 Jingtao Gui
Jingtao Gui Kaiwen Liang
Kaiwen Liang Yahui Yang
Yahui Yang Lian Du
Lian Du- 1Department of Psychiatry, The First Affiliated Hospital of Chongqing Medical University, Chongqing, China
- 2Gele Mountain Hospital of Chongqing Mental Health Center, Chongqing, China
- 3Health Management Center, The First Affiliated Hospital of Chongqing Medical University, Chongqing, China
- 4Key Laboratory of Major Brain Disease and Aging Research (Ministry of Education), Chongqing Medical University, Chongqing, China
Background: Social support is a critical factor in maintaining the mental health of healthcare workers in high-pressure occupational settings. However, few studies have systematically explored the different types of social support and their influencing factors. This study aims to investigate the current status of social support for healthcare workers under high pressure, along with the related protective and risk factors.
Methods: This cross-sectional study collected data through an online questionnaire involving 625 doctors and nurses from the First Affiliated Hospital of Chongqing Medical University. The Social Support Rating Scale (SSRS) was used to assess levels of social support, including objective support, subjective support, and support utilization. Data analysis was conducted using SPSS 26.0, employing univariate and linear regression analyses to examine gender differences and the impact of various factors on social support.
Results: The study found that the total social support score was increased by factors such as family cohesion, living with others, older age, and professional identity (with doctors achieving higher scores than nurses), while insecure attachment and being an only child reduced the total social support score.
Conclusion: This study reveals the multidimensional impact of various factors on social support for healthcare workers in high-pressure occupational settings. These findings provide a basis for promoting individual mental health and also highlights the need to pay more attention to the mental health of those healthcare workers with poor interpersonal relationships, younger individuals, and nurses in high-pressure environments.
Introduction
The importance of social support becomes increasingly evident when addressing psychological stress and the unique challenges faced by healthcare workers in high-pressure occupational settings. Social support can be categorized into two primary types: objective support, which refers to tangible or actual assistance, and subjective support, which pertains to emotional or psychological support experienced by individuals. Additionally, the capacity of individuals to utilize social support should also be considered (Xiao, 1999). Social support is widely recognized as a protective factor for mitigating psychological distress and promoting mental well-being.
The buffering model, first proposed by Cobb (1976), explains how social support acts as a barrier to mitigate the stress experienced by individuals. This model suggests that individuals with robust social support networks feel less affected by stress on their health and well-being due to the shielding or “buffering” effects of social support, which includes various forms such as informational support, recognition, emotional support, and practical assistance (Cobb, 1976; Cohen and McKay, 1984). Essentially, social support derived from interpersonal relationships, particularly family relationships, helps alleviate stress levels, which are directly related to an individual’s quality of life and mental health status, such as depression. Ortiz-Calvo et al. (2022) found a negative correlation between resilience, self-perceived social support, and mental health problems after controlling for potential confounding factors. Similarly, Schug et al. (2021) demonstrated that higher levels of social support and an optimistic attitude are associated with lower symptoms of depression and generalized anxiety.
Healthcare workers in high-pressure occupational settings, such as those in China, experience significant psychological stress due to the demanding nature of their roles, which often encompass the simultaneous responsibilities of clinical practice, research, and teaching (Wu et al., 2010; Zhang et al., 2020). In addition to routine pressures, healthcare workers often face crisis events such as public health emergencies (Liu et al., 2020), medical disputes (Sun et al., 2017), and other unforeseen challenges, all of which can significantly impact their mental health and overall well-being (Wu et al., 2010; Zhang et al., 2020). However, it has also been observed that not all healthcare workers develop psychological problems under such circumstances (Alonso et al., 2021; Saragih et al., 2021; Sun et al., 2017; Zhang et al., 2020). The varying outcomes are thought to be possibly related to the significant mediating role of social support (Dong et al., 2022; Hutten et al., 2021).
Despite the recognized importance of social support, previous studies have not systematically investigated the different types of social support, as well as the influencing factors related to various forms of social support (Carter et al., 2023; Khoury et al., 2021). Therefore, this study explored the social support systems of healthcare workers in such environments and examined the protective and risk factors associated with these systems. The findings aim to provide valuable insights for future mental health initiatives designed to support healthcare workers.
Methods
Participants and methods
This study utilized a cross-sectional research design to investigate healthcare workers in Chongqing. Data were collected via the “Wenjuanxing” platform1 from December 12 to December 30, 2022. This platform enabled us to collect data efficiently from geographically dispersed participants. The initial questionnaire draft was developed based on preliminary studies and expert suggestions from psychiatry professionals. Feedback from healthcare professionals was incorporated to refine the language and content, resulting in the final version.
The survey link and data collection forms were distributed in QR code format across various WeChat workgroups at the First Affiliated Hospital of Chongqing Medical University (CQMU), targeting doctors, nurses, clinical staff, and medical students. However, the study included only data from doctors and nurses, excluding responses from medical students and administrative personnel. Participation was voluntary, with the survey’s first page clearly outlining the study’s background and objectives, emphasizing anonymity and confidentiality. Participants were required to provide informed consent to proceed with the questionnaire, ensuring voluntariness and independence. The survey was programmed to allow only one submission per participant to ensure data accuracy. This study adhered to ethical research guidelines and was approved by the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University (K2023-177).
Questionnaires
Social Support Rating Scale (SSRS)
The Xiao Shuiyuan Social Support Scale (SSRS) was used to assess participants’ social support status. This scale is widely utilized in domestic settings and possesses high reliability and validity. It consists of three dimensions: objective support, subjective support, and support utilization, including 10 items with scores ranging from 0 to 66. Objective support refers to the actual support received in life, subjective support refers to perceived support and satisfaction, and support utilization reflects the individual’s ability to effectively utilize support when needed. Higher scores indicate greater social support.
Chinese Family Adaptability and Cohesion Evaluation Scale (FACES II-CV)
The Chinese version of the Family Adaptability and Cohesion Evaluation Scale, Second Edition (FACES II-CV) (Fei, 1991) was utilized to evaluate family functioning. This scale measures family communication, interaction, and emotional connection, as well as the ability to cope with changes through two dimensions: family cohesion and adaptability. Cohesion reflects the emotional connection and support among family members, and adaptability refers to the family’s flexibility and coping abilities in the face of stress and change.
Adult Attachment Scale (AAS)
This study utilized the Revised Adult Attachment Scale (RAAS) developed by Collins and Read (1996). Previous research has demonstrated that this scale exhibits good reliability and validity when applied in China (Wu et al., 2004). The scale consists of 18 items rated on a 5-point Likert scale, ranging from 1 (Not at all characteristic of me) to 5 (Extremely characteristic of me), and is divided into three subscales: Anxiety, Comfort with Closeness, and Comfort with Depending on Others. To compare attachment profiles, participants were categorized into their respective attachment styles (secure, preoccupied, dismissing, fearful) based on whether their scores on the dimensions of attachment-related anxiety and avoidance were above or below the scale’s midpoint. This study classified preoccupation, avoidance, and fear patterns as insecure attachment patterns, as each individual’s attachment model was either secure or insecure, and this classification was incorporated into the statistical analysis.
Other questionnaires
A series of questionnaires were utilized to collect comprehensive data on participants’ health and well-being, with detailed descriptions provided in our previously published articles (Liang et al., 2024).
Basic information and mental health status
A self-designed questionnaire was deployed to collect participants’ demographic information, including age, gender and educational background, and to assess their mental health status.
Sleep evaluation
Selected items from the Hamilton Depression Rating Scale (HAMD-24) (Hamilton, 1967) were used to assess participants’ sleep quality.
Visual Analogue Scale (VAS)
This tool evaluated participants’ emotional state, physical health, and perceived stress levels on a scale from 0 to 10.
Assessment of perceived stress and psychosomatic health
The perceived stress of healthcare workers was assessed using the Visual Analog Scale (VAS). Scores were recorded, and a threshold score of greater than 8 was employed as a criterion to indicate severe stress.
Assessment of general psychological health
This evaluation categorized participants’ psychosomatic distress levels based on their reported emotional, somatic, and sleep-related issues.
Data analysis
Data analysis was conducted by IBM SPSS 26.0 statistical software. Continuous variables were expressed as means ± standard deviations (M ± SD) and compared using two sample t-test or one-way analysis of variance. Categorical variables were expressed as frequencies (percentage) [n (%)] and compared using non-parametric tests. A p-value of less than 0.05 was deemed statistically significant. In this study, linear regression analysis was used to explore the impact of various factors on social support, with a p-value of less than 0.05 also considered statistically significant.
Results
Gender differences among healthcare workers
In this study, 625 healthcare professionals participated, with three questionnaires excluded due to irregularities in completion, resulting in a valid questionnaire rate of 99.5%. Participants included 378 doctors and 244 nurses, with an average age of 38.97 years (SD 10.03), ranging from 18 to 75 years. In terms of gender distribution, 28% were male (174 individuals) and 72% were female (448 individuals). Most participants held a bachelor’s degree or higher (84.7%) and primarily originated from nuclear family backgrounds (93.2%).
The comparative analysis revealed significant gender-related disparities across several statistical indicators. Profound differences were observed in profession, age, permanent address, and educational background between genders, achieving high statistical significance (p < 0.001). Additionally, gender differences in household income levels, perceived stress scores, and emotional state were statistically significant, with p-values of 0.006, 0.003, and 0.002, respectively. Males reported higher perceived stress scores and a greater incidence of abnormal emotional state than females. However, gender differences in social support were not statistically significant (Table 1).
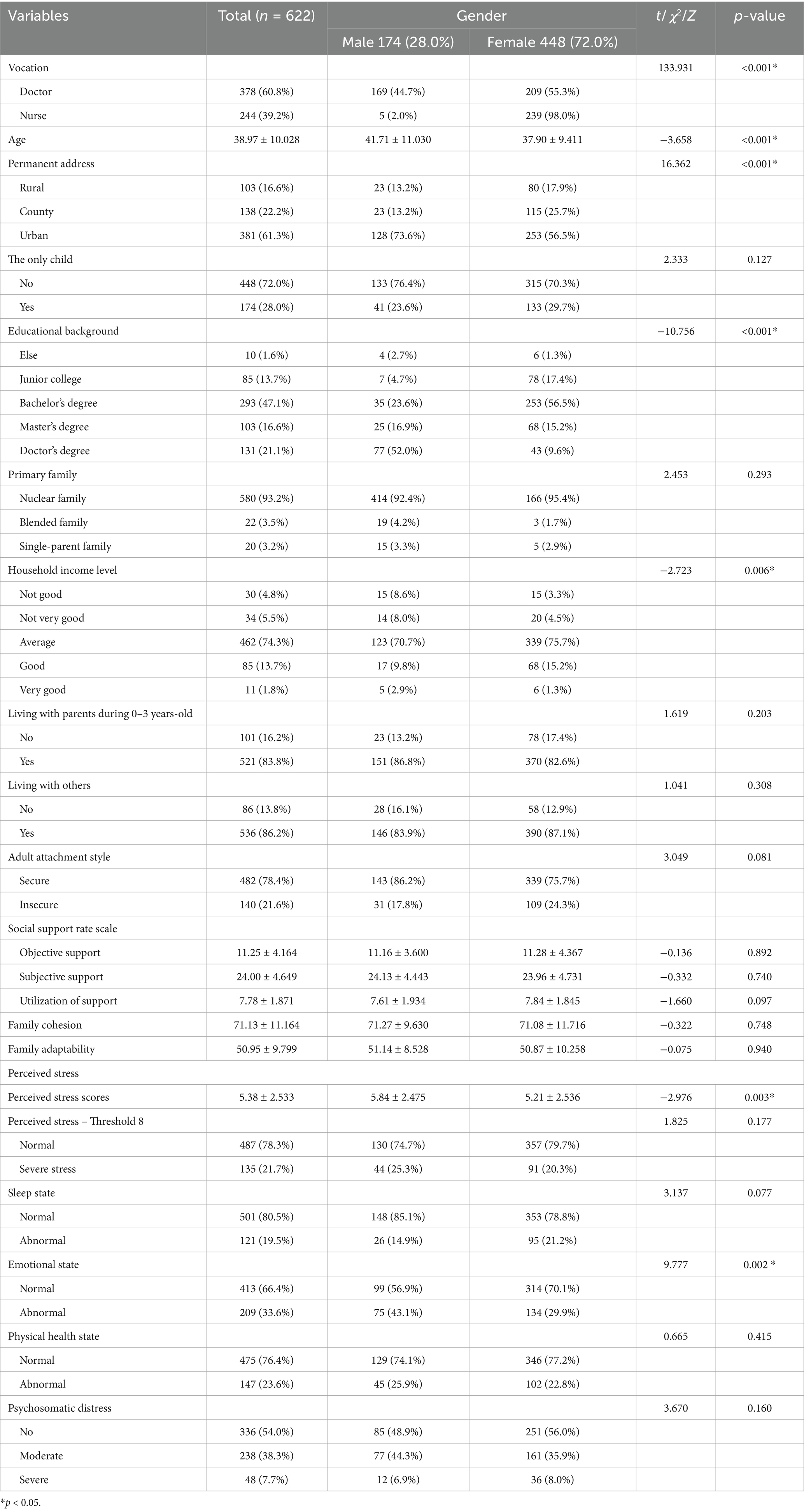
Table 1. Gender differences in demographic and psychometric characteristics of healthcare workers.
Univariate analysis of social support
A comparative analysis was conducted to assess the impact of various independent variables on social support. Tables 2, 3 indicated significant differences in the total social support score concerning only-child status, primary family, household income level, living with others, attachment style, perceived stress, sleep state, emotional state, psychosomatic distress, age, family cohesion, and family adaptability (p < 0.05).
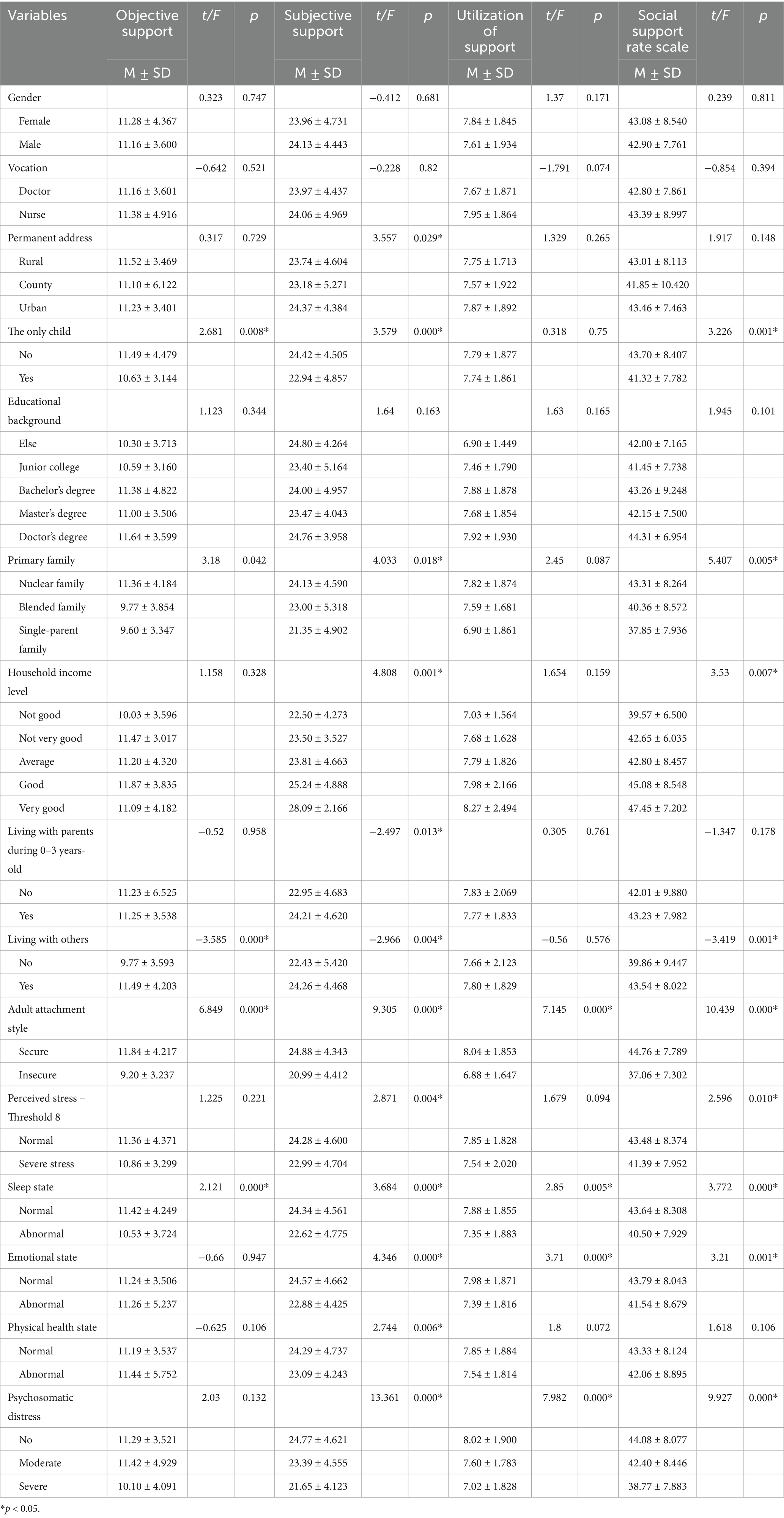
Table 2. Univariate analysis of social support in healthcare workers.
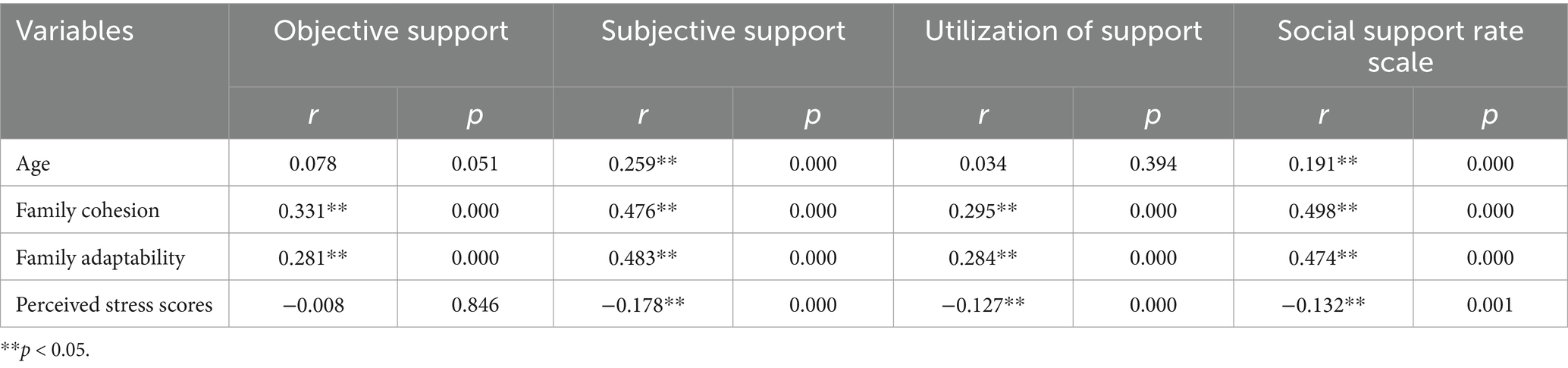
Table 3. Univariate analysis of social support in healthcare workers (continuous variables).
For objective support, significant differences were observed in variables such as only-child status, primary family, living with others, attachment style, sleep state, family cohesion, and family adaptability (p < 0.05).
Regarding subjective support, factors such as permanent address, only-child status, primary family, household income level, living with parents between ages 0–3, living with others, attachment style, perceived stress, sleep state, emotional state, physical health state, psychosomatic distress, age, family cohesion, family adaptability, and perceived stress exhibited statistical differences (p < 0.05).
In terms of support utilization, significant differences were identified in variables such as attachment style, sleep state, emotional state, psychosomatic distress, family cohesion, family adaptability, and perceived stress (p < 0.05) (Tables 2, 3).
Regression analysis of social support
Total social support score
A linear regression analysis was performed to evaluate comprehensively the variables associated with social support, constructing a regression model. The R-squared value was 0.358, indicating that the model accounted for 35.8% of the variance in the data. In this model, higher family cohesion, living with others, older age, and doctor status (as opposed to a nurse) positively increased the level of social support. Conversely, insecure attachment styles and only-child status decreased social support levels (Tables 4, 5, Model 1).
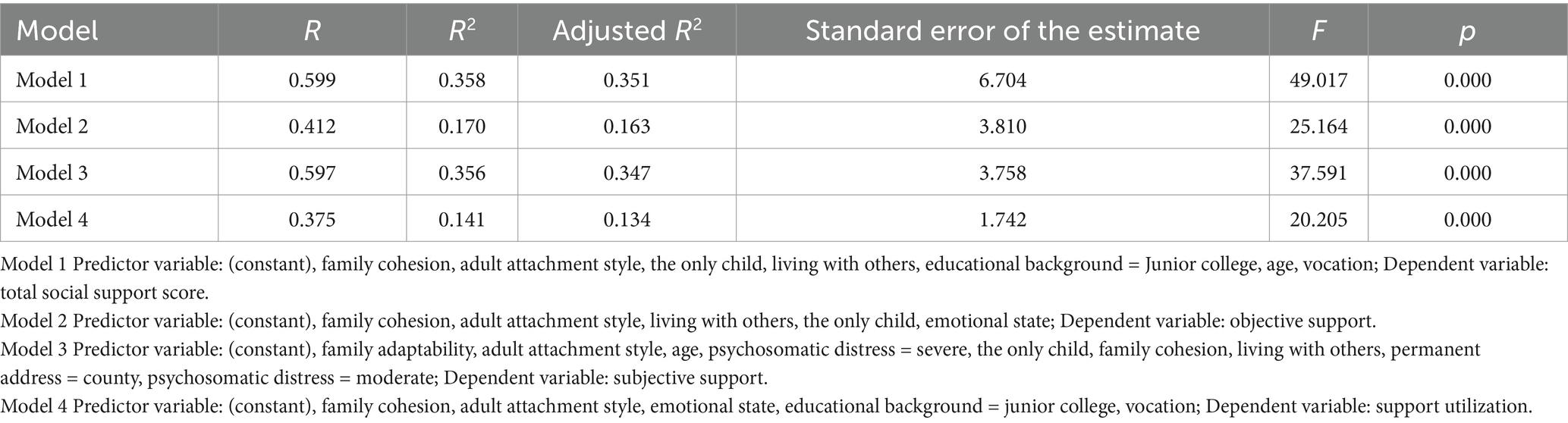
Table 4. Regression model summary.
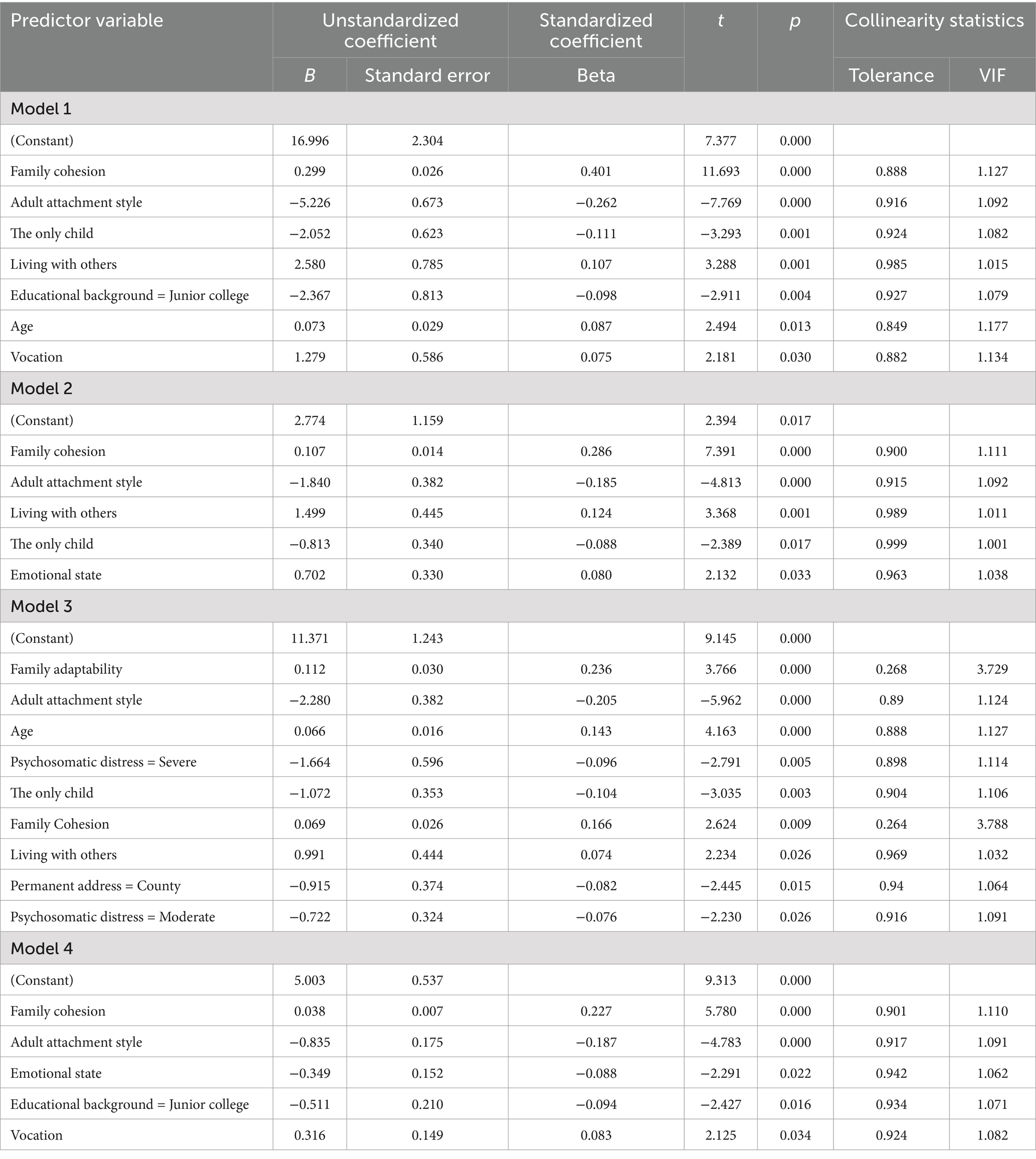
Table 5. Linear regression analysis of factors influencing healthcare workers’ social support.
Objective support
For the regression analysis of objective support, the R-squared value was 0.170, indicating that the model explained 17% of the variance in objective support scores. In this model, higher family cohesion, living with others, and a normal emotional state (as opposed to abnormal emotional state) increased objective support scores. In contrast, insecure attachment styles and only-child status decreased objective support scores (Tables 4, 5, Model 2).
Subjective support
In the analysis of subjective support, the R-squared value was 0.356, indicating that the model explained 35.6% of the variance in subjective support. Here, higher family adaptability and cohesion, older age, and living with others increased subjective support scores. Conversely, insecure attachment styles and only-child status decreased subjective support scores (Tables 4, 5, Model 3).
Support utilization
Finally, the R-squared value for the regression analysis of support utilization was 0.141, indicating that the model explained 14.1% of the variance in support utilization. In this model, higher family cohesion and doctor status (as opposed to a nurse) increased support utilization. Insecure attachment styles and abnormal emotional state decreased support utilization (Tables 4, 5, Model 4).
Discussion
Previous studies on healthcare workers’ mental health in challenging work contexts have mainly focused on anxiety, depression, and sleep quality, with relatively little exploration of social support. Social support, however, is a multidimensional construct that encompasses various forms, including subjective support, objective support, and support utilization. Despite its recognized importance, these specific dimensions of social support have been insufficiently studied, which somewhat limits our comprehensive understanding of healthcare workers’ mental health.
This study compared gender differences among healthcare workers. The results revealed significant gender differences in profession, age, permanent address, educational background, household income level, perceived stress scores, and abnormal emotional state. In this study’s sample, the nurse group was predominantly female, and the average age of females was lower than that of males, which could contribute to occupational and age differences. Differences in educational background may arise from varying tendencies between males and females in accessing higher education opportunities and professional choices (White et al., 2012). Generally, males are more inclined to choose technical medical specialties, while females tend to choose nursing and similar professions. Female healthcare workers may bear greater economic pressure (Jolly et al., 2014), particularly when shouldering family responsibilities, such as caring for children or the elderly. This may restrict their career choices and development opportunities, contributing to gender differences in family economic status. Additionally, gender differences in perceived stress and abnormal emotional states differ from previous studies (Pappa et al., 2020), potentially because male healthcare workers might have taken on more high-risk tasks or leadership roles in these challenging work contexts, roles typically accompanied by higher stress and a sense of responsibility (Morgan et al., 2022). In many cultures, men are expected to appear strong and refrain from expressing emotions. This social expectation may lead males to internalize emotions when facing pressure rather than seeking support or expressing feelings. In the linear regression analysis conducted in this study, several factors were identified as influencing levels of social support. Specifically, higher family cohesion, living with others, older age, and doctor status (as opposed to a nurse) positively increased the level of social support. Conversely, insecure attachment styles and only-child status decreased social support levels. These findings highlight the significance of social support and family intimacy as protective factors for mental health (Wright and Davidson Mhonde, 2022). Furthermore, existing literature corroborates the notion that cohesive families can provide enhanced social support and encouragement (Farrell and Barnes, 1993; Souri and Ashoori, 2015; Wright and Davidson Mhonde, 2022). The increased social support reported by individuals living with others can be explained by social interaction theory in high-pressure occupational settings, living with family members or roommates provides opportunities for emotional exchange, practical assistance, and shared coping strategies, which collectively enhance the sense of social support and resilience (Cohen and McKay, 1984; Halbesleben, 2006; Holt-Lunstad et al., 2010). Additionally, age significantly influences social support levels. Previous literature suggests that as individuals grow older, they often accumulate more social resources and support networks, allowing them to enjoy higher social support (Kröner and Müller, 2022). The phenomenon of doctors having higher social support than nurses possibly relate to professional characteristics and work environments. Nurses interact more with patients in their work, and irregular working hours in demanding work contexts may lead to less perceived support (Pappa et al., 2020). In contrast, doctors often have more extensive professional networks established through their education and professional experiences, which can provide strong support when needed. Compared to doctors, nurses may face limitations in social status and resources, resulting in lower reported levels of social support. The link between insecure attachment styles and lower social support levels is consistent with previous research (Adar et al., 2022; Florian et al., 1995). Individuals with insecure attachment styles may encounter difficulties in forming and maintaining intimate relationships, thus limiting their sources of social support. They may be more prone to handling social relationships with avoidance or anxiety, leading to lower social support levels. Finally, the lower social support among only children may be partly due to the absence of sibling interactions, which help develop skills for forming external social relationships. Individuals who grow up without sibling interactions may lack certain skills for establishing and maintaining external social relationships.
This study illustrates that social support is significantly affected by a variety of factors. The primary determinants influencing social support and its different dimensions include family relationships, living environment, professional roles, age, and emotional state. Traditional research on social support often focuses solely on overall levels, overlooking its complexity. By separately analyzing objective support, subjective support, and support utilization, this study reveals the roles and influencing factors of different dimensions of social support in challenging work contexts. Decomposing social support into different dimensions allows for a more detailed identification of which factors significantly influence specific types of support. Specifically, family cohesion has a significant positive impact on subjective support, objective support, and support utilization, indicating that close family relationships play a central role in the perception, acquisition, and utilization of social support. Living with others has a significant positive effect on both subjective support and objective support, suggesting that a shared living environment can enhance the perception of emotional support and provide tangible resources. The impact of emotional state varies across dimensions: normal emotional state significantly improves objective support, while abnormal emotional state may hinder support utilization. Professional identity has a significant effect on support utilization, indicating that occupational resources and social status play an important role in the effective use of support resources. Only-child status has a significant negative impact on both subjective support and objective support, highlighting the importance of family structure in shaping the perception and acquisition of social support. However, the effect of only-child status on support utilization is not significant, which may reflect that support utilization is more influenced by other factors, such as professional identity and emotional state, rather than family structure. Although objective support is visible and tangible, subjective support—perceived support—often has a more direct impact on mental health and behavior. Support utilization, a relatively understudied dimension, considers how individuals effectively use resources once obtained, which is crucial for understanding the practical utility of social support.
Despite its findings, this study has several limitations. Firstly, the study sample was limited to healthcare workers from a single hospital, potentially introducing regional bias that may not reflect broader circumstances. To enhance representativeness and generalizability, future studies should expand the sample size and include more diverse populations. Secondly, the cross-sectional design limits exploration of causal relationships between variables. To better explore the interactions between variables, future research should consider employing longitudinal designs to track variable changes over time and reveal causal relationships. Furthermore, reliance on self-reports may introduce recall and social desirability biases, reducing result accuracy. To address this limitation, future research could consider incorporating multiple data collection methods, such as observations, interviews, and physiological measurements, to cross-verify the authenticity and reliability of self-reported data. Finally, despite controlling for several confounding variables, unmeasured factors may still influence results. For example, differences in work nature among departments and recent significant family events might have potential impacts on study results. Therefore, future data collection processes should enhance the gathering and analysis of participants’ background information to adequately consider and control these potential variables during analysis.
Conclusion
This study found that family cohesion, living with others, and older age increased social support levels, whereas insecure attachment and only-child status decreased social support. Future mental health support for healthcare workers should take into account gender, age, family background, and occupational characteristics to design personalized psychological support plans. In particular, professional psychological counseling and support services are recommended for managing perceived stress and negative emotions. At both hospital and community levels, support groups and resource networks should be established, especially providing more professional support and development opportunities for nurses to enhance their social support levels. Additionally, mental health education and relationship management training should be implemented to help healthcare workers develop more secure attachment styles, thereby improving their psychological resilience and sense of social support in high-pressure occupational settings.
Data availability statement
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
JG: Conceptualization, Data curation, Methodology, Writing – original draft. KL: Conceptualization, Data curation, Methodology, Writing – original draft. YY: Conceptualization, Data curation, Writing – original draft. LD: Conceptualization, Methodology, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by Natural Science Foundation of Chongqing, China (CSTB2022NSCQ-MSX0057), High-level Medical Reserved Personnel Training Project of Chongqing (2021), and the Chongqing Yuzhong District Basic and Frontier Exploration Project (20210127).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
Adar, T., Davidof, M., and Elkana, O. (2022). Social support mediates the association between attachment style and psychological distress during COVID-19 in Israel. Viruses 14:693. doi: 10.3390/v14040693
Alonso, J., Vilagut, G., Mortier, P., Ferrer, M., Alayo, I., Aragón-Peña, A., et al. (2021). Mental health impact of the first wave of COVID-19 pandemic on Spanish healthcare workers: a large cross-sectional survey. Rev. Psiquiatría Salud Mental 14, 90–105. doi: 10.1016/j.rpsm.2020.12.001
Carter, H., Dennis, A., Williams, N., and Weston, D. (2023). Identity-based social support predicts mental and physical health outcomes during COVID-19. Br. J. Soc. Psychol. 62, 845–865. doi: 10.1111/bjso.12600
Cobb, S. (1976). Social support as a moderator of life stress. Psychosom. Med. 38, 300–314. doi: 10.1097/00006842-197609000-00003
Cohen, S., and McKay, G. (1984). Social support, stress and the buffering hypothesis: a theoretical analysis. London: Routledge.
Collins, N. L., and Read, S. J. (1996). A revised Adult Attachment Scale (RAAS). In: JA Simpson and WS Rholes, editors. Attachment Theory and Close Relationships. New York: Guilford Press. p. 46–76.
Dong, Y., Xu, L., Wu, S., Qin, W., Hu, F., Li, M., et al. (2022). The mediating effect of perceived social support on mental health and life satisfaction among residents: a cross-sectional analysis of 8500 subjects in Taian City, China. Int. J. Environ. Res. Public Health 19:14756. doi: 10.3390/ijerph192214756
Farrell, M. P., and Barnes, G. M. (1993). Family systems and social support: a test of the effects of cohesion and adaptability on the functioning of parents and adolescents. J. Marriage Fam. 55, 119–132. doi: 10.2307/352963
Fei, L. (1991). Preliminary evaluation of the ‘Family Closeness and Adaptability Scale’ and the ‘Family Environment Scale’ - A controlled study of normal families and family members with schizophrenia. Chinese J Ment Health. 198–202.
Florian, V., Mikulincer, M., and Bucholtz, I. (1995). Effects of adult attachment style on the perception and search for social support. J. Psychol. 129, 665–676. doi: 10.1080/00223980.1995.9914937
Halbesleben, J. R. B. (2006). Sources of social support and burnout: a meta-analytic test of the conservation of resources model. J. Appl. Psychol. 91, 1134–1145. doi: 10.1037/0021-9010.91.5.1134
Hamilton, M. (1967). Development of a rating scale for primary depressive illness. Br. J. Soc. Clin. Psychol. 6, 278–296. doi: 10.1111/j.2044-8260.1967.tb00530.x
Holt-Lunstad, J., Smith, T. B., and Layton, J. B. (2010). Social relationships and mortality risk: a meta-analytic review. PLoS Med. 7:e1000316. doi: 10.1371/journal.pmed.1000316
Hutten, E., Jongen, E. M. M., Vos, A. E. C. C., van den Hout, A. J. H. C., and van Lankveld, J. J. D. M. (2021). Loneliness and mental health: the mediating effect of perceived social support. Int. J. Environ. Res. Public Health 18:11963. doi: 10.3390/ijerph182211963
Jolly, S., Griffith, K. A., DeCastro, R., Stewart, A., Ubel, P., and Jagsi, R. (2014). Gender differences in time spent on parenting and domestic responsibilities by high-achieving young physician-researchers. Ann. Intern. Med. 160, 344–353. doi: 10.7326/M13-0974
Khoury, J. E., Atkinson, L., Bennett, T., Jack, S. M., and Gonzalez, A. (2021). COVID-19 and mental health during pregnancy: the importance of cognitive appraisal and social support. J. Affect. Disord. 282, 1161–1169. doi: 10.1016/j.jad.2021.01.027
Kröner, F., and Müller, A. (2022). Those who need it the most get it the least: age specific reciprocal effects between social support and mental strain. Acta Psychol. 231:103778. doi: 10.1016/j.actpsy.2022.103778
Liang, K., Yang, Y., Chen, K., Lv, F., and Du, L. (2024). The risk and protective factors on the mental health of healthcare workers during the lockdown period due to covid-19 pandemic. Sci. Rep. 14:11628. doi: 10.1038/s41598-024-62288-5
Liu, Q., Luo, D., Haase, J. E., Guo, Q., Wang, X. Q., Liu, S., et al. (2020). The experiences of health-care providers during the COVID-19 crisis in China: a qualitative study. Lancet Glob. Health 8, e790–e798. doi: 10.1016/S2214-109X(20)30204-7
Morgan, R., Tan, H.-L., Oveisi, N., Memmott, C., Korzuchowski, A., Hawkins, K., et al. (2022). Women healthcare workers’ experiences during COVID-19 and other crises: a scoping review. Int. J. Nurs. Stud. Adv. 4:100066. doi: 10.1016/j.ijnsa.2022.100066
Ortiz-Calvo, E., Martínez-Alés, G., Mediavilla, R., González-Gómez, E., Fernández-Jiménez, E., Bravo-Ortiz, M.-F., et al. (2022). The role of social support and resilience in the mental health impact of the COVID-19 pandemic among healthcare workers in Spain. J. Psychiatr. Res. 148, 181–187. doi: 10.1016/j.jpsychires.2021.12.030
Pappa, S., Ntella, V., Giannakas, T., Giannakoulis, V. G., Papoutsi, E., and Katsaounou, P. (2020). Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav. Immun. 88, 901–907. doi: 10.1016/j.bbi.2020.05.026
Saragih, I. D., Tonapa, S. I., Saragih, I. S., Advani, S., Batubara, S. O., Suarilah, I., et al. (2021). Global prevalence of mental health problems among healthcare workers during the Covid-19 pandemic: a systematic review and meta-analysis. Int. J. Nurs. Stud. 121:104002. doi: 10.1016/j.ijnurstu.2021.104002
Schug, C., Morawa, E., Geiser, F., Hiebel, N., Beschoner, P., Jerg-Bretzke, L., et al. (2021). Social Support and Optimism as Protective Factors for Mental Health among 7765 Healthcare Workers in Germany during the COVID-19 Pandemic: Results of the VOICE Study. Int J Environ Res Public Health, 18:3827. doi: 10.3390/ijerph18073827
Souri, A., and Ashoori, J. (2015). The relationship between perceived social support, psychological hardiness and family communication patterns with quality of life among patients with type II diabetes. J. Diabetes Nurs., 53–65.
Sun, T., Gao, L., Li, F., Shi, Y., Xie, F., Wang, J., et al. (2017). Workplace violence, psychological stress, sleep quality and subjective health in Chinese doctors: a large cross-sectional study. BMJ Open 7:e017182. doi: 10.1136/bmjopen-2017-017182
White, F. S., McDade, S., Yamagata, H., and Morahan, P. S. (2012). Gender-related differences in the pathway to and characteristics of U.S. medical school deanships. Acad. Med. 87, 1015–1023. doi: 10.1097/ACM.0b013e31825d3495
Wright, K. B., and Davidson Mhonde, R. (2022). Faith-based community members, family, and COVID-19: the role of family cohesion, social support, and spiritual support on quality of life, depression, and COVID-19-prevention behaviors. Int. J. Environ. Res. Public Health 19:12267. doi: 10.3390/ijerph191912267
Wu, W., Zhang, W., and Liu, X. (2004). The reliability and validity of adult attachment scale (AAS-1996 revised edition): a report on its application in China. Sichuan Da Xue Xue Bao Yi Xue Ban 35, 536–538.
Wu, H., Zhao, Y., Wang, J.-N., and Wang, L. (2010). Factors associated with occupational stress among Chinese doctors: a cross-sectional survey. Int. Arch. Occup. Environ. Health 83, 155–164. doi: 10.1007/s00420-009-0456-z
Xiao, S. (1999). Theoretical basis and research application of the social support rating scale. J. Clin. Psychiatry 9, 98–100.
Keywords: social support, healthcare workers, high-pressure occupational settings, mental health, protective and risk factors
Citation: Gui J, Liang K, Yang Y and Du L (2025) Protective and risk factors of social support for healthcare workers in high-pressure occupational settings. Front. Psychol. 16:1547777. doi: 10.3389/fpsyg.2025.1547777
Edited by:
Silvia Cristina da Costa Dutra, University of Zaragoza, SpainReviewed by:
Magda Guimarães de Araujo Faria, Rio de Janeiro State University, BrazilRahul Shil, Sapthagiri Institute of Medical Sciences and Research Centre, India
M. Kemal Kuscu, Koç University, Türkiye
Copyright © 2025 Gui, Liang, Yang and Du. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lian Du, Zm1yaWR1bEAxMjYuY29t
†These authors have contributed equally to this work