 Patrícia M. Pascoal1,2,3,4*
Patrícia M. Pascoal1,2,3,4* Gerhard Andersson1,5,6,7
Gerhard Andersson1,5,6,7 Vinicius J. Fischer8,9
Vinicius J. Fischer8,9 Andreia A. Manão1Cátia Oliveira1Catarina F. Raposo1,4Pedro J. Rosa1,10
Andreia A. Manão1Cátia Oliveira1Catarina F. Raposo1,4Pedro J. Rosa1,10 Magda Sofia Roberto11Graça Santos12
Magda Sofia Roberto11Graça Santos12 Nuno Tomada13,14Annamaria Giraldi15,16
Nuno Tomada13,14Annamaria Giraldi15,16- 1Lusófona University, HEI-Lab: Digital Human-Environment Interaction Labs, Lisbon, Portugal
- 2Clínica Universitária de Psiquiatria e Psicologia Médica, Faculdade de Medicina, Universidade de Lisboa, Lisbon, Portugal
- 3PSYLAB, Instituto de Saúde Ambiental (ISAMB), Faculdade de Medicina, Universidade de Lisboa, Lisbon, Portugal
- 4Center for Psychology at the University of Porto, Faculty of Psychology and Educational Sciences of the University of Porto, Porto, Portugal
- 5Department of Behavioural Sciences and Learning, Department of Biomedical and Clinical Sciences, Linköping University, Linköping, Sweden
- 6Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden
- 7Department of Health, Education and Technology, Luleå University of Technology, Luleå, Sweden
- 8Centre Hospitalier Neuro-Psychiatrique (CHNP), Rehaklinik, Zentrum fir Psychotherapie, Ettelbruck, Luxembourg
- 9University of Luxembourg, Student Services, Esch-sur-Alzette, Luxembourg
- 10Instituto Superior Manuel Teixeira Gomes, Portimão, Portugal
- 11CICPSI—Centro de Investigação em Ciência Psicológica, Faculdade de Psicologia, Universidade de Lisboa, Lisbon, Portugal
- 12Hospital da Luz, Odivelas, Portugal
- 13Instituto de Investigação e Inovação em Saúde, Porto, Portugal
- 14School of Psychology and Life Sciences (EPCV) of Lusófona University, Lisbon, Portugal
- 15Sexological Clinic, Mental Health Center Copenhagen, Copenhagen University Hospital, Copenhagen, Denmark
- 16Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark
Introduction: Sexual distress is interrelated with mental health and relationship quality and is fundamental for establishing a diagnosis of sexual dysfunction, even though it also affects people who do not seek professional clinical help. Research on sexual distress related to partnered sexual activity is limited, and no comprehensive model exists to guide research or clinical interventions. We conducted an online cross-sectional qualitative study to: 1) explore the reasons why people experiencing sexual distress in partnered face-to-face sexual activity do not seek professional clinical help; 2) analyze the experiences of participants’ of sexual distress in partnered sexual activity; 3) reflexively compare the experiences reported by participants who seek and do not seek professional help; and 4) reflexively compare experiences across genders.
Methods: We performed reflexive thematic analysis on 438 heterosexual people answers (Mage = 41.06, SD = 12.19), including 306 women (69.7%) and 132 men (30.1%).
Results: Most participants (54.1%) had not sought professional clinical help but wanted to do so. Some participants (13.2%) expressed a desire for clinical consultations but reported financial or time constraints. Using the reflexive thematic analysis on the qualitative data provided, we created three themes: (1) Sexual (dys)function (It’s the function), which focuses on sexual function and lack of pleasure; (2) Intimacy dynamics (It’s us!), which discusses relationship challenges; (3) Intrapersonal struggles (It’s me!), which highlight individual factors, some influenced by social messages. Comparison across groups revealed that people who sought professional clinical help emphasise genital function and negative emotions, and women highlighted experiencing sexual pain, while men emphasised desire discrepancies and erectile disorder.
Discussion: Our results demonstrate that difficulties related to sexual pleasure and with penetrative sex are important sources of distress in partnered sexual activity, which is in line with DSM and ICD frameworks of sexual dysfunction. Participants’ accounts show that pre-existing psychological characteristics, partnered communication, cognitive, and emotional factors are key factors to shape the experience of sexual distress related to sexual dysfunctions. This has implications for clinical work as interventions should target transdiagnostic individual factors that may not be sexual specific (e.g., repetitive negative thinking) as well as couple-level factors (e.g., communication). Internet-based integrative therapies directed at these factors may be a promising venue for those who experience sexual distress with partnered sexual activity and are reluctant to seek in-person sexual healthcare.
1 Introduction
According to DSM-5-TR (American Psychiatric Association, 2022) and ICD-11 (World Health Organization, 2019), the experience of some level of sexual distress is an essential condition to establish a diagnosis of sexual dysfunction, and different researchers and clinicians have advocated for its essential role in the experience of sexual dysfunction (Hendrickx et al., 2013). Distress related to face-to-face partnered sexual activity is essentially linked to problems with sexual function (Zheng et al., 2020) and, despite its crucial significance in clinical settings, can also be found in community samples (Zheng et al., 2020). In both contexts (i.e., clinical settings, community samples), the experience of sexual distress related to sexual function in the context of face-to-face partnered sexual activity is associated with poorer mental health (e.g., Ventus et al., 2017) and poorer relationship quality (e.g., Nickull et al., 2022), which establishes it as an important correlate of people’s overall health. Understanding the nuances of sexual distress, namely distress related to face-to-face partnered sexual activity and why people do not seek health services contributes to the Sustainable Development Goals of the United Nations (United Nations, 2015), specifically to Goal 3: Good Health and Well-Being For All.
Research developed worldwide consistently demonstrates that not everyone experiencing distressing sexual problems actively seeks or receives clinical professional help. In a study developed in Europe, America, Africa, Asia, and Australia, data were collected in 31 countries (Moreira et al., 2005) and found that among those who experienced a sexual problem, only 18.0% of men and 18.8% of women had sought medical help. According to Moreira et al. (2005), the reasons for participants not seeking professional help were some beliefs, such as considering sexual problems a normal part of ageing, doubting a doctor’s ability to help, or lacking the confidence to discuss these issues with healthcare providers. Other research, meanwhile, developed in France (Buvat et al., 2009), the United States (Laumann et al., 2009), Belgium (Hendrickx et al., 2016a, 2016b) and Canada (Lafortune et al., 2023) report similar data, confirming most of those with sexual problems reported to be distressed. Still, most of them did not seek professional clinical help. While the reasons for avoiding professional help may vary (e.g., low level of distress, long waiting lists), many individuals experience distressing sexual problems without having clinical support. Considering this data, a comprehensive approach to sexual distress needs to include reports and knowledge derived from people in clinical settings (patients and professionals) but also from those who are not receiving professional help, receiving professional help and nonetheless experience distress and distress and may be compatible with or at risk for a formal clinical diagnosis but remain understudied.
Sexual distress is an umbrella concept and has been defined in multiple ways. For example, Witting et al. (2008, p. 5288) state that sexual distress is “characterized by negative feelings and anxiety about one’s sexuality or sexual activities” and Hendrickx et al. (2016a, 2016b, p. 1662) define it as “distress that is experienced due to a sexual impairment.” Furthermore, sexual distress has been assessed using multiple measures that are aligned with different visions of the concept. For example, the Sexual Satisfaction Scale for Women (SSS-W, Meston and Trapnell, 2005) describes sexual distress as distress about sexual self-concerns, and the widely used Sexual Distress Scale-Revised (SDS-R, Derogatis et al., 2008; Santos-Iglesias and Walker, 2018) describes it as sexuality related personal distress (e.g., distress about sex life). Some other studies that measure sexual distress do not use a scale and instead ask questions such as “During the past 4 weeks, how much distress or worry has your own sexuality caused you?” (Bancroft et al., 2003) or “For each type of impairment reported, women can indicate whether impairment is causing them personal, perceived partner, and interpersonal distress” (Hendrickx et al., 2016a, 2016b). This diversity reveals the various perspectives that researchers can take and reveals the inherent difficulties with providing a basis for comparison across studies, as well as developing an empirical ground to sustain a comprehensive model of sexual distress, namely of sexual distress in partnered face-to-face sexual activity.
Recent research using the SDS-R has demonstrated that sexual distress and psychological distress are statistically significantly associated, but not to the extent that may be considered equivalent dimensions (Raposo et al., 2023; Raposo et al., 2025). The proximity among these two concepts (psychological distress and sexual distress) may be the reason why sexual dysfunctions, characterized by the experience of sexual distress, can be included in the internalizing spectrum of psychopathology (Forbes and Schniering, 2013; Forbes et al., 2016) which is in line with a dimensional approach to psychopathology that looks at common explanatory processes across disorders (Kotov et al., 2017). This view is corroborated by recent research that has found that emotional problems (e.g., depression; Ventus et al., 2017), transdiagnostic cognitive processes (e.g., worry; Pascoal et al., 2020) and difficulties with emotion regulation (Raposo et al., 2023) are related to sexual distress. However, due to the widespread use of the SDS-R, which adopts a generalist approach to measuring sexual distress, it remains unclear whether the identified transdiagnostic factors are specifically linked to sexual activity or to other types of sexual problems that may be a source of distress, such as discomfort with one’s sexual identity, which are not directly related to sexual activity.
The difficulties with describing with precision what sexual distress is have already been presented by diverse researchers (e.g., Hendrickx et al., 2013). Between 2008 and 2009, a project about how laypeople conceptualize distressing sexual problems developed in Portugal produced some preliminary data from different qualitative studies (Pascoal et al., 2008; Pascoal et al., 2009). These qualitative studies highlighted that people defined distressful sexual problems as problems with sexual function (e.g., “not having a good erection”), dissatisfaction with sexual life (e.g., “not having the type of sex I would like”), partner problems related to sexuality (e.g., “selfish partners that only want to reach orgasm and please themselves”), problems related to sexual orientation (e.g., “I find it difficult to find a place in the gay scene”) or gender identity (e.g., “I feel I live a lie, I wish I were a man”) or problems related to the preference for sexual practices (e.g., “my partner is not into kink, but I am”). Even though this exploratory preliminary set of studies was promising because they highlighted that sexual problems should be considered outside a focus on genital performance, their results were insufficient as they reflected a broad conception of sexual distress and did not address the specificity of sexual distress with partnered face-to-face sexual activity.
More recently, a study with clinical sexologists exploring how professionals approach sexual distress related to sexual function (SDRSF) (Raposo et al., 2024) showed that SDRSF is explained by problematic sexual function, as expected, but this is interrelated with individual emotional (e.g., emotional disorders) and cognitive (e.g., internalized sexual stigma) processes, as well as interpersonal (e.g., communication difficulties) and societal (e.g., media pressure) processes. This study focused specifically on distress related to sexual function and did not aim to address distress related to overall sexual activity. However, the results revealed though clinician’s answers moved beyond a strict focus on sexual function, suggesting a broader perspective to be taken. It highlighted that when approaching SDSRF a comprehensive approach that looks at factors involved in sexual distress related to partnered face-to-face sexual activity as a whole moving beyond a strict genital focus.
Despite its clinical relevance, research about sexual distress with partnered face-to-face sexual activity has been scarce, and there is no comprehensive model to understand it and, subsequently, guide research or clinical intervention. Previous research has explored sexual distress related to sexual activity in LGB + (i.e., lesbian, gay, bisexual, or other minoritized sexual orientations) individuals (Manão et al., 2023) and identified that this population faces specific distressing sexual problems—stemming from contextual and interpersonal factors—that go beyond the current criteria for ICD-11 (World Health Organization, 2019) and DSM-5 (American Psychiatric Association, 2022). In our current study, we aim to broaden the understanding of this field and expand the current knowledge by taking an experience-based approach by thoroughly examining how cis heterosexual people who self-report having distressing sexual problems during partnered face-to-face sexual activity describe this experience. The main research question we seek to answer is: “How is distressful partnered face-to-face sexual activity described by those who experience it?”. Complementarily, we aim to compare the answers of those who had and do not have sought professional clinical help. We will outline the reasons why our participants did not seek professional help and expand the knowledge derived from existing studies worldwide. We also intend to explore how experiences of partnered sexual distress may differ across genders. We intend to utilize an online qualitative methodology to gather data from diverse experiences, in line with Epstein’s (2023) argument that knowledge from non-experts may contribute to broadening and informing practices of citizenship, advocacy, and, in our view, healthcare practices. This approach is particularly valuable in fields such as sexology (Braun and Clarke, 2020), where qualitative studies can provide insights that enhance clinical practice and improve healthcare (e.g., Paulsen et al., 2023; Raposo et al., 2024) for individuals experiencing sexual distress in partnered face-to-face sexual activity.
2 Materials and methods
2.1 Participants
The study included 438 heterosexual participants (Mage = 41.1, SD = 12.2) who self-identified as having distressing sexual problems during partnered face-to-face sexual activity, of which 306 self-identified as ciswomen (69.9%) and 132 as cismen (30.1%). Regarding the relational configuration, 331 were in a monogamous relationship (75.6%), 56 stated that they did not have significant/s relationship/s (12.8%), 29 were having casual relationships (6.6%), 14 were in “Other not mentioned” (3.2%), and 8 were in a non-monogamous relationship (1.8%). Regarding nationality, 422 participants were Portuguese (95.13%) 12 were Brazilian (2.73%), 1 participant was Argentinian (0.23%), 1 was Cabo Verdian (0.23%), 1 was Finnish (0.23%), 1 was from EUA (0.23%), and 1 stated “I prefer not to say” (0.23%).
Of all participants, 157 identified as Catholic (37.7%), 135 declared themselves Atheist (32.5%), 28 indicated that they identified with “another option” (6.7%), 26 opted to state that they preferred not to answer, 63 identified as Agnostic (15.1%), 5 as Protestant (1.2%), 1 as Orthodox Christian (0.2%), and 1 as Hindu (0.2%).
Concerning the participants’ educational level, our data indicates that 169 individuals have attained an university degree (40.6%), 130 have pursued postgraduate studies (31.3%), 75 have completed secondary education (18%), 32 have participated in technical or vocational training courses (7.7%), 8 have attained the ninth grade (1.9%), 1 has not reached the ninth grade (0.2%), and 1 participant did not respond to this question (0.2%).
2.2 Dataset generation
The current study is part of a larger cross-sectional, online, mixed-methods project on sexual distress. It employed participatory design techniques (Cornwall and Jewkes, 1995) and involved collaboration with MUSEX – the Pedagogical Museum for Sex, Associação Gerador, and sex therapists certified by the Portuguese Society of Clinical Sexology (SPSC). These sex therapists provided expertise by reviewing the project’s content to ensure it was relevant, inclusive, and appropriately concise. Additionally, we sought feedback from laypeople, including LGBTQIA+ people, to review the inclusive language used in the project. We chose online recruitment by mutual agreement to expand our geographic reach and make participation more accessible and less time-consuming (Terry and Braun, 2017). After appreciation and approval by from all people involved, the study was disseminated online on different social media (e.g., Instagram, LinkedIn) through the research team’s professional accounts, by different groups in social media and through a collaboration with (MUSEX - the Pedagogical Museum for Sex, Associação Gerador, the Master’s Degree in Sexology at Universidade Lusófona, and SPSC), which also advertised the study on their social media. Following the advice of Braun et al. (2020), both the qualitative and quantitative content of the questionnaire were tested with individuals from the general population to confirm its clarity and comprehensibility before advertising the study. Using a snowball-like sampling technique, participants were also invited to share the questionnaire with others. Due to these recruitment strategies, we do not know how many people the study reached. We followed the qualitative research guidelines, recognising that it is problematic to determine a priori an ideal number of participants. Consequently, we did not prioritise a specific participant composition but focused on obtaining informative answers (Sim et al., 2018). Data was generated between March 9, 2023, and October 21, 2024.
In the larger cross-sectional, online, mixed-methods project, when accessing the study’s URL, participants were asked to read the informed consent in the first part of the survey and then provide their agreement or disagreement regarding participation. The second part of the survey involved answering a sociodemographic questionnaire. The third and final part of the survey had quantitative and qualitative questions. For the current study, we selected people who met two inclusion criteria: (1) self-identification as a heterosexual cisgender person and (2) self-reporting as having one or more distressing sexual problems during face-to-face sexual activity. We defined sexual activity as “sexual activity refers to mutual stimulation of genitals, oral sex, anal sex, intercourse, and other forms of face-to-face sexual stimulation” (Dove and Wiederman, 2000). We asked people about their help-seeking behavior in the context of their distress related to face-to-face sexual activity. “Our aim was to understand the context of distressing sexual problems related to partnered face-to-face sexual activity of heterosexual people, so we presented the following open question that we analyzed: Can you please describe your distressful experience with partnered face-to-face sexual activity?”.
The Ethical and Deontological Committee of the Ethical and Deontological Committee for Scientific Research of the School of Psychology and Life Sciences (CEDIC) of Lusófona University in Lisbon approved the study. All the ethical and deontological guidelines were followed, namely, the Helsinki Declaration and the European Textbook on Ethics in Research (European Commission: Directorate-General for Research and Innovation, 2010). All IP and geolocation information was deleted, and only the research team has access to the database, which is password protected. The informed consent indicated that the data set would not be shared and provided additional details about the study (e.g., aim, duration, no financial compensation). At both the beginning and end of the questionnaire, the contact details of the principal researcher were provided, along with a list of contacts for clinical and sexual support, should participants feel it would be beneficial to access them.
2.3 Reflexive statement
The following reflexive statement follows Braun & Clarke’s guidelines (Braun and Clarke, 2024) and refers to the people involved in the reflexive thematic analysis and the roles and activities they were performing during this analytical process.
Patrícia M. Pascoal is a cisgender Portuguese woman. She holds a European PhD in Clinical Psychology, teaches undergraduate students, and supervises postgraduate students pursuing master’s and doctoral degrees in medicine, psychology and sexology using qualitative and quantitative research methods. She also has experience in clinical practice in psychology and sexology as a cognitive-behavioral therapist (CBT) and CBT supervisor. She is involved in the executive boards and committees of diverse national (e.g., Portuguese Association for Behavioral Therapy) and international scientific associations (e.g., European Federation of Sexology; International Society for Sexual Medicine).
Andreia A. Manão is a cisgender woman from Portugal. She is pursuing her PhD in Clinical Psychology (CBT), focusing on both quantitative and qualitative research methods, while also receiving clinical training to become a clinical psychologist and sex therapist. Additionally, she teaches courses in the Bachelor’s program in Psychology and the Master’s programme in Sexology.
Catarina F. Raposo is a cisgender woman and a PhD candidate in human sexuality. She has experience in clinical practice within psychology and sexology and is currently training to become a clinical CBT therapist. She is a non-tenured invited lecturer, teaching mental health and sexology-related topics. Her role also includes supervising students pursuing master’s degrees in psychology and sexology during their internships.
2.4 Data analysis
We used SPSS 27 (IBM SPSS) for descriptive statistics (e.g., average age and standard deviation) and Microsoft Word for the reflexive thematic analysis.
The answers about having had/sought professional help were subjected to summative content analysis (Hsieh and Shannon, 2005) and were consolidated with the procedures for qualitative coding (Zhang and Wildmuth, 2009).
Regarding the qualitative answers to distressing sexual problems related to face-to-face sexual activity, we analyzed the data using reflexive thematic analysis to understand meaningful patterns in participants’ responses (Braun and Clarke, 2021). We adopted a contextual perspective, acknowledging that experiences are subjective (Braun and Clarke, 2022), meaning that the analysis occurs at the intersection of the researchers, the data and broader contexts. Our analysis was mainly inductive but also shaped by our knowledge and experience in psychology and/or sexual health content and related issues, making it, in this sense, also deductive. We followed the guidelines of reflexive thematic analysis (Braun and Clarke, 2021), which involved familiarizing ourselves with the data as it was submitted to the Qualtrics platform (Provo, UT, United States)—i.e., an online, secure survey platform. We then copied the data into a Word document and began to code it at both a surface and a deeper level, that is, in a semantic and latent way, respectively. This process was performed independently and simultaneously by three researchers, Patrícia M. Pascoal, Andreia A. Manão, and Catarina F. Raposo. Subsequently, the analysis was compared and refined collaboratively through reflexive discussion until we achieved a cohesive understanding of the data. Different opinions were encouraged to improve our data analysis and discussion rather than to achieve consensus. Comparisons across genders regarding experiences of sexual distress during partnered face-to-face sexual activity were conducted and discussed. Of the 438 participants, 22 offered unclear responses about the distressing partnered face-to-face sexual activity (e.g., it’s tough). To ensure our analysis accurately represents participants’ views, we excluded these 22 responses from our reflexive thematic analysis. Answers about self-reported excessive sexual interest were not analysed (e.g., Every 16 seconds, I think about sex; 58 years, man, without professional help) as they are not related to distress related to partnered face-to-face sexual activity. Thus, we excluded more 10 answers from our reflexive thematic analysis. Consequently, we analyzed 406 responses related to the question concerning distressing partnered face-to-face sexual activity. When reporting answers, in the “Results” section, minor adjustments have been made to some sentences to enhance their clarity. However, it is essential to emphasise that the meaning of these sentences has been totally preserved.
According to Braun and Clarke (2024), it is not recommended to split the “Results” and the “Discussion” sections in papers with reflexive thematic analysis (2024). However, considering the journal’s template, the authors decided it was adequate to follow the journal’s guidelines and therefore, we will separate the “Results” from the “Discussion” section, a possibility acknowledged by Braun and Clarke (2021).
In the upcoming sections, themes will be emphasized in bold, subthemes will be underlined, and quotes will be italicized. Every quote example includes concise sociodemographic details about the participants to protect their anonymity, such as age, gender, and the status of their experience with professional clinical help related to sexual problems (indicated as “with professional help” for those who have professional clinical help, “without professional help” for those who have not, and “did not indicate professional help status” for those who did not provide an answer about it).
3 Results
We will first present the results that describe the context and reasons for people who had and do not have sought professional clinical help, and then we will proceed with the reflexive thematic analysis results.
3.1 Professional help
Considering whether the participants had sought professional clinical help, our analysis revealed that 237 participants (54.1%) had not yet attended but expressed a desire to do so. Meanwhile, 47 participants (10.7%) had already attended clinical sexology/sexual medicine sessions, 59 (13.5%) were attending at the moment of data collection, and 58 (13.2%) expressed a desire to attend but were unable to do so.
Table 1 describes the reasons for not seeking professional clinical help. Of the 58 participants who expressed a desire to attend but were unable to do so, 21 (36.2%) did not answer this question.
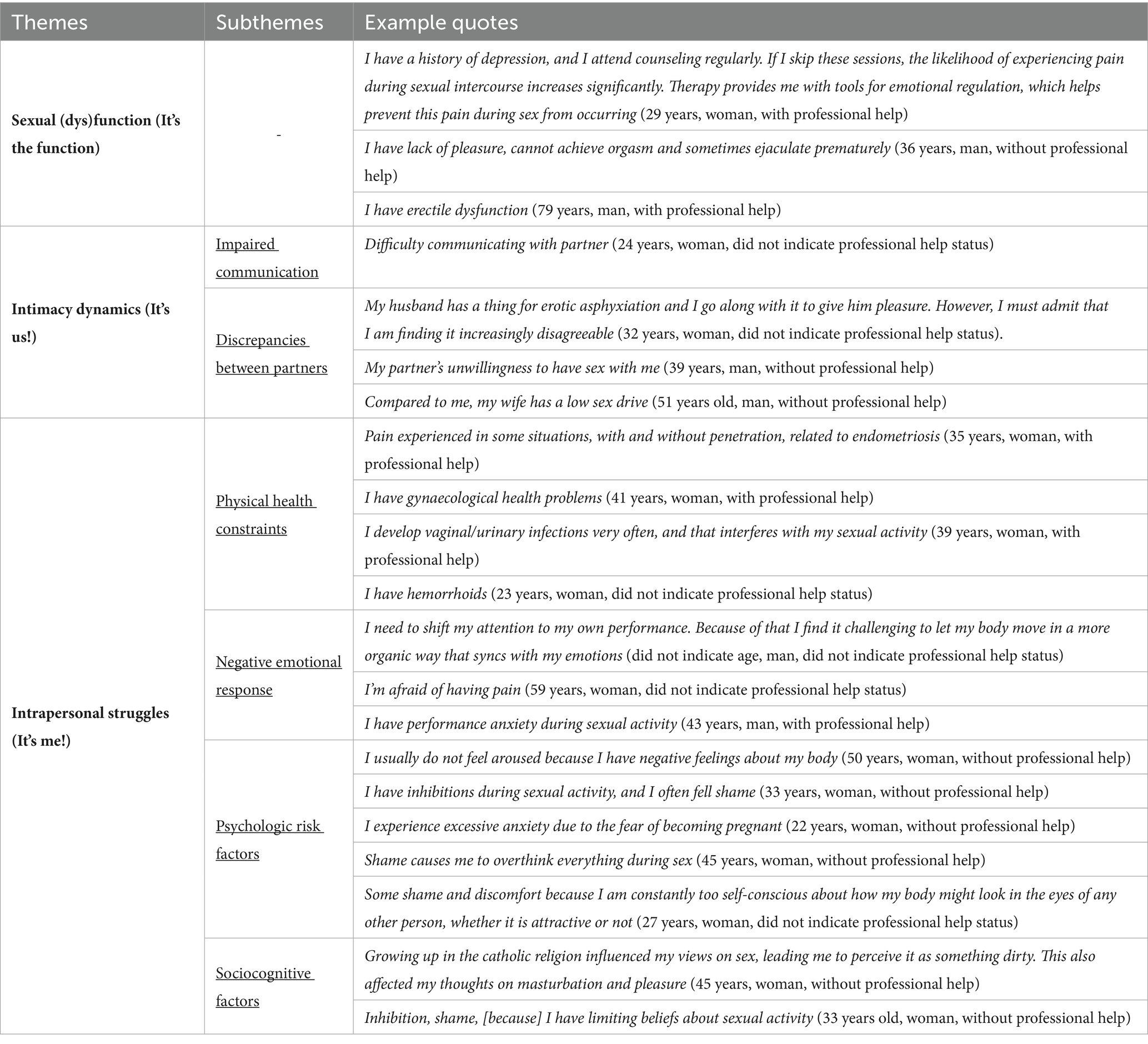
Table 1. Frequency of code regarding the reasons for being unable to attend clinical consultations.
3.2 Reflexive thematic analysis
The length of the answers varied, from short answers (i.e., two or three words; e.g., I have impotence; 68 years, man, with professional help) to rich and descriptive answers (i.e., several sentences and rich content, for example, I have a history of depression, and I go to therapy regularly. If I do not, the likelihood of having pain during sex again is significant. Therapy helps me to have emotional regulation tools so that this does not happen; 29 years, woman, with professional help).
The themes are globally interrelated, as answers aggregate contents from several themes and subthemes (e.g., My ex-boyfriend experienced premature ejaculation and erectile dysfunction. These issues contributed to the end of our relationship because he was unwilling to seek help and tell me about it. He even went as far as to take viagra without telling me. I only found out about this after we had not been sexually active for a while, and he began to feel unwell due to the increased heart rate caused by the stimulant) (Age not disclosed, woman, did not indicate professional help status).
In terms of seeking professional clinical help, our analysis revealed a pattern of help-seeking behavior among people reporting experiences of pain during sexual activity, sexual dysfunctions (e.g., premature ejaculation), and physical medical conditions (e.g., haemorrhoids). Conversely, the answer of people experiencing sexual problems characterized by partner dynamics (e.g., poor communication, differences in sexual desire between partners) seems to be associated with lesser inclination to seek professional help.
We will now describe each theme, its corresponding subtheme/s, and provide detailed information with examples in the text and in Table 2.
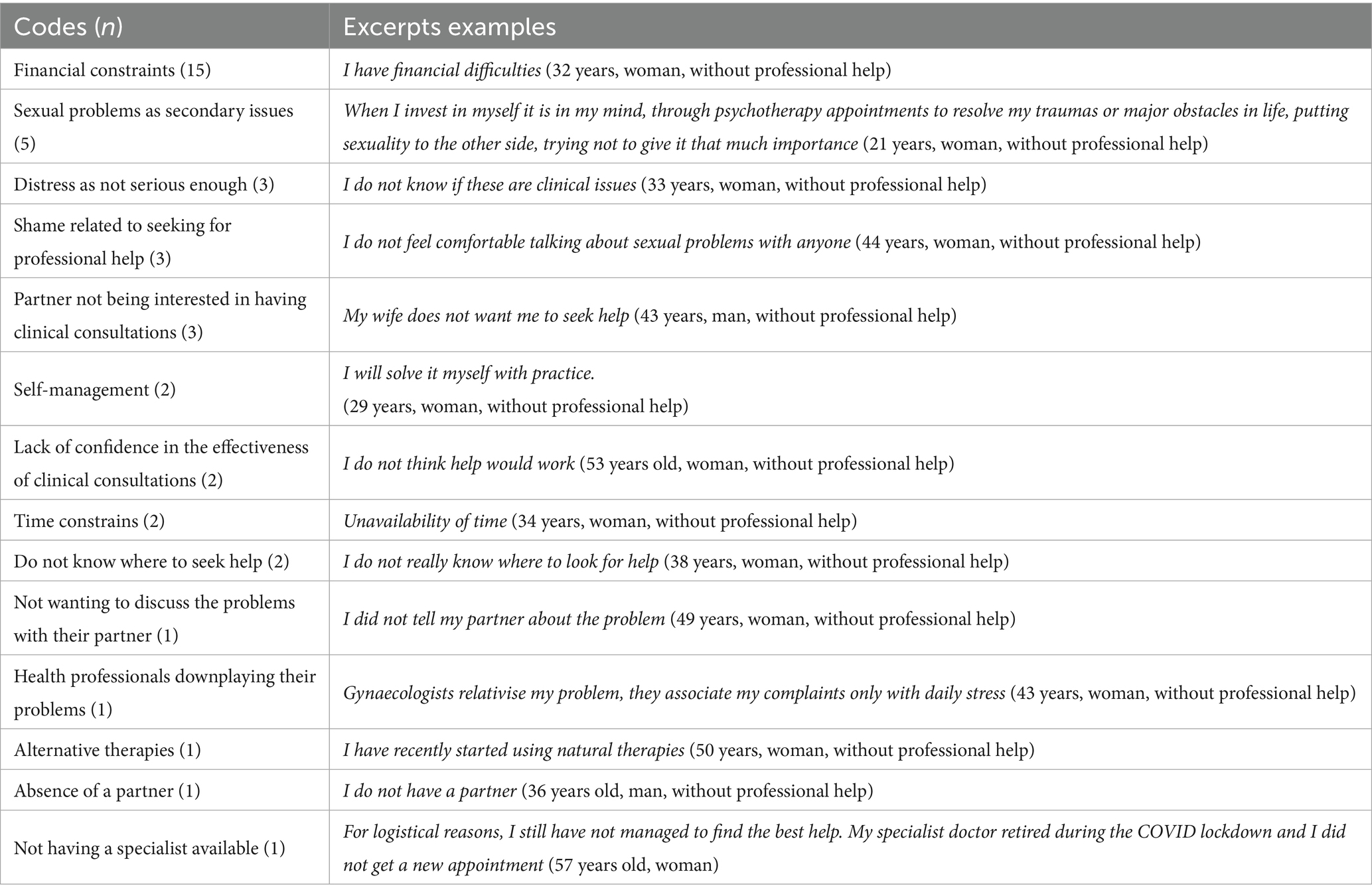
Table 2. Results from the reflexive thematic analysis.
The theme Sexual (dys)function (It’s the function) centers on distressing problems related to face-to-face sexual activity involving the genitals. These problems are typically described in terms that align with diagnostic criteria for sexual dysfunction, including erectile difficulties, premature ejaculation, challenges or inability to reach orgasm, lack of pleasure during sexual activity, pain during penetration, vaginismus, vulvodynia, and bleeding during vaginal penetration. This theme represents a key conceptual thread in the data and does not include subthemes.
The theme of Intimacy dynamics (it’s us!) includes distressing experiences grounded in a relationship. Its subthemes are Impaired Communication, which pertains to difficulties in self-disclosing oneself to the partner, and Discrepancies between partners, which describe problems in managing discrepancies related to sexuality, for example, sexual preferences and levels of sexual desire.
Finally, the theme of Intrapersonal struggles (it’s me!) aggregates descriptions of sexual distress with partnered face-to-face sexual activity that are related to individual characteristics, physical or psychological, of the respondent. A relationship may accentuate or diminish these characteristics, but they are not relationship-dependent. Its subthemes are: Physical health constraints that aggregates distress related to organic conditions that make sexual activity difficult (e.g., vaginal dryness, endometriosis, chronic pelvic pain, side effects of medications that affect sexual function); Negative emotional response a subtheme that pertains to negative emotional experiences during sexual activity (e.g., performance anxiety; fear); Psychological risk factors a subtheme that includes existing psychological traits that are risk factors for psychopathology and for psychological distress and that interfere with a complete experience of sexual activity (e.g., excessive anxiety/worry/fear, neuroticism, inhibition, feelings of inadequacy regarding one’s body); and Sociocognitive factors a subtheme specifically about negative attitudes towards sex and rigid beliefs derived from one’s education and socialization regarding what sexual activity should be (e.g., sex as dirty and immoral) that accentuate the distressful experience.
Concerning the participants’ gender, our analysis revealed distinct patterns. Among women, the predominant pattern was characterised by a lack of sexual desire, experiences of sexual pain, difficulties in achieving orgasms, and inadequate lubrication. In contrast, men exhibited a pattern of answers that emphasised premature ejaculation, erectile dysfunction, and a lack of interest from their partners in being involved in sexual activity.
Concerning the patterns of the content of the answers between people who had sought or not sought professional clinical help, our However, our study adds more layers to current formulations by emphasizing the professional clinical help present answers where relevance is placed on genital function together with a negative emotional experience, namely intense negative emotions related to sexual pain.
4 Discussion
This study analyzes self-reported experiences of people who self-identify has having sexual distress in partnered face-to-face sexual activity. It uses summative content analysis to describe and quantify their patterns of help-seeking. It has as a main goal to explore how people who self-report experiencing one or more sexual problems describe their sexual distress during face-to-face partnered sexual activities, utilizing reflexive thematic analysis to examine their responses. We will discuss the patterns of help-seeking behavior, the results of the reflexive thematic analysis, and the comparison across the answers across genders and between those who seek and do not seek professional.
A central theme that we developed, Sexual (dys)function (It’s the function), relates to the impairment of sexual distress response, a crucial aspect for the diagnosis of sexual dysfunction supporting current diagnosis manuals [ICD-11 (World Health Organization, 2019), DSM-5 (American Psychiatric Association, 2022)] and supporting that problems with sexual response are an essential precursor for sexual distress. However, our study adds more layers to current formulations by emphasizing the sexual distress related to the absence of pleasure. Sexual pleasure has gained attention due to its central role as a sexual right (World Association for Sexual Health, 2021), and its study has received immense attention in the last years, resulting in a comprehensive proposal for its understanding (Laan et al., 2021). Despite this interest, currently, sexual pleasure is modestly mentioned in category-based diagnosis manuals, and, except for its mention in sexual interest arousal problems, there is no solid and clear role for sexual pleasure as an central concept or a criterion that contributes to the diagnosis of a sexual dysfunction or problem. Taken together, the results of the current study and existing research on sexual pleasure (Laan et al., 2021; Manão et al., 2023; Pascoal et al., 2020) accentuate the need to integrate sexual pleasure as a fundamental factor in the assessment, intervention, and clinical research of distressful sexual problems related to partnered face-to-face sexual activity.
The theme named Intimacy dynamics (It’s us!) is in line with previous research that reinforces that relationship factors are fundamental for the experience of sexual distress (Martins et al., 2024). Our results identify the relationship elements that operate during partnered face-to-face activity, namely sexual communication and the existence of discrepancies among sexual preferences. Depending on the type of relationship, it is well known that both expressive and instrumental communication (MacNeil and Byers, 2009) are fundamental for positive outcomes, for example, sexual satisfaction (Frederick et al., 2016). However, most research about communication during sexual activity focuses on the role that “sexual talk” or “dirty talk” has as a maximizer of sexual arousal and promoting orgasm (Frederick et al., 2018). Our results complement this data by highlighting that inhibition to speak and challenges with sexual self-disclosure during sexual activity are also characteristics of during partnered face-to-face sexual activity. This implies that communication during sexual activity follows a dual path: while certain types of communication may enhance arousal and satisfaction, inhibition and difficulties in communicating may intensify the experience of distress. The latest may be particularly detrimental when difficulties in communicating with a partner about sexual pain lead to painful, distressing partnered sexual activity (Oesterling et al., 2025). Furthermore, our results also support the notion that discrepancies in sexual preferences (e.g., levels of desire or arousal for certain emotions or practices) (Dewitte et al., 2020; Cardoso et al., 2023) are characteristic of sexual distress during sexual activity. There is an interrelation between these two subthemes, as the ability to express preferences and communicate about discrepancies is important to overcome the negative impact that these discrepancies may have. Logically, those whose communication is compromised due to relational factors may have a heightened experience of distressing partnered sexual activity. Additionally, recognizing this discrepancy and the challenges in sexual communication may lead individuals to become cognitively distracted during sexual activity. This distraction arises from an increased focus on communication difficulties during sexual activity, which can undermine arousal and pleasure (Tavares et al., 2020). Our results highlight the role that communication behaviors and sexual self-disclosure skills (Döring and Byers, 2024) have in minimizing sexual distress with partnered sexual activity.
In the theme named Intrapersonal struggles (it’s me!), a puzzle of individual determinants is presented. If the experience of bodily-related difficulties, primarily due to illness or medication, is not a novelty as a determinant of distress (e.g., Zanolari et al., 2023), the participant’s descriptions accentuate that this sexual distress is marked and defined by the intense experience of negative emotions, namely experiences of anxiety and anguish. These descriptions are in line with research that places sexual dysfunctions and problems with partnered sexual activity as clinically meaningful experiences that can be approached clinically from a dimensional perspective within the spectrum of internalised disorders (Forbes et al., 2016). It is possible that these negative emotional experiences may interfere with the standard processing of arousal cues, particularly in assessing them. The vulnerability psychological factors developed in subtheme Psychologic risk factors (e.g., body awareness) seem to be traits or steady psychological characteristics that may be triggered or maximised during sexual activity. They may compromise the total immersion in the erotic experience, namely, by promoting cognitive distraction (Barlow, 2016), for example, distraction with one’s body appearance (Carvalheira et al., 2017; Dove and Wiederman, 2000; Manão and Pascoal, 2023; Pascoal et al., 2019). These steady cognitive characteristics and psychological traits frame cognitive processing during sexual activity, which is consistent with cognitive models of sexual dysfunction that defend that cognitive processes define and shape the erotic experience and are explanatory processes that define the experience of sexual dysfunction. Our results highlight that these processes also shape the experience of distress, accentuating it and aligning it with cognitive models of sexual dysfunction. Sociocognitive factors is a subtheme that is linked to socialization, encompassing negative messages that have been internalised about sexuality, which further compromise the sexual experience. These factors, commonly referred to as sexual beliefs, are significant components of cognitive models of sexual response (Nobre, 2023). These sexual beliefs, shared by men and women, tend to be rigid (Pascoal et al., 2018) and compromise complete immersion and openness to experience (Peixoto and Nobre, 2017). They play a crucial role as predictors of negative sexual experiences as they disrupt attentional focus during sexual activity by promoting ongoing surveillance of the experience in accordance with these beliefs, potentially undermining the whole experience of satisfactory arousal. In the current study, it is emphasised that social norms and beliefs may also impact the experience of distress.
The current results refine the clinical meaning of sexual distress with partnered face-to-face sexual activity, differentiating it from sexual distress as a global concept and from psychological distress and describing its unique features. It has important implications for theory building, sex therapy/clinical intervention, and clinical research. The study highlights that sexual distress with partnered face-to-face sexual activity is a detrimental sexual outcome associated with strong negative emotions essentially related to sexual response, personal physical difficulties (e.g., illness) and psychological factors (e.g., shame, body dissatisfaction) that promote cognitive distraction during sexual activity, problems with partnered communication about sexual preferences and discrepancies and negative attitudes and rigid beliefs about sexual activity. These factors point to the direction of a comprehensive theoretical model of sexual distress related to sexual activity that includes SDRSF and conceals conceals both cognitive (Barlow, 2016; Nobre and Barlow, 2023) as well as relationship factors (Martins et al., 2024). We propose that, following a top-down approach, a flexible, integrative, and comprehensive theoretical model of distress with partnered face-to-face partnered sexual activity should integrate SDRSF features namely: the experience of some level of impairment and negative emotions related to sexual function and response, including difficulties in experiencing pleasure and satisfaction; discrepancies between partner desires and preferences as well as difficulties in expressing and communicating about sexuality with partners; and both non-sexual related (body dissatisfaction, inhibition, neuroticism) and sexual-related (rigid negative beliefs) personal characteristics, some of which are derived from broader cultural contexts (e.g., family, religion). Integrating our findings and overcoming the limitations of this and previous research will contribute to establishing such an endeavour.
In terms of implications for sex therapy/clinical intervention, the current study calls for attention to the need to develop integrative approaches that address negative emotions (e.g., anxiety) that we found associated with sexual distress with partnered face-to-face sexual activity. These emotions are often maintained by latent psychological factors such as neuroticism and may benefit from transdiagnostic approaches to emotional problems (Sauer-Zavala et al., 2017) Interventions should include cognitive processes, such as CBT (Brotto et al., 2025) particularly those tailored to sexual dysfunction in the context of illness (Pieramico et al., 2024). Additionally, couple-focused and systemic interventions that target relationship dynamics, particularly fostering positive and respectful communication about sexual discrepancies, are also recommended (Davies et al., 2021). This raises important issues related to the education of sexual health professionals, namely sex therapists, reinforcing that addressing sexual dysfunctions requires a solid training background that needs to be combined with deep knowledge of relevant, empirically based theoretical models of intervention to ground best standards for clinical practice. Furthermore, sex therapists should complement it with professional updates in relevant techniques. The current results therefore support that professional education in sex therapy should be grounded in pre-existing formal training in relevant psychotherapies and should include content related to mental health, psychopathology, CBT approaches, and integrative and systemic models of intervention. Regarding research, the most significant impact of the current study pertains to the development of randomized controlled trials (RCTs) to intervene in sexual dysfunction or partnered face-to-face sexual activity related problems, as these need to be integrative and focus on a “an adequate” outcome measure of sexual distress. This measure should address sexual response issues while also being sensitive to therapeutic change, such as the SFEQ (Mitchell et al., 2022), which aligns more with our current findings. However, it also needs to incorporate secondary outcome measures, including sexual pleasure (Manão et al., 2023; Martins et al., 2024) and assessments of negative emotional experiences, such as anxiety and depression (Soler et al., 2021). Furthermore, future interventions should target processes known to influence negative emotional states (e.g., repetitive negative thinking) and the features and maintaining processes of sexual distress with partnered sexual activity that can be altered through therapeutic means (e.g., cognitive distraction, communication skills, sexual beliefs/psychological flexibility). It is important to note that the existing RCTs are aimed at specific clinical conditions (e.g., Banbury et al., 2021; Brotto et al., 2021) and that the results of this study support the possibility of crossdiagnostic RCTs, i.e., RCTS aimed at people with different diagnoses of sexual dysfunctions. At the same time, it is also highlighted that gender differences may be considered in designing such RCTs as women and men participants in crossdiagnostic interventions may differ in their complaints.
As our results highlight, many reasons that prevent people from seeking professional clinical help are related to accessing professional sexual healthcare (such as shame about sexual issues, cost, and geographic distance), we propose that developing internet interventions (whether blended or not) may be a practical solution for delivering pilot studies that incorporate such integrative transdiagnostic-based approaches. Regarding the reasons for not seeking professional clinical help, our results are in line with research in the field, revealing that most people who experience a sexual problem related to partnered face-to-face sexual activity do not seek professional help (e.g., Lafortune et al., 2023; Moreira et al., 2005), namely due to time and financial constraints.
Furthermore, this research reveals that institutional and professional trust-related factors prevent people from seeking help. It would be important to better understand if these factors are related to reports of bad experiences or just a lack of knowledge about the ongoing education and certification that exists in the field of clinical sexology and sex therapy and/or about existing specialized services that exist in Portugal (Alarcão et al., 2017; Raposo et al., 2024). The lack of confidence in specialized services and the pursuit of alternative approaches render people who suffer from sexual problems vulnerable to the practice of non-evidence-based practices, a problem that could only be overcome with higher levels of health literacy (Liu et al., 2020).
It is worth highlighting that partners’ compliance is also a significant obstacle that may be linked to a dominant representation of sexual problems as an individual problem and not a systemic, relationship-embedded issue. This position may reflect a view based on healthism, which tends to overemphasize a person’s role in determining their own health outcomes, ignoring the contexts in which these outcomes are shaped and embedded (Crawford, 1980).
Lastly, viewing sexual problems as a minor concern may explain why some people do not seek help, as they might not experience significant distress during partnered sexual activity. This has also been suggested by Hendrickx et al. (2016a, 2016b). Overall, the results reveal that there are people who are distressed by their sexual activity and are not accessing healthcare services due to different obstacles and that these should be approached through better education regarding the available services and professionals who are licensed and prepared to act on sexual problems. Moreover, these people, independent of the severity of the symptoms and compatibility with a formal diagnosis of sexual dysfunction, may benefit from internet-delivered treatment options. These solutions not only demonstrate positive results for their specific outcomes of interest (e.g., sexual function; Zarski et al., 2022) but also are a solution to barriers to treatment, such as improving time management, reducing stigma of asking help/having a sexual problem, reducing financial limitations and geographic barriers (Costa et al., 2023; Rodda and Luoto, 2023). Furthermore, these options likely address broader systemic problems, including social inequalities and deficiencies in health and sexual health follow-up care among minority groups, including people with physical disabilities, who do not have to face physical barriers to receiving treatment if the intervention is delivered online (Costa et al., 2023).
Finally, the comparison of content across genders is in line with research that demonstrates women experience more distressful sexual problems related to sexual function than men (Cobbs et al., 2022), which stresses that pursuing penetrative sex is more detrimental for women as they are more exposed to pain derived from penile-vaginal penetration. Because they prioritize their partners’ sexual enjoyment they are subsequently exposed to more distress related to sexual activity. The findings may be influenced by the sample composition, which was predominantly female (72.5%) and there could be a response bias, as men may experience sexual distress but might be unable or unwilling to disclose it. It could also be because men give more relevance to their spouse’s lack of sexual desire as a cause for their distress, and not to other problems their spouses may face, such as painful sex. It can be that men’s pressure to diminish the discrepancy between sexual desire results in more frequent non-desired sexual activity because women do not disclose their difficulties and, subsequently, have more painful sex. This possibility has been explored (Oesterling et al., 2025) and reveals that even in the presence of function problems, sexual distress is inbound to relationship factors.
Overall, our results have similarities with both the DSM-5 and ICD-11, indicating that sexual dysfunctions arise from a complex interplay of biological, psychological, and sociocultural factors. This is particularly evident in the theme Sexual (dys)function (It’s the function), which highlights difficulties related to sexual function, and was the most prominent pattern of meaning developed. Our findings support the emphasis of these psychopathology manuals on considering a range of contributing factors when assessing sexual dysfunctions, including relationship dynamics, such as poor communication and discrepancies in desire, as illustrated in the theme Dynamics of Intimacy (It’s us!). Interestingly, participants did not identify partner-related issues as significant sources of distress, possibly due to the self-referential nature of the online questionnaire used. Our results also emphasize individual vulnerability factors (e.g., negative body image), psychiatric comorbidities (e.g., depression and anxiety), and sociocultural influences (e.g., religious or moral beliefs about sexuality) that contribute to the theme Intrapersonal Struggles (It’s me!). Nonetheless, our findings expand the psychopathology framework of the DSM-5 and ICD-11. While manuals focus on problems that meet clinical thresholds, participants reported distress related to sexual experiences that may not fit these criteria, yet remain significant. Issues such as feelings of inadequacy and unmet expectations can lead or be components of sexual distress. Unmet expectations, for example, may account for lack of sexual pleasure, which can be a critical factor not adequately addressed by DSM-5 and ICD-11 criteria. In other words, manuals do not explicitly include the subjective absence of sexual pleasure as a standalone clinical concern, nor explore its relationship to the experience of distress. Additionally, both DSM-5 and ICD-11 tend to underrepresent the impact of socioculturally shaped meanings and internalized scripts, which were central to the experiences of our participants. Therefore, our findings support and extend the ICD-11 framework by advocating for a more comprehensive understanding of sexual problems.
The current study presents several limitations that need to be considered to frame the results and their interpretation, as well as to inform future studies. Firstly, it is not possible to determine whether the participants are eligible to have a diagnosis of sexual dysfunction, which could further inform our analysis. They do self-report distress and problems during partnered sexual activity, but these may be explained by factors that were not properly addressed and evaluated (e.g., organic cause, the existence of severe psychopathology). Furthermore, we did not evaluate the sexual distress with partenered face-to-face sexual activity levels, which could have facilitated the determination of whether seeking professional clinical help is associated with the sexual problem/s themselves or the distress concomitantly experienced. Future research should aim to measure sexual distress levels using targeted measures (e.g., SFEQ). The study design, i.e., relying on straightforward answers that were not discussed or explored in-depth, which can happen during interviews, did not allow us to gain a more nuanced understanding of the context in which the experience of distress emerged. It can be that some people report distress related to sexual activity that emerges after the sexual encounter and that derives from a lack of pleasure, satisfaction, or shame. Also, the fact that we gave a definition of sexual activity that focused on specific practices may have primed participants to focus more on distress related to sexual function or intercourse. It is also important to note that some participants, predominantly men, whose answers were not included in the reflexive thematic analysis, reported that experiencing high levels of sexual interest or drive was a distressing sexual problem for them. Although this problem did not appear to be directly related to sexual activity, it warrants further investigation in future studies. This suggests that sexual distress related to partnered face-to-face sexual activity may persist after the sexual encounter and be the focus of concerns. This finding that was not analyzed, should be taken into account in future studies. Additionally, we could not determine whether the notable gender differences were related to the sexual double standard, which refers to the tendency to evaluate genders differently for identical sexual behaviors (Milhausen and Herold, 2008, Gómez-Berrocal et al., 2022), such as men enjoying greater sexual freedom while women’s sexuality is more taboo (Raposo et al., 2024). Research suggests that sexual responses experienced by women are associated with this standard, which negatively impacts sexual response (Álvarez-Muelas et al., 2022). This should be examined in future studies. Finally, it is vital to consider the sociocultural context of our predominantly Portuguese participants and their influence on results. To our knowledge, there are no existing studies specifically examining help-seeking for sexual problems within the Portuguese population. However, available evidence suggests that sexology in Portugal has gradually gained visibility and recognition (Alarcão, 2017). Moreover, a recent study (Manão et al., 2024) found that Portuguese individuals’ understanding of sexual health includes the notion of seeking support from healthcare services, suggesting a growing openness to professional help. However, this positive perception did not fully translate into behavior, as our findings showed that some of the participants reported experiencing sexual distress without seeking help, which is in accordance with other research about help-seeking behavior (e.g., Moreira et al., 2005; Moreira et al., 2008). Conducting similar studies in different cultural settings could help clarify whether these findings are context-dependent or reflect a more widespread phenomenon. Not only, but especially, we recommend that future studies on this topic be conducted outside of Western, Educated, Industrialized, Rich, and Democratic (WEIRD) populations, in order to fully capture the diversity of sexual distress with partnered face-to-face sexual activity. This recommendation aligns with the calls of scholars such as Klein et al. (2022a, 2022b) to decolonize science and promote greater contextual diversity in sex research.
5 Conclusion
The analysis of people’s definitions of sexual distress with partnered face-to-face sexual activity reveals its strong interrelation and overlap with SDRSF (with a strong focus on genital response and penile-vaginal penetrative sex), relationship factors, and specific individual factors. This result aligns with the current approach to sexual dysfunctions by both DSM and ICD, which emphasises the contextual nature of sexual dysfunctions and recognises both individual and interpersonal features in diagnosing sexual dysfunction. However, the current study innovates by offering a nuanced perspective on how sexual distress with partenered face-to-face sexual activity should be assessed and approached, demonstrating that some of the associated features (e.g., anxiety/worry; inhibition; lack of communication skills) are crucial components of this distress that must be targeted in intervention. Our results support an integrative approach to clinical intervention and research that combines a transdiagnostic approach with CBT-derived and systemic theoretical models of intervention, considering sexual distress with partenered face-to-face sexual activity or SDRSF as the primary outcome but that also includes sexual pleasure and psychopathology as necessary outcomes of clinical intervention.
Data availability statement
The datasets presented in this article are not readily available because the dataset can be shared upon reasonable request to the corresponding author. Only raw anonymized data will be shared. Requests to access the datasets should be directed to cGF0cmljaWEucGFzY29hbEB1bHVzb2ZvbmEucHQ=.
Ethics statement
The studies involving humans were approved by Ethical and Deontological Committee for Scientific Research of the School of Psychology and Life Sciences (CEDIC) of Lusófona University in Lisbon. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their informed consent to participate in this study.
Author contributions
PP: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. GA: Writing – review & editing. VF: Writing – review & editing. AM: Formal analysis, Methodology, Writing – original draft, Writing – review & editing. CO: Writing – review & editing. CR: Formal analysis, Writing – review & editing. PR: Writing – review & editing. MR: Writing – review & editing. GS: Writing – review & editing. NT: Writing – review & editing. AG: Supervision, Conceptualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research project was funded by the European Society for Sexual Medicine Research Grant (RG 21-01) and was partially supported by national funds from the Foundation for Science and Technology (FCT) under project https://doi.org/10.54499/2022.09087.PTDC. Additionally, this work was financed by the FCT through the HEI-Lab R&D Unit (https://doi.org/10.54499/UIDB/05380/2020).
Acknowledgments
We would like to thank Marta Crawford, Musex (https://musex.pt) and Associação Gerador for regularly disseminating the questionnaire through their social media networks. We also thank Marta Crawford, Tiago Sigorelho, Daniel Cardoso and Carolina Caeiro for their support during the review of the survey’s content.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Gen AI was used in the creation of this manuscript because the authors used Grammarly to check for spelling mistakes, grammatical problems and punctuation inaccuracies. After using this tool, the authors reviewed and edited the content as needed. The authors take full responsibility and authorship for the publication’s content.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Reference
Alarcão, V., Ribeiro, S., Almeida, J., and Giami, A. (2017). Clinical practice in Portuguese sexology. J. Sex Marital Ther. 43, 760–773.
Álvarez-Muelas, A., Sierra, J. C., Gómez-Berrocal, C., Arcos-Romero, A. I., Calvillo, C., and Granados, R. (2022). Study of sexual concordance in men and women with different typologies of adherence to the sexual double standard. Int. J. Clin. Health Psychol. 22:100297. doi: 10.1016/j.ijchp.2022.100297
American Psychiatric Association (2022). Diagnostic and statistical manual of mental disorders: DSM-5-TR™ (5th ed. text revision). United States American Psychiatric Publishing, Inc.
Alarcão, V., Ribeiro, S., Almeida, J., and Giami, A. (2017). Clinical practice in Portuguese sexology. Journal of Sex \u0026amp; Marital Therapy, 43, 760–773. doi: 10.1080/0092623X.2016.1266537
Banbury, S., Lusher, J., Snuggs, S., and Chandler, C. (2021). Mindfulness-based therapies for men and women with sexual dysfunction: a systematic review and meta-analysis. Sex. Relatsh. Ther. 36, 533–555. doi: 10.1080/14681994.2021.1883578
Bancroft, J., Loftus, J., and Long, J. S. (2003). Distress about sex: a national survey of women in heterosexual relationships. Arch. Sex. Behav. 32, 193–208. doi: 10.1023/a:1023420431760
Barlow, D. H. (2016). “Causes of sexual dysfunction: The role of anxiety and cognitive interference” in The neurotic paradox. (New York, United States: Routledge). isbn:9781315724539
Braun, V., and Clarke, V. (2021). Thematic analysis: A practical guide. London, UK: SAGE Publications.
Braun, V., and Clarke, V. (2022). Conceptual and design thinking for thematic analysis. Qual. Psychol. 9, 3–26. doi: 10.1037/qup0000196
Braun, V., and Clarke, V. (2024). Supporting best practice in reflexive thematic analysis reporting in palliative medicine: a review of published research and introduction to the reflexive thematic analysis reporting guidelines (RTARG). J. Palliat. Med. 38, 608–616. doi: 10.1177/14799731231163873
Brotto, L. A., Atallah, S., Carvalho, J., Gordon, E., Pascoal, P. M., Reda, M., et al. (2025). Psychological and interpersonal dimensions of sexual function and dysfunction: recommendations from the fifth international consultation on sexual medicine (ICSM 2024). Sexual Medicine Reviews, 13, 118–143. doi: 10.1093/sxmrev/qeae073
Brotto, L. A., Zdaniuk, B., Chivers, M. L., Jabs, F., Grabovac, A., Lalumière, M. L., et al. (2021). A randomized trial comparing group mindfulness-based cognitive therapy with group supportive sex education and therapy for the treatment of female sexual interest/arousal disorder. J. Consult. Clin. Psychol. 89, 626–639. doi: 10.1037/ccp0000661
Braun, V., Clarke, V., Boulton, E., Davey, L., and McEvoy, C. (2020). The online survey as a qualitative research tool. International journal of social research methodology, 24, 641–654. doi: 10.1080/13645579.2020.1805550
Buvat, J., Glasser, D., Neves, R. C. S., Duarte, F. G., Gingell, C., and Moreira, E. D. Jr. (2009). Sexual problems and associated help‐seeking behavior patterns: Results of a population‐based survey in France. International journal of urology, 16, 632–638. doi: 10.1111/j.1442-2042.2009.02316.x
Carvalheira, A., Godinho, L., and Costa, P. (2017). The impact of body dissatisfaction on distressing sexual difficulties among men and women: The mediator role of cognitive distraction. J. Sex Res. 54, 331–340. doi: 10.1080/00224499.2016.1168771
Cobbs, L., Householder, N., Raghuram, A., Thipaphay, S., Agyare, K., and Tuazon, C. (2022). Analysis of gender differences in sexual dysfunction perception, prevalence, and help-seeking behavior among medical students and faculty at Texas Tech University health science center (TTUHSC). Med. J. Obstet. Gynecol. 10:1163. doi: 10.47739/2333-6439/1163
Cornwall, A., and Jewkes, R. (1995). What is participatory research? Soc. Sci. Med. 41, 1667–1676. doi: 10.1016/0277-9536(95)00127-S
Costa, I. B., Manão, A. A., and Pascoal, P. M. (2023). Clinical sexologists’ perceptions of the potentials, downfalls, and best practices for digitally delivered therapy: a lesson from lockdown due to COVID-19 in Portugal. Behav. Sci. 13:376. doi: 10.3390/bs13050376
Crawford, R. (1980). Healthism and the medicalisation of everyday life. Int. J. Health Serv. 10, 365–388. doi: 10.2190/3H2H-3XJN-3KAY-G9NY
Cardoso, D., Pascoal, P. M., and Quaresma, R. (2023). Navigating dissonant desires. The power of BDSM: Play, communities, and consent in the 21st century, 117.
Dewitte, M., Carvalho, J., Corona, G., Limoncin, E., Pascoal, P., Reisman, Y., et al. (2020). Sexual desire discrepancy: A position statement of the European Society for Sexual Medicine. Sexual Medicine, 8, 121–131. doi: 10.1016/j.esxm.2020.02.008
Davies, B., Gibbons, I., and Hughes, A. (2021). Treating comorbid sexual dysfunctions using the intersystem sex therapy approach. Contemp. Fam. Ther. 43, 12–19. doi: 10.1007/s10591-020-09552-8
Derogatis, L., Clayton, A., Lewis-D'Agostino, D., Wunderlich, G., and Fu, Y. (2008). Validation of the female sexual distress scale-revised for assessing distress in women with hypoactive sexual desire disorder. J. Sex. Med. 5, 357–364. doi: 10.1111/j.1743-6109.2007.00672.x
Döring, N., and Byers, E. S. (2024). “Dyadic sexual communication skills” in Encyclopedia of sexual psychology and behavior. Cham, Switzerland: Springer Nature.
Dove, N. L., and Wiederman, M. W. (2000). Cognitive distraction and women’s sexual functioning. J. Sex Marital Ther. 26, 67–78. doi: 10.1080/009262300278650
Epstein, S. (2023). “The meaning and significance of lay expertise” in The Oxford Handbook of Expertise and Democratic Politics. xual double standard: a gender-based prejudice referring to (Oxford University Press Oxford Handbooks), 76–102.
European Commission: Directorate-General for Research and Innovation . (2010). European textbook on ethics in research. Luxembourg: Publications Office of theEuropean Union.
Forbes, M. K., Baillie, A. J., and Schniering, C. A. (2016). Should sexual problems be included in the internalizing spectrum? A comparison of dimensional and categorical models. J. Sex Marital Ther. 42, 70–90. doi: 10.1080/0092623X.2014.996928
Forbes, M. K., and Schniering, C. A. (2013). Are sexual problems a form of internalizing psychopathology? A structural equation modeling analysis. Arch. Sex. Behav. 42, 23–34. doi: 10.1007/s10508-012-9948-0
Frederick, D. A., John, H. K. S., Garcia, J. R., and Lloyd, E. A. (2018). Differences in orgasm frequency among gay, lesbian, bisexual, and heterosexual men and women in a U.S. national sample. Arch. Sex. Behav. 47, 273–288. doi: 10.1007/s10508-017-0939-z
Frederick, D. A., Lever, J., Gillespie, B. J., and Garcia, J. R. (2016). What keeps passion alive? Sexual satisfaction is associated with sexual communication, mood setting, sexual variety, oral sex, orgasm, and sex frequency in a national U.S. study. J. Sex Res. 54, 186–201. doi: 10.1080/00224499.2015.1137854
Gómez-Berrocal, C., Moyano, N., Álvarez-Muelas, A., and Sierra, J. C. (2022). Sexual double standard: a gender-based prejudice referring to sexual freedom and sexual shyness. Front. Psychol. 13. doi: 10.3389/fpsyg.2022.1006675
Hendrickx, L., Gijs, L., and Enzlin, P. (2013). Distress, sexual dysfunctions, and DSM: dialogue at cross purposes? J. Sex. Med. 10, 630–641. doi: 10.1111/j.1743-6109.2012.02971.x
Hendrickx, L., Gijs, L., and Enzlin, P. (2016a). Sexual difficulties and associated sexual distress in Flanders (Belgium): a representative population-based survey study. J. Sex. Med. 13, 650–668. doi: 10.1016/j.jsxm.2016.01.014
Hendrickx, L., Gijs, L., Janssen, E., and Enzlin, P. (2016b). Predictors of sexual distress in women with desire and arousal difficulties: distinguishing between personal, partner, and interpersonal distress. J. Sex. Med. 13, 1662–1675. doi: 10.1016/j.jsxm.2016.09.016
Hsieh, H. F., and Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qual. Health Res. 15, 1277–1288. doi: 10.1177/1049732305276687
Klein, V., Laan, E., Brunner, F., and Briken, P. (2022a). Sexual pleasure matters (especially for women)—data from the German sexuality and health survey (GeSiD). Sex. Res. Soc. Policy 19, 1879–1887. doi: 10.1007/s13178-022-00694-y
Klein, V., Savaş, Ö., and Conley, T. D. (2022b). How WEIRD and androcentric is sex research? Global inequities in study populations. J. Sex Res. 59, 810–817. doi: 10.1080/00224499.2021.1918050
Kotov, R., Krueger, R. F., Watson, D., Achenbach, T. M., Althoff, R. R., Bagby, R. M., et al. (2017). The hierarchical taxonomy of psychopathology (HiTOP): a dimensional alternative to traditional nosologies. J. Abnorm. Psychol. 126, 454–477. doi: 10.1037/abn0000258
Laan, E. T., Klein, V., Werner, M. A., van Lunsen, R. H., and Janssen, E. (2021). In pursuit of pleasure: a biopsychosocial perspective on sexual pleasure and gender. Int. J. Sex. Health 33, 516–536. doi: 10.1080/19317611.2021.1965689
Lafortune, D., Girard, M., Dussault, É., Philibert, M., Hébert, M., Boislard, M. A., et al. (2023). Who seeks sex therapy? Sexual dysfunction prevalence and correlates, and help-seeking among clinical and community samples. PLoS One 18:e0282618. doi: 10.1371/journal.pone.0282618
Liu, C., Wang, D., Liu, C., Jiang, J., Wang, X., Chen, H., et al. (2020). What is the meaning of health literacy? A systematic review and qualitative synthesis. Fam. Med. Community Health. 8:e000351. doi: 10.1136/fmch-2020-000337
Laumann, E. O., Glasser, D. B., Neves, R. C., and Moreira, E. D. (2009). A population-based survey of sexual activity, sexual problems and associated help-seeking behavior patterns in mature adults in the United States of America. International journal of impotence research, 21, 171–178. doi: 10.1038/ijir.2009.7
Milhausen, R. R., and Herold, E. S. (2008). Reconceptualizing the sexual double standard. Journal of Psychology and Human Sexuality, 13, 63–83. doi: 10.1300/J056v13n02_05
MacNeil, S., and Byers, E. S. (2009). Role of sexual self-disclosure in the sexual satisfaction of long-term heterosexual couples. J. Sex Res. 46, 3–14. doi: 10.1080/00224490802398399
Manão, A. A., Brazão, M., and Pascoal, P. M. (2024). How to define sexual health? A qualitative analysis of people’s perceptions. Int. J. Sex. Health 37, 131–152. doi: 10.1080/19317611.2024.2422512
Manão, A. A., Martins, E., and Pascoal, P. M. (2023). What sexual problems does a sample of LGB+ people report having, and how do they define sexual pleasure: a qualitative study to inform clinical practice. Healthcare 11:2856. doi: 10.3390/healthcare11212856
Manão, A. A., and Pascoal, P. M. (2023). Body dissatisfaction, cognitive distraction, and sexual satisfaction in a sample of LGB+ people: a mediation study framed by cognitive psychology models of sexual response. Healthcare 11:2930. doi: 10.3390/healthcare11222930
Martins, E. M., Pascoal, P. M., Manão, A. A., and Rosa, P. J. (2024). The interplay of worry and relationship satisfaction to understand sexual distress: an APIM study with heterosexual couples using cross-sectional data. J. Sex Marital Ther. 50, 878–893. doi: 10.1080/0092623X.2024.2391390
Meston, C., and Trapnell, P. (2005). Development and validation of a five-factor sexual satisfaction and distress scale for women: the sexual satisfaction scale for women (SSS-W). J. Sex. Med. 2, 66–81. doi: 10.1111/j.1743-6109.2005.20107.x
Mitchell, K. R., Gurney, K., McAloney-Kocaman, K., Kiddy, C., and Parkes, A. (2022). The sexual function evaluation questionnaire (SFEQ) to evaluate effectiveness of treatment for sexual difficulties: development and validation in a clinical sample. J. Sex Res. 59, 426–434. doi: 10.1080/00224499.2021.1986800
Moreira, E. D., Glasser, D. B., and Gingell, C.GSSAB Investigators' Group (2005). Sexual activity, sexual dysfunction and associated help-seeking behaviours in middle-aged and older adults in Spain: a population survey. World. J. Urol. 23, 422–429. doi: 10.1007/s00345-005-0035-1
Moreira, E. D., Glasser, D. B., Nicolosi, A., Duarte, F. G., and Gingell, C. (2008). Sexual problems and help-seeking behaviour in adults in the United Kingdom and continental Europe. BJU Int. 101, 1005–1011. doi: 10.1111/j.1464-410X.2008.07453.x
Nickull, S., Källström, M., and Jern, P. (2022). An exploratory network analysis of sexual and relationship satisfaction comparing partnered cisgendered men and women. J. Sex. Med. 19, 711–718. doi: 10.1016/j.jsxm.2022.02.006
Nobre, P. J., and Barlow, D. H. (2023). “Barlow’s cognitive-affective model of sexual dysfunction” in Encyclopedia of sexuality and gender. ed. A. D. Lykins (Cham: Springer), 1–9.
Nobre, P. J. (2023). Nobre’s cognitive-emotional model of sexual dysfunction. In A. D. Lykins (Ed.), Encyclopedia of sexuality and gender. Cham: Springer. 1–9. doi: 10.1007/978-3-319-59531-3_116-1
Oesterling, C. F., Borg, C., and de Jong, P. (2024). Factors influencing women’s persistence in sexual activity amidst painful experiences. J. Sex. Med. 21:qdae041.066. doi: 10.1093/jsxmed/qdae041.066
Oesterling, C., Harder, A., Borg, C., and de Jong, P. (2025). Factors involved in vulvar pain during sexual activity and persistence in sexual activity amidst pain. PLoS One 20:e0306086. doi: 10.1371/journal.pone.0306086
Pascoal, P., Narciso, I., and Pereira, N. (2009). Women's definition of sexual problems: a qualitative analysis of 576 online respondents. Poster presented at the 19th world congress for sexual health, Gothenburg.
Pascoal, P., Pereira, N., and Narciso, I. (2008), November. O que são Dificuldades Sexuais? Estudo qualitativo das respostas de uma amostra de 530 mulheres e 397 homens portugueses. Oral communication presented at IV Congresso Nacional de Psiquiatria, Luso.
Pascoal, P. M., Raposo, C. F., and Roberto, M. S. (2020). A transdiagnostic approach to sexual distress and sexual pleasure: a preliminary mediation study with repetitive negative thinking. Int. J. Environ. Res. Public Health 17:7864. doi: 10.3390/ijerph17217864
Pascoal, P. M., Rosa, P. J., and Coelho, S. (2019). Does pregnancy play a role? Association of body dissatisfaction, body appearance cognitive distraction, and sexual distress. J. Sex. Med. 16, 551–558. doi: 10.1016/j.jsxm.2019.01.317
Pascoal, P. M., Rosa, P. J., Silva, E. P. D., and Nobre, P. J. (2018). Sexual beliefs and sexual functioning: the mediating role of cognitive distraction. Int. J. Sex. Health 30, 60–71. doi: 10.1080/19317611.2018.1424064
Paulsen, A., Vistad, I., and Fegran, L. (2023). Nurse–patient sexual health communication in gynaecological cancer follow-up: a qualitative study from nurses' perspectives. J. Adv. Nurs. 79, 4648–4659. doi: 10.1111/jan.15755
Peixoto, M. M., and Nobre, P. (2017). “Macho” beliefs moderate the association between negative sexual episodes and activation of incompetence schemas in sexual context, in gay and heterosexual men. J. Sex. Med. 14, 518–525. doi: 10.1016/j.jsxm.2017.02.002
Pieramico, S., Castro, R., Aguiar, S., Bismarck, F., Ferreira, D., Carvalho, J., et al. (2024). A systematic review on the efficacy of CBT interventions for the mental and sexual health of survivors of prostate cancer. Sex. Med. Rev. 12, 48–58. doi: 10.1093/sxmrev/qead024
Raposo, C. F., Nobre, P. J., Manão, A. A., and Pascoal, P. M. (2024). Understanding sexual distress related to sexual function (SDRSF): a preliminary framework based on a qualitative study with clinical sexologists. Int. J. Clin. Health Psychol. 24:100473. doi: 10.1016/j.ijchp.2024.100473
Raposo, C. F., Nobre, P. J., Rosa, P. J., and Pascoal, P. M. (2025). Difficulties in emotion regulation, repetitive negative thinking, and sexual and psychological distress: a two-wave longitudinal mediation study using a transdiagnostic approach. Sex. Med. 13, 118–143. doi: 10.1093/sexmed/qfaf052
Raposo, C. F., Pascoal, P. M., Faustino, B., and Nobre, P. J. (2023). The effect of emotional regulation difficulties on sexual and psychological distress using repetitive negative thinking as a mediator. J. Sex. Med. 20, 1466–1469. doi: 10.1093/jsxmed/qdad136
Rodda, S. N., and Luoto, S. (2023). The feasibility and impact of a brief internet intervention for pornography reduction. Sexual Health and Compulsivity, 30:57–80. doi: 10.1080/26929953.2022.2153772
Santos-Iglesias, P., and Walker, L. M. (2018). Psychometric validation of the sexual distress scale in men with prostate cancer. J. Sex. Med. 15, 1010–1020. doi: 10.1016/j.jsxm.2018.05.015
Sauer-Zavala, S., Gutner, C. A., Farchione, T. J., Boettcher, H. T., Bullis, J. R., and Barlow, D. H. (2017). Current definitions of “transdiagnostic” in treatment development: a search for consensus. Behav. Ther. 48, 128–138. doi: 10.1016/j.beth.2016.09.004
Sim, J., Saunders, B., Waterfield, J., and Kingstone, T. (2018). Can sample size in qualitative research be determined apriori? Int. J. Soc. Res. Methodol. 21, 619–634. doi: 10.1080/13645579.2018.1454643
Soler, F., Granados, R., Arcos-Romero, A. I., Calvillo, C., Álvarez-Muelas, A., Sanchez-Fuentes, M. D. M., et al. (2021). Association between psychopathological dimensions and sexual functioning/sexual arousal in young adults. Int. J. Environ. Res. Public Health 18:3584. doi: 10.3390/ijerph18073584
Tavares, I. M., Moura, C. V., and Nobre, P. J. (2020). The role of cognitive processing factors in sexual function and dysfunction in women and men: a systematic review. Sex. Med. Rev. 8, 403–430. doi: 10.1016/j.sxmr.2020.03.002
Terry, G., and Braun, V. (2017). “Short but often sweet: the surprising potential of qualitative survey methods” in Collecting qualitative data: A practical guide to textual, media and virtual techniques. eds. V. Braun, V. Clarke, and D. Gray (Cambridge: Cambridge University Press), 15–44.
United Nations . (2015). Transforming our world: The 2030 Agenda for Sustainable Development. https://www.un.org/sustainabledevelopment/
Ventus, D., Gunst, A., Kärnä, A., and Jern, P. (2017). No evidence for long-term causal associations between symptoms of premature ejaculation and symptoms of anxiety, depression, and sexual distress in a large, population-based longitudinal sample. J. Sex Res. 54, 264–272. doi: 10.1080/00224499.2016.1255301
Witting, K., Santtila, P., Varjonen, M., Jern, P., Johansson, A., Von Der Pahlen, B., et al. (2008). Female sexual dysfunction, sexual distress, and compatibility with partner. J. Sex. Med. 5, 2587–2599. doi: 10.1111/j.1743-6109.2008.00984.x
World Association for Sexual Health . (2021). Declaration on sexual pleasure. Available online at: https://worldsexualhealth.net/resources/declaration-on-sexual-pleasure/ [Accessed November 29, 2024].
World Health Organization . (2019). International classification of diseases, 11th revision (ICD-11). World Health Organization. Available online at: https://icd.who.int/en
Zanolari, D., Händler-Schuster, D., Clarenbach, C., and Schmid-Mohler, G. (2023). A qualitative study of the sources of chronic obstructive pulmonary disease-related emotional distress. Chronic Respir. Dis. 20:14799731231163873. doi: 10.1177/1479973123116387
Zarski, A. C., Velten, J., Knauer, J., Berking, M., and Ebert, D. D. (2022). Internet- and mobile-based psychological interventions for sexual dysfunctions: a systematic review and meta-analysis. NPJ Digit. Med. 5:139. doi: 10.1038/s41746-022-00670-1
Zheng, J., Islam, R. M., Bell, R. J., Skiba, M. A., and Davis, S. R. (2020). Prevalence of low sexual desire with associated distress across the adult life span: an Australian cross-sectional study. J. Sex. Med. 17, 1885–1895. doi: 10.1016/j.jsxm.2020.07.007
Keywords: sexual distress, sexual pleasure, sexual dysfunction, partnered sexual activity, help-seeking, clinical practice, qualitative approach, sexual problems
Citation: Pascoal PM, Andersson G, Fischer VJ, Manão AA, Oliveira C, Raposo CF, Rosa PJ, Roberto MS, Santos G, Tomada N and Giraldi A (2025) Sexual distress with partnered face-to-face sexual activity: an exploratory qualitative study with heterosexual cis people who seek and do not seek professional help. Front. Psychol. 16:1553893. doi: 10.3389/fpsyg.2025.1553893
Edited by:
F. Javier Del Río Olvera, University of Cádiz, SpainReviewed by:
Norbert Meskó, University of Pécs, HungaryColleen Mills-Finnerty, Stanford University, United States
Copyright © 2025 Pascoal, Andersson, Fischer, Manão, Oliveira, Raposo, Rosa, Roberto, Santos, Tomada and Giraldi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Patrícia M. Pascoal, cGF0cmljaWEucGFzY29hbEB1bHVzb2ZvbmEucHQ=