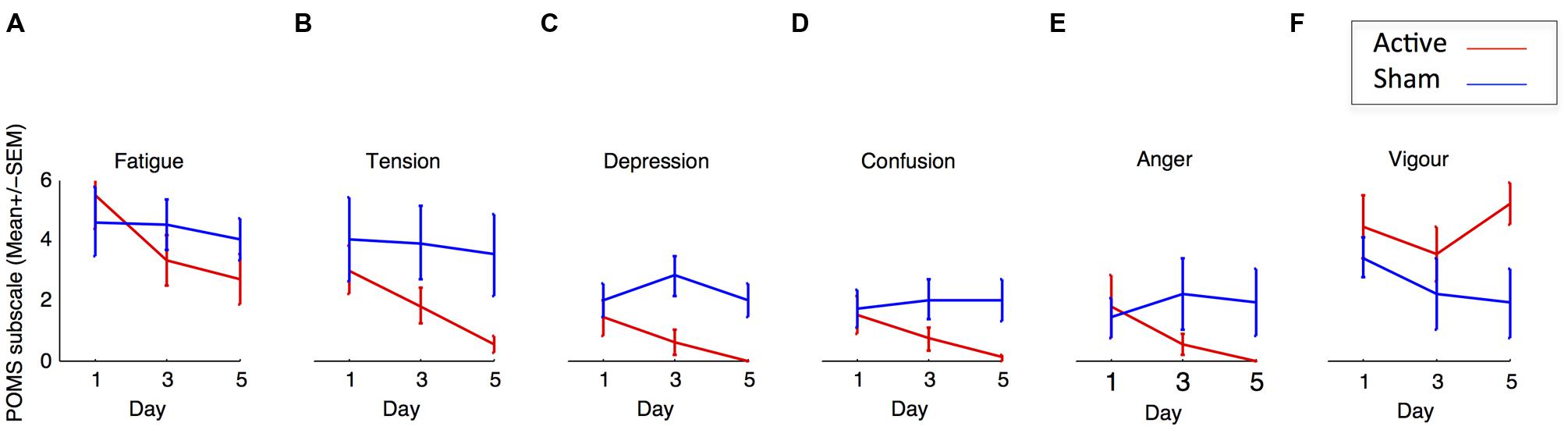
FIGURE 3. (A–F) Evolution of self-evaluation for each dimensions of the POMS throughout the 3 days of brain stimulation in the active and sham conditions in experiment 1. Error bars represent the SEM.
Discussion
In two sham-controlled experiments, we found that repeated daily prefrontal tDCS sessions over 5 several days could effectively modulate how non-depressed individuals self-assess their mood states. Results show that participants experienced less psychological distress from daily stressors, a well established cause in the establishment of a negative emotional state (Bolger et al., 1989). We replicated this finding in an independent, randomized, double-blind experiment applying similar protocol and stimulation on 3 consecutive days.
To our knowledge, the present research is the first to show that the amount negative mood states, in unmedicated non-depressed individuals, can be reduced with repeated prefrontal tDCS. This is consistent with prior body of clinical research demonstrating that repeated tDCS significantly reduces symptoms of major depressive episodes (see Kalu et al., 2012 and Meron et al., 2015 for recent systematic reviews). It is also true that a few conflicting studies failed to find a reduction in psychological distress following prefrontal tDCS. However, the body of research in question either examined individuals with treatment-resistant depression, or else participant samples that were concurrently taking various medication treatments known to interact with tDCS (Loo et al., 2010; Blumberger et al., 2012; Bennabi et al., 2015). For example, the administration of GABA-agonist benzodiazepines (Lorazepam) delays, enhances, and prolonges the elevation in cortical excitability resulting from anodal tDCS (Nitsche et al., 2004), while serotonin selective reuptake inhibitors such as citalopram concurrently increases anodal effects, and transforms cathodal inhibition into facilitation (Nitsche et al., 2009; Brunoni et al., 2013; Bennabi et al., 2015).
Only a few other studies have examined the possibility of modulating mood using tDCS in healthy individuals, these however, failed to show significant effect (Koenigs et al., 2009; Plazier et al., 2012; Morgan et al., 2014). While it is difficult to discuss the absence of significant effect, we believe these could be accounted for by radically different research designs, stimulation program, electrode montages, or in the way current mood was evaluated. For example, in both experiments reported here, participants underwent either 5 or 3 consecutive days of active (or sham) bifrontal tDCS, and our conclusions are therefore founded upon comparisons between an active group and a sham group, and self reported modulation of mood occurring across days. In contrast, Plazier et al.’s (2012) goals were rather different and the research was looking for alterations in mood, following a single session of tDCS, utilizing six forms of bifrontal and bioccipital stimulation, upon the same participant. Although such an attempt is both interesting and commendable, it is difficult to conceive that biochemical alterations within the cortex or detectable effects on mood resulting from a single 20 min tDCS session would be of similar origins to mood modulation observed across days of repeated stimulation. Of importance, we also think that Plazier et al.’s (2012) way of administering mood questionnaires directly before and after the stimulation, is far from optimal: The short time period between repeated assessments, and a participants’ initial responses will likely have influenced, to some degree, latter responses to the questionnaires re-administered directly following stimulation. This observation regarding the limits of repeated questionnaire administration also applies to Koenigs et al. (2009) and Morgan et al. (2014) for the Positive Affect Negative Affect Schedule (PANAS), and the POMS, respectively. Of importance, Koenigs et al. (2009) rather placed the anode on the frontal poles bilaterally (Fp1 and Fp2), and used an extracephalic reference electrode, but detected no mood improvement after any of three usual tDCS conditions.
Discussion of certain methodological questions is needed to further inform future investigations. For instance, our data may have implications for the interpretation of numerous findings in which prefrontal tDCS induces cognitive improvements (e.g., Kadosh et al., 2010; Jacobson et al., 2011). Cognitive processing is affected by mood, with positive mood being associated with improved cognitive performance (Nadler et al., 2010), and since we show that tDCS reduces self reported psychological distress, it is possible that tDCS-induced cognitive improvement are actually mediated by a mood improvement (or vice-versa). Current neuromodulatory work in our team address this issue, and aims at disentangling the complex interaction between mood and cognitive performance. Another pertinent issue relates to the duration of the tDCS-induced mood modulation. In clinical studies, researchers have reported mood improvement effects to be maintained for at least one month after the last stimulation (Kalu et al., 2012). However, these studies involve a greater number of stimulation sessions (N = 10), over a longer period of time (2 weeks), possibly suggesting that the optimal program of stimulation needed to warrant a potentiated reduction of psychological distress in a non-clinical population still has to be determined.
Both past studies in depression, and the present work suggest that tDCS is effective in reducing depressive symptoms and psychological distress, respectively. An important question to consider concerns the identification of the neurophysiological mechanisms that are able to induce these changes. One possible explanation follows from two programs of research. One that examined the relationship between GABA levels and depression, and evidenced that GABA-agonist drugs and agents all tend to ameliorate the depressive symptomatology in human, and in animals (Kalueff and Nutt, 2007). Another, more recent body of research, showed that tDCS could lower cortical GABA and glutamate level locally (Stagg et al., 2009). Although the latter effect was obtained in regions of the frontal cortex that are not directly causally related to mood regulation, unlike the DLPFC, we believe that it provides a general framework for the generation of testable hypotheses. The details of the interaction between GABAergic neuromodulation within the DLPFC and mood regulation are likely to be complex, as the DLPFC forms part of a network involving loops through striatum and thalamus as well as numerous connections to other cortical and subcortical areas relevant for regulating mood. Similarly, the apparent contradiction between the effect of a technique which lowers levels of GABA and a general GABA deficit theory in depression has to be understood in this context, and treated with great care. It is indeed possible that the tDCS-induced local reduction in GABA concentration results in potentiated GABAergic neurotransmission along these extended networks (for similar reasoning, see discussion in Boy et al., 2011).
Author Contributions
SR, AA, FB collected data; SR, FB analyzed data; FB, SR, ND, SN, RMC, GJB wrote or commented on different versions of the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
FB filed the patent application no. 1503004.2 (Intellectual Property Office, Newport, UK) for a novel tDCS device. GJB, SR and FB hold shares in NeuroTherapeutics Limited, a UK registered Company. RMC is an indirect shareholder. The other authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. At the time of data collection, students who gave tDCS stimulation and collected behavioral responses were blind to the hypotheses and previous findings.
Acknowledgments
The authors wish to thank the BIAL Foundation for funding this research and providing salary for one of the researcher (grant 94/12), and value the efforts of the students who collected the data (in particular Cathy Ghalib and Martin Stevenson). Swansea University and the College of Human and Health Science (Swansea university) also provided financial and technical support.
References
Banks, S. J., Eddy, K. T., Angstadt, M., Nathan, P. J., and Phan, K. L. (2007). Amygdala-frontal connectivity during emotion regulation. Soc. Cogn. Affect. Neurosci. 2, 303–312. doi: 10.1093/scan/nsm029
Bennabi, D., Nicolier, M., Monnin, J., Tio, G., Pazart, L., Vandel, P., et al. (2015). Pilot study of feasibility of the effect of treatment with tDCS in patients suffering from treatment-resistant depression treated with escitalopram. Clin. Neurophysiol. 126, 1185–1189. doi: 10.1016/j.clinph.2014.09.026
Blumberger, D. M., Tran, L. C., Fitzgerald, P. B., Hoy, K. E., and Daskalakis, Z. J. (2012). A randomized double-blind sham-controlled study of transcranial direct current stimulation for treatment-resistant major depression. Front. Psychiatry 3:74. doi: 10.3389/fpsyt.2012.00074
Boggio, P. S., Rigonatti, S. P., Ribeiro, R. B., Myczkowski, M. L., Nitsche, M. A., Pascual-Leone, A., et al. (2008). A randomized, double-blind clinical trial on the efficacy of cortical direct current stimulation for the treatment of major depression. Int. J. Neuropsychopharmacol. 11, 249–254. doi: 10.1017/S1461145707007833
Bolger, N., DeLongis, A., Kessler, R. C., and Schilling, E. A. (1989). Effects of daily stress on negative mood. J. Pers. Soc. Psychol. 57, 808–818. doi: 10.1037/0022-3514.57.5.808
Boy, F., Evans, C. J., Edden, R. A. E., Lawrence, A. D., Singh, K. D., Husain, M., et al. (2011). Dorsolateral prefrontal γ-aminobutyric acid in men predicts individual differences in rash impulsivity. Biol. Psychiatry 70, 866–872. doi: 10.1016/j.biopsych.2011.05.030
Brunoni, A. R., Ferrucci, R., Bortolomasi, M., Vergari, M., Tadini, L., Boggio, P. S., et al. (2011b). Transcranial direct current stimulation (tDCS) in unipolar vs. bipolar depressive disorder. Progr. Neuro Psychopharmacol. Biol. Psychiatry 35, 96–101. doi: 10.1016/j.pnpbp.2010.09.010
Brunoni, A. R., Nitsche, M. A., Bolognini, N., Bikson, M., Wagner, T., Merabet, L., et al. (2012). Clinical research with transcranial direct current stimulation (tDCS): challenges and future directions. Brain Stimul. 5, 175–195. doi: 10.1016/j.brs.2011.03.002
Brunoni, A. R., Valiengo, L., Baccaro, A., Zanão, T. A., de Oliveira, J. F., Goulart, A., et al. (2013). The sertraline vs electrical current therapy for treating depression clinical study. JAMA Psychiatry 70:383. doi: 10.1001/2013.jamapsychiatry.32
Brunoni, A. R., Valiengo, L., Baccaro, A., Zanao, T. A., de Oliveira, J. F., Vieira, G. P., et al. (2011a). Sertraline vs. electrical current therapy for treating depression clinical trial - select tdcs: design, rationale and objectives. Contemp. Clin. Trials 32, 90–98. doi: 10.1016/j.cct.2010.09.007
Charles, S. T., Piazza, J. R., Mogle, J., Sliwinski, M. J., and Almeida, D. M. (2013). The Wear and tear of daily stressors on mental health. Psychol. Sci. 24, 733–741. doi: 10.1177/0956797612462222
Curran, S. L., Andrykowski, M. A., and Studts, J. L. (2004). Short form of the profile of mood states (POMS-SF): psychometric information. Psychol. Assess. 7, 1–4.
Dell’Osso, B., Zanoni, S., Ferrucci, R., Vergari, M., Castellano, F., D’Urso, N., et al. (2012). Transcranial direct current stimulation for the outpatient treatment of poor-responder depressed patients. Eur. Psychiatry 27, 513–517. doi: 10.1016/j.eurpsy.2011.02.008
Fregni, F., Boggio, P. S., Nitsche, M. A., Marcolin, M., Rigonatti, S. P., and Pascual-Leone, A. (2006a). Treatment of major depression with transcranial direct current stimulation. Bipolar. Disord. 8, 203–204. doi: 10.1111/j.1399-5618.2006.00291.x
Fregni, F., Boggio, P. S., Nitsche, M. A., Rigonatti, S. P., and Pascual-Leone, A. (2006b). Cognitive effects of repeated sessions of transcranial direct current stimulation in patients with depression. Depress. Anxiety 23, 482–484. doi: 10.1002/da.20201
Gandiga, P. C., Hummel, F. C., and Cohen, L. G. (2006). Transcranial DC stimulation (tDCS): a tool for double-blind sham-controlled clinical studies in brain stimulation. Clin. Neurophysiol. 117, 845–850. doi: 10.1016/j.clinph.2005.12.003
Jacobson, L., Javitt, D. C., and Lavidor, M. (2011). Activation of inhibition: diminishing impulsive behavior by direct current stimulation over the inferior frontal gyrus. J. Cogn. Neurosci. 23, 3380–3387. doi: 10.1162/jocn_a_00020
Jung, Y.-J., Kim, J.-H., and Im, C.-H. (2013). COMETS: a MATLAB toolbox for simulating local electric fields generated by transcranial direct current stimulation (tDCS). Biomed. Eng. Lett. 3, 39–46. doi: 10.1007/s13534-013-0087-x
Kadosh, R. C., Soskic, S., Iuculano, T., and Kanai, R. (2010). Modulating neuronal activity produces specific and long-lasting changes in numerical competence. Curr. Biol. 20, 2016–2020. doi: 10.1016/j.cub.2010.10.007
Kalu, U. G., Sexton, C. E., Loo, C. K., and Ebmeier, K. P. (2012). Transcranial direct current stimulation in the treatment of major depression: a meta-analysis. Psychol. Med. 42, 1791–1800. doi: 10.1017/S0033291711003059
Kalueff, A. V., and Nutt, D. J. (2007). Role of GABA in anxiety and depression. Depress. Anxiety 24, 495–517. doi: 10.1002/da.20262
Kim, S., Stephenson, M. C., Morris, P. G., and Jackson, S. R. (2014). tDCS-induced alterations in GABA concentration within primary motor cortex predict motor learning and motor memory: A 7T magnetic resonance spectroscopy study. Neuroimage 99, 237–243. doi: 10.1016/j.neuroimage.2014.05.070
Koenigs, M., Ukueberuwa, D., Campion, P., Grafman, J., and Wassermann, E. (2009). Bilateral frontal transcranial direct current stimulation: failure to replicate classic findings in healthy subjects. Clin. Neurophysiol. 120, 80–84. doi: 10.1016/j.clinph.2008.10.010
Lévesque, J., Eugène, F., Joanette, Y., Paquette, V., Mensour, B., Beaudoin, G., et al. (2003). Neural circuitry underlying voluntary suppression of sadness. Biol. Psychiatry 53, 502–510. doi: 10.1016/S0006-3223(02)01817-6
Loo, C. K., Alonzo, A., Martin, D., Mitchell, P. B., Galvez, V., and Sachdev, P. (2012). Transcranial direct current stimulation for depression: 3-week, randomised, sham-controlled trial. Br. J. Psychiatry 200, 52–59. doi: 10.1192/bjp.bp.111.097634
Loo, C. K., Sachdev, P., Martin, D., Pigot, M., Alonzo, A., Malhi, G. S., et al. (2010). A double-blind, sham-controlled trial of transcranial direct current stimulation for the treatment of depression. Int. J. Neuropsychopharmacol. 13, 61–69. doi: 10.1017/S1461145709990411
Meron, D., Hedger, N., Garner, M., and Baldwin, D. S. (2015). Transcranial direct current stimulation (tDCS) in the treatment of depression: systematic review and meta-analysis of efficacy and tolerability. Neurosci. Biobehav. Rev. 57, 46–62. doi: 10.1016/j.neubiorev.2015.07.012
Morgan, H. M., Davis, N. J., and Bracewell, R. M. (2014). Does transcranial direct current stimulation to prefrontal cortex affect mood and emotional memory retrieval in healthy individuals. PLoS ONE 9:e92162. doi: 10.1371/journal.pone.0092162
Nadler, R. T., Rabi, R., and Minda, J. P. (2010). Better mood and better performance: learning rule-described categories is enhanced by positive mood. Psychol. Sci. 21, 1770–1776. doi: 10.1177/0956797610387441
Nitsche, M. A., Kuo, M.-F., Karrasch, R., Wächter, B., Liebetanz, D., and Paulus, W. (2009). Serotonin affects transcranial direct current–induced neuroplasticity in humans. Biol. Psychiatry 66, 503–508. doi: 10.1016/j.biopsych.2009.03.022
Nitsche, M. A., Liebetanz, D., Schlitterlau, A., Henschke, U., Fricke, K., Frommann, K., et al. (2004). GABAergic modulation of DC stimulation-induced motor cortex excitability shifts in humans. Eur. J. Neurosci. 19, 2720–2726. doi: 10.1111/j.0953-816X.2004.03398.x
Plazier, M., Joos, K., Vanneste, S., Ost, J., and De Ridder, D. (2012). Bifrontal and bioccipital transcranial direct current stimulation (tDCS) does not induce mood changes in healthy volunteers: a placebo controlled study. Brain Stimul. 5, 454–461. doi: 10.1016/j.brs.2011.07.005
Pollock, V., Cho, D. W., Reker, D., and Volavka, J. (1979). Profile of mood states: the factors and their physiological correlates. J. Nerv. Ment. Dis. 167, 612–614. doi: 10.1097/00005053-197910000-00004
Poreisz, C., Boros, K., Antal, A., and Paulus, W. (2007). Safety aspects of transcranial direct current stimulation concerning healthy subjects and patients. Brain Res. Bull. 72, 208–214. doi: 10.1016/j.brainresbull.2007.01.004
Romero Lauro, L. J., Rosanova, M., Mattavelli, G., Convento, S., Pisoni, A., Opitz, A., et al. (2014). TDCS increases cortical excitability: direct evidence from TMS-EEG. Cortex 58, 99–111. doi: 10.1016/j.cortex.2014.05.003
Stagg, C. J., Bachtiar, V., and Johansen-Berg, H. (2011). The role of GABA in human motor learning. Curr. Biol. 21, 480–484. doi: 10.1016/j.cub.2011.01.069
Stagg, C. J., Best, J. G., Stephenson, M. C., O’Shea, J., Wylezinska, M., Kincses, Z. T., et al. (2009). Polarity-sensitive modulation of cortical neurotransmitters by transcranial stimulation. J. Neurosci. 29, 5202–5206. doi: 10.1523/JNEUROSCI.4432-08.2009
Keywords: mood, tDCS, emotion regulation, GABA antagonists, GABA agonists
Citation: Austin A, Jiga-Boy GM, Rea S, Newstead SA, Roderick S, Davis NJ, Clement RM and Boy F (2016) Prefrontal Electrical Stimulation in Non-depressed Reduces Levels of Reported Negative Affects from Daily Stressors. Front. Psychol. 7:315. doi: 10.3389/fpsyg.2016.00315
Received: 08 October 2015; Accepted: 18 February 2016;
Published: 04 March 2016.
Edited by:
Michael Banissy, Goldsmiths University of London, UKReviewed by:
Neil Gerald Muggleton, National Central University, TaiwanIon Juvina, Wright State University, USA
Copyright © 2016 Austin, Jiga-Boy, Rea, Newstead, Roderick, Davis, Clement and Boy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Frederic Boy, Zi5hLmJveUBzd2Fuc2VhLmFjLnVr