Abstract
Purpose:
This longitudinal study aimed to explore the bidirectional causal relationship between depressive symptoms and physical exercise among college students, with a focus on the mediating roles of social support and psychological resilience.
Methods:
The Self-Rating Depression Scale (SDS) was used to assess depression. Physical activity Rating Scale (PARS-3), Perceived Social Support Scale (PSSS), Connor-Davidson Resilience Scale (CD-RISC), A longitudinal study of 1,413 college students was conducted over three months, collecting data at two time points (T1: September 15, 2024; T2: 17 December 2024). In this longitudinal study, 1,350 valid samples were obtained. Primary analyses included independent samples t-test, chi-square test, and Pearson correlation. Amos 28.0 was used to construct the cross-lag model and structural equation model for analysis.
Results:
(1) Depressive symptoms at T1 negatively predicted physical activity at T2 (β = −0.07, p < 0.05). Physical exercise at T1 negatively predicted depressive symptoms at T2 (β = −0.08, p < 0.05), and depressive symptoms and physical exercise could predict each other. (2) Social support at T2 played a delayed mediating role in depressive symptoms at T1 and physical exercise at T2 (β = −0.02, [−0.049, −0.006], p < 0.01). (3) Resilience at T2 played a delayed mediating role in depressive symptoms at T1 and physical exercise at T2 (β = −0.03, [−0.049, −0.002], p < 0.01). (4) Social support and resilience at T2 played a delayed chain mediating role in depressive symptoms and physical exercise at T1 (β = −0.01, [−0.024, −0.005], p < 0.01).
Conclusion:
This study highlights the importance of social support and resilience in promoting physical exercise and alleviating depressive symptoms in college students, as well as the interrelationship between depressive symptoms and physical exercise. The results showed that depressive symptoms not only directly affected physical exercise of college students, but also indirectly affected physical exercise of college students through the independent mediating effect of social support and psychological resilience and the chain mediating effect of social support-psychological resilience. In practice, we should improve the social support system and improve the psychological resilience of college students, which can effectively alleviate the depressive symptoms of college students and enhance physical exercise.
1 Introduction
In recent years, mental health issues among college students have become increasingly prominent, with depressive symptoms emerging as a critical challenge affecting academic performance, social interactions, and quality of life. Multiple studies indicate that approximately 20–30% of college students experience varying degrees of mental health issues, with depressive symptoms being particularly prevalent (Wang et al., 2025). Concurrently, physical exercise participation rates in this population remain low, as academic pressures and digitalized lifestyles exacerbate sedentary behaviors and insufficient physical activity—only 40% of college students meet recommended physical activity levels (Schmitter et al., 2020). The transition from high school to university further aggravates these issues, characterized by heightened academic demands and social changes, which increase vulnerability to mental health challenges (Tao et al., 2024). Consequently, depressive symptoms and physical inactivity are widespread among college students globally. While physical exercise has been proven effective in alleviating depressive mood (Noetel et al., 2024), the bidirectional causal relationship between depressive symptoms and physical exercise, as well as their underlying mechanisms, requires further exploration.
Existing research suggests that individuals with higher depressive symptoms often lack exercise motivation due to low mood. However, social support—such as encouragement from friends, family, or peers—can enhance their willingness to engage in physical activity (Ma et al., 2023; Templeton et al., 2025). For instance, team sports or group activities foster social interaction, thereby improving perceived social support and indirectly promoting exercise behavior. Social support not only acts as a direct mediator but also indirectly facilitates exercise adherence by enhancing psychological resilience. Individuals with strong social support are more likely to access external resources when facing stress, bolstering their ability to cope with challenges and maintain long-term exercise habits (Lin et al., 2025). Longitudinal studies reveal that social support exhibits delayed effects in the relationship between depressive symptoms and physical exercise (Cao and Luo, 2024). While depressive symptoms may temporarily reduce perceived social support, its cumulative effects over time can mitigate the inhibitory impact of depression on exercise participation. Additionally, research demonstrates that students with higher psychological resilience can sustain exercise behaviors even during depressive states by setting goals and adjusting strategies (Kuang et al., 2024). Psychological resilience often interacts with social support in a chain-like mechanism, where social support strengthens psychological resources (e.g., self-confidence and optimism), further reinforcing resilience and forming an indirect pathway of “social support → psychological resilience → physical exercise” (Wu et al., 2024). For example, family support may enhance students’ psychological resilience, enabling them to proactively address exercise-related challenges. This occurs because psychological resilience directly alleviates the negative impact of depressive symptoms on physical exercise by improving self-regulation and stress tolerance. College students with higher resilience are more likely to view exercise as a proactive coping strategy rather than avoidance behavior, thereby maintaining regular exercise patterns (Gong et al., 2023). Furthermore, psychological resilience helps individuals overcome physical fatigue or psychological barriers (e.g., self-doubt), thereby enhancing exercise intensity and frequency.
In summary, the mechanisms linking depressive symptoms, physical exercise, social support, and psychological resilience are not unidirectional but complex and dynamic. Despite existing research, gaps persist in understanding the bidirectional relationship between depressive symptoms and physical exercise, as well as the mediating roles of social support and psychological resilience. Most studies employ cross-sectional designs, limiting causal inferences. To address these limitations, this study utilizes a three-month cross-lagged model to investigate the longitudinal and bidirectional relationships between depressive symptoms and physical exercise, while testing the mediating effects of social support and psychological resilience. The aims are to clarify predictive relationships between depressive symptoms and physical exercise among college students and to elucidate the dynamic interplay of social support and psychological resilience within these relationships. Based on theoretical and empirical foundations, the following hypotheses are proposed:
H1: T1 depressive symptoms negatively predict T2 physical exercise.
H2: T1 physical exercise negatively predicts T2 depressive symptoms.
H3: Depressive symptoms and physical exercise mutually predict each other.
H4: T2 social support mediates the longitudinal relationship between T1 depressive symptoms and T2 physical exercise.
H5: T2 psychological resilience mediates the longitudinal relationship between T1 depressive symptoms and T2 physical exercise.
H6: T2 social support and T2 psychological resilience exhibit a delayed chain-mediating effect between T1 depressive symptoms and T2 physical exercise.
2 Participants and methods
2.1 Participants
This study targeted undergraduate students from Sichuan University. A cluster sampling method was employed to recruit 1,413 participants for a questionnaire survey. The questionnaire comprised five sections: demographic information (e.g., gender, age), the Self-Rating Depression Scale (SDS), the Physical Activity Rating Scale, the Perceived Social Support Scale, and the Psychological Resilience Scale. Data collection was conducted in two waves at the university gymnasium, with a three-month interval between assessments (T1: September 15, 2024; T2: December 17, 2024). Identical questionnaires were administered to the same cohort at both time points. After data collection, 1,413 questionnaires were obtained. To ensure data authenticity and reliability, inclusion criteria were applied: (1) Questionnaires completed within 5–15 min. (2) Participants who completed both waves of assessments with matching student IDs and names. Following data filtering and matching, 1,350 valid samples were retained (attrition: 63; validity rate: 95.54%). Among them, 21 people were lost to follow-up due to dropping out of school, withdrawing from school or changing majors. 42 unqualified questionnaires were excluded (incomplete questionnaires). The final sample included: Gender: male (n = 902, 66.8%), female (n = 448, 33.2%). Academic year: freshmen (n = 817, 60.5%), sophomores (n = 525, 38.9%), juniors (n = 6, 0.4%), seniors (n = 2, 0.1%). Only-child status: yes (n = 609, 45.1%), no (n = 741, 54.9%). Residential background: urban (n = 941, 69.7%), rural (n = 409, 30.3%). The mean age of participants was 18.51 ± 0.79 years. This study adhered to the principles of the Declaration of Helsinki and was approved by the Medical Ethics Committee of Sichuan University (approval no.: K2022016). All participants provided written informed consent prior to participation.
2.2 Methods
2.2.1 Self-rating depression scale (SDS)
Depressive symptoms were assessed using the Self-Rating Depression Scale (SDS) developed by Zung at Duke University School of Medicine in 1965 (Zung, 1965). The SDS comprises 20 items, with half positively worded and half reverse-scored. The scale includes four subdimensions: psycho-affective symptoms (2 items), somatic disturbances (8 items), psychomotor disturbances (2 items), and depressive psychological disturbances (8 items). Participants rated their emotional experiences over the past week on a 4-point Likert scale, ranging from 1 (“a little or none of the time”) to 4 (“most or all of the time”). Prior to analysis, reverse-scored items were recoded, and the total raw score was summed and converted to a standardized score by multiplying by 1.25, yielding a range of 25–100. Higher scores indicate more severe depressive symptoms. Based on prior research in Chinese populations (Liu et al., 1995; Wang et al., 2024), severity thresholds were defined as follows: SDS score <50 (no depression), 50–59 (mild depression), 60–69 (moderate depression), and 70–100 (severe depression). The SDS has demonstrated robust cross-cultural validity and reliability. In this study, Cronbach’s α coefficients were 0.847 (T1) and 0.854 (T2), with a test–retest reliability of 0.531, confirming adequate internal consistency and temporal stability.
2.2.2 Physical activity rating scale (PARS-3)
Professor Liang Deqing’s physical activity rating Scale, which was compiled by Japanese psychologist Hashimoto Gongxio and revised by Liang et al., Wuhan Institute of Physical Education, was adopted (Liang, 1994). It mainly reflected the physical exercise of the subjects in the past month. Relevant studies in China have shown that the Chinese version of PARS can better evaluate the physical activity of ordinary college students (Cao and Luo, 2024). The Cronbach’s α coefficients of the two tests in this study were 0.646 and 0.746, respectively, and the test–retest reliability was 0.746. The scale involved three indicators of physical exercise intensity, time and frequency. Each indicator was scored by 5-point Likert. The intensity and frequency were scored as “1–5 points,” and the time was scored as “0–4 points.” The amount of exercise was calculated using the formula: “intensity × time × frequency,” so the scale scores range from “0 to 100. According to previous studies in China, the physical activity levels of college students were classified as follows: “≤19 as small exercise (insufficient physical activity), 20–42 as medium exercise, ≥43 as large exercise.”
2.2.3 Perceived social support scale (PSSS)
The English version of the Perceived Social Support Scale was developed by Blumenthal and others in 1987 and translated into Chinese by Huang and Ren (1996). It is a social support scale that measures the individual’s self-understanding and self-feeling of social support and is widely used in Chinese college students (Lin et al., 2025). The scale included 12 items and consisted of three dimensions: family support, friend support and other support. A 7-point Likert scale was used, ranging from 1 = strongly agree to 7 = strongly agree. The total score ranged from 12 to 84, with higher scores indicating higher overall social support. In this study, the Cronbach’s α coefficient of the first measurement of the scale was 0.945. Family support included 4 items, and its α coefficient was 0.897, and the test–retest reliability was 0.848. Friend support contained 4 items, the α coefficient was 0.913, and the test–retest reliability was 0.845. The other support contained 4 items, and its α coefficient was 0.890, and the test–retest reliability was 0.647. The Cronbach’s α coefficients of social support and each dimension in the second measurement were 0.946, 0.885, 0.898 and 0.916, respectively. The Cronbach’s α coefficient of each subscale ranged from 0.890 to 0.913, indicating that it had good reliability and validity.
2.2.4 Connor-Davidson resilience scale (CD-RISC)
The Resilience Scale was developed by Connor and Davidson (2003), and the Chinese version was used in this study (Yu and Zhang, 2007), which has been widely used to assess resilience among Chinese college students and adults (Yu et al., 2023). The 25-item scale is divided into three dimensions: resilience (e.g., I am not easily defeated), strength (e.g., I am proud of my achievements), and optimism (e.g., I try to look at the humorous side of things when faced with problems). A 5-point Likert scale was used, that is, from 1(not at all) to 5(absolutely), with 1 = never, 2 = rarely, 3 = sometimes, 4 = often, and 5 = all the time. The total score of the scale is 100, with higher total scores in each dimension and overall scale indicating higher resilience in each dimension and overall. The Cronbach’s α coefficient of the first measurement of the scale in this study was 0.938. Among them, hardiness contained 13 items, the α coefficient was 0.898, and the test–retest reliability was 0.662. Strength contained 8 items, the α coefficient was 0.856, and the test–retest reliability was 0.5. Optimism contained 4 items, and its α coefficient was 0.600, and the test–retest reliability was 0.716. In the second measurement, the Cronbach’s α coefficients of the scale and each dimension were 0.936, 0.894, 0.847 and 0.600, respectively. The Cronbach’s α coefficient of each subscale ranged from 0.600 to 0.898. Numerous studies have shown that the scale has good reliability and validity.
2.3 Statistical processing
This study used SPSS 22.0 and AMOS 28.0 for data analysis. The former was used for descriptive analysis, preliminary analysis and correlation analysis, and the latter was used to construct the cross-lag model and the mediation analysis of structural equation modeling procedures. Firstly, SPSS 27.0 was used for preliminary analysis, and common method bias test, descriptive statistics, Pearson correlation analysis and the difference analysis of each variable in time were performed on the data to comprehensively understand the relationship between sample characteristics and variables. Specifically, descriptive statistics, including means, standard deviations, and frequencies, were calculated and analyzed. Pearson correlation coefficients were calculated to examine bivariate associations between study variables. Cronbach α coefficients were also calculated to assess the reliability of the scale, and values greater than 0.7 were considered available for further analysis. For ease of interpretation, Pearson’s correlation coefficients were divided into five levels according to Cohen’s (2013) criterian: negligible (≤0.19), low (0.20–0.39), medium (0.40–0.59), medium-high (0.60–0.79), and high (≥0.80).
Finally, to test the hypothesized causal relationship and the mediating effect between variables, Amos 28.0 was used to construct the Cross-lagged model and structural equation model. The χ2 statistical index and root mean square error (RMSEA) were used as the absolute fitting index. The comparative fit index (CFI), Tucker-Lewis index (TLI), and goodness-of-fit index (GFI) were used as incremental fit indices. The standardized root mean square residual (SRMR) of χ2/df < 5, RMSEA < 0.08, CFI, TLI and GFI values > 0.9 was less than 0.08, indicating that the model fit was good. The bias-corrected Bootstrap method was used for testing, with a random sampling number of 1,000 (Hayes, 2017). Data are presented as mean ± standard deviation (M ± SD). The level of significance for statistical analysis was set as p < 0.05 for statistical difference, p < 0.01 for statistically significant difference, and p < 0.001 for statistically very significant difference.
3 Results
3.1 Test of common method biases
To test the degree to which the two sets of measurement data were influenced by common method bias, Harman’s single—factor test was used (Livingstone et al., 1997). The results showed that the variance explained by the first factor was 32.10 and 31.92% respectively, both below the critical value of 40%. This indicates that there is no serious common method bias.
3.2 Descriptive statistics and correlation analysis
Means, standard deviations, and correlation coefficients for depressive symptoms, social support, psychological resilience, and physical exercise are in Table 1. The two—measurement results show that T1 depressive symptoms are significantly correlated with T1 social support, T1 psychological resilience, T1 depressive symptoms, T2 depressive symptoms, T2 social support, T2 psychological resilience, and T2 physical exercise (p < 0.01). Depressive symptoms are negatively correlated with physical exercise, with correlation coefficients of r = − 0.131 (p < 0.01) at T1 and r = − 0.139 (p < 0.01) at T2. T1 depressive symptoms are significantly negatively correlated with T2 physical exercise behavior (r = − 0.139, p < 0.01), and T2 depressive symptoms are significantly negatively correlated with T1 physical exercise (r = − 0.131, p < 0.01). The significant correlation between depressive symptoms and physical exercise meets the prerequisite conditions for cross—lagged analysis.
Table 1
| Variable | M ± SD | SDS (T1) | RE (T1) | SS (T1) | PE (T1) | SDS (T2) | RE (T2) | PSS (T2) | PE (T2) |
|---|---|---|---|---|---|---|---|---|---|
| SDS (T1) | 33.93 ± 7.446 | 1 | |||||||
| RE (T1) | 92.77 ± 14.36 | −0.696** | 1 | ||||||
| SS (T1) | 68.23 ± 11.56 | −0.562** | 0.648** | 1 | |||||
| PE (T1) | 53.99 ± 30.64 | −0.131** | 0.179** | 0.089** | 1 | ||||
| SDS (T2) | 34.25 ± 7.47 | 0.897** | −0.696** | −0.562** | −0.131** | 1 | |||
| RE (T2) | 92.20 ± 14.59 | −0.696** | 0.894** | 0.648** | 0.179** | −0.696** | 1 | ||
| SS (T2) | 67.68 ± 11.71 | −0.556** | 0.643** | 0.997** | 0.087** | −0.556** | 0.643** | 1 | |
| PE (T2) | 30.50 ± 25.15 | −0.139** | 0.208** | 0.111** | 0.915** | −0.139** | 0.208** | 0.108** | 1 |
Descriptive statistics and correlation analysis of depressive symptoms, physical exercise, social support, and psychological resilience in two measurements (N = 1,350).
SDS, Symptoms of depression; RE, Resilience of mind; SS, Social Support; PE, Physical exercise. *p < 0. 05, **p < 0. 01, ***p < 0. 001.
3.3 Analysis of the basic status of depression level of college students
3.3.1 Analysis of depression level of college students
Among the college students surveyed in this study, 1,087 (80.5%) had no depression (normal), 193 (14.3%) had mild depression, 65 (4.8%) had moderate depression, and 5 (0.4%) had severe depression. See Table 2 for the results.
Table 2
| Depression level | Frequency | Percentage (%) |
|---|---|---|
| No depression | 1,087 | 80.5 |
| Mild depression | 193 | 14.3 |
| Moderate depression | 65 | 4.8 |
| Severe depression | 5 | 0.4 |
| Total | 1,350 | 100 |
Analysis of depression levels among college students.
3.3.2 Analysis of differences in depression scores among different grades of college students
As shown in Table 3, the depressive symptom scores of college students from different grades are as follows: Freshmen have a mean of 41.43 (SD = 9.25), sophomores a mean of 44.59 (SD = 9.02), juniors a mean of 50.21 (SD = 16.48), and seniors a mean of 51.88 (SD = 2.65). A one-way ANOVA reveals a significant difference in the mean depressive scores among the different grades (F = 16.06, p < 0.05).
Table 3
| Grade (M ± SD) | ||||||
|---|---|---|---|---|---|---|
| Grade | Freshmen (n = 817) | Sophomores (n = 525) | Juniors (n = 6) | Seniors (n = 2) | F | P |
| Depressive score | 41.43 ± 9.25 | 44.59 ± 9.02 | 50.21 ± 16.48 | 51.88 ± 2.65 | 16.06 | 0.009 |
Analysis of variance in depressive scores among college students of different grades.
3.4 Analysis of physical exercise status of college students
3.4.1 Analysis of physical exercise volume of college students
Of the college students surveyed, 360 (26.7%) engaged in high-intensity exercise, 381 (28.2%) in moderate-intensity exercise, and 609 (45.1%) in low-intensity exercise. See Table 4 for details.
Table 4
| Exercise level | Frequency | Percentage (%) |
|---|---|---|
| Low | 609 | 45.1 |
| Moderate | 381 | 28.2 |
| High | 360 | 26.7 |
| Total | 1,350 | 100 |
Physical exercise level statistics among college students.
3.4.2 Analysis of differences in physical exercise volume among different grades of college students
As shown in Table 5, among the surveyed college students, freshmen, sophomores, and seniors had mean exercise scores of 28.6, 33.48, and 19.45, respectively, indicating moderate—intensity exercise. Juniors had a mean score of 51.33, indicating vigorous—intensity exercise. A one—way ANOVA showed no significant difference in exercise levels across grades (p > 0.05).
Table 5
| Grade (M ± SD) | ||||||
|---|---|---|---|---|---|---|
| Grade | Freshmen (n = 817) | Sophomores (n = 525) | Juniors (n = 6) | Seniors (n = 2) | F | P |
| Exercise score | 28.6 ± 24.09 | 33.48 ± 26.34 | 51.33 ± 33.67 | 19.50 ± 6.36 | 5.18 | 0.06 |
Comparative analysis of exercise volume of college students in different grades.
3.5 Analysis of differences in time for each variable
Paired—samples t—tests were run on the data of depressive symptoms, social support, psychological resilience, and physical exercise from the first and second measurements. Results are in Table 6 Between the two measurements, except for stable social support scores, depressive symptom scores dropped significantly (t = −2.074, p = 0.038), psychological resilience scores decreased significantly (t = 1.994, p = 0.046), and physical exercise scores fell markedly (t = 23.538, p < 0.001).
Table 6
| Variable | T1 | T2 | t | p |
|---|---|---|---|---|
| SDS | 33.93 ± 7.446 | 34.25 ± 7.47 | −2.074 | 0.038 |
| RE | 92.77 ± 14.36 | 92.20 ± 14.59 | 1.994 | 0.046 |
| SS | 68.23 ± 11.56 | 67.68 ± 11.71 | 1.355 | 0.176 |
| PE | 53.99 ± 30.64 | 30.50 ± 25.15 | 23.538 | <0.001 |
Analysis of differences in depressive symptoms, social support, psychological resilience and physical exercise (N = 1,350).
SDS, Symptoms of depression; RE, Resilience of mind; SS, Social Support; PE, Physical exercise.
3.6 The cross-lagged model
Based on the significant correlation between depressive symptoms and physical exercise, this study used a cross—lagged model to analyze data from two assessments three months apart, testing for bidirectional effects between depressive symptoms and physical exercise. The model was built using four T1 depressive symptom dimensions (psychotic, somatic, psychomotor, and psychological) and three T2 physical exercise dimensions (intensity, time, frequency) as indicator variables. Amos 28.0 was used with maximum likelihood estimation for model fitting. The model showed good fit indices (χ2/df = 2.42, CFI = 0.981, GFI = 0.982, TLI = 0.976, RMSEA = 0.032, SRMR = 0.04). The cross—lagged path diagram (Figure 1) shows that T1 depressive symptoms negatively predict T2 physical exercise (β = −0.07, [−0.140, −0.001], p = 0.045), supporting Hypothesis 1. Similarly, T1 physical exercise negatively predicts T2 depressive symptoms (β = −0.08, [−0.151, −0.008], p = 0.027), supporting Hypothesis 2. Thus, depressive symptoms and physical exercise can predict each other, supporting Hypothesis 3. The results indicate mutual negative effects between depressive symptoms and physical exercise.
Figure 1

Cross-lagged model plots of depressive symptoms and physical exercise. SDS1, Psycho-affective symptoms; SDS2, Somatic disorders; SDS3, Psychomotor disorders; SDS4, Depressive disorders; PE1, Intensity of exercise; PE2, Time to exercise; PE3, Frequency of exercise. *p < 0.05, **p < 0.01, ***p < 0.001.
3.7 Mediation analysis
This study used a structural equation model to test the delayed chain—mediated effects of social support and psychological resilience on the longitudinal link between college students’ depressive symptoms and physical exercise.
T1 depressive symptoms (four dimensions: psychotic—affective, somatic, psychomotor, and psychological) were the predictor, and T2 physical exercise (three dimensions: intensity, time, frequency) was the outcome. T2 social support (three dimensions: family, friend, and other support) and T2 psychological resilience (three dimensions: toughness, strength, and optimism) were mediators. Maximum likelihood estimation was used for model fitting. The model fit was good: χ2/df = 4.6, RMSEA = 0.05, CFI = 0.979, GFI = 0.969, TLI = 0.972, and SRMR = 0.03. The significance of the mediated effects was tested using a bias—corrected Bootstrap method with 1,000 repeated samples. Figure 2 shows the standardized path coefficients of the model.
Figure 2
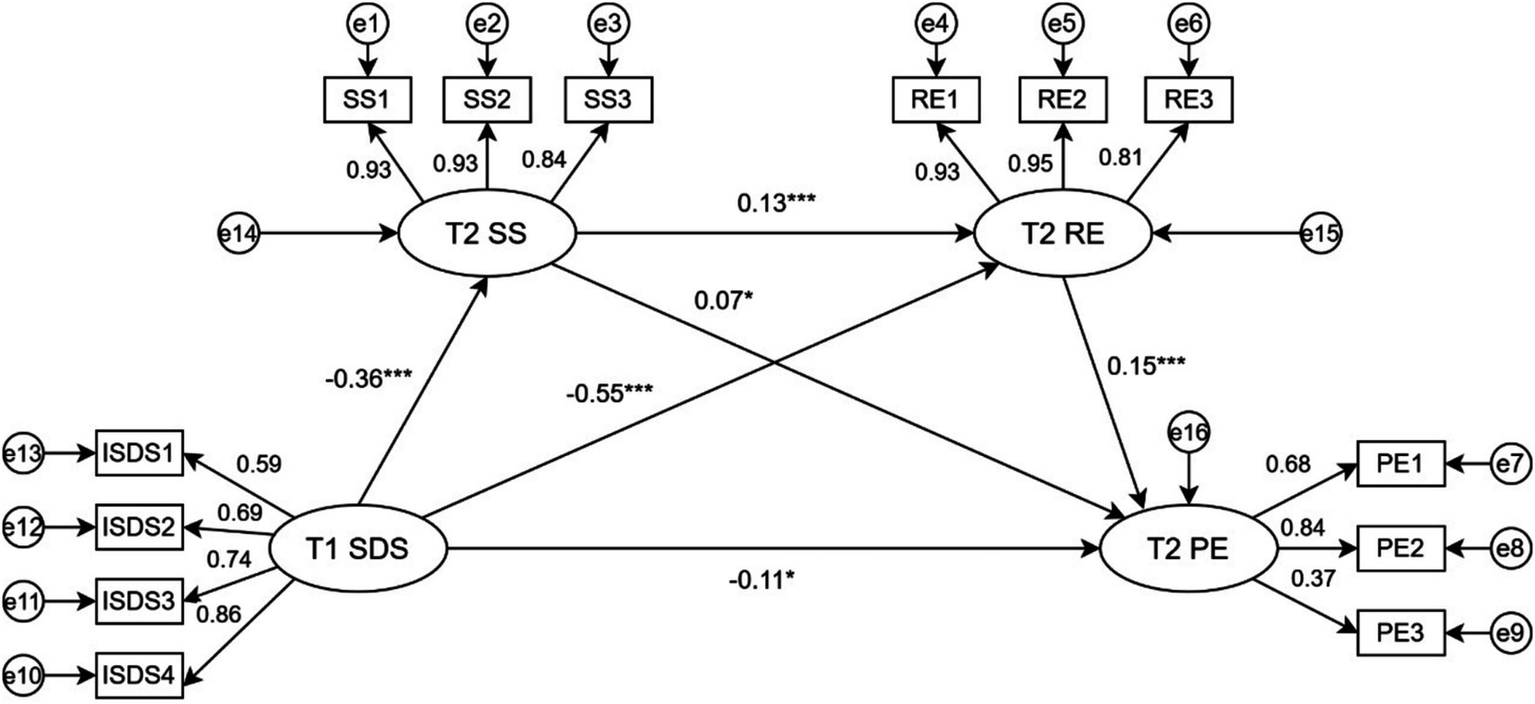
Plot of standardized path coefficients for the time-lapse chain mediation model. SDS, Symptoms of depression; RE, Resilience of mind; SS, Social Support; PE, Physical exercise; SDS1, Psycho-affective symptoms; SDS2, Somatic disorders; SDS3, Psychomotor disorders; SDS4, Depressive disorders; SS1, Family support, SS2, Support from friends; SS3, Other Support; RE1, Strength of force; RE2, Hardiness; RE3, Optimism; PE1, Intensity of exercise; PE2, Time to exercise; PE3, Frequency of exercise. *p < 0. 05, **p < 0. 01, ***p < 0. 001.
As shown in Table 7, T1 depressive symptoms directly and negatively predict T2 physical exercise (β = −0.11, [−0.204, −0.010], p = 0.015), accounting for 47.83% of the total effect. The mediating effect of T2 social support between T1 depressive symptoms and T2 physical exercise is significant (β = −0.03, [−0.101, −0.002], p = 0.046), accounting for 13.04% of the total effect, which supports Hypothesis H4. The mediating effect of T2 psychological resilience between T1 depressive symptoms and T2 physical exercise is also significant (β = −0.08, [−0.271, −0.048], p = 0.008), making up 34.78% of the total effect, which supports Hypothesis H5. Moreover, the chain mediating effect of T2 social support and T2 psychological resilience between T1 depressive symptoms and T2 physical exercise is significant (β = −0.01, [−0.024, −0.005], p = 0.004), representing 4.35% of the total effect, thus supporting Hypothesis H6.
Table 7
| Effect | Path | 95%CI | β | Effect size |
|---|---|---|---|---|
| Direct effect | T1 SDS → T2 PE | [−0.204, −0.010] | −0.11 | 47.83% |
| Effect of mediation | T1 SDS → T2 SS → T2 PE | [−0.101, −0.002] | −0.03 | 13.04% |
| T1 SDS → T2 RE → T2 PE | [−0.271, −0.048] | −0.08 | 34.78% | |
| T1 SDS → T2 SS → T2 RE → T2 PE | [−0.024, −0.005] | −0.01 | 4.35% | |
| Indirect effect | [−0.358, −0.085] | −0.12 | 52.17% | |
| Total effect | [−0.574, −0.283] | −0.23 |
Bootstrap results for standardized path coefficients of the model (N = 1,350).
SDS, Symptoms of depression; RE, Resilience of mind; SS, Social Support; PE, Physical exercise.
4 Discussion
4.1 Results discussion
This study used cross-lagged and structural equation models to analyze the causal relationship between college students’ depressive symptoms and physical exercise, as well as the mediating effects of social support and psychological resilience. Over three months, from Time 1 (T1) to Time 2 (T2), both depressive symptoms and exercise levels decreased. Depressive symptoms (SDS) and physical exercise (PE) were negatively correlated, with T1 depressive symptoms negatively predicting T2 physical exercise (β = −0.07), and T1 physical exercise negatively predicting T2 depressive symptoms (β = −0.08). This suggests a bidirectional causal relationship where each can predict the other, indicating a dynamic interaction (Kandola and Stubbs, 2019).
This implies that depressive symptoms may reduce physical exercise participation by lowering motivation and energy, while insufficient exercise may worsen low mood, creating a vicious cycle. The neurobiological mechanisms of depression, such as reduced dopamine secretion, decrease motivation for exercise, and insufficient exercise increases inflammatory factors, further worsening mood (Kandola et al., 2019). Physical exercise enhances psychological resilience by promoting brain—derived neurotrophic factor (BDNF) secretion, which in turn promotes exercise participation (Rebar et al., 2015).
Based on Cohen and Wills (1985) buffer hypothesis, social support can reduce the negative impact of depressive symptoms on behavior like exercise by providing emotional support, resources, and a sense of belonging. This study found that T1 depressive symptoms indirectly suppress T2 physical exercise by reducing T2 social support (β = −0.03), confirming the Social Support Buffering Theory. Depressive symptoms may reduce perceived support by causing social withdrawal, and low social support further decreases exercise participation (Pearce et al., 2022; Yuan et al., 2025). Psychological resilience helps individuals maintain behavioral stability under stress (Hobfoll, 1989). This study shows that T1 depressive symptoms indirectly lower T2 physical exercise by depleting psychological resilience (β = −0.08), indicating depression may impair exercise adherence through a “resource—loss cycle.” Those with high resilience are more likely to use alternative resources to maintain exercise habits (Xu et al., 2021; Jiang and Xiao, 2024), aligning with the COR theory’s “resource—gain spiral.” Additionally, the significant chain mediating effect of social support and psychological resilience (β = −0.01) suggests depressive symptoms can indirectly inhibit exercise by reducing social support and resilience. The combined effect of psychological resilience and social support reflects the interaction between individual traits and microsystems like family and peers (Wu et al., 2025; LIU et al., 2025). Family support can enhance psychological resilience by boosting self‐efficacy, promoting exercise behavior. Social support can also strengthen resilience through resource transfer; peer encouragement helps overcome exercise challenges, accumulating resilience resources like persistence (Shah et al., 2024; Visted et al., 2024; Visted et al., 2023).
The direct effect accounts for 47.83% of the total effect, indicating other potential mechanisms, like neurobiological factors, need further exploration. Our findings align with recent longitudinal studies supporting the bidirectional relationship between depression and exercise but further reveal the chain mediating mechanism of social support and psychological resilience, addressing the limitation of previous studies focusing on single mediators. Moreover, the mediating effect of social support (13.04%) is lower than that of psychological resilience (34.78%), suggesting internal resources like resilience may be more crucial than external support for exercise behavior in college students. Other psychological factors, such as personality traits, or situational factors, such as academic stressors and environmental support, may also mediate or moderate the effects observed in our study. Future research could examine how personality traits influence an individual’s response to depressive symptoms and their subsequent engagement in physical activity. In addition, studying academic how stress either exacerbates or alleviates the relationship between depression and exercise could yield valuable insights. Environmental support, including sports facilities and university health programs, is also a potential factor that may influence this relationship. Future studies should incorporate these variables to gain a more comprehensive understanding of the complex interplay between mental health and physical activity.
4.2 Research significance
This research explores the bidirectional relationship between depressive symptoms and physical exercise, as well as the mediating role of social support and psychological resilience. It offers valuable insights for developing targeted interventions to enhance college students’ mental health and promote physical activity. By strengthening social support systems and building psychological resilience, universities and policymakers can effectively reduce depressive symptoms and encourage regular exercise, improving students’ overall well-being. In practice, the findings guide college mental health interventions: Universities and mental health practitioners can develop integrated programs combining social support enhancement and psychological resilience training. For example, organizing group exercise activities can promote social connections and support networks, potentially alleviating depressive symptoms and encouraging regular physical exercise. Additionally, resilience—building initiatives like stress—management workshops and cognitive—behavioral training can help students deal more effectively with academic and personal challenges. These programs can be implemented through campus recreation centers, student affairs departments, and mental health services. Furthermore, mental health practitioners can use our findings to develop targeted interventions for students with elevated depressive symptoms, focusing on enhancing psychological resilience and promoting physical activity as a supplementary treatment approach. By integrating these strategies into existing mental health programs, universities can create a more supportive environment that promotes overall student well—being and academic success.
4.3 Limitations and future directions
This study has some limitations despite its rigorous design. First, the sample was only from Chinese college students, which may limit the generalizability of the findings. Caution is needed when applying these results to other cultural or age groups. More diverse samples from different cultural and institutional backgrounds will be included in the future. Second, the longitudinal interval of the study was three months, a time frame chosen to take into account practical feasibility and the need to observe initial behavioral and emotional changes, however, we are aware that this may not fully capture the long-term effects of changes in psychological structure, such as the development of psychological resilience. The reliance on self-reported measures may also introduce common method bias, and future studies could use objective exercise data to enhance validity. Third, the study did not explore other potential mediators or moderators, like personality traits or environmental factors, which might influence the relationship between depressive symptoms and physical exercise.
Future research should address these limitations by incorporating diverse samples and objective measurement tools. Extending the follow-up period to over one year would help explore the long-term stability of mediating effects, and longitudinal studies with multiple time points could deepen our understanding of the dynamic relationships between these variables. Additionally, integrating multimodal data (such as physiological indicators and behavioral records) to build more comprehensive theoretical models and designing intervention experiments would help test the effectiveness of interventions targeting social support and psychological resilience.
5 Conclusion
This longitudinal study explores the bidirectional relationship between college students’ depressive symptoms and physical exercise, revealing a negative predictive relationship over time. Social support and psychological resilience significantly mediate this relationship, both independently and through a chain mediation model.
Theoretical contributions of this study include a deeper understanding of the interplay between mental health and physical activity, and the importance of internal and external resources. For practice, the findings highlight the need to strengthen social support systems and build psychological resilience to effectively reduce depressive symptoms and promote physical exercise among college students.
Statements
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Medical Ethics Committee of Sichuan University (approval number: K2022016). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
YH: Writing – original draft, Methodology, Investigation, Writing – review & editing. XL: Writing – review & editing, Investigation, Methodology. ZL: Investigation, Writing – review & editing. SH: Writing – review & editing, Investigation. WC: Investigation, Writing – review & editing. YJ: Writing – review & editing, Investigation. PH: Investigation, Writing – review & editing. JS: Writing – review & editing. HH: Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by Sichuan University (no. 2021CXC27), National key research and development program (2022YFC3600304 and 2022YFC2704700) and Social Science Foundation of Ministry of Education of China under Grant [24XJC890004], the Fundamental Research Funds for the Central Universities, and the Centre for Sport and Policy Studies, Institute of Physical Education, Sichuan.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1
Cao Y. Luo L. (2024). A longitudinal examination of the effect of physical exercise on the emotional states of college students: exploring the sense of coherence as a mediator through a cross-lagged panel analysis. Front. Behav. Neurosci.18:1428347. doi: 10.3389/fnbeh.2024.1428347
2
Cohen J. (2013). Statistical power analysis for the behavioral sciences. New York, NY: Academic Press.
3
Cohen S. Wills T. A. (1985). Stress, social support, and the buffering hypothesis. Psychol. Bull.98, 310–357. doi: 10.1037/0033-2909.98.2.310
4
Connor K. M. Davidson J. R. T. (2003). Development of a new resilience scale: the Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety18, 76–82. doi: 10.1002/da.10113
5
Gong Z. Wang H. Zhong M. Shao Y. (2023). College students' learning stress, psychological resilience and learning burnout: status quo and coping strategies. BMC Psychiatry23:389. doi: 10.1186/s12888-023-04783-z
6
Hayes A. F. (2017). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (2nd ed.). Guilford Publications. doi: 10.1038/s41591-019-0203-5
7
Hobfoll S. E. (1989). Conservation of resources. A new attempt at conceptualizing stress. Am. Psychol.44, 513–524. doi: 10.1037/0003-066X.44.3.513
8
Huang L. J. Q. Ren W. (1996). An investigation into the interrelation among coping mechanisms, societal support, and psychosomatic manifestations in cancer patients. Chin. Ment. Health J.10, 160–161.
9
Jiang Y. Xiao Y. (2024). The association between family physical activity environment and exercise adherence in adolescents: a chain mediation model. Sci. Rep.14:22117. doi: 10.1038/s41598-024-72964-1
10
Kandola A. Ashdown-Franks G. Hendrikse J. Sabiston C. M. Stubbs B. (2019). Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev.107, 525–539. doi: 10.1016/j.neubiorev.2019.09.040
11
Kandola A. Stubbs B. (2019). Physical activity and inflammation in depression: a review of the evidence and neurobiological mechanisms. Brain Behav. Immun.75, 10–16. doi: 10.1016/j.bbi.2018.11.008
12
Kuang S. Wang W. Yan S. Wu Y. Zhang Y. Li J. et al . (2024). Psychological resilience and depression among college students during the COVID-19 pandemic: the mediating role of self-forgiveness and the moderating role of isolation. Curr. Psychol.43, 23320–23330. doi: 10.1007/s12144-024-05701-6
13
Liang D. Q. (1994). Stress levels of college students and their relationship with physical exercise. Chin. J. Ment. Health8, 5–6.
14
Lin Y. He M. Zhou W. Zhang M. Wang Q. Chen Y. et al . (2025). The relationship between physical exercise and psychological capital in college students: the mediating role of perceived social support and self-control. BMC Public Health25:581. doi: 10.1186/s12889-025-21856-8
15
Liu X. Han H. Li Z. Wang K. Liu D. Zhang J. et al . (2025). Barriers and facilitators to participation in physical activity for students with disabilities in an integrated school setting: a meta-synthesis of qualitative research evidence. Front. Public Health13, 1–14. doi: 10.3389/fpubh.2025.1496631
16
Liu X. C. Tang M. Q. Chen K. Hu L. Wang A. Z. (1995). Comparison of SDS and CES-D assessment results of depressive symptoms in college students. Chin. Mental Health J.1, 19–20.
17
Livingstone L. P. Nelson D. L. Barr S. H. (1997). Person-environment fit and creativity: an examination of supply-value and demand-ability versions of fit. J. Manage.23, 119–146. doi: 10.1177/014920639702300202
18
Ma C. M. S. Law M. Y. M. Ma A. M. Y. (2023). “The relationship between social support and physical activity: a moderated mediation model based on the self-determination theory” in Self-determination theory and socioemotional learning. ed. NgB. (Singapore: Springer).
19
Noetel M. Sanders T. Gallardo-Gómez D. Taylor P. Del Pozo Cruz B. van den Hoek D. et al . (2024). Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials. BMJ (Clin. Res. Ed.).384:e075847. doi: 10.1136/bmj-2023-075847
20
Pearce M. Garcia L. Abbas A. Strain T. Schuch F. B. Golubic R. et al . (2022). Association between physical activity and risk of depression: a systematic review and Meta-analysis. JAMA Psychiatry79, 550–559. doi: 10.1001/jamapsychiatry.2022.0609
21
Rebar A. L. Stanton R. Geard D. Short C. E. Duncan M. J. Vandelanotte C. (2015). A meta-meta-analysis of the effect of physical activity on depression and anxiety in community-dwelling adults. Sports Med.45, 367–374. doi: 10.1080/17437199.2015.1022901
22
Schmitter C. Fuhrmann J. Tsirigotis K. Kranz M. Kociánová D. Heinz A. et al . (2020). Exercise as an adjunct treatment for depression: a systematic review and meta-analysis. J. Affect. Disord.276, 1–10. doi: 10.1016/j.jad.2020.06.069
23
Shah S. A. A. Zaman R. Anwar M. Khan M. I. Ali S. Ullah H. et al . (2024). Psychological resilience and depression among college students: the mediating role of positive and negative affect. J. Affect. Disord.374, 467–474. doi: 10.1016/j.jad.2024.03.066
24
Tao Y. Wu J. Huang L. Zheng K. Liu H. Tian H. et al . (2024). The relationship between health-promoting behaviors and negative emotions in college freshmen: a cross-lagged analysis. Front. Public Health12:1348416. doi: 10.3389/fpubh.2024.1348416
25
Templeton J. M. Dixon W. E. Jr. Williams S. Morelen D. Driggers-Jones L. Robertson C. (2025). The mediating role of social support on the link between adverse childhood experiences and adult mental health. J. Exp. Child Psychol.252:106148. doi: 10.1016/j.jecp.2024.106148
26
Visted E. Johnsen T. L. Bø A. M. Evertsson M. (2023). Reciprocal relationship between resilience and depression: a systematic review and meta-analysis. Psychol. Med.53, 1175–1186. doi: 10.1017/S0033291722004053
27
Visted E. Johnsen T. L. Bø A. M. Evertsson M. (2024). Reciprocal relationship between resilience and depression: a systematic review and meta-analysis. Psychol. Med.54, 843–853. doi: 10.1017/S0033291723000290
28
Wang K. Li Y. Liu H. Zhang T. Luo J. (2024). Relationship between different levels of internet use and depressive tendencies in Chinese college students: the chain mediating effect based on physical activity and social adaptability. BMC Psychol12:670. doi: 10.1186/s40359-024-02153-2
29
Wang Z. Zhu Y. Li C. Xin X. Wang G. Chen J. et al . (2025). Correlation between physical exercise levels, depressive symptoms, and sleep quality in college students: evidence from electroencephalography. J. Affect. Disord.369, 789–799. doi: 10.1016/j.jad.2024.10.043
30
Wu N. Ding F. Ai B. Zhang R. Cai Y. (2024). Mediation effect of perceived social support and psychological distress between psychological resilience and sleep quality among Chinese medical staff. Sci. Rep.14:19674. doi: 10.1038/s41598-024-70754-3
31
Wu J. Shao Y. Zang W. Hu J. (2025). Is physical exercise associated with reduced adolescent social anxiety mediated by psychological resilience?: evidence from a longitudinal multi-wave study in China. Child Adolesc. Psychiatry Ment. Health19:17. doi: 10.1186/s13034-025-00867-8
32
Xu S. Liu Z. Tian S. Ma Z. Jia C. Sun G. (2021). Physical activity and resilience among college students: the mediating effects of basic psychological needs. Int. J. Environ. Res. Public Health18:3722. doi: 10.3390/ijerph18073722
33
Yu X. Zhang J. (2007). Factor analysis and psychometric evaluation of the Connor–Davidson resilience scale (CD-RISC) with Chinese people. Soc. Behav. Pers.35, 19–30. doi: 10.2224/sbp.2007.35.1.19
34
Yu S. Zhang C. Xu W. (2023). Self-compassion and depression in Chinese undergraduates with left-behind experience: mediation by emotion regulation and resilience. J. Clin. Psychol.79, 168–185. doi: 10.1002/jclp.23375
35
Yuan Y. Tu Y. Su Y. Jin L. Tian Y. Chang X. et al . (2025). The mediating effect of self-efficacy and physical activity with the moderating effect of social support on the relationship between negative body image and depression among Chinese college students: a cross-sectional study. BMC Public Health25:285. doi: 10.1186/s12889-025-21350-1
36
Zung W. W. K. (1965). A self-rating depression scale. Arch. Gen. Psychiatry12, 63–70. doi: 10.1001/archpsyc.1965.01720310065008
Summary
Keywords
physical exercise, depressive symptoms, social support, psychological resilience, cross-lagged study, mediating effects
Citation
Hou Y, Liu X, Li Z, Huang S, Chen W, Jiang Y, He P, Sun J and Han H (2025) Association between depressive symptoms and physical exercise in college students: longitudinal mediating effects of social support and psychological resilience. Front. Psychol. 16:1598936. doi: 10.3389/fpsyg.2025.1598936
Received
24 March 2025
Accepted
09 June 2025
Published
23 June 2025
Volume
16 - 2025
Edited by
Lisa Amalia Denza Webster, Leeds Trinity University, United Kingdom
Reviewed by
Antonia Cascales-Martinez, University of Murcia, Spain
Agnieszka Wojtowicz, University School of Physical Education in Krakow, Poland
Updates
Copyright
© 2025 Hou, Liu, Li, Huang, Chen, Jiang, He, Sun and Han.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jingquan Sun, sunjingquan@scu.edu.cnHaijun Han, 78567387@qq.com
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.