 Luca Queirolo
Luca Queirolo Christian Bacci
Christian Bacci Andrea Roccon
Andrea Roccon Gastone Zanette
Gastone Zanette Carla Mucignat
Carla Mucignat- 1Section of Clinical Dentistry, Department of Neurosciences, University of Padua, Padua, Italy
- 2Department of Philosophy, Sociology, Education and Applied Psychology, University of Padua, Padua, Italy
- 3Department of Molecular Medicine, University of Padua, Padua, Italy
Introduction and aim: Dentistry is a highly demanding profession with a strong mental and physical involvement, possibly generating anxiety. Very few studies assessed psychophysiological activity in dentists, while none tried to relate it with gender during a routine working day. This study aims at evaluating correlations between gender, psychophysiological indexes, and psychological variables.
Materials and methods: Data were acquired at the Dental Clinic of the University of Padua on 20 healthy young dentists (10 M-10F) during a 24 h period of a working day. Physiological variables (measured with E4 Empatica) were electrodermal activity (EDA), heart rate variability (HRV) and heart rate (HR). Participants anxiety was measured through a self-reported scale on patient-relationship anxiety and through the Generalized Anxiety Disorder-7 Questionnaire (GAD-7).
Results: 5 (3F, 2 M) participants over 20 had a GAD-7 score ≥ 10. Female gender, in comparison to Male, was associated with higher perceived patient relationship anxiety (p = 0.002) and lower HRV (p-adj = 0.022). The gender Male, although being associated with lower level of self-reported anxiety (p = 0.002), showed an equal number of subjects with a GAD-7 score ≥ 10 (p = 0.371). No interaction between gender and EDA was found, nor an effect of GAD score on EDA, HRV and HR values. Higher values of EDA were found during sleep time; a difference between sleep time and working time EDA (p = 0.037) and a difference between sleep time and daytime (p = 0.0045). A different HR between sleep and all daytime (p < 0.001) was also highlighted.
Conclusion: 25% of dentists fell within generalized anxiety disorder diagnosis, compared to a maximum of 8.6% in the general population. A possible general biomarker of excessive stress response was measured: a shift of circadian sympathetic activity was found in dentists; a higher activity during sleep in comparison to working time and daytime. The Female gender was associated with higher perceived patient-approach anxiety, lower parasympathetic activity, and a comparable sympathetic activity to the Male gender, thus fostering a possible vulnerability to excessive stress. This study underlines the need to empower the psychological approach to stress and patient-relationship in dentistry.
Introduction
Patients’ anxiety for dental procedures is a well-established problem, but who cares about the dentist’s point of view (Armfield and Heaton, 2013)? Stress and anxiety were examined among dental and health professionals and from these studies, it appears that the quality of life of dentists is lower than the general population (Myers and Myers, 2004). Probably this is related to the intrinsic nature of the helping professions (Maslach and Pines, 1977; Rada and Johnson-Leong, 2004), but not solely; being a dentist is a high demanding profession with a strong mental and physical involvement, possibly generating stress and anxiety (DiMatteo et al., 1993). Besides the intrinsic issues of a helping profession, dentists have often to face the management of the dental office. Indeed, the relationship with the patient, the scheduling pressure and the management of employees represent the main causes of stress for dentists (Myers and Myers, 2004). According to some authors, this occupational stress can also lead to a higher risk for cardiovascular diseases (Cutright et al., 1977; Cooper et al., 1978, 1988). The need for professionals to access techniques to manage their stress and improve the communication with the patient is also reported (Moore and Brødsgaard, 2001). It remains to be clarified whether gender differences in anxiety and occupational stress exist. The literature reports a predisposition for anxiety in women, although the factors that may cause this vulnerability remain unclear, Kessler et al. found that the prevalence of a generalized anxiety disorder in women (6.6%) is higher than in men (3.6%) (Kessler et al., 1994; Altemus et al., 2014). Conversely, when anxiety is evaluated in dentists during work, this gender difference seems not to be relevant (Altemus et al., 2014; Davidovich et al., 2015; Asif et al., 2022). The data on anxiety and stress in dentists often derive from questionnaires without ever providing objective measures. However, wearable monitoring devices can measure parameters such as electrodermal activity (EDA), heart rate (HR) and heart rate variability (HRV) and thus provide a step toward an objective psychophysiological measurement of anxiety and stress during the working day (Lu et al., 2020; Posada-Quintero and Chon, 2020; Schuurmans et al., 2020). These psychophysiological data are very important. An increase in HR is associated with increased risk of death (Nauman et al., 2011), more specifically higher HR is associated with both cardiovascular mortality and non-cardiovascular mortality (Woodward et al., 2014; Alhalabi et al., 2017). A reduced HRV is associated with increased cardiovascular risk (Weber et al., 2010), lower resiliency (stress tolerance) in the face of stressful situations (Hansen et al., 2009). Noteworthy longer periods of reduced HRV are associated with worrying, with decreased explicit positive affect, and with increased tension (Verkuil et al., 2016). Furthermore HRV it is highly related to a flexible control over behavior (Thayer et al., 2012), that is hugely important in helping professions such dentistry. The well-known flight or fight memorandum still holds to this day (Cannon, 1915). EDA (being a pure sympathetic index), can provide information on the sympathetic activity and the flight or fight response, because an excessive sympathetic activity can thus fostering healthy related issues (Dickerson and Kemeny, 2004; Andela et al., 2015; Resmini et al., 2016; Richardson et al., 2016; Mohd Azmi et al., 2021). Synthesizing the relevance of all the above-mentioned data, this study aims to investigate the relationships between peripheral psychophysiological parameters measured with a wearable monitoring device and working hours, gender, self-reported anxiety while confronting the patient (VAS-anxiety) and questionnaire measured anxiety (GAD-7) in young dentists.
Materials and methods
Participants and setting
Psychophysiological measures and psychological data were acquired from 20 healthy young dentists with at least 1 year of employment attending a post-graduate course at the Dental Clinic of the University of Padua (Padua, Italy). The age of the 20 participants ranged from 26 to 36 years (M = 28.95, SD = 2.98), 50% were Male. Exclusion criteria were cardiovascular pathologies or psychiatric disorders. Inclusion criteria were being a dentist at the Dental Clinic of the University of Padua, with less than 5 years of clinical experience. Participants enrolled in the present study have signed informed consent prior to participation. The study was approved by the Ethical Committee of Department of General Psychology, University of Padua, n. 3274/2019.
Procedure
Participants were invited and informed about the aim of the study through an information leaflet, and written informed consent was obtained from all subjects after they received all necessary information on the study. Participants were asked to wear a Empatica E4 (Empatica Inc.) wristband, for 24 consecutive hours while they were working, during sleep and during other daytime activities. Furthermore, subjects were asked to fill-in a diary reporting start and end time of the three different conditions (“work,” “sleep,” “daytime”). Data were collected between March and July 2022.
Anxiety assessment
Anxiety levels were scored with the Generalized Anxiety Disorder questionnaire GAD-7 and with a Visual Analog Scale (VAS) about Self Perceived Anxiety (Spitzer et al., 2006; Swinson, 2006; Facco et al., 2011). Anxiety scores during the clinical activity were obtained through a self-reported VAS, stating a single item question: “on a scale from 0 to 10, were 0 is nothing at all and 10 is extremely, how do you rate yourself anxious while relating to patients”? A value of 7 (or more) at VAS analog test was taken as the cutoff in defining subjects anxious in relating to patients (ANX+). Participants that reported a VAS-anxiety<7 were defined “ANX−”. GAD-7 was also used as gold-standard measure to report general anxiety symptoms. A value of GAD ≥10 was considered as a positive GAD and defined as “GAD+,” while a value <10 was reported as “GAD−”.
Physiological assessments
The physiological parameters were obtained through Empatica E4, a wearable device in the form of a wristband that allows for measuring Electrodermal Activity (EDA), blood volume pulse – from which heart rate (HR) and heart rate variability (HRV) are derived, skin temperature, and movement (Garbarino et al., 2014). EDA is a property of the skin that underlines the variation of the electrical conduction in response to sweat secretions and it is a sympathetic index (Boucsein, 2012). HRV is the physiological phenomenon of variation in the time interval between heartbeats. It is a parasympathetic index that reflects vagal activity, it is measured with the root mean square of the successive differences between inter beats intervals (Ernst, 2017; Kim et al., 2018). Participants were asked to wear the Empatica E4 for 24 h on their non-dominant hand. HR was expressed in beats per minute (bpm) and derived through Empatica algorithms to the blood volume pulse. They provide also the inter beats intervals (IBI) from photoplethysmography (PPG) signal. HRV was obtained by extraction of the root mean square of successive differences between normal heartbeats (RMSSD) extracted by first calculating from IBI each successive time difference between heartbeats in ms, over a short-term period of 30 s. Then, each of the values was squared and averaged before the square root of the total was obtained. The sensor used to detect blood volume pulse is a PPG sensor, which is known to be subject to missing data as a result of movement or pressure artifacts (Chen et al., 2015). Artifacts were removed, discarding zero values and other single data point outliers. The analysis of EDA included the extraction of a parameter called skin conductance level (SCL). The electrodes used were silver coated with copper underlay on brass electrodes. The threshold for the amplitude of significant signal was set to a minimum rise of 0.005 μSiemens. SCL values were then normalized using the min-max method. Physiological data were down-sampled to 1hz and labeled as belonging to one of the three monitoring periods (defined as condition “work,” “sleep” and “daytime”). Data of each subject were then aggregated into periods, expressing their mean values.
Statistical methods
As a first step, characteristics of subjects with anxiety (N = 5; GAD≥10) were compared to subjects with no anxiety (N = 15; GAD<10) using independent t tests and a chi-square test, the same analysis was performed splitting groups according to Self-Perceived Anxiety cut-off. We then evaluated if the physiological parameters differed among subjects during the three periods of the day (factor “condition,” 3 levels, within-subjects) and according to the anxiety symptoms reporting both using GAD-7 and Self Perceived Anxiety, (factor “anxiety,” 2 levels, between subjects). The statistical model to test this was a two-way mixed ANOVA model. We then repeated the analysis considering gender differences (factor “gender,” 2 levels, between-subjects) and anxiety symptoms reporting. The analyzes were performed with R version 3.5.1, also used to check for assumptions of normally distributed residuals on all levels of the model. Separate models were considered for each type of parameter (EDA, HR, and HRV). Post-hoc tests were then performed using Tukey for multiple comparisons.
Results
Male and Female groups were comparable (Table 1). An initial qualitative outcome was that 5 participants showed a GAD-7 score ≥ 10 (3F, 2M) and that 10 participants reported a VAS anxiety ≥7 (7F, 3M). Chi-square statistics showed a significant imbalance of Gender distribution as regards Self-Perceived Anxiety [χ2(1,30), p = 0.002], a higher number of women in comparison to men reported anxiety in confronting the patients (Table 2). However, there was no effect of Gender distribution when considering GAD+ vs. GAD-population (p = 0.371; Table 3). Therefore, Two-Way Mixed ANOVA analyzes were performed considering only GAD as anxiety factor.
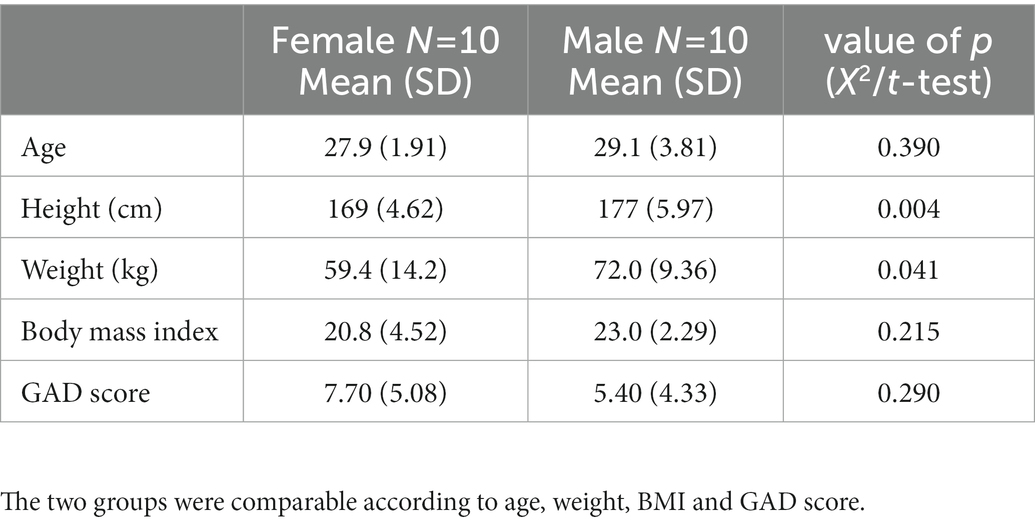
Table 1. Participant characteristics according to gender.
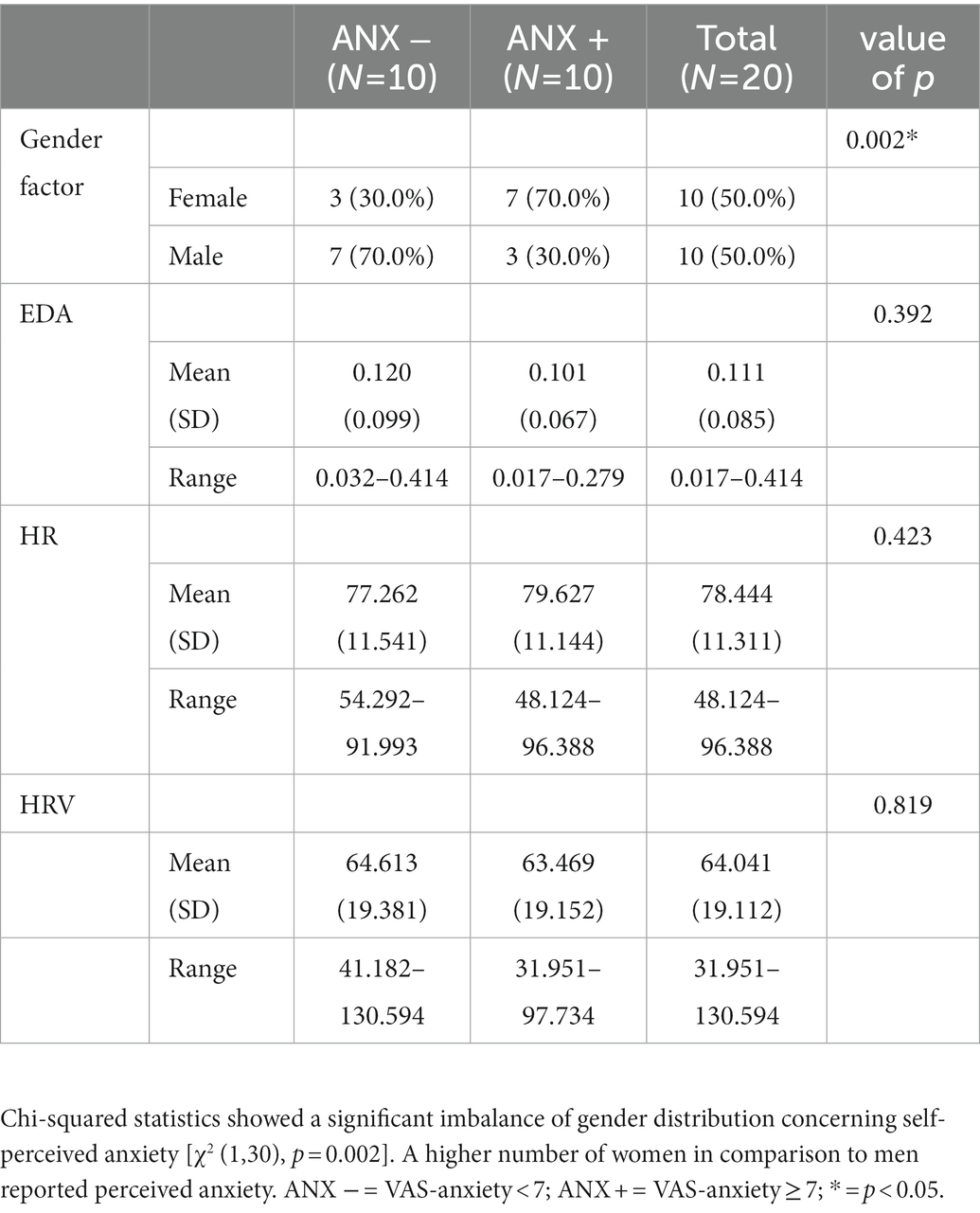
Table 2. Gender factor and EDA, HRV, HR values in ANX− and ANX+ dentists.
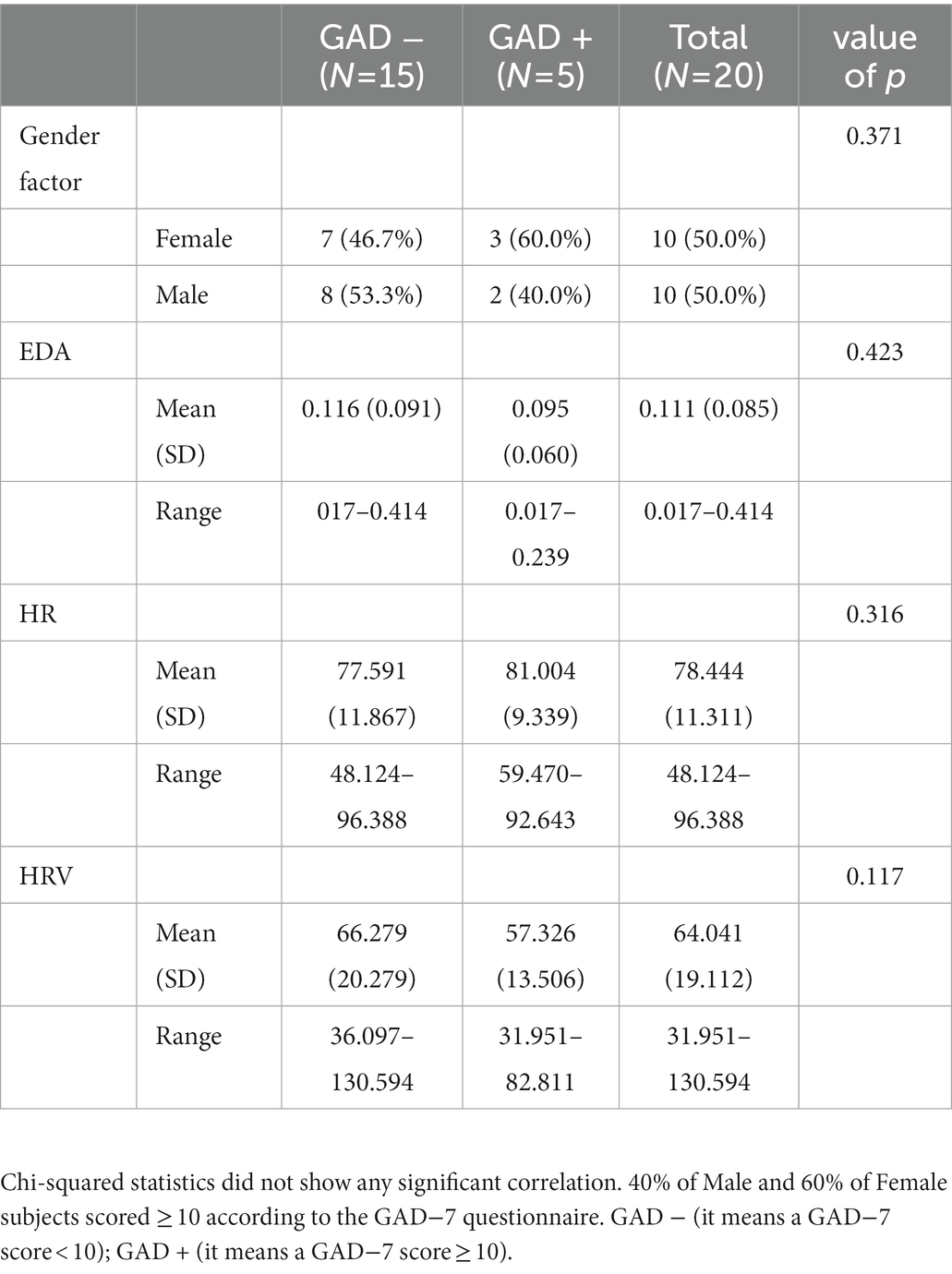
Table 3. Gender factor and EDA, HRV, HR values in GAD − and GAD + dentists.
Electrodermal activity
The results of the Two-Way Mixed ANOVA showed that there was a significant main effect of conditions [F (2,54) = 5.2118, p = 0.0085] on physiological value EDA. A pairwise comparisons using t-tests with pooled SD revealed significant pairwise differences between conditions “sleep” and “daytime” (p = 0.0045) and between “sleep” and “work” (p = 0.0367), showing a higher EDA activity during “sleep” in comparison to “daytime” and “work” (Figure 1). There was no interaction effect for EDA, when considering Gender and GAD ± [F (1,56) = 1.1432, p = 0.2896], with GAD+ (Mean 0.095, SD = 0.091) and GAD− (Mean = 0.116, SD =0.116) performing overall similarly during the different conditions (Figure 2).
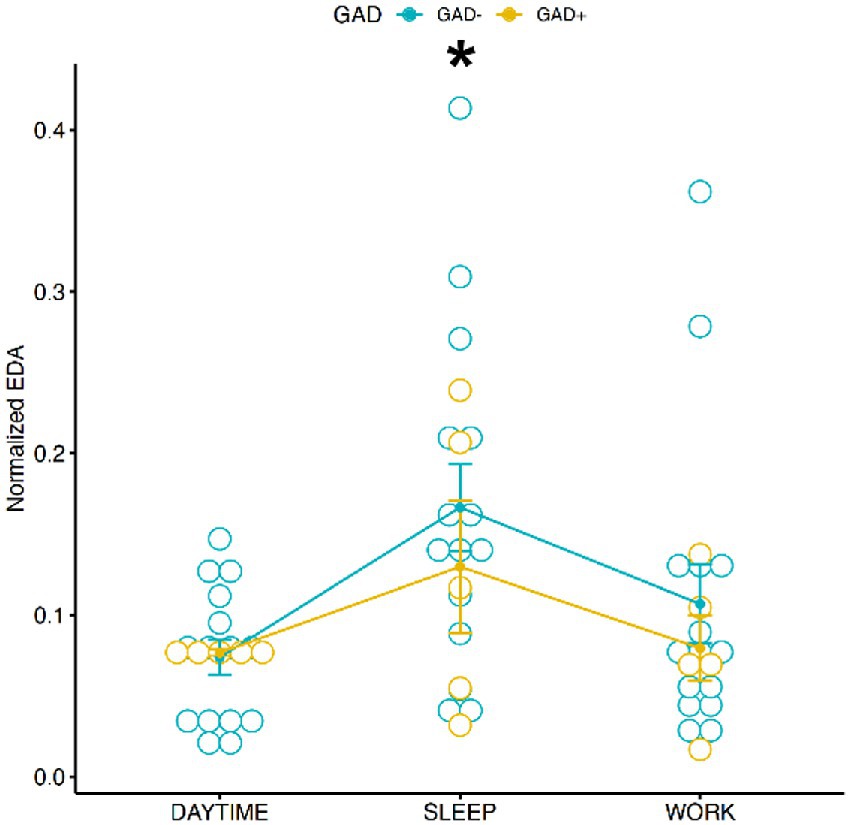
Figure 1. Distribution of normalized EDA during the 3 conditions according to GAD ±. There was no difference between groups according to factor GAD-or GAD+ while EDA values were clearly different during daytime or work in comparison to sleep. Eda values were higher during sleep than daytime and work conditions. * = p < 0.05.
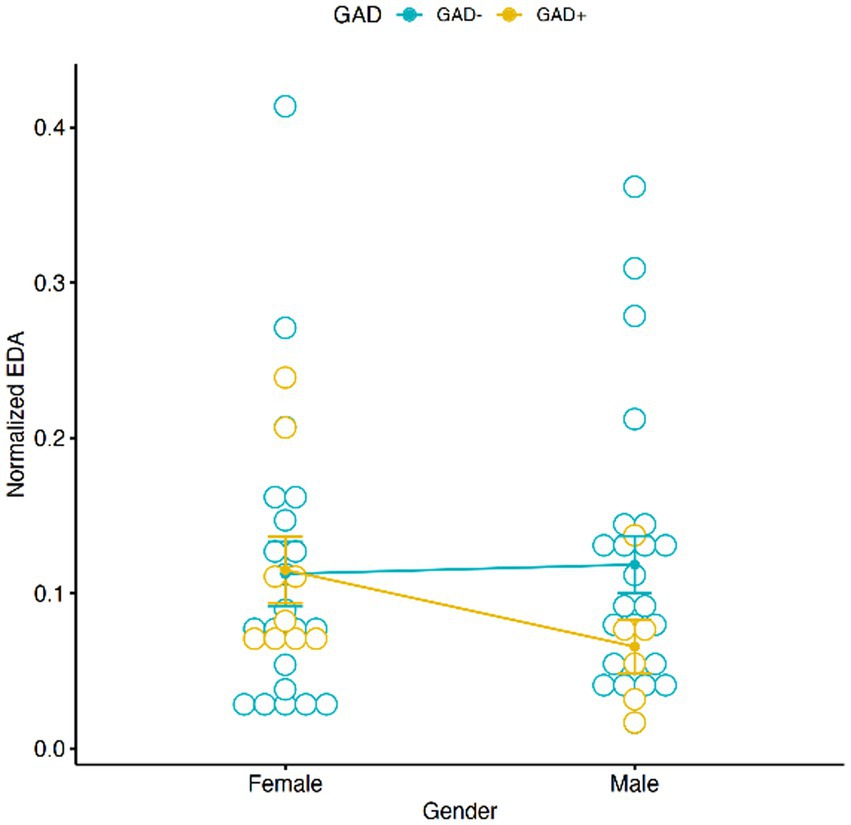
Figure 2. Graphic distribution of normalized EDA according to GAD ± and Gender. No significant interaction was found between Gender, EDA and GAD ±.
Heart rate variability
Analysis on HRV did not show any significant correlation with GAD ± and conditions (Figure 3), nor among GAD ± and gender effect (Figure 4). However, the Tukey multiple comparisons of means showed a statistically significant difference between Male and Female HRV values (p-adj = 0.022), with Females showing a lower HRV in comparison to Males.
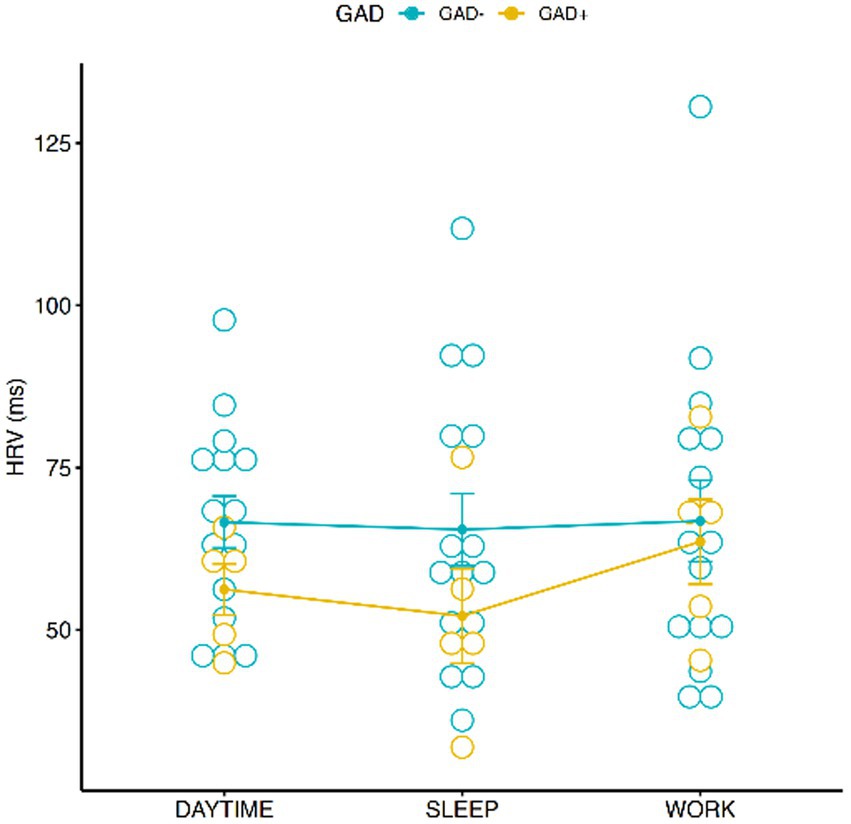
Figure 3. Graphic distribution of HRV values during the 3 conditions according to GAD ±.
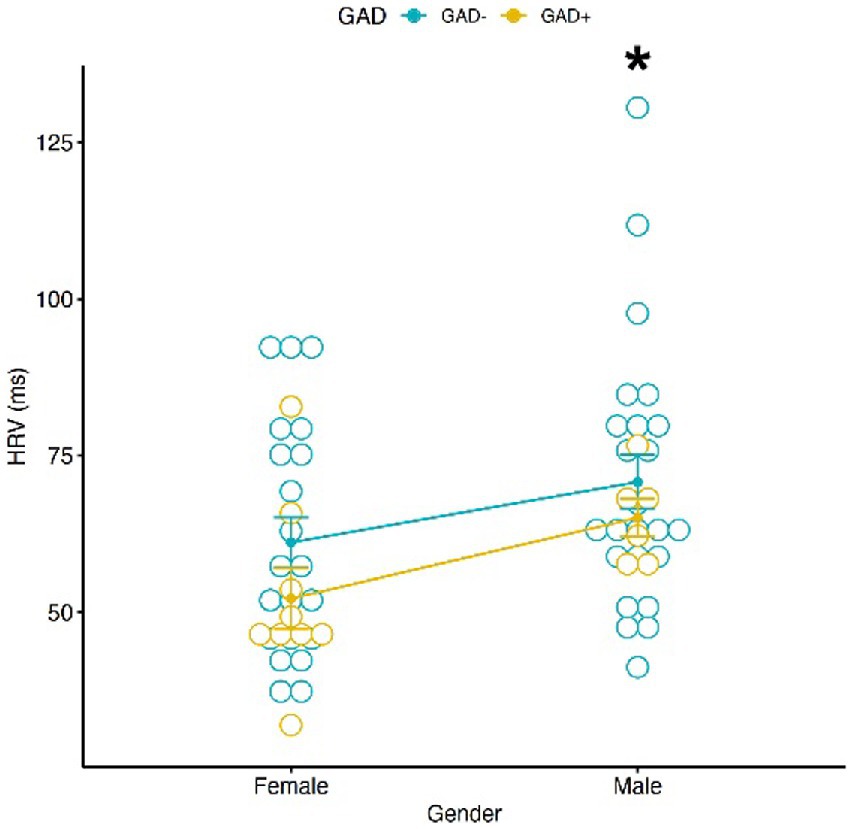
Figure 4. Graphic distribution of HRV values according to GAD ± and Gender. A significant different HRV value according to Gender was found. No significant interaction was found between Gender, HRV and GAD±. * = p < 0.05.
Heart rate
A significant main effect of conditions on HR was found [F(2,54) = 25.94, p < 0.001; Figure 5], the pairwise comparisons using t-tests with pooled SD showed a significant difference between “sleep” and “daytime” (p < 0.001) and “sleep” and “work” (p < 0.001). No correlation was found between HR, Gender and GAD ± (Figure 6). Females showed an average HR value 5.59 bpm higher than Males, without reaching the accepted alpha statistical significance level. Tukey multiple comparisons did not show any significative difference between Female and Male HR values (p-adj = 0.057).
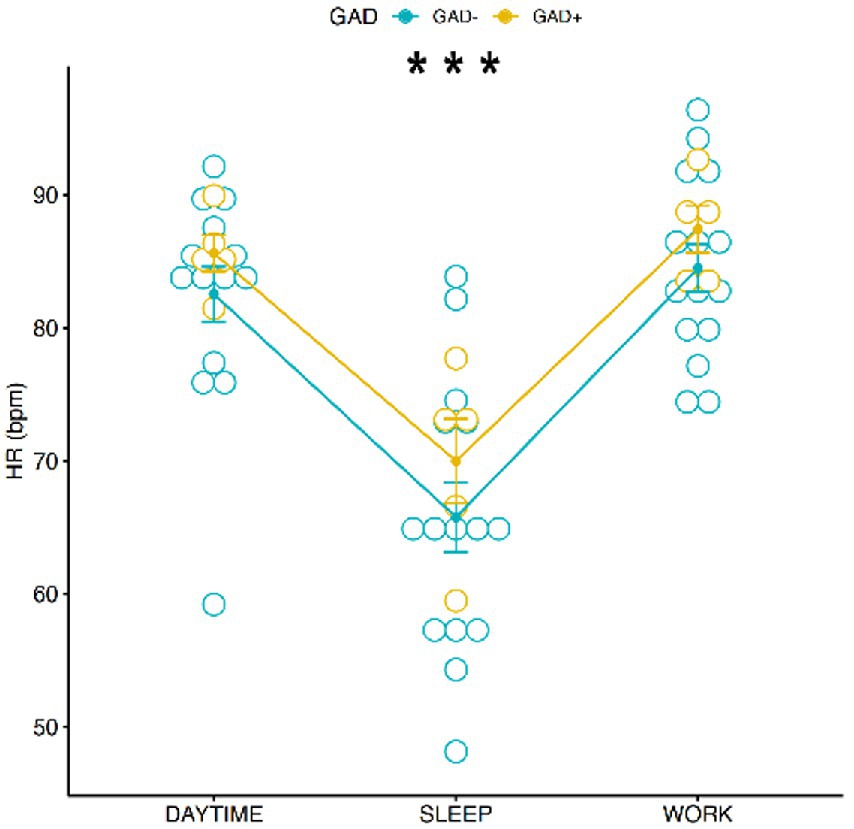
Figure 5. Graphic distribution of HR values during the 3 conditions according to GAD ±. *** = p < 0.0001.
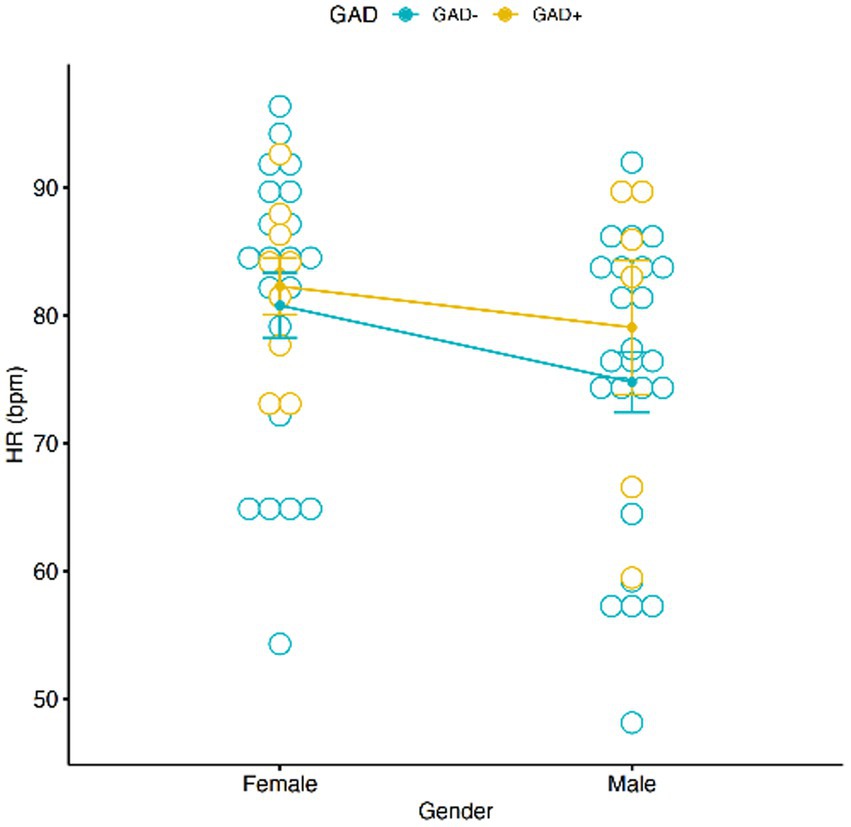
Figure 6. Graphic distribution of HR values according to GAD ± and Gender. No significant interaction was found between Gender, HR and GAD ±.
Discussion
In this study, several interesting issues have been elucidated. Curiously, neither GAD-7 scores nor self-reported anxiety values interact with the physiological condition in a statically significant way, a result possible due to the limited number of subjects participating. This study nonetheless showed some interesting data from an innovative psychological and physiological perspective. The Female gender is associated with a higher HR (although not statistically significant, but useful, given the consistency of the other parameters, to Figure out a global pattern of activation), higher perceived patient relationship anxiety and, a lower HRV. However, the Male gender although being associated with a lower level of self-reported anxiety, showed an equal number of subjects with a level compatible with a moderate Generalized Anxiety Disorder; a comparable number to the Female group. HR was higher in our Female sample confirming the existing literature, however the difference with the Male sample values was not statistically significant as expected. Maybe this can be attributed to a higher level of anxiety in our Male sample in comparison to the general Male population. Our findings also highlight that women show lower vagal activity compared to men, providing an interesting relationship between self-report anxiety and physiological data. This work underlines differences in HRV values based on RMSSD that are novel compared to the current scientific literature (Koenig and Thayer, 2016). Usually there is no difference between RMSSD according to gender and, if any is reported, Females show higher parasympathetic activity. The current scientific literature has showed the association between an increased morning cortisol concentration and stress levels in dentists (Nijakowski et al., 2022). It has been also highlighted the usefulness of salivary tests to evaluate sympathetic activity (Tammayan et al., 2021). Furthermore in tracking stress the efficacy of oximetry have been already showed (Hunasgi et al., 2018), but no information about dentists’ sympathetic activity during sleep have been previously reported. The present paper highlights differences in EDA circadian rhythms. More specifically dentists maintained a similar sympathetic activity across daytime and working time. In contrast with the literature a higher sympathetic activity was found during the night in comparison to the rest of day (Grassi et al., 2010). This could open some interesting perspectives about EDA values during sleep stages and working day values in order to deepen our understanding of circadian rhythms in dentists that refer to be stressed or actually have anxiety issues. The shift of EDA circadian rhythms (if shown to be consistent by future research) could represent a possible biomarker of work-related stress. Future studies will uncover if in dentists there is any association between nocturnal excessive sympathetic activity, sleep stage, quality of sleep, perceived stress and anxiety. Usually the above-mentioned indexes are associated with bad health and impaired mental health (Sano et al., 2015; Zhang et al., 2018). In the Introduction several important studies were elucidated, that showed the relevance of this psychophysiological perspective, so it will be interesting to evaluate the results of this study not solely according to a Gender comparison but also to the reference population according to age. A comparison with the reference population according to HRV, HR [both defined in Umetani et al., (1998)] and EDA, showed that HRV was higher in our sample 64.041 ms (±19.112) in comparison to 43 ms (±19), reported by the general population paired by age. HR was perfectly in line with the expected results: 79 bpm (±10) in the general population in comparison to 78.444 bpm (±11.311), provided by our sample. EDA values cannot be compared to the general population because a wrist-worn EDA general classification is still lacking, but nonetheless the shift in sympathetic night activity, according to EDA, remains valuable. Noteworthy 50% of participants reported a self-Perceived VAS Anxiety ≥7 and 5 over 20 (3F, 2 M) were compatible with a moderate GAD diagnosis (GAD-7 score ≥ 10). This is more than expected, as reported by Spitzer et al. (2006): the disorder has an estimated current prevalence in the general medical practice of 2.8 to 8.5% and in the general population of 1.6 to 5.0% (Leon et al., 1995; Olfson et al., 1997; Roy-Byrne and Wagner, 2004; Kessler et al., 2005). No interactions between gender and EDA were found, nor an interaction between GAD score and EDA value. It is relevant to underline that probably this lack of interaction may be caused by the limited sample. A further limitation of this study is the impossibility of comparison of self-reported anxiety with gender due to inhomogeneous samples. The relevance of a psychological approach in a very demanding profession such as dentistry was highlighted by the high number of professionals with a moderate generalized anxiety disorder. The Female gender correlation with higher heart rate activity (although non statistically significant), lower parasympathetic activity (HRV) and with comparable sympathetic activity to the Male gender, can thus provide a possible vulnerability to excessive stress. This hypothesis can be confirmed by the higher Female self-reported anxiety related to patient approach. However, this also poses some interrogatives about Males’ perceived stress because GAD-7 Males scores were comparable with Females’ ones and there was no statistically significant difference between Male and Female HR values, giving rise to a question: “Do Females exaggerate perceived anxiety or Males underestimate it?.” Studies with higher numbers are needed to disentangle more clearly the relationship between self-reported anxiety, questionnaires, and psychophysiological activity.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Comitato etico della ricerca in psicologia, Dipartimento di Psicologia, Padova. The patients/participants provided their written informed consent to participate in this study.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Acknowledgments
LQ sincerely thanks Giovanni Gentile for support and help during all the procedures. LQ also sincerely thanks Katherine Neville and Dr. Karl Pribram for their blessing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alhalabi, L., Singleton, M. J., Oseni, A. O., Shah, A. J., Zhang, Z.-M., and Soliman, E. Z. (2017). Relation of higher resting heart rate to risk of cardiovascular versus noncardiovascular death. Am. J. Cardiol. 119, 1003–1007. doi: 10.1016/j.amjcard.2016.11.059
Altemus, M., Sarvaiya, N., and Neill, E. C. (2014). Sex differences in anxiety and depression clinical perspectives. Front. Neuroendocrinol. 35, 320–330. doi: 10.1016/j.yfrne.2014.05.004
Andela, C. D., van Haalen, F. M., Ragnarsson, O., Papakokkinou, E., Johannsson, G., Santos, A., et al. (2015). Mechanisms in endocrinology: Cushing’s syndrome causes irreversible effects on the human brain: a systematic review of structural and functional magnetic resonance imaging studies. Eur. J. Endocrinol. 173, R1–R14. doi: 10.1530/EJE-14-1101
Armfield, J. M., and Heaton, L. J. (2013). Management of fear and anxiety in the dental clinic: a review. Aust. Dent. J. 58, 390–407. doi: 10.1111/adj.12118
Cannon, W. B. (1915). Bodily Changes in Pain, Hunger, Fear and Rage: An Account of Recent Researches into the Function of Emotional Excitement. Boston: D Appleton & Company.
Chen, W., Jaques, N., Taylor, S., Sano, A., and Fedor, S. P. R. (2015). Wavelet-based motion artifact removal for electrodermal activity. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2015, 6233–6236. doi: 10.1109/EMBC.2015.7319814.Wavelet-Based
Cooper, C. L., Mallinger, M., and Kahn, R. (1978). Identifying sources of occupational stress among dentists. J. Occup. Psychol. 51, 227–234. doi: 10.1111/j.2044-8325.1978.tb00419.x
Cooper, C. L., Watts, J., Baglioni, A. J., and Kelly, M. (1988). Occupational stress amongst general practice dentists. J. Occup. Psychol. 61, 181–192. doi: 10.1111/j.2044-8325.1988.tb00280.x
Cutright, D. E., Carpenter, W. A., Tsaknis, P. G., and Lyon, T. C. (1977). Survey of blood pressures of 856 dentists. J. Am. Dent. Assoc. 94, 918–919. doi: 10.14219/jada.archive.1977.0078
Davidovich, E., Pessov, Y., Baniel, A., and Ram, D. (2015). Levels of stress among general practitioners, students and specialists in pediatric dentistry during dental treatment. J. Clin. Pediatr. Dent. 39, 419–422. doi: 10.17796/1053-4628-39.5.419
Dickerson, S. S., and Kemeny, M. E. (2004). Acute stressors and cortisol responses: a theoretical integration and synthesis of laboratory research. Psychol. Bull. 130, 355–391. doi: 10.1037/0033-2909.130.3.355
DiMatteo, M. R., Shugars, D. A., and Hays, R. D. (1993). Occupational stress, life stress and mental health among dentists. J. Occup. Organ. Psychol. 66, 153–162. doi: 10.1111/j.2044-8325.1993.tb00524.x
Ernst, G. (2017). Hidden signals-the history and methods of heart rate variability. Front. Public Health 5:265. doi: 10.3389/fpubh.2017.00265
Facco, E., Zanette, G., Favero, L., Bacci, C., Sivolella, S., Cavallin, F., et al. (2011). Toward the validation of visual analogue scale for anxiety. Anesth. Prog. 58, 8–13. doi: 10.2344/0003-3006-58.1.8
Garbarino, M., Lai, M., Tognetti, S., Picard, R., and Bender, D. (2014). Empatica E3 - a Wearable Wireless Multi-Sensor Device for Real-time Computerized Biofeedback and Data Acquisition. International Conference on Wireless Mobile Communication and Healthcare, pp. 39–42.
Grassi, G., Bombelli, M., Seravalle, G., Dell’Oro, R., and Quarti-Trevano, F. (2010). Diurnal blood pressure variation and sympathetic activity. Hypertens. Res. 33, 381–385. doi: 10.1038/hr.2010.26
Hansen, A. L., Johnsen, B. H., and Thayer, J. F. (2009). Relationship between heart rate variability and cognitive function during threat of shock. Anxiety Stress Coping 22, 77–89. doi: 10.1080/10615800802272251
Hunasgi, S., Koneru, A., Rudraraju, A., Manvikar, V., and Vanishree, M. (2018). Stress recognition in dental students using smartphone sensor and a software: a pilot study. J. Oral Maxillofac. Pathol. 22, 314–317. doi: 10.4103/jomfp.JOMFP_168_18
Kessler, R. C., Brandenburg, N., Lane, M., et al. (2005). Rethinking the duration requirement for generalized anxiety disorder: evidence from the national comorbidity survey replication. Psychol. Med. 35, 1073–1082. doi: 10.1017/S0033291705004538
Kessler, R. C., Mcgonagle, K. A., Zhao, S., Nelson, C. B., Hughes, M., Eshleman, S., et al. (1994). Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Arch. Gen. Psychiatry 51, 8–19. doi: 10.1001/archpsyc.1994.03950010008002
Kim, H. G., Cheon, E. J., Bai, D. S., Lee, Y. H., and Koo, B. H. (2018). Stress and heart rate variability: a meta-analysis and review of the literature. Psychiatry Investig. 15, 235–245. doi: 10.30773/pi.2017.08.17
Koenig, J., and Thayer, J. F. (2016). Sex differences in healthy human heart rate variability: a meta-analysis. Neurosci. Biobehav. Rev. 64, 288–310. doi: 10.1016/j.neubiorev.2016.03.007
Leon, A. C., Olfson, M., Broadhead, W. E., Barrett, J. E., Blacklow, R. S., Keller, M. B., et al. (1995). Prevalence of mental disorders in primary care: implications for screening. Arch. Fam. Med. 4, 857–861. doi: 10.1001/archfami.4.10.857
Lu, L., Zhang, J., Xie, Y., Gao, F., Xu, S., Wu, X., et al. (2020). Wearable health devices in health care: narrative systematic review. JMIR Mhealth Uhealth 8:e18907. doi: 10.2196/18907
Mohamed Asif, S., Ibrahim Assiri, K., Mohammed Al Muburak, H., Hamid Baig, F. A., Abdullah Arem, S., Arora, S., et al. (2022). Anxiety and depression among dentists in the Kingdom of Saudi Arabia. Risk Manag Healthc. Policy 15, 497–507. doi: 10.2147/RMHP.S350277
Maslach, C., and Pines, A. (1977). The burn-out syndrome in the day care setting. Child Care Q. 6, 100–113. doi: 10.1007/BF01554696
Mohd Azmi, N. A. S., Juliana, N., Azmani, S., Mohd Effendy, N., Abu, I. F., Mohd Fahmi Teng, N. I., et al. (2021). Cortisol on circadian rhythm and its effect on cardiovascular system. Int. J. Environ. Res. Public Health 18:676. doi: 10.3390/ijerph18020676
Moore, R., and Brødsgaard, I. (2001). Dentists’ perceived stress and its relation to perceptions about anxious patients. Community Dent. Oral Epidemiol. 29, 73–80. doi: 10.1034/j.1600-0528.2001.00011.x
Myers, H. L., and Myers, L. B. (2004). “It’s difficult being a dentist”: stress and health in the general dental practitioner. Br. Dent. J. 197, 89–93. doi: 10.1038/sj.bdj.4811476
Nauman, J., Janszky, I., Vatten, L. J., and Wisløff, U. (2011). Temporal changes in resting heart rate and deaths from ischemic heart disease. JAMA 306, 2579–2587. doi: 10.1001/jama.2011.1826
Nijakowski, K., Gruszczyński, D., Łaganowski, K., Furmańczak, J., Brożek, A., Nowicki, M., et al. (2022). Salivary morning cortisol as a potential predictor for high academic stress level in dental students: a preliminary study. Int. J. Environ. Res. Public Health 19:3132. doi: 10.3390/ijerph19053132
Olfson, M., Fireman, B., Weissman, M. M., Leon, A. C., Sheehan, D. V., Kathol, R. G., et al. (1997). Mental disorders and disability among patients in a primary care group practice. Am. J. Psychiatry 154, 1734–1740. doi: 10.1176/ajp.154.12.1734
Posada-Quintero, H. F., and Chon, K. H. (2020). Innovations in electrodermal activity data collection and signal processing: a systematic review. Sensors (Switzerland). 20:479. doi: 10.3390/s20020479
Rada, R. E., and Johnson-Leong, C. (2004). Stress, burnout, anxiety and depression among dentists. J. Am. Dent. Assoc. 135, 788–794. doi: 10.14219/jada.archive.2004.0279
Resmini, E., Santos, A., and Webb, S. M. (2016). Cortisol excess and the brain. Front. Horm. Res. 46, 74–86. doi: 10.1159/000443868
Richardson, R. V., Batchen, E. J., Denvir, M. A., Gray, G. A., and Chapman, K. E. (2016). Cardiac GR and MR: from development to pathology. Trends Endocrinol. Metab. 27, 35–43. doi: 10.1016/j.tem.2015.10.001
Roy-Byrne, P. P., and Wagner, A. (2004). Primary care perspectives on generalized anxiety disorder. J. Clin. Psychiatry 65, 20–26.
Sano, A., Phillips, A. J., Yu, A. Z., McHill, A. W., Taylor, S., Jaques, N., et al. (2015). Recognizing academic performance, sleep quality, stress level, and mental health using personality traits, wearable sensors and Mobile phones. Int. Conf. Wearable Implant Body Sens Netw. 2015:1109. doi: 10.1109/BSN.2015.7299420
Schuurmans, A. A. T., de Looff, P., Nijhof, K. S., Rosada, C., Scholte, R. H. J., Popma, A., et al. (2020). Validity of the Empatica E4 wristband to measure heart rate variability (HRV) parameters: a comparison to electrocardiography (ECG). J. Med. Syst. 44:190. doi: 10.1007/s10916-020-01648-w
Spitzer, R. L., Kroenke, K., Williams, J. B. W., and Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Intern. Med. 166, 1092–1097. doi: 10.1001/archinte.166.10.1092
Swinson, R. P. (2006). The GAD-7 scale was accurate for diagnosing generalised anxiety disorder. Evid. Based Med. 11:184. doi: 10.1136/ebm.11.6.184
Tammayan, M., Jantaratnotai, N., and Pachimsawat, P. (2021). Differential responses of salivary cortisol, amylase, and chromogranin a to academic stress. PLoS One 16:e0256172. doi: 10.1371/journal.pone.0256172
Thayer, J. F., Åhs, F., Fredrikson, M., Sollers, J. J., and Wager, T. D. (2012). A meta-analysis of heart rate variability and neuroimaging studies: implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 36, 747–756. doi: 10.1016/j.neubiorev.2011.11.009
Umetani, K., Singer, D. H., McCraty, R., and Atkinson, M. (1998). Twenty-four hour time domain heart rate variability and heart rate: relations to age and gender over nine decades. J. Am. Coll. Cardiol. 31, 593–601. doi: 10.1016/s0735-1097(97)00554-8
Verkuil, B., Brosschot, J. F., Tollenaar, M. S., Lane, R. D., and Thayer, J. F. (2016). Prolonged non-metabolic heart rate variability reduction as a physiological marker of psychological stress in daily life. Ann. Behav. Med. 50, 704–714. doi: 10.1007/s12160-016-9795-7
Weber, C. S., Thayer, J. F., Rudat, M., Wirtz, P. H., Zimmermann-Viehoff, F., Thomas, A., et al. (2010). Low vagal tone is associated with impaired post stress recovery of cardiovascular, endocrine, and immune markers. Eur. J. Appl. Physiol. 109, 201–211. doi: 10.1007/s00421-009-1341-x
Woodward, M., Webster, R., Murakami, Y., Barzi, F., Lam, T. H., Fang, X., et al. (2014). The association between resting heart rate, cardiovascular disease and mortality: evidence from 112,680 men and women in 12 cohorts. Eur. J. Prev. Cardiol. 21, 719–726. doi: 10.1177/2047487312452501
Keywords: dentistry, anxiety, stress, gender, psychophysiology
Citation: Queirolo L, Bacci C, Roccon A, Zanette G and Mucignat C (2023) Anxiety in a regular day of work: A 24 hour psychophysiological investigation in young dentists with gender comparison. Front. Psychol. 14:1045974. doi: 10.3389/fpsyg.2023.1045974
Edited by:
Hugo F. Posada-Quintero, University of Connecticut, United StatesReviewed by:
Syed Wali Peeran, Jazan University, Saudi ArabiaRicardo Cartes-Velásquez, Universidad de Concepción School of Medicine, Chile
Copyright © 2023 Queirolo, Bacci, Roccon, Zanette and Mucignat. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luca Queirolo, ✉ bHVjYS5xdWVpcm9sb0B1bmlwZC5pdA==
†These authors have contributed equally to this work
‡ORCID: Luca Queirolo https://orcid.org/0000-0001-7372-1202
Christian Bacci https://orcid.org/0000-0002-6956-6227
Andrea Roccon https://orcid.org/0000-0002-6302-1090
Gastone Zanette https://orcid.org/0000-0003-0110-1017
Carla Mucignat https://orcid.org/0000-0001-5307-0414