 Lukáš Psohlavec
Lukáš Psohlavec Mike Rogerson
Mike Rogerson Tomáš Brtník1
Tomáš Brtník1 Jiří Baláš
Jiří Baláš- 1Faculty of Physical Education and Sport, Charles University, Prague, Czechia
- 2School of Sport, Rehabilitation and Exercise Sciences, University of Essex, Colchester, United Kingdom
Despite the widespread use of height exposure in adventure-based programs to foster resilience, effectiveness has largely been evaluated through self-reported measures, with limited objective psychophysiological assessments. This study aimed to identify which physiological stress markers best determine the acute stress response to height. A secondary aim of the study was to assess the concurrent validity of the Competitive State Anxiety Inventory-2 Revised (CSAI-2R) questionnaire with ventilatory and heart rate variability (HRV) markers. A total of 55 healthy university students participated in a controlled experiment involving three walks on a log positioned at varying heights (0.3 m and 10.5 m). Psychometric measures were recorded using the Competitive State Anxiety Inventory-2 Revised, while physiological responses were monitored through HRV and respiratory markers. High-obstacle conditions significantly increased somatic (↑6.1 ± 5.7; p < 0.01) and cognitive anxiety (↑2.9 ± 5.9; p < 0.01) while reducing self-confidence (↓3.0 ± 5.6; p < 0.01). Based on the effect size (ηp2), the largest differences between low- and high-height conditions for physiological markers were observed in heart rate (HR) (ηp2 = 0.910), ventilation (ηp2 = 0.906), oxygen uptake (ηp2 = 0.891; p < 0.001), and tidal volume (VT) (ηp2 = 0.872). Smaller differences were found for HRV markers, including the parasympathetic nervous system (PNS) index (ηp2 = 0.860) and the sympathetic nervous system (SNS) index (ηp2 = 0.798). Notably, weak correlations were observed between physiological markers and self-reported anxiety measures (R = −0.454 to 0.323), raising questions about the concurrent validity of psychometric tools. The findings suggest that while height exposure induces a pronounced stress response, the combination of HR and respiratory measures with psychological tools provides a more comprehensive understanding of stress coping during height exposure.
Introduction
Based on the doxa assumption that height is stressful for many individuals, exposure to height via adventure activities—such as high ropes courses, climbing, and abseiling—is often used in outdoor adventure-based programs as a challenging and potentially stressful experience for educational purposes. Acute stress-related physiological and psychological responses are often measured, as they can provide valuable insights into stress coping mechanisms and resilience (Bailey et al., 2017; Baláš et al., 2017; Bunting et al., 2000; Bunting and Gibbons, 2001; Davidson et al., 2016; Draper et al., 2010; Ewert et al., 2016; Gajdošík et al., 2020).
Physiological markers of stress
More broadly, acute physiological responses to adventure activities have been assessed using salivary cortisol (Draper et al., 2010; Ewert et al., 2016; Magiera et al., 2018), urine catecholamines (Bunting et al., 2000), EEG activity (Bailey et al., 2017), venous blood catecholamines and cortisol (Baláš et al., 2017; Bunting and Gibbons, 2001), heart rate (HR) (Draper et al., 2010; Giles et al., 2020; Magiera et al., 2018; Watts et al., 1999), and respiratory markers (Draper et al., 2010; Gajdošík et al., 2020; Giles et al., 2020; Watts et al., 1999).
While hormones from both the hypothalamic–pituitary–adrenal (HPA) axis and the sympathetic-adrenal-medullary axis reflect the stress response, the use of cortisol can be challenging due to individual variation in reactivity (i.e., how long it takes for an associated peak in cortisol to be reached after a stressor), especially when data are collected at a set time following the event of interest, individual variation in diurnal rhythms, and the expense of processing samples. The use of other catecholamines can be problematic in outdoor settings due to rapid degradation after stress cessation (Ewert, 2015; Zouhal et al., 2008).
Therefore, utilizing heart rate, respiratory markers, and heart rate variability (HRV) is often a more financially and logistically viable way for assessing the stress response in outdoor settings such as adventure activities. For instance, HRV has been shown to reflect vagal activity in these settings (Gladwell et al., 2016), and heart rate is a frequently used measure in sports and exercise sciences and has also been shown to respond to various stressors (Taelman et al., 2009).
Therefore, the current study sought to address the literature gap regarding physiological markers of stress measured during an adventure activity at elevated heights.
Psychological markers of stress and their validity
Either to focus on the mental aspect or to triangulate and provide a more holistic understanding of the potentially stressful activity, psychological self-report is often employed. Anxiety responses, which are of particular interest in adventure activity-based programs, can be assessed using a range of questionnaires, such as the Competitive State Anxiety Inventory-2 (CSAI-2) (Baláš et al., 2017; Draper et al., 2010; Giles et al., 2020), State–Trait Anxiety Inventory (STAI), Anxiety Thermometer (Pijpers et al., 2003, 2005), and Spielberg State Anxiety Inventory (SSAI) (Bunting and Gibbons, 2001). Anxiety is an emotion characterized by feelings of tension, worried thoughts, and physical changes in the body (Foa et al., 2005). It is made up of multiple components, although the exact number and nature of these components remain a topic of debate in the literature (Brodbeck et al., 2011; Clark and Watson, 1991). The CSAI-2 questionnaire models anxiety as comprising three components—cognitive, somatic, and self-confidence. Although stress and anxiety are interrelated, it makes sense that for adventure activities at height, anxiety—as a future-oriented state—will likely be most pertinent before performing the activity, whereas stress will be more pertinent during the performance.
Although combinations of physiological markers and self-reported anxiety are frequently used in research and practice, very little is currently known about the concordant validity between psychometric tools such as the CSAI and some physiological markers of stress (Goyal et al., 2016), particularly when they are being used in adventure domains. In activity-based adventure programs, participants often report or are observed to experience high anxiety immediately before the activity at height. It would be useful for practitioners to understand the extent to which pre-activity anxiety translates into stress during the activity itself. Therefore, the secondary aim of this study was to assess the concordant validity of the Competitive State Anxiety Inventory-2 Revised (CSAI-2R) questionnaire with respiratory and cardio markers of stress in order to understand the extent to which stress and anxiety are separate ‘constructs’ and whether self-reporting can be used as a proxy measure for physiological markers.
Materials and methods
Participants
A total of 55 university students (weight 72.2 ± 11.2 kg, height 177.1 ± 8.1 cm, age 20.3 ± 2.1 years) participated voluntarily in this study. They were healthy and asked to refrain from high-intensity exercise (24 h), caffeine (12 h), and heavy meals (2 h) prior to the experiment. All participants signed an informed consent at the beginning of the study. The local university’s ethics committee granted approval for the study (EK238/2020). All participants participated voluntarily.
Study design
All participants completed three 4-min walks on a narrow log at two different heights. The first walk took place on a log 0.3 m above the ground at a self-selected speed and was used only for psychometric assessments. The second walk was conducted at 10.5 m above the ground, also at a self-selected speed. The third walk was performed again at 0.3 m above the ground, but this time at the same speed as the high-obstacle trial, ensuring a consistent walking speed for subsequent physiological comparisons.
Randomization of the conditions was not possible for the following reasons:
a. The first walk at the low-obstacle height served as a familiarization trial with the log, aiming to reduce stress caused by a lack of skills needed to overcome the obstacle.
b. Standardizing walking speed across conditions was essential for accurately assessing physiological responses, as walking speed is a key factor influencing physiological changes. Since it was not possible to control the walking speed during the high-obstacle trial due to participants’ heightened stress responses, the high-obstacle trial had to be completed first. This allowed the walking speed from the high-obstacle trial to be replicated during the second low-obstacle trial, ensuring consistency for physiological comparisons.
c. Administering the CSAI-2R questionnaire during the low-obstacle condition after the high-obstacle trial could have introduced bias, as the participants’ successful completion of the high-obstacle walk may have influenced their responses.
A portable metabolic system was worn on the chest, and anxiety metrics were recorded during all three conditions, as depicted in Figure 1. Participants completed the CSAI-2R immediately before the first and the second walk.
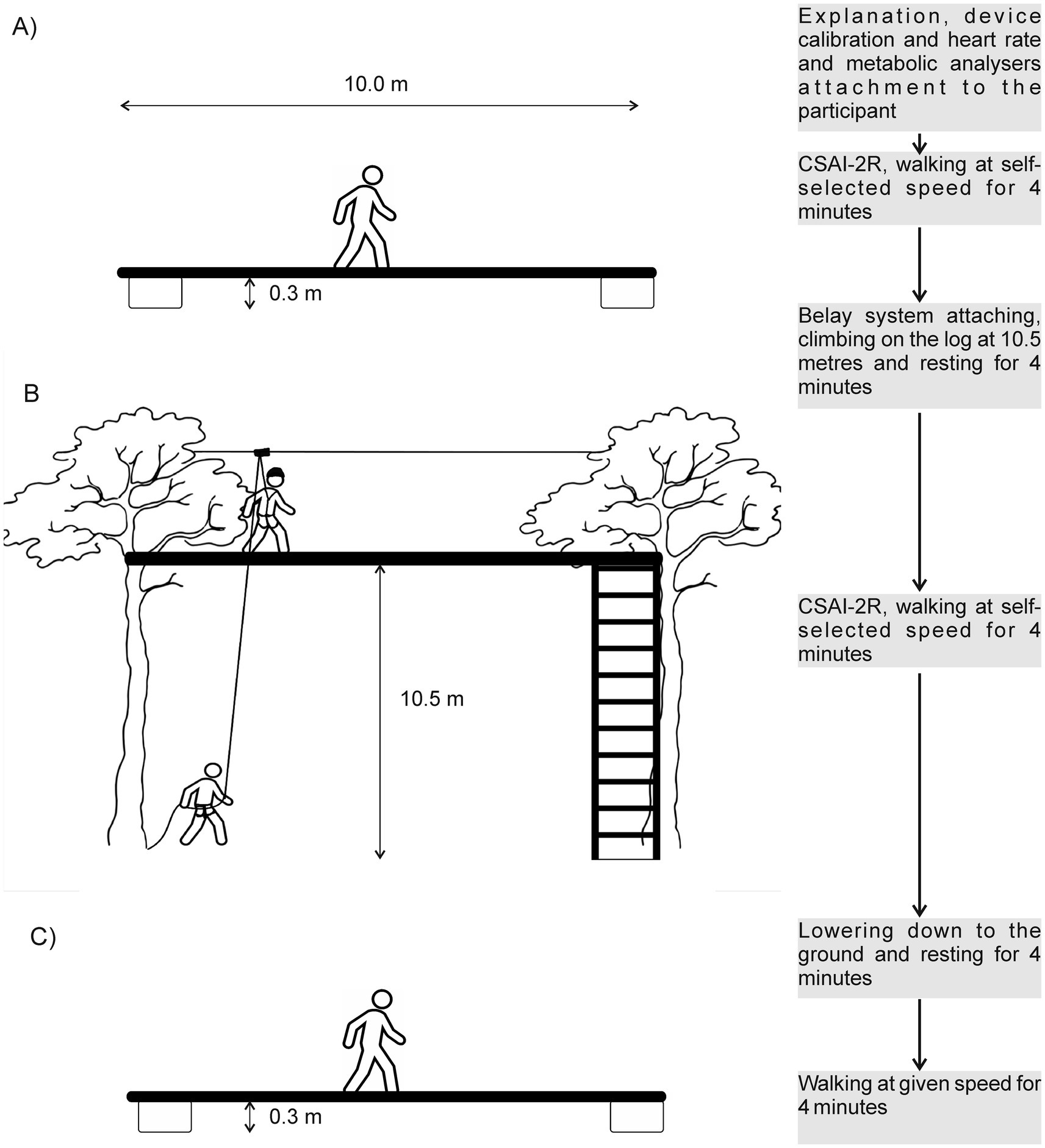
Figure 1. Design of the study. (A) Walking at a self-selected speed on a log 0.3 m above the ground. (B) Walking at a self-selected speed on a log 10.5 m above the ground. (C) Walking at a given speed on a log 0.3 m above the ground.
High- and low-obstacle courses
The same two rounded wooden logs (13 m long, 0.25 m in diameter) were placed at 0.3 m (low-obstacle) and 10.5 m (high-obstacle) above the ground, respectively. The middle 10-m section was marked at 1-m intervals using colored marks. The participants wore a full-body harness during both low- and high-obstacle conditions. However, only during the high-obstacle condition, the participants were belayed by an experienced instructor using a preinstalled rope. The rope was fixed on the participants’ backs so that they could not see it. The rope passed through a carabiner with a pulley, which was running freely on a metallic wire 4 m above the log. From the carabiner, the rope went back to the belayer at the ground level. To control the walking speed during the third walk, the bottom log was highlighted with colored marks every meter, and a researcher verbally guided the participants to accelerate or decelerate their walking pace. At the end of the log, a small balance support attached to a tree was provided to assist with turning.
Physiological responses
Physiological responses were assessed using an indirect calorimetry open system and HRV.
Gas analysis
A portable breath-by-breath metabolic system (MetaMax 3B, Cortex Biophysik, Germany) was worn by the participants using a chest harness (total weight 1.4 kg). Gas calibration was performed with a reference gas (15% O2 and 5% CO2), and volume calibration was performed using a 3-L syringe. Ambient air calibration was performed before each measurement. Breath-by-breath data were averaged over 20-s intervals for oxygen uptake (VO2), carbon dioxide production (VCO2), expiratory ventilation (VE), and breath frequency (BF), then exported to Excel for further analysis.
Heart rate variability
A chest belt (Polar Electro H10 OY, Finland) was used for monitoring heart rate (HR) and HRV. Data were measured continuously and stored using a Polar watch (Polar Grit X Pro, Kempele, Finland), then they were exported and analyzed using the Kubios HRV software (Biosignal Analysis and Medical Imaging Group, Kuopio, Finland). The analyzed HRV markers were selected according to previous recommendations for short-term HRV analysis (Castaldo et al., 2015; Kim et al., 2018; Pereira et al., 2017; Shaffer and Ginsberg, 2017) and were as follows.
Time-domain parameters
Mean heart rate (HR), average time between consecutive heartbeats (RR), root mean square of successive differences between RR intervals (RMSSD), number of successive RR interval pairs that differ by more than 50 ms (NN50), stress index (SI), and mean of the standard deviations of RR intervals in 5-min segments (SDNN).
Frequency-domain parameters
Absolute low-frequency power (0.04–0.15 Hz) measured using the fast Fourier transform (FFT) (LFpow_FFT (ms2)), high-frequency power (0.15–0.4 Hz) measured using the FFT (HFpow_FFT (ms2)), normalized low-frequency power expressed in normalized units (LFpow_FFT (n.u.)), high-frequency power expressed in normalized units (HFpow_FFT (n.u.)), and low-frequency power to high-frequency power ratio (LF/HF Ratio (FFT)).
Non-linear HRV parameters
Standard Deviation 1 (SD1): a measure of short-term HRV, specifically derived from the Poincaré plot, and detrended fluctuation analysis, Alpha 1: a non-linear HRV measure that assesses short-term correlations in the time series of heart rate data (DFA1).
Parasympathetic nervous system (PNS) index and the sympathetic nervous system (SNS) index
The PNS index was calculated using three parameters: RR, RMSSD, and SD1. The SNS index was calculated using the following three parameters: HR, SI, and the Poincaré Plot index SD2 expressed in normalized units.
Psychological responses
Self-confidence, somatic anxiety, and cognitive anxiety were assessed using the CSAI-2R questionnaire. This inventory was selected for its three subscales and its widespread use in outdoor settings, ensuring a comprehensive and contextually relevant anxiety assessment. The CSAI-2R is a 17-item inventory, with each item scored on a Likert scale ranging from 1 (“not at all”) to 4 (“very much so”). Scores for each participant were combined to produce a score for each of the three subscales: (1) somatic anxiety (e.g., my heart is racing), (2) cognitive anxiety (e.g., I am concerned about performing poorly), and (3) self-confidence (e.g., I am confident because I can mentally picture myself reaching my goal). Just before the test during the first and second walks, the 17 statements were read and recorded by an examiner, and the participants verbally answered the appropriate number (1: Not at all, 2: Somewhat, 3: Moderately so, and 4: Very much so) to indicate how they felt at the moment (Cox et al., 2003).
Statistical analysis
Descriptive statistics (mean ± standard deviation) were used to characterize physiological and psychological responses to low and high obstacles. Differences in the CSAI-2R scores between low and high obstacles were assessed between the first and second walks, while differences in HRV and respiratory markers were evaluated between the second and third walks, when walking speed was controlled. Repeated-measures ANOVA was conducted to assess statistical differences and effect sizes. Furthermore, Pearson correlation analysis was used to assess the relationship between physiological markers and the CSAI-2R results. Statistical significance was set at a p-value < 0.05. The correlations and squared association indices were interpreted as follows: strong effect: R ≥ 0.8; R2 ≥ 0.64, moderate effect: R ≥ 0.5; R2 ≥ 0.25, and low effect: R ≥ 0.2; R2 ≥ 0.04. All calculations were performed using Microsoft Excel and statistical software (IBM Corp., 2019, IBM SPSS Statistics for Windows, Version 28.0, Armonk, NY, USA).
Results
CSAI-2R
During the high-obstacle condition, the participants significantly (p < 0.01) decreased their self-confidence scores (↓3.0 ± 5.6) and increased both somatic anxiety (↑6.1 ± 5.7) and cognitive anxiety (↑2.9 ± 5.9) compared to the low-obstacle condition (Table 1).
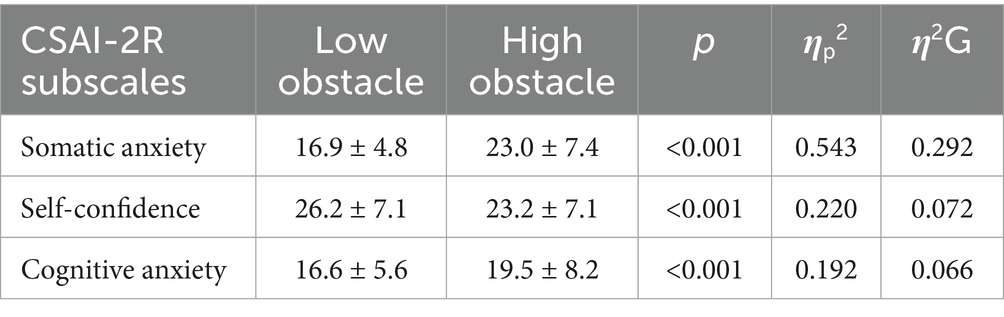
Table 1. Mean ± SD responses for somatic anxiety, cognitive anxiety, and self-confidence from the CSAI-2R during walking on low- and high-obstacle courses at self-selected speeds.
Physiological response
Heart rate variability markers
Walking on the high-obstacle course significantly (p < 0.05) increased HR (↑32.6 ± 10.3 beats.min−1), SNS (↑7.2 ± 3.6), and SI (↑22.8 ± 15.2) and decreased NN50 (↓9.3 ± 17.1 beats), PNS (↓1.3 ± 0.5), RR (↓145.7 ± 55.8 ms), SDNN (↓13.5 ± 9.0 ms), RMSSD (↓9.9 ± 9.1 ms), SD1 (↓7 ± 6.4 ms), and DFA1 (↓0.1 ± 0.4) compared to the low-obstacle course (Table 2). The frequency-domain metrics did not show any significant differences (p > 0.05) between the low- and high-obstacle conditions: LFpow (n.u.) (↑3.5 ± 15.4), HFpow (n.u.) (↓3.6 ± 15.4), and LF/HF ratio (FFT) (↑1.1 ± 5.4) (Table 2). Based on the effect size magnitude, a strong effect (ηp2 > 0.064) was found only for HR, RR, PNS index, SNS index, SI, and SDNN (Table 2).
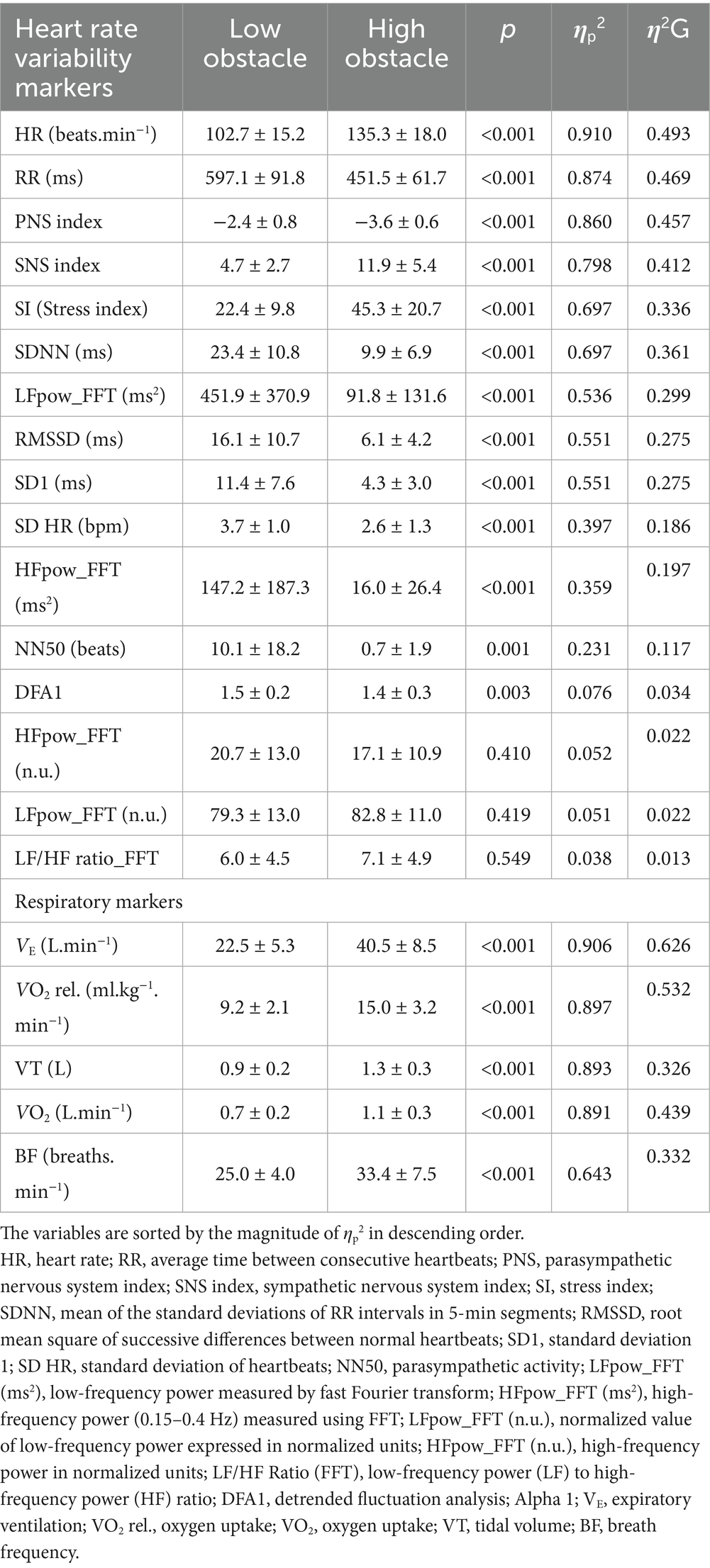
Table 2. Mean ± SD responses for heart rate variability and respiratory markers during walking on low- and high-obstacle courses at the same walking speed.
Respiratory markers
Walking on the high-obstacle course significantly (p < 0.001) increased VO2 (↑0.4 ± 0.1 L.min−1), VE (↑ 18.1 ± 5.9 L.min−1), tidal volume (VT) (↑0.3 ± 0.1 L), and BF (↑8.5 ± 6.4 breaths.min−1) compared to walking on the low-obstacle course (Table 2). A strong effect of height (ηp2 > 0.064) was found for all variables (Table 2).
Relationships between physiological and psychological responses
No meaningful correlations were found between HRV, respiratory markers, and psychometric stress markers. Only HR and the SNS index showed a moderate positive correlation with VE (R > 0.47) (Table 3).
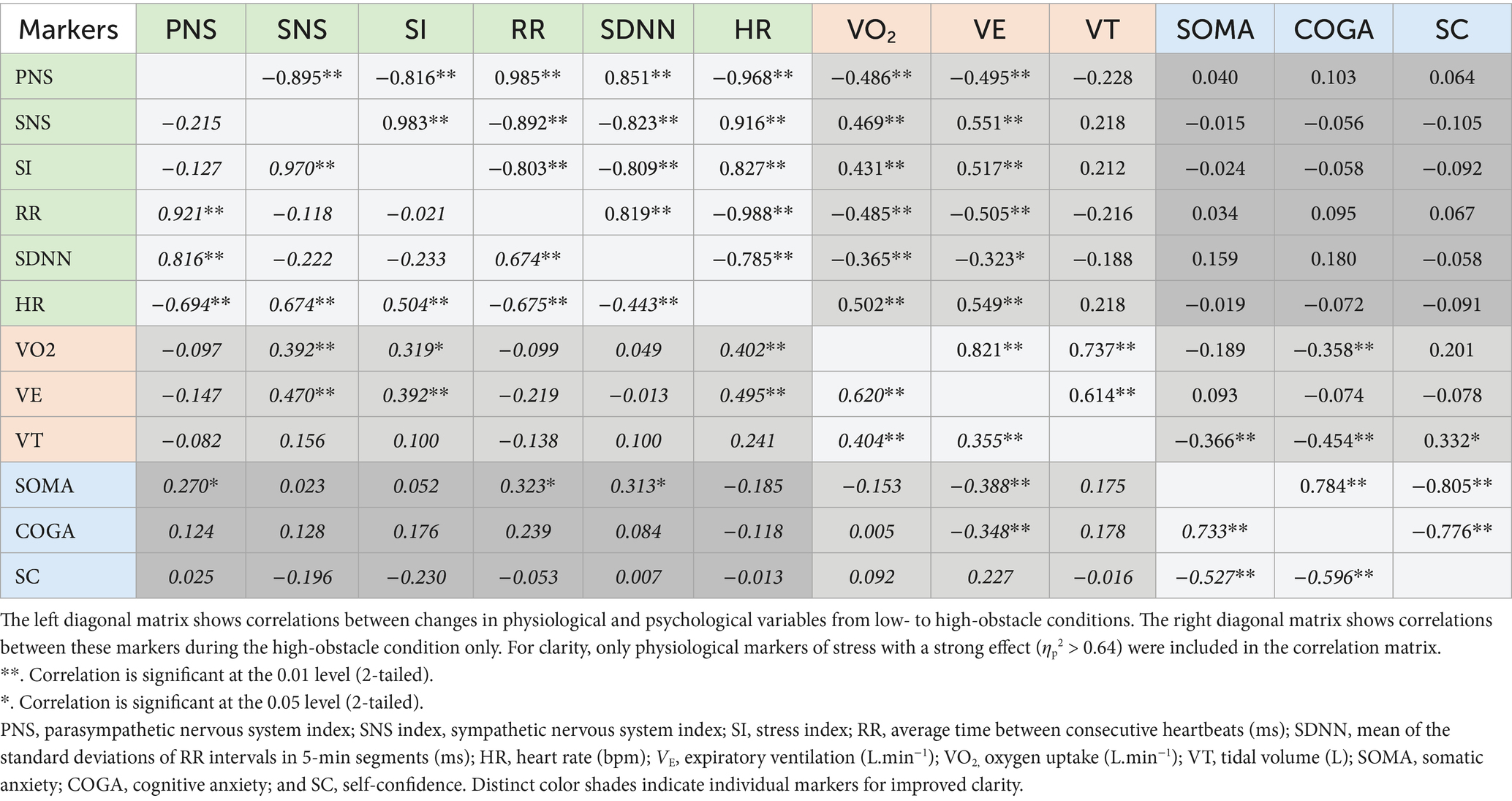
Table 3. Correlations between heart rate variability (green), respiratory markers (red), and anxiety markers (blue).
Discussion
The results indicate that walking on a high-obstacle course significantly increased somatic and cognitive anxiety, sympathetic nervous activity, and metabolic demands, while reducing parasympathetic activity and self-confidence compared to walking on a low-obstacle course. Based on the magnitude of the effect size, the study identified key respiratory and HRV markers that determine the acute stress response to height. Surprisingly, it was found that physiological markers of stress and psychological metrics of somatic anxiety responses did not correlate, raising questions about their use and interpretation, for example, in outdoor adventure-based programs.
CSAI-2R
The CSAI-2R is a commonly used and popular inventory for assessing anxiety in sport (Cox et al., 2003; Lundqvist and Hassmén, 2005; Martinent et al., 2010). In the current study, scores from all three dimensions of the questionnaire differed significantly between the low- and high-obstacle conditions, affirming that the CSAI-2R effectively reflects acute stress induced by height. Height induced nearly a threefold greater effect on somatic anxiety compared to cognitive anxiety or loss of self-confidence. However, somatic anxiety demonstrated only a low correlation with respiratory and HRV markers (R = 0.02–0.39), raising questions about the concurrent validity of this CSAI-2R dimension in assessing physiological changes related to the stress response. Similarly, Souza et al. (2019) did not find any meaningful correlation (R = 0.0–0.21) between somatic anxiety from the CSAI-2 and salivary cortisol or LF/HF ratio in the pre-competition state of sub-elite athletes. To the best of our knowledge, the psychometric properties of the CSAI-2R have primarily focused on reliability and factorial validity (Cox et al., 2003; Fernandes et al., 2013; Martinent et al., 2010), while the concurrent validity of the inventory dimensions, notably somatic anxiety, with physiological stress markers has not been established. In the current study, we observed the strongest correlation between VT and cognitive anxiety (R = −0.45) and between VE and somatic anxiety (R = −0.39). However, these relationships were not consistent across both correlation matrices, and their significance is questionable.
The low correlations between somatic anxiety and physiological markers of acute stress responses suggest that self-reports using the CSAI-R do not reliably reflect objective physiological changes in the body. This finding supports the notion of a dissociation between cognitive-affective and autonomic elements, thereby contributing to debates about the extent to which subjective and physiological stress responses operate via partially independent pathways depending somewhat on individual differences, such as interoceptive accuracy (Thayer and Lane, 2000; Thayer and Lane, 2009; Critchley et al., 2004; LeDoux, 1996). Therefore, integrating psychometric tools with multi-dimensional physiological monitoring may provide a more accurate assessment of acute stress responses.
HR and HRV
HR increased significantly during the high-obstacle task (103 ± 15 beats.min−1 for the low-obstacle task and 135 ± 18 beats.min−1 for the high-obstacle task, respectively). This increase was accompanied by a marked reduction in RR intervals (597.1 ± 91.8 ms to 451.5 ± 61.7 ms), reflecting heightened cardiac workload and a shift toward sympathetic dominance during the more stressful task, while intensity was held constant. These two HR markers showed the greatest differences between low- and high-obstacle conditions based on the ηp2 magnitude.
Time-domain HRV measures showed significant reductions, with SDNN decreasing from 23.4 ± 10.8 ms to 9.9 ± 6.9 ms and RMSSD dropping from 16.1 ± 10.7 ms to 6.1 ± 4.2 ms, indicating diminished parasympathetic activity and reduced autonomic flexibility.
Frequency-domain HRV measures showed a slight decrease in parasympathetic activity and a minor increase in sympathetic modulation during the high-obstacle task. The LF/HF ratio also increased slightly, indicating a trend toward sympathetic dominance. However, the lack of significant changes suggests that sympathetic and parasympathetic shifts occurred proportionally, maintaining relative autonomic balance. These results emphasize that task difficulty has a stronger impact on time-domain HRV measures than on frequency-domain proportional metrics.
High-obstacle tasks led to a significant reduction in the PNS index (−2.4 ± 0.8 to −3.6 ± 0.6) and a nearly threefold increase in the SNS index (4.7 ± 2.7–11.9 ± 5.4). The stress index (SI) doubled during high-obstacle tasks (22.4 ± 9.8–45.3 ± 20.7). These results demonstrate a pronounced shift toward sympathetic dominance, consistent with the “fight-or-flight” response to the heightened physical and mental demands of the task.
Respiratory responses
High-obstacle tasks significantly increased respiratory and metabolic demands, specifically with VE rising from 22.5 ± 5.3 L.min−1 to 40.5 ± 8.5 L.min−1 from the low- to high-obstacle condition. This increase in VE is much higher than the 7.7% increase reported during high versus low overground climbing (Gajdošík et al., 2020) in a similar population. It appears that the stress response to height is more pronounced when arm contact with a support is not possible and free space under the feet is present throughout the entire exercise. It should be noted that the increase in respiratory and metabolic responses was due to height exposure alone, as the speed of walking was kept the same as in the low-obstacle task. These responses also show that stress itself may increase the metabolic cost by 63%, as measured by VO2.
There are several limitations that must be acknowledged. The sample consisted of a relatively homogenous group of Czech university students, which limits the study’s generalizability to the broader population and to the general domain of education or therapeutic programs. Future research should include participants with greater heterogeneity to enable cross-cultural comparisons in the analyses presented.
Across all measures, there is a possibility for learning effects across multiple trials. Habituation, increased task familiarity, and task sequence may have combined to sequentially reduce physiological and psychological stress measures, most notably during the second low-obstacle trial. Furthermore, in the long term, it is unknown how longitudinal repeated exposures might influence stress and anxiety responses. Indeed, substantial variability in stress responses was observed across all variables, reflecting individual differences in stress adaptation and perception. This variability is likely influenced by factors such as prior experience with height (Ewert et al., 2016; Gajdošík et al., 2020; Giles et al., 2014), personality traits (Brouwer et al., 2015; Luo et al., 2023; Penley and Tomaka, 2002), social perceptions (Gillman et al., 2023), and other individual characteristics. In addition, external factors such as temperature, wind, light rain, humidity, and physiological needs (e.g., hunger, thirst, fatigue) may have also affected the outcomes (Ewert et al., 2016). Future research should explore the mediating or moderating roles of these confounding factors in stress responses and examine how adventure-based programs influence changes in stress markers. Although our study focused on HRV, respiratory measures, and self-reported anxiety to assess acute stress responses, future research could benefit from incorporating a broader set of physiological and micro-behavioral indicators. For example, facial micro-expression analysis (e.g., orbicularis oculi electromyography) and posture or gait dynamics may offer more nuanced real-time insights into participants’ experiences of height. Integrating these measures into multimodal models, along with temporal self-reporting, HRV, and ventilatory measures, would enable continuous, ecologically valid stress monitoring. This approach would allow for improved temporal resolution in detecting stress responses and could enhance intervention strategies in high-stress environments such as outdoor adventure programs.
Conclusion
Walking at height induces a high level of perceived subjective stress, which is reflected in changes in both psychological and physiological markers. Using HR and respiratory markers such as VE, VO2, or VT, along with anxiety questionnaires during log walking, may be a relatively simple way to assess stress coping in outdoor adventure programs. This approach may also serve as a simple method for evaluating the effectiveness of these programs. However, combining physiological and psychometric tools is essential, as they measure different dimensions of the stress response.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Faculty of Physical Education and Sport, Charles University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
LP: Writing – review & editing, Visualization, Formal analysis, Investigation, Data curation, Writing – original draft, Conceptualization. MR: Supervision, Writing – review & editing. TB: Investigation, Writing – review & editing. JB: Writing – original draft, Writing – review & editing, Supervision, Conceptualization, Methodology.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by Charles University programme GAUK, Effect of a shortterm outdoor activities program on the psychophysiological response during acute stress (nr. 82426).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that Gen AI was used in the creation of this manuscript. Generative AI was used as a collaborator to inform the authors about aspects raised by Reviewers such as micro-behavioral stress indicators, and to suggest edits to drafted new sections in response to Reviewer comments.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Bailey, A. W., Johann, J., and Kang, H.-K. (2017). Cognitive and physiological impacts of adventure activities: beyond self-report data. J. Exp. Educ. 40, 153–169. doi: 10.1177/1053825917701250
Baláš, J., Giles, D., Chrastinová, L., Kárníková, K., Kodejška, J., Hlaváčková, A., et al. (2017). The effect of potential fall distance on hormonal response in rock climbing. J. Sports Sci. 35, 989–994. doi: 10.1080/02640414.2016.1206667
Brodbeck, J., Abbott, R. A., Goodyer, I. M., and Croudace, T. J. (2011). General and specific components of depression and anxiety in an adolescent population. BMC Psychiatry 11:191. doi: 10.1186/1471-244X-11-191
Brouwer, A.-M., Van Schaik, M. G., Korteling, J. E., Van Erp, J. B. F., and Toet, A. (2015). Neuroticism, extraversion, conscientiousness and stress: physiological correlates. IEEE Trans. Affect. Comput. 6, 109–117. doi: 10.1109/TAFFC.2014.2326402
Bunting, C. J., and Gibbons, E. S. (2001). Plasma catecholamine and cardiovascular reactivity during an acute high ropes course event. Int J Psychophysiol 42, 303–314. doi: 10.1016/s0167-8760(01)00152-0
Bunting, C. J., Tolson, H., Kuhn, C., Suarez, E., and Williams, R. B. (2000). Physiological stress response of the neuroendocrine system during outdoor adventure tasks. J. Leis. Res. 32, 191–207. doi: 10.1080/00222216.2000.11949913
Castaldo, R., Melillo, P., Bracale, U., Caserta, M., Triassi, M., and Pecchia, L. (2015). Acute mental stress assessment via short term HRV analysis in healthy adults: a systematic review with meta-analysis. Biomed Signal Process Control 18, 370–377. doi: 10.1016/j.bspc.2015.02.012
Clark, L. A., and Watson, D. (1991). Tripartite model of anxiety and depression: psychometric evidence and taxonomic implications. J. Abnorm. Psychol. 100, 316–336. doi: 10.1037/0021-843X.100.3.316
Cox, R. H., Martens, M. P., and Russell, W. D. (2003). Measuring anxiety in athletics: the revised competitive state anxiety inventory–2. J. Sport Exerc. Psychol. 25, 519–533. doi: 10.1123/jsep.25.4.519
Critchley, H. D., Wiens, S., Rotshtein, P., Öhman, A., and Dolan, R. J. (2004). Neural systems supporting interoceptive awareness. Nat. Neurosci. 7, 189–195. doi: 10.1038/nn1176
Davidson, C., Ewert, A., and Chang, Y. (2016). Multiple methods for identifying outcomes of a high challenge adventure activity. J. Exp. Educ. 39, 164–178. doi: 10.1177/1053825916634116
Draper, N., Jones, G. A., Fryer, S., Hodgson, C. I., and Blackwell, G. (2010). Physiological and psychological responses to lead and top rope climbing for intermediate rock climbers. Eur. J. Sport Sci. 10, 13–20. doi: 10.1080/17461390903108125
Ewert, A. (2015). The use of biomarkers in outdoor education research: promises, challenges, and the development of evidence. Res. Outdoor Educ. 13, 1–15. doi: 10.1353/roe.2015.0001
Ewert, A., Davidson, C., and Chang, Y. (2016). The body doesn’t lie: measuring stress in adventure recreation activities. J. Leis. Res. 48, 327–337. doi: 10.18666/JLR-2016-V48-I4-6807
Fernandes, M. G., Nunes, S. A., Raposo, J. V., Fernandes, H. M., and Brustad, R. (2013). The CSAI-2: an examination of the instrument’s factorial validity and reliability of the intensity, direction and frequency dimensions with Brazilian athletes. J. Appl. Sport Psychol. 25, 377–391. doi: 10.1080/10413200.2012.744780
Foa, E. B., Costello, E. J., Franklin, M., Kagan, J., Kendall, P., Klein, R., et al. (Eds.) (2005). “161 Defining anxiety disorders” in Treating and preventing adolescent mental health disorders: what we know and what we don’t know. A research agenda for improving the mental health of our youth (Oxford University Press). doi: 10.1093/9780195173642.003.0010
Gajdošík, J., Baláš, J., and Draper, N. (2020). Effect of height on perceived exertion and physiological responses for climbers of differing ability levels. Front. Psychol. 11:997. doi: 10.3389/fpsyg.2020.00997
Giles, D., Draper, N., Gilliver, P., Taylor, N., Mitchell, J., Birch, L., et al. (2014). Current understanding in climbing psychophysiology research. Sports Technol. 7, 108–119. doi: 10.1080/19346182.2014.968166
Giles, D., Fryer, S., Dickson, T., Moore, L., and Draper, N. (2020). Effect of chronic exposure to height on the psychophysiological responses to a climbing task. J. Sport Exerc. Sci. 4, 106–111. doi: 10.36905/jses.2020.02.06
Gillman, J. C., Turner, M. J., and Slater, M. J. (2023). The role of social support and social identification on challenge and threat cognitive appraisals, perceived stress, and life satisfaction in workplace employees. PLoS One 18:e0288563. doi: 10.1371/journal.pone.0288563
Gladwell, V., Kuoppa, P., Tarvainen, M., and Rogerson, M. (2016). A lunchtime walk in nature enhances restoration of autonomic control during night-time sleep: results from a preliminary study. Int. J. Environ. Res. Public Health 13:280. doi: 10.3390/ijerph13030280
Goyal, A., Singh, S., Vir, D., and Pershad, D. (2016). Automation of stress recognition using subjective or objective measures. Psychol. Stud. 61, 348–364. doi: 10.1007/s12646-016-0379-1
Kim, H.-G., Cheon, E.-J., Bai, D.-S., Lee, Y. H., and Koo, B.-H. (2018). Stress and heart rate variability: a meta-analysis and review of the literature. Psychiatry Investig. 15, 235–245. doi: 10.30773/pi.2017.08.17
LeDoux, J. E. (1996). The emotional brain: the mysterious underpinnings of emotional life. New York: Simon & Schuster.
Lundqvist, C., and Hassmén, P. (2005). Competitive state anxiety inventory-2 (CSAI-2): evaluating the Swedish version by confirmatory factor analyses. J. Sports Sci. 23, 727–736. doi: 10.1080/02640410400021484
Luo, J., Zhang, B., Cao, M., and Roberts, B. W. (2023). The stressful personality: a meta-analytical review of the relation between personality and stress. Personal. Soc. Psychol. Rev. 27, 128–194. doi: 10.1177/10888683221104002
Magiera, A., Roczniok, R., Sadowska-Krępa, E., Kempa, K., Placek, O., and Mostowik, A. (2018). The effect of physical and mental stress on the heart rate, cortisol and lactate concentrations in rock climbers. J. Hum. Kinet. 65, 111–123. doi: 10.2478/hukin-2018-0024
Martinent, G., Ferrand, C., Guillet, E., and Gautheur, S. (2010). Validation of the French version of the competitive state anxiety inventory-2 revised (CSAI-2R) including frequency and direction scales. Psychol. Sport Exerc. 11, 51–57. doi: 10.1016/j.psychsport.2009.05.001
Penley, J. A., and Tomaka, J. (2002). Associations among the big five, emotional responses, and coping with acute stress. Personal. Individ. Differ. 32, 1215–1228. doi: 10.1016/S0191-8869(01)00087-3
Pereira, T., Almeida, P. R., Cunha, J. P. S., and Aguiar, A. (2017). Heart rate variability metrics for fine-grained stress level assessment. Comput. Methods Prog. Biomed. 148, 71–80. doi: 10.1016/j.cmpb.2017.06.018
Pijpers, J. R., Oudejans, R. R. D., and Bakker, F. C. (2005). Anxiety-induced changes in movement behaviour during the execution of a complex whole-body task. Quart. J. Exp. Psychol. Sect. A 58, 421–445. doi: 10.1080/02724980343000945
Pijpers, J. R., Oudejans, R. R. D., Holsheimer, F., and Bakker, F. C. (2003). Anxiety–performance relationships in climbing: a process-oriented approach. Psychol. Sport Exerc. 4, 283–304. doi: 10.1016/S1469-0292(02)00010-9
Shaffer, F., and Ginsberg, J. P. (2017). An overview of heart rate variability metrics and norms. Front. Public Health 5:258. doi: 10.3389/fpubh.2017.00258
Souza, R. A., Beltran, O. A. B., Zapata, D. M., Silva, E., Freitas, W. Z., Junior, R. V., et al. (2019). Heart rate variability, salivary cortisol and competitive stateanxiety responses during pre-competition and pre-trainingmoments. Biology of Sport, 36, 39–46. doi: 10.5114/biolsport.2018.78905
Taelman, J., Vandeput, S., Spaepen, A., and Van Huffel, S. (2009). “Influence of mental stress on heart rate and heart rate variability” in 4th European conference of the International Federation for Medical and Biological Engineering. eds. J. Vander Sloten, P. Verdonck, M. Nyssen, and J. Haueisen, vol. 22 (Berlin Heidelberg: Springer), 1366–1369.
Thayer, J. F., and Lane, R. D. (2000). A model of neurovisceral integration in emotion regulation and dysregulation. J. Affect. Disord. 61, 201–216. doi: 10.1016/S0165-0327(00)00338-4
Thayer, J. F., and Lane, R. D. (2009). Claude Bernard and the heart–brain connection: further elaboration of a model of neurovisceral integration. Neurosci. Biobehav. Rev. 33, 81–88. doi: 10.1016/j.neubiorev.2008.08.004
Watts, P. B., Coleman, B., Clure, C., Daggett, M., Gallagher, P., Sustrich, P., et al. (1999). Metabolic and cardiovascular responses during work on a high ropes course. J. Sports Med. Phys. Fitness 39, 37–41.
Keywords: ropes course, CSAI-2R oxygen consumption, respiration, metabolic cost, height
Citation: Psohlavec L, Rogerson M, Brtník T and Baláš J (2025) Evaluating acute stress responses to height: validity of heart rate variability, respiratory markers, and competitive state anxiety inventory. Front. Psychol. 16:1597839. doi: 10.3389/fpsyg.2025.1597839
Edited by:
Pedro Forte, Higher Institute of Educational Sciences of the Douro, PortugalReviewed by:
Li Wang, Shanghai Ocean University, ChinaRafael Peixoto, Instituto Superior de Ciências Educativas, Portugal
Copyright © 2025 Psohlavec, Rogerson, Brtník and Baláš. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lukáš Psohlavec, bHVrYXMucHNvaGxhdmVjQGZ0dnMuY3VuaS5jeg==