 Natalia Angarita-Osorio
Natalia Angarita-Osorio Rosa M. Escorihuela
Rosa M. Escorihuela Toni Cañete
Toni Cañete- 1Department of Psychiatry and Forensic Medicine, Faculty of Medicine, Universitat Autònoma de Barcelona, Bellaterra, Spain
- 2Mental Health Research Group, Hospital del Mar Research Institute, Barcelona, Spain
- 3Centre for Biomedical Research in Mental Health Network (CIBERSAM), Madrid, Spain
- 4Institut de Neurociències, Universitat Autònoma de Barcelona, Bellaterra, Spain
Introduction: In recent decades, researchers have assessed the relationship between mindfulness and personality traits, including neuroticism, a known target in mental health associated with the development of mental health disorders and physical illnesses. The main aim of mindfulness practice is to help individuals develop the ability to regulate and accept their experiences, emotions, and thoughts. Therefore, it could be suggested that mindfulness may be useful in reducing the expression and negative experience of neuroticism. The aim of our review was to assess the relationship between neuroticism and mindfulness.
Methods: We conducted a scoping review of the literature in December 2023, using the databases PubMed and PsycINFO.
Results: Forty-nine studies were included in the review, with four common themes identified: (i) mental health, (ii) cognitive outcomes, (iii) physiological symptoms, and (iv) mindfulness-based interventions. Across most of the studies, mindfulness negatively correlated with neuroticism, supporting the idea that mindfulness may be useful in reducing neuroticism and its negative effects on mental and physical health.
Discussion: While several limitations were identified, the overall results are promising. Future research in this area should focus on overcoming the current limitations to provide a better understanding of the relationship between mindfulness and neuroticism.
1 Introduction
In recent decades, there has been a growing interest and body of literature regarding the impact and relationship of mindfulness with several psychological constructs. Among those, personality traits described as patterns of thoughts, feelings, and behaviors that tend to be stable throughout our lifetime (VandenBos, 2007). These traits have been combined and organized into several models that propose different structures for personality.
Eysenck (1947) proposed a personality trait theory based on two primary dimensions of personality: extraversion (E) and neuroticism (N), to which he later added a third dimension called psychoticism (P, risk-taking, impulsiveness) after studying individuals suffering from mental illness (Eysenck and Eysenck, 1976). In parallel, the “Five Factor Model” (FFM), offers another structure organizing the personality traits into five factors (McCrae and John, 1992): Extraversion (E, sociable, outgoing, openly expressive, oriented to the outer world), Agreeableness (A, cooperative, unselfish, compassionate), Conscientiousness (C, organized, responsible, self-disciplined), Neuroticism (N, emotionally unstable, anxious, prone to experience psychological distress and negative emotions) and Openness to experience (O, imaginative, creative, willing to experience new things) (VandenBos, 2007). Lewis Goldberg contributed to this area by developing the Big Five Factor structure and the scales using different samples and factorial analytic methods and proposed the name “Big Five” (Goldberg, 1992; Boudreaux and Ozer, 2015).
Since then, multiple instruments have been developed, used and revised, such as the NEO Personality Inventory (NEO-PI-R) (Costa and McCrae, 1992; McCrae and Costa, 2010), the Big Five Inventory (BFI) (John et al., 1991), the International Personality Item Pool (IPIP) (Goldberg, 1999)– a repository of over 2000 personality items that are used to develop personality inventories-, the Eysenck Personality Questionnaire (EPQ) (Eysenck and Eysenck, 1975) and the Zuckerman-Kuhlman Personality Questionnaire (ZKPQ) (Zuckerman, 2002).
In addition to its primary role in Eysenck’s theory, and its inclusion as a factor in the Big Five, neuroticism is a substantial target in mental health. It is strongly linked to emotional instability and the experience of psychological distress (e.g., anxiety, hostility, depressed mood) (Costa and McCrae, 1992; Diener et al., 2003). These experiences are correlated with low quality of life and low overall satisfaction. Furthermore, evidence also suggests that neuroticism might be related to susceptibility to the development of mental health disorders (e.g., mood and substance disorders) (Kotov et al., 2010), as well as physical illness (e.g., cardiac problems, immune functioning, irritable bowel syndrome) (Lahey, 2009), and the way people interact with and respond to these and other afflictions. Taken together, this indicates that neuroticism has important health implications and a large impact on daily life (Widiger and Oltmanns, 2017).
Mindfulness, based on Buddhist contemplative practices adapted to the Western population, context, and needs, was introduced in research a few decades ago by Kabat-Zinn. He defined mindfulness as “the awareness that emerges through paying attention on purpose, in the present moment, and nonjudgmentally to the unfolding of experience moment by moment” (Kabat-Zinn, 2003). Kabat-Zinn pioneered the development of the Mindfulness-Based Stress Reduction Program (MBSR) designed to treat stress, anxiety, and pain by developing awareness and acceptance of feelings, thoughts, and body sensations through a combination of mindfulness meditation, body awareness, and therapeutic yoga postures (de Vibe et al., 2012). Since then, scientific interest in this practice has grown, and so has the literature exploring its effect on overall health. According to PubMed, in the past year, the term “mindfulness” appeared in the titles of 3,660 articles.
One of the main goals of mindfulness practice is to develop skills and a different relationship with our emotions, thoughts, and experiences. This practice does not aim to eliminate negative experiences, but rather to learn how to approach them with equanimity, non-judgmentally, and in a more flexible way (Kabat-Zinn, 2003). There are two main elements included in the practice of mindfulness: attention with intentionality and the quality thereof. Mindfulness focus is to bring awareness or attention to the present moment, but with specific attitudes, such as non-judgment, openness, acceptance, and curiosity (Baer et al., 2022). Recognizing what is happening from a place of experiential awareness, without trying to change or control anything.
In this sense, mindfulness can be conceptualized as a trait, or dispositional mindfulness, considering that there are some people who tend to display the skills of being mindfully aware in the daily lives without specific mindfulness training or meditation practice (Hart et al., 2013). However, this way of engaging with everyday life, can be trained and the mindful skills can be developed by means of specific interventions and trainings. In the present study, the term “mindfulness” addresses this inherent capacity, while mindfulness-based interventions (MBIs) will be address as such and refers to structured methods designed to teach and reinforce mindfulness skills. On the other hand, the facets of mindfulness are the specific components or variables that make up the overall mindfulness skill and are assessed by questionnaires.
MBIs are used to cultivate and develop this attitudes. They are 6 or 8-week programs that include mindfulness meditation (MM) and encourage home practice of meditation and other components (e.g., yoga practice). In addition to the MBSR program pioneered by Kabbat-Zin to reduce stress, anxiety, and chronic pain, other MBIs, such as Mindfulness-Based Cognitive Therapy (MBCT), have been studied. MBCT, combines MM with cognitive therapy, was adapted from the MBSR to prevent relapse in depression (Segal et al., 2013). Moreover, mindfulness principles are also included in other therapies including Dialectical Behavior Therapy (DBT), used to treat borderline personality disorder (BPD), which is based on cognitive-behavioral therapy (CBT) and the acceptance of feelings and behaviors (Dimeff and Linehan, 2001), or Acceptance and Commitment Therapy (ACT), aimed at increasing psychological flexibility by means of mindfulness and the acceptance of one’s own feelings and thoughts (Hayes et al., 2006).
As interest in mindfulness, MBIs and their applications has grown, so has the need for instruments to empirically assess it. This has allowed for a better understanding of the psychological processes involved and to determine its relationship with other psychological constructs (Baer et al., 2006). In this regard, some of the instruments currently available and commonly used are (Baer et al., 2022): the Mindful Attention Awareness Scale (MAAS) (Brown and Ryan, 2003), the Five Facet Mindfulness Questionnaire (FFMQ) (Baer et al., 2006), the Kentucky Inventory of Mindfulness Skills (KIMS) (Baer et al., 2004), the Freiburg Mindfulness Inventory (FMI) (Buchheld et al., 2001), and the Cognitive Affective Mindfulness Scale—Revised (CAMS–R) (Hayes and Feldman, 2004). Despite their differences, all these questionnaires assess central facets of mindfulness practice, such as acting with awareness (e.g., fully engaging with the present), observing (e.g., noticing internal and external experiences), describing (e.g., being able to express experiences with words), non-judging (e.g., observing experiences without judging them), and non-reactivity (e.g., observing experiences without reacting to them) (Baer et al., 2022).
Given that the main goal of MBIs is to develop abilities to regulate and accept how we relate to our experiences, emotions, and thoughts -particularly negative ones- it is hypothesized that these interventions could reduce the expression and experience of neuroticism.
Previous studies have shed some light on this claim. Giluk (2009) studied the relationship between mindfulness and the Big Five personality traits and found that neuroticism had the strongest correlation with mindfulness. Neuroticism was also positively associated with worry, avoidance, and rumination, and inversely associated with mindfulness. Higher scores of neuroticism and lower scores with the remaining personality traits were associated with maladaptive emotional regulation strategies (Barańczuk, 2019).
Considering neuroticism is one of the most robust higher-order personality traits associated with negative emotionality, where self-awareness is focused on distress and negative emotions, and risk of mental disorders, and mindfulness is a strategy to develop self-awareness based on equanimity, non-judgmentally, and flexibility, we objective of this review was to analyze and discuss the relationship between neuroticism as a personality trait and mindfulness. We first identified the studies according to these terms, selected those following the eligibility criteria, and then organized and summarized the results. We first describe the studies addressing this relationship in a broad sense, then refer to this relationship in more constricted areas such as mental health (depression, anxiety, stress, post-traumatic stress disorder, or other diseases) and cognitive and psychological variables (inflexibility, hardiness, cognitive reappraisal), and finally address the outcomes of those studies, including mindfulness-based interventions.
2 Methods
2.1 Search strategy
To conduct the present review, we consulted two databases to identify the literature: PubMed and PsycINFO, from inception until December 2023. We used the terms “neuroticism” AND “mindfulness” to identify literature with no restrictions regarding population, date or awareness-based interventions.
Articles for selection were recorded using Rayyan, a web-based data synthesis software program (Ouzzani et al., 2016).
2.2 Eligibility criteria
From the search using the terms “neuroticism” AND “mindfulness” the articles were selected according to the following inclusion criteria: (i) to be in English or Spanish and (ii) to contain primary outcome measures that assessed neuroticism and/or mindfulness using validated instruments (e.g., FFMQ, MAAS, NEO-PI, or BFI). Articles were excluded if they were in other languages, described as protocols, dissertations, or validations of instruments, or if the primary outcomes were different from mindfulness and/or neuroticism. No awareness-based interventions were excluded.
2.3 Method of synthesis
To summarize the results, we opted for a scoping review that allowed us to organize and synthesize the main findings. Following the recommendations of Aveyard (2014) and other published reviews (McVeigh et al., 2021), we analyzed our articles’ main findings, identified the themes that would allow us to answer our research questions, and to summarize the results, outline the relationship between the evidence, and draw conclusions. The scoping review was conducted by two independent reviewers using pretested forms.
3 Results
After the search, 258 articles were identified and saved in Rayyan, and all duplicates were removed, 195 articles (Figure 1). First, titles and abstracts were screened, and 81 articles were excluded for various reasons (e.g., different languages, protocols, and validation of instruments). The remaining 114 were selected for full-text review by one author (information removed for anonymized review) to ensure that all eligibility criteria were met. Discrepancies or doubts about the inclusion of articles were discussed with two authors (information removed for anonymized review), and finally, 49 articles were included in this review. For additional information, see the references listed in Table 1 (main characteristics of the participants) and Tables 2–6 (main characteristics of the studies, including conclusions).
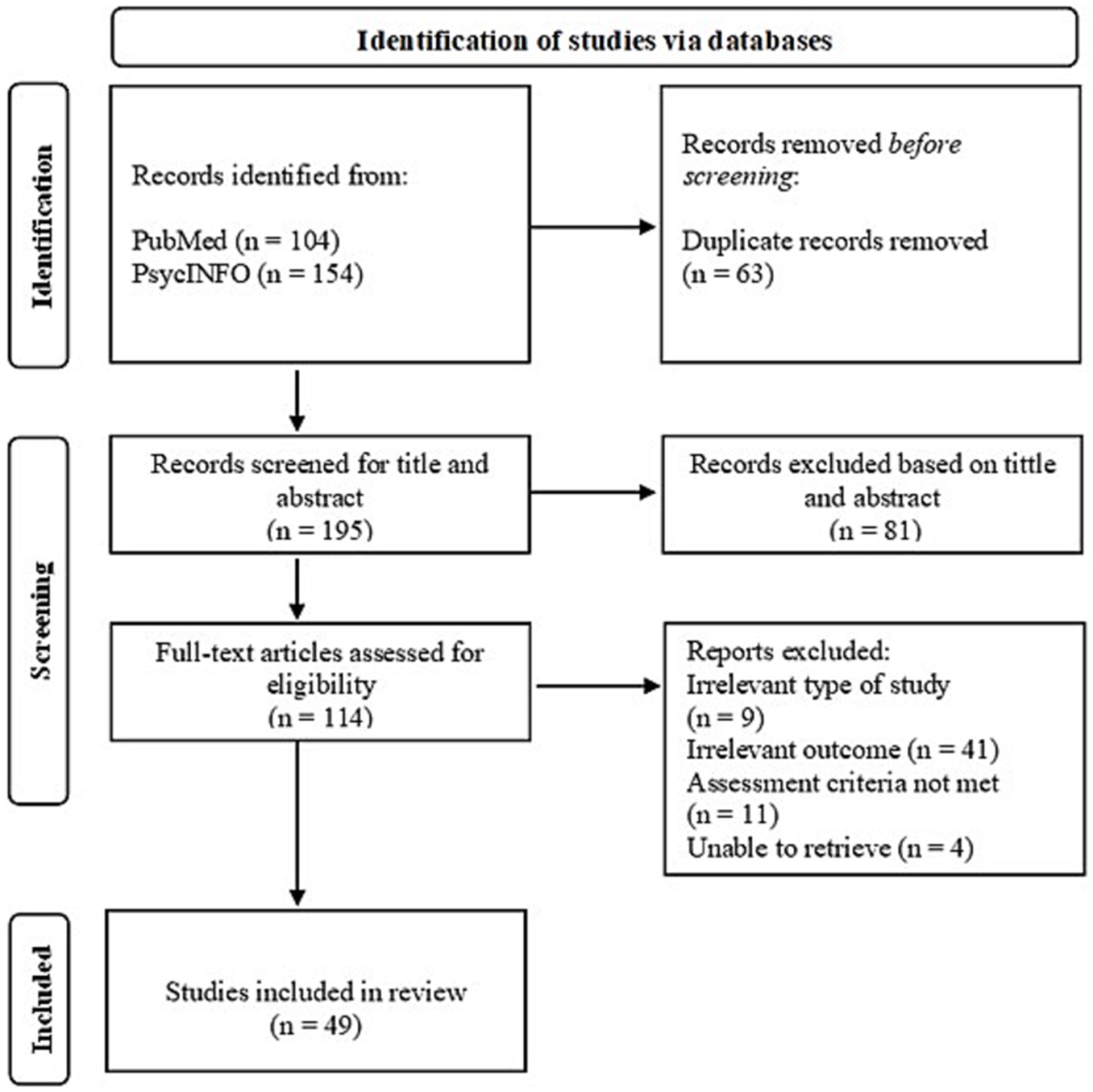
Figure 1. Search strategy flow diagram.
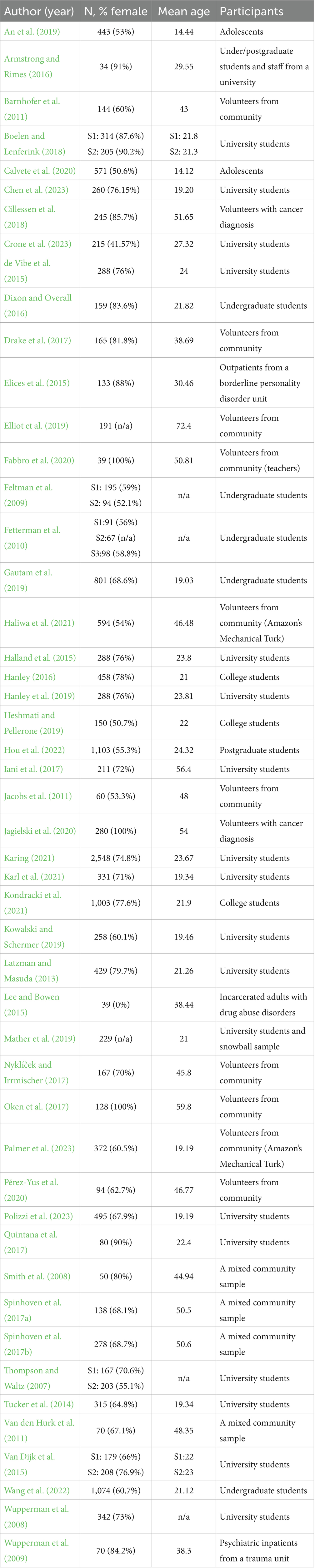
Table 1. Main characteristics of the sample’s studies.

Table 2. Brief description and main findings of the relationship between mindfulness and neuroticism.
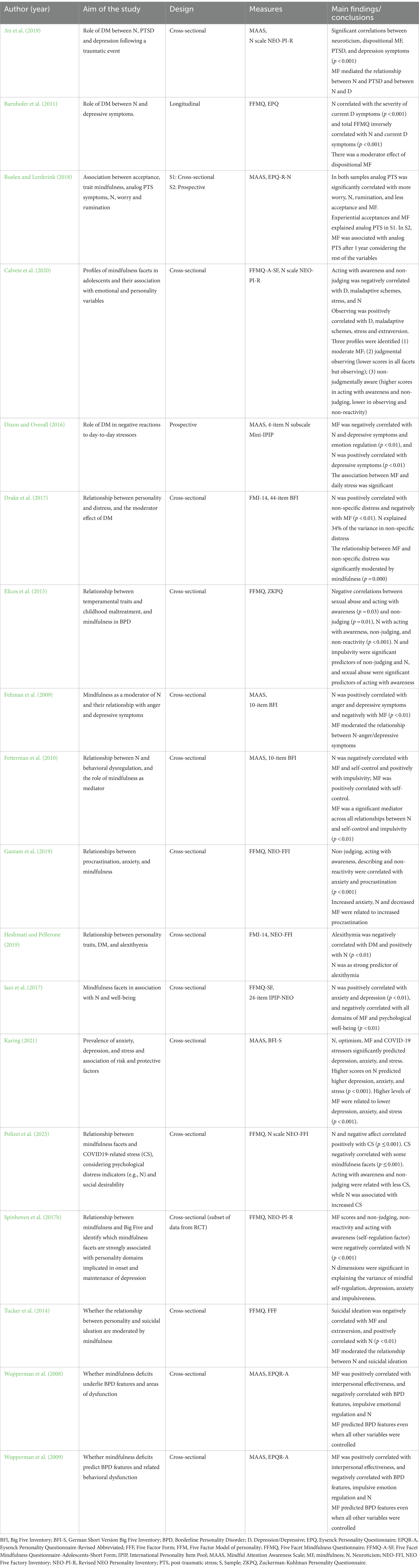
Table 3. Brief description and main findings of mindfulness and neuroticism in relation with mental health.
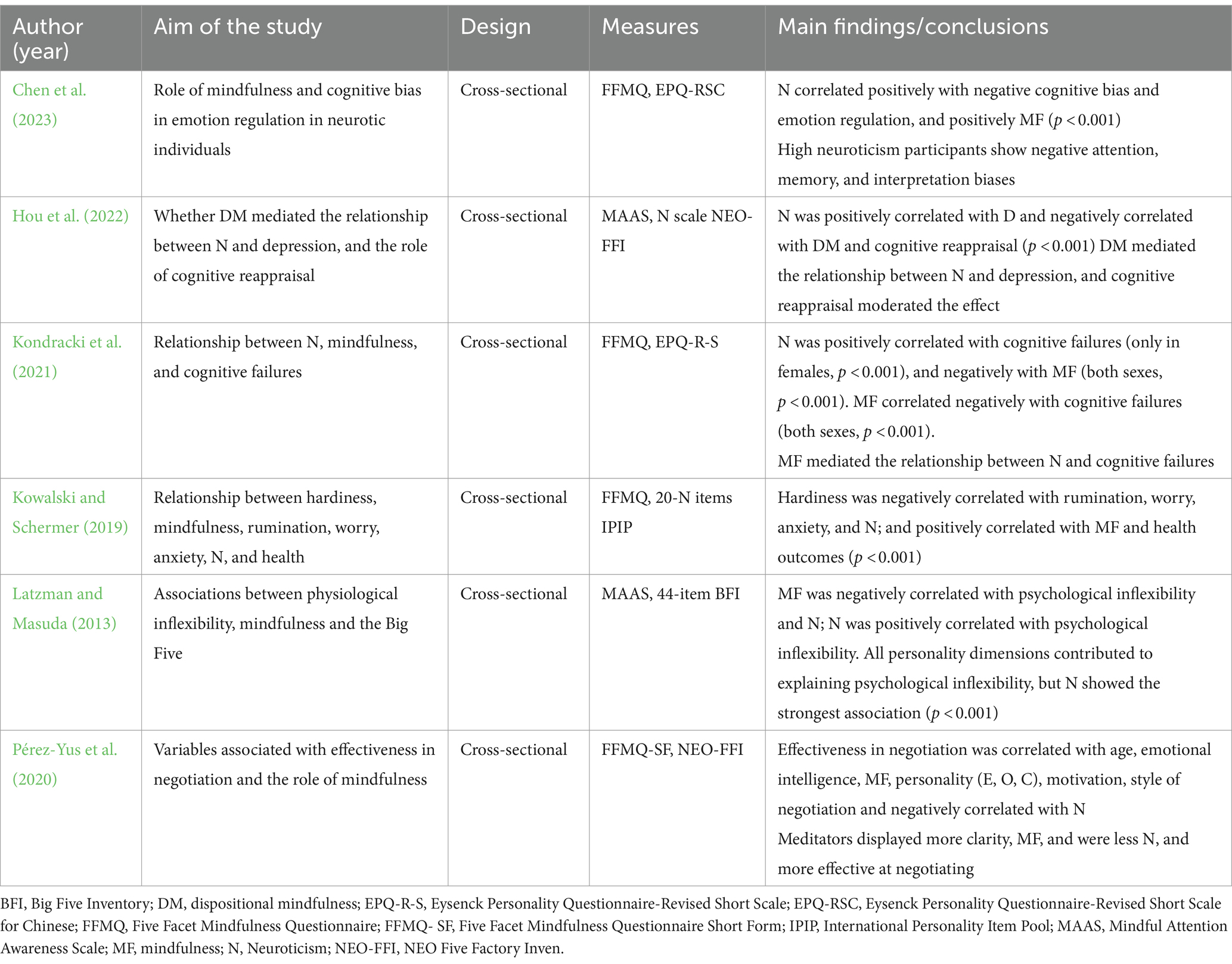
Table 4. Brief description and main findings of mindfulness and neuroticism in relation with cognitive outcomes.
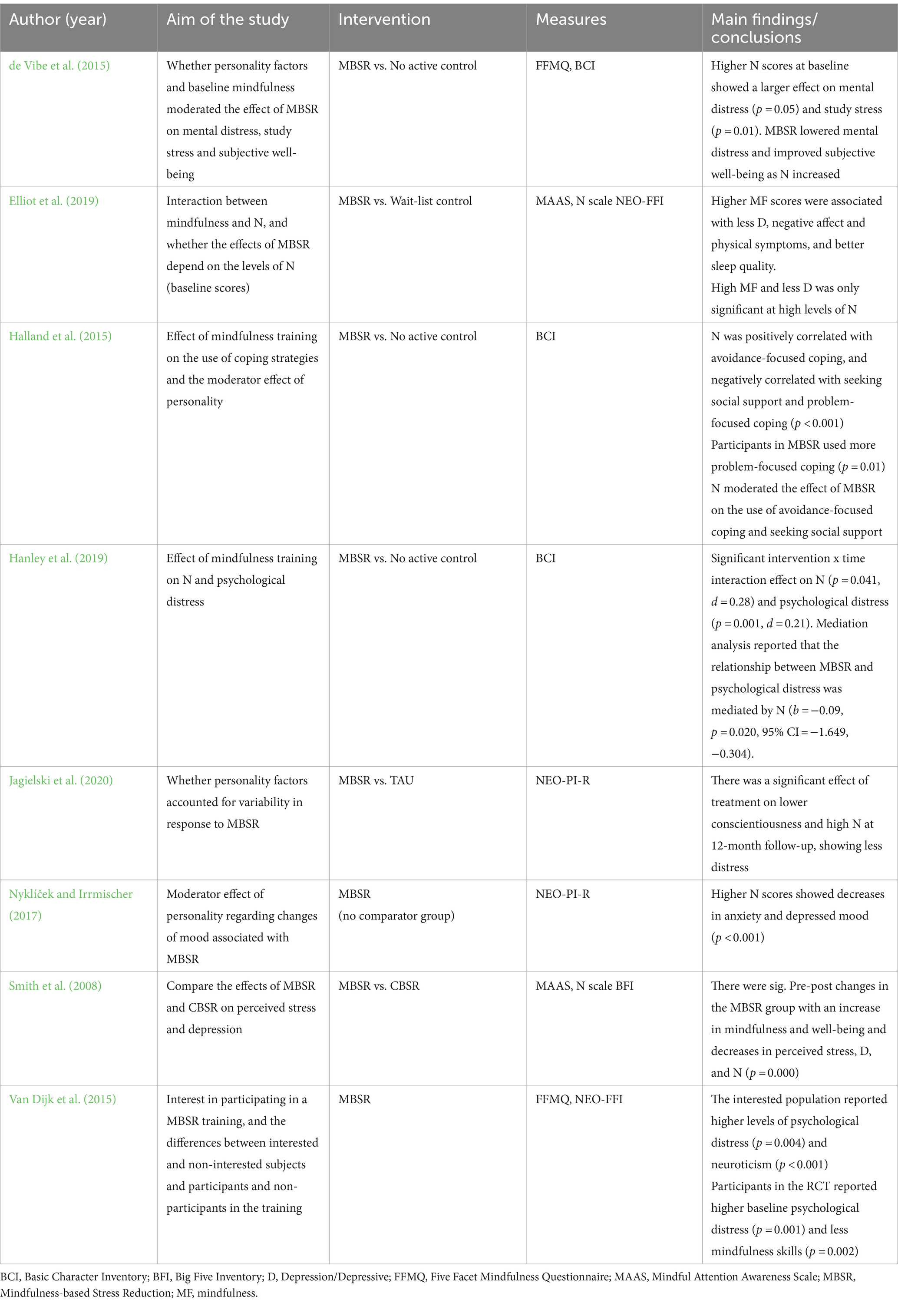
Table 5. Brief description and main findings of studies evaluating MBSR.
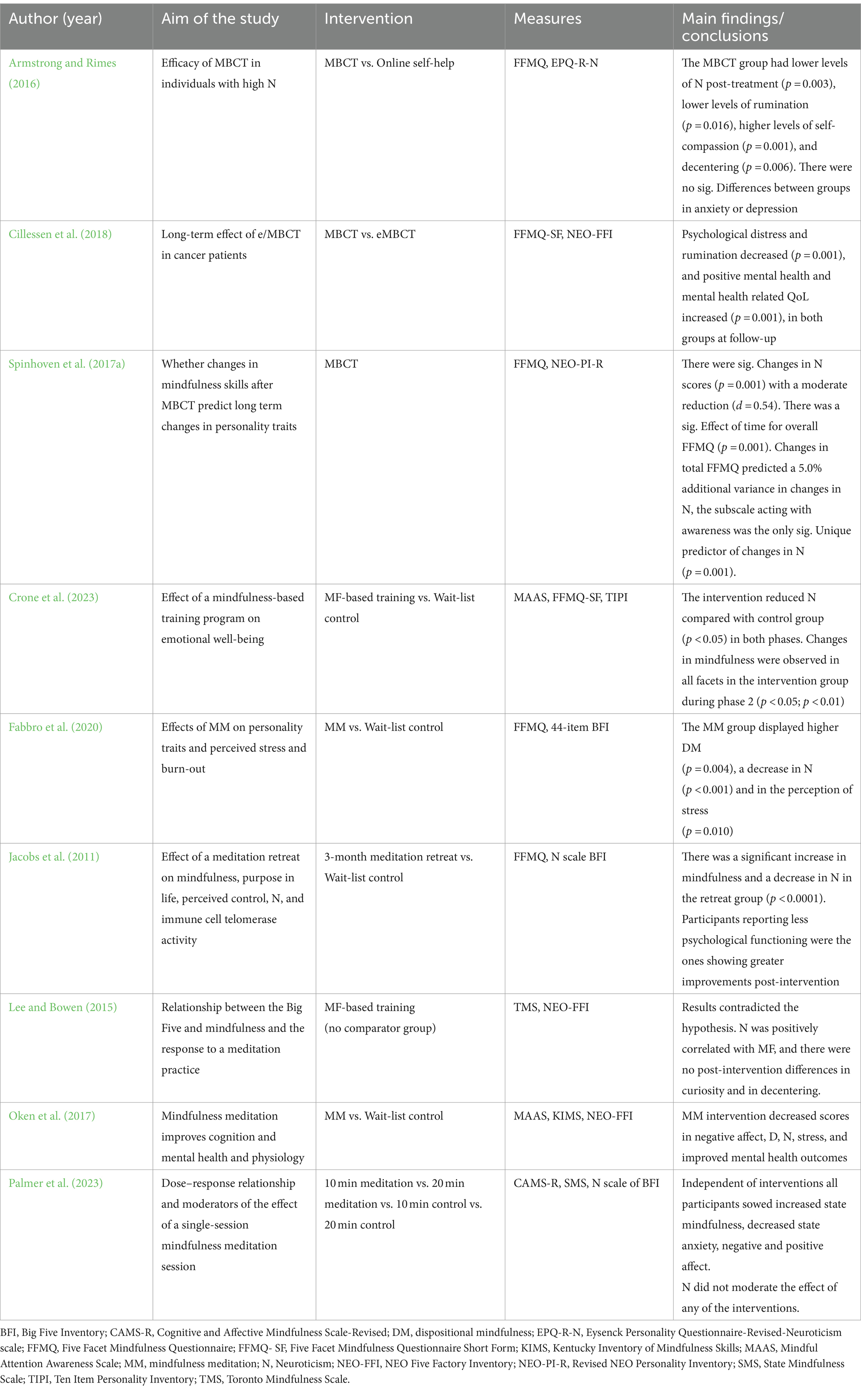
Table 6. Brief description and main findings of the effects of other mindfulness-based interventions.
3.1 Characteristics of the studies included
The 49 studies selected for the present review (see Table 1) took place in different countries (Australia, Canada, China, Iran, Italy, Denmark, Germany, the Netherlands, New Zealand, Norway, Spain, Taiwan, the UK, and the USA), resulting in a total sample drawn from several different cultures. The sample sizes of the studies ranged from 34 to 2,548 participants (n = 17,451), with a mean age of 32.25 years (range from 14.44 to 72.4 years). A percentage of 81.11 of the sample was women, except for one study that included an all-male sample (Lee and Bowen, 2015). The samples comprised students, volunteers from the community, or mixed volunteers from the community with a specific pathology and adolescents. Most of the included studies used a cross-sectional design, while others were randomized controlled trials, longitudinal studies, quasi-experimental studies or other types (the design of each study is indicated in Table 2).
The final 49 studies were grouped and presented over the following sections, starting with the relationship between neuroticism and mindfulness reported in the studies that assessed neuroticism and/or mindfulness using validated instruments. Next, we describe the relationship of these two dimensions and the mindfulness facets with mental health; more specifically with depression, anxiety, posttraumatic stress syndrome and borderline personality disorder. The relationship of mindfulness and neuroticism have been also studied in regard with cognitive impairments; these results are presented in the next section. The last two sections refer to those studies evaluating the effects of Mindfulness-Based Stress Reduction Program (MBSR), and the other mindfulness-based interventions used in the studies included (MBIs, section five).
3.2 Relationship between neuroticism and mindfulness
Although all eight studies (Table 2) used different sets of instruments, similar results reported a significant negative correlation, indicating that high mindfulness was associated with low neuroticism (Quintana et al., 2017). When comparing the neuroticism scores between meditators and non-meditators, even if there were no significant differences between the two groups, more experience on meditation was negatively correlated with neuroticism, and this relationship was mediated by the mindfulness facets “acting with awareness” and “non-judging” (van den Hurk et al., 2011). Accordingly, when assessing neuroticism and mindfulness at 4-time points over a year in a sample of undergraduate students, mindfulness was found to be negatively correlated with neuroticism (Wang et al., 2022).
Mindfulness states, particularly emphasizing facets such as self-awareness (“Acting with Awareness”) and emotional processing (“Non-Judgmental Acceptance”) seem to be linked to negative affect and underscored that personality traits and behavioral inhibition did not affect nor predict changes in emotional affect after the exposure to a negative stimulus. The authors posited that a potential constraint lay in the contextual backdrop of the study, coinciding with the onset of the COVID-19 pandemic. They propose that participants, undergraduate students, may have already experienced elevated initial stress levels, potentially masking the underlying connections between personality traits and negative affect (Karl et al., 2021).
Mather et al. (2019) reported negative correlations of three mindfulness facets, non-judging, non-reactivity, and acting with awareness, with all neuroticism components (anxiety, anger, hostility, depression, impulsiveness, vulnerability, and self-consciousness). Consistently, Hanley (2016) outlined the “self-regulation cluster,” which is composed of self-regulation skills associated with three mindfulness facets (non-judging, non-reactivity and acting with awareness) that are negatively correlated with neuroticism. Another study examining the association of mindfulness facets with specific neuroticism aspects (anxiety, anger, depression, self-consciousness, immoderation, and vulnerability) reported that three mindfulness facets were negatively correlated with anxiety, depression and vulnerability, but not with the other neuroticism components. Moreover, the facets observing and describing showed no relationship with anxiety and depression, which aligns with other work showing no relationship between observing and broad neuroticism (Iani et al., 2017).
Furthermore, an investigation of the relationship between the Five-Factor Model and everyday mindfulness (e.g., being mindful during everyday activities) and mindfulness during meditation (e.g., formal meditation practice) revealed that there were no significant differences between the types of mindfulness (Thompson and Waltz, 2007). Haliwa et al. (2021) assessed mindfulness using multiple questionnaires (FFMQ, CAMS-R, and MAAS) and found that all mindfulness measures were negatively correlated with neuroticism, thus strengthening the evidence for this relationship.
3.3 Mindfulness and neuroticism in relation with mental health
Iani et al. (2017) assessed the dimensions of mindfulness and their relationship with psychological well-being and neuroticism and found that neuroticism had a positive correlation with depression and anxiety, while a negative relationship with all facets of mindfulness (except for the “observe” and “describe” facets) and psychological well-being. In adolescents, acting with awareness and non-judging was negatively correlated with depression, maladaptive schemes, stress, and neuroticism (Calvete et al., 2020). More specifically, the authors identified a profile of adolescents that exhibited the lowest scores in non-judgment and acting with awareness and who experienced higher levels of depressive symptoms, maladaptive schemes, stress, and neuroticism; as a result, their psychobiological adjustment was poorer among older adolescents. Another profile of adolescents displayed higher scores in acting with awareness and non-judging, and lower scores in observing and non-reactivity; as a result, they exhibited better psychobiological adjustment, characterized by fewer maladaptive schemes, less stress, and less neuroticism.
When Gautam et al. (2019) assessed the presence of anxiety and distress, similar results were obtained. Increased anxiety and neuroticism and decreased mindfulness scores were related to increased procrastination among undergraduate students. Furthermore, Drake et al. (2017) found that non-specific psychological distress was positively correlated with neuroticism and a negatively correlated with mindfulness, which predicted the presence of non-specific distress. Likewise, Dixon and Overall (2016) found that university students who were more “mindful” reported less depressed mood scores even on stressful days, and that daily stress seemed to have a greater impact on depressed mood when individuals scored high on neuroticism, depressive symptoms, and emotional regulation difficulties.
Several studies have confirmed a positive correlation between neuroticism and depressive symptoms and a negative correlation between neuroticism and mindfulness (Feltman et al., 2009; Barnhofer et al., 2011). Neuroticism was also a predictor of depressive symptoms in a study of adolescents who had experienced a tornado (An et al., 2019), and a predictor of depression, anxiety, and stress in a sample of university students (Karing, 2021). In contrast, mindfulness predicted an opposite relationship with depression, anxiety, and stress during the first COVID-19 lockdown in a later study (Karing, 2021). Additionally, neuroticism scores assessed 6 years before assessing depressive symptoms correlated with the severity of current depressive symptoms in a longitudinal cohort study (Barnhofer et al., 2011). It should be noted that in this study, the predictive value of neuroticism on depressive scores was significant when participants displayed low and moderate mindfulness scores. Similarly, Feltman et al. (2009) reported that higher levels of depression were present in a sample that displayed higher levels of neuroticism and less mindfulness, while a study assessing more severe depressive symptoms in a sample of university students reported a positive correlation between the appearance of suicidal ideation and neuroticism and a negative correlation between suicidal ideation and mindfulness (Tucker et al., 2014).
In a cross-sectional study of participants with recurrent depression in remission, which assessed the mindfulness dimensions associated with personality domains and implicated in the relapse of depression, Spinhoven et al. (2017a,b) reported that non-judging, non-reactivity, and acting with awareness skills, described as the “self-regulation factor,” correlated with less expression of neuroticism in terms of depression, anxiety, and impulsiveness.
Regarding trauma-related outcomes, neuroticism was a significant predictor of post-traumatic stress disorder (PTSD) in adolescents who had experienced a tornado (An et al., 2019). Boelen and Lenferink (2018) evaluated the association between experiential acceptance, mindfulness and “analog PTS”—understood as post-traumatic stress associated with negative life events (e.g., mental/physical illness of others, relationship break up, serious interpersonal conflict…), but not compliant with formal PTSD criteria—and their relationship with neuroticism in university students. They found positive correlations between neuroticism and analog PTS, worry, and rumination, and a negative correlation with mindfulness.
On the other hand, Polizzi et al. (2023) assessed the impact of a mass traumatic event and the experience of COVID-19-related stress (CS). Their results indicated that neuroticism was a significant factor explaining CS and that certain mindfulness facets, such as acting with awareness and non-judging, may play an important role in reducing or preventing stress responses.
In contrast, Elices et al. (2015), assessed the relationship between mindfulness, neuroticism, and childhood maltreatment in a sample of outpatients from a borderline personality disorder (BPD) unit, and found that neuroticism-anxiety was negatively correlated with acting with awareness, non-judging, and non-reactivity. This negative association indicated that neuroticism and impulsive sensation seeking were predictors of non-judging, and that neuroticism was also predictive of acting with awareness. In the same study, sexual abuse was correlated with mindfulness deficits, with a negative impact on acting with awareness, and difficulties being present-oriented instead of being more judgmental-oriented, which is a characteristic of BPD.
Similarly, Wupperman et al. (2008, 2009) assessed the relationship between mindfulness deficits and BPD features (e.g., difficulties with emotional regulation, interpersonal effectiveness, and impulsivity). First, they evaluated a student sample without BPD and found that mindfulness was positively correlated with interpersonal effectiveness and negatively correlated with impulsivity, emotional regulation, and neuroticism. Subsequently, they evaluated a sample of psychiatric inpatients and found similar results, confirming that mindfulness deficits are predictors of the expression of BPD (Wupperman et al., 2008).
Assessing behavioral regulation, a related outcome, Fetterman et al. (2010), found that in undergraduate students, neuroticism was negatively correlated with behavioral regulation variables such as self-control, and positively correlated with impulsivity, while higher mindfulness predicted less impulsivity and neuroticism, and more self-control. In relation with this, a core component of successful emotional regulation is the ability to identify and describe our feelings, in contrast with the inability to process emotional information and difficulties in emotional regulation which is known as alexithymia. Related to this, Heshmati and Pellerone (2019) found that alexithymia correlated negatively with dispositional mindfulness and positively with neuroticism and that neuroticism predicted the presence of alexithymia. Additional details can be found on Table 3.
3.4 Mindfulness and neuroticism in relation with cognitive outcomes
Latzman and Masuda (2013) evaluated students to study the relationship between mindfulness and psychological inflexibility, understood as a rigid psychological reaction characterized by experiential avoidance and diminished daily function, and associated with depression, anxiety, and general distress. The results indicated that participants who scored higher on neuroticism displayed greater psychological inflexibility, whereas those with higher mindfulness scores displayed less psychological inflexibility.
Kowalski and Schermer (2019) assessed hardiness, characteristic of individuals who remain healthy under stressful conditions. Hardiness is characterized by the belief that one can influence events, commitment to activities, and a tendency to alter the cognitive appraisal of stressful events from negative to positive, viewing them as challenges to be overcome. The authors found that hardiness was negatively correlated with rumination, worry, anxiety, and neuroticism and positively correlated with mindfulness and health outcomes. However, when neuroticism was controlled for the analyses, the relationship between hardiness, rumination, and health was not significant, and the level of significance of the correlations between hardiness, mindfulness, anxiety, and worry was attenuated.
Additionally, Kondracki et al. (2021) reported in that college students that higher neuroticism scores were associated with lower mindfulness and higher everyday cognitive failures. In line with this, Hou et al. (2022), found that neuroticism was positively correlated with depression and negatively with dispositional mindfulness and cognitive reappraisal in postgraduate students. Chen et al. (2023) found that the level of neuroticism exhibited a positive correlation with negative emotion regulation. Negative cognitive bias served as a mediator in the relationship between neuroticism and emotion regulation, while mindfulness played a mediating role in the relationship with negative cognitive bias, forming a sequential connection.
Pérez-Yus et al. (2020) evaluated the role of mindfulness and its association with negotiation effectiveness in an adult sample and found that negotiation effectiveness was positively correlated with age, emotional intelligence, mindfulness, several personality domains (E, O, and C), motivation, and style of negotiation, whereas it was negatively correlated with neuroticism. Furthermore, the results indicated that people who meditated more displayed increased clarity (emotional intelligence), greater mindfulness, less neuroticism, and greater effectiveness in negotiation. Additional information can be found in Table 4.
3.5 Evidence from studies evaluating MBSR
MBSR is the most used intervention. In university samples, the results indicated positive effects; MBSR lowered mental distress and study stress and improved subjective well-being as baseline neuroticism increased (de Vibe et al., 2015). Similarly, Halland et al. (2015) reported that following a MBSR intervention, students used more problem-focused coping, and those displaying higher neuroticism scores reduced avoidance coping and increased seeking social support. Moreover, mindfulness training decreased neuroticism and psychological distress during the 6-year follow-up period, and this decrease was associated with reduced psychological distress at the 6-year follow-up (Hanley et al., 2019). Finally, Van Dijk et al. (2015) assessed the interest in participating in a MBSR training and found that interested participants reported higher levels of psychological distress and neuroticism. Furthermore, those who participated displayed lower baseline mindfulness skills compared to non-participants in the training, which could be explained by sampling bias.
The effects of training were also tested in volunteers from the community, and the results were similar. Nyklíček and Irrmischer (2017) assessed the effect of personality on mood changes after MBSR training and found that neuroticism was associated with benefits3 in the reduction of anxiety and depressed mood. Similarly, Smith et al. (2008) compared MBSR with an intervention based on cognitive behavioral stress reduction and found that those participants in the MBSR group displayed higher scores on mindfulness and well-being, and a reduction in perceived stress, depression, and neuroticism than those in the other group. A similar pattern was reported by Jagielski et al. (2020) in a sample of women with breast cancer; the results after the MBSR training indicated that women displaying low conscientiousness (e.g., being relaxed, adaptable, spontaneous) and high neuroticism, reported less distress at 12-month follow-up.
Finally, Elliot et al. (2019), who reported baseline scores before the intervention—found that higher scores of mindfulness were associated with fewer depressive symptoms, negative affect, physical symptoms, and better sleep quality; however, the association of higher mindfulness with fewer depressive symptoms was only significant when the participants displayed higher levels of neuroticism, and neuroticism did not interact with the rest of the outcomes. Additional details have been summarized in Table 5.
3.6 Effects of other mindfulness-based interventions
Armstrong and Rimes (2016) used MBCT to compare its efficacy with an online self-help intervention in a sample of university students and staff with high neuroticism. Participants in the MBCT group reported significantly lower levels of neuroticism and rumination, as well as higher levels of self-compassion and decentering (the ability to observe thoughts and feelings as passing mental events) than participants in the online self-help group. There were no changes in levels of depression or anxiety. Another study examining the long-term effects of MBCT compared to internet-based MBCT in a sample of distressed cancer patients indicated that less psychological distress, rumination, and neuroticism at baseline predicted less psychological distress at follow-up in both interventions. The intervention also improved the mental health-related quality of life and positive mental health (Cillessen et al., 2018). Finally, Spinhoven et al. (2017b) analyzed whether MBCT predicted long-term changes in personality and found a significant reduction in neuroticism scores. Additionally, improvements in mindfulness skills predicted changes in neuroticism, and acting with awareness was associated with these changes.
Other nonstandard mindfulness-based interventions. The impact of a single session of mindfulness meditation, regardless of its duration, enhanced state mindfulness. Surprisingly, neuroticism does not mediate these effects (Palmer et al., 2023).
Another study explored the effects of adapted mindfulness training on the well-being of graduate students and reported that the intervention caused a significant reduction in neuroticism, while the effect on mindfulness facets was found only in a subsample (Crone et al., 2023).
Participants trained in mindfulness-oriented meditation (MOM) (based on MBSR, sessions included a 30 min discussion followed by 30 min MOM meditation) reported higher mindfulness scores and decreased neuroticism scores and burnout levels vs. participants on a waiting list in an all-female sample of teachers (Fabbro et al., 2020). By contrast, Lee and Bowen (2015) tested a mindfulness-based training program in an all-male sample of incarcerated men receiving drug abuse treatment. The treatment content included the core components of mindfulness, relapse prevention, and a balanced lifestyle. However, contrary to their own hypothesis, the post-intervention results indicated lower levels of curiosity and decentering and revealed an unexpected positive correlation between mindfulness and neuroticism.
Oken et al. (2017) assessed the effects of mindfulness meditation (MM) vs. a waitlist control in a sample of mildly stressed adults. The intervention lasted 6 weeks and was carried out one-on-one, in contrast to the typical group setting. The results indicated no change in cognitive measures, sleep, positive affect, physiological outcomes (e.g., salivary cortisol, health rate), or, surprisingly, mindfulness measures. However, MM improved negative affect, stress, mental health component, and self-efficacy.
Finally, Jacobs et al. (2011) conducted an experiment that compared a 3-month meditation retreat with a waitlist control to test its effects on telomerase activity, stress, and neuroticism. The intervention was intense and was conducted in an isolated retreat setting; it included two daily group-guided meditations followed by a mean of 6 h solitary meditation during the day and had a weekly individual meeting with an experienced practitioner. The authors reported a significant increase in mindfulness, perceived control, and telomerase activity (measured after treatment), and a decrease in neuroticism in the retreat group compared to the waitlist control group. Additionally, participants who reported less favorable psychological functioning at baseline showed greater improvements post-intervention. Complementary information can be found in Table 6.
4 Discussion
Neuroticism, a well-known personality trait with established negative effects on well-being and relationships with several mental, physiological, or cognitive health problems (Lahey, 2009). Meanwhile, the past decade has provided plenty of evidence on beneficial the effects of mindfulness on health-related outcomes (Tomlinson et al., 2017) and mindfulness-based interventions (MBIs) on psychiatric disorders (Goldberg et al., 2018). Our main goal was to review the relationship and the interaction between mindfulness and neuroticism.
4.1 Relationship between neuroticism and mindfulness
Consistent findings across various studies indicate that when neuroticism scores are high, mindfulness scores tend to be low, and vice versa. This relationship has been corroborated across different populations of all ages and in several countries. Neuroticism and mindfulness are related to diverse mental health outcomes. Neuroticism shares core characteristics with anxiety and depressive symptoms (Jylhä and Isometsä, 2006) and is a predictor of mental health symptomatology (Newton-Howes et al., 2015). Studies related to emotional and behavioral regulation and psychological inflexibility, once again common characteristics of neuroticism and core components of several mental health problems, are also supported by previous evidence (Paulus et al., 2016).
Giluk (2009) reported that neuroticism is the personality trait most strongly related with mindfulness. Subsequent studies have identified a common pattern of high scores in facets such as “acting with awareness,” “non-judging,” and “non-reactivity,” which have been identified as the “self-regulation cluster” (Hanley, 2016) or “unbiased awareness” (Elices et al., 2015; Spinhoven et al., 2017a,b; Mather et al., 2019; Calvete et al., 2020). These “clusters” have been linked to improved physical and psychological health and coping strategies (Beaulieu et al., 2022; Zhu et al., 2020). However, the possibility that this negative relationship may in all circumstances cannot be ruled out. Since some authors have reported an unexpected positive correlation between mindfulness and neuroticism, further work needs to be done in larger samples to improve understanding of these relationships, both in broad terms and specifically between the mindfulness dimensions and neuroticism components.
Most characteristics of neuroticism correlate with the expression of, predict, or worsen diverse mental and physical health problems. MBIs have shown that training core components can help alleviate or improve symptoms; if not, they can help people suffering from these conditions to manage them or cope with them more adaptively.
4.2 Impact on mental health outcomes
Additionally, we assessed the impact of MBIs on other health outcomes (e.g., depression, anxiety, cognitive outcomes). Despite the heterogeneity, the results were mainly consistent across the outcomes.
MBIs were useful for improving symptom management and stress-related disease outcomes in different patient populations, suggesting that these benefits can come from increasing stress resilience pathways in the brain and regulating stress reactivity (hypothalamic pituitary adrenal and sympathetic adrenal medullary axis) (Creswell et al., 2019). Both dispositional and trained mindfulness, can improve patient-reported symptoms across different diagnoses. It is becoming clear that the benefit of mindfulness training comes from the acquisition of coping abilities to deal with ailments, including making conscious healthy decisions and reducing habitual reactions (Greeson and Chin, 2019).
Studies have demonstrated that MBIs significantly affect alexithymia, enhancing awareness of emotions, curiosity about inner experiences, and connection with one’s thoughts and feelings (Norman et al., 2019). Evidence, although limited, indicates that MBIs are promising for treating trauma-related outcomes, such as PTSD, helping individuals tolerate their physical and emotional distress and reduce their hyperarousal symptoms (Niles et al., 2018). Similarly, MBI have proven effective in reducing depression and anxiety among individuals diagnosed with anxiety disorders (Sevilla-Llewellyn-Jones et al., 2018). A Meta-Analytic review with 998 participants examined the effects of MBIs on biomarkers in psychiatric illness, results showed low but significant effects on health status related to biomarkers of low-grade inflammation (Sanada et al., 2020).
Recent studies have explored the long-term effects of mindfulness on mental health, revealing outcomes in areas such as depression, anxiety, and stress management. For instance, a study evaluated the -short, −medium and long-term efficacy of a combined mindfulness intervention (face-to-face intervention plus app), a face-to-face mindfulness intervention alone, and a mindfulness app alone, compared with an active control group (communication training) during the COVID-19 pandemic. The results indicated improvements in mindfulness, emotional regulation and attentional skills up to 12 months after the intervention. In contrast, no significant differences were found between the groups on measures of stress or mental health (anxiety or depression) in the long term. But both the intervention groups and the active control group improved in anxiety in the short and medium term. For depression, only a significant time effect was observed4 months after the intervention. In addition, it was observed that greater use of the mindfulness app could negatively affect stress (Karing, 2024). Another study indicates that a short-term MBI and active control group (relaxation training) improved trait mindfulness and psychological well-being compared with an inactive wait-list group. However, no group differences were found on any of the other variables like decentering depression, anxiety, executive attention, and coping style (Josefsson et al., 2014). A systematic review suggests that MBI’s was effective in reducing stress in the short term, but not in the medium or long term, showing a small effect on stress reduction over a 3-month period. Nevertheless, no significant evidence was found for stress reduction from 3 months onwards (Sosa-Cordobés et al., 2022). This indicates that other strategies, such as ongoing booster sessions, are needed to maintain improvements in the long term.
4.3 Impact on cognitive health outcomes
Research supports the benefits of MBIs not only on emotional and behavioral regulation and psychological inflexibility, common features of neuroticism, but also that mindfulness emerges as a significant moderator in the relationship between self-control and psychological symptoms. This suggests that a mindful approach complements self-discipline in improving mental health (Bowlin and Baer, 2012).
In this respect, greater degree of mindful awareness may buffer the effects of psychological inflexibility on distress variables, particularly somatization and anxiety (Masuda et al., 2022). For example, a brief-MBI integrated into a school curriculum enhanced children’s socio-emotional and academic development. Positive changes in dispositional mindfulness led to reductions anxiety and psychological inflexibility. The authors discuss that dispositional mindfulness and emotion regulation work as processes of change that underlie the intervention’s impact (García-Rubio et al., 2023). A longer intervention improved executive functioning measures related to susceptibility to cognitive interference and working memory in high school students (Frank et al., 2021).
Both MBIs and CBT, along with Acceptance and Commitment Therapy (ACT), emphasize that people should focus on the way they relate to their symptoms or thoughts instead of trying to eliminate them, without identifying with them and in a kind manner. They are thus grouped under what are known as third-wave cognitive-behavioral therapies (Hayes, 2004). These combined therapies can help patients observe their thoughts from a more distanced and less reactive perspective, without getting caught up in them. Similarly, accepting thoughts and emotions without judging or trying to change them immediately helps individuals with neuroticism avoid internal struggles against their emotional experiences. Identifying levels of neuroticism and adjusting interventions accordingly—such as allowing them to choose between guided or silent meditation, or different types of practices like walking meditation or mindful yoga - can be beneficial. Introducing mindfulness practices gradually, starting with short sessions and increasing the duration as participants become more comfortable, can make MBIs more effective. Dialectical Behavior Therapy (DBT), the gold-standard treatment for Borderline Personality Disorder (BPD), integrates behavioral and mindfulness practices (focusing on the ability to manage emotions, tolerate distress, and improve interpersonal relationships), putting a particular focus on acceptance (Stiglmayr et al., 2014). Similarly, mindfulness-based cognitive therapy (MBCT) and mindfulness-integrated cognitive behavior therapy (MiCBT) are transdiagnostic approaches that focus on reducing avoidance and addressing interoceptive deficits and emotional reactivity. Accordingly, focusing on shared factors across psychological disorders and using transdiagnostic treatment protocols instead of multiple single disorder protocols can be a more resource-efficient approach for addressing comorbidity (Francis et al., 2024).
A systematic review examined the long-term effects and durability of mindfulness-based interventions (MBCT and MBSR) on mental health and well-being, using mediation analysis methods. Evidence was identified that mindfulness, rumination, and worry are significant mediators of the effects of MBIs on mental health outcomes, supporting the key theoretical premises underlying MBSR and MBCT. These findings suggest that cultivating mindfulness skills leads to understanding and acceptance of one’s own experience (Gu et al., 2015).
4.4 Limitations
Despite all the promising and positive findings, several limitations must be considered, and this review must be interpreted with these limitations in mind. Owing to the design of our review, we did not conduct a strict quality assessment of the studies, but there are some concerns that need to be discussed.
Currently, there is still debate about the conceptual and operational definitions of what “mindfulness” is and is not. MBI’s designed in one practice context may not be applicable in other contexts, because meaning is not transferred between settings. A scoping review identified four themes central to the concept of mindfulness, corresponding to the four domains of mindfulness research: mental health, behavioral change, cognitive neuroscience, and ethical mindfulness. However, operational definitions of mindfulness are not clearly articulated within these domains. Authors suggest greater attention should be given to developing operational definitions specific to each research domain, to avoid differing practices and definitions resulting in varied outcomes and benefits (Phan-Le et al., 2022).
Several methodological concerns were identified despite many of them not being new and having already been addressed (Davidson and Kaszniak, 2015). More than half of the included studies had an observational design, preventing causal inferences. Experimental studies often lacked follow-up assessments, had selection biases, or did not include active control groups. Moreover, most studies relied on self-reported measures, which introduced potential biases (e.g., social desirability and lack of objectivity). Along the same line, the heterogeneity of the instruments might complicate the task of comparing the results reported in the selected studies and once again reduce the generalizability of the findings. Several studies (Lee and Bowen, 2015; Iani et al., 2017; Heshmati and Pellerone, 2019; Kowalski and Schermer, 2019; Calvete et al., 2020) have also reported some concerns regarding the use of mindfulness instruments, as they were not certain that the instruments were assessing their desired outcome or were valid (Latzman and Masuda, 2013). As is the case with the FFMQ which gives a multifaceted view of mindfulness, compared with the MAAS that focus on a more general assessment of mindful attention, this fact may be contributing to inconsistent results (Hanley and Garland, 2017).
Sample characteristics also posed limitations. Participants were mostly young, educated, Caucasian females, limiting the generalizability of the findings. Future research should aim for more diverse samples and consider recruiting more male participants and individuals from various cultural backgrounds in mindfulness research (Bodenlos et al., 2017). It would be helpful to carry out interventions in areas traditionally dominated by men or male-oriented cultures, to recruit more male participants. An example is the study of the effects of an MBI on physiological and psychological criteria in a non-selective sample of police officers, where the results showed that participants with higher neuroticism and openness benefited more, and the effectiveness was greater for those who perceived a favorable social norm toward MBIs (Krick and Felfe, 2020). Furthermore, adapting MBIs for racial and ethnic minoritized communities could potentially make them more relevant and acceptable (Morales and Burnett-Zeigler, 2024). Low adherence to interventions among young people might be improved by incorporating technological supplements to the IMB, making the implementation more attractive and better suited for other study populations (Lucas-Thompson et al., 2020).
We believe it is crucial to focus mindfulness-based interventions on young adulthood (typically defined as mind-20 s), once brain maturation is largely complete. The prefrontal cortex, which plays a key role in emotional regulation and the modulation of personality traits like neuroticism, reaches full development during this period. Neuroticism predisposes individuals to depression by increasing the likelihood of ruminative responses to low mood (Barnhofer et al., 2011). Research indicates that mindfulness training can foster emotional regulation skills, reducing emotional reactivity and rumination, which are hallmark features of neuroticism (Kuehner et al., 2023). Introducing these interventions at this stage of life can be an effective preventive strategy to mitigate the manifestation of neuroticism throughout life.
Therefore, we recommend that mental health policies and professional practices incorporate mindfulness programs into educational and healthcare settings, specifically targeting young adults. This approach can help reduce the negative impact of neuroticism on mental health across the lifespan.
In the general adult population, facilitating the formation of practice groups where participants can share their experiences and support each other can be beneficial for improving adherence and overall well-being. Additionally, sampling methods were a limitation and likely a source of bias, as most studies used convenience samples. In the case of students, participation was compensated with academic credits. When sampling for experimental studies, there was a self-selection concern, as some studies recruited participants from populations that already had an interest in MBI interventions.
Future research should focus on developing high-quality, including randomized controlled trials, long-term follow-ups, recruiting larger and diverse samples, and exploring objective measures, to address these limitations.
5 Conclusion
Despite the limitations, these results can provide some insight and guide future research as well as future practice and policy-making decisions. A population-based study by Cuijpers et al. (2010) assessed the economic costs of neuroticism in a representative sample (N = 5,504) and found that the costs associated with neuroticism exceeded those of common mental disorders. Their results also suggest that there is a need to use interventions that target neuroticism as a cause of psychopathology, and here is where MBIs could serve as a useful intervention to aid in the development of abilities that can help people deal with the difficulties that neuroticism poses.
This evidence supports not only the relationship between neuroticism and mindfulness but also the effectiveness of MBIs in various mental and physical conditions, influencing core components shared with neuroticism. Targeting the development of behavioral and cognitive regulation skills may be particularly helpful in reducing neuroticism and thereby decreasing the risk of developing future affective disorders (Hanley and Garland, 2017).
One important question remains: Can neuroticism, as a personality trait, be changed through intervention? Cuijpers et al. (2010) proposed considering neuroticism as a fundamental component underlying mental disorders. Another question is to what extent mindfulness training can reduce neuroticism, even in adverse situations where past experiences and pain surface? Current literature trends emphasize a transdiagnostic approach to address the shared processes of mental disorders, improving the understanding of their heterogeneity and comorbidities (Dalgleish et al., 2020). A well-known transdiagnostic approach is the Unified Protocol (UP) (Barlow et al., 2017), an emotion-focused cognitive behavioral intervention that aims to target temperamental characteristics, especially neuroticism, by addressing mechanisms such as avoidance of emotional experience. It has shown promising results in the treatment of neuroticism (Sauer-Zavala et al., 2021), though further research is needed.
This review supports the relationship between neuroticism and mindfulness and their impact on mental and cognitive health. Despite the limitations, these findings provide insights for future research and practice. Emphasizing the need for more high-quality experimental studies is crucial, which will capture long-term follow-up studies, randomized controlled trials with larger and more diverse samples would be helpful. As well as the use of objective measures and integration with existing therapeutic frameworks could enhance our understanding and application of mindfulness interventions in addressing neuroticism-related health issues.
In conclusion, the negative correlation between neuroticism and its core components (e.g., negative mood, anxiety, and depression) with mindfulness and their impact on mental health and cognitive responses are evident. Future research should explore the clinical implications of these findings in high-quality experimental studies to further validate and expand upon these promising results.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
NA-O: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. RE: Conceptualization, Funding acquisition, Supervision, Validation, Writing – review & editing. TC: Conceptualization, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by 2021SGR-00806 funded by the Catalan Government. Funding institutions had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgments
NA-O acknowledges the continuous support by CIBER - Consorcio Centro de Investigación Biomédica en Red – (CB/07/09/0010), Instituto de Salud Carlos III, Ministerio de Ciencia e Innovación.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2024.1401969/full#supplementary-material
References
An, Y., Fu, G., Yuan, G., Zhang, Q., and Xu, W. (2019). Dispositional mindfulness mediates the relations between neuroticism and posttraumatic stress disorder and depression in Chinese adolescents after a tornado. Clin. Child Psychol. Psychiatry 24, 482–493. doi: 10.1177/1359104518822672
Armstrong, L., and Rimes, K. A. (2016). Mindfulness-based cognitive therapy for neuroticism (stress vulnerability): a pilot randomized study. Behav. Ther. 47, 287–298. doi: 10.1016/j.beth.2015.12.005
Aveyard, H. (2014). “Doing a literature review in health and social care: a practical guide” in McGraw-Hill education. 3rd ed (London: Open University Press).
Baer, R., Gu, J., and Strauss, C. (2022). “Five facet mindfulness questionnaire (FFMQ) BT - handbook of assessment in mindfulness research” in Handbook of assessment in mindfulness research. eds. O. N. Medvedev, C. U. Krägeloh, R. J. Siegert, and N. N. Singh (Cham: Springer International Publishing), 1–23.
Baer, R. A., Smith, G. T., and Allen, K. B. (2004). Assessment of mindfulness by self-report: the Kentucky inventory of mindfulness skills. Assessment 11, 191–206. doi: 10.1177/1073191104268029
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., and Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment 13, 27–45. doi: 10.1177/1073191105283504
Barańczuk, U. (2019). The five factor model of personality and emotion regulation: a meta-analysis. Pers Individ Dif 139, 217–227. doi: 10.1016/J.PAID.2018.11.025
Barlow, D. H., Farchione, T. J., Bullis, J. R., Gallagher, M. W., Murray-Latin, H., Sauer-Zavala, S., et al. (2017). The unified protocol for Transdiagnostic treatment of emotional disorders compared with diagnosis-specific protocols for anxiety disorders: a randomized clinical trial. JAMA Psychiatry 74, 875–884. doi: 10.1001/JAMAPSYCHIATRY.2017.2164
Barnhofer, T., Duggan, D. S., and Griffith, J. W. (2011). Dispositional mindfulness moderates the relation between neuroticism and depressive symptoms. Pers Individ Dif 51, 958–962. doi: 10.1016/j.paid.2011.07.032
Beaulieu, D. A., Proctor, C. J., Gaudet, D. J., Canales, D., and Best, L. A. (2022). What is the mindful personality? Implications for physical and psychological health. Acta Psychol. 224:103514. doi: 10.1016/J.ACTPSY.2022.103514
Bodenlos, J. S., Strang, K., Gray-Bauer, R., Faherty, A., and Ashdown, B. K. (2017). Male representation in randomized clinical trials of mindfulness-based therapies. Mindfulness 8, 259–265. doi: 10.1007/s12671-016-0646-1
Boelen, P. A., and Lenferink, L. I. M. (2018). Experiential acceptance and trait-mindfulness as predictors of analogue post-traumatic stress. Psychol. Psychother. Theory Res. Pract. 91, 1–14. doi: 10.1111/papt.12138
Boudreaux, M. J., and Ozer, D. J. (2015). Five factor model of personality, assessment of international encyclopedia of the social & behavioral sciences. 2nd ed. Oxford: Elsevier.
Bowlin, S. L., and Baer, R. A. (2012). Relationships between mindfulness, self-control, and psychological functioning. Pers Individ Dif 52, 411–415. doi: 10.1016/J.PAID.2011.10.050
Brown, K. W., and Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 84, 822–848. doi: 10.1037/0022-3514.84.4.822
Buchheld, N., Grossman, P., and Walach, H. (2001). Measuring mindfulness in insight meditation (Vipassana) and meditation-based psychotherapy: the development of the Freiburg mindfulness inventory (FMI). J. Medit. Medit. Res. 1, 11–34.
Calvete, E., Fernández-González, L., Echezarraga, A., and Orue, I. (2020). Dispositional mindfulness profiles in adolescents and their associations with psychological functioning and hypothalamic–pituitary–adrenal axis hormones. J. Youth Adolesc. 49, 1406–1419. doi: 10.1007/s10964-019-01128-6
Chen, L., Liu, X., Weng, X., Huang, M., Weng, Y., Zeng, H., et al. (2023). The emotion regulation mechanism in neurotic individuals: the potential role of mindfulness and cognitive Bias. Int. J. Environ. Res. Public Health 20:896. doi: 10.3390/IJERPH20020896
Cillessen, L., Schellekens, M. P. J., Van de Ven, M. O. M., Donders, A. R. T., Compen, F. R., Bisseling, E. M., et al. (2018). Consolidation and prediction of long-term treatment effect of group and online mindfulness-based cognitive therapy for distressed cancer patients. Acta Oncol. 57, 1293–1302. doi: 10.1080/0284186X.2018.1479071
Costa, P. T., and McCrae, R. R. (1992). Revised NEO personality inventory (NEO-PI-R) and NEO five-factor inventory (NEO-FFI) professional manual. Odessa, FL: Psychological Assessment Resources.
Creswell, J. D., Lindsay, E. K., Villalba,, and Chin, B. (2019). Mindfulness Training and Physical Health: Mechanisms and Outcomes. Psychosomatic Medicine 81, 224–232. doi: 10.1097/PSY.0000000000000675
Crone, W. C., Kesebir, P., Hays, B., Mirgain, S. A., Davidson, R. J., and Hagness, S. C. (2023). Cultivating well-being in engineering graduate students through mindfulness training. PLoS One 18:e0281994. doi: 10.1371/JOURNAL.PONE.0281994
Cuijpers, P., Smit, F., Penninx, B. W. J. H., De Graaf, R., Ten Have, M., and Beekman, A. T. F. (2010). Economic costs of neuroticism: a population-based study. Arch. Gen. Psychiatry 67, 1086–1093. doi: 10.1001/ARCHGENPSYCHIATRY.2010.130
Dalgleish, T., Black, M., Johnston, D., and Bevan, A. (2020). Transdiagnostic approaches to mental health problems: current status and future directions. J. Consult. Clin. Psychol. 88, 179–195. doi: 10.1037/CCP0000482
Davidson, R. J., and Kaszniak, A. W. (2015). Conceptual and methodological issues in research on mindfulness and meditation. Am. Psychol. 70, 581–592. doi: 10.1037/A0039512
de Vibe, M., Bjørndal, A., Tipton, E., Hammerstrøm, K., and Kowalski, K. (2012). Mindfulness based stress reduction (MBSR) for improving health, quality of life, and social functioning in adults. Campbell Syst. Rev. 8, 1–127. doi: 10.4073/CSR.2012.3
de Vibe, M., Solhaug, I., Tyssen, R., Friborg, O., Rosenvinge, J. H., Sørlie, T., et al. (2015). Does personality moderate the effects of mindfulness training for medical and psychology students? Mindfulness 6, 281–289. doi: 10.1007/S12671-013-0258-Y
Diener, E., Oishi, S., and Lucas, R. E. (2003). Personality, culture, and subjective well-being: emotional and cognitive evaluations of life. Annu. Rev. Psychol. 54, 403–425. doi: 10.1146/ANNUREV.PSYCH.54.101601.145056
Dimeff, L., and Linehan, M. M. (2001). Dialectical behavior therapy in a nutshell. Calif. Psychol. 34, 10–13.
Dixon, H. C., and Overall, N. C. (2016). Dispositional mindfulness attenuates the link between daily stress and depressed mood. J. Soc. Clin. Psychol. 35, 255–268. doi: 10.1521/jscp.2016.35.3.255
Drake, M. M., Morris, D. M., and Davis, T. J. (2017). Neuroticism’s susceptibility to distress: moderated with mindfulness. Pers Individ Dif 106, 248–252. doi: 10.1016/j.paid.2016.10.060
Elices, M., Pascual, J. C., Carmona, C., Martín-Blanco, A., Feliu-Soler, A., Ruiz, E., et al. (2015). Exploring the relation between childhood trauma, temperamental traits and mindfulness in borderline personality disorder. BMC Psychiatry 15:180. doi: 10.1186/S12888-015-0573-Z
Elliot, A. J., Gallegos, A. M., Moynihan, J. A., and Chapman, B. P. (2019). Associations of mindfulness with depressive symptoms and well-being in older adults: the moderating role of neuroticism. Aging Ment. Health 23, 455–460. doi: 10.1080/13607863.2017.1423027
Eysenck, H. J. (1947) in Dimensions of personality. ed. K. Paul (London: Kegan Paul, Trench, Trubner & Co.).
Eysenck, H. J., and Eysenck, S. B. G. (1975). Manual of the Eysenck personality questionnaire. London: Hodder and Stoughton.
Eysenck, H. J., and Eysenck, S. B. G. (1976). Psychoticism as a dimension of personality. London: Hodder & Stoughton.
Fabbro, A., Fabbro, F., Capurso, V., D’Antoni, F., and Crescentini, C. (2020). Effects of mindfulness training on school teachers’ self-reported personality traits as well as stress and burnout levels. Percept. Mot. Skills 127, 515–532. doi: 10.1177/0031512520908708
Feltman, R., Robinson, M. D., and Ode, S. (2009). Mindfulness as a moderator of neuroticism–outcome relations: a self-regulation perspective. J. Res. Pers. 43, 953–961. doi: 10.1016/j.jrp.2009.08.009
Fetterman, A. K., Robinson, M. D., Ode, S., and Gordon, K. H. (2010). Neuroticism as a risk factor for behavioral dysregulation: a mindfulness-mediation perspective. J. Soc. Clin. Psychol. 29, 301–321. doi: 10.1521/jscp.2010.29.3.301
Francis, S. E. B., Shawyer, F., Cayoun, B. A., Grabovac, A., and Meadows, G. (2024). Differentiating mindfulness-integrated cognitive behavior therapy and mindfulness-based cognitive therapy clinically: the why, how, and what of evidence-based practice. Front. Psychol. 15:1342592. doi: 10.3389/fpsyg.2024.1342592
Frank, J. L., Broderick, P. C., Oh, Y., Mitra, J., Kohler, K., Schussler, D. L., et al. (2021). The effectiveness of a teacher-delivered mindfulness-based curriculum on adolescent social-emotional and executive functioning. Mindfulness 12, 1234–1251. doi: 10.1007/s12671-021-01594-9
García-Rubio, C., Herrero, M., Luna-Jarillo, T., Albert, J., and Rodríguez-Carvajal, R. (2023). Effectiveness and mechanisms of change of a mindfulness-based intervention on elementary school children: a cluster-randomized control trial. J. Sch. Psychol. 99:101211. doi: 10.1016/j.jsp.2023.04.001
Gautam, A., Polizzi, C. P., and Mattson, R. E. (2019). Mindfulness, procrastination, and anxiety: assessing their interrelationships. Psychol. Conscious. Theory Res. Pract. doi: 10.1037/cns0000209
Giluk, T. L. (2009). Mindfulness, big five personality, and affect: a meta-analysis. Pers Individ Dif 47, 805–811. doi: 10.1016/J.PAID.2009.06.026
Goldberg, L. R. (1992). The development of markers for the big-five factor structure. Psychol. Assess. 4, 26–42. doi: 10.1037/1040-3590.4.1.26
Goldberg, L. R. (1999). “A broad-bandwidth, public domain, personality inventory measuring the lower-level facets of several five-factor models” in Personality psychology in Europe. eds. I. Mervielde, I. Deary, F. Fruyt, and F. Ostendorf (Tilburg: Tilburg University Press), 7–28.
Goldberg, S. B., Tucker, R. P., Greene, P. A., Davidson, R. J., Wampold, B. E., Kearney, D. J., et al. (2018). Mindfulness-based interventions for psychiatric disorders: a systematic review and meta-analysis. Clin. Psychol. Rev. 59, 52–60. doi: 10.1016/J.CPR.2017.10.011
Greeson, J. M., and Chin, G. R. (2019). Mindfulness and physical disease: a concise review. Curr. Opin. Psychol. 28, 204–210. doi: 10.1016/J.COPSYC.2018.12.014
Gu, J., Strauss, C., Bond, R., and Cavanagh, K. (2015). How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clin. Psychol. Rev. 37, 1–12. doi: 10.1016/j.cpr.2015.01.006
Haliwa, I., Wilson, J. M., Spears, S. K., Strough, J., and Shook, N. J. (2021). Exploring facets of the mindful personality: dispositional mindfulness and the big five. Pers Individ Dif 171:110469. doi: 10.1016/j.paid.2020.110469
Halland, E., de Vibe, M., Solhaug, I., Friborg, O., Rosenvinge, J. H., Tyssen, R., et al. (2015). Mindfulness training improves problem-focused coping in psychology and medical students: results from a randomized controlled trial. Coll. Stud. J. 49, 387–398.
Hanley, A. W. (2016). The mindful personality: associations between dispositional mindfulness and the five factor model of personality. Pers Individ Dif 91, 154–158. doi: 10.1016/j.paid.2015.11.054
Hanley, A. W., de Vibe, M., Solhaug, I., Gonzalez-Pons, K., and Garland, E. L. (2019). Mindfulness training reduces neuroticism over a 6-year longitudinal randomized control trial in Norwegian medical and psychology students. J. Res. Pers. 82:103859. doi: 10.1016/j.jrp.2019.103859
Hanley, A. W., and Garland, E. L. (2017). The mindful personality: a meta-analysis from a cybernetic perspective. Mindfulness 8, 1456–1470. doi: 10.1007/s12671-017-0736-8
Hart, R., Ivtzan, I., and Hart, D. (2013). Mind the gap in mindfulness research: a comparative account of the leading schools of thought. Rev. Gen. Psychol. 17, 453–466. doi: 10.1037/a0035212
Hayes, S. C. (2004). Acceptance and commitment therapy, relational frame theory and the third wave of behavioral and cognitive therapies. Behav. Ther. 35, 639–665. doi: 10.1016/S0005-7894(04)80013-3
Hayes, A. M., and Feldman, G. (2004). Clarifying the construct of mindfulness in the context of emotion regulation and the process of change in therapy. Clin. Psychol. Sci. Pract. 11, 255–262. doi: 10.1093/CLIPSY.BPH080
Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., and Lillis, J. (2006). Acceptance and commitment therapy: model, processes and outcomes. Behav. Res. Ther. 44, 1–25. doi: 10.1016/J.BRAT.2005.06.006
Heshmati, R., and Pellerone, M. (2019). The big five personality traits and dispositional mindfulness as predictors of alexithymia in college students. Clin. Neuropsychiatr. 16, 98–106.
Hou, L., Chang, L., Chen, L., Fei, J., and Zhou, R. (2022). Exploring the roles of dispositional mindfulness and cognitive reappraisal in the relationship between neuroticism and depression among postgraduate students in China. Int. J. Public Health 67:1605074. doi: 10.3389/ijph.2022.1605074
Iani, L., Lauriola, M., Cafaro, V., and Didonna, F. (2017). Dimensions of mindfulness and their relations with psychological well-being and neuroticism. Mindfulness 8, 664–676. doi: 10.1007/s12671-016-0645-2
Jacobs, T. L., Epel, E. S., Lin, J., Blackburn, E. H., Wolkowitz, O. M., Bridwell, D. A., et al. (2011). Intensive meditation training, immune cell telomerase activity, and psychological mediators. Psychoneuroendocrinology 36, 664–681. doi: 10.1016/j.psyneuen.2010.09.010
John, O. P., Donahue, E. M., and Kentle, R. L. (1991). The big five inventory – Versions 4a and 54. Berkeley, CA: University of California,Institute of Personality and Social Research.
Jagielski, C. H., Tucker, D. C., Dalton, S. O., Mrug, S., Würtzen, E., and Johansen, C. (2020). Personality as a predictor of well-being in a randomized trial of a mindfulness-based stress reduction of Danish women with breast cancer. Journal of Psychosocial Oncology, 38, 4–19. doi: 10.1080/07347332.2019.1626524
Josefsson, T., Lindwall, M., and Broberg, A. G. (2014). The effects of a short-term mindfulness based intervention on self-reported mindfulness, decentering, executive attention, psychological health, and coping style: examining unique mindfulness effects and mediators. Mindfulness 5, 18–35. doi: 10.1007/s12671-012-0142-1
Jylhä, P., and Isometsä, E. (2006). The relationship of neuroticism and extraversion to symptoms of anxiety and depression in the general population. Depress. Anxiety 23, 281–289. doi: 10.1002/DA.20167
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: past, present, and future. Clin. Psychol. Sci. Pract. 10, 144–156. doi: 10.1093/CLIPSY.BPG016
Karing, C. (2021). Prevalence and predictors of anxiety, depression and stress among university students during the period of the first lockdown in Germany. J Affect Disord Rep 5:100174. doi: 10.1016/j.jadr.2021.100174
Karing, C. (2024). Long-term effects of combined mindfulness intervention and app intervention compared to single interventions during the COVID-19 pandemic: a randomized controlled trial. Front. Psychol. 15:1355757. doi: 10.3389/fpsyg.2024.1355757
Karl, J. A., Fischer, R., and Jose, P. E. (2021). The development of mindfulness in young adults: the relationship of personality, reinforcement sensitivity, and mindfulness. Mindfulness 12, 1103–1114. doi: 10.1007/s12671-020-01576-3
Kondracki, A. J., Riedel, M. C., Crooks, K., Perez, P. V., Flannery, J. S., Laird, A. R., et al. (2021). The link between neuroticism and everyday cognitive failures is mediated by self-reported mindfulness among college students. Psychol. Rep. 126, 265–287. doi: 10.1177/00332941211048467
Kotov, R., Gamez, W., Schmidt, F., and Watson, D. (2010). Linking “big” personality traits to anxiety, depressive, and substance use disorders: a meta-analysis. Psychol. Bull. 136, 768–821. doi: 10.1037/A0020327
Kowalski, C. M., and Schermer, J. A. (2019). Hardiness, perseverative cognition, anxiety, and health-related outcomes: a case for and against psychological hardiness. Psychol. Rep. 122, 2096–2118. doi: 10.1177/0033294118800444
Krick, A., and Felfe, J. (2020). Who benefits from mindfulness? The moderating role of personality and social norms for the effectiveness on psychological and physiological outcomes among police officers. J. Occup. Health Psychol. 25, 99–112. doi: 10.1037/ocp0000159
Kuehner, C., Schricker, I. F., Nayman, S., Reinhard, I., Zamoscik, V., Kirsch, P., et al. (2023). Effects of rumination and mindful self-focus inductions during daily life in patients with remitted depression: An experimental ambulatory assessment study. Behav. Ther. 54, 902–915. doi: 10.1016/j.beth.2023.04.002
Lahey, B. B. (2009). Public health significance of neuroticism. Am. Psychol. 64, 241–256. doi: 10.1037/A0015309
Latzman, R. D., and Masuda, A. (2013). Examining mindfulness and psychological inflexibility within the framework of big five personality. Pers Individ Dif 55, 129–134. doi: 10.1016/j.paid.2013.02.019
Lee, K.-H., and Bowen, S. (2015). Relation between personality traits and mindfulness following mindfulness-based training: a study of incarcerated individuals with drug abuse disorders in Taiwan. Int J Ment Health Addict 13, 413–421. doi: 10.1007/s11469-014-9533-y
Lucas-Thompson, R. G., Rayburn, S., Seiter, N. S., Broderick, P. C., Smyth, J. M., Coatsworth, J. D., et al. (2020). Learning to BREATHE "plus": a multi-modal adaptive supplement to an evidence-based mindfulness intervention for adolescents. Front. Public Health 8:579556. doi: 10.3389/fpubh.2020.579556
Masuda, A., Barile, J. P., Spencer, S. D., Juberg, M., Martin, T. J., and Vibell, J. (2022). Mindful awareness moderates the association between psychological inflexibility and distress variables: a cross-sectional investigation. J. Am. Coll. Health 70, 607–614. doi: 10.1080/07448481.2020.1759607
Mather, P., Ward, T., and Cheston, R. (2019). Presence and personality: a factoral exploration of the relationship between facets of dispositional mindfulness and personality. Couns. Psychol. Rev. 34, 27–40. doi: 10.53841/bpscpr.2019.34.1.27
McCrae, R. R., and Costa, P. T. (2010). NEO inventories professional manual. Lutz, FL: Psychological Assessment Resources.
McCrae, R. R., and John, O. P. (1992). An introduction to the five-factor model and its applications. J. Pers. 60, 175–215. doi: 10.1111/J.1467-6494.1992.TB00970.X
McVeigh, C., Ace, L., Ski, C. F., Carswell, C., Burton, S., Rej, S., et al. (2021). Mindfulness-based interventions for undergraduate nursing students in a university setting: a narrative review. Healthcare 9:1493. doi: 10.3390/HEALTHCARE9111493
Morales, A., and Burnett-Zeigler, I. (2024). A scoping review of culturally adapted mindfulness-based interventions for communities of color. J. Integr. Complement. Med. doi: 10.1089/jicm.2023.0807
Newton-Howes, G., Horwood, J., and Mulder, R. (2015). Personality characteristics in childhood and outcomes in adulthood: findings from a 30 year longitudinal study. Aust. N. Z. J. Psychiatry 49, 377–386. doi: 10.1177/0004867415569796
Niles, B. L., Mori, D. A. L., Polizzi, C., Pless Kaiser, A., Weinstein, E. S., Gershkovich, M., et al. (2018). A systematic review of randomized trials of mind-body interventions for PTSD. J. Clin. Psychol. 74, 1485–1508. doi: 10.1002/JCLP.22634
Norman, H., Marzano, L., Coulson, M., and Oskis, A. (2019). Effects of mindfulness-based interventions on alexithymia: a systematic review. BMJ Ment Health 22, 36–43. doi: 10.1136/EBMENTAL-2018-300029
Nyklíček, I., and Irrmischer, M. (2017). For whom does mindfulness-based stress reduction work? Moderating effects of personality. Mindfulness 8, 1106–1116. doi: 10.1007/S12671-017-0687-0
Oken, B. S., Wahbeh, H., Goodrich, E., Klee, D., Memmott, T., Miller, M., et al. (2017). Meditation in stressed older adults: improvements in self-rated mental health not paralleled by improvements in cognitive function or physiological measures. Mindfulness 8, 627–638. doi: 10.1007/s12671-016-0640-7
Ouzzani, M., Hammady, H., Fedorowicz, Z., and Elmagarmid, A. (2016). Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 5:210. doi: 10.1186/s13643-016-0384-4
Palmer, R., Roos, C., Vafaie, N., and Kober, H. (2023). The effect of ten versus twenty minutes of mindfulness meditation on state mindfulness and affect. Sci. Rep. 13:20646. doi: 10.1038/S41598-023-46578-Y
Paulus, D. J., Vanwoerden, S., Norton, P. J., and Sharp, C. (2016). Emotion dysregulation, psychological inflexibility, and shame as explanatory factors between neuroticism and depression. J. Affect. Disord. 190, 376–385. doi: 10.1016/J.JAD.2015.10.014
Pérez-Yus, M. C., Ayllón-Negrillo, E., Delsignore, G., Magallón-Botaya, R., Aguilar-Latorre, A., and Oliván Blázquez, B. (2020). Variables associated with negotiation effectiveness: the role of mindfulness. Front. Psychol. 11:1214. doi: 10.3389/FPSYG.2020.01214
Phan-Le, N. T., Brennan, L., and Parker, L. (2022). The search for scientific meaning in mindfulness research: insights from a scoping review. PLoS One 17:e0264924. doi: 10.1371/journal.pone.0264924
Polizzi, C. P., Sleight, F. G., Aksen, D. E., McDonald, C. W., and Lynn, S. J. (2023). Mindfulness and COVID-19-related stress: staying present during uncertain times. Mindfulness 14, 1135–1147. doi: 10.1007/S12671-023-02132-5
Quintana, M., González Ordi, H., and Anchía, R. J. (2017). Mindfulness, personalidad y sugestionalibilidad: Estudio correlacional exploratorio = mindfulness, personality and suggestibility: a correlational study. Int. J. Psychol. Psychol. Ther. 17, 49–56.
Sanada, K., Montero-Marin, J., Barceló-Soler, A., Ikuse, D., Ota, M., Hirata, A., et al. (2020). Effects of mindfulness-based interventions on biomarkers and low-grade inflammation in patients with psychiatric disorders: a meta-analytic review. Int. J. Mol. Sci. 21:2484. doi: 10.3390/ijms21072484
Sauer-Zavala, S., Fournier, J. C., Jarvi Steele, S., Woods, B. K., Wang, M., Farchione, T. J., et al. (2021). Does the unified protocol really change neuroticism? Results from a randomized trial. Psychol. Med. 51, 2378–2387. doi: 10.1017/S0033291720000975
Segal, Z. V., Williams, J. M. G., and Teasdale, J. D. (2013). Mindfulness-based cognitive therapy for depression: a new approach to preventing relapse : Guilford Press.
Sevilla-Llewellyn-Jones, J., Santesteban-Echarri, O., Pryor, I., McGorry, P., and Alvarez-Jimenez, M. (2018). Web-based mindfulness interventions for mental health treatment: systematic review and Meta-analysis. JMIR Mental Health 5:e10278. doi: 10.2196/10278
Smith, B. W., Shelley, B. M., Dalen, J., Wiggins, K., Tooley, E., and Bernard, J. (2008). A pilot study comparing the effects of mindfulness-based and cognitive-behavioral stress reduction. J. Altern. Complement. Med. 14, 251–258. doi: 10.1089/acm.2007.0641
Sosa-Cordobés, E., Ramos-Pichardo, J. D., Sánchez-Ramos, J. L., García-Padilla, F. M., Fernández-Martínez, E., and Garrido-Fernández, A. (2022). How effective are mindfulness-based interventions for reducing stress and weight? A systematic review and Meta-analysis. Int. J. Environ. Res. Public Health 20:446. doi: 10.3390/ijerph20010446
Spinhoven, P., Huijbers, M., Ormel, J., and Speckens, A. E. M. (2017b). Improvement of mindfulness skills during mindfulness-based cognitive therapy predicts long-term reductions of neuroticism in persons with recurrent depression in remission. J. Affect. Disord. 213, 112–117. doi: 10.1016/j.jad.2017.02.011
Spinhoven, P., Huijbers, M. J., Zheng, Y., Ormel, J., and Speckens, A. E. M. (2017a). Mindfulness facets and big five personality facets in persons with recurrent depression in remission. Pers Individ Dif 110, 109–114. doi: 10.1016/j.paid.2017.01.045
Stiglmayr, C., Stecher-Mohr, J., Wagner, T., Meibner, J., Spretz, D., Steffens, C., et al. (2014). Effectiveness of dialectic behavioral therapy in routine outpatient care: the Berlin borderline study. Borderl. Pers. Disord. Emot. Dysregul. 1, 1–11. doi: 10.1186/2051-6673-1-20/TABLES/5
Thompson, B. L., and Waltz, J. (2007). Everyday mindfulness and mindfulness meditation: overlapping constructs or not? Pers. Individ. Dif. 43, 1875–1885. doi: 10.1016/j.paid.2007.06.017
Tomlinson, E. R., Yousaf, O., Vittersø, A. D., and Jones, L. (2017, 2017). Dispositional mindfulness and psychological health: a systematic review. Mindfulness 9, 23–43. doi: 10.1007/S12671-017-0762-6
Tucker, R. P., O’Keefe, V. M., Cole, A. B., Rhoades-Kerswill, S., Hollingsworth, D. W., Helle, A. C., et al. (2014). Mindfulness tempers the impact of personality on suicidal ideation. Pers. Individ. Dif. 68, 229–233. doi: 10.1016/j.paid.2014.05.001
van den Hurk, P. A. M., Wingens, T., Giommi, F., Barendregt, H. P., Speckens, A. E. M., and van Schie, H. T. (2011). On the relationship between the practice of mindfulness meditation and personality—an exploratory analysis of the mediating role of mindfulness skills. Mindfulness 2, 194–200. doi: 10.1007/s12671-011-0060-7
Van Dijk, I., Lucassen, P. L. B. J., and Speckens, A. E. M. (2015). Mindfulness training for medical students in their clinical clerkships: two cross-sectional studies exploring interest and participation. BMC Med. Educ. 15:24. doi: 10.1186/S12909-015-0302-9
VandenBos, G. R. (2007). APA dictionary of psychology. American Psychological Association. Available at: https://psycnet.apa.org/record/2006-11044-000 (Accessed January 29, 2023).
Wang, H., Wang, M., Wen, Z., Wang, Y., and Fang, J. (2022). Which comes first? Modeling the longitudinal association between mindfulness and neuroticism. Pers. Individ. Dif. 184:111226. doi: 10.1016/j.paid.2021.111226
Widiger, T. A., and Oltmanns, J. R. (2017). Neuroticism is a fundamental domain of personality with enormous public health implications. World Psychiatry 16, 144–145. doi: 10.1002/WPS.20411
Wupperman, P., Neumann, C. S., and Axelrod, S. R. (2008). Do deficits in mindfulness underlie borderline personality features and core difficulties. J. Personal. Disord. 22, 466–482. doi: 10.1521/pedi.2008.22.5.466
Wupperman, P., Neumann, C. S., Whitman, J. B., and Axelrod, S. R. (2009). The role of mindfulness in borderline personality disorder features. J. Nerv. Ment. Dis. 197, 766–771. doi: 10.1097/NMD.0b013e3181b97343
Zhu, L., Wang, J., and Schroevers, M. J. (2020). Looking beyond the value of individual facets of mindfulness: a person-centered examination of mindfulness. Mindfulness 11, 2349–2359. doi: 10.1007/s12671-020-01452-0
Keywords: mindfulness, neuroticism, scoping review, personality traits, mindfulness-based interventions
Citation: Angarita-Osorio N, Escorihuela RM and Cañete T (2024) The relationship between neuroticism as a personality trait and mindfulness skills: a scoping review. Front. Psychol. 15:1401969. doi: 10.3389/fpsyg.2024.1401969
Edited by:
Adelinda Araujo Candeias, University of Evora, PortugalReviewed by:
Maria Da Glória Salazar D’Eça Costa Franco, University of Madeira, PortugalFerda Alper Ay, Cumhuriyet University, Türkiye
Copyright © 2024 Angarita-Osorio, Escorihuela and Cañete. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Toni Cañete, YW50b25pLmNhbmV0ZUB1YWIuY2F0