 Sonia Diéguez1*
Sonia Diéguez1* Helena García-Llana1
Helena García-Llana1 David Lobato2
David Lobato2 M. Teresa Marín3
M. Teresa Marín3 M. Dolores Arenas3
M. Dolores Arenas3 Fabiola Dapena3
Fabiola Dapena3 Francisco Montesinos2*
Francisco Montesinos2*- 1Centro de Enseñanza Superior Cardenal Cisneros, Madrid, Spain
- 2Faculty of Biomedical and Health Sciences, Universidad Europea de Madrid, Madrid, Spain
- 3Fundación Renal Española, Madrid, Spain
Depression is a prevalent issue among patients with chronic kidney disease, particularly those undergoing hemodialysis. Its presence is associated with reduced quality of life, poor treatment adherence, and an increased risk of hospitalization and clinical deterioration. There is a pressing need for further research into effective psychological interventions aimed at improving the mental health of this population. This open-label pilot clinical trial involved five hemodialysis patients residing in Madrid who had been receiving treatment for over 3 months and exhibited clinically significant depressive symptoms. The intervention consisted of eight weekly, individual, 60-min face-to-face sessions based on a structured Acceptance and Commitment Therapy (ACT) protocol, delivered during dialysis. Outcomes were assessed using standardized questionnaires measuring quality of life, psychological symptoms, psychological inflexibility, and coping strategies at four time points: pre-treatment, post-treatment, and at 3- and 8-month follow-ups. A within-subject analysis was conducted, and the Reliable Change Index was applied to evaluate clinical significance. All participants completed the intervention, which was well accepted and deemed feasible, with high levels of satisfaction reported. Sustained reductions in depressive symptoms were observed in all participants, and improvements in quality of life were noted in three. No significant changes were found in psychological inflexibility or coping strategies. This pioneering pilot study in a Western context provides preliminary evidence supporting the feasibility and potential effectiveness of ACT for treating depression in hemodialysis patients. It highlights the viability of delivering psychological interventions within dialysis units and suggests ACT as a promising therapeutic approach for this population.
1 Introduction
Chronic kidney disease (CKD) is considered a silent epidemic due to its high impact on Public Health, affecting 15.1% of the population (Gorostidi et al., 2018). In the last decade, the number of new patients requiring renal replacement therapy in Spain has increased by 11.6% to reach 141.4 people per million population in 2020 (Sociedad Española de Nefrología, 2022). It has a higher incidence and comorbidity with diabetes mellitus, hypertension, older people, women and racial minorities, being one of the causes of the highest mortality in the world and as well as loss of quality of life (QoL), early retirement and work incapacity (Martín and Lorenzo, 2024). CKD, hemodialysis (HD) and the uncertainty associated with the transplant waiting list lead to significant losses and serious stress in patients, which affect the quality of life and have emotional and behavioral consequences (Shery et al., 2019; Marín et al., 2022), demanding the ability to adjust to changes (Aránega-Gavilán et al., 2022; Heilman et al., 2017).
Depending on the assessment method used, depression is estimated to be present in 21–39% of renal patients (Marín et al., 2022; Palmer et al., 2013). Its presence is associated with the use of steroids and immunosuppressive drugs, female gender, older age, lower educational level, and low QoL, and is more likely if HD is used and also the longer the period of time on dialysis (Ćwiek et al., 2017; Drayer et al., 2006; García-Llana et al., 2014; Vázquez-Martínez et al., 2016). Depression is associated with poorer adherence to treatment and a higher risk of hospitalization and deterioration (Erbay et al., 2021) and is the greatest predictor of health-related QoL (Marín et al., 2022). Depression predicts mortality in CKD after adjusting for age, sex, race, and medical comorbidities (Drayer et al., 2006).
Cognitive-behavioral psychological therapies (CBT) have demonstrated evidence in their application to CKD, improving self-efficacy and self-care (Kim, 2018; Yang et al., 2015; Weiner et al., 2010), reducing depressive symptoms associated with the course of the disease and HD, and improving adherence to pharmacological treatment and the establishment of dietary preventive measures such as fluid restriction or reduction of salt intake (Othman et al., 2020; Nozaki et al., 2005; Payne et al., 2013). Research has revealed certain limitations in the effectiveness of CBT interventions, particularly with regard to reducing the perception of pain, disability, and emotional distress in chronic diseases (Williams et al., 2020).
Ground-breaking therapeutic approaches are being explored in the field of health psychology that seek to promote acceptance and psychological flexibility (PF) to transform the relationship with emotional discomfort, thus facilitating more effective, functional, and sustainable behavioral change processes over time. PF has been defined as being in touch with the present moment without defense and persisting in a behavior or changing it based on chosen values (Hayes et al., 2012). Among the most innovative approaches with the greatest empirical support is Acceptance and Commitment Therapy (ACT), a third-generation cognitive-behavioral therapy based on functional contextualism and relational frame theory (Hayes, 2016). Given that renal patients face a context of chronic loss and uncertainty, unlike CBT approaches—which are more focused on cognitive and emotional control through promoting positive emotions and thoughts—ACT, which assumes that the human ability to arbitrarily relate verbal events is intrinsic to our condition, emphasizes psychological acceptance and flexibility. Therefore, it may offer these patients effective skills to openly and mindfully engage with feelings of loss and future-related concerns inherent to the illness. At the same time, it may help them remain focused and active in vital life domains such as relationships with partners, family, and friends, health, and treatment adherence, maintaining balance among these important areas. In this way, the experience of suffering associated with the loss of health can be reframed as an opportunity for personal growth (Hayes, 2019; Kashdan and Rottenberg, 2010).
Acceptance and Commitment Therapy has been shown to be effective in addressing different psychological problems such as anxiety, stress, depression, obsessive-compulsive disorder and drug abuse (Gloster et al., 2020). In health psychology, its effectiveness has been proven in different chronic diseases to improve the QoL and reduce the symptoms of anxiety and depression (Konstantinou et al., 2023), highlighting its development in chronic pain (Feliu-Soler et al., 2018) and psycho-oncology (Zhao et al., 2021). In CKD, ACT has revealed its contribution to improving emotional well-being (Arnout, 2019), quality of life (Kalbasi et al., 2021; Rouhi et al., 2023), disease perception (Karimi et al., 2019), therapeutic adherence (Rzeszut, 2011; Sadeghi et al., 2024), resilience (Tajbakhsh et al., 2023), emotional well-being (Sarizadeh et al., 2019), spiritual health (Kazemi Daluee and Samari, 2021), decreased depression (Azemi Zeynal et al., 2016), fatigue and enhanced PF (Elander et al., 2023), most studies having been conducted with non-Western patient populations. Although ACT is a promising approach that has already been recognized as a treatment with strong empirical support in applications in health psychology such as chronic pain (Feliu-Soler et al., 2018), there is a lack of studies with CKD in a Western population that evaluate the feasibility and usefulness of ACT on depressive symptoms. Studies are needed that adapt ACT to the needs of Spanish patients on HD with depression. This pilot study aims to explore the feasibility and potential utility of ACT in chronic kidney patients undergoing dialysis residing in Spain with significant levels of depression. It also seeks to evaluate the relevance and practicality of conducting a clinical trial on this topic. Reductions in depression and emotional distress and improvement in QoL were expected after treatment. Changes in symptomatology were expected to be accompanied by changes in processes such as psychological inflexibility and coping strategies. Another objective is to assess whether psychological intervention could be delivered during treatment at the hemodialysis ward, which could lead to greater acceptability. Furthermore, this study is part of a larger project aimed at obtaining evidence to justify conducting a randomized clinical trial with a larger sample. Given the lack of controlled studies in Western populations, we developed this open-label pilot trial as an initial step to evaluate the feasibility and acceptability of an ACT intervention. These results will inform the design of a fully powered randomized controlled trial that directly addresses this gap.
2 Method
2.1 Design
Open-label pilot clinical trial with no control group. Measures were collected using standardized questionnaires before the intervention, at post-treatment and at 3-month and 8-month follow-up, to evaluate both medium-term and longer-term maintenance of treatment effects. The 3-month time point allowed us to assess the stability of immediate gains, while the 8-month follow-up provided insight into whether improvements persisted over time in the context of a chronic health condition. These time frames were also feasible within the organizational context of the dialysis units and maximized retention given the clinical vulnerability of the sample.
2.2 Participants
The study included five patients diagnosed with CKD who were undergoing HD at the Santa Engracia Dialysis Center in Madrid, operated by the Fundación Renal Española. The sample comprised four men and one woman, with a mean age of 51.6 years (SD = 7.26). Only one participant was actively employed, while the remaining four were retired. The average duration on dialysis was 2.6 years. Inclusion criteria were (1) on HD for at least 3 months, (2) total score on HADS ≥14, following the criteria suggested by Preljevic et al. (2012) and (3) clinically significant levels of depression. Exclusion criteria were (1) diagnosis of severe mental disorder, (2) cognitive impairment, (3) on psychiatric treatment or with antidepressant drugs and (4) advanced disease. As shown in Figure 1, a total of 66 patients were evaluated as candidates for the study, of which only 5 met the inclusion criteria and constituted the final sample for this study.
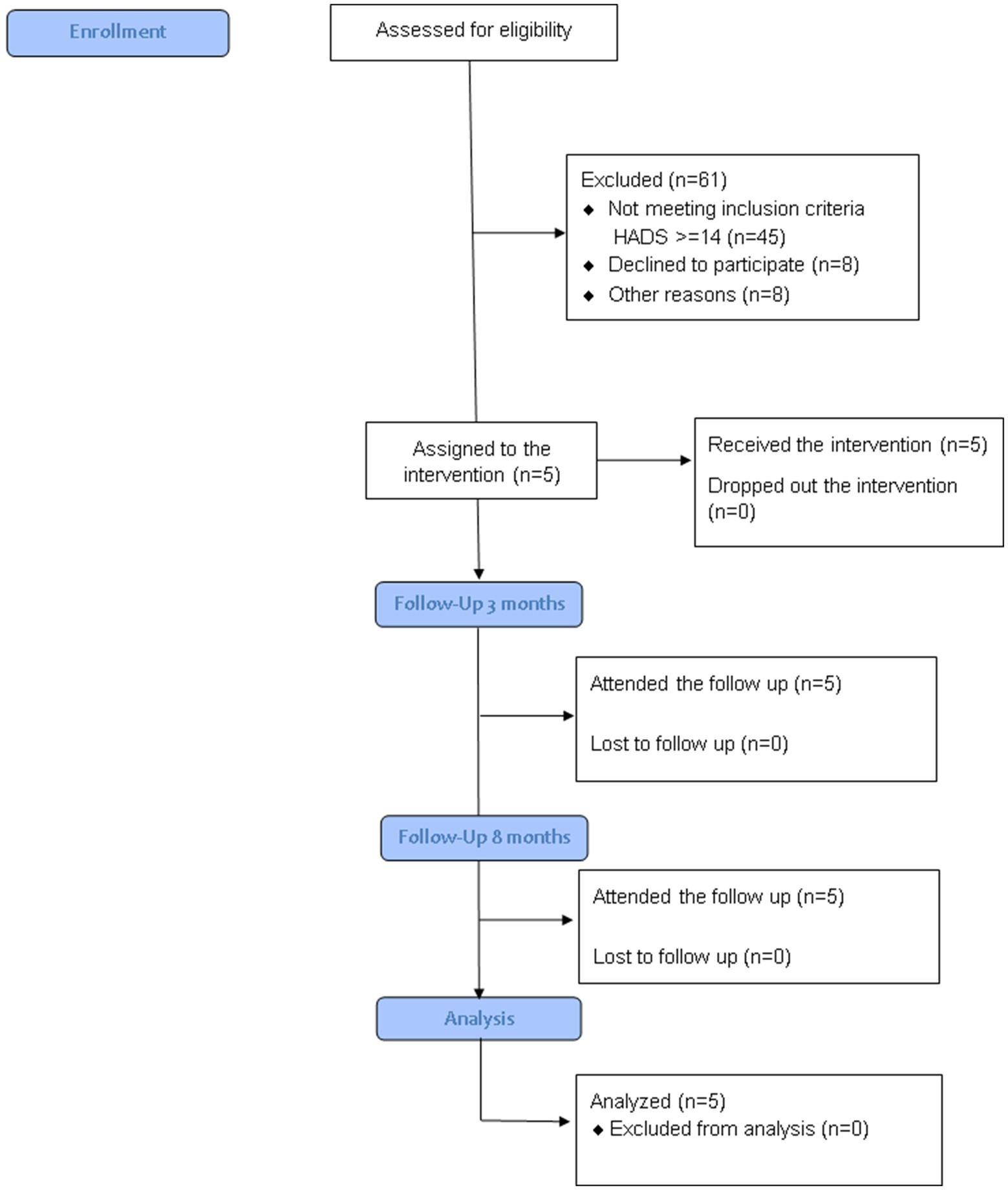
Figure 1. Consort flow diagram.
2.3 Outcomes
The primary outcomes were QoL, depression and emotional distress assessed through standardized questionnaires. Secondary outcomes evaluated anxiety, psychological inflexibility and coping strategies through standardized questionnaires. Additional secondary outcomes included treatment satisfaction, which was assessed using a questionnaire specifically developed for the present study. This ad hoc instrument comprised Likert-scale items evaluating overall usefulness, perceived support, communication with the therapist, the weekly exercises, and perceived difficulty.
2.4 Measures
Anxiety, depression and emotional distress measured by the Hospital Anxiety and Depression Scale (HADS). It is a 14-item four-point Likert-type scale. Scores range between 0 and 42. Higher scores in the overall score indicate higher levels of emotional distress. It includes two subscales, which, respectively, assess generalized anxiety and depression. By avoiding somatic symptoms like fatigue or insomnia, which can coexist with physical disorders, the HADS ensures a more accurate evaluation of psychological symptoms. Designed for chronic patients, it has been validated in Spanish patients (Herrero et al., 2003) demonstrating adequate reliability and validity.
Health Related Quality of Life (QoL) measured by the COOP/WONCA questionnaire, composed of 9 sheets commonly used in primary care and adapted to Spanish CKD patients with adequate reliability and validity (Arenas et al., 2004). Cartoon drawings are included in the questionnaire to make it simple for patients to comprehend and rate their current state of health. The 7-item five-point Likert-type version of the scale was selected. Scores range between 0 and 35. Higher scores indicate lower levels of QoL.
Psychological inflexibility (PI) measured by the Spanish version of the Acceptance and Action Questionnaire-II adapted to the context of patients undergoing hemodialysis (AAQHD-II) (Domínguez et al., 2020). PI is a persistent pattern of behavior characterized by avoidance of discomfort that interferes with the achievement of valued goals. It is a 7-item, seven-point Likert-type scale. Scores range between 7 and 49. Higher scores indicate higher levels of PI. Published studies have shown adequate validity and reliability in Spanish hemodialysis patients (Domínguez et al., 2020).
Coping strategies measured through the Coping Strategies Inventory Short-Form (CSI-SF). It is a 15-item, five-point Likert-type scale that includes 4 subscales: Problem Focused Engagement (PFE), Problem Focused Disengagement (PFD), Emotion Focused Engagement (EFE) and Emotion Focused Disengagement (EFD). Engagement scales refer to exposure to stressors, while disengagement scales allude to avoidance. The Spanish adaptation showed adequate reliability and validity (Tous-Pallarés et al., 2022).
Satisfaction with therapy, evaluated using a custom-designed Therapy Satisfaction Questionnaire, assessing the perceived usefulness of treatment strategies, difficulty and the overall satisfaction with therapy on a scale of 1 to 10.
2.5 Procedure
The study was authorized by the Ethics Committee of the Fundación Jiménez Díaz. All participants signed an informed consent form and the voluntary nature of their participation and confidentiality of the data were guaranteed. Recruitment, assessment, and intervention were carried out while the patients were undergoing hemodialysis at the Fundación Renal Española centers in Madrid. At the beginning, an evaluation session was carried out through a semi-structured interview, which allowed for the functional analysis and adaptation of the intervention to each patient. The intervention included a closed protocol applied over 8 individual face-to-face 60-min sessions on a weekly basis based on ACT (Hayes et al., 2012). Although administered flexibly, the intervention in all patients included the same therapeutic methods applied in the same order. A summary of the clinical methods in each session can be found in Table 1. The intervention protocol is available to interested parties upon reasonable request. The intervention was administered by one therapist with specialized training in ACT, the first author supervised by the study director (last author). Measures were collected at pre and post-treatment and at 3 and 8-month follow-up. Given that patients undergoing hemodialysis frequently experience fatigue, if a patient reported feeling unwell or lacking energy at the scheduled time for an assessment or intervention session, the session was postponed to the next available day for the researcher. This decision was made only after ensuring that the rescheduling would not inadvertently reinforce the patient’s avoidance behaviors.
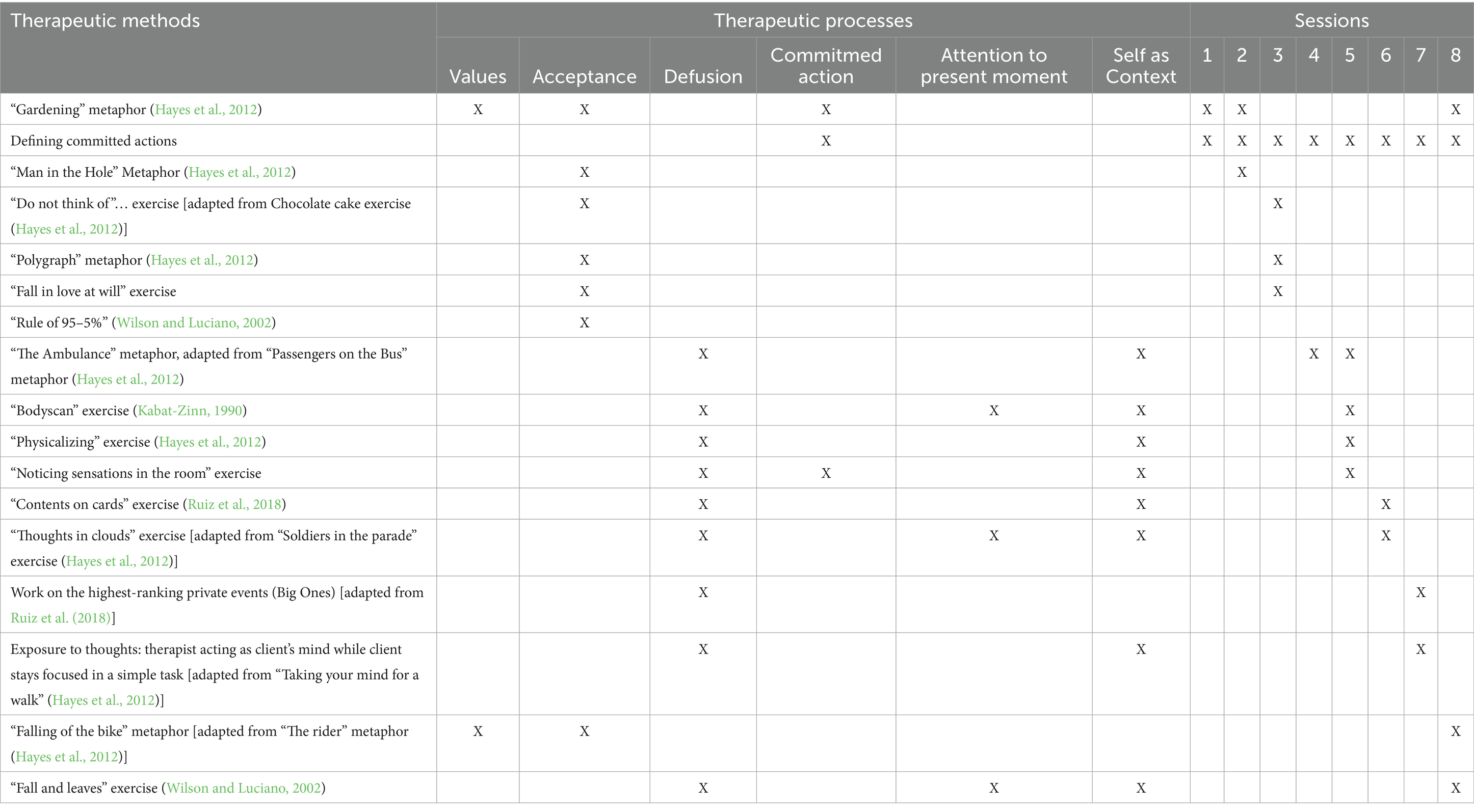
Table 1. Summary of the intervention protocol.
2.6 Statistical analysis
Considering the small number of participants, a within-subject analysis was performed. To determine whether the psychological intervention was clinically significant, the Reliable Change Index (RCI) was used for the dependent variables. The researchers used the method proposed by Jacobson and Truax (1991), which allows observing whether the change in the variables collected is clinically significant and reliable. Three different criteria are proposed by the authors, each with its respective cut-off points. In this study, Criterion A was selected — defined as a post-treatment score falling two standard deviations beyond the mean of the clinical sample — because it best fits the data structure and design of this pilot trial. They maintain that this occurs when there is a return to normal functioning and the change becomes part of the functional population (Castillo, 2010). Three different criteria are proposed, each with its respective cut-off points. The first criterion is the one that best fits this study: a point of two standard deviations beyond the range of the mean in the pre-measure [Cutoff A (Jacobson and Truax, 1991)]. For the analysis of the effect of the intervention, the global scales of the variables were considered.
3 Results
3.1 Adherence and feasibility
The intervention had a high adherence rate. None of the participants dropped out of the intervention. All five patients completed the eight intervention sessions and provided all requested data both at post-treatment and at 3 and 8 month follow-up. Satisfaction with the intervention was high (mean: 8.6 out of 10). The most highly valued aspect was the support obtained from the therapist (9.4), followed by communication with the therapist (9), weekly tasks (8.4) and therapeutic methods (8). The average perceived difficulty was 6.4 and the overall usefulness 8.4. The implementation of the intervention showed its feasibility and acceptability. The study also showed the feasibility of administering the individual intervention to patients in the dialysis room. Patients readily accepted the loss of privacy that came with receiving the intervention in this space and thus not having to spend more time in the healthcare center. The initially planned duration of the 60-min sessions proved to be slightly excessive, as most patients were able to maintain attention for only 50 to 55 min. Consequently, the session content was adjusted and condensed accordingly to better align with participants’ attention spans.
3.2 Within-subject analysis
Figure 2 shows the temporal evolution of the direct scores on the depression and QoL measures in each of the participants. The results regarding the clinical significance of the changes after the intervention evaluated through standardized questionnaires revealed by the RCI are shown in Table 2.
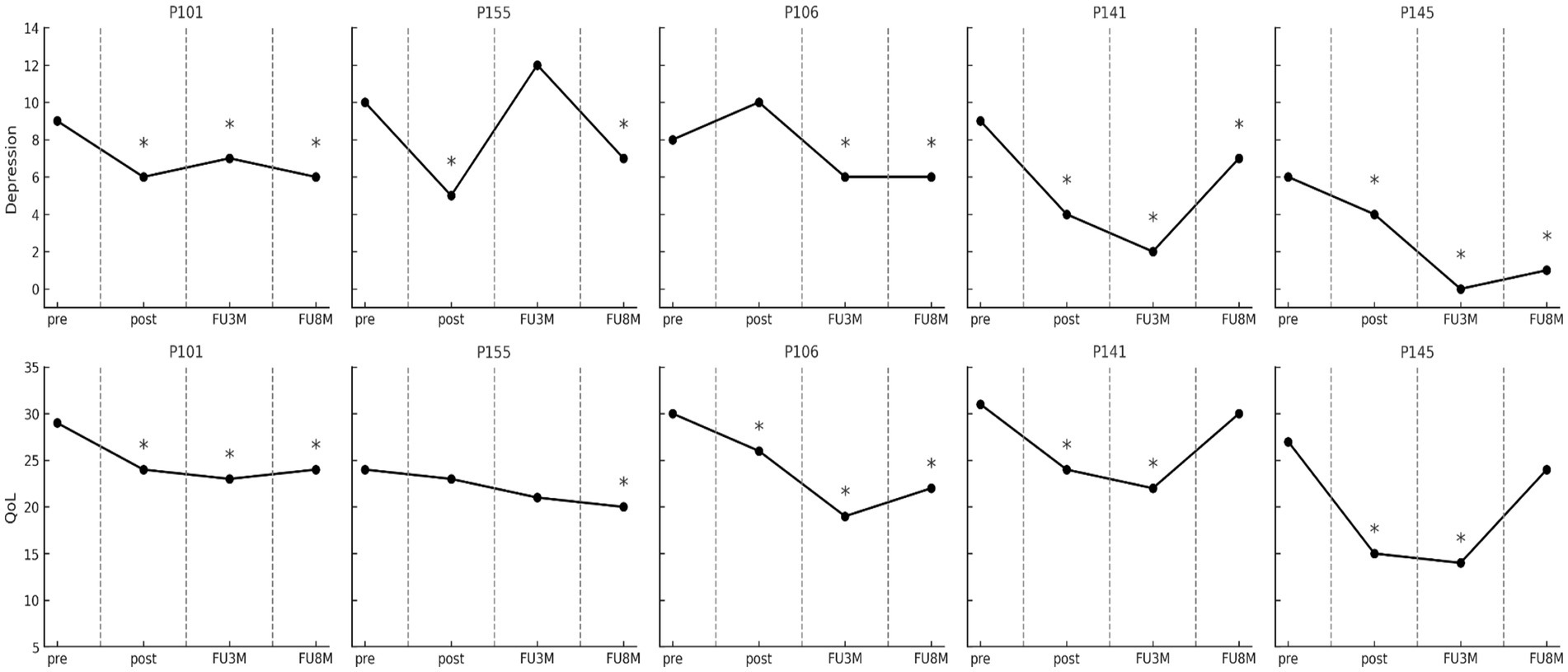
Figure 2. Evolution in depression and quality of life measures in every participant. Pre, pre-treatment; Post, post-treatment; FU3m, three-month follow-up; FU8m, 8-month follow-up. COOP-Wonca score reductions reflect QoL improvements. * indicates a clinically significant recovery according to criterion “A” of the Jacobson and Truax method (Jacobson and Truax, 1991).
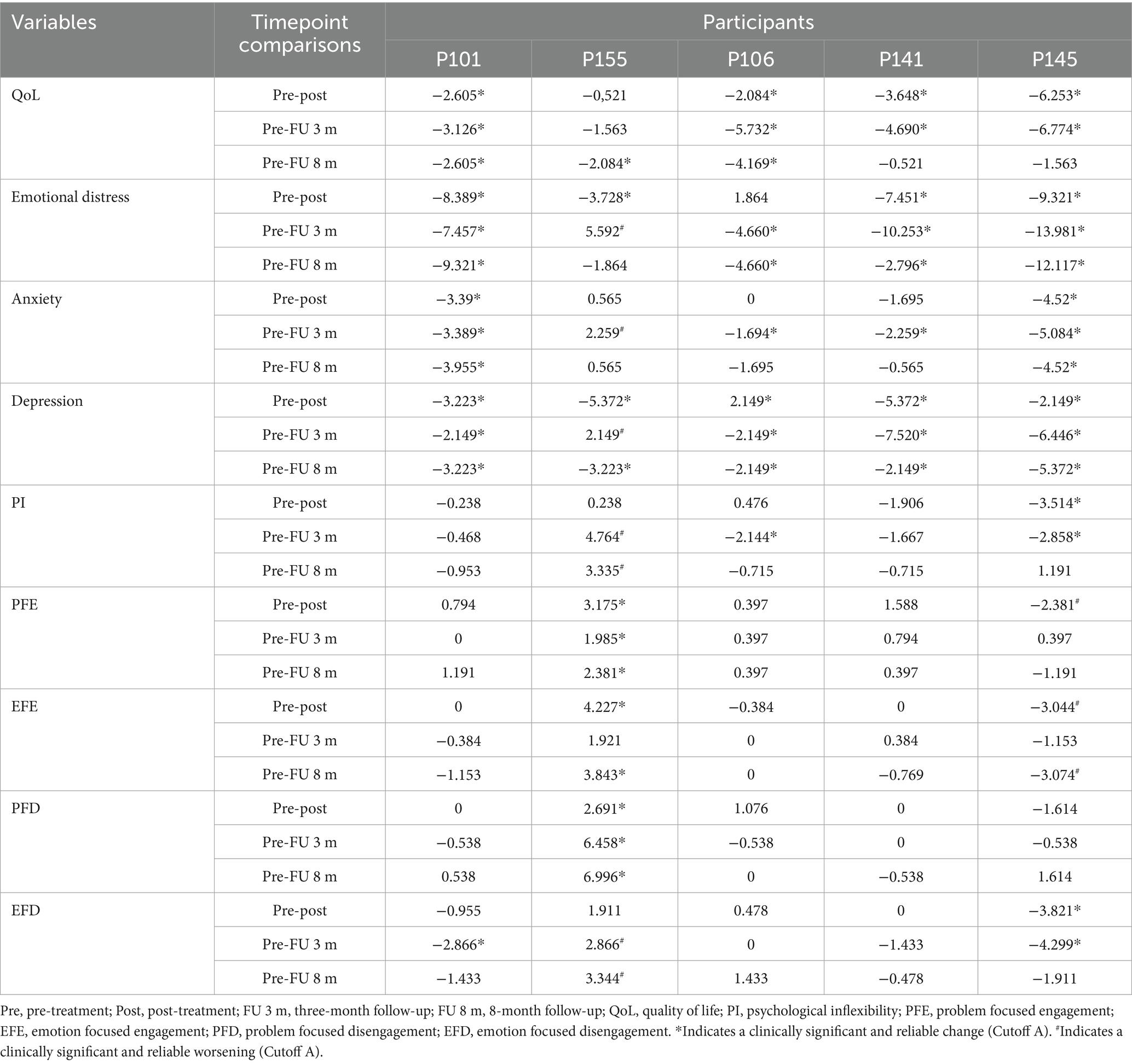
Table 2. Clinical significance of changes in measures through the reliable change index (RCI).
The QoL showed clinically significant improvement in four of the five patients both at the end of the intervention and at the three-month follow-up. Furthermore, three participants maintained this improvement at 8 months. The intervention was followed by a clinically significant decrease in depression levels in all patients at the end of the intervention. While these effects were maintained in four of them at the three-month follow-up, one of them (P155) worsened. However, all patients, including the one who worsened at 3 months, showed clinical recovery at 8 months.
Psychological treatment was followed by a reduction in overall anxiety levels. Two participants achieved clinically significant improvements at the end of the intervention, and this number increased to four at the three-month follow-up. However, one participant showed clinical worsening during this period. These improvements in anxiety were maintained at 8 months in two participants. Regarding emotional distress, which was considered one of the inclusion criteria, four participants showed clinically significant improvements at post-treatment, at three and 8 months. In this case, one of the participants who had improved (P155) worsened at the three-month follow-up and showed no change from pre-intervention levels at 8 months. However, the participant who did not show improvements at post-treatment (P106) did show improvements at both follow-ups.
Regarding IP, one participant improved after the intervention, two improved at 3 months, but one returned to pre-treatment levels. At 8 months, the changes were not maintained, and one participant worsened. For adaptive coping strategies related to engagement, one participant improved in PFE and one worsened after the intervention. At the three-and eight-month follow-ups, only one participant maintained recovery. In terms of EFE, one participant improved and one worsened after the intervention. There were no changes at 3 months, but at 8 months, one participant improved and one worsened. For maladaptive disengagement coping strategies, one participant improved in PFD after the intervention, maintaining the effects at 3 and 8 months. One participant showed recovery in EFD after the intervention, two at 3 months, but one worsened. At 8 months, one participant worsened.
3.3 Main changes reported by patients
All patients reported greater satisfaction with their health management, and four of them improved their satisfaction with family, friendship, and leisure activities. Regarding behavioral changes, all patients reported spending more time with family and friends after the intervention, and four of them increased their frequency of physical activity and improved their eating and fluid intake habits.
4 Discussion
This pilot study provides preliminary evidence for the feasibility and usefulness of a brief Acceptance and Commitment Therapy (ACT)-based protocol in patients with Chronic Kidney Disease (CKD) undergoing hemodialysis who present clinically significant depressive symptoms. Despite the inherent limitations of pilot studies, the findings offer a positive perspective on the intervention and pave the way for larger-scale research. In terms of acceptability and adherence, the results were exceptional. All patients completed the treatment protocol without dropping out of the study, and high levels of satisfaction with the intervention were reported. This is particularly relevant, as it demonstrates that dialysis patients—often perceived as having low willingness to engage in psychological interventions—can benefit from such therapies even in a clinically complex environment like the hemodialysis room. This high adherence may be related to the fact that the intervention was delivered within a setting already integrated into the patients’ routine, thus removing logistical barriers such as transportation or the stress associated with attending additional healthcare appointments to receive psychological treatment.
Regarding the clinical outcomes, a significant improvement in QoL and a reduction in depressive and anxiety symptoms were observed in the majority of patients, with these improvements maintained at the eight-month follow-up in a considerable proportion of the sample. This suggests that the ACT-based protocol may have sustainable effects, even in the absence of continuous therapeutic support. The decrease in emotional distress in four out of the five patients is another positive indicator, suggesting that the intervention may have been associated with improved emotional well-being, although causal conclusions cannot be drawn in the absence of a control group.
The fact that some patients, such as P155, experienced a temporary worsening of depression and anxiety at the three-month follow-up, followed by an improvement at 8 months, reflects a possible intermediate relapse that may be common in patients with chronic illnesses. The patient’s lack of short-term response to treatment may have been hypothetically attributed to challenges within his family context. During the week of the second follow-up, he disclosed having received distressing news regarding his mother’s health. He reported experiencing considerable emotional turmoil, including sadness and frustration, stemming from his inability to travel to his home country to visit her. In any case, this also suggests that, while the intervention may have contributed to recovery, the process of emotional adaptation to a chronic illness like CKD can be non-linear, with ups and downs over time and highly influenced by the patients’ personal context, due to their special vulnerability. This pattern could be interpreted as a reminder that emotional management in patients with chronic illnesses often requires ongoing interventions and adjustments over time.
Improving QoL, rather than symptom reduction, is considered the overall aim of ACT and its improvement after ACT administration is in line with the evidence found in previous studies in a wide range of chronic health conditions (Konstantinou et al., 2023) and CKD patients (Kalbasi et al., 2021; Rouhi et al., 2023), and may be related to the fact that the intervention is focused on improving functioning and not so much on alleviating discomfort. Likewise, the results are in line with previous studies that have shown a reduction in depression in chronically ill patients (Konstantinou et al., 2023) and CKD patients (Azemi Zeynal et al., 2016). A desirable and noteworthy outcome is the sustained improvement over time (Hoffmann et al., 2018), which could be a consequence of the continued practice of the acquired skills. This is an encouraging result that suggests the potential usefulness of the intervention; however, caution is warranted due to the absence of a control group and the small sample size.
Changes in both QoL and depression may be related to the fact that therapy motivates patients to take action and introduce changes in their daily lives (Konstantinou et al., 2023). Since the goal of ACT is not to reduce distress or depressive mood, but rather to ensure that the patient remains active regardless of mood fluctuations (Hayes et al., 2012), the reduction of depressive symptoms is not a primary goal of therapy, although such reduction may be an effect of newly acquired skills. Thus, the goal of accepting CKD and living with the disease becomes equivalent to acting to actively and continuously cultivate the different valued facets and, in particular, to addressing the risk of abandoning facets related to leisure, interpersonal relationships, and health or self-care, whether or not the discouragement or worry associated with CKD is present. In this sense, it is possible that, although no direct changes in PI or coping strategies were observed, the intervention may have contributed to patients learning to continue behaving actively, which could have led to the observed improvements in QoL and reduction in depressive symptoms. The focus for adapting to the chronic illness condition would be on improving functioning and maintaining balance among important life domains. This goal could have been achieved by systematically defining committed actions and inviting patients to implement these commitments between sessions, specifying details such as the day, place, or people with whom they would carry out the actions.
A notable and innovative aspect of this study is the fact that patients received psychological treatment during hemodialysis. This context for administering the psychological intervention represents a considerable advantage that may have contributed to the excellent adherence, as travel did not represent additional stress for patients already burdened by significant treatment-related burdens. Similarly, administering an ACT-based intervention in a setting where many triggers of distress are present (e.g., awareness of illness while undergoing hemodialysis, feelings of lack of freedom associated with the time spent on hemodialysis, low blood pressure, witnessing health crises in other patients, learning about colleagues whose health is deteriorating or who have died, etc.) may have provided valuable opportunities for emotional exposure and the practice of emotion regulation skills. However, further research is needed to evaluate the usefulness of ACT in managing the impact of these contextual factors. Even so, it was a significant challenge for the therapist to operate in the presence of a multitude of noises from the dialysis machines and interference related to medical procedures and the work of other professionals sharing the space, although the therapeutic benefits outweighed the discomfort this situation caused for the therapist. This characteristic, along with the abbreviated format of the intervention, represented considerable advantages of the intervention studied.
4.1 Limitations
The small number of participants, mostly middle-aged men, prevents the results from being generalized to the CKD patient population. The measures used were exclusively self-report, which may lead to biases related to social desirability, subjectivity, or difficulties in detecting or remembering changes. It would be desirable in future studies to complement the self-report measures with objective measures related to behavioral changes, for example, collected through self-monitoring or external observers, as well as other medical indicators.
Given that a number of patients declined to participate in the study, it can be assumed that those who agreed were those who showed greater motivation to receive psychological support, and the sample selection may have shown this bias toward patients with a particular motivation for treatment. This sample selection bias could be reduced by conducting studies with larger samples that included patients with different levels of motivation.
Future research exploring effects of ACT on CKD should include more controlled studies with larger samples. In any case, given the complexity and vulnerability of this patient population, small-N feasibility studies represent a necessary preliminary step before progressing to controlled trials. This approach aligns with prior and ongoing ACT-based pilot studies conducted in clinical populations facing comparable challenges (Hoffmann et al., 2018; Meuret et al., 2012; Martin et al., 2016). Although the limited sample size in the present study precludes generalizability, the observed improvements suggest that brief ACT interventions may represent a promising strategy for reducing depression in this population. These findings, while preliminary, should be interpreted with caution. Nevertheless, they provide a valuable foundation for the design of a fully powered randomized controlled trial to evaluate the intervention’s efficacy under more stringent conditions. This pilot study supports the rationale for our team to initiate such a trial. Randomized controlled trials might compare the effectiveness of ACT versus CBT, face-to-face versus online delivery of ACT, and individual versus group-based ACT formats. Future studies could also explore the impact of psychological interventions on medical therapeutic adherence and CKD symptoms and CKD symptoms. Health psychologists could use this information to plan, improve and implement additional interventions. Specifically, we strongly recommend exploring the usefulness of an intensive ACT-based approach in predialysis preventive interventions to promote patient adherence and well-being before initiating a treatment as demanding as renal replacement therapy. We must not forget that by striving to improve adherence and well-being in kidney patients, we facilitate a more rational use of resources.
In summary, despite the small number of participants, this contribution strengthens person-centered care (Morton and Sellars, 2019), lays the groundwork for expanding the range of available psychotherapeutic approaches, and enhances the interdisciplinary management of CKD. It represents a new way of understanding the design and delivery of services for people with kidney disease that focuses on functioning rather than emotional symptoms and can be administered in the dialysis room, representing a shift from the way nephrology services have historically been designed. This study highlights the importance of implementing a person-centered approach to renal patients undergoing hemodialysis. It is essential to recognize that the technical skills required to resolve issues such as a central venous catheter are equally important as the competencies needed to address the emotional distress of patients. We should not forget that skills for unblocking a problem with a central venous catheter are just as important as those for unblocking the emotional state of a distressed patient. Ultimately, the implementation of an ACT-based psychological intervention during hemodialysis for patients experiencing depression related to kidney disease appears to be a potentially valuable therapeutic approach. However, determining its effectiveness warrants further investigation under more rigorous experimental conditions.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study involving humans was approved by Comité de Ética de la Investigación de la Fundación Jiménez Díaz (Madrid, Spain). The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SD: Conceptualization, Data curation, Investigation, Methodology, Writing – review & editing, Writing – original draft, Formal analysis. HG-L: Writing – review & editing, Conceptualization, Investigation. DL: Writing – review & editing, Formal analysis, Methodology, Software, Investigation. MM: Conceptualization, Investigation, Writing – review & editing, Data curation, Resources. MA: Funding acquisition, Writing – review & editing, Conceptualization, Investigation, Resources. FD: Writing – review & editing, Conceptualization, Investigation, Resources, Funding acquisition. FM: Conceptualization, Investigation, Supervision, Writing – review & editing, Visualization, Funding acquisition, Resources, Validation, Formal analysis, Writing – original draft, Project administration.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was conducted with funding from Fundación Renal Española, within the framework of a research agreement between Universidad Europea de Madrid, Fundación Renal Española, and Fundación Universitaria Fray Francisco Jiménez de Cisneros.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Aránega-Gavilán, S., Guillén-Gómez, I., Blanco-García, M., and Crespo-Montero, R. (2022). Aspectos psicosociales del paciente en diálisis. Una revisión bibliográfica. Enferm. Nefrol. 25, 216–227. doi: 10.37551/52254-28842022022
Arenas, M. D., Moreno, E., Reig, A., Millán, I., Egea, J. J., Amoedo, M. L., et al. (2004). Evaluation of health-related quality of life (HRQL) based on information from Coop/Wonca sheets in hemodialysis patients. Nefrologia 24, 470–479.
Arnout, B. I. (2019). The effectiveness of a brief program based on the acceptance and commitment therapy to increase psychological well-being in a sample of patients with renal failure. Majallat Ulūm Tarbawīyah wa al-Nafsīyah. 3, 158–141. doi: 10.26389/AJSRP.B071118
Azemi Zeynal, A., Ghaffari, A., and Sharghi, A. (2016). The effectiveness of acceptance and commitment therapy based on depression, mental health, and physical health in hemodialysis patients. J. Fundam. Ment. Health. 18, 412–418. doi: 10.22038/jfmh.2016.7859
Castillo, I. I. (2010). Evaluación de resultados clínicos (y III): índices de cambio fiable (ICF) como estimadores del cambio clínicamente significativo. Norte Salud Ment. 8, 105–122.
Ćwiek, A., Czok, M., Kurczab, B., Kramarczyk, K., Drzyzga, K., and Kucia, K. (2017). Association between depression and hemodialysis in patients with chronic kidney disease. Psychiatr. Danub. 29, 499–503.
Domínguez, C. J. D., García, J. V., Ruiz, F. J., Delgado Domínguez, C. J., Espejo, B. D., Guerrero, P. C., et al. (2020). Psychological inflexibility and clinical impact: adaptation of the acceptance and action questionnaire-II in a sample of patients on haemodialysis treatment. Nefrología 40, 160–170. doi: 10.1016/j.nefroe.2019.06.006
Drayer, R. A., Piraino, B., Reynolds, C. F. III, Houck, P. R., Mazumdar, S., Bernardini, J., et al. (2006). Characteristics of depression in hemodialysis patients: symptoms, quality of life and mortality risk. Gen. Hosp. Psychiatry 28, 306–312. doi: 10.1016/j.genhosppsych.2006.03.008
Elander, J., Stalker, C., Arborg, M., Coyne, E., Kapadi, R., Taal, M. W., et al. (2023). Living well on haemodialysis: feasibility and acceptability trial of an online acceptance and commitment therapy (ACT) programme for people receiving kidney haemodialysis. J. Context. Behav. Sci. 30, 41–49. doi: 10.1016/j.jcbs.2023.08.008
Erbay, E., Arslan, K., Hatipoğlu, E., and Yildirim, T. (2021). The quality of life, depression levels and coping styles of patients on kidney transplant waiting list. Soc. Work Public Health 36, 432–447. doi: 10.1080/19371918.2021.1903645
Feliu-Soler, A., Montesinos, F., Gutiérrez-Martínez, O., Scott, W., McCracken, L. M., and Luciano, J. V. (2018). Current status of acceptance and commitment therapy for chronic pain: a narrative review. J. Pain Res. 11, 2145–2159. doi: 10.2147/JPR.S144631
García-Llana, H., Remor, E., Peso, G. D., and Selgas, R. (2014). El papel de la depresión, la ansiedad, el estrés y la adhesión al tratamiento en la calidad de vida relacionada con la salud en pacientes en diálisis: revisión sistemática de la literatura. Nefrologia 34, 637–657. doi: 10.3265/Nefrologia.pre2014.Jun.11959
Gloster, A. T., Walder, N., Levin, M. E., Twohig, M. P., and Karekla, M. (2020). The empirical status of acceptance and commitment therapy: a review of meta-analyses. J. Contextual Behav. Sci. 18, 181–192. doi: 10.1016/j.jcbs.2020.09.009
Gorostidi, M., Sánchez-Martínez, M., Ruilope, L. M., Graciani, A., de la Cruz, J. J., Santamaría, R., et al. (2018). Prevalencia de enfermedad renal crónica en España: impacto de la acumulación de factores de riesgo cardiovascular. Nefrologia 38, 606–615. doi: 10.1016/j.nefro.2018.04.004
Hayes, S. C. (2016). Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies–republished article. Behav. Ther. 47, 869–885. doi: 10.1016/j.beth.2016.11.006
Hayes, S. C., Strosahl, K., and Wilson, K. G. (2012). Acceptance and commitment therapy: the processes and practice of mindful change. 2nd Edn. New York: The Guilford Press.
Heilman, R. L., Green, E. P., Reddy, K. S., Moss, A., and Kaplan, B. (2017). Potential impact of risk and loss aversion on the process of accepting kidneys for transplantation. Transplantation 101, 1514–1517. doi: 10.1097/TP.0000000000001715
Herrero, M. J., Blanch, J., Peri, J. M., de Pablo, J., Pintor, L., and Bulbena, A. (2003). A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen. Hosp. Psychiatry 25, 277–283. doi: 10.1016/S0163-8343(03)00043-4
Hoffmann, D., Rask, C. U., Hedman-Lagerlöf, E., Ljótsson, B., and Frostholm, L. (2018). Development and feasibility testing of internet-delivered acceptance and commitment therapy for severe health anxiety: pilot study. JMIR mental health. 5:e28. doi: 10.2196/mental.9198
Jacobson, N. S., and Truax, P. (1991). Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. J Consult Clin Psychol 59, 12–19. doi: 10.1037/10109-042
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. New York: Delta Book.
Kalbasi, R., Hatami, M., Seyrafi, M., Hakemi, M. A., and Sabet, M. (2021). The effectiveness of acceptance and commitment therapy in quality of life and blood pressure index of hemodialysis patients. EBNESINA 23, 25–34.
Karimi, S., Moradimanesh, F., Asgari, P., and Bakhtiyarpour, S. (2019). The effectiveness of acceptance and commitment therapy on the illness perception in Dialysis patients. J Pharm Res Int. 30, 1–8. doi: 10.9734/jpri/2019/v30i130260
Kashdan, T. B., and Rottenberg, J. (2010). Psychological flexibility as a fundamental aspect of health. Clin. Psychol. Rev. 30, 865–878. doi: 10.1016/j.cpr.2010.03.001
Kazemi Daluee, A., and Samari, A. (2021). Effectiveness of ACT with and without mindfulness plus exercises on spiritual health in hemodialysis. Health Spiritual. Med. Ethics. 8, 171–180. doi: 10.32598/hsmej.8.3.6
Kim, E. S. (2018). Development and effect of a rational-emotive-behaviour-therapy-based self-management programme for early renal dialysis patients. J. Clin. Nurs. 27, 4179–4191. doi: 10.1111/jocn.14608
Konstantinou, P., Ioannou, M., Melanthiou, D., Georgiou, K., Almas, I., Gloster, A. T., et al. (2023). The impact of acceptance and commitment therapy (ACT) on quality of life and symptom improvement among chronic health conditions: a systematic review and meta-analysis. J. Context. Behav. Sci. 29, 240–253. doi: 10.1016/j.jcbs.2023.08.004
Marín, M. T., Rodríguez-Rey, R., Montesinos, F., Rodríguez, S., Ágreda-Ladrón, M. R., and Hidalgo, E. (2022). Factores asociados a la calidad de vida y su predicción en pacientes renales en hemodiálisis. Nefrologia 42, 318–326. doi: 10.1016/j.nefro.2021.03.010
Martín, A. L., and Lorenzo, V. (2024). “Enfermedad renal crónica” in Nefrología al día. eds. V. Lorenzo and J. M. López. (Madrid: Grupo Editorial Sociedad Española de Nefrología).
Martin, S., Wolters, P. L., Toledo-Tamula, M. A., Schmitt, S. N., Baldwin, A., Starosta, A., et al. (2016). Acceptance and commitment therapy in youth with neurofibromatosis type 1 (NF1) and chronic pain and their parents: a pilot study of feasibility and preliminary efficacy. Am. J. Med. Genet. A 170, 1462–1470. doi: 10.1002/ajmg.a.37623
Meuret, A. E., Twohig, M. P., Rosenfield, D., Hayes, S. C., and Craske, M. G. (2012). Brief acceptance and commitment therapy and exposure for panic disorder: a pilot study. Cogn. Behav. Pract. 19, 606–618. doi: 10.1016/j.cbpra.2012.05.004
Morton, R. L., and Sellars, M. (2019). From patient-centered to person-centered Care for Kidney Diseases. Clin. J. Am. Soc. Nephrol. 14, 623–625. doi: 10.2215/CJN.10380818
Nozaki, C., Oka, M., and Chaboyer, W. (2005). The effects of a cognitive behavioural therapy programme for self-care on haemodialysis patients. Int. J. Nurs. Pract. 11, 228–236. doi: 10.1111/j.1440-172X.2005.00525.x
Othman, A. A., Wan Jaafar, W. M., Zainuddin, Z. N., and Yusop, M. Y. (2020). Effectiveness of cognitive behaviour therapy on depression among haemodialysis patients: a systematic review of literature. Cogent Psychol. 7:1794680. doi: 10.1080/23311908.2020.1794680
Palmer, S., Vecchio, M., Craig, J. C., Tonelli, M., Johnson, D. W., Nicolucci, A., et al. (2013). Prevalence of depression in chronic kidney disease: systematic review and meta-analysis of observational studies. Kidney Int. 84, 179–191. doi: 10.1038/ki.2013.77
Payne, M. E., Eaton, C. K., Mee, L. L., and Blount, R. L. (2013). Promoting medication adherence and regimen responsibility in two adolescents on hemodialysis for end-stage renal disease: a case study. Clin. Case Stud. 12, 95–110. doi: 10.1177/1534650112467079
Preljevic, V. T., Østhus, T. B. H., Sandvik, L., Opjordsmoen, S., Nordhus, I. H., Os, I., et al. (2012). Screening for anxiety and depression in dialysis patients: comparison of the hospital anxiety and depression scale and the Beck depression inventory. J. Psychosom. Res. 73, 139–144. doi: 10.1016/j.jpsychores.2012.04.015
Rouhi, M., Manzari Tavakoli, A., and Tajrobehkar, M. (2023). Comparing the effectiveness of acceptance and commitment therapy and dialectical behavioral therapy on coherent self-knowledge, emotional regulation, and life quality of hemodialysis patients. Shenakht J. Psychol. Psychiatry 10, 131–146. doi: 10.32598/shenakht.10.2.131
Ruiz, F. J., Flórez, C. L., García-Martín, M. B., Monroy-Cifuentes, A., Barreto-Montero, K., García-Beltrán, D. M., et al. (2018). A multiple-baseline evaluation of a brief acceptance and commitment therapy protocol focused on repetitive negative thinking for moderate emotional disorders. J. Contextual Behav. Sci. 9, 1–14. doi: 10.1016/j.jcbs.2018.04.004
Rzeszut, M. E. (2011). The application of acceptance and commitment therapy with hemodialysis treatment adherence: a case study. J. Nephrol. Soc. Work. 35, 17–25.
Sadeghi, A. H., Ahmadi, S. A., and Ghodrati-Torbati, A. (2024). The effectiveness of acceptance and commitment therapy on clinical symptoms and treatment adherence in dialysis patients. J. Educ. Health Promot. 13:28. doi: 10.4103/jehp.jehp_1704_22
Sarizadeh, M., Rafieinia, P., Sabahi, P., and Tamaddon, M. (2019). Effectiveness of acceptance and commitment therapy on subjective well-being among hemodialysis patients: a randomized clinical trial study. Koomesh 21:e153038.
Shery, S. P., Col, A. R., and Manjunath, J. (2019). A study on quality of life in haemodialysis patients. Int. J. Sci. Res. 8, 48–52.
Sociedad Española de Nefrología (2022). La Enfermedad Renal Crónica (ERC) en España. Available online at: https://www.nefrologiaaldia.org (Accessed June 1, 2025).
Tajbakhsh, R., Haddadi, S., Zeighami Mohammadi, S., Malihi Alzakerini, S., and Borumand, M. (2023). Comparison of the effect of acceptance and commitment therapy and metacognitive therapy on the resilience of women undergoing hemodialysis. J. Health Promot. Manag. 12, 82–94. doi: 10.22034/JHPM.12.3.82
Tous-Pallarés, J., Espinoza-Díaz, I. M., Lucas-Mangas, S., Valdivieso-León, L., and Gómez-Romero, M. R. (2022). CSI-SF: propiedades psicométricas de la versión española del inventario breve de estrategias de afrontamiento. An. Psicol. 38, 85–92. doi: 10.6018/analesps.478671
Vázquez-Martínez, V. H., Ortega-Padrón, M., and Cervantes-Vázquez, D. A. (2016). Factores asociados a la depresión en pacientes bajo tratamiento con hemodiálisis. Atenc. Fam. 23, 29–33. doi: 10.1016/S1405-8871(16)30074-8
Weiner, S., Kutner, N. G., Bowles, T., and Johnstone, S. (2010). Improving psychosocial health in hemodialysis patients after a disaster. Soc. Work Health Care 49, 513–525. doi: 10.1080/00981380903212107
Williams, A. C., Fisher, E., Hearn, L., and Eccleston, C. (2020). Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst. Rev. 2021:CD007407. doi: 10.1002/14651858.CD007407.pub4
Wilson, M. C., and Luciano, K. G. (2002). Terapia de aceptación y compromiso (ACT). Un tratamiento conductual orientado a los valores. Madrid: Pirámide.
Yang, B., Xu, J., Xue, Q., Wei, T., Xu, J., Ye, C., et al. (2015). Non-pharmacological interventions for improving sleep quality in patients on dialysis: systematic review and meta-analysis. Sleep Med. Rev. 23, 68–82. doi: 10.1016/j.smrv.2014.11.005
Zhao, C., Lai, L., Zhang, L., Cai, Z., Ren, Z., Shi, C., et al. (2021). The effects of acceptance and commitment therapy on the psychological and physical outcomes among cancer patients: a meta-analysis with trial sequential analysis. J. Psychosom. Res. 140:110304. doi: 10.1016/j.jpsychores.2020.110304
Keywords: acceptance and commitment therapy, chronic kidney disease, health psychology, hemodialysis, depression
Citation: Diéguez S, García-Llana H, Lobato D, Marín MT, Arenas MD, Dapena F and Montesinos F (2025) Acceptance and commitment therapy for depression in chronic kidney patients: a pilot study. Front. Psychol. 16:1656929. doi: 10.3389/fpsyg.2025.1656929
Edited by:
Federica Mauro, Sapienza University of Rome, ItalyReviewed by:
Amjad Oraibi, Al-Manara College for Medical Sciences, IraqKhairul Anwar Mastor, Islamic Science University of Malaysia, Malaysia
Copyright © 2025 Diéguez, García-Llana, Lobato, Marín, Arenas, Dapena and Montesinos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sonia Diéguez, c2RpZWd1ZXpAY2VzY2lzbmVyb3MuZXM=; Francisco Montesinos, ZnJhbmNpc2NvLm1vbnRlc2lub3NAdW5pdmVyc2lkYWRldXJvcGVhLmVz