 Leonardo Gonçalves1,2,3†
Leonardo Gonçalves1,2,3† Lorenzo Casagrande Reggiani1,2,3*†
Lorenzo Casagrande Reggiani1,2,3*† Josiane Maliuk3 Gianfranco Rizzotto de Souza3
Josiane Maliuk3 Gianfranco Rizzotto de Souza3 Renato Gorga Bandeira de Mello4
Renato Gorga Bandeira de Mello4 Bruno Perosa Carniel1,2,3
Bruno Perosa Carniel1,2,3 Neusa Sica da Rocha1,2,3,5
Neusa Sica da Rocha1,2,3,5- 1Clinical Research Center, Hospital De Clínicas De Porto Alegre, Porto Alegre, Brazil
- 2Graduate Program in Psychiatry and Behavior Science, Universidade Federal Do Rio Grande Do Sul, Porto Alegre, Brazil
- 3Innovations and Interventions in Quality of Life Research Group, Universidade Federal Do Rio Grande Do Sul, Porto Alegre, Brazil
- 4Geriatrics Team, Internal Medicine Service, Hospital De Clínicas De Porto Alegre, Porto Alegre, Brazil
- 5Psychiatry Service, Hospital De Clínicas De Porto Alegre, Porto Alegre, Brazil
Introduction: Resilience scores are usually higher among older adults, but the COVID-19 pandemic and the associated social isolation in this risk group necessitate a reevaluation of this characteristic.
Objectives: To investigate the differences in resilience among young, middle-aged, and elderly individuals and to explore the mediating factors (quality of life, spirituality, social support, depressive symptoms) in the relationship between age and resilience.
Methods: A cross-sectional study was conducted in April 2020 through online collection using the snowball method, enrolling 3,278 participants. They were divided into three age groups (18–36, 37–59, 60+), and resilience was assessed using the CD-RISC-10 scale. Mediation analyses examined the roles of depressive symptoms (PHQ-9), quality of life (EUROHIS-QOL-8), spirituality (WHOQOL-SRPB), and social support (MOS).
Results: The sample comprised 1,207 young, 1,680 middle-aged, and 391 older adults. Resilience scores were significantly higher in the elderly population compared to middle-aged and young adults [F(2,3251) = 81.12; p = 0.001]. Quality of life (β = 0.23; p = 0.001) and spirituality (β = 0.28; p = 0.001) showed positive mediating effects, while depressive symptoms (β = −0.18; p = 0.001) had a negative effect. Social support did not show a statistically significant mediating effect.
Conclusion: Older age was associated with higher resilience scores, even during COVID-19 pandemic. Spirituality and quality of life were identified as mediators of this relationship. These findings underscore the need for longitudinal research to confirm whether these factors predict resilience and to guide mental health interventions.
Introduction
Resilience is a dynamic process of successful adaptation to adversity, from minor threats to significant trauma (American Psychological Association, 2024). Biological, environmental, social, and cultural factors are known to influence individual responses to adversity (Southwick et al., 2014; Gaffey et al., 2016). Old age is often associated with higher resilience compared to younger age groups (Gooding et al., 2012; Eshel et al., 2016; Na et al., 2022; Staneva et al., 2022). However, evidence supporting this difference is somewhat limited, as most studies compare young and older adults without including middle-aged individuals. This omission restricts the understanding of whether resilience increases progressively throughout life. Additionally, factors such as quality of life, spirituality, social support, and depressive symptoms have been shown to directly impact resilience (Nygren et al., 2005; Lamond et al., 2008; Hildon et al., 2010; Zhang et al., 2017; Schmitt et al., 2021; Londero and da Rocha, 2024). Their influence on the age-resilience relationship remains poorly understood until this moment.
The COVID-19 pandemic has highlighted the importance of resilience in mitigating the psychological impacts of prolonged stress and social isolation. Older adults, for instance, faced higher risks of morbidity and mortality (Banerjee and Rai, 2020; Jawaid, 2020), along with emotional and social challenges resulting from confinement (Griffiths et al., 2015; Shi et al., 2015). Despite these vulnerabilities, studies have paradoxically shown that older adults often report higher levels of resilience compared to younger individuals during crises prior to COVID-19 pandemic (Hansen and Slagsvold, 2012; Hikichi et al., 2016; Rafiey et al., 2016). This observation raises questions about the protective factors that contribute to resilience in different age groups and how these factors interact to shape adaptive capacities under stress.
Most studies on resilience focus on comparisons between younger and older adults, but often overlook middle-aged individuals. Gooding et al. (2012) examined resilience in young and older populations without including middle-aged adults as a distinct group. Similarly, Eshel et al. (2016) provided broader insights yet did not directly address whether middle age significantly influences resilience. Meanwhile, Na et al. (2022) stratified age into four groups, including middle age, but assessed resilience as a moderating variable in the relationship between age and mental distress, rather than as the main outcome.
Quality of life, encompassing both physical and psychological well-being, has been consistently linked to higher resilience (Hildon et al., 2010; Pardeller et al., 2020; Brinkhof et al., 2021). Individuals with better overall quality of life tend to cope more effectively with stress and adapt more readily to challenges (Hildon et al., 2010; MacLeod et al., 2016). Spirituality also plays an essential role in resilience, offering a sense of purpose and meaning that can strengthen individuals during periods of adversity (Nygren et al., 2005). On the other hand, depressive symptoms undermine resilience, making individuals more vulnerable to the psychological impacts of stress and adversity (Lamond et al., 2008; Schmitt et al., 2021; Londero and da Rocha, 2024). Finally, social support has been shown to provide both emotional and practical resources, acting as a crucial buffer against stress and promoting better mental health outcomes during crises (Gaffey et al., 2016; Southwick et al., 2016; Weitzel et al., 2021).
Despite these findings, little is known about how these factors interact to shape resilience across different age groups. Most existing research focuses on binary comparisons between young and older adults or is exclusively centered on older populations, often neglecting the transitional dynamics of resilience in middle-aged individuals (De Pue et al., 2021) and the role of psychosocial factors such as quality of life, spirituality, social support, and depressive symptoms. Investigating these interactions may help clarify the mechanisms underlying age-related differences in resilience and provide a more nuanced understanding of how protective and harmful factors influence resilience across the lifespan.
Objectives and hypothesis
The primary objective of this study was to investigate whether there was a difference in resilience between age groups during the COVID-19 pandemic. We hypothesized that resilience levels increased according to age group. The secondary objective was to evaluate whether quality of life, social support, depressive symptoms, and spirituality mediate the relationship between age and resilience, by exploring how these mediators differ across age groups in the COVID-19 pandemic. We hypothesize that quality of life, social support and spirituality would exert a positive mediating effect, while depressive symptoms would act with a negative mediating effect.
Materials and methods
Data availability statement
Technical appendix, statistical code, and raw dataset available by contacting the corresponding author. This study was not pre-registered. Clinical trial number: not applicable.
Study design and setting
This cross-sectional study, conducted during the early stages of the COVID-19 pandemic (April 14–23, 2020), utilized a structured online survey distributed via Google Forms. A snowball sampling method was employed to recruit participants. To comply with social isolation measures, the study was promoted through the virtual platforms of the Federal University of Rio Grande do Sul and social media, where the link to the research protocol was made available. Participants, all aged 18 years or older, provided informed consent before completing a 7-part questionnaire.
At the time of data collection (April 2020), Brazil was entering a critical phase of the pandemic, characterized by rapidly increasing infection rates, national lockdown recommendations, and significant uncertainty regarding the healthcare system’s capacity. Many participants were already experiencing restrictions on mobility, social isolation, and disruption to work and family routines. Since then, global COVID-19 cases had reached 676,609,955, with 6,881,955 reported deaths, as per data from the Johns Hopkins University Coronavirus Resource Center (Johns Hopkins University Coronavirus Resource Center, 2023), as of its final update in March 2023. In Brazil, by September 2024, 37,915,370 cases of infection and 713,205 deaths had been recorded, according to the Ministry of Health (BR) (2024).
Instruments
The main research instrument was the Connor-Davidson resilience scale (CD-RISC-10), developed by Connor and Davidson (2003), and consists of 10 questions using a 5-point Likert scale. The scale has good psychometric properties, such as its convergent validity and predictive capacity, and was validated in Brazilian Portuguese by Solano et al. (2016). This protocol included demographic data, primarily age, but also gender, ethnicity, marital status, occupation, and education.
This protocol included demographic data, primarily age, but also gender, ethnicity, marital status, occupation, and education. The subsequent split of participants into three groups, which will be called Young Adults (YA) between 18 and 36 years old, Middle-aged Adults (MA) between 37 and 60 years old, and Older Adults (OA) over 60 years. The definition of older adults as people aged over 60 years was based on the concept established by the World Health Organization (WHO) for developing countries. For most developed countries, this age group includes people over 65. The other cut-off point was 35 years, as it is generally considered that an average adult is twice the minimum age of 18 years.
For mediation analysis, quality of life was assessed using the EUROHIS-QOL-8 questionnaire, validated in Brazilian Portuguese by Pires et al. (2018); spirituality using the WHOQOL-SRPB instrument, validated in Brazilian Portuguese by Fleck et al. (2000); social support by the MOS score, validated in Brazilian Portuguese by Griep et al. (2005), Preacher and Hayes (2004); and depressive symptoms using the PHQ-9 questionnaire, validated in Brazilian Portuguese by Santos et al. (2013).
Statistical methods
The continuous variables were presented as means and standard deviations (SD). Categorical variables (gender, ethnicity, occupation, and education) were presented as percentages and compared using the chi-squared test. One-way analysis of variance (ANOVA) was used to compare age groups regarding resilience. Tukey’s post-hoc tests evaluated pairwise differences between groups. The mediation analysis was performed with the statistically significant factors obtained in the logistic regression using the bootstrapping method described by Preacher and Hayes (2004). The level of significance was set at p < 0.05. All analyses were performed using software SPSS version 21 (IBM Corporation, Armonk, USA).
Ethics and consent to participate
This research followed the National Health Council (CNS) resolution 516/2016 determinations and the Declaration of Helsinki. It was assessed by the Research Ethics Committee of Hospital Gianfranco Rizzotto Renato Gorga Bandeira de Mello Souza Clínicas de Porto Alegre and approved by GPPG 2020/0141. Data were anonymized before constructing the database to be analyzed, not allowing participant identification. Informed consent was obtained from all individual participants included in this study.
Results
The flowchart (Figure 1) provides us with an overview of the result of the inclusion of participants and age group split. In total, 3278 participants were obtained, divided into three groups, which will be called Young Adults (YA) between 18 and 36 years old, Middle-aged Adults (MA) between 37 and 60 years old, and Older Adults (OA) over 60 years. We obtained a total of 1207 (36.8%) in the YA group, 1680 (51.3%) in the MA group and 391 (11.9%) individuals in the EA group.
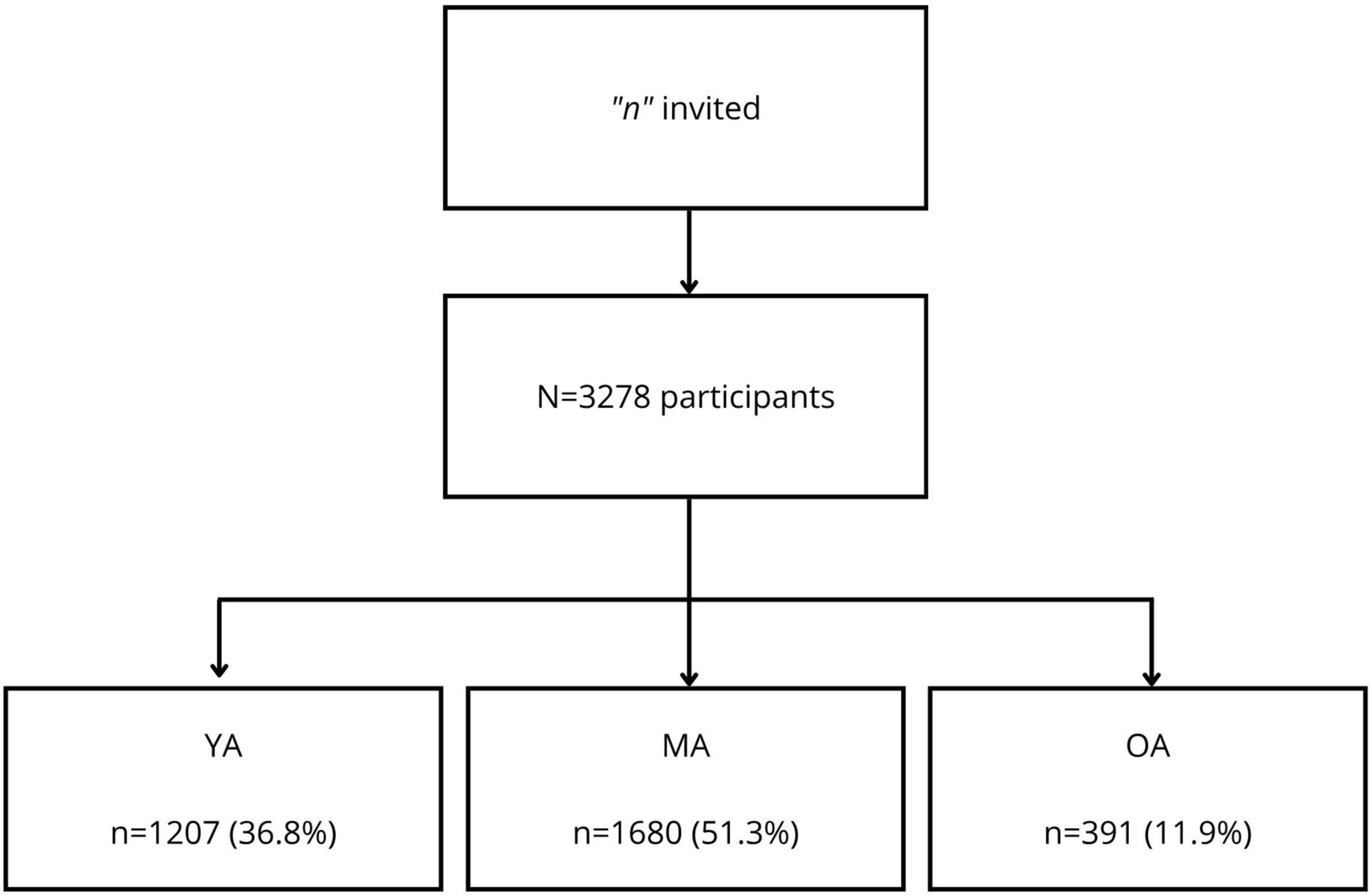
Figure 1. Flowchart of the sample of 3,278 adults during the COVID-19 pandemic. YA, Young adults; MA, Middle-aged adults; and OA, Older adults.
Table 1 shows the sociodemographic characteristics of each group. The mean age in the YA group was 28.4 years (SD ± 5.03); in the MA group, it was 47.1 years (SD ± 6.72); and in the OA group, it was 65.1 years (SD ± 4.62). In the three groups, women were predominant (54%–87%) of white ethnicity (88%–95.3%) and who had at least completed high school (63.5%–84.3%). Regarding marital status, there was a predominance of married individuals in the YA (50.9%) and MA (72.1%) groups and Widow/widower individuals in the OA group (68.4%). As for occupation, there was a predominance of individuals with paid employment in the YA (64.5%) and MA (80.2%) groups, while in the OA group, retired people were predominant due to age (57.4%). Responders were mainly health care professionals (31.8%) and young or middle-aged adults; only 11.9% were categorized as older adults. Out of all participants, 0.4% stated being a suspected case of COVID-19, and 16.5% reported having some chronic disease, of which middle-aged adults presented the most (55.7%).
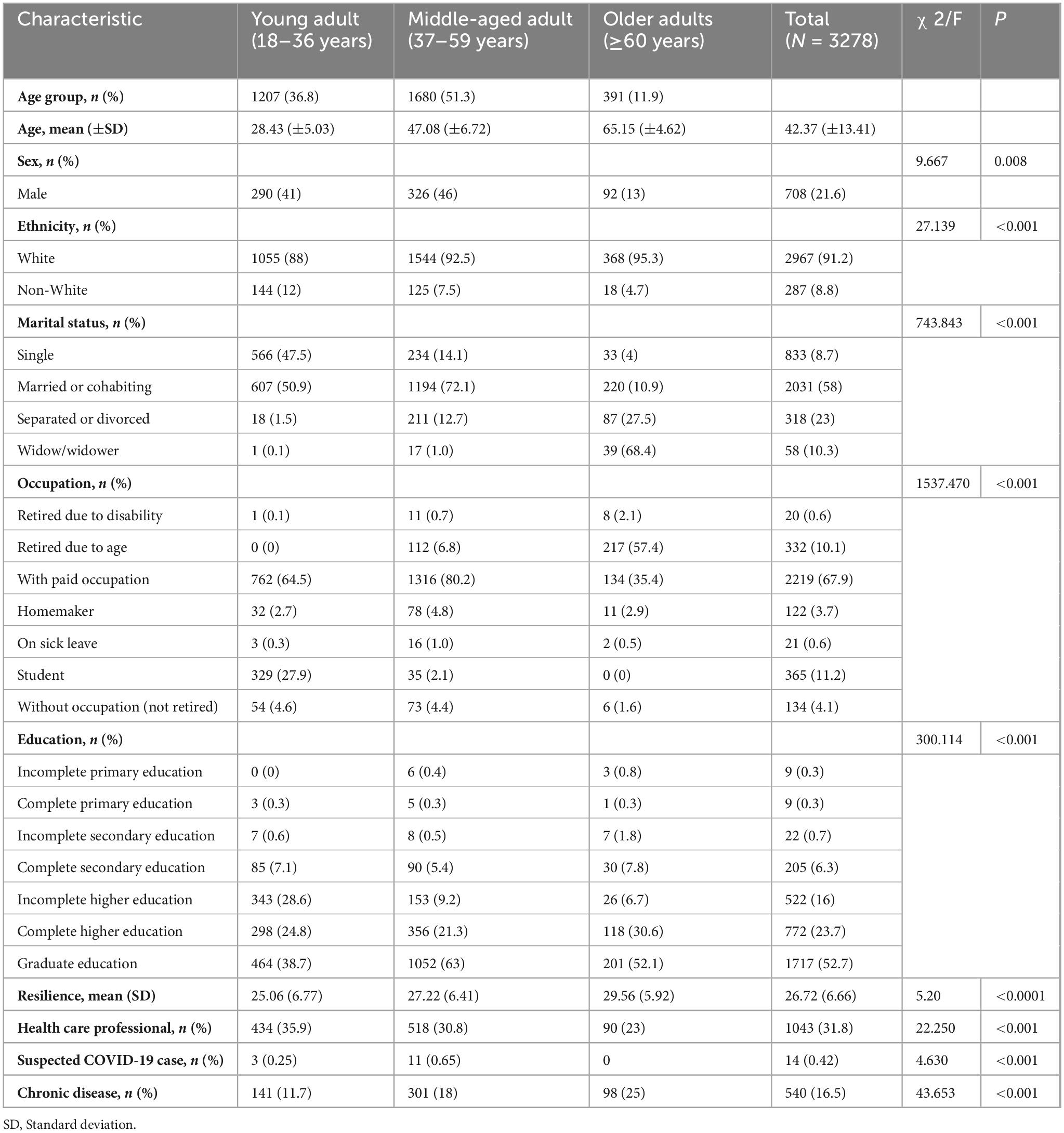
Table 1. Sociodemographic characteristics of the sample of 3,278 adults.
When comparing resilience levels (Figure 2), there was a significant difference between age groups [F (2,3251) = 81.12; p = 0.001]. A Tukey’s post-hoc test showed significant differences both between young and middle-aged adults [ΔM = −2.16; 95% confidence interval (CI), −2.74 to −1.58; p = 0.001)] and between middle-aged and older adults (ΔM = −2.34; 95% CI, −3.20 to −1.48; p = 0.001). Subgroup analyses showed that older adults aged over 70 years presented higher mean resilience than older adults below this age. Still, this difference was not statistically significant, possibly due to the small sample size within this age range.
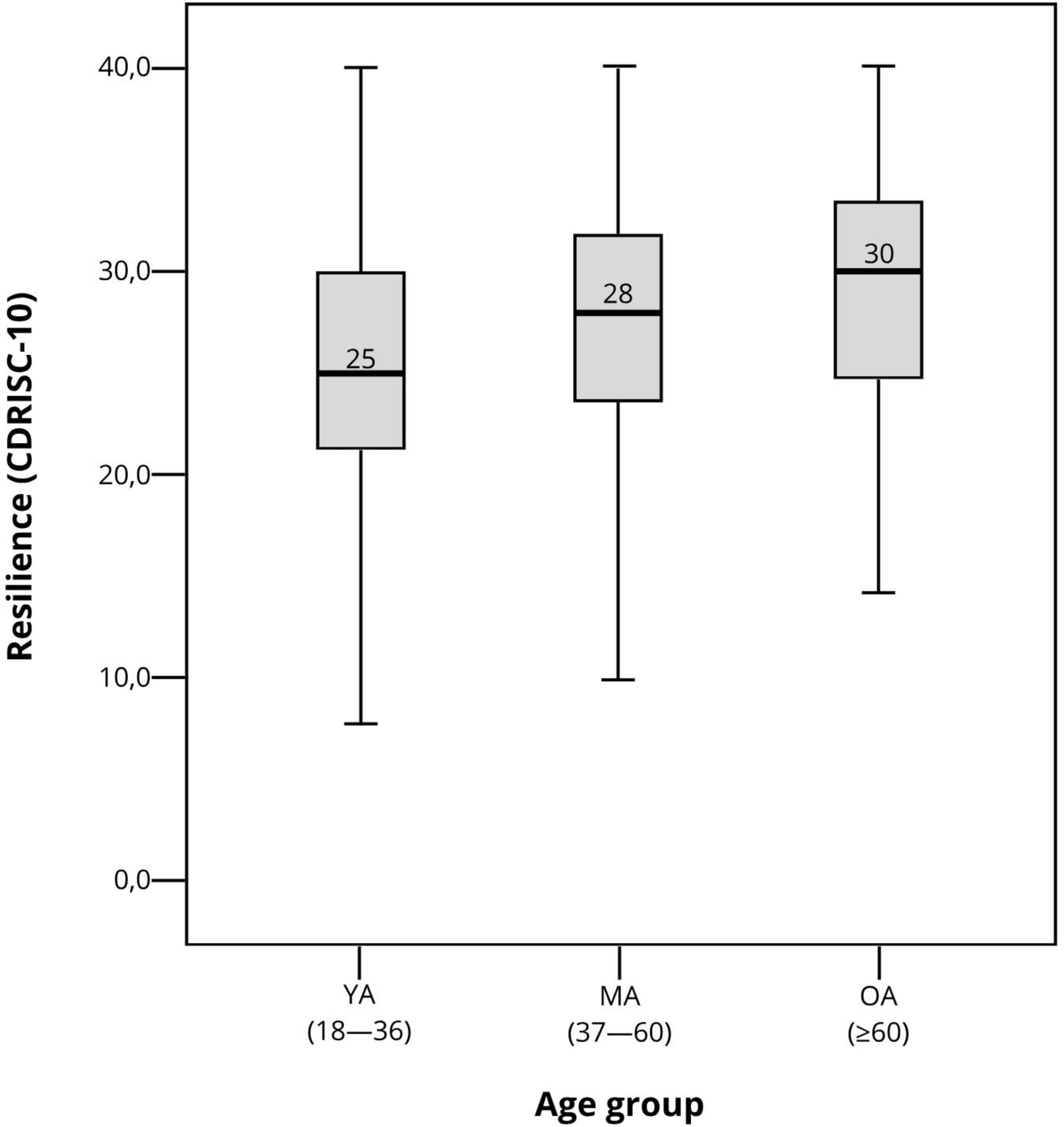
Figure 2. Box plot of resilience levels by age group during the COVID-19 pandemic. YA, Young adults; MA, Middle-aged adults; and OA, Older adults.
The univariate analysis included the following factors associated with resilience: age, gender, quality of life (EUROHIS-QOL), spirituality (WHO-QOL SRPB), social support (MOS), diagnosis of depression (PHQ-9 > 5), and depressive symptoms (PHQ-9) (Table 2). Quality of life (ρ = 0.446; p = 0.001) and spirituality (ρ = 0.417; p = 0.001) had the greatest positive associations, while depressive symptoms presented a negative association (ρ = –0.506; p = 0.001).
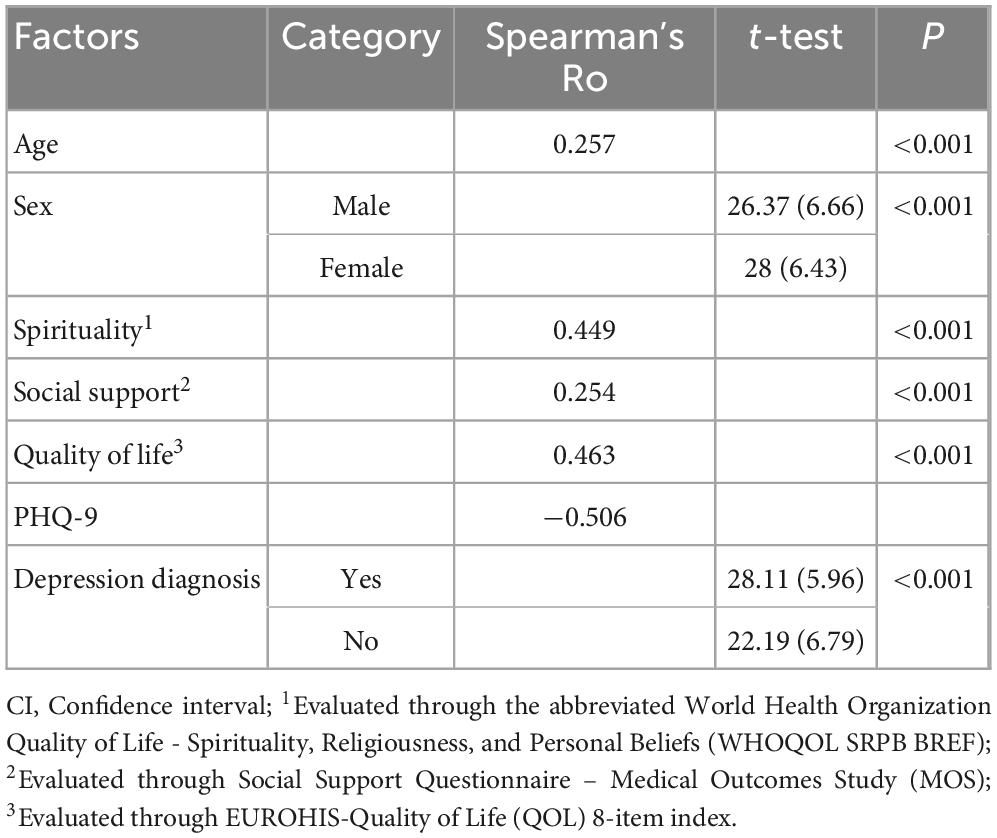
Table 2. Univariate analysis of factors associated with resilience during the COVID-19 pandemic.
In the stepwise multivariate analysis (Table 3), the depression diagnosis (PHQ-9 > 5) predictor presented no significant association (p > 0.2) and was excluded from the final model. The complete model explained 34.3% (B = 34.3, p = 0.0001) of the variations in resilience, corresponding to a moderate effect size. The most important predictor of higher resilience scores was spirituality (β = 0.28; p = 0.001). A depression diagnosis was a negative predictor of resilience levels (β = −0.18; p = 0.001).
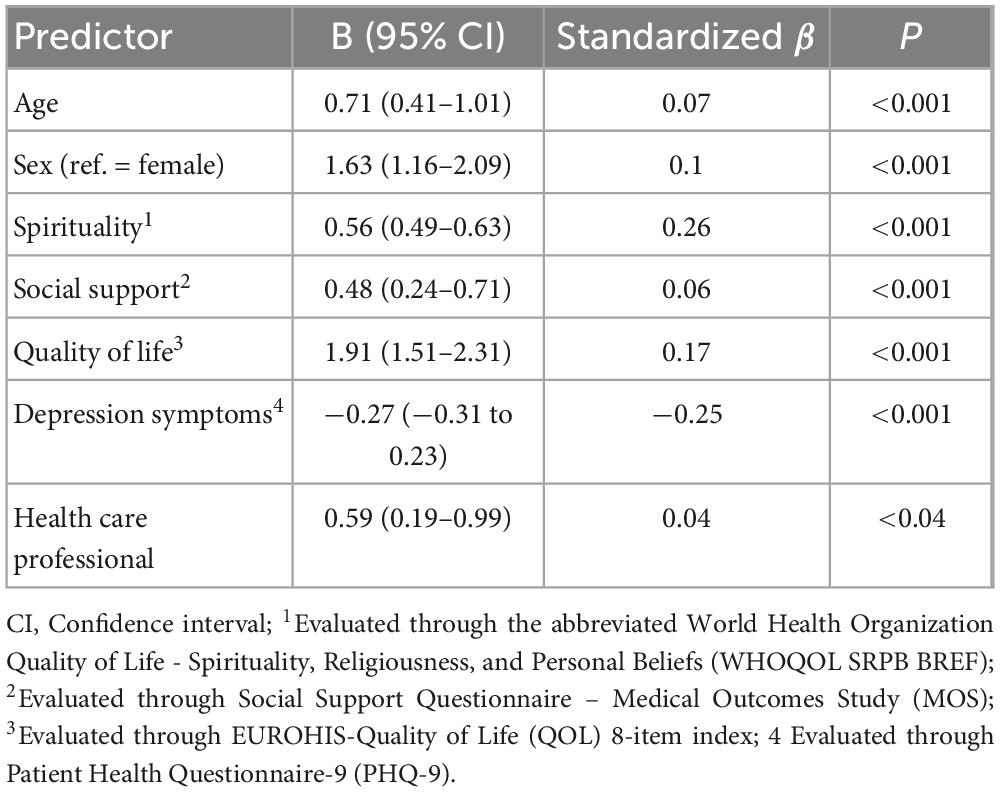
Table 3. Multivariate analysis of resilience predictors during the COVID-19 pandemic.
The age group model for resilience used spirituality, quality of life, social support, and depressive symptoms as mediators. Figure 3 shows that the mediation effect was statistically significant for spirituality [b = 0.83; BCaCI 95% (0.68, 1.0); R2 = 0.22; p = 0.001], quality of life [b = 0.73; BCaCI 95% (0.57, 0.89); R2 = 0.23; p = 0.001], and depressive symptoms [b = 1.52; BCaCI 95% (1.34, 1.72); R2 = 0.26; p = 0.001).
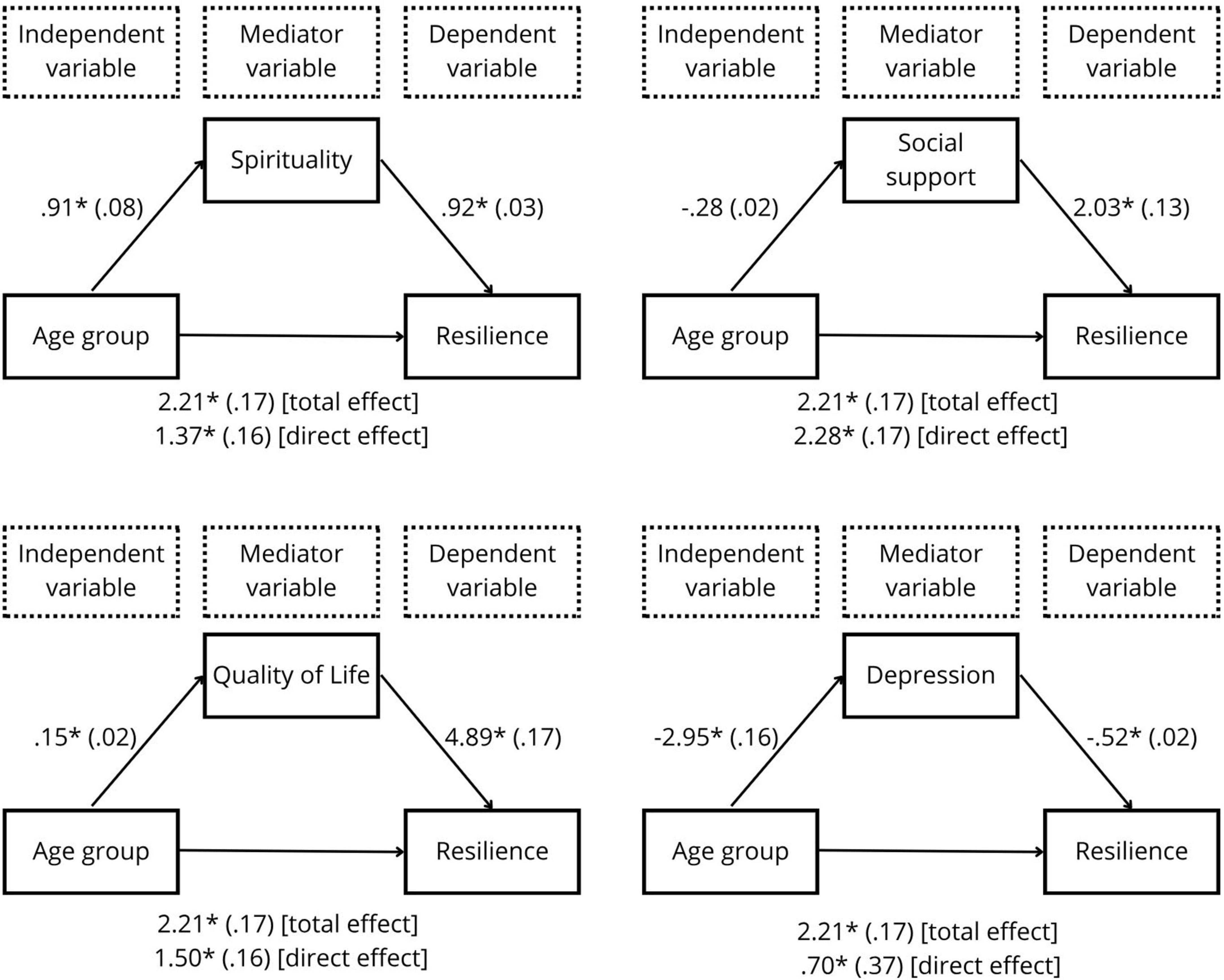
Figure 3. Age group model as a predictor of resilience, mediated by spirituality, quality of life, social support, and depressive symptoms. All coefficients represent unstandardized beta coefficients (standard errors in parentheses) *p = 0.001.
Discussion
This study is the first to identify significant differences in resilience among young, middle-aged, and older adults, and to analyze the mediating effects of quality of life, spirituality, depressive symptoms, and social support in the age–resilience relationship during the COVID-19 pandemic. Our findings confirm that resilience increases with age, a pattern significantly mediated by spirituality, quality of life, and depressive symptoms. However, social support did not emerge as a significant mediator in this context.
The primary result showed that resilience increased by approximately 2 points between age groups, with the older population (>60 years) being the most resilient. In the subgroup analysis of older people, those aged over 70 years still presented higher mean resilience by 1 point, although this difference was not statistically significant, likely due to the small sample size in this age group. This finding suggests the existence of a subpopulation known as the oldest-old, as proposed in previous studies (Shen and Zeng, 2010; Zeng and Shen, 2010). Studies attributing higher resilience with age highlight factors such as expanded coping strategies (Fontes and Neri, 2019), emotional stability, and better social resources (Nygren et al., 2005; Fontes and Neri, 2015; Hayman et al., 2017). However, other studies emphasize challenges such as the prevalence of chronic diseases and social isolation (Beutel et al., 2009, 2010), which can reduce resilience when stressors become overwhelming (Crane et al., 2019).
The mediation analysis revealed notable findings. Spirituality and quality of life emerged as strong positive mediators, underscoring their clinical importance in supporting resilience, particularly among older adults. In contrast, depressive symptoms were negatively associated with resilience, reinforcing the need for early detection and treatment, especially during crises. The overall increase in protective factors with age suggests a generally healthier older population, which may reflect a socioeconomic bias in the sample. Notably, the mediation models did not include sex or health care professional status as covariates, as this was not among the objectives of the study. These variables, however, were included in the multivariate regression analyses (Table 3).
Although social support showed a direct positive association with resilience, its contribution to the mediation model was not statistically significant. Previous studies have shown a positive association (Hayman et al., 2017) or no association (Silva Júnior et al., 2019) between these constructs. The impact of social support may have been minimized by restricted access to resources, such as family, friends, and religious or social groups, during the early quarantine period when the sample was collected. The instrument used (MOS score) did not specifically consider the alternative forms of contact, such as social networks and videoconferencing, which became crucial during this time. Additionally, social support is not universally effective, as its benefits depend on the type of support provided and how well it matches the individual’s needs (Southwick et al., 2016).
This study contributes to consolidating the hypothesis that levels of resilience are higher among older individuals, who, despite being the focus of health concern during the COVID-19 pandemic, were possibly not the most affected in terms of quality of life. Research has shown that children and adolescents experienced significant decline in quality of life during the pandemic, influenced by reduced social interaction and increased unpredictability, which are linked to higher rates of depression (Araujo et al., 2024; Ye et al., 2024). Resilience has been associated with better mental health outcomes in these younger groups, including reduced anxiety and depression when paired with strong social support and adaptive coping mechanisms (Jones et al., 2021). Similarly, among young adults, higher resilience during the pandemic was linked to more positive coping with traumatic experiences (Xu et al., 2024). These findings highlights the clinical importance of assessing resilience across all age groups, particularly younger individuals, to better inform mental health interventions.
This study has several strengths. By analyzing the mediating effects of psychosocial factors–such as quality of life, spirituality, depressive symptoms, and social support–on the age-resilience relationship, it provides valuable insights into resilience dynamics across different age groups. The inclusion of three distinct age groups goes beyond traditional young-versus-older comparisons, offering a broader understanding of how resilience evolves throughout life. The large sample size (>3,000 participants) strengthens the robustness of the findings, while the study’s focus on resilience during the COVID-19 pandemic adds relevance for understanding psychological responses during crises.
Despite the strengths of this study, some limitations should be noted. First, its cross-sectional design limits the ability to establish causal relationships. Longitudinal, prospective studies are needed to clarify how age, resilience, and psychosocial variables interact over time. Second, the use of self-report measures may have introduced social desirability bias, a common limitation, especially in studies conducted during the first months of the COVID-19 pandemic. Third, the online snowball sampling likely led to selection bias. Most participants were predominantly White (91.2%), while national census data indicate that only 43.5% of Brazilians identify as White (Federal Government (BR), 2023). Other ethnic groups, such as Black, Indigenous, and Asian individuals, were underrepresented. In addition, more than half of the participants held a graduate degree, and 31.8% were healthcare professionals, mostly among YA (35.9%) and MA adults (30.8%). These patterns suggest an overrepresentation of individuals with higher education, socioeconomic status, and digital access, as noted in similar studies (Li et al., 2020; Zhang and Ma, 2020), which limits the generalizability of the findings. Finally, although sex and health care professional status were included as control variables in the multivariate regression models (Table 3), they were not included in the mediation models, as this was not among the study’s objectives. Future research may benefit from employing more advanced statistical approaches, such as structural equation modeling, to account for demographic covariates in mediation analyses. Additionally, more inclusive recruitment strategies may help improve representativeness and external validity.
Conclusion
This study aimed to evaluate the associations of resilience in the COVID-19 outbreak among three age groups and its mediators, such as quality of life, spirituality, depressive symptoms, and social support. Resilience was found to be higher among older individuals, with quality of life and spirituality serving as significant positive mediators. Notably, depressive symptoms negatively contributed, whereas social support did not present a significant mediating effect.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Hospital de Clínicas de Porto Alegre Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
LG: Writing – original draft, Writing – review and editing. LR: Writing – original draft, Writing – review and editing. JM: Writing – review and editing. GS: Writing – review and editing. RM: Writing – review and editing. BC: Writing – review and editing. NR: Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the Institutional Scientific Initiation Scholarship Program (PIBIC, No. 102212/2020-0), the Hospital de Clínicas de Porto Alegre Research Incentive Fund (FIPE), the Fundação de Amparo à Pesquisa do Rio Grande do Sul (No. 19/251-0001930-0), and the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq, No. 303652/2019-5).
Acknowledgments
We thank all participants who contributed to this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
American Psychological Association. (2024). The road to resilience. Washington, DC: American Psychological Association.
Araujo, C. P., Piva, J. Vettoretti Nicoladeli, A. Paniz Hartwig, J., Vieira, A. P. R. Sica Rocha, N., et al. (2024). Lifestyle and quality of life in children and adolescents during the covid-19 social distancing period. J. Pediatr. 100, 53–59. doi: 10.1016/j.jped.2023.07.006
Banerjee, D., and Rai, M. (2020). Social isolation in Covid-19: The impact of loneliness. Int. J. Soc. Psychiatry 66, 525–527. doi: 10.1177/0020764020922269
Beutel, M. E., Glaesmer, H., Decker, O., Fischbeck, S., and Brähler, E. (2009). Life satisfaction, distress, and resiliency across the life span of women. Menopause 16, 1132–1138. doi: 10.1097/gme.0b013e3181a857f8
Beutel, M. E., Glaesmer, H., Wiltink, J., Marian, H., and Brähler, E. (2010). Life satisfaction, anxiety, depression and resilience across the life span of men. Aging Male 13, 32–39. doi: 10.3109/13685530903296698
Brinkhof, L. P., Huth, K. B. S., Murre, J. M. J., de Wit, S., Krugers, H. J., and Ridderinkhof, K. R. (2021). The interplay between quality of life and resilience factors in later life: A network analysis. Front. Psychol. 12:752564. doi: 10.3389/fpsyg.2021.752564
Connor, K. M., and Davidson, J. R. T. (2003). Development of a new resilience scale: The Connor-davidson resilience scale (CD-RISC). Depress Anxiety 18, 76–82. doi: 10.1002/da.10113
Crane, M. F., Searle, B. J., Kangas, M., and Nwiran, Y. (2019). How resilience is strengthened by exposure to stressors: The systematic self-reflection model of resilience strengthening. Anxiety Stress Coping 32, 1–17. doi: 10.1080/10615806.2018.1506640
De Pue, S., Gillebert, C., Dierckx, E., Vanderhasselt, M.-A., De Raedt, R., and Van den Bussche, E. (2021). The impact of the COVID-19 pandemic on wellbeing and cognitive functioning of older adults. Sci. Rep. 11:4636. doi: 10.1038/s41598-021-84127-7
Eshel, Y., Kimhi, S., Lahad, M., and Leykin, D. (2016). Individual, community, and national resiliencies and age: Are older people less resilient than younger individuals? Am. J. Geriatr. Psychiatry 24, 644–647. doi: 10.1016/j.jagp.2016.03.002
Federal Government (BR). (2023). Pardos são maioria da população brasileira pela primeira vez, indica IBGE. Available online at: https://www.gov.br/secom/pt-br/assuntos/noticias/2023/12/pardos-sao-maioria-da-populacao-brasileira-pela-primeira-vez-indica-ibge (accessed February 12, 2025).
Fleck, M. P., Louzada, S., Xavier, M., Chachamovich, E., Vieira, G., Santos, L., et al. (2000). Aplicação da versão em português do instrumento abreviado de avaliação da qualidade de vida “WHOQOL-bref.”. Rev. Saude Publ. 34, 178–183. doi: 10.1590/S0034-89102000000200012
Fontes, A. P., and Neri, A. L. (2015). Resilience in aging: Literature review. Cien Saude Colet 20, 1475–1495. doi: 10.1590/1413-81232015205.00502014
Fontes, A. P., and Neri, A. L. (2019). Estratégias de enfrentamento como indicadores de resiliência em idosos: Um estudo metodológico. Cien Saude Colet 24, 1265–1276. doi: 10.1590/1413-81232018244.05502017
Gaffey, A. E., Bergeman, C. S., Clark, L. A., and Wirth, M. M. (2016). Aging and the HPA axis: Stress and resilience in older adults. Neurosci. Biobehav. Rev. 68, 928–945. doi: 10.1016/j.neubiorev.2016.05.036
Gooding, P. A., Hurst, A., Johnson, J., and Tarrier, N. (2012). Psychological resilience in young and older adults. Int. J. Geriatr. Psychiatry 27, 262–270. doi: 10.1002/gps.2712
Griep, R. H., Chor, D., Faerstein, E., Werneck, G. L., and Lopes, C. S. (2005). Validade de constructo de escala de apoio social do medical outcomes study adaptada para o português no Estudo Pró-Saúde. Cad Saude Publ. 21, 703–714. doi: 10.1590/S0102-311X2005000300004
Griffiths, F. E., Boardman, F. K., Chondros, P., Dowrick, C. F., Densley, K., Hegarty, K. L., et al. (2015). The effect of strategies of personal resilience on depression recovery in an Australian cohort: A mixed methods study. Health Interdiscipl. J. Soc. Study Health Illness Med. 19, 86–106. doi: 10.1177/1363459314539774
Hansen, T., and Slagsvold, B. (2012). The age and subjective well-being paradox revisited: A multidimensional perspective. Norsk Epidemiol. 22, 187–195. doi: 10.5324/nje.v22i2.1565
Hayman, K. J., Kerse, N., and Consedine, N. S. (2017). Resilience in context: The special case of advanced age. Aging Ment. Health 21, 577–585. doi: 10.1080/13607863.2016.1196336
Hikichi, H., Aida, J., Kondo, K., Tsuboya, T., Matsuyama, Y., Subramanian, S. V., et al. (2016). Increased risk of dementia in the aftermath of the 2011 Great East Japan Earthquake and Tsunami. Proc. Natl. Acad. Sci. 113, E6911–E6918. doi: 10.1073/pnas.1607793113
Hildon, Z., Montgomery, S. M., Blane, D., Wiggins, R. D., and Netuveli, G. (2010). Examining resilience of quality of life in the face of health-related and psychosocial adversity at older ages: What is “right”. About the Way We Age? Gerontologist 50, 36–47. doi: 10.1093/geront/gnp067
Jawaid, A. (2020). Protecting older adults during social distancing. Science 368, 145–145. doi: 10.1126/science.abb7885
Johns Hopkins University Coronavirus Resource Center. (2023). COVID-19 Dashboard. Available online at: https://coronavirus.jhu.edu/map.html (accessed February 12, 2025).
Jones, E. A. K., Mitra, A. K., and Bhuiyan, A. R. (2021). Impact of COVID-19 on mental health in adolescents: A systematic review. Int. J. Environ. Res. Public Health 18:2470. doi: 10.3390/ijerph18052470
Lamond, A. J., Depp, C. A., Allison, M., Langer, R., Reichstadt, J., Moore, D. J., et al. (2008). Measurement and predictors of resilience among community-dwelling older women. J. Psychiatr. Res. 43, 148–154. doi: 10.1016/j.jpsychires.2008.03.007
Li, S., Wang, Y., Xue, J., Zhao, N., and Zhu, T. (2020). The Impact of COVID-19 epidemic declaration on psychological consequences: A study on active weibo users. Int. J. Environ. Res. Pubblic Health 17:2032. doi: 10.3390/ijerph17062032
Londero, I., and da Rocha, N. S. (2024). Personality dimensions, resilience, and depression during COVID-19 pandemic: A one-year longitudinal study. Acta Psychol. 245:104229. doi: 10.1016/j.actpsy.2024.104229
MacLeod, S., Musich, S., Hawkins, K., Alsgaard, K., and Wicker, E. R. (2016). The impact of resilience among older adults. Geriatr. Nurs. 37, 266–272. doi: 10.1016/j.gerinurse.2016.02.014
Ministry of Health (BR). (2024). Ministério da Saúde - COVID-19 NO BRASIL. Available online at: https://infoms.saude.gov.br/extensions/covid-19_html/covid-19_html.html (accessed February 12, 2025).
Na, L., Yang, L., Mezo, P. G., and Liu, R. (2022). Age disparities in mental health during the COVID19 pandemic: The roles of resilience and coping. Soc. Sci. Med. 305:115031. doi: 10.1016/j.socscimed.2022.115031
Nygren, B., Aléx, L., Jonsén, E., Gustafson, Y., Norberg, A., and Lundman, B. (2005). Resilience, sense of coherence, purpose in life and self-transcendence in relation to perceived physical and mental health among the oldest old. Aging Ment. Health 9, 354–362. doi: 10.1080/1360500114415
Pardeller, S., Kemmler, G., Hoertnagl, C. M., and Hofer, A. (2020). Associations between resilience and quality of life in patients experiencing a depressive episode. Psychiatry Res. 292:113353. doi: 10.1016/j.psychres.2020.113353
Pires, A. C., Fleck, M. P., Power, M., and da Rocha, N. S. (2018). Psychometric properties of the EUROHIS-QOL 8-item index (WHOQOL-8) in a Brazilian sample. Rev. Bras. Psiquiatria 40, 249–255. doi: 10.1590/1516-4446-2017-2297
Preacher, K. J., and Hayes, A. F. (2004). SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instruments Comput. 36, 717–731. doi: 10.3758/BF03206553
Rafiey, H., Momtaz, Y., Alipour, F., Khankeh, H., Ahmadi, S., Sabzi Khoshnami, M., et al. (2016). Are older people more vulnerable to long-term impacts of disasters? Clin. Interv. Aging 11, 1791–1795. doi: 10.2147/CIA.S122122
Santos, I. S., Tavares, B. F., Munhoz, T. N., Almeida, L. S. P., de, Silva, N. T. B., et al. (2013). Sensibilidade e especificidade do Patient Health Questionnaire-9 (PHQ-9) entre adultos da população geral. Cad Saude Publ. 29, 1533–1543. doi: 10.1590/0102-311X00144612
Schmitt, A. A., Brenner, A. M., Primo, de Carvalho Alves, L., Claudino, F. C., de, A., et al. (2021). Potential predictors of depressive symptoms during the initial stage of the COVID-19 outbreak among Brazilian adults. J. Affect. Disord. 282, 1090–1095. doi: 10.1016/j.jad.2020.12.203
Shen, K., and Zeng, Y. (2010). The association between resilience and survival among Chinese elderly. Demogr. Res. 23, 105–116. doi: 10.4054/DemRes.2010.23.5
Shi, M., Wang, X., Bian, Y., and Wang, L. (2015). The mediating role of resilience in the relationship between stress and life satisfaction among Chinese medical students: A cross-sectional study. BMC Med. Educ. 15:16. doi: 10.1186/s12909-015-0297-2
Silva Júnior, E. G., da, Eulálio, M., do, C., Souto, R. Q., Santos, K., et al. (2019). A capacidade de resiliência e suporte social em idosos urbanos. Cien Saude Colet 24, 7–16. doi: 10.1590/1413-81232018241.32722016
Solano, J. P. C., Bracher, E. S. B., Faisal-Cury, A., Ashmawi, H. A., Carmona, M. J. C., Lotufo Neto, F., et al. (2016). Factor structure and psychometric properties of the connor-davidson resilience scale among Brazilian adult patients. Sao Paulo Med. J. 134, 400–406. doi: 10.1590/1516-3180.2015.02290512
Southwick, S. M., Bonanno, G. A., Masten, A. S., Panter-Brick, C., and Yehuda, R. (2014). Resilience definitions, theory, and challenges: Interdisciplinary perspectives. Eur. J. Psychotraumatol. 5, doi: 10.3402/ejpt.v5.25338
Southwick, S. M., Sippel, L., Krystal, J., Charney, D., Mayes, L., and Pietrzak, R. (2016). Why are some individuals more resilient than others: The role of social support. World Psychiatry 15, 77–79. doi: 10.1002/wps.20282
Staneva, A., Carmignani, F., and Rohde, N. (2022). Personality, gender, and age resilience to the mental health effects of COVID-19. Soc. Sci. Med. 301:114884. doi: 10.1016/j.socscimed.2022.114884
Weitzel, E. C., Löbner, M., Röhr, S., Pabst, A., Reininghaus, U., and Riedel-Heller, S. G. (2021). Prevalence of high resilience in old age and association with perceived threat of COVID-19—results from a representative survey. Int. J. Environ. Res. Public Health 18:7173. doi: 10.3390/ijerph18137173
Xu, Y., Ni, Y., Yang, J., Wu, J., Lin, Y., Li, J., et al. (2024). The relationship between the psychological resilience and post-traumatic growth of college students during the COVID-19 pandemic: A model of conditioned processes mediated by negative emotions and moderated by deliberate rumination. BMC Psychol. 12:357. doi: 10.1186/s40359-024-01853-z
Ye, Z., Wei, X., Zhang, J., Li, H., and Cao, J. (2024). The impact of adverse childhood experiences on depression: The role of insecure attachment styles and emotion dysregulation strategies. Curr. Psychol. 43, 4016–4026. doi: 10.1007/s12144-023-04613-1
Zeng, Y., and Shen, K. (2010). Resilience significantly contributes to exceptional longevity. Curr. Gerontol. Geriatr. Res. 2010, 1–9. doi: 10.1155/2010/525693
Zhang, H., Zhao, Q., Cao, P., and Ren, G. (2017). Resilience and quality of life: Exploring the mediator role of social support in patients with breast cancer. Med. Sci. Monitor 23, 5969–5979. doi: 10.12659/MSM.907730
Keywords: COVID-19, resilience, older adults, quality of life, spirituality
Citation: Gonçalves L, Reggiani LC, Maliuk J, de Souza GR, Bandeira de Mello RG, Carniel BP and da Rocha NS (2025) Age and resilience amid COVID-19 pandemic adversity: the mediating roles of quality of life, spirituality, and depressive symptoms. Front. Psychol. 16:1576150. doi: 10.3389/fpsyg.2025.1576150
Received: 13 February 2025; Accepted: 28 July 2025;
Published: 12 August 2025.
Edited by:
Mateusz Krystian Grajek, Medical University of Silesia in Katowice, PolandReviewed by:
Helena Chui, Charles Darwin University, AustraliaIuliia Pavlova, Lviv State University of Physical Culture, Ukraine
Copyright © 2025 Gonçalves, Reggiani, Maliuk, de Souza, Bandeira de Mello, Carniel and da Rocha. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lorenzo Casagrande Reggiani, bHJlZ2dpYW5pQGhjcGEuZWR1LmJy
†These authors have contributed equally to this work and share first authorship