 Rogelio Hernández-Díaz1,2†Lucas Navarro-Vásquez1†
Rogelio Hernández-Díaz1,2†Lucas Navarro-Vásquez1† Alejandra Aguilar-Latorre3,4,5*
Alejandra Aguilar-Latorre3,4,5* Fátima Méndez-López4,5,6
Fátima Méndez-López4,5,6 Santiago Gascón-Santos3,5,7
Santiago Gascón-Santos3,5,7 Rosa Magallón-Botaya1,4,5
Rosa Magallón-Botaya1,4,5- 1Department of Medicine, Psychiatry and Dermatology, Faculty of Medicine, University of Zaragoza, Zaragoza, Spain
- 2Torrero Primary Care Health Center - Zaragoza II Sector, Aragonese Health Service, Zaragoza, Spain
- 3Department of Psychology and Sociology, Faculty of Human Sciences and Education, University of Zaragoza, Huesca, Spain
- 4Aragonese Primary Care Research Group (GAIAP), Institute for Health Research Aragón (IIS Aragón), Zaragoza, Spain
- 5Research Network on Chronicity, Primary Care and Health Promotion RD24/0005/0004, RICAPPS, Madrid, Spain
- 6Department of Physiatry and Nursing, Faculty of Health Sciences, University of Zaragoza, Zaragoza, Spain
- 7Department of Psychology and Sociology, Faculty of Social and Human Sciences, University of Zaragoza, Teruel, Spain
Introduction: Loneliness, a multidimensional emotional experience resulting from unmet social needs, affects individuals across demographics and is particularly prevalent among youth. It can be social or emotional and is linked to developmental transitions, reduced social networks, mental health conditions, and excessive social media use. Unlike desired solitude, loneliness is involuntary and associated with significant physical and mental health risks, including depression, suicide, and chronic illnesses. Despite its public health impact, youth loneliness remains underrecognized, necessitating tailored interventions. This study examines its prevalence and relationship with sociodemographic factors, social support, social media use, self-esteem, and health among students in Aragon.
Methods: This cross-sectional study investigated loneliness among adolescents and young adults (14–30 years) studying in Zaragoza, Spain, using online surveys conducted in March–April 2024. A sample of 536 participants was selected based on inclusion criteria, including informed consent. Loneliness was assessed using the UCLA Loneliness Scale and the De Jong Gierveld Loneliness Scale, alongside sociodemographic, social, and psychological variables such as self-esteem, health, mental health, and social media use. Descriptive, correlational, and regression analyses were performed to identify predictors of loneliness.
Results: The study sample comprised 73.7% women, with an average age of 20 years. Among participants, 45.9% were high school students and 54.1% university students. Higher loneliness levels are associated with spending more time on social media, fewer and lower-quality relationships, lower self-esteem, poorer self-perceived health, and having mental health problems. While no significant gender or age differences were found, the UCLA Loneliness Scale identified 31.2% of participants as lonely, and the De Jong Gierveld Loneliness Scale classified 49.1% with moderate loneliness and 27.1% with severe loneliness.
Discussion: This study highlights the high prevalence of loneliness among young individuals, affecting approximately two-thirds of the population aged 14–30. The findings underscore the importance of addressing loneliness as a public health concern, with particular attention to vulnerable groups. Further research is needed to develop effective prevention, detection, and intervention strategies tailored to youth, which could be implemented through Primary Care and educational institutions.
Introduction
Loneliness is a complex and multifaceted emotional experience that emerges from the discrepancy between the social relationships individuals desire and those they actually have (Xia and Li, 2018). Defined by Montero and Sánchez (Montero et al., 2001) as “a potentially stressful multidimensional psychological phenomenon,” loneliness can arise from perceived or actual deficiencies in affective, social, or physical domains. It affects individuals of all ages, genders, and socio-economic backgrounds and can fluctuate in intensity, appearing temporarily, intermittently, or becoming chronic (Cacioppo and Cacioppo, 2012; Sota-Velásquez et al., 2021). The experience of loneliness is not static and manifests differently across contexts. It is important to differentiate between social loneliness, characterized by an absence of group belonging (Szapu et al., 2022), and emotional loneliness, which reflects a perceived lack of close and meaningful relationships (Montero et al., 2001; Szapu et al., 2022). Additionally, the distinction between desired solitude and unwanted loneliness is critical. Desired solitude can be enriching and rejuvenating, whereas unwanted loneliness is involuntary and often linked to isolation, exclusion, and significant emotional suffering (Díez Nicolás and Morenos Páez, 2015; World Health Organization, 2023). Unwanted loneliness has been recognized as a growing global public health concern. Studies in Spain reveal that 25.5% of young individuals aged 16 to 29 reports experiencing unwanted loneliness, with women and those aged 22 to 27 disproportionately affected (Tuñón et al., 2023). The prevalence of loneliness follows a U-shaped distribution, peaking during adolescence and old age, while being less common at intermediate life stages (Catalonia Red Cross, 2022; Tuñón et al., 2023). Despite this, research efforts have historically focused on the elderly, often neglecting youth loneliness, which remains an underexplored and invisible issue (Dumont et al., 1990).
Youth loneliness stems from a confluence of social, psychological, and environmental factors. Adolescence and early adulthood are periods marked by significant developmental and social transitions, such as entering university or the workforce, which often disrupt existing support networks (Luhmann and Hawkley, 2016). The quality and quantity of friendships and family ties play pivotal roles, as do socioeconomic challenges, immigration without a support network, and physical or mental disabilities (McIntyre et al., 2018; Thomas et al., 2020). Chronic mental health conditions such as anxiety and depression exhibit a bidirectional relationship with loneliness, both exacerbating and resulting from it. Personality traits such as shyness, pessimism, and low self-esteem further predispose individuals to loneliness (Mann et al., 2022). University students are particularly vulnerable during their first academic year, as they face heightened academic pressures, relocation challenges, and the need to establish new social networks (McIntyre et al., 2018).
The digital era has reshaped the social landscape, particularly for Generation Z, often referred to as “digital natives” (Álvarez-Ramos et al., 2019). Social media platforms provide opportunities for connection but also pose risks of fostering superficial interactions and unrealistic social comparisons. Excessive use of social media has been linked to poorer mental health outcomes and diminished real-world social engagement (Pérez and Quiroga-Garza, 2019). A survey by Zaragoza University (Government of Aragon, 2023) found that 38% of students used social media to cope with discomfort, often intensifying feelings of loneliness by reducing the time spent nurturing meaningful relationships (Government of Aragon, 2023). While social media is not inherently detrimental, its overuse can lead to dependency, poorer academic performance, and social isolation. Healthy use of technology—balancing online and offline interactions—is essential to mitigate its adverse effects (Cacioppo and Cacioppo, 2012; Echeburúa and De Corral, 2010).
Loneliness significantly affects both physical and mental health through direct and indirect mechanisms. Directly, it is associated with increased cortisol levels, systemic inflammation, and weakened immune responses. Indirectly, it contributes to unhealthy lifestyle behaviors such as poor diet, physical inactivity, and substance use (Holt-Lunstad et al., 2015; Steptoe et al., 2013). The UK Loneliness Commission equates the health risks of loneliness to smoking 15 cigarettes a day, underscoring its profound public health implications (Jo Cox Commission, 2017). The mental health consequences of loneliness are equally severe, encompassing heightened risks of anxiety, depression, and suicidal ideation (Mann et al., 2022). Adolescents and young adults experiencing loneliness report higher rates of self-harm and suicide attempts (Pearce et al., 2021). Additionally, loneliness exacerbates sleep disturbances, leading to fragmented and poor-quality rest, which further diminishes daytime functioning (Matthews et al., 2017). Chronic loneliness has also been implicated in long-term health outcomes, including cardiovascular disease, cognitive decline, and increased mortality. Addressing loneliness at an early age may be associated with better long-term health outcomes, potentially mitigating the risk of conditions such as cardiovascular disease, cognitive decline, and increased mortality (Valtorta et al., 2016).
Despite its profound impact, youth loneliness remains underrecognized in healthcare systems. Primary care services often prioritize loneliness interventions for older adults, leaving younger populations underserved (Gené-Badia et al., 2016). Collaborative approaches involving mental health professionals, educators, and community organizations are critical to addressing youth loneliness. Tailored interventions can significantly improve mental health outcomes, reduce social isolation, and enhance overall wellbeing (Masi et al., 2011).
Loneliness in youth can be better understood within established theoretical frameworks. The Biosocial Model of Health emphasizes the dynamic interplay between biological predispositions, psychological processes, and social environments in shaping health outcomes (Cacioppo et al., 2015; Engel, 1977). This model provides a useful lens through which to examine how factors such as digital hyperconnectivity, family structures, and mental health conditions interact to influence loneliness. Additionally, the Social Baseline Theory (Beckes and Coan, 2011) suggests that humans are biologically adapted to rely on social proximity to conserve energy and regulate affect. A lack of reliable social support systems may therefore lead to increased emotional and physiological costs, making adolescents and young adults particularly vulnerable to the effects of loneliness. In this context, the present study focuses on the region of Zaragoza (Aragón), which presents a relevant case study due to its distinctive demographic and social characteristics. Zaragoza (Aragon) has experienced recent demographic shifts, including increased youth migration and growing diversity in educational settings.
This study hypothesizes that loneliness is a prevalent but under-researched issue among adolescents and young adults, potentially driven by increased use of mobile phones, lack of social support, the impact of the COVID-19 pandemic and mental health conditions like anxiety and depression. The objectives are to determine the prevalence of loneliness among students in Aragon and to examine its association with sociodemographic factors, social support, social media usage, self-esteem, health, and mental health.
Materials and methods
Design
This study is a descriptive observational cross-sectional investigation.
Population and sample
The target population comprises adolescents and young adults aged 14–30 years who are currently studying in high school or university in Zaragoza, Northern Spain. According to annual statistical reports from the Ministries of Education and Universities, this population consists of 5,570,725 students (Ministerio de Educación y Formación Profesional, 2023; Ministerio de Universidades, 2023). Based on a confidence level of 95%, a margin of error of 5%, and an assumed loneliness prevalence of 25.5% (Tuñón et al., 2023), a sample size of 292 participants was required.
The selection criteria included young individuals aged 14–30 years, enrolled in the 2023/2024 academic year in Compulsory Secondary Education, Baccalaureate, Intermediate Vocational Training, University Degree, Master's, or Doctorate programs, who agreed to participate in the study, provided informed consent, and accepted the Privacy Policy of the University of Zaragoza and Google. Exclusion criteria encompassed any individuals who did not meet these inclusion requirements.
Procedure
Data were collected during March and April 2024 using two online surveys created specifically for this study via Google Forms. One survey targeted high school students, and the other university students. The questionnaire ensured anonymity and included both closed-ended questions with predefined answer options and a few open-ended questions. The first page provided the informed consent form and privacy policies from Google and the University of Zaragoza. Participants had to accept these to proceed. The survey for university students offered an optional short-answer question for personal contributions and an option to receive the study's results via email.
For university students, the survey was disseminated via social networks. Additionally, faculty representatives and professors assisted in encouraging participation. For high school students, school principals and administration from several high schools situated in the autonomous region of Zaragoza (Spain) facilitated the study after reviewing the proposal. Tutors invited students to complete the questionnaire during school hours using their computers or mobile devices. The high schools were chosen by convenience sampling (Galloway, 2005) and the sampling technique was non-probabilistic snowball sampling (Johnson, 2005). It should be noted that the sampling strategy, which relied on voluntary participation and online dissemination, may have introduced self-selection bias. This is particularly relevant considering the overrepresentation of female participants (73.7%), which could influence the generalizability of the results and should be considered when interpreting findings.
Study variables
Sociodemographic variables included age (measured in years), gender (female, male), place/province of origin (Spain, foreigner), having or not having a partner, belonging to the LGTBIQ+ community (yes, no, prefer not to say), current educational level (high school or university), living situation (alone, with family or company), and participation in associative, sporting, solidarity, union or other activities (yes, no).
Variables related to loneliness included:
• The UCLA Loneliness Scale (Sheffield Hallam University, 2022) consists of three items that measure relational connection, social integration, and self-perceived isolation, with response options: “almost never,” “sometimes,” and “frequently” (replacing “often” for clarity). Scores range from 3 to 9 points, classifying individuals as not lonely (3–5 points) or lonely (6–9 points). Its validated Spanish version for the general population has a Cronbach's alpha of 0.78 (Pedroso-Chaparro et al., 2022), and in this study, reliability was also acceptable (alpha = 0.74).
• The De Jong Gierveld Loneliness Scale (Sheffield Hallam University, 2022) includes six items assessing emotional loneliness (lack of intimate relationships) and social loneliness (limited social networks). Responses are “yes,” “more or less (sometimes),” and “no.” Emotional loneliness items are scored as follows: “yes” and “more or less” = 1 point, “no” = 0 points; for social loneliness items, “yes” = 0 points, and “more or less” and “no” = 1 point. Total scores range from 0 to 6, categorizing individuals as not lonely (0–1 points), moderately lonely (2–4 points), or severely lonely (5–6 points). Although the Spanish version of this scale was originally validated for adults aged 60 and over (Ayala et al., 2012), we chose to include it in this study to explore its potential applicability in younger populations. No prior studies, to our knowledge, have validated the DJG scale specifically in adolescents or young adults. The Spanish version validated for individuals aged 60+ has a Cronbach's alpha of 0.77 (Ayala et al., 2012), with this study showing an acceptable reliability of 0.74.
Additional variables assessed include the frequency and duration of perceived loneliness, its associated causes, seeking help, the age group with the highest loneliness prevalence, its relationship with the COVID-19 pandemic, the societal importance of the issue, and the perceived quantity and quality of family, friendship, and peer/classmate relationships. Some questions were adapted from the State Observatory of Unwanted Loneliness's youth loneliness study questionnaire (Tuñón et al., 2023).
Other variables:
• Mobile phone and social media use: Daily time spent (in hours) and opinions on the relationship between loneliness and excessive internet use.
• Self-esteem, which is assessed using a Likert scale ranging from 1 to 5, with responses to the statement “I have high self-esteem” (strongly agree, agree, neutral, disagree, strongly disagree).
• Perceived health, rated on a Likert scale from 1 to 5, with options: very good, good, fair, bad, or very bad.
• Mental health problems, with the following response options: “No,” indicating the absence of mental health issues; “Yes, diagnosed by a doctor,” for individuals who have received a formal diagnosis; “Yes, I think I have a problem and have sought help,” for those who believe they have a mental health problem and have already sought professional assistance; and “Yes, I think I have a problem but have not sought help,” for individuals who acknowledge a mental health issue but have not yet pursued help.
Statistical analysis
Firstly, a descriptive analysis was conducted to characterize the sample, using frequencies and percentages for categorical variables and means and standard deviations for continuous variables. Subsequently, Chi-square tests and Student's t-tests were used to evaluate gender differences. Secondly, Pearson correlation coefficients were calculated to analyze associations between the UCLA Loneliness Scale and the De Jong Gierveld Loneliness Scale (DJG) and the rest of the variables. Finally, a multiple linear regression analysis was performed to examine the relationship between DJG scale scores and the correlated variables, employing a stepwise method to refine the model and identify the best-fitting predictors (Núñez et al., 2011). This stepwise approach iteratively excluded the least correlated variables to optimize the statistical model (Hamilton, 1994). Data collection and analyses were carried out using Microsoft Excel and SPSS software (Version 29.0) (IBM Corp, 2023). Statistical significance was set at p < 0.05.
Ethical aspects
This study was reviewed and approved by the Research Ethics Committee of the Autonomous Community of Aragon (CEICA; PI24/050) and authorized by the University of Zaragoza for data processing (RAT 2024-9). Online informed consent was obtained from all participants, integrated into the survey itself. For minors, consent was also obtained from their parents or guardians. The informed consent detailed the study's objectives and its anonymous nature, emphasizing that the results could not, under any circumstances, be linked to individual participants. No identifying information was collected, and the data were anonymized and processed in compliance with current personal data protection legislation. The risk/benefit analysis indicated no associated risks, as completing the survey posed no harm to participants. Additionally, no financial compensation was provided, as the data collected were used solely for the purpose of this project.
Results
A total of 536 individuals participated in the survey, comprising 290 students (54.1%) from the University of Zaragoza and 246 students (45.9%) from Aragonese high schools (Table 1). The descriptive analysis revealed that 73.7% of respondents were women and 26.3% were men. The participants had a mean age of 20.09 years with a standard deviation of 3.67. For analytical clarity, ages were grouped into four categories: 14–17 years (24.6%), 18–19 years (23.5%), 20–22 years (28.9%), and 23–30 years (22.9%).
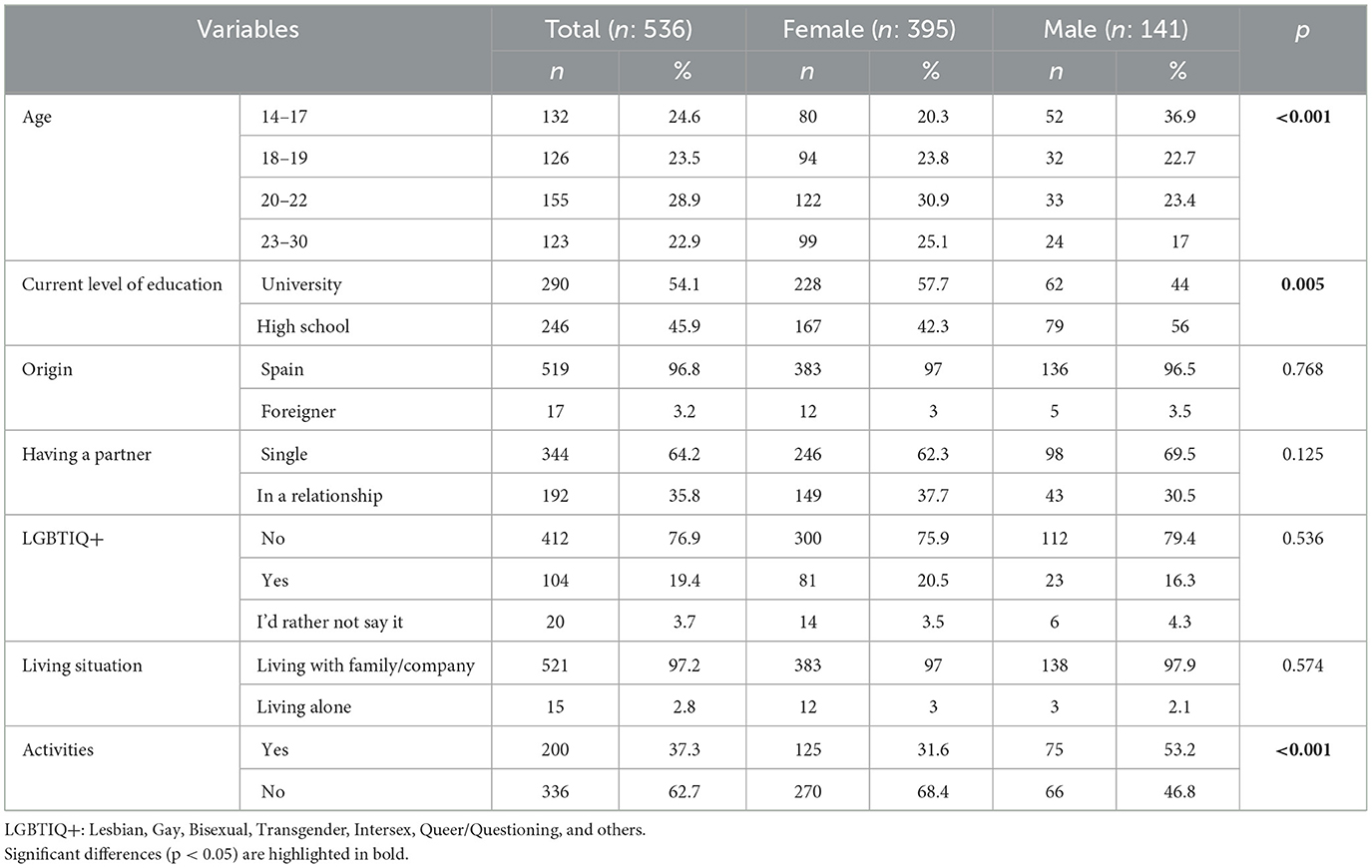
Table 1. Descriptive analysis of sociodemographic variables.
There were significant differences in age distribution by gender (p < 0.001), with a higher proportion of males in the youngest group (14–17 years: 36.9% vs. 20.3% in females) and a greater proportion of females in the 20–22 and 23–30 age groups. Regarding education level, university students were more likely to be female (57.7% vs. 44% in males, p = 0.005), whereas high school students had a higher proportion of males (56% vs. 42.3% in females).
In terms of relationship status, 64.2% of respondents identified as single, while 35.8% reported being in a romantic relationship. No significant gender differences were observed (p = 0.125). Regarding sexual orientation and identity, 19.4% identified as Lesbian, Gay, Bisexual, Transgender, Intersex, Queer/Questioning, and others (LGBTIQ+), while 76.9% identified as non-LGBTIQ+, and 3.7% preferred not to disclose this information. No significant differences were found between men and women (p = 0.536). The vast majority (97.2%) reported living with their families or in shared housing, with no significant gender difference (p = 0.574).
However, gender differences emerged in extracurricular activities (p < 0.001), where a higher percentage of men (53.2%) reported participating in associative, sporting, solidarity, or union activities compared to women (31.6%).
Regarding loneliness, 22.6% of respondents reported never feeling lonely, while 57.1% experienced loneliness sometimes, 18.7% frequently, and 1.7% always (Table 2). Gender differences were significant (p < 0.001), with men more likely to report never feeling lonely (34.8% vs. 18.2% in women), and women more frequently reporting occasional loneliness (63% vs. 40.4% in men). No significant gender differences were found in the self-reported duration of loneliness (p = 0.766), but more women (43.3%) than men (35.5%) reported experiencing loneliness for more than a year.
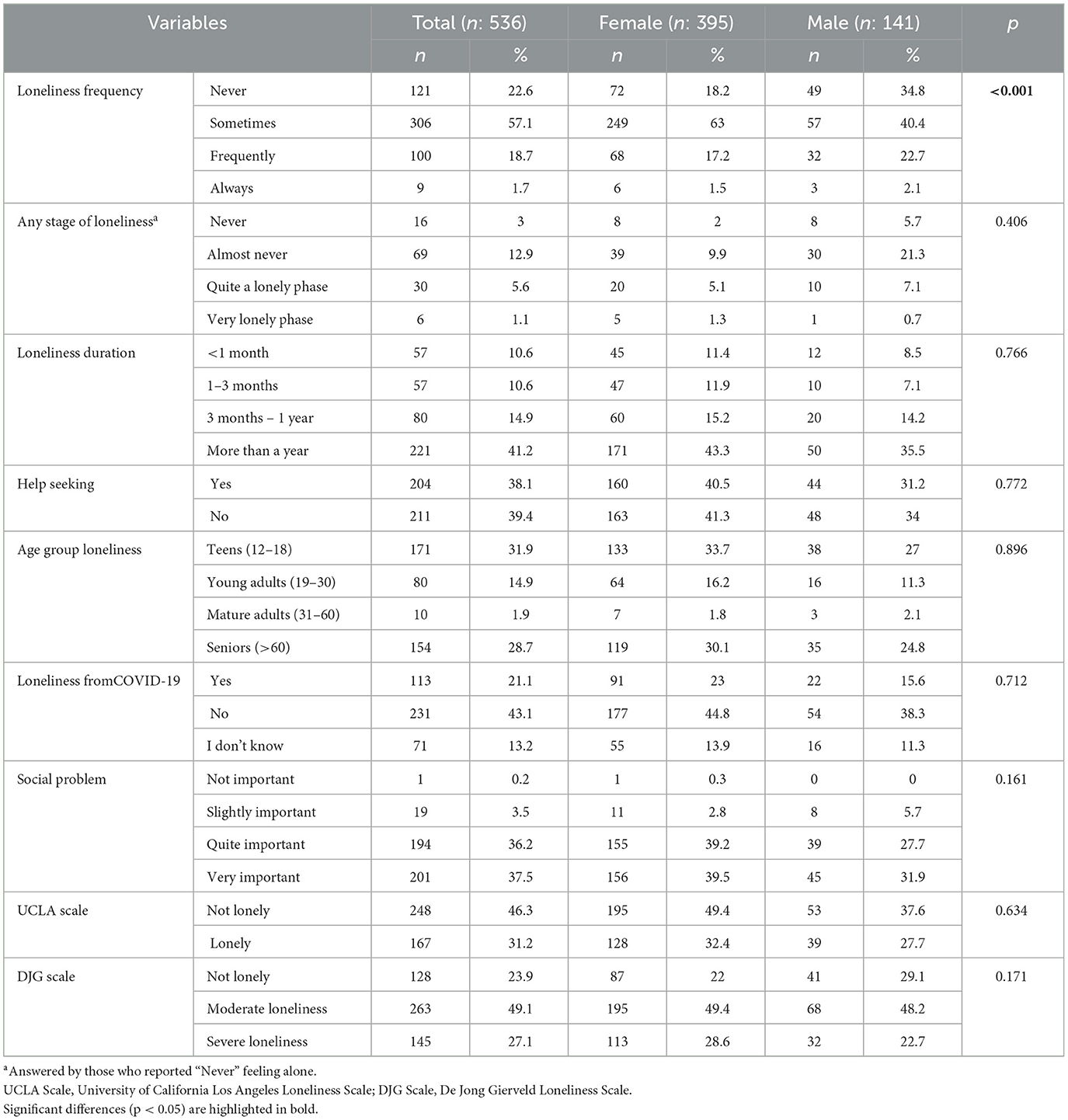
Table 2. Descriptive analysis of loneliness variables.
Regarding help-seeking for loneliness, 38.1% of participants had sought support, while 39.4% had not, with no significant gender differences (p = 0.772). When asked about the age group most associated with loneliness, 31.9% pointed to adolescence (12–18 years), followed by seniors over 60 (28.7%). No significant gender differences were observed in these perceptions (p = 0.896).
Perceived impact of the COVID-19 pandemic on loneliness was reported by 21.1% of participants, while 43.1% disagreed and 13.2% were unsure, with no gender-based differences (p = 0.712). When evaluating loneliness as a social issue, 37.5% of respondents considered it very important and 36.2% as quite important, again without significant gender differences (p = 0.161).
Loneliness scales also revealed gender variations. On the UCLA Loneliness Scale, men were more likely to be categorized as “not lonely” (37.6% vs. 49.4% in women), though this difference was not statistically significant (p = 0.634). The De Jong Gierveld Loneliness Scale (DJG) identified 23.9% of respondents as not lonely, 49.1% as experiencing moderate loneliness, and 27.1% as suffering from severe loneliness, with no statistically significant gender differences (p = 0.171).
The analysis of causes associated with loneliness revealed several contributing factors, with no significant gender differences in most variables (Table 3). A notable proportion of participants reported not having enough friends (16.8%), difficulty relating to others (25.2%), or not having time to socialize (21.6%). Females were more likely to cite lack of time to relate as a cause of loneliness (25.1% vs. 12.1%, p = 0.016). Other frequently reported causes included family conflicts (15.9%) and physical or mental health issues preventing social interactions (13.4%).
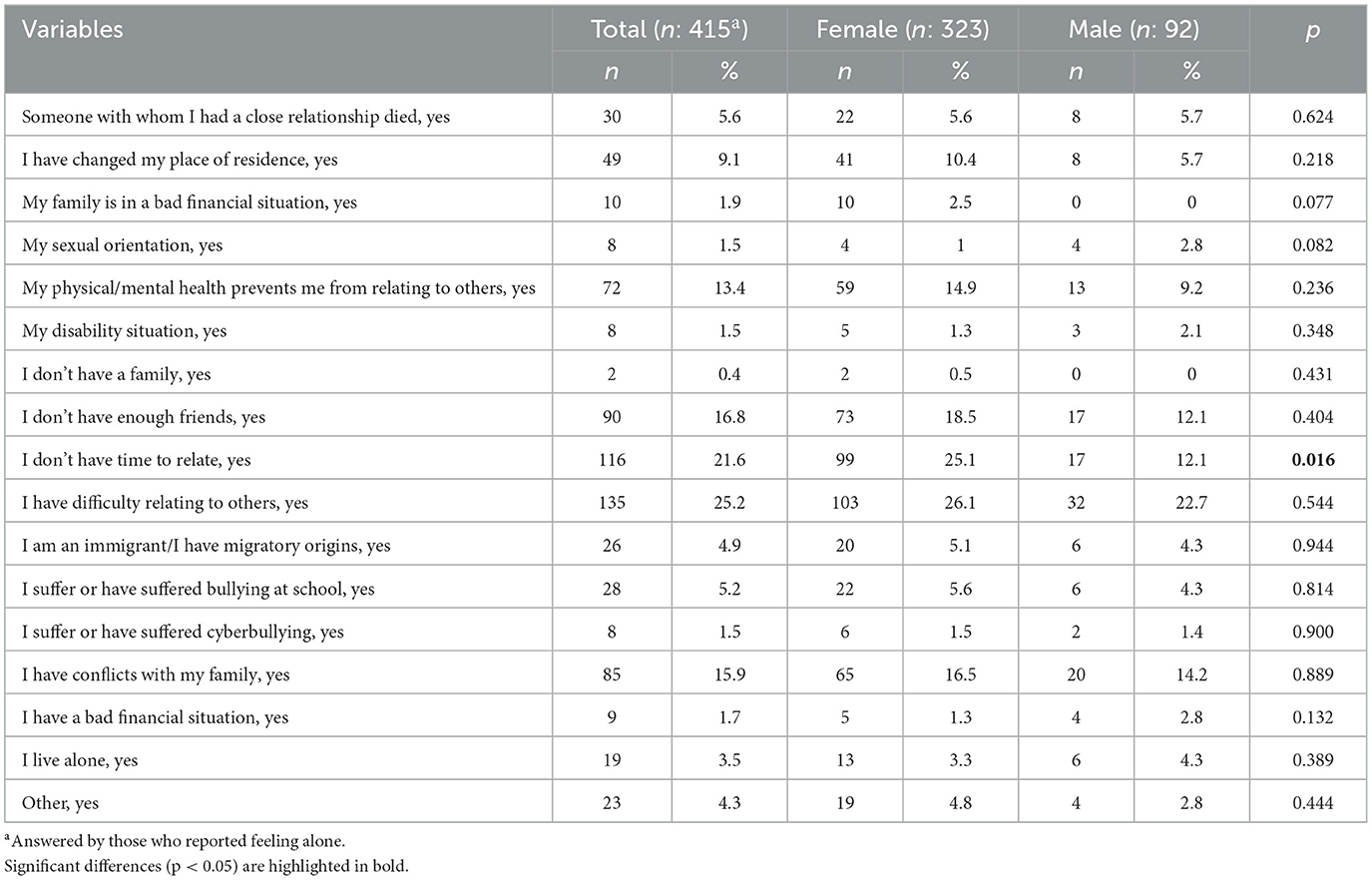
Table 3. Descriptive analysis of causes associated with loneliness.
Variables related to social support, the use of social networks, self-esteem and self-perceived health were analyzed (Table 4). The analysis of social relationships revealed no significant gender differences in the perceived quantity and quality of family, friends, or classmates. Most participants reported having the desired amount of family (66.2%), friends (65.7%), and classmates (57.3%), with smaller proportions indicating “less than desired” relationships in these categories. Regarding quality, the majority rated their family relationships as good (71.3%), and only 6.5% perceived them as poor. Similarly, 97.8% reported good or fair quality in friendships.
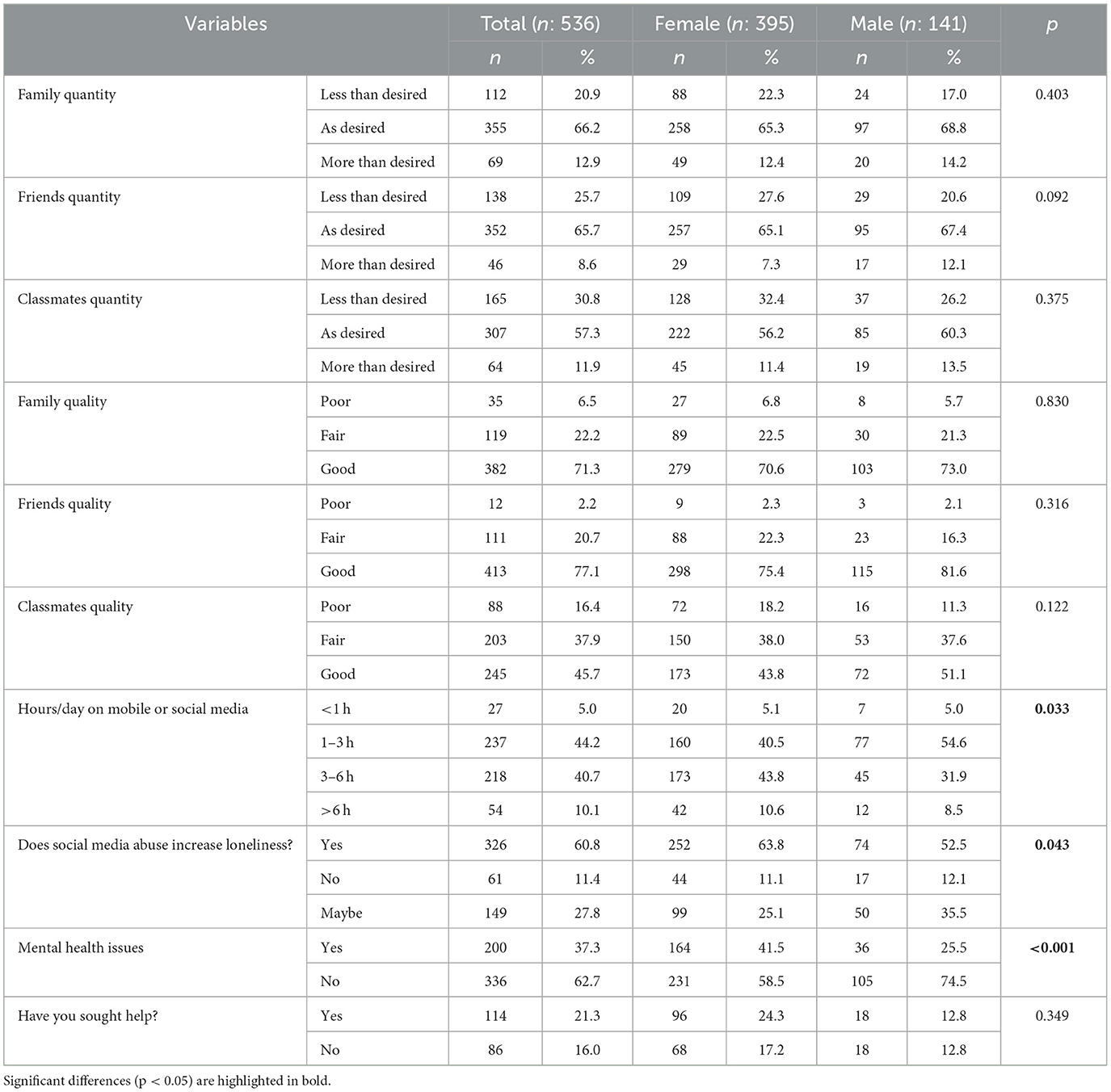
Table 4. Descriptive analysis social support variables, use of social media and mental health.
Regarding hours spent on mobile or social media, females were more likely to use social media for 3–6 h daily (43.8% vs. 31.9%), while males were more likely to use it for 1–3 h daily (54.6% vs. 40.5%; p = 0.033). A higher percentage of females (63.8%) than males (52.5%) believed that excessive social media use increased loneliness (p = 0.043).
A higher percentage of females (41.5%) than males (25.5%) reported having mental health issues (p < 0.001), though no significant difference was found in seeking professional help (24.3% females vs. 12.8% males; p = 0.349).
Moreover, the descriptive analysis of the quantitative variables was carried out, the mean and standard deviation were analyzed (Table 5). The mean age was 20 years, the mean score on the UCLA Loneliness Scale was 5 (corresponding to “not lonely”), and the mean score on the DJG scale was 2 (“moderate loneliness”). An average of 2 causes associated with the feeling of loneliness was found. Regarding gender differences, males were slightly younger on average than females (19.48 vs. 20.30 years, p = 0.022). While no gender differences were observed in the number of loneliness causes or UCLA Loneliness Scale scores, males scored lower on the DJG compared to females (2.77 vs. 3.18, p = 0.026). Males also reported significantly higher self-esteem (3.33 vs. 2.98, p = 0.001) and better self-perceived health (4.01 vs. 3.82, p = 0.010).
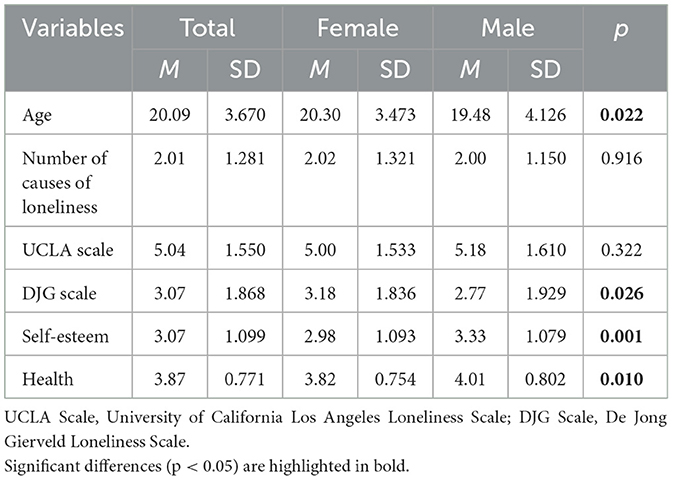
Table 5. Descriptive analysis of quantitative variables.
Next, the correlation analysis of the UCLA Loneliness Scale and the De Jong Gierveld Loneliness Scale with the other variables was performed (Table 6). A higher level of loneliness according to the UCLA Loneliness Scale is positively correlated with belonging to the LGBTIQ+ community (r = 0.156, p < 0.001), being a high school student (r = 0.137, p < 0.05), loneliness frequency (r = 0.569, p < 0.001), loneliness duration (r = 0.361, p < 0.001), and the total number of causes of loneliness (r = 0.420, p < 0.001), friend quantity (r = −0.316, p < 0.001) and quality (r = −0.288, p < 0.001), family quality (r = −0.145, p < 0.01), classmates quantity (r = −0.176, p < 0.001), and quality (r = −0.203, p < 0.001), self-esteem (r = −0.328, p < 0.001), health (r = −0.335, p < 0.001), and having a mental health problem (r = 0.303, p < 0.001).
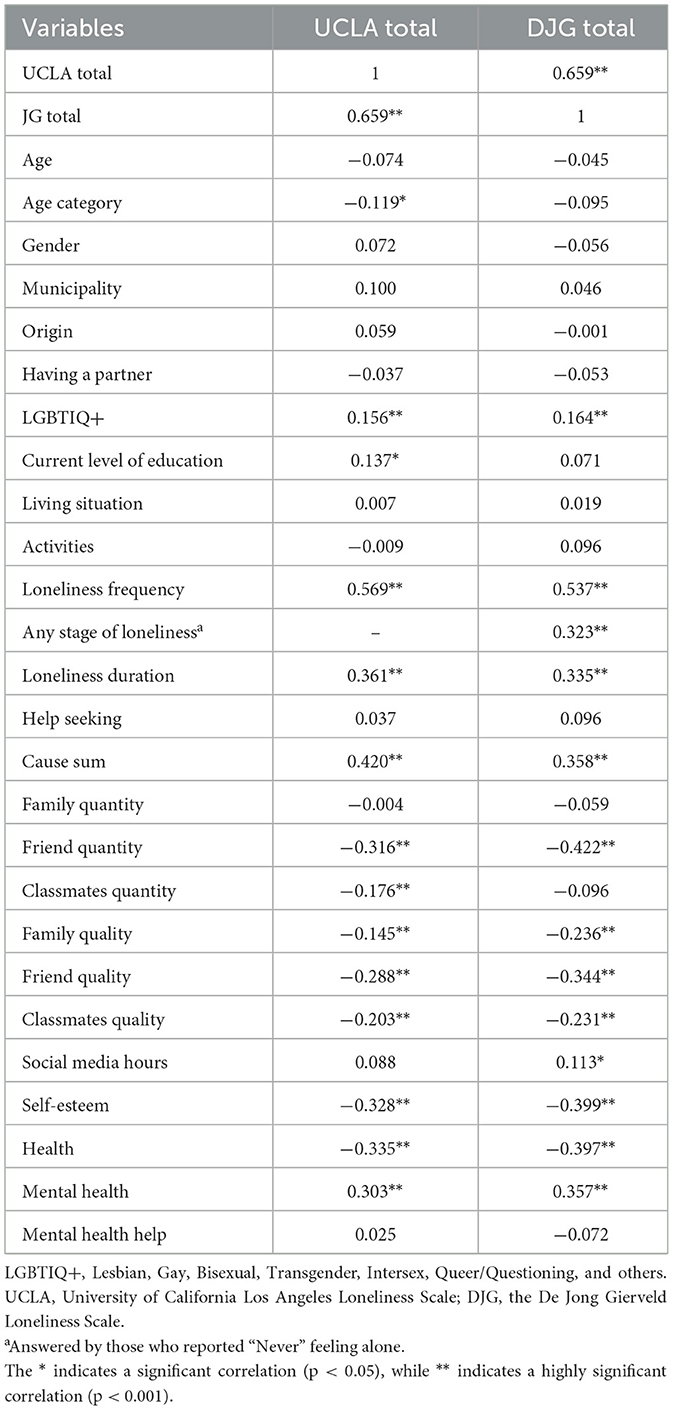
Table 6. Correlation of the variables with the UCLA Loneliness Scale and the De Jong Gierveld Loneliness Scale.
For the De Jong Gierveld Loneliness Scale, a higher level of loneliness is positively correlated with belonging to the LGBTIQ+ community (r = 0.164, p < 0.001), loneliness frequency (r = 0.537, p < 0.001), loneliness duration (r = 0.335, p < 0.001), and the total number of causes of loneliness (r = 0.358, p < 0.001). It is also negatively correlated with the quantity (r = −0.422, p < 0.001) and quality (r = −0.344, p < 0.001) of friends, family quality (r = −0.236, p < 0.001), classmates quality (r = −0.231, p < 0.001), hours spend on social media (r = 0.113, p < 0.05), self-esteem (r = −0.399, p < 0.001), health (r = −0.397, p < 0.001), and mental health (r = 0.357, p < 0.001).
Finally, the regression analysis identified key predictors of loneliness, as measured by the De Jong Gierveld Loneliness Scale (Table 7). Better self-perceived health [B = −0.416, β = −0.173, p < 0.001, 95% CI (−0.626, −0.205)], a greater number of friends [B = −0.809, β = −0.246, p < 0.001, 95% CI (−1.061, −0.558)], higher-quality friendships [B = −0.594, β = −0.156, p < 0.001, 95% CI (−0.883, −0.305)], and higher self-esteem [B = −0.225, β = −0.134, p = 0.002, 95% CI (−0.367, −0.083)] were significantly associated with lower levels of loneliness. In contrast, more mental health problems [B = 0.516, β = 0.134, p = 0.002, 95% CI (0.188, 0.843)] and more hours spent on social media [B = 0.207, β = 0.083, p = 0.029, 95% CI (0.021, 0.392)] were associated with higher loneliness scores. The regression model explained 28.7% of the variance in loneliness (adjusted R2 = 0.287, F(6, 509) = 35.561, p < 0.001).
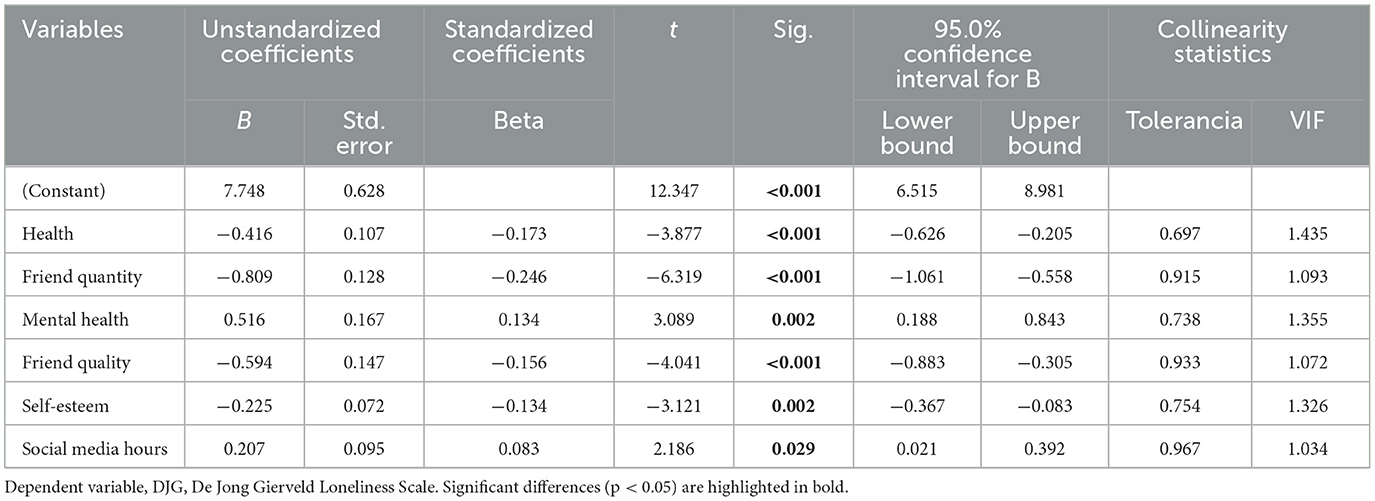
Table 7. Linear regression analysis of variables associated with the De Jong Gierveld Loneliness Scale.
Discussion
In this study, we examined feelings of loneliness among 536 adolescents and young adults in our community. Of the participants, 20.4% reported feeling lonely frequently or always. Loneliness was found to be associated with time spent on social media, the quantity and quality of friendships, low self-esteem, and poorer physical and mental health. When dividing the sample by gender, the majority of participants were women. This may be attributed to the higher likelihood of women participating in surveys compared to men (Smith, 2008). Regarding age, participants ranged from 14 to 30 years old, with 54.6% falling within the typical age range of Spanish university students (18–21 years), consistent with this sample (Ministerio de Universidades, 2023).
Significant gender differences were observed in various variables, including age and level of education (with most boys in high school and most girls in university), extracurricular activities (boys participated in more activities), frequency of loneliness (a higher proportion of men reported never feeling lonely), hours spent on social media (higher in women), self-esteem (higher in men), perception of health status (better in men), and mental health problems (more frequent in women). Additionally, women scored higher on the De Jong Gierveld Loneliness Scale (DJG) when treated as a continuous measure. However, no significant correlation was found between gender and loneliness levels on either the University of California Los Angeles Loneliness Scale (UCLA Loneliness Scale) or the DJG Scale. Given the relationship between these characteristics and loneliness, one might expect women to have higher loneliness scores than men. However, our findings align with some studies (Maes et al., 2019) while differing from others that report higher loneliness prevalence among women (Tuñón et al., 2023).
More than half of young people reported feeling lonely sometimes, and one in five frequently or always. Approximately 41.2% had experienced loneliness for more than a year, underscoring the need for effective interventions to address this issue. Additionally, nearly all participants considered loneliness to be a quite or very important social problem. Correlation and regression analyses revealed that higher frequency and longer duration of loneliness were associated with higher scores on the loneliness scales, indicating greater loneliness levels. At least one in five young people believed their loneliness was exacerbated or caused by the COVID-19 pandemic, a period marked by increased isolation and a rise in mental health issues (Wilkialis et al., 2021). The general consensus among participants was that loneliness is most prevalent among adolescents and individuals over 60 years of age. Only 1.9% associated significant loneliness with adults aged 31 to 60 years. These findings align with previous studies [State Observatory of Unwanted Loneliness (SoledadES), 2022] and reflect the “U-shaped” distribution of loneliness across the lifespan (Martín Roncero and González-Rábago, 2021). Despite recognizing loneliness as a serious issue, about half of the participants had not sought help. This discrepancy may stem from a lack of perceived or actual close relationships to rely on, a lack of tools or resources for seeking support, or the stigma surrounding loneliness, which might make individuals hesitant to discuss it even with family members.
The UCLA Loneliness Scale classified 46.3% of participants as non-lonely and 31.2% as lonely, while the De Jong Gierveld Loneliness Scale identified 49.1% as experiencing moderate loneliness, 27.1% as severe loneliness, and only 23.9% as non-lonely. These findings are similar to those of the Red Cross of Catalonia's study, where only 20.25% of young people aged 18 to 29 were categorized as non-lonely according to the De Jong Gierveld Loneliness Scale (Catalonia Red Cross, 2022). However, they differ significantly from other studies reporting a lower prevalence of youth loneliness, with rates of 25.5% or less (Casal-Rodríguez et al., 2023; Tuñón et al., 2023). The study also examined numerous causes that participants linked to their feelings of loneliness. The most common were “I have difficulty relating to others,” “I don't have time to socialize,” “I don't have enough friends,” and “I have conflicts with my family.” These associations align with prior research findings (Casal-Rodríguez et al., 2023; Tuñón et al., 2023). While there is substantial knowledge about the protective factors and risk factors for loneliness and social isolation in older adults, these may not fully apply to younger populations. Further research is needed to identify the specific factors most relevant to loneliness in young people.
Regarding mobile phone and social network use, approximately half of the young people in the study reported spending at least 3 h daily on these platforms, with one in 10 spending 6 h or more. These findings differ significantly from the 2023 Annual Social Media Study, which reported that adolescents spend an average of 1 h and 14 min, and young adults 1 h and 32 min (IAB Spain, 2023). Correlation analysis revealed that increased time spent on mobile phones and social networks was associated with higher levels of loneliness, consistent with other studies (Pérez and Quiroga-Garza, 2019; Sota-Velásquez et al., 2021). This may be explained by reduced time available for face-to-face social interactions. Additionally, most participants (60.8%) believed that excessive internet use could promote loneliness. Given that younger individuals are gaining earlier access to technology, it is crucial to address this as a potential risk factor for youth loneliness and to promote healthy usage patterns to protect social relationships. Lower levels of self-esteem were also found to correlate with greater loneliness. A lack of confidence may hinder socialization, while negative self-perceptions could lead individuals to misinterpret their relationships as inadequate or insufficient. Similarly, those with poorer self-perceived health and mental health problems reported significantly higher levels of loneliness. Participants often attributed their loneliness directly to health issues, consistent with previous findings (Martín Roncero and González-Rábago, 2021; Tuñón et al., 2023). Poor health may limit social interactions, fostering feelings of loneliness, while loneliness itself has well-documented negative effects on health (Martins Barroso et al., 2023). Interestingly, no significant correlation was found between loneliness and relationship status, contrasting with prior studies where having a partner served as a protective factor against loneliness (Hernan-Montalban and Rodríguez-Moreno, 2017; Luhmann and Hawkley, 2016). However, belonging to the LGBTIQ+ community emerged as a significant risk factor for loneliness, with participants in this group scoring higher on both the UCLA Loneliness Scale and the De Jong Gierveld Loneliness Scale. This association is likely influenced by the discrimination and social challenges faced by this minority group. Overall, loneliness is increasingly recognized as a risk factor for various diseases (Mann et al., 2022; Matthews et al., 2017).
Given the high prevalence and duration of loneliness among adolescents and young adults observed in this study, practical steps are needed to address the issue systematically. First, integrating loneliness screenings into school and university health programs could help in early identification of at-risk individuals. Second, the development of targeted social media literacy curricula may mitigate the negative impact of excessive online activity on social connection. Third, promoting structured opportunities for social engagement, particularly for vulnerable groups such as LGBTIQ+ youth, can serve as protective buffers. Finally, training school staff and mental health professionals to recognize and address loneliness as a legitimate concern could improve both detection and support outcomes.
Limitations
This study analyzed a total of 536 surveys, exceeding the calculated sample size of 292 needed to achieve statistical significance. This larger sample size enhances the external validity of the project, allowing for more robust inference of the results. However, the use of non-probabilistic convenience sampling meant that participants voluntarily chose to respond to the survey. This approach could potentially affect the representativeness of the sample and, consequently, the external validity of the study. Furthermore, it may have introduced self-selection bias, as individuals who feel more connected to the topic of loneliness may have been more inclined to participate, potentially inflating the prevalence of loneliness in the sample.
The study utilized an online form, incorporating questions and questionnaires that have been validated in similar contexts. One of the scales used, the De Jong Gierveld Loneliness Scale, has been validated in Spain for use with elderly populations but not for young people. Due to the lack of a validated loneliness scale tailored to youth, the De Jong Gierveld Loneliness Scale was chosen. This limitation underscores the need for instruments specifically designed to measure loneliness in younger populations.
Additionally, as the data were obtained through self-report measures, the results may be subject to social desirability and recall biases. Participants might have under- or over-reported certain behaviors or experiences, either unintentionally or in an effort to present themselves in a more socially acceptable manner. Finally, since the study was conducted in Zaragoza, Spain, the generalizability of the findings to other regions or countries may be limited due to cultural, social, or contextual differences. Further studies in diverse settings would be necessary to confirm the broader applicability of the results.
Conclusions
Loneliness is highly prevalent among young students in Aragón, affecting two-thirds of individuals aged 14 to 30, with at least half experiencing loneliness for over a year. Higher loneliness levels are associated with spending more time on social media, fewer and lower-quality relationships, lower self-esteem, poorer self-perceived health, and having mental health problems. While no significant gender or age differences were found, the UCLA Loneliness Scale identified 31.2% of participants as lonely, and the De Jong Gierveld Scale classified 49.1% with moderate loneliness and 27.1% with severe loneliness. The lack of a youth-specific loneliness scale highlights the need for tailored tools to better detect, prevent, and address loneliness in this age group through social, health, and educational services.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Research Ethics Committee of the Autonomous Community of Aragon (CEICA; PI24/050). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
RH-D: Conceptualization, Project administration, Writing – original draft, Writing – review & editing. LN-V: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. AA-L: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. FM-L: Data curation, Formal analysis, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SG-S: Writing – original draft, Writing – review & editing. RM-B: Conceptualization, Funding acquisition, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to acknowledge the University of Zaragoza; the Aragonese Primary Care Research Group (GAIAP, B21_23R), funded by the Department of Innovation, Research and University of the Government of Aragón, Spain; the Institute for Health Research Aragón (IIS Aragón); and the Research Network on Chronicity, Primary Care and Health Promotion (RICAPPS), grant RD24/0005/0004, funded by the Carlos III Health Institute of the Spanish Ministry of Economy and Competitiveness, and co-financed by European Union ERDF funds.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Álvarez-Ramos, E., Heredia-Ponce, H., and Romero-Oliva, M. F. (2019). Generation Z and Social Networks. A view from adolescents in Spain. Revista Espacios. Available online at: https://www.revistaespacios.com/a19v40n20/a19v40n20p09.pdf (accessed May 12, 2025).
Ayala, A., Rodríguez-Blázquez, C., Frades-Payo, B., Forjaz, M. J., Martínez-Martín, P., Fernández-Mayoralas, G., et al. (2012). Propiedades psicométricas del Cuestionario de Apoyo Social Funcional y de la Escala de Soledad en adultos mayores no institucionalizados en España. Gac. Sanit. 26, 317–324. doi: 10.1016/j.gaceta.2011.08.009
Beckes, L., and Coan, J. A. (2011). Social baseline theory: the role of social proximity in emotion and economy of action. Soc. Personal. Psychol. Compass 5, 976–988. doi: 10.1111/j.1751-9004.2011.00400.x
Cacioppo, J. T., and Cacioppo, S. (2012). The phenotype of loneliness. Eur. J. Dev. Psychol. 9, 446–452. doi: 10.1080/17405629.2012.690510
Cacioppo, J. T., Cacioppo, S., Capitanio, J. P., and Cole, S. W. (2015). The neuroendocrinology of social isolation. Annu. Rev. Psychol. 66, 733–767. doi: 10.1146/annurev-psych-010814-015240
Casal-Rodríguez, B., Rivera-Castiñeira, B., and Rodríguez-Míguez, E. (2023). The cost of unwanted loneliness in Spain. Available online at: https://www.soledades.es/sites/default/files/contenidos/Estudio%20El%20coste%20de%20la%20soledad%20no%20deseada%20en%20Espa%C3%B1a_3.pdf (accessed May 12, 2025).
Catalonia Red Cross (2022). First study on “Unwanted Loneliness.” Available online at: https://www2.cruzroja.es/documents/1043607101/1078461912/doc+presentaci%C3%B3+soledat+no+volguda+Observatori+%281%29+%281%29_compressed.pdf/793facea-b75b-892e-a22f-2320abe2de45?t=1663601991393andutm_campaign=observatori+Soledat+1andutm_medium=emailandutm_content=catandutm_source=Cat_voluntariat_socis (accessed May 12, 2025).
Díez Nicolás, J., and Morenos Páez, M. (2015). Loneliness in Spain. Fundación ONCE y de la Fundación AXA. Available online at: https://www.fundacionseres.org/Lists/Informes/Attachments/995/151127%20La%20Soledad%20en%20Espa%C3%B1a.pdf (accessed May 12, 2025).
Dumont, M., Blanchet, L., and Tremblay, P. H. (1990). La solitude chez les jeunes: recension des écrits. Santé Ment. Québec 15, 129–148. doi: 10.7202/031566ar
Echeburúa, E., and De Corral, P. (2010). Adicción a las nuevas tecnologías y a las redes sociales en jóvenes: un nuevo reto. Adicciones 22:91. doi: 10.20882/adicciones.196
Engel, G. L. (1977). The need for a new medical model: a challenge for biomedicine. Science 196, 129–136. doi: 10.1126/science.847460
Galloway, A. (2005). Non-probability sampling. Encycl. Soc. Meas. 2, 859–864. doi: 10.1016/B0-12-369398-5/00382-0
Gené-Badia, J., Ruiz-Sánchez, M., Obiols-Mas,ó, N., Oliveras Puig, L., and Lagarda Jiménez, E. (2016). Aislamiento social y soledad: ‘qué podemos hacer los equipos de atención primaria? Aten. Prim. 48, 604–609. doi: 10.1016/j.aprim.2016.03.008
Government of Aragon (2023). Study on mental health and use of social networks in students of the university of Saragossa. Available online at: http://prensa.unizar.es/notasprensa/anexos/0_estudio_salud_mental.pdf
Hernan-Montalban, M. J., and Rodríguez-Moreno, S. I. (2017). Unwanted loneliness in the city of Madrid. Results report 2017. Available online at: https://madridsalud.es/pdf/Soledad_ciudaddeMadrid.pdf (accessed May 12, 2025).
Holt-Lunstad, J., Smith, T. B., Baker, M., Harris, T., and Stephenson, D. (2015). Loneliness and social isolation as risk factors for mortality. Perspect. Psychol. Sci. 10, 227–237. doi: 10.1177/1745691614568352
IAB Spain (2023). Social media study 2023. Available online at: https://iabspain.es/estudio/estudio-de-redes-sociales-2023/ (accessed May 12, 2025).
Jo Cox Commission (2017). Combatting loneliness one conversation at a time: a call to action. Available online at: https://www.jocoxfoundation.org/wp-content/uploads/2023/07/rb_dec17_jocox_commission_finalreport.pdf (accessed May 12, 2025).
Johnson, T. P. (2005). “Snowball sampling,” in Encyclopedia of Biostatistics, eds. P. Armitage and T. Colton (John Wiley & Sons, Ltd.). doi: 10.1002/0470011815.b2a16070
Luhmann, M., and Hawkley, L. C. (2016). Age differences in loneliness from late adolescence to oldest old age. Dev. Psychol. 52, 943–959. doi: 10.1037/dev0000117
Maes, M., Qualter, P., Vanhalst, J., Van den Noortgate, W., and Goossens, L. (2019). Gender differences in loneliness across the lifespan: a meta–analysis. Eur. J. Pers. 33, 642–654. doi: 10.1002/per.2220
Mann, F., Wang, J., Pearce, E., Ma, R., Schlief, M., Lloyd-Evans, B., et al. (2022). Loneliness and the onset of new mental health problems in the general population. Soc. Psychiatry Psychiatr. Epidemiol. 57, 2161–2178. doi: 10.1007/s00127-022-02261-7
Martín Roncero, U., and González-Rábago, Y. (2021). Soledad no deseada, salud y desigualdades sociales a lo largo del ciclo vital. Gac. Sanit. 35, 432–437. doi: 10.1016/j.gaceta.2020.07.010
Martins Barroso, S., Silva e Sousa, A. A., and dos Santos Rosendo, L. (2023). Impact of loneliness on the quality of life of university students in Minas Gerais. Psychol. Sci. Profess. 43:e243909. Available online at: https://www.scielo.br/j/pcp/a/P8nLnZPQxtPRp5z8vyy7PGr/
Masi, C. M., Chen, H.-Y., Hawkley, L. C., and Cacioppo, J. T. (2011). A Meta-analysis of interventions to reduce loneliness. Personal. Soc. Psychol. Rev. 15, 219–266. doi: 10.1177/1088868310377394
Matthews, T., Danese, A., Gregory, A. M., Caspi, A., Moffitt, T. E., and Arseneault, L. (2017). Sleeping with one eye open: loneliness and sleep quality in young adults. Psychol. Med. 47, 2177–2186. doi: 10.1017/S0033291717000629
McIntyre, J. C., Worsley, J., Corcoran, R., Harrison Woods, P., and Bentall, R. P. (2018). Academic and non-academic predictors of student psychological distress: the role of social identity and loneliness. J. Ment. Health 27, 230–239. doi: 10.1080/09638237.2018.1437608
Ministerio de Educación y Formación Profesional (2023). Datos y cifras. Curso escolar 2022-2023. Available online at: https://www.educacionfpydeportes.gob.es/servicios-al-ciudadano/estadisticas/indicadores/cifras-educacion-espana/2022-2023.html (accessed May 12, 2025).
Ministerio de Universidades (2023). Estadística de Estudiantes Universitarios (EEU). Curso 2022-2023 (Avance). Available online at: https://www.universidades.gob.es/wp-content/uploads/2023/06/Principales-resultados_EEU_2022-23.pdf (accessed May 12, 2025).
Montero, M., López, L., and Sánchez-Sosa, J. J. (2001). La soledad como fenómeno psicológico: un análisis conceptual. Salud Ment. 24, 19–27. Available online at: https://www.medigraphic.com/pdfs/salmen/sam-2001/sam011d.pdf
Núñez, E., Steyerberg, E., and Núñez, J. (2011). Estrategias para la elaboración de modelos estadísticos de regresión. Rev Esp Cardiol. 64, 501–507. doi: 10.1016/j.recesp.2011.01.019
Pearce, E., Myles-Hooton, P., Johnson, S., Hards, E., Olsen, S., Clisu, D., et al. (2021). Loneliness as an active ingredient in preventing or alleviating youth anxiety and depression: a critical interpretative synthesis incorporating principles from rapid realist reviews. Transl. Psychiatry 11:628. doi: 10.1038/s41398-021-01740-w
Pedroso-Chaparro, M., del, S., Márquez-González, M., Fernandes-Pires, J.-A., Gallego-Alberto, L., Jiménez-Gonzalo, L., et al. (2022). Validation of the Spanish version of the Three-Item Loneliness Scale [Validación de la versión española de la Escala de Soledad de Tres Ítems]. Stud. Psychol. 43, 311–331. doi: 10.1080/02109395.2021.1989889
Pérez, M., and Quiroga-Garza, A. (2019). Uso compulsivo de sitios de redes sociales, sensación de soledad y comparación social en jóvenes. Redes. Rev. Hisp. Para E. Anál. Redes Soc. 30, 68–78. doi: 10.5565/rev/redes.809
Sheffield Hallam University (2022). Campaign to end loneliness. Evaluation and measurement. Available online at: https://www.campaigntoendloneliness.org/evaluation/ (accessed May 12, 2025).
Smith, W. (2008). Does gender influence online survey participation? A Record-linkage analysis of university faculty online survey response behavior [San José State University]. Available online at: https://eric.ed.gov/?id=ED501717
Sota-Velásquez, A., Maldonado-López, M., Ytuza-Cusirramos, M., Cornejo-Torres, M., del, C., and Cusirramos-Carpio, Y. (2021). Uso excesivo del celular, calidad de sueño y soledad en jóvenes de la ciudad de Arequipa. Rev. Psicol. 11, 207–223. doi: 10.36901/psicologia.v11i1.1368
State Observatory of Unwanted Loneliness (SoledadES) (2022). Study on the perception of unwanted loneliness. Available online at: https://www.soledades.es/sites/default/files/contenidos/Informe_percepcion_social_soledad_v2.pdf (accessed May 12, 2025).
Steptoe, A., Shankar, A., Demakakos, P., and Wardle, J. (2013). Social isolation, loneliness, and all-cause mortality in older men and women. Proc. Nat. Acad. Sci. 110, 5797–5801. doi: 10.1073/pnas.1219686110
Szapu, E., Sulca, E. M., de los, Á., and Arevalos, D. H. (2022). El dolor social en tiempos de pandemia. Miedo y soledad de jóvenes estudiantes ante la pérdida de soportes afectivos. Rev. Educ. Polít. Soc. 7, 299–325. doi: 10.15366/reps2022.7.2.013
Thomas, L., Orme, E., and Kerrigan, F. (2020). Student loneliness: the role of social media through life transitions. Comput. Educ. 146:103754. doi: 10.1016/j.compedu.2019.103754
Tuñón, A., José, J., Fresno, M., Fernando, G., and Río Hernández, D. (2023). Estudio sobre juventud y soledad no deseada en España. Observatorio Estatal de La Soledad No Deseada. Available online at: https://www.soledades.es/ (accessed May 12, 2025).
Valtorta, N. K., Kanaan, M., Gilbody, S., Ronzi, S., and Hanratty, B. (2016). Loneliness and social isolation as risk factors for coronary heart disease and stroke: systematic review and meta-analysis of longitudinal observational studies. Heart 102, 1009–1016. doi: 10.1136/heartjnl-2015-308790
Wilkialis, L., Rodrigues, N. B., Cha, D. S., Siegel, A., Majeed, A., Lui, L. M. W., et al. (2021). Social isolation, loneliness and generalized anxiety: implications and associations during the COVID-19 quarantine. Brain Sci. 11:1620. doi: 10.3390/brainsci11121620
World Health Organization (2023). Loneliness and social isolation are health risks. Available online at: https://www.who.int/multi-media/details/loneliness-and-social-isolation-are-health-risks (accessed May 12, 2025).
Keywords: teenagers, young adults, loneliness, health, mental health
Citation: Hernández-Díaz R, Navarro-Vásquez L, Aguilar-Latorre A, Méndez-López F, Gascón-Santos S and Magallón-Botaya R (2025) Analysis of young students' perception of loneliness: a cross-sectional study. Front. Psychol. 16:1553490. doi: 10.3389/fpsyg.2025.1553490
Received: 30 December 2024; Accepted: 22 May 2025;
Published: 24 June 2025.
Edited by:
Manuel Gómez-López, University of Murcia, SpainReviewed by:
Anubhuti Dubey, Deen Dayal Upadhyay Gorakhpur University, IndiaCodruta Alina Popescu, University of Medicine and Pharmacy Iuliu Hatieganu, Romania
Copyright © 2025 Hernández-Díaz, Navarro-Vásquez, Aguilar-Latorre, Méndez-López, Gascón-Santos and Magallón-Botaya. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alejandra Aguilar-Latorre, YWFndWlsYXJAdW5pemFyLmVz
†These authors have contributed equally to this work and share first authorship