 Martine Hébert
Martine Hébert Valérie Théorêt
Valérie Théorêt Amélie Tremblay-Perreault
Amélie Tremblay-Perreault Antonio Zadra
Antonio Zadra- 1Département de Sexologie, Université du Québec à Montréal, Montréal, QC, Canada
- 2École de Criminologie, Université de Montréal, Montréal, QC, Canada
- 3Département de Psychologie, Université de Montréal, Montréal, QC, Canada
Introduction: Sleep disturbances represent a major concern for many adolescents. While adolescents with a history of trauma may be particularly vulnerable to sleep disturbances, the mechanisms underlying the association between childhood sexual abuse and sleep disturbances (e.g., having trouble falling asleep, nightmares) remain understudied. The present study aimed to: (1) explore sleep disturbances among adolescents with a history of childhood sexual abuse, and (2) investigate the mediating role of PTSD symptoms in the association between childhood sexual abuse and sleep disturbances.
Methods: Data were drawn from a representative sample of 8,194 adolescents in grades 9 to 11. The history of childhood sexual abuse and PTSD symptoms were assessed at Time 1, whereas sleep disturbances were assessed 6 months later (Time 2) using self-reported questionnaires.
Results: Adolescents who experienced childhood sexual abuse were more likely to report sleep disturbances than those who experienced other forms of childhood adversity. Sexual abuse was associated with higher levels of PTSD symptoms at Time 1, which, in turn, predicted more sleep disturbances at Time 2.
Discussion: These findings suggest that sleep disturbances should be monitored and addressed in trauma-focused therapy for youth victims of childhood sexual abuse.
1 Introduction
The importance of sleep in adolescence is well established, as it supports brain development, cognitive function, and mental well-being (Anastasiades et al., 2022; Spruyt, 2024; Tarokh et al., 2016). Many concerns have been expressed and documented regarding deficient sleep in adolescents. Factors such as natural changes in the circadian rhythm, school start times, and evening use of social media have all been linked to sleep problems in adolescents (Barlaan et al., 2022; Owens and Weiss, 2017; Tarokh et al., 2016). Trauma exposure in adolescence has also been found to have both immediate and long-lasting impacts on sleep (Barrera-Valencia et al., 2025; Giannakopoulos and Kolaitis, 2021; Zarchev et al., 2025). In their review, Langevin et al. (2022) reported that child sexual abuse (CSA) is associated with various sleep disturbances during adolescence, including lower levels of sleep efficiency, sleep satisfaction, and sleep duration. However, few studies have attempted to identify mechanisms explaining the association between exposure to trauma and sleep disturbances in youth, and even fewer have specifically focused on a sample of CSA victims. Given that CSA sometimes takes place in sleep-related contexts, CSA may have a particularly strong relationship with sleep disturbances when compared to other trauma types. Moreover, CSA appears to be the most synergistic form of trauma exposure, implying that having experienced CSA potentiates its consequences when paired with another adverse childhood experience (Briggs et al., 2021).
Among various mechanisms linking CSA to sleep disturbances, symptoms of post-traumatic stress disorder (PTSD) are of interest. PTSD is a well-known sequela of CSA (Hailes et al., 2019), and PTSD and sleep problems are so closely related that nightmares and other sleep disturbances are included as symptoms of intrusion and alterations in arousal in the DSM-5 criteria for PTSD (American Psychiatric Association, 2022). The hyperarousal-based theory of sleep disturbances posits that PTSD induces a state of heightened arousal that disrupts the conditions necessary for good sleep quality (Mellman, 1997). Additionally, PTSD can lead survivors to reexperience trauma-related cues in their minds, triggering physiological arousal and negative emotions, which further interfere with sleep (Giannakopoulos and Kolaitis, 2021). It should be noted, however, that sleep problems are not only a symptom of past trauma, but also a potential mechanism through which trauma contributes to long-term health and psychological difficulties (Anda et al., 2006; Chapman et al., 2011; Hillebrant-Openshaw and Wong, 2023). Several studies have supported PTSD as a predictor of sleep disturbances, although the vast majority of these have been conducted on adult participants (Babson and Feldner, 2010; Milanak et al., 2019; Zhang et al., 2019). Further research is warranted to better contextualize these associations in light of the unique developmental processes of adolescence.
CSA, as basically any other form of adverse childhood experience, is often experienced in co-occurrence with one or many other forms of trauma exposure (Hughes et al., 2017). To isolate the specific effect of CSA, other forms of trauma exposure need to be taken into account. Finally, most studies in this field have relied on cross-sectional designs and reviews have highlighted the need to better document the role of sex in the association between trauma and sleep disturbances (e.g., Kajeepeta et al., 2015; Langevin et al., 2022). Girls are more at risk of experiencing CSA and being diagnosed with PTSD (Haag et al., 2020; Hébert et al., 2019). Sex/gender differences have also been observed regarding sleep disturbances in youth, with girls generally reporting more sleep problems, such as sleep onset difficulties and nightmares (Forest et al., 2022; Wan et al., 2020).
To mitigate the limitations of past studies, this study aimed to: (1) compare the levels of sleep disturbances between youth with and without a history of CSA and with respect to sex, and (2) investigate the mediating role of PTSD symptoms in the association between CSA and sleep disturbances, while controlling for sex, age, and cumulative trauma.
2 Methods
2.1 Sample and participants
Data were drawn from the Youth Romantic Relationships Survey (YRRS). A total of 34 high schools in Quebec, Canada were selected to participate in the study using a one-stage stratified cluster sampling method. All students from grades 9 to 11 were invited to complete the survey at each selected school (response rate of 100% for 320 out of 329 classes; the response rate ranged from 90 to 98% for the remaining classes). Students completed the survey in class twice, the first time in the fall of 2011 (T1) and the second time approximately 6 months later (T2). A total of 8,194 adolescents participated in the study at T1. Because the present study focuses on the role of PTSD symptoms in the association between CSA and sleep disturbances, only adolescents who reported at least one childhood adverse experience at T1 on the Short form of the Early Trauma Inventory Self-Report (Bremner et al., 2007) were selected for the analyses (85% of the sample, n = 6,848). Of these, 4,993 completed the questionnaire at T2 (73% response rate). Eight adolescents were excluded from the final sample due to invalid responses. The final sample thus included 6,840 adolescents (58% girls, mean age = 15.5 years). Students agreed to participate on a voluntary basis and signed a written consent form. The institutional review board of the affiliated university approved this study.
2.2 Measures
2.2.1 Adverse childhood experiences
The Short Form of the Early Trauma Inventory Self-Report (Bremner et al., 2007) was used to screen participants who had been exposed to eight different adverse events, including, among others, the death or serious illness of a close relative, intrafamilial physical abuse, witnessing family violence, and parental divorce or separation. Participants who reported none of the events listed in this measure were excluded from the study.
2.2.2 Child sexual abuse
Two items adapted from Finkelhor et al. (1990) assessed unwanted sexual touching and unwanted sexual intercourse: “Have you ever been touched sexually when you did not want to, or have you ever been manipulated, blackmailed, or physically forced to touch sexually?” and “Has anyone ever used manipulation, blackmail, or physical force, to force or obligate you to have sex (including all sexual activities involving oral, vaginal or anal penetration)?” A dichotomized score was created based on the presence (1) or absence (0) of any sexual abuse.
2.2.3 Cumulative childhood trauma
Other forms of child maltreatment were assessed using various indicators. Physical abuse and exposure to physical violence were measured using two items from the Early Trauma Inventory Self-Report–Short Form (Bremner et al., 2007): “Have you ever been physically hit by a member of your family?” and “Have you ever witnessed violence against someone, including a member of your family?” Emotional abuse in childhood was evaluated using two items from the Inventory of Parent and Peer Attachment (Armsden and Greenberg, 1987): “My mother tells me hurtful and/or insulting things” and “My father tells me hurtful and/or insulting things.” Exposure to interparental violence was assessed using an adapted version of the Revised Conflict Tactics Scales (CTS2; Straus et al., 1996), consisting of eight items. These items captured the frequency of exposure to interparental psychological (e.g., “insult, swear, shout, yell”) and physical violence (e.g., “push, shove, slap, throw something that could hurt”), with participants indicating whether they had ever witnessed their mother or father engage in these behaviors. Each indicator was dichotomized, and a cumulative trauma score ranging from 0 to 4 was computed to reflect the number of different maltreatment types experienced.
2.2.4 Post-traumatic stress disorder (PTSD)
Nine items from the Abbreviated University of California at Los Angeles PTSD Reaction Index were used to assess PTSD symptoms following sexual abuse or other adverse life experiences listed in the questionnaire (Cohen et al., 2010). The core dimensions of PTSD were assessed, including intrusion symptoms, avoidance, alterations in arousal and reactivity, and negative alterations in cognitions and mood. We removed two items related to sleep difficulties (i.e., nightmares and difficulty falling/staying asleep) to avoid redundancy with our sleep disturbance measure. Adolescents were asked to rate “How much of the time during the past month” they experienced each symptom on a 5-point Likert scale ranging from None of the time (0) to Most of the time (4). The scale showed high internal consistency in the current study (α = 0.86).
2.2.5 Sleep disturbance
Four items were used to assess sleep disturbance at T2. Respondents rated on a 5-point Likert scale ranging from Never (0) to Very often (4) how often they experienced each sleep disturbance over the last 6 months. Items were as follows: “In the last 6 months…” (1) “Did you have trouble falling asleep or staying asleep?”; (2) “Did you have the feeling of not being rested in the morning?”; (3) “Did you have the feeling of not getting as much sleep as needed?,” and (4) “Did you have nightmares?” (Noll et al., 2006). A cumulative score ranging from 0 to 16 was calculated. The scale demonstrated high internal consistency (α = 0.82) in the present study.
2.3 Statistical analyses
We calculated the prevalence of CSA based on sex using the Pearson χ2 statistic. We also performed two-way ANOVAs to test the effects of sex, CSA, and the CSA x sex interaction on separate sleep disturbance items, PTSD, and the global score of sleep disturbances. We then conducted a mediation model to estimate the direct and indirect effects of CSA on sleep disturbances with PTSD as a mediator. Sex, age, and cumulative trauma were included as covariates in the mediation model. Little’s MCAR test was used to explore the pattern of missingness in the data, and revealed that the data were not MCAR (χ2 = 236.30, df = 9, p < 0.001). Results of logistic regressions found that the observed variables predicted missingness, which suggests that a missing at random (MAR) hypothesis is plausible. Hence, missing values were handled using Full Information Maximum Likelihood (FIML). The mediation model was tested using Mplus software version 8.3 (Muthén and Muthén, 2015). Indirect effects were tested with the ML estimator with the 95% confidence interval bootstrapping technique.
3 Results
3.1 Descriptive analyses
Overall, 10.4% of our youth sample reported having experienced CSA. A higher prevalence of CSA was observed for girls (15.3%) than boys (3.9%; χ2 = 276.41, p < 0.001). ANOVAs showed that scores on all four sleep disturbance items differed statistically by both sex and CSA status (see Table 1). Girls reported significantly higher mean scores for sleep disturbance and PTSD symptoms than boys. Adolescents with a history of CSA also reported more sleep disturbances and PTSD symptoms than those who did not report a history of CSA. The interaction between sex and CSA did not have a significant effect on the study variables. Pearson’s correlations (Table 2) revealed a significant associations between the independent variable (CSA history) and the mediator (PTSD symptoms), as well as between the mediator and the dependent variable (sleep disturbances), thereby meeting the prerequisites for testing a mediation model.
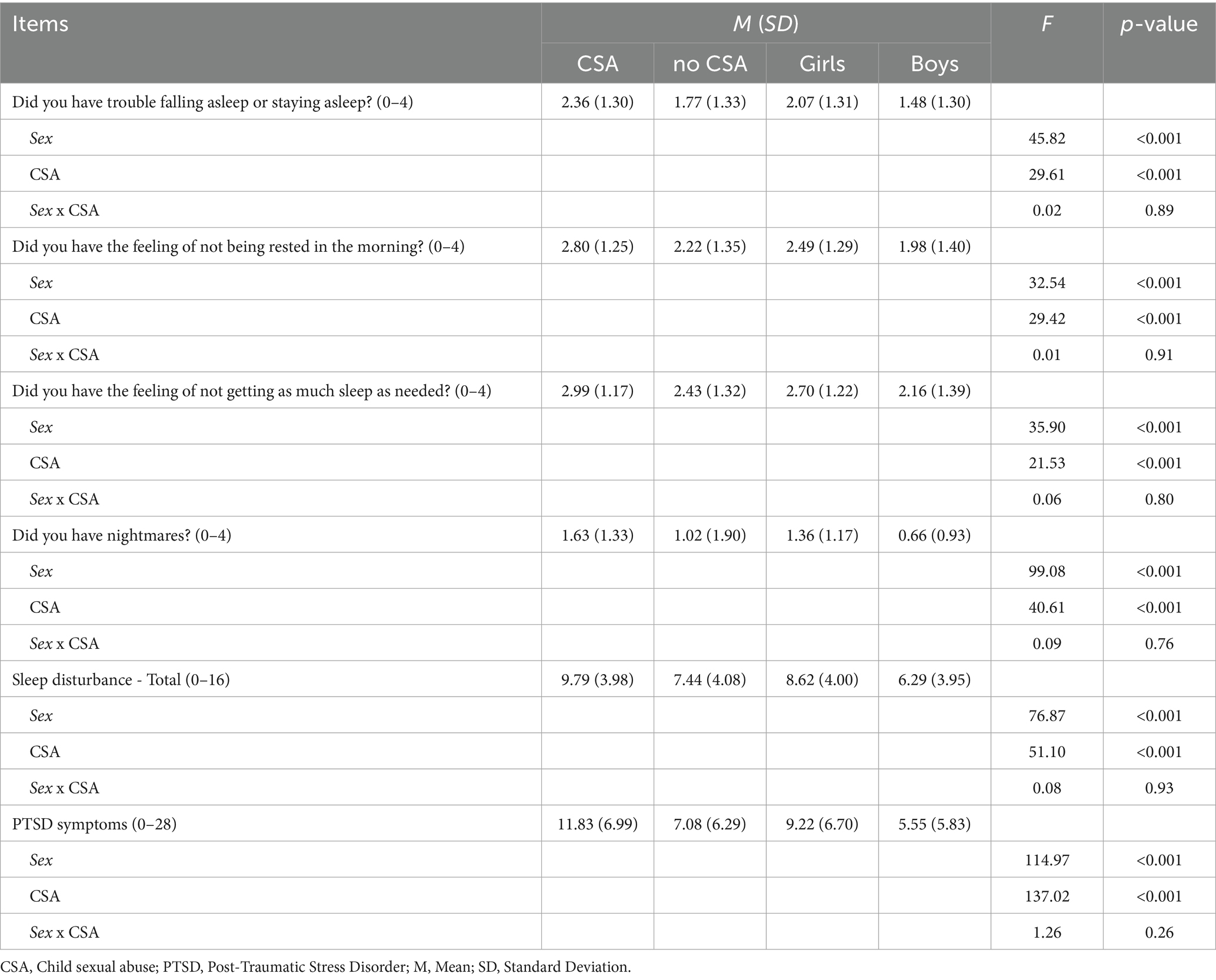
Table 1. ANOVAs results and descriptive statistics for sleep disturbance and PTSD symptoms by sex and sexual abuse history.
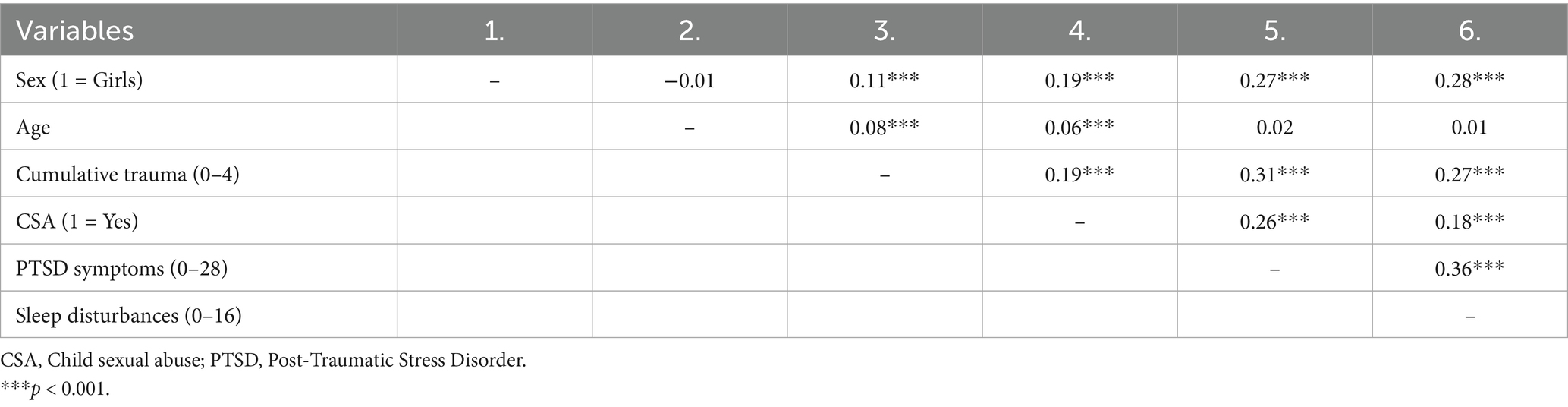
Table 2. Pearson correlations between study variables.
3.2 Mediation model results
A mediation analysis was conducted to examine whether PTSD symptoms mediated the association between CSA and sleep disturbances after controlling for covariates (sex, cumulative trauma, and age). The indirect effect between CSA and sleep disturbances through PTSD symptoms was significant [β = 0.04, 95% bootstrap CI (0.03, 0.05)]. CSA was thus associated with higher levels of PTSD symptoms at T1 [β = 0.16, 95% bootstrap CI (0.13, 0.18)], which, in turn, predicted greater sleep disturbances at T2 [β = 0.25, 95% bootstrap CI (0.21, 0.28)]. The direct effect between CSA and sleep disturbances remained significant [β = 0.07, 95% bootstrap CI (0.04, 0.10)]. The overall model accounted for 20% of explained variance for sleep disturbances and 18% of explained variance for PTSD symptoms. Model fit statistics are not reported as the model was just identified (zero degrees of freedom). Mediation model results are presented in Figure 1.
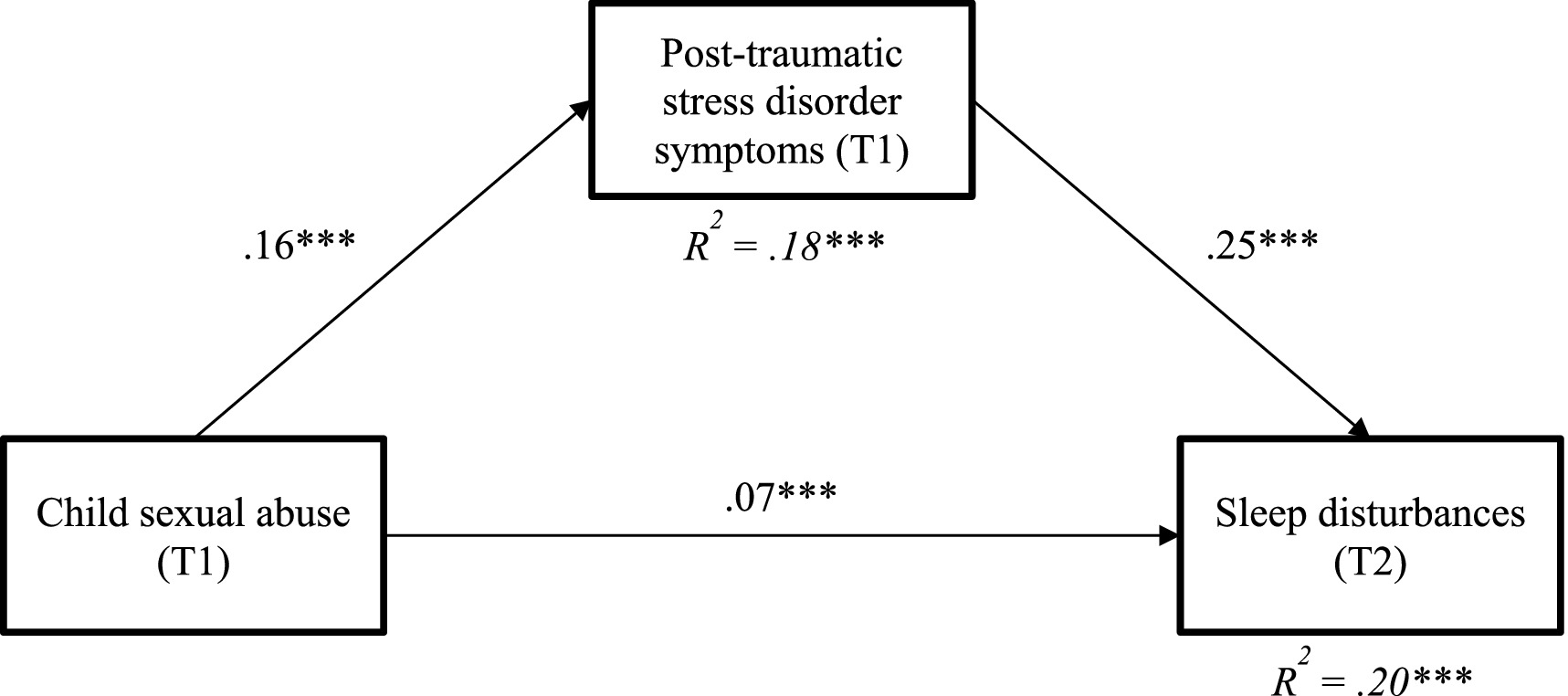
Figure 1. Results of mediation model linking child sexual abuse, post-traumatic stress disorde symptoms and sleep disturbances. Only significant paths are represented. Sex, cumulative trauma, and age included as controlling variables not depicted in the figure for parcimony.
4 Discussion
This study aimed to document sleep disturbances among adolescents with a history of CSA and to assess the role of PTSD symptoms in the association between CSA and sleep disturbances. The results indicate that adolescents with a history of CSA are more likely to experience sleep disturbances than those with other childhood adverse experiences. Moreover, CSA was related to sleep disturbances through PTSD symptoms. Possible explanations for these findings include the impact of PTSD-related hyperarousal and fear responses on sleep onset and sleep quality (Giannakopoulos and Kolaitis, 2021). Reporting a history of CSA also predicted sleep disturbances independently of PTSD symptoms, indicating that other mechanisms could be at play (e.g., Giannakopoulos and Kolaitis, 2021). The indirect association between child sexual abuse and sleep disturbances via PTSD symptoms was significant after controlling for other forms of child maltreatment experienced.
This study has several strengths, including its reliance on a longitudinal design to explore potential mechanisms underlying the link between CSA and sleep disturbances. However, the findings are subject to important limitations. First, this study relied on abbreviated measures of PTSD symptoms as well as of sleep disturbances. Future studies should employ more comprehensive assessments instruments to ensure a more thorough and inclusive evaluation of these constructs. For example, future studies assessing self-reported sleep disturbances in relation to CSA could include more comprehensive sleep assessment instruments such as the Pittsburgh Sleep Quality Index (Buysse et al., 1989), a validated questionnaire assessing several dimensions of self-reported sleep problems within the previous month, including subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. Second, the study’s design did not allow for the assessment of bidirectional relationships between PTSD symptoms and sleep disturbances. Further investigations are needed to explore the possible alternative temporal sequences of these variables. The 6-month follow-up interval may not fully capture the longer-term unfolding of mediation processes. In addition, while PTSD symptoms were modeled as a mediator, they could alternatively be conceptualized as covariates or co-occurring responses to trauma, and future longitudinal studies with multiple assessment points would help further disentangle these potential pathways. Finally, the developmental context of adolescence, characterized by biological changes in sleep–wake cycles, increased emotional reactivity, and evolving social demands, may further exacerbate the impact of trauma on sleep disturbances. Future studies would benefit from explicitly examining how developmental stages interact with trauma-related variables in predicting sleep outcomes.
Our results offer several implications for clinical practice. Given the association between PTSD and sleep disturbances in teenagers with a history of CSA, therapeutic interventions should integrate PTSD treatment with strategies specifically targeting sleep disturbances. An approach combining evidence-based practices tailored to address both PTSD (e.g., Trauma-Focused Cognitive Behavioral Therapy; Cohen et al., 2016) and its impact on sleep and persistent nightmares (e.g., imagery rehearsal therapy, cognitive behavioral therapy for insomnia; Miller et al., 2020) could be warranted.
5 Conclusion
This longitudinal study highlights the significant impact of CSA on sleep disturbances among adolescents, with PTSD symptoms playing a crucial mediating role. The findings underscore the necessity for practitioners to routinely assess sleep disturbances in adolescents with a history of CSA and to integrate PTSD-focused therapies with sleep-specific interventions.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study involving humans was approved by Université du Québec à Montréal. The study was conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent from the participants’ legal guardians/next of kin because in the province of Quebec, Canada, adolescents aged 14 to 18 years can consent to research participation without parental approval if the research involves minimal risk. This aligns with Quebec’s Civil Code, which grants minors 14 years and older the legal capacity to consent.
Author contributions
MH: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. VT: Formal analysis, Writing – original draft, Writing – review & editing. AT-P: Writing – original draft, Writing – review & editing. AZ: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Canadian Institutes of Health Research [Grant # 103944] and the Canada Research Chair in Interpersonal Traumas and Resilience [Grant # 2021-00254].
Acknowledgments
The authors wish to thank the teenagers and the school personnel that participated in the Youth Romantic Relationships Survey. Our thanks also extend to Catherine Moreau for project coordination, Manon Robichaud for data management and Essaïd Oussaïd for preliminary analyses.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
American Psychiatric Association (2022). Diagnostic and statistical manual of mental disorders. 5th Edn. American Psychiatric Association.
Anastasiades, P. G., de Vivo, L., Bellesi, M., and Jones, M. W. (2022). Adolescent sleep and the foundations of prefrontal cortical development and dysfunction. Prog. Neurobiol. 218:102338. doi: 10.1016/j.pneurobio.2022.102338
Anda, R. F., Felitti, V. J., Bremner, J. D., Walker, J. D., Whitfield, C., Perry, B. D., et al. (2006). The enduring effects of abuse and related adverse experiences in childhood. A convergence of evidence from neurobiology and epidemiology. Eur. Arch. Psychiatry Clin. Neurosci. 256, 174–186. doi: 10.1007/s00406-005-0624-4
Armsden, G. C., and Greenberg, M. T. (1987). The inventory of parent and peer attachment: individual differences and their relationship to psychological well-being in adolescence. J. Youth Adolesc. 16, 427–454. doi: 10.1007/BF02202939
Babson, K. A., and Feldner, M. T. (2010). Temporal relations between sleep problems and both traumatic event exposure and PTSD: a critical review of the empirical literature. J. Anxiety Disord. 24, 1–15. doi: 10.1016/j.janxdis.2009.08.002
Barlaan, D. R., Pangelinan, B. A., Johns, A., Schweikhard, A., and Cromer, L. D. (2022). Middle school start times and young adolescent sleep, behavioral health, and academic performance outcomes: a narrative review. J. Clin. Sleep Med. 18, 2681–2694. doi: 10.5664/jcsm.10224
Barrera-Valencia, M., Calderon-Delgado, L., and Adan, A. (2025). Sleep quality and cognitive impairments in children and adolescents with post traumatic stress disorder and/or depressive symptoms. J. Clin. Med. 14:1010. doi: 10.3390/jcm14031010
Bremner, J. D., Bolus, R., and Mayer, E. A. (2007). Psychometric properties of the early trauma inventory–self-report. J. Nerv. Ment. Dis. 195, 211–218. doi: 10.1097/01.nmd.0000243824.84651.6c
Briggs, E. C., Amaya-Jackson, L., Putnam, K. T., and Putnam, F. W. (2021). All adverse childhood experiences are not equal: the contribution of synergy to adverse childhood experience scores. Am. Psychol. 76, 243–252. doi: 10.1037/amp0000768
Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R., and Kupfer, D. J. (1989). The Pittsburgh sleep quality index (PSQI): a new instrument for psychiatric research and practice. Psychiatry Res. 28, 193–213. doi: 10.1016/0165-1781(89)90047-4
Chapman, D. P., Wheaton, A. G., Anda, R. F., Croft, J. B., Edwards, V. J., Liu, Y., et al. (2011). Adverse childhood experiences and sleep disturbances in adults. Sleep Med. 12, 773–779. doi: 10.1016/j.sleep.2011.03.013
Cohen, J. A., Bukstein, O., Walter, H., Benson, S. R., Chrisman, A., Farchione, T. R., et al. (2010). The work group on quality issues. Practice parameter for the assessment and treatment of children and adolescents with posttraumatic stress disorder. J. Am. Acad. Child. Adolesc. Psychiatry 49, 414–430.
Cohen, J. A., Mannarino, A. P., and Deblinger, E. (2016). Treating trauma and traumatic grief in children and adolescents. New York, NY: Guilford Publications.
Finkelhor, D., Hotaling, G., Lewis, I. A., and Smith, C. (1990). Sexual abuse in a national survey of adult men and women: prevalence, characteristics, and risk factors. Child Abuse Negl. 14, 19–28. doi: 10.1016/0145-2134(90)90077-7
Forest, G., Gaudreault, P., Michaud, F., and Green-Demers, I. (2022). Gender differences in the interference of sleep difficulties and daytime sleepiness on school and social activities in adolescents. Sleep Med. 100, 79–84. doi: 10.1016/j.sleep.2022.07.020
Giannakopoulos, G., and Kolaitis, G. (2021). Sleep problems in children and adolescents following traumatic life events. World J Psychiatry 11, 27–34. doi: 10.5498/wjp.v11.i2.27
Haag, K., Fraser, A., Hiller, R., Seedat, S., Zimmerman, A., and Halligan, S. L. (2020). The emergence of sex differences in PTSD symptoms across development: evidence from the ALSPAC cohort. Psychol. Med. 50, 1755–1760. doi: 10.1017/S0033291719001971
Hailes, H. P., Yu, R., Danese, A., and Fazel, S. (2019). Long-term outcomes of childhood sexual abuse: an umbrella review. Lancet Psychiatry 6, 830–839. doi: 10.1016/S2215-0366(19)30286-X
Hébert, M., Amédée, L. M., Blais, M., and Gauthier-Duchesne, A. (2019). Child sexual abuse among a representative sample of Quebec high school students: prevalence and association with mental health problems and health-risk behaviors. Can. J. Psychiatr. 64, 846–854. doi: 10.1177/0706743719861387
Hillebrant-Openshaw, M. J., and Wong, M. M. (2023). The mediating role of sleep quality, regularity, and insomnia on the relationship between adverse childhood experiences and resilience. J. Child Adolesc. Trauma 17, 1–11. doi: 10.1007/s40653-023-00595-1
Hughes, K., Bellis, M. A., Hardcastle, K. A., Sethi, D., Butchart, A., Mikton, C., et al. (2017). The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. Lancet Public Health 2, e356–e366. doi: 10.1016/S2468-2667(17)30118-4
Kajeepeta, S., Gelaye, B., Jackson, C. L., and Williams, M. A. (2015). Adverse childhood experiences are associated with adult sleep disorders: a systematic review. Sleep Med. 16, 320–330. doi: 10.1016/j.sleep.2014.12.013
Langevin, R., Kenny, S., Kern, A., Kingsland, E., and Pennestri, M.-H. (2022). Sexual abuse and sleep in children and adolescents: a systematic review. Sleep Med. Rev. 64:101628. doi: 10.1016/j.smrv.2022.101628
Mellman, T. A. (1997). Psychobiology of sleep disturbances in posttraumatic stress disorder. Ann. N. Y. Acad. Sci. 821, 142–149. doi: 10.1111/j.1749-6632.1997.tb48275.x
Milanak, M. E., Zuromski, K. L., Cero, I., Wilkerson, A. K., Resnick, H. S., and Kilpatrick, D. G. (2019). Traumatic event exposure, posttraumatic stress disorder, and sleep disturbances in a national sample of U.S. adults. J. Trauma. Stress. 32, 14–22. doi: 10.1002/jts.22360
Miller, K. E., Brownlow, J. A., and Gehrman, P. R. (2020). Sleep in PTSD: treatment approaches and outcomes. Curr. Opin. Psychol. 34, 12–17. doi: 10.1016/j.copsyc.2019.08.017
Noll, J. G., Trickett, P. K., Susman, E. J., and Putnam, F. W. (2006). Sleep disturbances and childhood sexual abuse. J. Pediatr. Psychol. 31, 469–480. doi: 10.1093/jpepsy/jsj040
Owens, J. A., and Weiss, M. R. (2017). Insufficient sleep in adolescents: causes and consequences. Minerva Pediatr. 69, 326–336. doi: 10.23736/s0026-4946.17.04914-3
Spruyt, K. (2024). Neurocognitive effects of sleep disruption in children and adolescents. Psychiatr. Clin. North Am. 47, 27–45. doi: 10.1016/j.psc.2023.06.003
Straus, M. A., Hamby, S. L., Boney-McCoy, S., and David, B. S. (1996). The revised conflict tactics scales (CTS2): development and preliminary psychometric data. J. Fam. Issues 17, 283–316. doi: 10.1177/019251396017003001
Tarokh, L., Saletin, J. M., and Carskadon, M. A. (2016). Sleep in adolescence: physiology, cognition and mental health. Neurosci. Biobehav. Rev. 70, 182–188. doi: 10.1016/j.neubiorev.2016.08.008
Wan, Y., Xu, H., Wang, S., Boyda, D., Mcfeeters, D., Sun, Y., et al. (2020). Gender differences in the relationship between sleep problems and suicide attempt in adolescents. Front. Psych. 11:133. doi: 10.3389/fpsyt.2020.00133
Zarchev, M., Kamperman, A. M., Hoepel, S. J. W., Hoogendijk, W. J. G., Mulder, C. L., and Grootendorst-van Mil, N. H. (2025). The association between childhood maltreatment and multidimensional sleep health in adolescents at high risk of emotional and behavioral problems. Sleep 48:zsae 281. doi: 10.1093/sleep/zsae281
Keywords: trauma, sexual violence, adolescents, sleep impairment, sexual abuse
Citation: Hébert M, Théorêt V, Tremblay-Perreault A and Zadra A (2025) Child sexual abuse and sleep disturbances among adolescents: the role of post-traumatic stress disorder symptoms. Front. Psychol. 16:1580679. doi: 10.3389/fpsyg.2025.1580679
Edited by:
Jeffrey S. Bedwell, University of Central Florida, United StatesReviewed by:
Kennedy Amone-P’Olak, University of the Witwatersrand, South AfricaAmrita Pal, University of California, Los Angeles, United States
Copyright © 2025 Hébert, Théorêt, Tremblay-Perreault and Zadra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martine Hébert, aGViZXJ0Lm1AdXFhbS5jYQ==
†ORCID ID: Martine Hébert, orcid.org/0000-0002-4531-5124
Valérie Théorêt, orcid.org/0000-0003-0751-9895
Amélie Tremblay-Perreault, orcid.org/0000-0002-2908-3976
Antonio Zadra, orcid.org/0000-0003-3671-7081