 Sérgio A. Carvalho1
Sérgio A. Carvalho1 Inês A. Trindade1*
Inês A. Trindade1* Joana Duarte2
Joana Duarte2 Paulo Menezes3,4
Paulo Menezes3,4 Bruno Patrão3,4
Bruno Patrão3,4 Maria Rita Nogueira4,5Raquel Guiomar1Teresa Lapa6,7José Pinto-Gouveia1Paula Castilho1
Maria Rita Nogueira4,5Raquel Guiomar1Teresa Lapa6,7José Pinto-Gouveia1Paula Castilho1- 1University of Coimbra, Center for Research in Neuropsychology and Cognitive Behavioral Intervention, Coimbra, Portugal
- 2Lund University, Department of Psychology, Lund, Sweden
- 3University of Coimbra, Department of Electrical and Computer Engineering, Coimbra, Portugal
- 4Institute of Systems and Robotics, Coimbra, Portugal
- 5University of Coimbra, College of Arts, Coimbra, Portugal
- 6Coimbra Hospital and University Center, Pain Unit, Coimbra, Portugal
- 7Faculty of Health Sciences, University of Beira Interior, Covilhã, Portugal
Background: Chronic pain (CP) has serious medical and social consequences and leads to economic burden that threatens the sustainability of healthcare services. Thus, optimized management of pain tools to support CP patients in adjusting to their condition and improving their quality of life is timely. Although acceptance and commitment therapy (ACT) is considered an evidence-based psychological approach for CP, evidence for the efficacy of online-delivered ACT for CP is still scarce. At the same time, studies suggest that self-compassion mediates the change in disability and psychopathological symptoms in ACT interventions for CP, although self-compassion is not a specific target in ACT. Thus, an explicit focus on self-compassion might increase the efficacy of ACT interventions for CP, although this hypothesis has not been tested. This study aims to develop an eHealth ACT and compassion-based self-management intervention for CP, the iACTwithPain, and to compare its efficacy in improving health outcomes to a similar ACT-only intervention and a medical TAU group.
Methods: The eHealth platform that will host the interventions will be developed using a flat design identity and will be interactive. The iACTwithPain intervention will comprise eight weekly self-management sessions and will be developed taking into consideration the psychological flexibility model applied to CP, with the addition of explicit compassion-based components. To analyze whether the iACTwithPain intervention will present superiority in improving CP’s impact and related health markers over the two other conditions, this study will follow an RCT design with three arms. CP patients will be recruited through direct contact with patient associations and healthcare services and a national press release in Portugal. Outcome measurement will be conducted at baseline, post-intervention and at 3- and 6-month follow-ups. The interventions’ acceptability will also be assessed.
Discussion: The iACTwithPain intervention is expected to improve CP patients’ psychosocial functioning, quality of life, and empowerment, by promoting adaptive disease management and regulation of pain-related internal experiences. Results will contribute to a better understanding on the pertinence of adding compassion elements to ACT for CP and to reach an optimized intervention for CP.
Clinical Trial Registration: This trial has been registered at ClinicalTrials.Gov (NCT04200183; 16 December 2019; https://clinicaltrials.gov/ct2/show/NCT04200183). The current manuscript comprises the first version of this clinical trial’s protocol.
Background
Chronic pain (CP), defined as sporadic or constant pain or discomfort lasting for more than 3 months (Elliott et al., 1999), is a major public health issue that affects 19% of adult Europeans and impairs the quality of their social and working lives (Breivik et al., 2006). In Portugal, a recent study estimated that CP has a median duration of 10 years, with 85% of CP patients with recurrent or continuous pain and 68% of CP patients with moderate to severe pain intensity (Azevedo et al., 2012). In addition, CP yields a great economic burden to the healthcare system and society at large. It is estimated that CP presents serious costs to economics and health services (Phillips, 2009). Moreover, evidence suggests that up to 50% of non-malignant pain patients are addicted to pain medication (Højsted and Sjøgren, 2007), which leads to further health problems (Højsted and Sjøgren, 2007) and imposes a cost burden on health systems (Shei et al., 2015).
Chronic pain is a multifaceted experience that results from an interplay of physiological states and psychological processes (i.e., thoughts, emotions), and current approaches to CP recognize the value of addressing the cognitive and affective aspects of pain (Eccleston et al., 2013). Studies show that CP is associated with psychiatric disorders (Dominick et al., 2012), with a significant impact on the quality of life and functioning of CP patients (Breivik et al., 2006). However, the current provision of care to CP sufferers vastly disregards psychological interventions. Also, traditional psychological interventions for CP focus primarily on controlling pain and overall symptoms’ reduction. Nonetheless, research has shown that an exclusive and overly focus on pain control might be frustrating and damaging and actually result in more disability (McCracken, 1998), higher pain intensity, pain-related anxiety, and depression (McCracken and Vowles, 2006).
In contrast, for the last two decades the evidence has suggested that acceptance of pain is a major key process in successfully adapting to CP (Vowles et al., 2007; Vowles and McCracken, 2008) and is associated with less pain, disability, depression, and pain-related anxiety (McCracken and Eccleston, 2003). This led to a growing interest in acceptance-based approaches, focusing not so much in reducing and controlling pain, but rather in increasing the acceptance of pain (Costa and Gouveia, 2013; Pinto-Gouveia et al., 2015).
Acceptance and commitment therapy (ACT), which focuses on function improvement rather than symptom reduction, is an empirically supported intervention for CP (APA Presidential Task Force on Evidence-Based Practice, 2006). An ACT intervention for CP aims to promote emotional acceptance and engagement with values-consistent actions, despite CP symptoms (Hayes et al., 1999; Vowles et al., 2007; Vowles and McCracken, 2008). Recently, some studies suggested that ACT interventions also promote self-compassion (Yadavaia et al., 2014; Luoma and Platt, 2015), a non-judgmental and mindful approach to one’s pain and suffering (Neff, 2003), which presents known links with pain regulation systems, such as heart-rate variability (Rockliff et al., 2008), and oxytocin-endorphin systems (Rockliff et al., 2011). Self-compassion has been the focus of growing attention in CP due to its protective role against depressive symptomatology in this condition (Carvalho et al., 2019), its negative association with pain disability (Wren et al., 2016), and the promising results showing the positive effects of compassion-based interventions in CP (Chapin et al., 2014; Ziemer et al., 2015; Parry and Malpus, 2017; Gooding et al., 2020).
Interestingly, self-compassion appears be associated with important ACT processes (Costa and Pinto-Gouveia, 2013; Carvalho et al., 2018a; Edwards et al., 2019), and although ACT interventions do not specifically incorporate explicit self-compassionate exercises, self-compassion was found to mediate the change in disability and psychopathological symptoms in an ACT intervention for CP (Vowles et al., 2014). This raises the possibility that self-compassion may be an under-recognized mechanism of change in ACT and that an explicit focus on self-compassion in ACT might increase the efficacy of ACT interventions. Further, although ACT interventions with elements from compassion-based approaches seem to significantly improve mental health in a number of clinical populations (Skinta et al., 2015; Palmeira et al., 2017; Pinto-Gouveia et al., 2017; Trindade et al., 2020), the individual role of self-compassion in ACT for CP and the benefit of adding explicit compassionate exercises to such interventions are still unclear.
There is a growing interest in using online interventions to improve health (i.e., eHealth). In fact, eHealth is expected to contribute to the sustainability of healthcare systems, with advantages such as reducing therapist time and waiting lists, increased cost-effectiveness, ability of patients to work at their own pace, accessibility to large clinical samples, and accessibility to rural and remote clinical cohorts (Bergmo, 2015). Also, it seems to provide an effective way of dealing with the inadequate training of health professionals in the psychological aspects of CP and of bypassing the shortage of psychological therapists in the national healthcare system. Some studies tested the efficacy of online ACT interventions for CP (Buhrman et al., 2013; Trompetter et al., 2014; Fledderus et al., 2015; Vilardaga et al., 2020), which resulted in reduction of pain intensity, pain-related distress, anxiety and depressive symptoms, and an increase of activity engagement and pain-willingness (Buhrman et al., 2013). However, there were several methodological limitations to these studies (small sample size and non-randomization). Further research is thus needed to better comprehend the efficacy of eHealth ACT interventions for CP and, in addition, the contribution of self-compassion to this approach.
Aims of This RCT
This study has three main aims: (1) to develop an ACT and compassion-based eHealth tool for CP management (iACTwithPain); (2) to analyze whether the iACTwithPain intervention will present superiority in improving CP’s impact and related health and quality-of-life markers over an ACT-only intervention and a wait-list condition; and (3) to examine whether the interventions’ efficacy will be explained by changes in therapeutic processes (e.g., self-compassion and psychological flexibility).
We hypothesize that the platform will present high acceptability and that both the ACT-only and iACTwithPain interventions will have efficacy in improving CP’s impact, mental health, and quality of life. Further, we also hypothesize that the intervention with explicit self-compassion components, the iACTwithPain, will present superiority in decreasing self-criticism and increasing self-compassion, quality of social relationships, and social safeness through the activation of the affiliative system and subsequent stimulation of oxytocin activity. The efficacy of the ACT-only intervention is expected to be explained by increases in psychological flexibility and mindfulness abilities, and decreases in cognitive fusion and rumination. The iACTwithPain intervention’s efficacy is expected to be explained by changes in the same processes and, in addition, by changes in self-compassion and self-criticism (Figure 1).
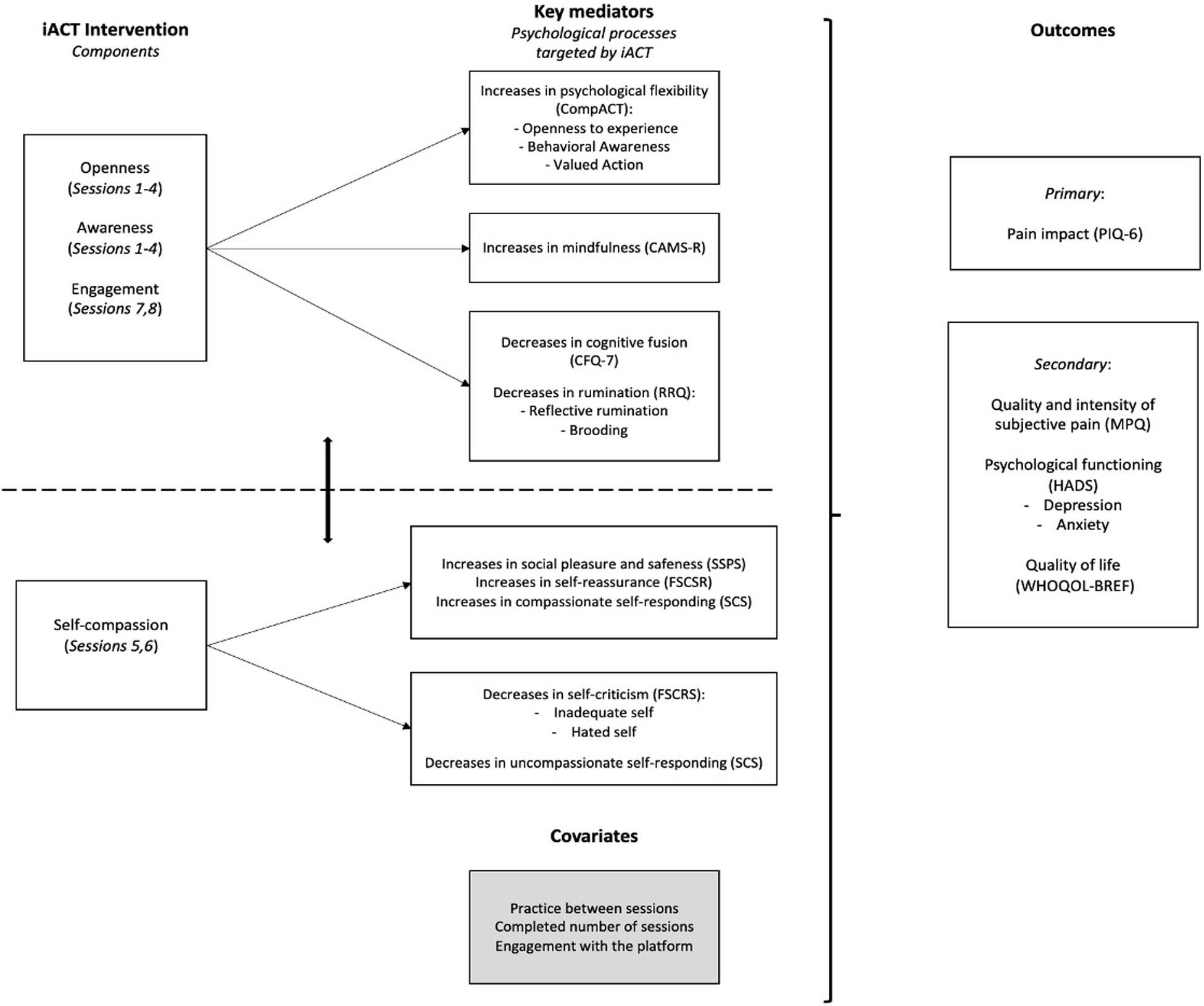
Figure 1. Examples of session screens. This study’s team holds the copyright of this image.
Methods/Design
This study is funded by the Portuguese Foundation for Science and Technology and is registered at ClinicalTrials.gov (Identifier: NCT04200183, date assigned 16/12/2019). Ethical approval has been obtained from the Ethics Committee of the Faculty of Psychology and Education Sciences of the University of Coimbra. Eventual protocol amendments will be communicated to this Committee.
Participant Recruitment
Recruitment will be facilitated by advertisement in Portuguese press and social media. Individuals interested in the study will sign up in the platform and then be asked to sign an informed consent fill out questionnaires designed to assess inclusion and exclusion criteria.
Participant Selection
Patients are eligible to participate if they:
• are aged between 18 and 50 years;
• have had a CP diagnosis for the last 3 months;
• have access to internet and willingness to do it regularly (at least once a week);
• are willing to be randomized;
• can read and write Portuguese; and
• can give informed consent.
Patients are ineligible to participate if they:
• are undergoing any other form of psychological intervention for CP;
• present a severe psychiatric problem (e.g., severe depression, psychotic illness, bipolar disorder, and borderline personality disorder)—assessed using several questions (self-reported) based on the diagnostic criteria according to DSM-V; and
• present pain due to malignancy, trauma, or surgery.
Participants who do not meet the eligibility criteria will be given feedback and advised to seek medical/psychological/group support.
Sample Size
Results from G∗Power calculations for repeated measures analysis, assuming a p-value = 0.05, an effect size of f = 0.25 (Scott et al., 2018), with a statistical power of 0.95, three groups, and four measurements, recommend a sample size of 171. Giving the 30% drop-out rate in previous ACT-based intervention studies (Melville et al., 2010), the total sample size to be collected will be 246 (each group will be composed of 82 participants).
Randomization of Participants
Participants will be randomized (computer-generated random allocation) to one of three conditions: experimental condition 1 (ACT-only intervention); experimental condition 2 (iACTwithPain + self-compassion); and control condition (medical TAU). All participants will continue their treatment as usual for CP. Each participant will be randomly assigned with a number between 1 and 246; after number assignment, participants with numbers 1–82 will be allocated to experimental condition 1, 83–164 to experimental condition 2, and 84–246 to the control condition. Only participants from the experimental conditions will be blind to their allocation; we do not expect any need for unblinding participants in these conditions.
Participants in the two experimental conditions will then access to the respective version of the platform, where they will be asked to complete pre-intervention questionnaires (T0). The control group will only be provided access to the questionnaires.
Intervention Development
The iACTwithPain intervention will be developed by the psychologist members of this research team taking into consideration the psychological flexibility model applied to CP (e.g., Vowles et al., 2009; Dahl and Lundgren, 2016), with the addition of compassion-based elements (Gilbert, 2009; Neff and Germer, 2018) specifically adapted to CP. The research team’s experience on CP’s psychosocial impact and related psychological processes (Carvalho et al., 2018a,b, 2019, 2020), and in developing and delivering ACT and compassion-based interventions to chronically ill populations such as CP, cancer (Trindade et al., 2020), inflammatory bowel disease (ClinicalTrial.gov NCT03840707, undergoing), as well as psychiatric populations (Pinto-Gouveia et al., 2017; ClinicalTrial.gov NCT04101032, undergoing) will be integrated to assure the development of an adequate and rigorous intervention.
The iACTwithPain Intervention
The iACTwithPain intervention (Table 1) will comprise core themes: (a) theme 1: pain acceptance (psychological flexibility in the presence of thoughts, feelings and behaviors associated with pain through mindfulness and acceptance practices); (b) theme 2: values-based action (promotion of behaviors consistent with personal goals, despite pain symptoms); and (c) theme 3: self-compassion (fostering a compassionate stance toward one’s struggles and suffering), which will only be incorporated in the intervention for experimental condition 2. These themes will be delivered through eight sessions that will be available to participants throughout an 8-week period. Each session will be composed of video-animations, real-image videos, complementary texts, and audio files with the experiential exercises/practices targeting the specific topic of the session. An introductory brief session (session 0) will welcome the participant to the intervention and guide him/her through the use of the platform. From session 1, all sessions will begin with a brief soft-landing exercise. Participants will be asked to complete between-session mindfulness and/or compassion-based meditative exercises as often as they can. These between-session assignments will aim to promote skills introduced in the previous session.
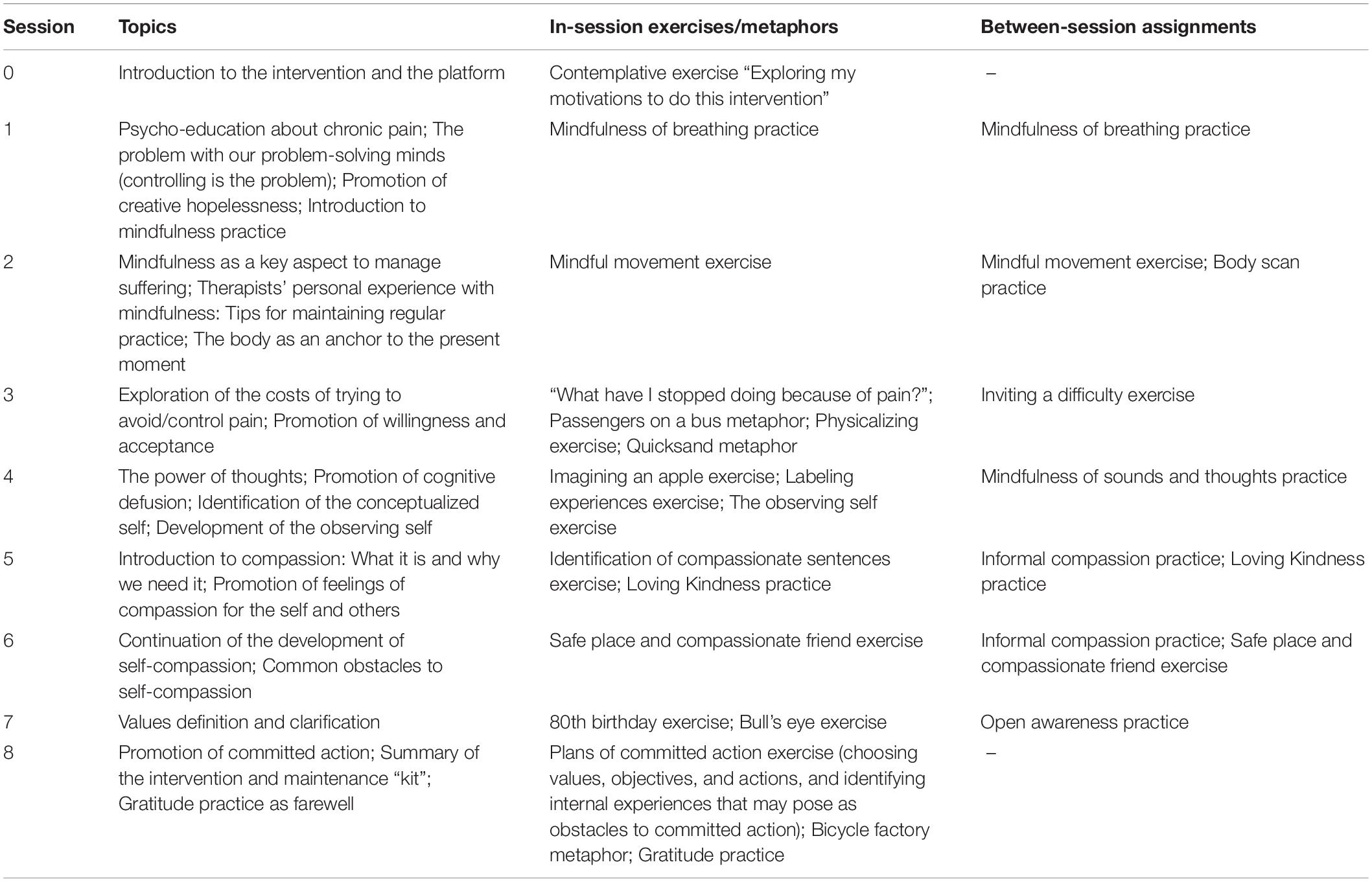
Table 1. Overview of the iACTwithPain intervention.
The ACT-Only Intervention
The ACT-only intervention will follow the same structure and contents as iACTwithPain’s, with the exception of sessions 5 and 6, which, instead of presenting compassion elements, will reinforce and further address willingness, acceptance, defusion, and observing self topics, without adding new information or practices. This intervention will be delivered via the same platform as the iACTwithPain intervention.
Treatment Integrity
Several aspects of treatment integrity guidelines for ACT (Plumb and Vilardaga, 2010) will be followed during the development of the intervention: (a) integrity was thought as a crucial part of the study, in which therapists′ competence was ensured by previous training in ACT and compassion-based approaches as well as supervision throughout the intervention; (b) the intervention was developed having in mind issues of integrity, by including ACT-consistent informative texts, exercises, and therapist lines and tips in videos; and (c) the intervention was developed following clearly operationalized processes of change from the ACT and compassion-based models.
Platform Development
The platform will aim at offering access to the interventions’ contents via either personal computers or mobile devices. The platform will have an app-like functioning when accessed from a mobile device. It is based on a well-established CMS that will integrate new modules to support the user registration, enquities, and content delivery on pre-established sequence. The platform will include a set of sessions, each one composed of explanations, video animations, experimental exercises, supplementary texts, support material, daily tasks, audio meditation, and other practices.
Upon the agreement of the patients, usage data will be collected that will have two different purposes: (1) identifying usability issues and (2) understand how pain and suffering should be considered in the interaction design processes. With the exception of data that are required for the RCT, such as usage frequency, most of the usage-related data will be anonymized only keeping the relationships strictly necessary to guide the usability studies. The result of this effort will be to try to maximize the adherence and avoid dropouts due to usability issues and therefore contribute to retain participants in the study.
The platform’s interface design will be based on a calmness-related message. Taking into consideration the target users and the fact that possibly they may be experiencing pain during the usage, all the elements will be designed taking that into account. The simple and flat design approach chosen is expected to eliminate or reduce to a minimum the existence of misleading cues that may induce frustration or distraction.
Implementation of the Interventions
Participants will follow the sessions in a given order (from session 1 to 8, one session per week). All data will be linked to a data hub tracking participants’ interaction with the platform (i.e., number of logins, duration of interaction with platform, number of visualization of videos/audios, and feedback on each session). Each week, participants will receive an email prompting them to login to the platform and complete the week’s session (that becomes available 1 week after the previous session was completed by the participant). Participants will also receive automatically generated reminders via email with supporting messages: (a) if they do not login for more than 3 days and (b) if they practice continuously (contingency management by reinforcing frequent engagement and practice). This will be particularly important to remind participants to practice the between-session assignments. Contact with the research team will be made available to participants during the intervention period through a one-to-one chat incorporated in the platform. As neither intervention will present risks to participants, a data monitoring committee is not expected to be involved. Adverse events are also not expected. Participants who skip more than two sessions will not be considered for the RCT (in the iACTwithPain group participants who do not complete both of the compassion sessions will be additionally excluded).
Primary and Secondary Outcomes in the RCT
Before (T0) and after (T1) the interventions, and in the 3-month (T2) and 6-month (T3) follow-ups, participants in the experimental conditions and in the waiting-list control condition will be assessed through several self-report questionnaires. Participants will receive notifications via email to complete the self-report measures. These data will be collected in the iACTwithPain platform using high standard security mechanisms which will ensure confidentiality. Only the research team will have access to the collected data, including the final dataset, which will be managed by the study’s PI (PC) and kept for 5 years after the study ends. Participants will only be identified by a generated code.
Participants will provide sociodemographic and clinical information and complete self-report measures (in their validated Portuguese versions) to assess primary and secondary outcomes see Table 2.
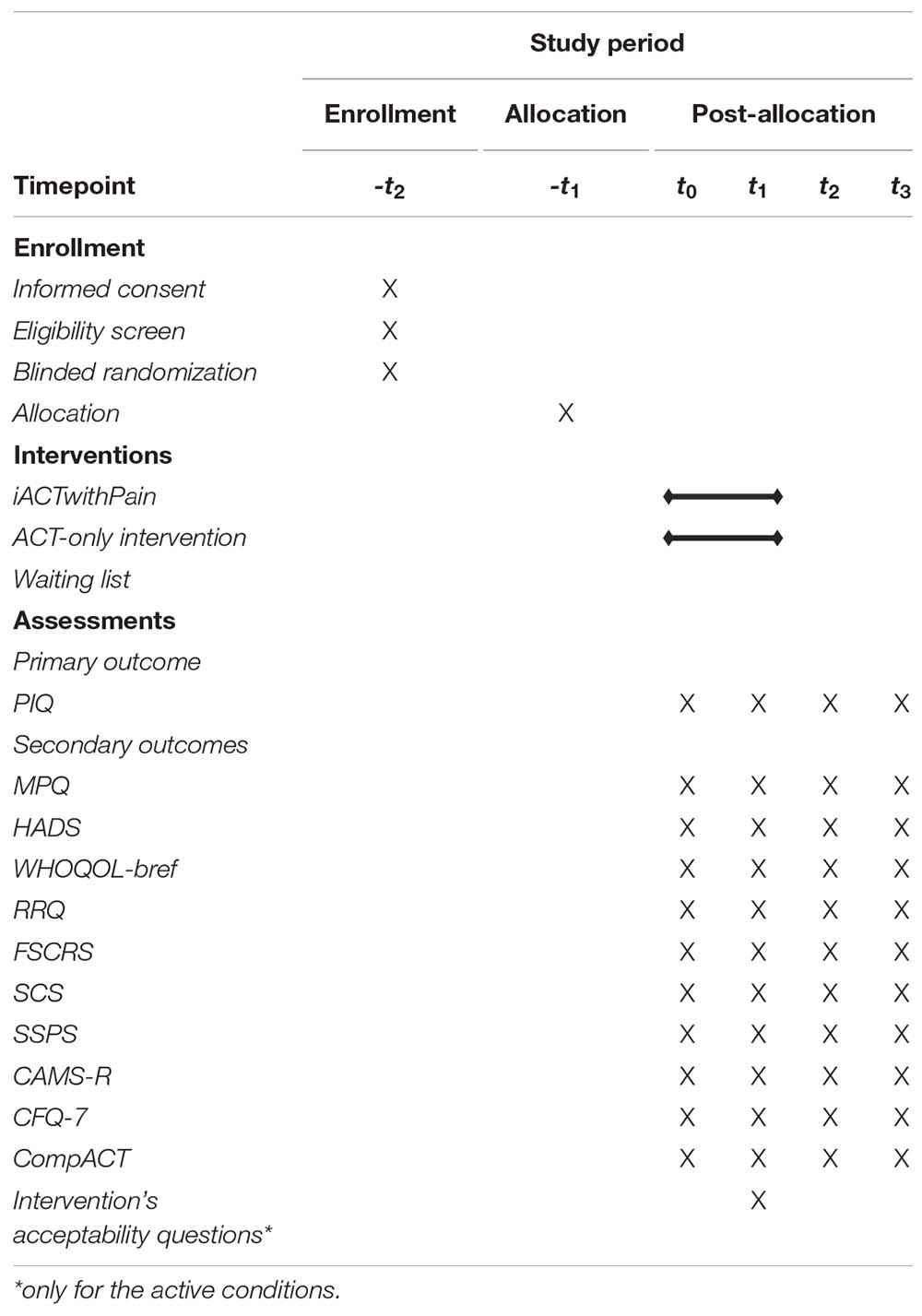
Table 2. Schedule of enrollment, interventions, and assessments.
Primary Outcome
Pain impact
The six-item Pain Impact Questionnaire (PIQ-6; Becker et al., 2007; Cavalheiro et al., 2011) will be used to assess participants’ perceived pain severity (1 item rated on a 6-point scale) and impact on emotional well-being, leisure activities, and work functioning (five items rated on a 5-point scale).
Key Mediators
ACT-Related Variables
Psychological flexibility, as conceptualized by ACT, will be measured by the comprehensive assessment of ACT processes (CompACT; Francis et al., 2016; Trindade et al., under review), an 18-item measure with three subscales: openness to experience, behavior awareness, and valued action, in which items are rated on a 7-point response scale (0—“Strongly disagree” to 6—“Strongly agree”). Mindfulness abilities will be measured using the Cognitive and Affective Mindfulness Scale-Revised (CAMS-R; Feldman et al., 2007; Teixeira et al., 2017) which presents 12 items answered on a 4-point Likert scale from 1 (Not at all) to 4 (Almost always). Cognitive fusion will be assessed by the seven-item Cognitive Fusion Questionnaire (CFQ-7; Gillanders et al., 2014; Pinto-Gouveia et al., 2020), in which the response scale ranges from 1 (“Never true”) to 7 (“Always true”).
Rumination
This outcome will be assessed by the Ruminative Responses Questionnaire (RRQ; Treynor et al., 2003; Dinis et al., 2011), a 10-item measure with two subscales, reflective rumination and brooding, which are rated on a 4-point Likert scale (0—Almost Never; 3—Almost Always).
Self-criticism, self-reassurance, self-compassion, and social safeness
Self-criticism will be measured by the Forms of Self-Criticizing/Attacking and Self-Reassuring Scale (FSCSR; Gilbert et al., 2004; Castilho et al., 2015b), a scale with 22 items measuring self-criticism (inadequate self and hated self) and the ability to self-reassure. Respondents rate items on a 5-point Likert scale (0 = not at all like me; 4 = extremely like me). Further, the Self-Compassion Scale (SCS; Neff, 2003; Castilho et al., 2015a) will provide the measurement of self-compassion. The SCS is composed of 26 items that assess six components: Self-Kindness, Self-Judgment, Common Humanity, Isolation, Mindfulness, and Over-Identification. Each item is rated on a 5-point Likert scale accordingly to how frequently participants act that way toward themselves in difficult times (1—“Almost never” to 5—“Almost always”). To assess social safeness, the Social Safeness and Pleasure Scale (SSPS; Gilbert et al., 2009) will be used. This is a 11-item instrument that measures, on a 5-point Likert scale, current feelings of safeness, belonging, acceptance, and a sense of connectedness.
Secondary Outcomes
Quality and Intensity of Subjective Pain
The McGill Pain Questionnaire (MPQ; Melzack, 1975; Figueiral, 2002), a three-part pain assessment tool, will be used to evaluate several dimensions of the participants’ pain experience—location, intensity, and verbal description.
Psychological Functioning
Anxiety and depression symptoms will be assessed by the Hospital Anxiety and Depression Scales (HADS; Zigmond and Snaith, 1983; Pais-Ribeiro et al., 2007), in which participants rate the 14 items (7 items for each subscale) on a 4-point scale between 0 and 3 (the scale varies). For each subscale, scores between 0 and 7 are considered normal, 8–10 mild, 11–14 moderate, and 15–21 severe.
Quality of life
To assess this outcome, the World Health Organization Quality of Life—Bref (The WHOQOL Group, 1998; Vaz Serra et al., 2006), a 26-item multidimensional measure of subjective quality of life, will be used. This instrument measures four dimensions of quality of life (physical, psychological, social relations, and environment) on a 5-point Likert scale.
Acceptability Assessment
The intervention’s acceptability will be assessed in the experimental conditions by analyzing (a) participants’ adherence (attrition rate) and (b) results from the Client Satisfaction Questionnaire (Attkisson and Zwick, 1982) adapted to the eHealth intervention context.
Statistical Analysis
The efficacy of the iACTwithPain will be assessed by comparing pre-intervention, post-intervention, and 3- and 6-month follow-up questionnaires’ scores through MANOVAs, repeated measures, within-between interaction (with Bonferroni correction). Changes in the primary outcome and in the secondary outcomes between pre-intervention, post-intervention, and follow-ups will be compared between the three conditions (iACT, iACTwithPain, and waiting-list). MANOVAs’ assumptions (multivariate normality, linearity, absence of multicollinearity, and equality of covariance matrices) will be analyzed prior to analysis.
Additionally, changes in painkillers dependence and hospital visits (self-disclosed) will also be compared between the three groups. Cohen’s d will be calculated to measure the between-group effect size on both primary and secondary outcomes. Changes in psychological processes (e.g., self-compassion, mindfulness, and psychological flexibility) will also be tested as potential mechanisms of change of the iACTwithPain intervention, using mediation modeling procedures. Missing data will be imputed with PASW Missing Value Analysis (SPSS Inc., United States) (Blankers et al., 2010).
Discussion
To our current knowledge, iACTwithPain will be the first eHealth intervention that incorporates ACT and explicit self-compassion elements. This intervention is expected to improve CP patients’ psychosocial functioning and quality of life, by promoting adaptive disease management and regulation of pain-related internal experiences. By providing access to specialized treatment with an online delivery format and self-management nature, the intervention is also expected to promote patients’ empowerment and accessibility to treatment. Results will contribute to better understand self-compassion’s individual role in ACT for CP, the pertinence of adding compassion-promoting exercises to those interventions, and to reach an optimized intervention for this population.
One of this study’s strengths is the analysis of the potential mechanisms of change of the tested interventions, which will shed light on which therapeutic processes are responsible for improvements in CP, in both the iACTwithPain intervention and the ACT-only intervention. Another strength is the platform itself, which will be developed aiming at being intuitive and graphically attractive and which will track participants’ interaction, providing objective data on participants’ between-session practice and engagement with the interventions, which will be examined and accounted for in the efficacy test.
One of the most significant challenges will be the prevention of drop-outs. A strategic way of decreasing this risk will be to email participants with supportive and motivating messages every time the platform registers inactivity for more than 3 days. Another limitation will be that participants allocated to the control group (medical TAU) will not be blind to their allocation due to the nature of this condition, which might influence self-reported outcomes.
In conclusion, this study will contribute with a new eHealth self-management intervention for CP, which, if proven effective, will significantly help CP patients manage their pain and improve their mental health and quality of life and improve accessibility to treatment of remote clinical cohorts or with limited mobility. With this RCT, specific knowledge will be obtained about the role of self-compassion in ACT for CP and the potential benefits of adding explicit self-compassion elements to ACT.
Ethics Statement
The studies involving human participants were reviewed and approved by Comité de Ética e Deontologia (CEDI), Faculty of Psychology and Education Sciences, University of Coimbra. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
PC, JP-G, SC, JD, PM, BP, and TL wrote this project’s grant proposal and attracted funding. IT adapted the proposal to this manuscript. All authors read, provided feedback, and approved the final manuscript.
Funding
This study was funded by the project PTDC/PSI-GER/28829/2017 | POCI-01-0145-FEDER-028829 by the Fundo Europeu de Desenvolvimento Regional (FEDER), through Portugal 2020 - Programa Operacional Competitividade e Internacionalização (POCI) and by the State budget, through the Fundação para a Ciência e Tecnologia, I.P. (FCT). The role of this sponsor solely relates to the attribution of funding and monitoring of the project’s evolution, according to the established chronogram. Study design, collection, management, analysis, and interpretation of data, writing of reports and outputs, and decisions to publish are the responsibility of this project’s team.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
APA Presidential Task Force on Evidence-Based Practice (2006). Evidence-Based practice in psychology. Am. Psychol. 61, 271–285.
Attkisson, C. C., and Zwick, R. (1982). The client satisfaction questionnaire: psychometric properties and correlations with service utilization and psychotherapy outcome. Eval. Program Plann. 5, 233–237. doi: 10.1016/0149-7189(82)90074-X
Azevedo, L. F., Costa-Pereira, A., Mendonça, L., Dias, C. C., and Castro-Lopes, J. M. (2012). Epidemiology of chronic pain: a population-based nationwide study on its prevalence, characteristics and associated disability in Portugal. J. Pain 13, 773–783. doi: 10.1016/j.jpain.2012.05.012
Becker, J., Schwartz, C., Saris-baglama, R. N., Kosinski, M., and Bjorner, J. B. (2007). Using item response theory (IRT) for developing and evaluating the Pain Impact Questionnaire (PIQ-6TM). Pain Med. 8, S129–S144. doi: 10.1111/j.1526-4637.2007.00377.x
Bergmo, T. S. (2015). How to measure costs and benefits of ehealth interventions: an overview of methods and frameworks. J. Med. Internet Res. 17:e254. doi: 10.2196/jmir.4521
Blankers, M., Koeter, M. W. J., and Schippers, G. M. (2010). Missing data approaches in eHealth research: simulation study and a tutorial for nonmathematically inclined researchers. J. Med. Internet Res. 12:e54. doi: 10.2196/jmir.1448
Breivik, H., Collett, B., Ventafridda, V., Cohen, R., and Gallacher, D. (2006). Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur. J. Pain 10, 287–333. doi: 10.1016/j.ejpain.2005.06.009
Buhrman, M., Skoglund, A., Husell, J., Bergström, K., Gordh, T., Hursti, T., et al. (2013). Guided internet-delivered acceptance and commitment therapy for chronic pain patients: a randomized controlled trial. Behav Res Ther. 51, 307–315. doi: 10.1016/j.brat.2013.02.010
Carvalho, S. A., Gillanders, D., Palmeira, L., Pinto-Gouveia, J., and Castilho, P. (2018a). Mindfulness, selfcompassion, and depressive symptoms in chronic pain: the role of pain acceptance. J. Clin. Psychol. 74, 2094–2106. doi: 10.1002/jclp.22689
Carvalho, S. A., Trindade, I. A., Gillanders, D., Pinto-Gouveia, J., and Castilho, P. (2019). Cognitive fusion and depressive symptoms in women with chronic pain: a longitudinal growth curve modelling study over 12 months. Clin. Psychol. Psychother. 26, 616–625. doi: 10.1002/cpp.2386
Carvalho, S. A., Trindade, I. A., Gillanders, D., Pinto-Gouveia, J., and Castilho, P. (2020). Self-Compassion and depressive symptoms in chronic pain (CP): a 1-Year longitudinal study. Mindfulness (N Y). 11, 709–719. doi: 10.1007/s12671-019-01292-7
Carvalho, S. A., Xavier, A., Gillanders, D., Pinto-Gouveia, J., and Castilho, P. (2018b). Rumination and valued living in women with chronic pain: how they relate to the link between mindfulness and depressive symptoms. Curr. Psychol. doi: 10.1007/s12144-018-0052-z [Epub ahead of print].
Castilho, P., Pinto-Gouveia, J., and Duarte, J. (2015a). Evaluating the multifactor structure of the long and short versions of the self-compassion scale in a clinical sample. J. Clin. Psychol. 71, 856–870. doi: 10.1002/jclp.22187
Castilho, P., Pinto-Gouveia, J., and Duarte, J. (2015b). Exploring self-criticism: confirmatory factor analysis of the FSCRS in clinical and nonclinical samples. Clin. Psychol. Psychother. 22, 153–164. doi: 10.1002/cpp.1881
Cavalheiro, L. M., Gil, J. A. N., Gonçalves, R. S., Pacheco, M. P., Ferreira, P. L., and Fã, L. (2011). Measuring the pain impact in adults with a chronic pain condition: adaptation and validation of the pain impact questionnaire (PIQ-6) to the portuguese culture. Pain Med. 12, 1538–1543. doi: 10.1111/j.1526-4637.2011.01222.x
Chapin, H. L., Darnall, B. D., Seppala, E. M., Doty, J. R., Hah, J. M., and Mackey, S. C. (2014). Pilot study of a compassion meditation intervention in chronic pain. J. Compassionate Health Care 1:4. doi: 10.1186/s40639-014-0004-x
Costa, J., and Gouveia, J. P. (2013). A new approach to explain the link between social support and depression in a 2-years arthritis rheumatoid sample. is there any moderation effect of acceptance? Int. J. Psychol. Psychol. Ther. 13, 65–82.
Costa, J., and Pinto-Gouveia, J. (2013). Experiential avoidance and self-compassion in chronic pain. J. Appl. Soc. Psychol. 43, 1578–1591. doi: 10.1111/jasp.12107
Dahl, J., and Lundgren, T. (2016). “Acceptance and commitment therapy (ACT) in the treatment of chronic pain,” in Mindfulness-Based Treatment Approaches: Clinician’s Guide to Evidence Base and Applications, ed. R. A. Baer (San Diego, CA: Elsevier Academic Press), 285–306. doi: 10.1016/B978-012088519-0/50014-9
Dinis, A., Gouveia, J. P., Duarte, C., and Castro, T. (2011). Estudo de validação da versão portuguesa da escala de respostas ruminativas – versão reduzida. Psychologica 54, 175–202. doi: 10.14195/1647-8606_54_7
Dominick, C. H., Blyth, F. M., and Nicholas, M. K. (2012). Unpacking the burden: understanding the relationships between chronic pain and comorbidity in the general population. Pain 153, 293–304. doi: 10.1016/j.pain.2011.09.018
Eccleston, C., Morley, S. J., and Williams, A. C. (2013). Psychological approaches to chronic pain management: evidence and challenges. Br. J. Anaesth. 111, 59–63. doi: 10.1093/bja/aet207
Edwards, K. A., Pielech, M., Hickman, J., Ashworth, J., Sowden, G., and Vowles, K. E. (2019). The relation of self-compassion to functioning among adults with chronic pain. Eur. J. Pain (United Kingdom) 23, 1538–1547. doi: 10.1002/ejp.1429
Elliott, A. M., Smith, B. H., Penny, K. I., Smith, W. C., and Chambers, W. A. (1999). The epidemiology of chronic pain in the community. Lancet 354, 1248–1252. doi: 10.1016/S0140-6736(99)03057-3
Feldman, G., Hayes, A., Kumar, S., Greeson, J., and Laurenceau, J. P. (2007). Mindfulness and emotion regulation: the development and initial validation of the Cognitive and Affective Mindfulness Scale-Revised (CAMS-R). J. Psychopathol. Behav. Assess. 29:177. doi: 10.1007/s10862-006-9035-8
Figueiral, A. (2002). Adaptação Cultural e Linguística do Instrumento de Medida: McGill Pain Questionnaire. Coimbra: Escola Superior de Tecnologia da Saúde de Coimbra.
Fledderus, M., Schreurs, K. M., Bohlmeijer, E. T., and Vollenbroek-Hutten, M. M. (2015). Development and pilot evaluation of an online relapse-prevention program based on acceptance and commitment therapy for chronic pain patients. JMIR Hum. Factors 2:e1. doi: 10.2196/humanfactors.3302
Francis, A. W., Dawson, D. L., and Golijani-Moghaddam, N. (2016). The development and validation of the comprehensive assessment of acceptance and commitment therapy processes (CompACT). J. Context. Behav. Sci. 5, 134–145. doi: 10.1016/j.jcbs.2016.05.003
Gilbert, P. (2009). Introducing compassion-focused therapy. Adv. Psychiatr. Treat. 15, 199–208. doi: 10.1192/apt.bp.107.005264
Gilbert, P., Clarke, M., Hempel, S., Miles, J. N. V., and Irons, C. (2004). Criticizing and reassuring oneself: an exploration of forms, styles and reasons in female students. Br. J. Clin. Psychol. 43, 31–50. doi: 10.1348/014466504772812959
Gilbert, P., McEwan, K., Mitra, R., Richter, A., Franks, L., Mills, A., et al. (2009). An exploration of different types of positive affect in students and patients with a bipolar disorder. Clin. Neuropsychiatry 6, 135–143.
Gillanders, D. T., Bolderston, H., Bond, F. W., Dempster, M., Flaxman, P. E., Campbell, L., et al. (2014). The development and initial validation of the cognitive fusion questionnaire. Behav. Ther. 45, 83–101. doi: 10.1016/j.beth.2013.09.001
Gooding, H., Stedmon, J., and Crix, D. (2020). ‘All these things don’t take the pain away but they do help you to accept it’: making the case for compassion-focused therapy in the management of persistent pain. Br. J. Pain 14, 31–41. doi: 10.1177/2049463719857099
Hayes, S. C., Strosahl, K. D., and Wilson, K. G. (1999). Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change. New York, NY: Guilford Publications.
Højsted, J., and Sjøgren, P. (2007). Addiction to opioids in chronic pain patients: a literature review. Eur. J. Pain 11, 490–518. doi: 10.1016/j.ejpain.2006.08.004
Luoma, J. B., and Platt, M. G. (2015). Shame, self-criticism, self-stigma, and compassion in acceptance and commitment therapy. Curr. Opin. Psychol. 2, 97–101. doi: 10.1016/j.copsyc.2014.12.016
McCracken, L. M. (1998). Learning to live with the pain: acceptance of pain predicts adjustment in persons with chronic pain. Pain 74, 21–27. doi: 10.1016/S0304-3959(97)00146-2
McCracken, L. M., and Eccleston, C. (2003). Coping or acceptance: what to do about chronic pain? Pain 105, 197–204. doi: 10.1016/S0304-3959(03)00202-1
McCracken, L. M., and Vowles, K. E. (2006). Acceptance of chronic pain. Curr. Pain Headache Rep. 10, 90–94. doi: 10.1007/s11916-006-0018-y
Melville, K. M., Casey, L. M., and Kavanagh, D. J. (2010). Dropout from internet-based treatment for psychological disorders. Br. J. Clin. Psychol. 49(Pt 4), 455–471. doi: 10.1348/014466509X472138
Melzack, R. (1975). The McGill pain questionnaire: major properties and scoring methods. Pain 1, 277–299. doi: 10.1016/0304-3959(75)90044-5
Neff, K., and Germer, C. (2018). The Mindful Self-Compassion Workbook: A Proven Way to Accept Yourself, Build Inner Strength, and Thrive. New York, NY: Guilford Publications.
Neff, K. D. (2003). The development and validation of a scale to measure self-compassion. Self Identity 2, 223–250. doi: 10.1080/15298860309027
Pais-Ribeiro, J., Silva, I., Ferreira, T., Martins, A., Meneses, R., and Baltar, M. (2007). Validation study of a portuguese version of the hospital anxiety and depression scale. Psychol. Health Med. 12, 225–235. doi: 10.1080/13548500500524088
Palmeira, L., Pinto-Gouveia, J., and Cunha, M. (2017). Exploring the efficacy of an acceptance, mindfulness & compassionate-based group intervention for women struggling with their weight (Kg-Free): a randomized controlled trial. Appetite 112, 107–116. doi: 10.1016/j.appet.2017.01.027
Parry, S. L., and Malpus, Z. (2017). Reconnecting the mind and body: a pilot study of developing compassion for persistent pain. Patient Exp. J. 4, 145–153. doi: 10.35680/2372-0247.1175
Phillips, C. J. (2009). The cost and burden of chronic pain. Rev. Pain 3, 2–5. doi: 10.1177/204946370900300102
Pinto-Gouveia, J., Carvalho, S. A., Palmeira, L., Castilho, P., Duarte, C., Ferreira, C., et al. (2017). BEfree: a new psychological program for binge eating that integrates psychoeducation, mindfulness, and compassion. Clin. Psychol. Psychother. 24, 1090–1098. doi: 10.1002/cpp.2072
Pinto-Gouveia, J., Costa, J., and Marôco, J. (2015). The first 2 years of rheumatoid arthritis: the influence of acceptance on pain, physical limitation and depression. J. Health Psychol. 20, 102–112. doi: 10.1177/1359105313499807
Pinto-Gouveia, J., Dinis, A., Gregório, S., and Pinto, A. M. (2020). Concurrent effects of different psychological processes in the prediction of depressive symptoms – the role of cognitive fusion. Curr. Psychol. 39, 528–539. doi: 10.1007/s12144-017-9767-5
Plumb, J. C., and Vilardaga, R. (2010). Assessing treatment integrity in acceptance and commitment therapy: strategies and suggestions. Int. J. Behav. Consult. Ther. 6, 263–295. doi: 10.1037/h0100912
Rockliff, H., Gilbert, P., McEwan, K., Lightman, S., and Glover, D. (2008). A pilot exploration of heart rate variability and salivary cortisol responses to compassion-focused imagery. Clin. Neuropsychiatry 5, 132–139.
Rockliff, H., Karl, A., McEwan, K., Gilbert, J., Matos, M., and Gilbert, P. (2011). Effects of intranasal oxytocin on “compassion focused imagery.”. Emotion 11, 1388–1396. doi: 10.1037/a0023861
Scott, W., Chilcot, J., Guildford, B., Daly-Eichenhardt, A., and McCracken, L. M. (2018). Feasibility randomized-controlled trial of online Acceptance and Commitment Therapy for patients with complex chronic pain in the United Kingdom. Eur. J. Pain (United Kingdom) 22, 1473–1484. doi: 10.1002/ejp.1236
Shei, A., Hirst, M., Kirson, N. Y., Enloe, C. J., Birnbaum, H. G., and Dunlop, W. C. N. (2015). Estimating the health care burden of prescription opioid abuse in five European countries. Clin. Outcomes Res. 7, 477–488. doi: 10.2147/CEOR.S85213
Skinta, M. D., Lezama, M., Wells, G., and Dilley, J. W. (2015). Acceptance and compassion-based group therapy to reduce HIV Stigma. Cogn. Behav. Pract. 22, 481–490. doi: 10.1016/j.cbpra.2014.05.006
Teixeira, R. J., Ferreira, G., and Pereira, M. G. (2017). Portuguese validation of the cognitive and affective mindfulness scale-revised and the Philadelphia Mindfulness Scale. Mindfulness Compassion 2, 3–8. doi: 10.1016/j.mincom.2017.03.001
The WHOQOL Group (1998). Development of the world health organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychol. Med. 28, 551–558. doi: 10.1017/S0033291798006667
Treynor, W., Gonzalez, R., and Nolen-Hoeksema, S. (2003). Rumination reconsidered: a psychometric analysis. Cognit. Ther. Res. 27, 247–259. doi: 10.1023/A:1023910315561
Trindade, I. A., Ferreira, C., and Pinto-Gouveia, J. (2020). Acceptability and preliminary test of efficacy of the Mind programme in women with breast cancer: an acceptance, mindfulness, and compassion-based intervention. J Context Behav Sci. 15, 162–171. doi: 10.1016/j.jcbs.2019.12.005
Trompetter, H. R., Bohlmeijer, E. T., Veehof, M. M., and Schreurs, K. M. G. (2014). Internet-based guided self-help intervention for chronic pain based on acceptance and commitment therapy: a randomized controlled trial. J. Behav. Med. 38, 66–80. doi: 10.1007/s10865-014-9579-0
Vaz Serra, A., Cristina Canavarro, M., Simões, M., Pereira, M., Gameiro, S., João Quartilho, M., et al. (2006). Estudos psicométricos do instrumento de avaliação da qualidade de vida da organização mundial de saúde (WHOQOL-Bref) para Português de Portugal. Psiquiatr. Clínica 27, 31–40.
Vilardaga, R., Davies, P. S., Vowles, K. E., and Sullivan, M. D. (2020). Theoretical grounds of pain tracker self manager: an acceptance and commitment therapy digital intervention for patients with chronic pain. J. Context. Behav. Sci. 15, 172–180. doi: 10.1016/j.jcbs.2020.01.001
Vowles, K. E., and McCracken, L. M. (2008). Acceptance and values-based action in chronic pain: a study of treatment effectiveness and process. J. Consult. Clin. Psychol. 76, 397–407. doi: 10.1037/0022-006X.76.3.397
Vowles, K. E., McCracken, L. M., and Eccleston, C. (2007). Processes of change in treatment for chronic pain: the contributions of pain, acceptance, and catastrophizing. Eur. J. Pain 11, 779–787. doi: 10.1016/j.ejpain.2006.12.007
Vowles, K. E., Wetherell, J. L., and Sorrell, J. T. (2009). Targeting acceptance, mindfulness, and values-based action in chronic pain: findings of two preliminary trials of an outpatient group-based intervention. Cogn. Behav. Pract. 16, 49–58. doi: 10.1016/j.cbpra.2008.08.001
Vowles, K. E., Witkiewitz, K., Sowden, G., and Ashworth, J. (2014). Acceptance and commitment therapy for chronic pain: evidence of mediation and clinically significant change following an abbreviated interdisciplinary program of rehabilitation. J Pain 15, 101–113. doi: 10.1016/j.jpain.2013.10.002
Wren, Y., Miller, L. L., Peters, T. J., Emond, A., and Roulstone, S. (2016). Prevalence and predictors of persistent speech sound disorder at eight years old: findings from a population cohort study. J. Speech Lang. Hear. Res. 59, 647–673. doi: 10.1044/2015_JSLHR-S-14-0282
Yadavaia, J. E., Hayes, S. C., and Vilardaga, R. (2014). Using acceptance and commitment therapy to increase self-compassion: a randomized controlled trial. J. Context. Behav. Sci. 3, 248–257. doi: 10.1016/j.jcbs.2014.09.002
Ziemer, K. S., Fuhrmann, A., and Hoffman, M. A. (2015). Effectiveness of a positive writing intervention for chronic pain: a randomized trial. MYOPAIN 23, 1–10. doi: 10.1080/24708593.2017.1307893
Keywords: acceptance and commitment therapy, chronic pain, compassion-based intervention, eHealth, ICT-delivered interventions, mindfulness, self-management
Citation: Carvalho SA, Trindade IA, Duarte J, Menezes P, Patrão B, Nogueira MR, Guiomar R, Lapa T, Pinto-Gouveia J and Castilho P (2021) Efficacy of an ACT and Compassion-Based eHealth Program for Self-Management of Chronic Pain (iACTwithPain): Study Protocol for a Randomized Controlled Trial. Front. Psychol. 12:630766. doi: 10.3389/fpsyg.2021.630766
Received: 18 November 2020; Accepted: 11 February 2021;
Published: 09 March 2021.
Edited by:
Ioana Roxana Podina, University of Bucharest, RomaniaReviewed by:
Francisco Javier Cano-García, Seville University, SpainLiviu Andrei Fodor, Babeş-Bolyai University, Romania
Copyright © 2021 Carvalho, Trindade, Duarte, Menezes, Patrão, Nogueira, Guiomar, Lapa, Pinto-Gouveia and Castilho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Inês A. Trindade, aW5lcy5hbG1laWRhdHJpbmRhZGVAZ21haWwuY29t