 Karina Badura-Brzoza
Karina Badura-Brzoza Patryk Główczyński
Patryk Główczyński Dominika Tatar
Dominika Tatar Paweł Dębski
Paweł Dębski- Clinical Department of Psychiatry, Faculty of Medical Sciences in Zabrze, Medical University of Silesia, Katowice, Poland
Aim: To assess perceived social support and its relationship with symptoms of depression and anxiety among secondary school students in a crisis situation such was the outbreak of the Russian-Ukrainian war and the ongoing Covid 19 pandemic.
Materials and methods: The study involved 1,456 students aged 14–19 (mean age 16.77 ± 1.33), including 776 girls and 680 boys. Data were collected during a single data collection period from February 2022 to May 2022. Participants completed the Multidimensional Scale of Perceived Social Support (MSPSS), Children’s Depression Inventory 2 (CDI-2), the State–Trait Anxiety Inventory (STAI-X1), and a sociodemographic questionnaire. Data were analyzed using non-parametric tests and correlation analyses.
Results: Girls reported significantly higher levels of perceived social support from significant people and friends as well as higher symptoms of depression and anxiety, compared to boys. Negative correlations were found between perceived social support and symptoms of depression and anxiety in both genders.
Conclusion: The conducted research indicates that perceived social support may play an important role in coping with symptoms of anxiety and depression in crisis situations.
1 Introduction
1.1 Social support: definition and significance
Social support encompasses all resources available to an individual, which are utilized in difficult situations to cope with stress arising from those circumstances (Cohen, 2004; Sikora, 2012; Lin et al., 1985). At every stage of life, people form more or less extensive social networks, maintained through bonds that connect them with others. Social support can have a direct impact on a person’s health at any point in their life regardless of the occurrence of challenging situations. It can also act as a moderator that positively influences well-being at the exact moment when a stressor occurs or immediately afterwards (Lin et al., 1985; Reicher, 1997; Yarchesky et al., 2001; Cohen and Hoberman, 1983). These two models are not mutually exclusive but rather complementary, offering a framework for understanding how specific aspects of social relationships influence mental health (Buszman and Przybyła-Basista, 2017). Research indicates that support networks are formed throughout the human lifespan and exist even when their activation is not immediately necessary. The most important networks are the natural ones, such as family, friends, close acquaintances, and social groups to which an individual belongs. Scholars emphasize the vital role of social support in shaping overall well-being and its significant effects on both physical and mental health (Uchino et al., 1996; Reblin and Uchino, 2008).
1.2 Adolescence and the role of social support
Adolescents constitute a group for which social support—particularly from peers—is of crucial importance. Maturation is inherently a challenging process, during which identity formation occurs alongside the development of social bonds. This period is marked by the creation of friendships that often lasts a lifetime, forming a key foundation of social support. It is also a time when young people tend to loosen ties with their parents in favor of emerging peer relationships (Sikora, 2012; Stanton-Salazar and Urso-Spina, 2005).
1.3 Global challenges and study aim
In recent years, the world has faced specific and unprecedented challenges related to the COVID-19 pandemic, compounded by the outbreak of the Russian–Ukrainian war. These two global events, largely unforeseen by most individuals, have become sources of immense stress (Kobylarczyk-Kaczmarek, 2023; Sikorska et al., 2021; Szredzińska and Włodarczyk, 2021; Cipora and Mielnik, 2022; Machniak, 2022). Such stress could be particularly pronounced among adolescents. Sudden changes in daily functioning, school closures, remote learning, and restrictions on leaving home were all factors that likely had a profound impact on teenagers. For this group, their understanding of the world is still developing and psychological defense mechanisms are often immature (Szredzińska and Włodarczyk, 2021; Pyżalski, 2021; Jaskulska et al., 2021). According to research, during this period, pre-existing mental health problems in adolescents tended to worsen, and many experienced mental health difficulties for the first time (Kobylarczyk-Kaczmarek, 2023; Sikorska et al., 2021; Szredzińska and Włodarczyk, 2021; Cipora and Mielnik, 2022; Machniak, 2022; Pyżalski, 2021). A significant increase in mental disorders was observed among school-aged youth. It is a trend that continues to rise (Kobylarczyk-Kaczmarek, 2023; Sikorska et al., 2021; Szredzińska and Włodarczyk, 2021; Poleszak and Katab, 2022). In such a challenging context, social support may have played a crucial protective role in reducing the risk of anxiety and depressive disorders (Kobylarczyk-Kaczmarek, 2023; Szredzińska and Włodarczyk, 2021; Pyżalski, 2021; Jaskulska et al., 2021; Poleszak and Katab, 2022; Maraszkiewicz, 2022). The aim of this study was to assess perceived social support and the severity of symptoms of depression and anxiety among students from Polish secondary schools in in the crisis situations of the COVID-19 pandemic and the war in Ukraine.
2 Procedure and participants
The study was conducted among secondary school students across the province of Silesian Voivodeship in Poland. Prior to data collection, written invitations to participate in the study were sent to 143 randomly selected secondary schools. School principals were informed in advance about the purpose and objectives of the study. From 143 schools, 56 agreed to take part in the project facilitated the distribution of the online survey to their students. The survey was administered electronically via a Google Form, which was sent to students through school email systems. Data were collected during a single data collection period from February 2022 to May 2022. The Google Form was constructed to accept only fully completed questionnaires. No distinction was made between specific sociopolitical or public health contexts (e.g., the COVID-19 pandemic or the war in Ukraine). However, it was noted in the introductory information that the study aimed to assess the relationship between the current well-being of the respondents and the context of difficult events such as the pandemic and the outbreak of the Russian-Ukrainian war.
A total of 1,456 students aged 14 to 19 participated in the study (M = 16.77, SD = 1.33), including 776 girls (M = 16.78, SD = 1.34) and 680 boys (M = 16.77, SD = 1.36). All respondents provided informed consent, and for those under the age of 18, parental consent was also obtained in accordance with ethical guidelines. Demographic data regarding the study group, divided into girls and boys, are presented in Table 1.
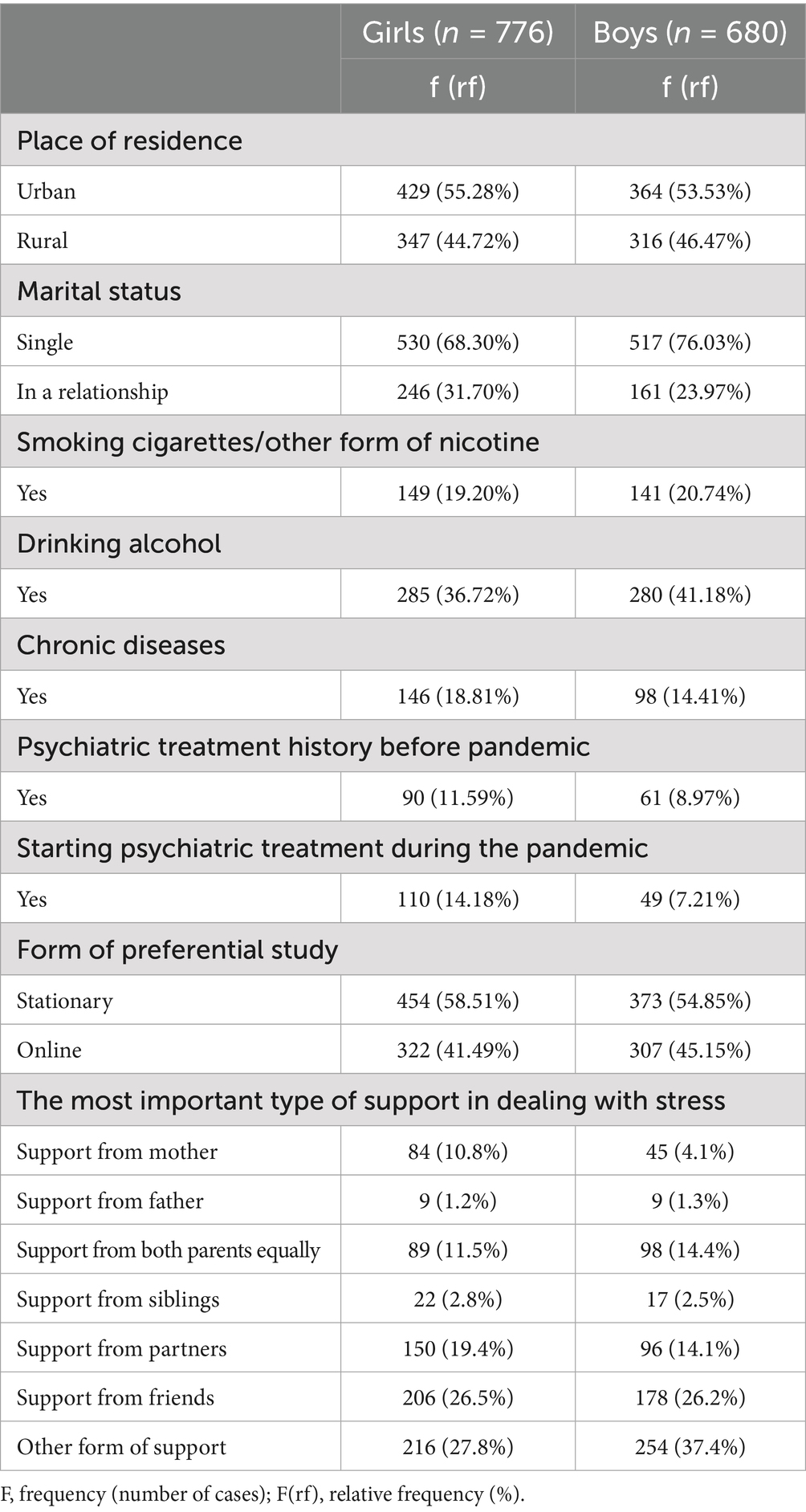
Table 1. Socio-demographic characteristics of the group (n = 1,456).
3 Measures
3.1 The multidimensional scale of perceived social support (MSPSS)
The multidimensional scale of perceived social support (MSPSS) takes into account the multidimensionality of perceived social support, considering three basic sources of support: a significant other, family and friends. The scale consists of 12 statements to which the respondent refers using a seven-point Likert scale, where 1 means “I strongly disagree” and 7 means “I strongly agree.” The scale was adapted to Polish conditions, and adaptation studies showed its satisfactory psychometric properties (Buszman and Przybyła-Basista, 2017).
3.2 Children’s depression inventory 2nd edition (CDI 2)
The instrument allows for the identification of children and adolescents suffering from depressive symptoms, and can also help in the diagnosis of clinical depression. As part of the Polish adaptation, standards were developed for people aged 7 to 18. The set of questionnaires includes versions intended for children and adolescents (self-assessment sheet), parents and teachers. The full version of the self-assessment sheet includes 28 items regarding depressive symptoms specific to a given developmental stage. The tool consists of the following subscales: emotional problems; negative mood; low self-esteem; problems in functioning; lack of effectiveness and interpersonal problems. Raw scores are converted into two standardized formats: a ten scale (ranging from 21 to 79) and a sten scale (ranging from 1 to 10). Both take into account the respondent’s age and gender, and in each case higher scores indicate greater severity of depressive symptoms. According to the ten scale, the following categories were distinguished: 21–39 (low), 40–59 (average), 60–64 (increased), 65–69 (high), and 70–79 (very high). In turn, the sten scale categories applied in this study were: 1–3 (low severity), 4–6 (moderate severity), and 7–10 (high severity) (Kovacs, 2015; Wrocławska-Warchala and Wujcik, 2017).
3.3 State–trait anxiety inventory (STAI)
The inventory contains 40 statements, half of which assess anxiety as a relatively stable personality trait (X2), and the remaining anxiety as a situationally conditioned state (X1). The instrument yields raw scores ranging from 20 to 80 for each subscale. These raw scores can be converted to standardized sten scores based on normative data to facilitate interpretation of anxiety levels (low, moderate, high). The sten scale ranges from 1 to 10. Sten 1–3 is defined as low; 4–7 as medium, and 8–10 as high. The higher the sten, the greater the severity of anxiety symptoms. The study used only a subscale assessing anxiety as a state (X1) The STAI (Spielberger, 1983) is a widely used self-report instrument designed to measure both state and trait anxiety in individuals aged 14 and older (Spielberger, 1983).
The author’s demographic data questionnaire included questions about gender, age, place of residence, type of school, preferred type of education, and psychiatric treatment. This questionnaire also includes definitions of the “significant other” which appears in the questionnaire MSPSS The term “significant other “was defined for participants as someone they would turn to first in times of distress and from whom they would expect support.
4 Statistical analysis
Standard statistical procedures were used in the analyses. The Kolmogorov–Smirnov test was used to assess the normality of distributions. Due to the fact that the distributions of variables deviated from the normal distribution, it was decided to use non-parametric methods in subsequent analyses. The Mann–Whitney U test was used to assess the significance of differences between the group of girls and boys in terms of variables such as perceived social support, and symptoms of depression and anxiety. The relationships between perceived social support and symptoms of depression and anxiety were analyzed separately for girls and boys. The Spearman rank correlation was used to examine the associations between the MSPSS total score and the CDI-2 and between the MSPSS total score and the STAI-X1, separately for girls and boys. The significance level of α < 0.05 was assumed as statistically significant. Calculations were performed in Statistical version 13.3.
5 Results
5.1 Description of the study group
In addition to socio-demographic data, the survey included a question about being in a relationship and the most important type of support. The following replies were received:
A. Both the majority of girls (68.30% (530)) and boys (76.03% (517)) were not in a permanent intimate relationship (Table 1).
B. Among girls, the largest number of respondents indicated support other than those mentioned (27.8%), support from friends (26.5%) and support from a partner (19.4%) as the most important in coping with stress. Among boys, the largest number of respondents indicated support other than those mentioned (37.4%), followed by the support of friends (26.2%) as the most important in coping with stress (Table 1). The respondents were also asked two separate questions about the stress they felt due to the COVID-19 pandemic and the stress related to the outbreak of the war in Ukraine. Respondents could answer on a scale of 0–10 points; where 0 – no sense of stress, and 10 – the greatest stress imaginable. In the boys’ population, the average COVID-19 stress score was 2.56 ± 2.58 SD points; while the average stress level result related to the outbreak of the war in Ukraine was assessed by the respondents as: 3.50 ± 2.89 SD points. The surveyed girls similarly scored: 4.31 ± 2.82 SD points and 5.46 ± 2.85 SD points. The cross-gender comparison using the Mann Whitney U test showed a statistically significant difference in stress related to the COVID-19 pandemic (Z = −12.227; p < 0.001), as well as stress related to the outbreak of the war in Ukraine (Z = −12.331; p < 0.001). In the case of stress related to the COVID-19 pandemic, girls (median = 4,000; Q1-Q3 = 2–6) showed higher stress levels compared to boys (median = 2,000; Q1-Q3 = 0–4). A similar trend was observed when comparing stress between girls (median = 6,000; Q1-Q3 = 3–8) and boys (median = 3,000; Q1-Q3 = 1–6) related to the outbreak of war in Ukraine. Before the pandemic, 8.97% (61) of surveyed boys and 11.59% (90) of girls were undergoing psychiatric treatment. During the COVID-19 pandemic, 7.21% (49) of surveyed boys and 14.18% (110) girls started psychiatric treatment (Table 1). A chi-square test was performed to assess the relationship between gender and the use of psychiatric treatment. In the case of initiation of psychiatric treatment before the indicated crisis event, no significant association with gender was noted (Chi-square = 2,691; p = 0.101). When psychiatric treatment was initiated after the onset of the COVID-19 pandemic, this tendency was observed to be significantly more common in girls (Chi-square = 18,096; p = 0.000).
5.2 Multidimensional scale of perceived social support (MSPSS)
Analyzing the results obtained in the MSPSS study group, the average overall score was 4.75 ± 1.51 points, in the family support subscale the average score was 4.38 ± 1.84 points, support from friends 4.90 ± 1.84 points, support from a significant other 4.98 ± 1.53 points. The differences between the group of girls and the group of boys were statistically significant in all the studied variables representing social support (Table 2).
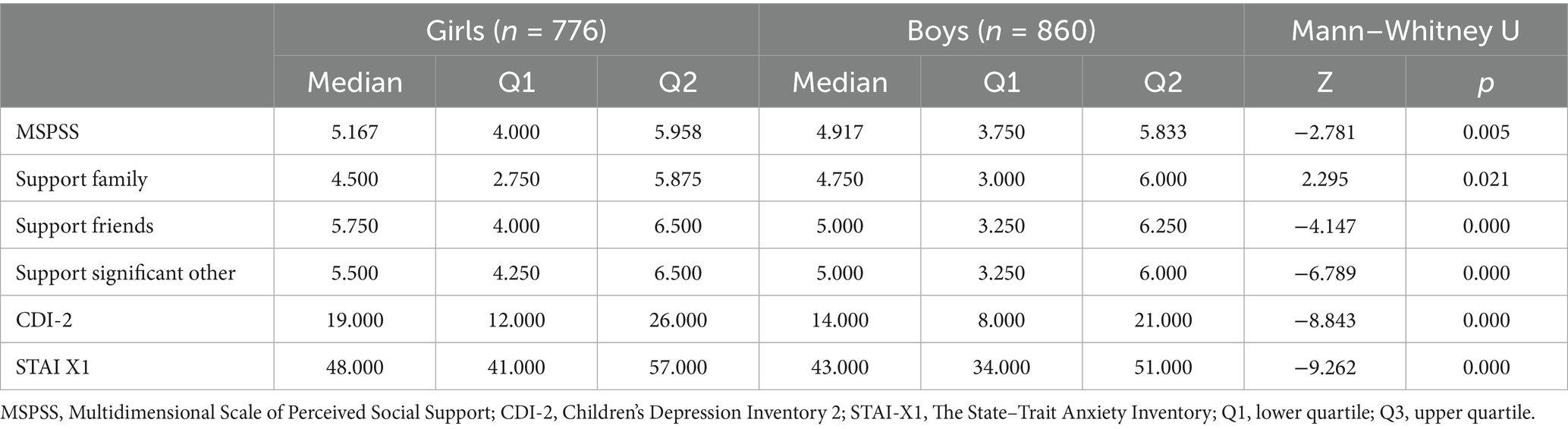
Table 2. Differences between girls and boys in examined parameters.
5.3 CDI-2 depressive symptoms rating scale
In the assessment of depression, the respondents scored an average of 17.36 ± 9.37 points. After dividing into groups according to gender, 19.44 ± 9.44 points were obtained, respectively for girls (61, increased depressive symptoms) and 14.99 ± 8.70 points for boys (56, average intensity of depressive symptoms). The difference between girls and boys groups in terms of the severity of depressive symptoms was statistically significant (Table 2).
5.4 Anxiety inventory – STAI-X1
In the anxiety assessment, the respondents scored an average of 46.39 ± 11.60 points. After dividing into groups according to gender, 49.08 ± 11.01 points were obtained, respectively for girls (sten 8 – high severity) and 43.33 ± 11.51 points for boys (sten 7, medium intensity). The difference between girls and boys groups in terms of the severity of anxiety as a state was statistically significant (Table 2).
5.5 Analysis of relationships between MSPSS, CDI-2, STAI-1
The Spearman rank correlations were used to examine the associations between the MSPSS total score and the CDI-2 and between the MSPSS total score and the STAI-X1, separately for girls and boys. Statistically significant negative correlations were observed between depressive symptoms (CDI-2) and anxiety symptoms (STAI-X1) and perceived social support (MSPSS), including its total score and all subscales, in both groups (see Tables 3, 4).
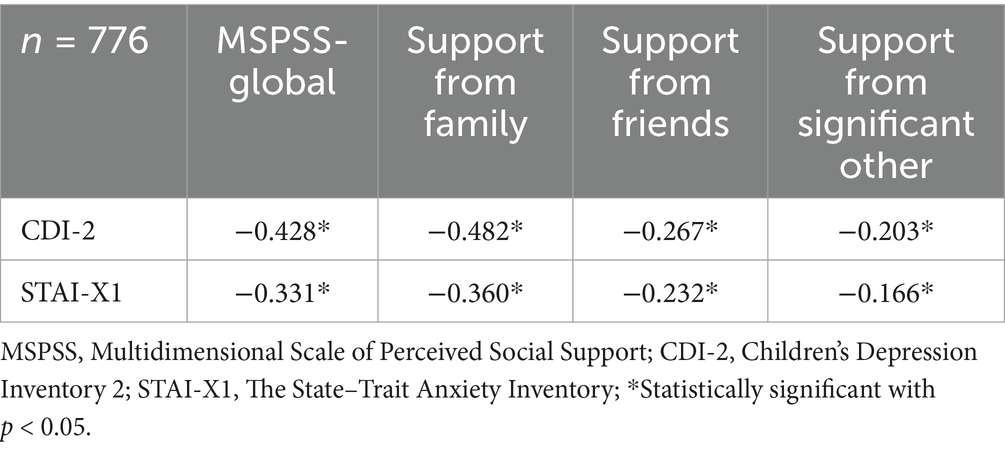
Table 3. Correlations between examined parameters – girls.
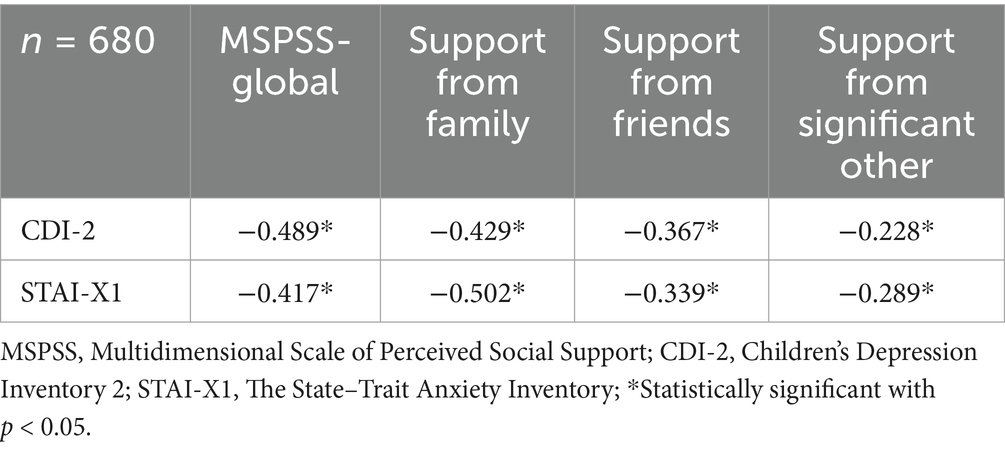
Table 4. Correlations between examined parameters – boys.
6 Discussion
6.1 Mental health during crises (COVID-19 and the war in Ukraine)
The changes that occurred in the surrounding reality during the COVID-19 pandemic were a source of significant stress for many people. Just when the world seemed to be returning to normal Russia’s aggression against Ukraine once again shocked the international community. During these two exceptional periods, a two-fold increase in the number of teenagers struggling with mental health problems was observed (Goto et al., 2024; Danese et al., 2025; Dąbkowska, 2020; Yoon and Kim, 2018). In our study, both girls and boys achieved high scores on the anxiety scale and average scores on the depression scale. Girls, however, scored higher on both scales than boys. Yoon et al. observed that affective symptoms tended to be more severe in women, which is consistent with epidemiological data indicating that women are more frequently diagnosed with affective and anxiety disorders (Chu et al., 2010). Men, on the other hand, are more frequently diagnosed with substance use disorders and schizoid personality disorder. Moreover, in our analysis, a higher percentage of girls than boys reported chronic illnesses and psychiatric treatment both before and during the pandemic (results were not statistically significant). Available research indicates that pre-existing psychiatric conditions and interventions may increase vulnerability to psychological stress during crises (Johansen et al., 2021; Pettit et al., 2011). However, it seems that it is not the fact of psychiatric treatment itself, but the previous mental health problems that led to it, that may make this group of teenagers more sensitive and prone to stress. In our study, adolescents of both sexes perceived the outbreak of war in Ukraine as a more stressful event than the ongoing COVID-19 pandemic. It is likely that the war represented a new and acute stressor, potentially triggering stronger emotional reactions than the prolonged, gradually easing restrictions related to the pandemic. The overall perceived stress level for both events was assessed by adolescents as moderate to low, with mean scores below the midpoint of the scale. It appears that the moderate level of stress associated with COVID-19 may have been caused by a significant easing of restrictions related to the pandemic, which has been ongoing for over 2 years. However, the outbreak of war may have seemed like an “abstract phenomenon” to young people, and its effects related to the influx of refugees from Ukraine during this period (February 2022–May 2022) were not yet felt.
6.2 Gender differences in anxiety, depression, and sources of support
The study showed that social support during crisis situations is more important for girls than for boys. Gender also differentiated the sources of support. The obtained results (statistically significant) showed that girls more often indicated that support from friends and significant other was important to them. “The significant other” was defined by participants as someone they would turn to first in times of distress and from whom they would expect support. Boys more often indicated family support as the most important. In the sociodemographic questionnaire, girls, on the other hand, indicated that mother’s support was particularly important to them, while boys indicated “other forms of support.” However, these results were not statistically analyzed. This may reflect gender-specific help-seeking behaviors and differences in emotional communication. The literature suggests that emotional support from peers and family has a protective effect on depressive symptoms in teenage girls (Dahlem et al., 1991; van der Wal et al., 2021). Boys, on the other hand, more often seek support in various types of activities or choose more instrumental support (Rueger et al., 2016).
6.3 Contextual factors: place of residence and protective role of social support
In our study, a significant percentage of participants lived in rural areas (approximately 45% of girls and 46% of boys). Rural youth may experience advantages associated with their place of residence, such as a close-knit community. Limited access to specialized mental health services may be a disadvantage. In such circumstances, informal support networks may become a particularly important coping resource when professional help is less accessible or less acceptable. The multifaceted relationship between place of residence and mental health was also discussed by Scardera et al. (2020). In our study, we also observed a relationship between perceived social support and scores on the CDI-2 and STAI-1 scales. The negative correlation between the aforementioned data may indicate a protective role of social support against anxiety and depressive symptoms. Similar results were obtained in the meta-analysis conducted by Jones et al. (2017) and the study by Cobham et al. (2020).
7 Conclusion
Social support during crisis situations was more important for girls than for boys in the group of Polish teenagers. Gender may have determined the sources of support.
Perceived social support may play an important role in coping with symptoms of anxiety and depression in crisis situations.
7.1 Study limitations
The presented study, like any study in which results were collected using the Internet, has certain limitations.
1. First, collecting data via an online form makes it impossible to monitor how the questionnaires are completed.
2. Using self-report questionnaires in the study is associated with the possibility of misunderstanding the instructions, and responses may be distorted by difficulties in the respondent’s self-assessment or unconscious manipulation.
3. Furthermore, the STAI questionnaire used in the study has not been validated in pediatric populations; the obtained results should be interpreted with caution.
4. The statistical methods used in the study only allow for the determination of the relationship between the parameters studied, not a cause-and-effect relationship.
5. Another limitation of this study is that the research material was collected exclusively in secondary schools, without creating control groups from other educational institutions at the same age.
6. Furthermore, the observed gender differences should be interpreted with caution, as they may be influenced by other unmeasured factors.
7. Another limitation of this study is the lack of data on the socioeconomic status of participants, which may influence mental health indicators.
8. Furthermore, the study did not differentiate between factors (the COVID-19 pandemic and the wars in Ukraine) that could have influenced participants’ emotional functioning.
9. The study is not longitudinal, so it is difficult to conclude whether the crisis situation had an impact on the mental state.
10. The term “significant other “was defined for participants as someone they would turn to first in times of distress and from whom they would expect support. The option “other form of support” did not allow for a precise assessment of the source of support.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by The Bioethics Committee of the Medical University of Silesia (PCN/CBN/0052/KB1/48/22). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
KB-B: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. PG: Conceptualization, Investigation, Writing – original draft. DT: Conceptualization, Investigation, Writing – original draft. PD: Formal analysis, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to thank all school pupils who anonymously participated in the study and all teachers who were engaged in helping them.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Buszman, K. , and Przybyła-Basista, H. (2017). Polska Adaptacja Wielowymiarowej Skali Spostrzeganego Wsparcia Społecznego. Polskie Forum Psychologiczne 22, 581–599. doi: 10.14656/PFP20170404
Chu, P. S. , Saucier, D. A. , and Hafner, E. (2010). Meta-analysis of the relationships between social support and well-being in children and adolescents. J. Soc. Clin. Psychol. 29, 624–645. doi: 10.1521/jscp.2010.29.6.624
Cipora, E. , and Mielnik, A. (2022). Wybrane aspekty medyczne i społeczne pandemii Covid-19. J. Educ. Health Sport 12, 11–20. doi: 10.12775/JEHS.2022.12.01.001
Cobham, V. E. , Hickling, A. , Kimball, H. , Thomas, H. J. , Scott, J. G. , and Middeldorp, C. M. (2020). Systematic review: anxiety in children and adolescents with chronic medical conditions. J. Am. Acad. Child Adolesc. Psychiatry 59, 595–618. doi: 10.1016/j.jaac.2019.10.010.31676391
Cohen, S. (2004). Social relationships and provision – health. Am. Psychol. 59, 676–684. doi: 10.1037/0003-066X.59.8.676
Cohen, S. , and Hoberman, H. M. (1983). Positive events and social supports as buffers of life change stress. J. Appl. Soc. Psychol. 13, 99–125.
Dąbkowska, M. (2020). Psychospołeczne konsekwencje pandemii koronawirusa (COVID-19) u dzieci i młodzieży–przegląd wybranych opracowań. Niepełnosprawność 39, 150–160.
Dahlem, N. W. , Zimet, G. D. , and Walker, R. R. (1991). The multidimensional scale of perceived social support: a confirmation study. J. Clin. Psychol. 47, 756–761. doi: 10.1002/1097-4679(199111)47:6<756::aid-jclp2270470605>3.0.co;2-l
Danese, A. , Martsenkovskyi, D. , Remberk, B. , Khalil, M. Y. , Diggins, E. , Keiller, E., et al. (2025). Scoping review: digital mental health interventions for children and adolescents affected by war. J. Am. Acad. Child Adolesc. Psychiatry 64, 226–248. doi: 10.1016/j.jaac.2024.02.017
Goto, R. , Pinchuk, I. , Kolodezhny, O. , Pimenova, N. , Kano, Y. , and Skokauskas, N. (2024). Mental health of adolescents exposed to the war in Ukraine. JAMA Pediatr. 178, 480–488. doi: 10.1001/jamapediatrics.2024.0295
Jaskulska, S. , Jankowiak, B. , Marciniak, M. , and Klichowski, M. (2021). Edukacja zdalna w czasie pandemii COVID-19 w doświadczeniach uczniów i uczennic: ocena relacji szkolnych i jej uwarunkowania. Wychowanie w Rodzinie 24, 133–146.
Johansen, R. , Espetvedt, M. N. , Lyshol, H. , Clench-Aas, J. , and Myklestad, I. (2021). Mental distress among young adults – gender differences in the role of social support. BMC Public Health 21:2152. doi: 10.1186/s12889-021-12109-5
Jones, L. C. , Mrug, S. , Elliott, M. N. , Toomey, S. L. , Tortolero, S. , and Schuster, M. A. (2017). Chronic physical health conditions and emotional problems from early adolescence through midadolescence. Acad. Pediatr. 17, 649–655. doi: 10.1016/j.acap.2017.02.002
Kobylarczyk-Kaczmarek, M. , and Ogińska-Bulik, N. Trauma u młodzieży. Konsekwencje i uwarunkowania. Warszawa: Difin. (2023). 220.
Kovacs, M. (2015). “Children's depression inventory (CDI and CDI 2)” in The Encyclopedia of clinical psychology. eds. R. L. Cautin and S. O. Lilienfeld . (Hoboken, NJ: Wiley-Blackwell), 1–6.
Lin, N. , Woelfel, M. W. , and Light, S. C. (1985). Buffering effect of social support subsequent to an important life event. J. Health Soc. Behav. 26, 247–263
Machniak, A . Doświadczanie objawów depresji wśród nastolatków w czasie pandemii COVID-19, [praca magisterska]. Kielce: Uniwersytet Jana Kochanowskiego. (2022)
Maraszkiewicz, M. (2022). Wsparcie ucznia cierpiącego z powodu chorób psychicznych w środowisku szkolnym. Piękna idea na papierze czy realna rzeczywistośc? Niepełn. Rehab. 87, 94–102.
Pettit, J. W. , Roberts, R. E. , Lewinsohn, P. M. , Seeley, J. R. , and Yaroslavsky, I. (2011). Developmental relations between perceived social support and depressive symptoms through emerging adulthood: blood is thicker than water. J. Fam. Psychol. 25, 127–136. doi: 10.1037/a0022320.21355652
Poleszak, W. , and Katab, G. (2022). Czynniki chroniące i czynniki ryzyka w radzeniu sobie z pandemią Covid-19 w środowisku młodzieży szkolnej. Kwart. Nauk. Fides Et Ratio 4:52. doi: 10.34766/fetr.v4i52.1123
Pyżalski, J. (2021). Zdrowie psychiczne i dobrostan młodych ludzi w czasie pandemii COVID-19– przegląd najistotniejszych problemów. Dziecko Krzywdzone Teoria Badan. Prakt. 20, 92–115.
Reblin, M. A. , and Uchino, B. N. (2008). Social and emotional support and links to physical health. Curr. Opin. Psychiatry 21, 211–215. doi: 10.1097/YCO.0b013e3282f3ad89
Reicher, H . Jaka jest funkcja zasobów psychospołecznych? Wpływ wsparcia społecznego, strategii radzenia sobie i życiowego stresu na psychologiczne funkcjonowanie młodzieży. Rocznik Naukowo-Dydaktyczny. Z. 180, Prace Psychologiczne. 6:189–202. Kraków: Wyższa Szkoła Pedagogiczna w Krakowie. (1997).
Rueger, S. Y. , Malecki, C. K. , Pyun, Y. , Aycock, C. , and Coyle, S. (2016). A meta-analytic review of the association between perceived social support and depression in childhood and adolescence. Psychol. Bull. 142, 1017–1067. doi: 10.1037/bul0000058.27504934
Scardera, S. , Perret, L. C. , Ouellet-Morin, I. , Gariépy, G. , Juster, R. P. , Boivin, M., et al. (2020). Association of Social Support during Adolescence with Depression, anxiety, and suicidal ideation in young adults. JAMA Netw. Open 3:e2027491. doi: 10.1001/jamanetworkopen.2020.27491.33275154
Sikora, R. (2012). Wsparcie społeczne i strategie radzenia sobie ze stresem a depresyjność młodzieży social support, strategies of coping with stress and depression in adolescents. Psychologia 17, 41–54.
Sikorska, I. , Lipp, N. , Wróbel, P. , and Wyra, M. (2021). Adolescent mental health and activities in the period of social isolation caused by the COVID-19 pandemic. Postepy Psychiatr. Neurol. 30, 79–95. doi: 10.5114/ppn.2021.108472
Spielberger, C. D. State-Trait Anxiety Inventory for Adults (STAI-AD) [database record]. Palo Alto, CA: Consulting Psychologists Press. (1983).
Stanton-Salazar, R. , and Urso-Spina, S. (2005). Adolescent peer networks as a context for social and emotional support. Youth Soc. 36, 379–417. doi: 10.1177/0044118X04267814
Szredzińska, R. , and Włodarczyk, J. (2021). Doświadczenia krzywdzenia oraz dobrostan psychiczny polskich nastolatków w pierwszym okresie pandemii. Dziecko Krzywdzone Teor. Badania Prakt. 20, 38–62.
Uchino, B. N. , Cacioppo, J. T. , and Kiecolt-Glaser, J. K. (1996). The relationship between social support and physiological processes: a review with emphasis on underlying mechanisms and implications for health. Psychol. Bull. 119, 488–531. doi: 10.1037/0033-2909.119.3.488
van der Wal, J. M. , van Borkulo, C. D. , Deserno, M. K. , Breedvelt, J. J. F. , Lees, M. , Lokman, J. C., et al. (2021). Advancing urban mental health research: from complexity science to actionable targets for intervention. Lancet Psychiatry 8, 991–1000. doi: 10.1016/S2215-0366(21)00047-X
Wrocławska-Warchala, E. , and Wujcik, R. (2017). Zestaw Kwestionariuszy do Diagnozy Depresji u Dzieci i Młodzieży. Podręcznik. Warszawa: Wydawnictwo PTP.
Yarchesky, A. , Mahon, N. , and Yarchesky, T. (2001). Social support and well-being in early adolescence. Clin. Nurs. Res. 10, 163–181. doi: 10.1177/C10N2R6
Keywords: social support, adolescence, psychiatry, war, COVID-19
Citation: Badura-Brzoza K, Główczyński P, Tatar D and Dębski P (2025) Youth in times of polycrises: the role of social support in connection with the depression and anxiety symptoms among young people in polish secondary schools during the COVID-19 threat and the outbreak of war in Ukraine. Front. Psychol. 16:1591218. doi: 10.3389/fpsyg.2025.1591218
Edited by:
Roger Gibson, University of the West Indies, JamaicaReviewed by:
Carolyn Szostak, University of British Columbia, CanadaKelly Romero, University of British Columbia, Canada
Copyright © 2025 Badura-Brzoza, Główczyński, Tatar and Dębski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Patryk Główczyński, cGF0cnlrLmdsb3djenluc2tpQHdwLnBs