 Alejandro González-González1
Alejandro González-González1 Patricia Andrade Palos2
Patricia Andrade Palos2 Rosa Estela García-Chanes1,3
Rosa Estela García-Chanes1,3 María Enriqueta Sánchez Hernández1
María Enriqueta Sánchez Hernández1 Diana Betancourt Ocampo1*
Diana Betancourt Ocampo1*- 1Faculty of Psychology, Universidad Anáhuac México, Mexico City, Mexico
- 2Faculty of Psychology, Universidad Nacional Autónoma de México, Mexico City, Mexico
- 3Research Department, Instituto Nacional de Geriatría, Mexico City, Mexico
Objective: This study analyzed the effect of spirituality and religiosity on subjective wellbeing in Mexican older adults, controlling some sociodemographic variables (e.g., sex, age, schooling, who they live with, monthly income) and health variables (e.g., health perception, difficulties in carrying out activities, presence of medical conditions, depression).
Methods: A non-probabilistic sample of 923 older adults (
Results: The results showed that spirituality and living with a partner have positive and significant effects on subjective wellbeing, while depression and difficulties in performing activities of daily living reduce it, this regression model explained 17% of the variability in subjective wellbeing.
Conclusion: In the present study, it was observed that in each of the models tested, spirituality played an important role as a predictor of subjective wellbeing, and even remained stable when demographic (sex, age, schooling, who they live with) and health (health perception, difficulties in carrying out activities, depression) variables were included.
1 Introduction
One of the fundamental premises in all countries is being able to guarantee a healthy life and promote the wellbeing of all people, regardless of their condition or age, which will contribute to the construction of prosperous and healthy societies, so it is important to consider what the outlook is in relation to population changes, in particular, with the increase in the number of older adults (OA) and their needs, projections for 2050 indicate that one out of every six people in the world will be over 65 years of age (United Nations, 2022), which represents an increase from 10% in 2022 to 16% in 2050.
In Mexico, as in other countries around the world, there is an accelerated increase in the number and proportion of OA. By 2030, one in six people worldwide is expected to be 60 years of age or older and it is expected that by 2050 this proportion will double, which represents one of the greatest challenges in terms of public health and the social conditions in which these OA will live (Organización Mundial de la Salud, 2025). In addition, the way in which people are aging is not observed in the best conditions, considering the prevalence of chronic diseases, diet and lifestyle habits, as well as persistent social and gender inequalities. In this regard, the Inter-American Development Bank indicates that chronic diseases are highly prevalent among OA in Latin America and increase with age, as well as being a major cause of mortality and morbidity (Aranco et al., 2022). According to data provided by Mexican Health and Aging Study (MHAS) 2021, 22.7% have diabetes, 38.5% have hypertension and 54.6% report having a regular state of health; in relation to their mental health and emotional wellbeing, 59.4% indicated that they have a bad to regular quality of memory, while 25.3% had depressive symptoms. Although these data reflect some problems, their evaluation of life satisfaction is high, since nine out of 10 OA reported being satisfied (Instituto Nacional de Estadística y Geografía, 2021).
Other studies (García-Chanes et al., 2024; López-Ortega et al., 2016) show that the psychosocial wellbeing of Mexican adults is associated with a positive perception of the economic situation, the absence of depressive symptoms, and social participation rather than with the presence of comorbidity. In this same vein, studies in Mexico (Instituto Nacional de Estadística y Geografía, 2021) indicate that among the older adult population, men have higher life satisfaction scores than women. Reyna-Barajas et al. (2025) found that older adult men report a better quality of life in terms of physical performance and perception of wellbeing, while women have a higher prevalence of chronic diseases. In addition, the authors point out that men and women may experience aging differently due to biological, psychological, social, and cultural factors, which can directly affect quality of life in old age.
Globally, the World Health Organization (Organización Mundial de la Salud, 2022) proposed the Healthy Ageing framework that focuses on developing and maintaining functional ability in older people, understood as the basis for achieving wellbeing in later life. In context, the Decade of Healthy Ageing 2020–2030 is an initiative aimed at improving the lives of older people, their families and communities and promoting healthy aging. To achieve this, collaboration between governments, civil society, international organizations, academia, the media and the private sector is encouraged.
In particular, subjective wellbeing (SW) refers to the evaluation that people make of their own wellbeing and is part of people’s quality of life. It arises from the importance of considering not only economic and social aspects to define people’s quality of life, since people react differently to the same circumstances and evaluate their conditions based on their expectations, values and experiences (Diener, 1984; Diener and Suh, 1997; Diener et al., 1999). SW is conceptualized as hedonic wellbeing because it emphasizes pleasure and satisfaction (Tov et al., 2022) and contemplates two dimensions: the cognitive one that is generated through satisfaction with oneself, family and society, and the affective one that focuses more on affections, emotions, feelings and positive and negative moods (Diener, 1984; Arévalo-Avecillas et al., 2019; Flores-Kanter et al., 2018).
Triyuliasari et al. (2024) made a systematic review of research that analyzes different factors that influence the SW of OA and conclude that there is empirical evidence that sociodemographic aspects (educational, marital and economic status), social activities (voluntary activities, religious), physiological (health and sleep quality) and psychological factors (family support, spirituality and religiosity, self-efficacy, internet use) all have an impact on the SW of OA. Regarding sociodemographic variables such as gender, age and economic income, the results are not consistent and perhaps this is due to the different measures of quality of life and wellbeing (Batz and Tay, 2018; Gobbens and Remmen, 2019; Lansford, 2018), it seems that life experiences and decisions play a more important role, as well as environmental variables.
In terms of health-related variables, it has been shown that physical health is positively related to SW (Cross et al., 2018), and in the case of OA, an important aspect is independence and autonomy, so maintaining the ability to perform daily activities and make personal decisions that are linked to greater satisfaction and wellbeing with life are fundamental in their personal situation (Jitdorn et al., 2021; Ladusingh and Ngangbam, 2016). However, given that physical health declines with age, one might expect SW to decline, but scientific evidence points to higher SW at older ages, suggesting that changes related to family, work, social networks, and physical capacity associated with aging individuals should rather be studied (Stone et al., 2020).
Some aspects of mental health related to SW and life satisfaction have also been studied (Hashmi et al., 2018; Lombardo et al., 2018; Ngamaba et al., 2017), but some measures of mental health have been done through self-reports, which consistently correlate; however, the relationship diminishes when objective measures are included (Diener et al., 2018). Depression is one of the most studied variables and has been found to decrease the SW of OA (Li et al., 2023; Lukaschek et al., 2017; Soósová et al., 2021).
Among the factors that some authors have found as part of the wellbeing of OA is religiosity and spirituality, referring to the fact that the practices of meditation, orientation, prayers and church events generate certain feelings of satisfaction, self-improvement and security that lead them to become stronger, in addition to providing them with a sense of life (Gallardo-Peralta and Sánchez-Moreno, 2020; Zapata, 2017). The experience of religiosity and spirituality can be shared collectively, but it is recognized that these experiences are unique and unrepeatable for each person who lives them, and particularly in the case of OA (Casanova et al., 2024; Guerrero-Castañeda et al., 2021; Tabatabaei and Ebrahimi, 2023; Watkins et al., 2022). Unlike religiosity, spirituality does not deny or affirm a divine origin, but refers to a search for meaning in life, which may or may not be related to belief in God or other equivalent cultural dimensions (De Freitas et al., 2022).
Dominguez et al. (2024) analyzed the evidence of the relationship between spirituality/religiosity with longevity and concluded that numerous epidemiological studies show that high levels of spirituality/religiosity in its different forms are associated with lower mortality rates. Likewise, Malone and Dadswell (2018) and Papadopoulos (2020) note the importance of religion and spirituality in positive aging as they can be a source of strength, comfort, and hope, as well as being a sense of community and belonging. Litalien et al. (2022) concluded that religiosity/spirituality have influence on healthy behaviors and wellbeing, but more studies by sex are needed.
Zimmer et al. (2016) indicate that although there is evidence that spirituality/religiosity is associated with long life and greater physical and mental health, the two constructs need to be investigated separately. While the two concepts are related and most people who consider themselves religious also consider themselves spiritual, not all people who are spiritual consider themselves religious. Religion is generally associated with beliefs, practices, and rituals, whereas spirituality is more difficult to define, as it means different things to different individuals in different places. The authors point out that it is easier to quantify religiosity than spirituality and some studies show that spirituality has greater weight than religiosity in the SW of OA (Gallardo-Peralta and Sánchez-Moreno, 2020; Saldías-Ortega and Moyano-Díaz, 2023).
Büssing (2018) did a systematic review of instruments measuring spirituality/religiosity in clinical settings and proposes like Zimmer et al. (2016) that they are two related constructs but with different definitions, so they should be measured as two independent constructs. He further notes that religiosity has generally been measured as adherence to beliefs, doctrines, ethics, rituals, texts, and practices associated with high power and spirituality is defined as a set of internal feelings and experiences through which a person seeks meaning and purpose, as well as relationship to self, family, society, nature, and the meaning of the sacred. Spirituality is something more subjective and different aspects of spirituality have been measured, such as levels of spirituality, spiritual wellbeing, spiritual distress, spiritual needs. In terms of religiosity, religious beliefs and practices and level of religiosity are generally measured.
Regarding religiosity, the findings indicate that it has a positive influence on the wellbeing of OA because its practices offer better ways of coping with the challenges of this stage, as well as preparing them to fulfill their life mission, although this is often uncertain (Coelho-Júnior et al., 2022; Soriano et al., 2021). In addition to this, it has been found that active involvement in a religious community, either by praying or doing work dedicated to others, generates greater feelings of belonging and usefulness; specifically in women, religiosity allows them to live together at a time when most of their time is spent at home (Tabatabaei and Ebrahimi, 2023; Vicente et al., 2018). Some studies show that maintaining social interactions, which occur through religious practices, contribute significantly to their sense of belonging and life satisfaction, which results in their overall wellbeing (Jitdorn et al., 2021; Cramm and Nieboer, 2015; Dorji et al., 2019; Du et al., 2023; Paul et al., 2024).
On the other hand, it has been found that spirituality has a positive influence on OA (Soósová et al., 2021) since it helps them to achieve a greater connection with themselves and with others, as well as allowing them to have a positive attitude towards the changes and stress that come with grief and challenging situations that they go through during this stage (Can Oz et al., 2022). Spirituality has also been considered a protective factor for OA as it helps them cope with physical, psychological and social changes, in addition to providing them with security, stability and meaning in their lives (Pérez et al., 2022). Neville et al. (2024) found that higher spirituality, independent of religiosity, was independently associated with good self-rated health in geriatric outpatients. Being able to enhance spirituality seems to represent one of the relevant intervention strategies in the prevention and treatment of depressive symptoms and improvement of wellbeing in OA (Soósová et al., 2021).
In general, religious practices and spirituality have been considered an important resource in OA, as they help them cope with stress and in several studies are associated with less depression and anxiety and greater hope. Religious/spiritual involvement has even been shown to be a powerful resource for psychiatric patients, as it is related to mental (Koenig and Al Zaben, 2021; Koenig et al., 2020) and physical health (Abu et al., 2018). However, in a review of studies on physical and mental health and religiosity/spirituality, Lucchetti et al. (2021) point out that the results are not conclusive, as some authors have not found significant relationships.
Hence, it is worthwhile to carry out studies with populations characterized by a series of unfavorable health conditions (for example, the presence of chronic diseases), as well as living conditions that represent some disadvantages to face aging (Aranco et al., 2022), and therefore it would be expected that their wellbeing would be affected. This is the case in Latin America, where OA live in conditions characterized by a series of structural deficiencies, including access to social and health services, which contributes to the transition through this stage of old age involving complications and obstacles that affect their perception of health and possibilities for improvement. In addition, a high percentage of OA continue to work and sometimes cannot count on a decent retirement, it is here where spirituality and religiosity would become relevant to contribute to a better wellbeing. All this would offer the possibility of incorporating these variables as promoters of wellbeing in contexts such as those experienced in Latin American countries where there are numerous disadvantages that imply a greater challenge for health and social care systems.
The aim of this study was to analyze the effect of spirituality and religiosity on SW in Mexican OA controlling for sociodemographic (e.g., sex, age, schooling, who they live with) and health (e.g., health perception, difficulties in carrying out activities, depression) variables. The central hypothesis of this research is that spirituality and religiosity are predictor variables of SW in OA independently of some sociodemographic and health characteristics.
2 Materials and methods
2.1 Participants
A non-probabilistic sample of OA residing in Mexico City was used, consisting of 923 OA between 60 and 100 years old (M = 74.49, SD = 7.46). The participants had some kind of contact with the Instituto para el Envejecimiento Digno (INED) in Mexico City, either because they attended spaces where they could regularly socialize with other OA, share experiences, and stay physically and mentally active. They could also be OA who were visited at home by staff from the institute to follow up on a particular need (e.g., physical, psychological, legal, etc.). It is important to note that the care provided by INED focuses mainly on older adults living in neighborhoods identified as having a low or very low Social Development Index.
2.2 Measures
2.2.1 Dependent variable
The Subjective Wellbeing Scale (EBS-8, acronym in Spanish) by Calleja and Mason (2020) was used, which measures life satisfaction (e.g., Likes his life, He is satisfied with his life) and positive affect (e.g., He is a happy person, Your life brings you joy), and consists of eight items in Likert-type format with four response options (from Disagree to Totally Agree), it is an instrument that was developed for the Mexican population and has been applied in adolescents, adults and OA, where it has shown empirical evidence of validity and reliability (α = 0.95).
2.2.2 Independent variables
The dimension of Religious Involvement was used, which is part of the main dimension of Religious Feelings of the Assessment Scale of Spirituality and Religious Feelings (ASPIRES) Scale, originally developed by Piedmont (2014) and validated in Spanish by Simkin (2017). The dimension used consists of eight items (α = 0.85) in a Likert-type format with 5–7 types of responses, and reflects how actively involved a person is in performing various religious rituals and activities (e.g., How often do you pray? How often do you attend mass or ceremonies specific to your religion?). It should be noted that this instrument does not have psychometric evidence in Mexico, which is why, as part of this study, its performance will be analyzed in the sample studied.
To evaluate spirituality, the dimension of importance of spiritual beliefs (α = 0.91) of the Spiritual Questionnaire by Parsian and Dunning (2009) was used, which consists of four items (e.g., Spirituality helps me define the goals I set in my life, Spirituality helps me decide who I am) in a Likert-type format with six responses ranging from never to always. The Spiritual Questionnaire did not report evidence of validity and reliability in the Mexican sample, which is why this study will analyze its performance in the sample studied. In addition, the scale adapted to the Mexican population (Salgado et al., 2024; Yesavage et al., 1983) of the Yesavage Geriatric Depression Scale (GDS) was used, consisting of 14 items (e.g., Do you feel happy most of the time? Have you dropped many of your activities and interests?) in dichotomous format (yes/no), which obtained adequate psychometric values in a sample of Mexican OA (α = 0.94).
A questionnaire with 16 closed-option questions was included based on items included in the Mexican Health and Aging Study (MHAS) 2021 (Instituto Nacional de Estadística y Geografía, 2022) and validated in the Mexican population, which evaluate: self-perception of health (excellent, very good, good, fair, or bad), the presence of medical conditions (e.g., diabetes, hypertension, arthritis) and, self-reported difficulty in performing activities of daily living (BAVD) was included using a dichotomous variable categorized as 0 (no difficulty) and ≥1 for difficulty in performing one or more of the following activities: walking, bathing, eating, lying down and using the toilet. In addition, a sociodemographic data questionnaire was included, asking for sex, age, education, marital status, who they lived with, current occupation and monthly income.
2.3 Procedure
The study was supported by the Secretaría de Bienestar e Igualdad Social of México City, through the Instituto para el Envejecimiento Digno (INED). Part of the work included a training process for the staff who participated in the study with the purpose of making them familiar with and learning how to improve the instruments that would be applied. After the training, the INED staff went to the home of each OA, where the objective and scope of the study was explained to them with the intention of obtaining their consent and voluntary participation. Likewise, they were informed that the information collected was confidential and would be used only as part of the research. The Mini-Cog (Borson et al., 2003) was applied to OA who initially agreed to participate, to confirm they had the cognitive capacity to answer the instruments. The criterion used was that if the older adult remembered two or three words, the rest of the instruments were applied in the form of an individual interview. The OA did not receive any incentive for participating in the study.
2.4 Data analysis
The analysis was conducted in the following sequential steps. First, a descriptive analysis was performed to examine the characteristics of the sample. Next, confirmatory factor analyses (CFA) were then performed for each of the scales used and the following values were considered as adequate fit indices (Hu and Bentler, 1999): the χ2/df ratio (CMIN/DF) with a value <3, the CFI (Comparative Fit Index) and TLI (Tucker–Lewis Index) indices with values >0.90; and RMSEA (Root Mean Square of Approximation) with a value <0.08. Reliability was calculated using Cronbach’s alpha. The means and standard deviations were calculated for the scales used.
Subsequently, the average scores of the SW scale were compared across various characteristics and health conditions using descriptive analysis. Depending on the type of variable, analysis of variance (ANOVA) tests and independent means tests were applied. Additionally, a correlation analysis was conducted to assess the strength and significance of the association between spirituality and SW scales and several quantitative covariates. These covariates included the dimension of religious involvement, age, self-reported health, depression scale and the number of basic activities affected (BAVD), with the Spearman test employed for this analysis.
To examine the role of spirituality in SW (dependent variable), three linear regression models were estimated. Model 0 focused solely on the effect of the spirituality scale on SW. In Model 1, sociodemographic variables were included to assess any changes in the coefficient associated with spirituality. Finally, Model 2 incorporated both sociodemographic variables and health conditions to provide a more comprehensive analysis. Statistical analyses were performed with STATA version 14.0 and Jamovi version 1.6.23.0.
3 Results
Regarding the sociodemographic characteristics of the participants, the majority were women (74.8%), with a mean age of 74.5 years. Half of the participants attained at least a mid-level education, with 30.2% having completed high school and 20.6% holding an undergraduate degree or higher. Additionally, 41.0% were married or in a partnership, while 16.3% are single. Only 10.4% were currently employed, 29.6% were retired, and 55.2% were homemakers. Furthermore, 15.7% live alone, 33.9% live with a partner, and half reside with other family members (Table 1). Regarding health conditions, the highest percentage reported good health, while one-third indicated that they had at least one medical condition, furthermore, 22.9% indicated difficulty performing at least one basic activity of daily living (Table 1).
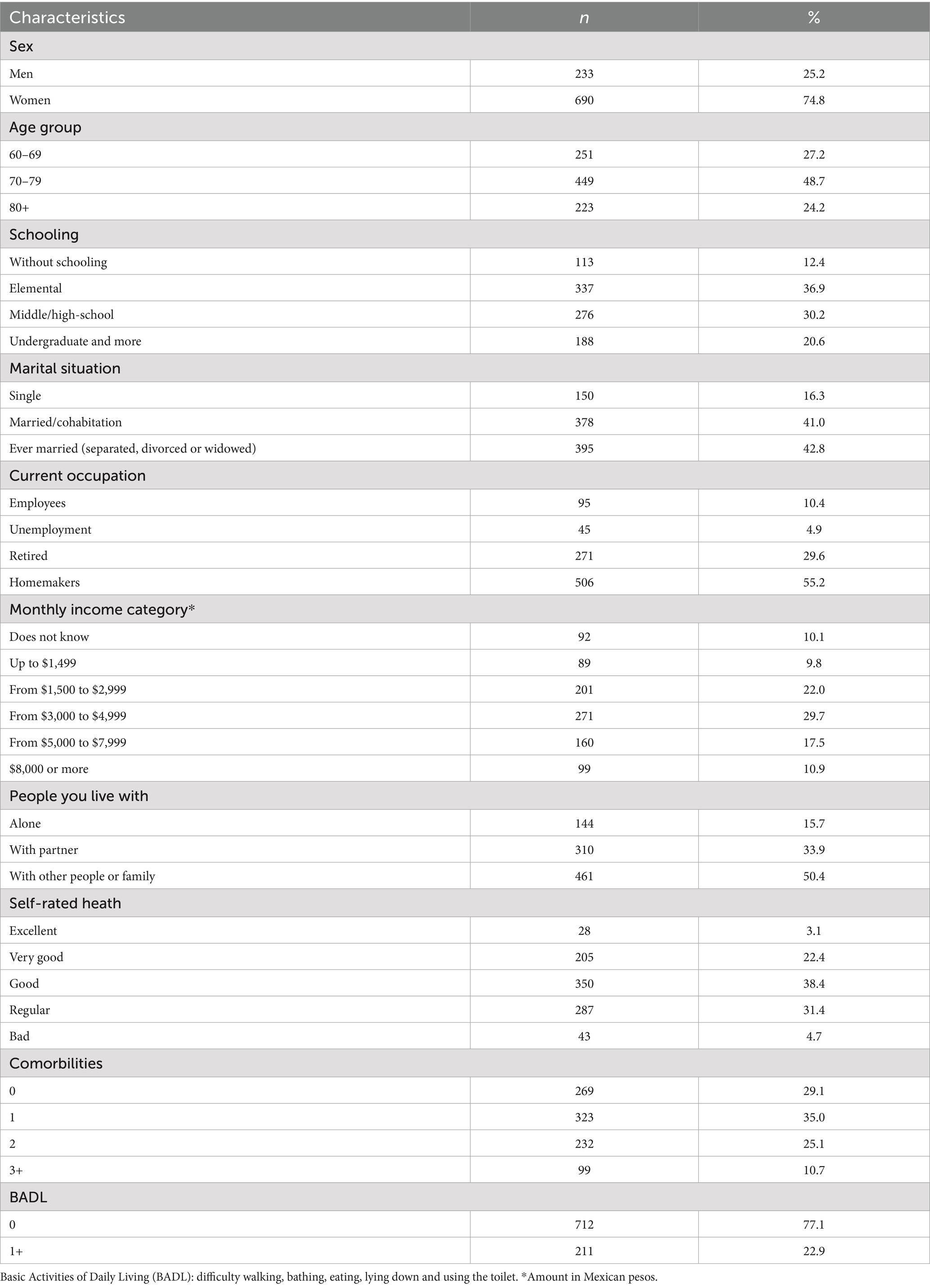
Table 1. Sociodemographic and health characteristics of the participants.
Table 2 shows the results regarding the CFA, Cronbach’s alpha, mean and standard deviation for the tools used in this study. As can be seen, in general the indices were adequate for all instruments. The results showed that for most of the instruments an adequate fit was found for CFA, in addition to obtaining adequate Cronbach’s alpha values. Only for religious involvement three items had to be eliminated (r1, r2 and r8) based on the modification indices for the instrument to show an adequate fit.
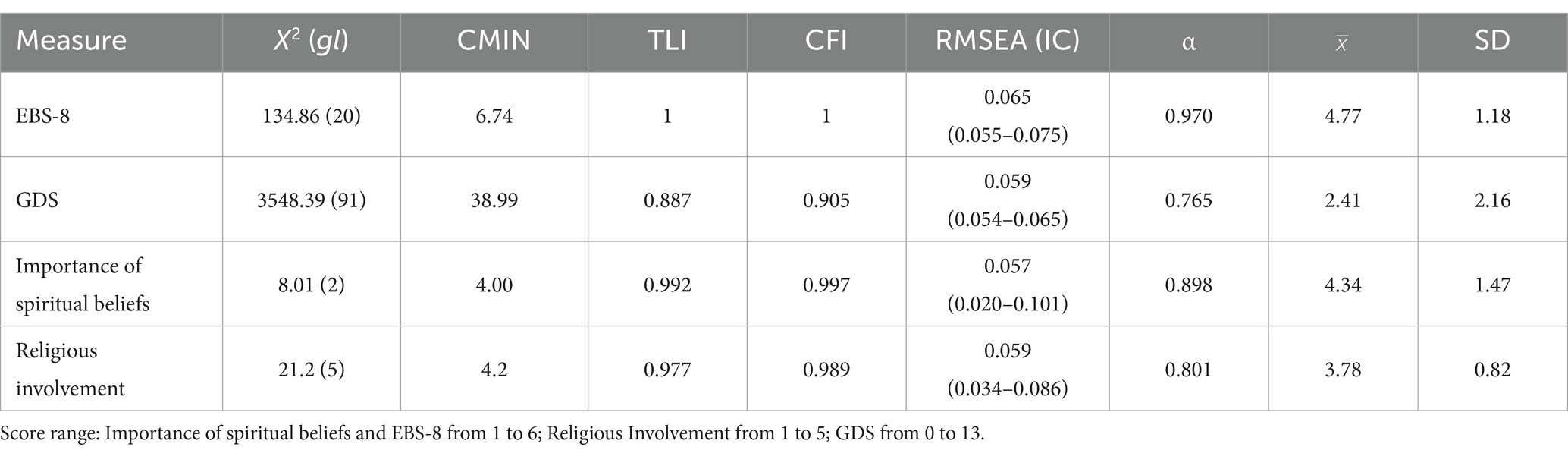
Table 2. Evidence of reliability and validity of the instruments used.
When comparing the average scores of the SW scale across various characteristics and conditions (Table 3), the results reveal distinct patterns. No significant differences were found based on sociodemographic characteristics such as gender, age, education level, marital status, or household arrangement. However, individuals with better self-perceived health and no functional limitations reported higher SW scores. In addition, OA with a greater number of health conditions had lower SW.
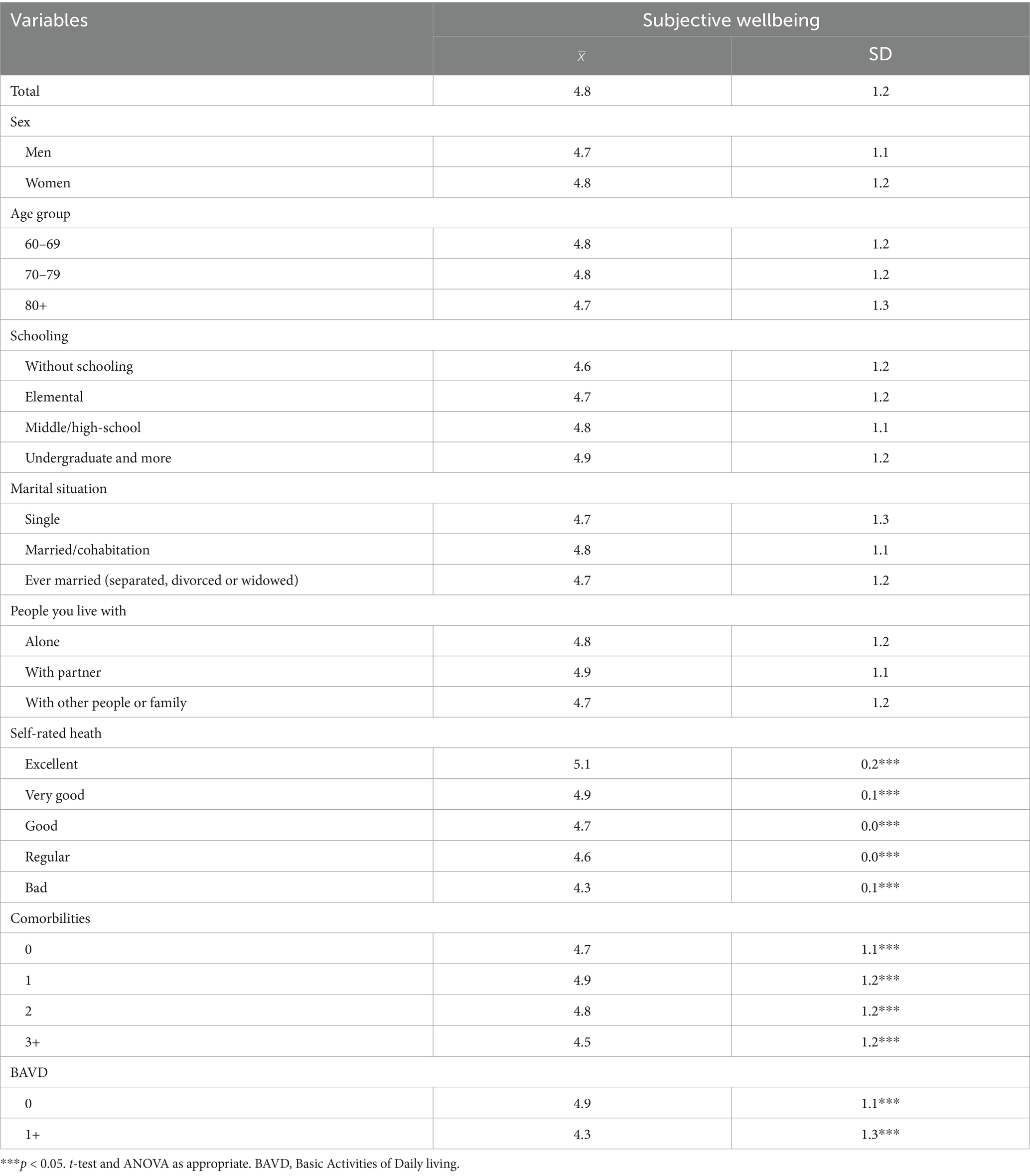
Table 3. Mean subjective wellbeing index by different characteristics and health conditions.
In terms of correlations (Table 4), SW shows a positive association with spirituality, religiosity, and self-reported health. On the other hand, an increase in SW is related to a significant decrease in depression and the number of basic activities affected. Similarly, as spirituality increases, religiosity, and SW also increase. However, in an inverse relationship, the associations of spirituality with depression and are weaker compared to those observed with SW. It is important to note that no association was found between SW and age.
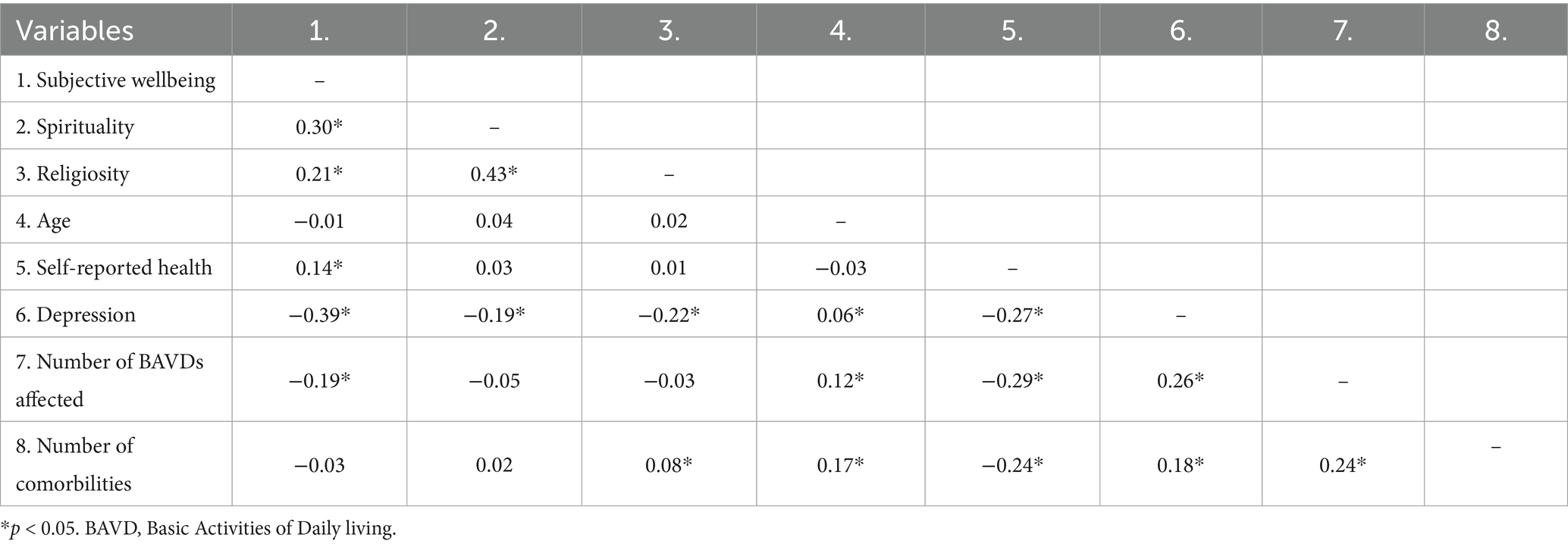
Table 4. Correlation of variables.
Table 5 presents the estimates from the linear regression models analyzing the effects of spirituality, religiosity, sociodemographic characteristics, and health conditions (physical and mental) on the SW index. In Model 0, SW increases significantly when spirituality enters the equation. When sociodemographic variables are added in Model 1, the significant effect of spirituality persists, although it slightly decreases and a significant effect of schooling is presented, where SW increases in OA with higher education. In Model 2, which incorporates health conditions, there were significant effects of spirituality and depression. Among the health variables, the results showed that difficulties in basic activities significantly reduce SW. In this final model, the R-squared value rises to 0.174, indicating that approximately 17% of the variability in SW is explained by the variables included in the model.
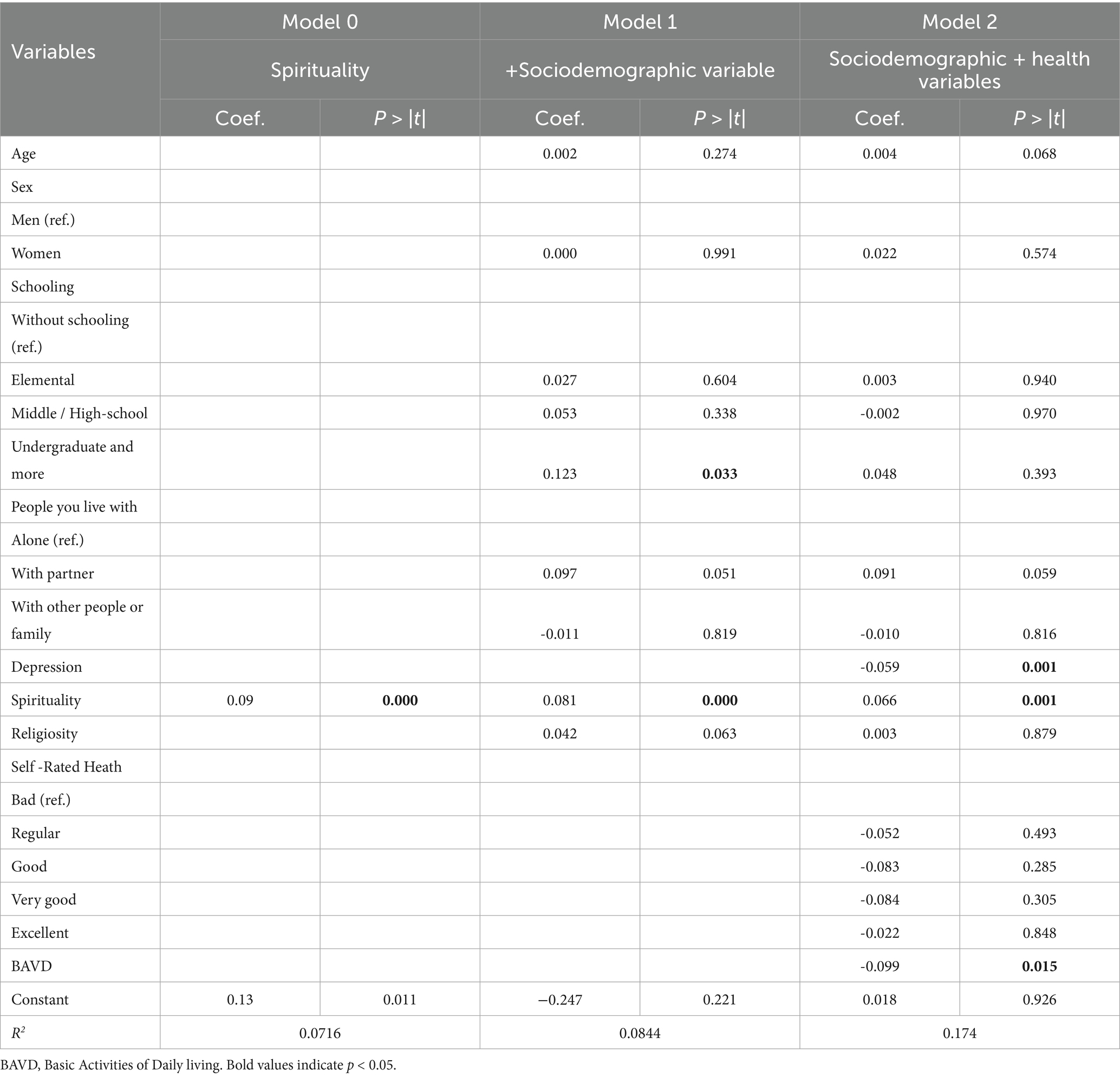
Table 5. Results of linear regression models with subjective wellbeing as the dependent variable.
4 Discussion
The central objective of this research was to analyze the importance of spirituality and religiosity in the SW of OA, controlling demographic and health variables, for which three models were tested, in the third model that explains 17% of the variance of SW it was found that spirituality, while depression and difficulties in daily life reduce SW.
The results allow affirming that spirituality plays an important role in the SW of OA, which coincides with the results of other authors (Soósová et al., 2021; Litalien et al., 2022; Can Oz et al., 2022; Pérez et al., 2022; Koenig and Al Zaben, 2021; Koenig et al., 2020) who affirm that spirituality can be a protective factor for OA as it helps them to cope with physical, psychological and social changes, in addition to providing them with some security, stability and sense of life. It also corroborates the importance of physical and mental health in the SW of OA as has been raised in several studies (Cross et al., 2018; Jitdorn et al., 2021; Ladusingh and Ngangbam, 2016; Hashmi et al., 2018; Lombardo et al., 2018), since physical health is related to functionality and autonomy, and for its part, taking care of mental health enables adequate management of the situations that arise in daily life, as well as adequate stress management.
It is important to highlight that in this study no significant differences were found in SW by sociodemographic variables, which contradicts the results of other studies (Lukaschek et al., 2017; Zhang and Sun, 2024), where it has been pointed out that there are differences, mainly in sex and age, where in the latter, there is not necessarily a decrease in SW as age advances, although on the other hand, differences are confirmed by health variables, such as self-perceived health and difficulties in daily activities reported by the people (Cross et al., 2018; Jitdorn et al., 2021), although it would be convenient for the case of the assessment of health conditions, to have objective data to corroborate these findings, beyond just assessing the self-perception of health status.
The correlation analysis showed relationships in the expected direction, the greater the spirituality, religiosity and self-perceived health, the greater the SW. This could confirm that these variables promote positive aspects in the OA, in this sense it can be mentioned that spirituality and religiosity have been shown to be variables that favor feelings of hope, as well as an adequate meaning of their own life and a greater belonging to their community and/or social groups. In the case of self-perceived health, this can be linked to an adequate SW as a result of the perception of their condition and their functionality, which is congruent with the correlation found between self-perceived health and the number of difficulties in carrying out activities of daily living, where the better the perception of health, the fewer the number of difficulties; in addition, the number of difficulties was negatively associated with SW.
The highest SW correlations were obtained with depression and spirituality, which is congruent and confirms that depression decreases the SW of OA (Li et al., 2023; Lukaschek et al., 2017; Soósová et al., 2021) by negatively impacting the lives of OA. Regarding the role of spirituality, it is observed to increase SW (Soósová et al., 2021; Can Oz et al., 2022; Abu et al., 2018) by fostering a sense of connection with themselves and others, as well as a sense of hope, transcendence, and wisdom in the face of the conditions that aging sometimes represents. An important finding was that spirituality is related to lower depressive symptomatology, which could represent a feasible intervention strategy in the prevention and treatment of depressive symptoms (Soósová et al., 2021; Gallardo-Peralta and Sánchez-Moreno, 2020), particularly as a coping mechanism in the face of adverse situations in the lives of OA, by mobilizing their internal resources to promote hope, a sense of belonging and connection with themselves, with others and with nature.
Another interesting result is that spirituality showed a stronger correlation with SW than religiosity, which confirms the results of other studies (Saldías-Ortega and Moyano-Díaz, 2023) and underlines the importance of measuring these two constructs independently as several authors have proposed (Zimmer et al., 2016; Büssing, 2018), in order to be able to evaluate the effect of each one, because although the two constructs are related, they are different, conceptually and operationally, otherwise, it will be assumed that both play the same role, and could even hinder the ability to differentiate possible additive effects between these two constructs.
In the present study, it was observed that in each of the models tested, spirituality played an important role as a predictor of SW, and even remained stable when the demographic variables of sex, age, schooling, and who the OA lives with were incorporated, maintaining itself even with the inclusion of variables related to the health conditions reported by the OA, and although it was found that, in particular depression and difficulties in performing activities of daily living negatively affected SW, spirituality continues to be a variable that favors SW in the sample analyzed.
These results contribute to the analysis of possible strategies that can promote healthy aging, such as spirituality, which showed a positive relationship with the subjective wellbeing of OA and a negative relationship with depression. Therefore, it would be important to take into account that, when developing interventions that promote the wellbeing of older adults, spirituality should be included as a central element, incorporating activities that promote internalization and mindfulness into interventions, such as meditation, mindfulness, reflection and meaning activities such as writing or reading that promote reflection and self-awareness, activities involving interaction with people and groups that promote helping others and, therefore, foster transcendence and purpose in life, as well as the inclusion of outdoor activities that bring older adults into contact with nature and other living beings.
One of the limitations of this study was that there were no objective measures to assess health status, so it would be advisable for future studies to use a more accurate indicator and avoid any kind of bias. In addition, this study had a non-probabilistic sample and most of the participants were women, so it is recommended that these results be confirmed in other samples of OA. Another major challenge is the measurement of spirituality, which, especially in older adults, could be confused with religiosity, particularly in populations that have deeply rooted religious practices as part of their history and culture. In spite of this, the present research provided elements on the role of spirituality and religiosity in a sample characterized by certain unfavorable health and life conditions that are difficult to modify and where specifically, spirituality could help OA in these conditions to age with greater wellbeing.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Research Bioethics Committee from the Health Sciences Faculty, Anahuac University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AG-G: Investigation, Conceptualization, Writing – original draft. PA: Writing – original draft. RG-C: Formal analysis, Writing – review & editing. MS: Writing – review & editing. DB: Writing – review & editing, Formal analysis, Investigation.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The authors would like to thank the Research Department of Anáhuac University Mexico for its support in publishing this article.
Acknowledgments
The authors express their gratitude to the Secretaría de Bienestar e Igualdad Social of México City, through the Instituto para el Envejecimiento Digno (INED), for their support in data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abu, H. O., Ulbricht, C., Ding, E., Allison, J. J., Salmoirago-Blotcher, E., Goldberg, R. J., et al. (2018). Association of religiosity and spirituality with quality of life in patients with cardiovascular disease: a systematic review. Qual. Life Res. 27, 2777–2797. doi: 10.1007/s11136-018-1906-4
Aranco, N., Bosch, M., Stampini, M., Azuara, O., Goyeneche, L., Ibarrarán, P., et al. (2022). Envejecer en América Latina y el Caribe. Protección social y calidad de vida de las personas mayores. Available online at: https://publications.iadb.org/es/envejecer-en-america-latina-y-el-caribe-proteccion-social-y-calidad-de-vida-de-las-personas-mayores (Accessed October 15, 2025).
Arévalo-Avecillas, D., Game, C., Padilla-Lozano, C., and Wong, N. (2019). Predictores de la calidad de vida subjetiva en adultos mayores de zonas urbanas y rurales de la provincia del Guayas, Ecuador. Inf. Tecnol. 30, 271–282. doi: 10.4067/S0718-07642019000500271
Batz, C., and Tay, L. (2018). “Gender and subjective well-being” in Handbook of well-being. eds. E. Diener, S. Oishi, and L. Tay (Salt Lake City, UT: DEP Publishers), 382–396.
Borson, S., Scanlan, J. M., Chen, P., and Ganguli, M. (2003). The Mini-cog as a screen for dementia: validation in a population-based sample. J. Am. Geriatr. Soc. 51, 1451–1454. doi: 10.1046/j.1532-5415.2003.51465.x
Calleja, N., and Mason, T. A. (2020). Escala de Bienestar Subjetivo (EBS- 20 y EBS-8): Construcción y validación. Rev. Iberoam. Diagn. Eval. Psicol. 55, 185–201. doi: 10.21865/RIDEP55.2.14
Can Oz, Y., Duran, S., and Dogan, K. (2022). The meaning and role of spirituality for older adults: a qualitative study. J. Relig. Health 61, 1490–1504. doi: 10.1007/s10943-021-01258-x
Casanova, G., Machado, I., and Melo, S. (2024). The role of spirituality in later life: a study of older adult university students in Portugal. J. Relig. Spiritual. Aging 36, 309–332. doi: 10.1080/15528030.2023.2216157
Coelho-Júnior, H. J., Calvani, R., Panza, F., Allegri, R. F., Picca, A., Marzetti, E., et al. (2022). Religiosity/spirituality and mental health in older adults: a systematic review and meta-analysis of observational studies. Front. Med. 9:877213. doi: 10.3389/fmed.2022.877213
Cramm, J. M., and Nieboer, A. P. (2015). Social cohesion and belonging predict the well-being of community-dwelling older people. BMC Geriatr. 15:30. doi: 10.1186/s12877-015-0027-y
Cross, M. P., Hofschneider, L., Grimm, M., and Pressman, S. D. (2018). “Subjective well-being and physical health” in Handbook of well-being. eds. E. Diener, S. Oishi, and L. Tay (Salt Lake City, UT: DEP Publishers), 472–489.
De Freitas, M., Leal, M., and Nwora, E. (2022). Praying for a miracle part II: idiosyncrasies of spirituality and its relations with religious expressions in health. Front. Psychol. 13:13. doi: 10.3389/fpsyg.2022.893780
Diener, E. (1984). Subjective well-being. Psychol. Bull. 95, 542–575. doi: 10.1037/0033-2909.95.3.542
Diener, E., Oishi, S., and Tay, L. (2018). “Introduction by the editors” in Handbook of well-being. eds. E. Diener, S. Oishi, and L. Tay (Salt Lake City, UT: DEP Publishers), 5–6.
Diener, E., and Suh, E. (1997). Measuring quality of life: economic, social, and subjective indicators. Soc. Indic. Res. 40, 189–216. doi: 10.1023/A:1006859511756
Diener, E., Suh, E. M., Lucas, R. E., and Smith, H. L. (1999). Subjective well-being: three decades of progress. Psychol. Bull. 125, 276–302. doi: 10.1037/0033-2909.125.2.276
Dominguez, L. J., Veronese, N., and Barbagallo, M. (2024). The link between spirituality and longevity. Aging Clin. Exp. Res. 36:32. doi: 10.1007/s40520-023-02684-5
Dorji, N., Dunne, M., and Gurung, M. (2019). Socio-demographic correlates of psychological well-being among older adults in Bhutan. Environ. Soc. Psychol. 4, 1–8. doi: 10.18063/esp.v4i2.782
Du, X., Zhou, M., Mao, Q., Luo, Y., and Chen, X. (2023). Positive aging: social support and social well-being in older adults-the serial mediation model of social comparison and cognitive reappraisal. Curr. Psychol. 42, 22429–22435. doi: 10.1007/s12144-022-03219-3
Flores-Kanter, P. E., Muñoz-Navarro, R., and Medrano, L. A. (2018). Concepciones de la felicidad y su relación con el bienestar subjetivo: un estudio mediante redes semánticas naturales. Liberabit 24, 115–130. doi: 10.24265/liberabit.2018.v24n1.08
Gallardo-Peralta, L., and Sánchez-Moreno, E. (2020). Espiritualidad, religiosidad y síntomas depresivos en personas mayores del norte de Chile. Ter. Psicol. 38, 169–187. doi: 10.4067/S0718-48082020000200169
García-Chanes, R. E., López-Ortega, M., and Torres-Castro, S. (2024). Life satisfaction trajectories and associated factors in middle-aged and older Mexican adults. Arch. Med. Res. 55:103040. doi: 10.1016/j.arcmed.2024.103040
Gobbens, R. J., and Remmen, R. (2019). The effects of sociodemographic factors on quality of life among people aged 50 years or older are not unequivocal: comparing SF-12, WHOQOL-BREF, and WHOQOL-OLD. Clin. Interv. Aging 14, 231–239. doi: 10.2147/CIA.S189560
Guerrero-Castañeda, R., García, A., Aguilar, P., and Albañil, S. (2021). Significado de la espiritualidad en la vivencia del adulto mayor hospitalizado. Rev. Cubana Enferm. 37:e3981.
Hashmi, J. F., Sharma, V., and Sarkar, S. (2018). Subjective well-being perceived physical and mental health status of elderly: a comparative study in urban and rural India. J. Psychiatr. Nurs. 7, 91–97. doi: 10.21088/jpn.2277.9035.7318.4
Hu, L. T., and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct. Equ. Model. 6, 1–55. doi: 10.1080/10705519909540118
Instituto Nacional de Estadística y Geografía. (2021). Encuesta Nacional sobre Salud y Envejecimiento en México. Available online at: https://www.inegi.org.mx/contenidos/programas/enasem/2021/doc/enasem_2021_presentacion.pdf (Accessed October 13, 2025).
Instituto Nacional de Estadística y Geografía (2021). Encuesta Nacional de Bienestar Autorreportado. ENBIARE 2021. México: INEGI.
Instituto Nacional de Estadística y Geografía. (2022). Estadísticas a propósito del día internacional de las personas adultas mayores. Available online at: https://www.inegi.org.mx/contenidos/saladeprensa/aproposito/2022/EAP_ADULMAY2022.pdf (Accessed October 13, 2025).
Jitdorn, J., Somprasert, C., Kongvattananon, P., and Soonthornchaiya, R. (2021). An integrative review of experience of well-being and happiness: insights from older adults in the community. Trends Sci. 18:20. doi: 10.48048/tis.2021.20
Koenig, H. G., and Al Zaben, F. (2021). Psychometric validation and translation of religious and spiritual measures. J. Relig. Health 60, 3467–3483. doi: 10.1007/s10943-021-01373-9
Koenig, H. G., Al-Zaben, F., and VanderWeele, T. J. (2020). Religion and psychiatry: recent developments in research. BJPsych Adv. 26, 262–272. doi: 10.1192/bja.2019.81
Ladusingh, L., and Ngangbam, S. (2016). Domains and determinants of well-being of older adults in India. J. Cross Cult. Gerontol. 31, 89–111. doi: 10.1007/s10823-016-9279-z
Lansford, J. E. (2018). “A lifespan perspective on subjective well-being” in Handbook of well-being. eds. E. Diener, S. Oishi, and L. Tay (Salt Lake City, UT: DEP Publishers), 1–15.
Li, C., Xia, Y., and Zhang, Y. (2023). Relationship between subjective well-being and depressive disorders: novel findings of cohort variations and demographic heterogeneities. Front. Psychol. 13:1022643. doi: 10.3389/fpsyg.2022.1022643
Litalien, M., Atari, D. O., and Obasi, I. (2022). The influence of religiosity and spirituality on health in Canada: a systematic literature review. J. Relig. Health 61, 373–414. doi: 10.1007/s10943-020-01148-8
Lombardo, P., Jones, W., Wang, L., Shen, X., and Goldner, E. M. (2018). The fundamental association between mental health and life satisfaction: results from successive waves of a Canadian national survey. BMC Public Health 18:342. doi: 10.1186/s12889-018-5235-x
López-Ortega, M., Torres-Castro, S., and Rosas-Carrasco, O. (2016). Psychometric properties of the satisfaction with life scale (SWLS): secondary analysis of the Mexican health and aging study. Health Qual. Life Outcomes 14:170. doi: 10.1186/s12955-016-0573-9
Lucchetti, G., Góes, L. G., Amaral, S. G., Ganadjian, G. T., Andrade, I., Almeida, P. O. D. A., et al. (2021). Spirituality, religiosity and the mental health consequences of social isolation during Covid-19 pandemic. Int. J. Soc. Psychiatry 67, 672–679. doi: 10.1177/0020764020970996
Lukaschek, K., Vanajan, A., Johar, H., Weiland, N., and Ladwig, K. H. (2017). “In the mood for ageing”: determinants of subjective well-being in older men and women of the population-based KORA-age study. BMC Geriatr. 17:126. doi: 10.1186/s12877-017-0513-5
Malone, J., and Dadswell, A. (2018). The role of religion, spirituality and/or belief in positive ageing for older adults. Geriatrics 3:28. doi: 10.3390/geriatrics3020028
Neville, S., Napier, S., Silulu, F. M. L., Wong Soon, H. N., and Tautolo, E. S. (2024). The influence of spirituality and religion on health and well-being for older Pacific people. J. Relig. Spiritual. Aging 36, 293–308. doi: 10.1080/15528030.2023.2221872
Ngamaba, K. H., Panagioti, M., and Armitage, C. J. (2017). How strongly related are health status and subjective well-being? Systematic review and meta-analysis. Eur. J. Health Econ. 27, 879–885. doi: 10.1093/eurpub/ckx081
Organización Mundial de la Salud. (2022). Envejecimiento y salud. Available online at: https://www.who.int/es/news-room/fact-sheets/detail/ageing-and-health (Accessed March 21, 2025).
Organización Mundial de la Salud. (2025). Envejecimiento y salud. Available online at: https://www.who.int/es/news-room/fact-sheets/detail/ageing-and-health (Accessed October 15, 2025).
Papadopoulos, D. (2020). The role of well-being, spirituality, and religiosity for successful aging in late life: a brief review. Adv. Life Course Res. 9, 23–31. doi: 10.4236/aar.2020.92003
Parsian, N., and Dunning, P. (2009). Developing and validating a questionnaire to measure spirituality: a psychometric process. Glob J Heath Sci. 1, 2–11. doi: 10.5539/gjhs.v1n1p2
Paul, C., Velciu, M., and Spiru, L. (2024). “Advancements in the understanding of what wellbeing at very old age is: an exploratory study” in Proceedings of the 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2024), 284–290.
Pérez, D., Álvarez, H., and Álvarez, M. (2022). Espiritualidad como factor protector en el adulto mayor. una revisión sistemática. Rev. Cient. Sci. 32, 125–138. doi: 10.48204/j.scientia.v32n2.a3135
Piedmont, R. L. (2014). “Assessment of spirituality and religious sentiments (ASPIRES) scale” in Encyclopedia of quality of life and well-being research. ed. A. C. Michalos (Dordrecht: Springer), 258–259.
Reyna-Barajas, G. V., Copertari-Isaacson, L. F., Samaniego-Garay, R. A., García-Alonzo, I., and Del Río-Mendoza, M. L. (2025). Percepción de la calidad de vida relacionada con la salud en adultos mayores según el género. Rev. Cient Acad. 6, 36–55. doi: 10.61368/r.s.d.h.v6i1.465
Saldías-Ortega, F., and Moyano-Díaz, E. (2023). Influencia de la espiritualidad y religiosidad sobre la felicidad en adultos mayores. Psykhe 32, 1–18. doi: 10.7764/psykhe.2021.29435
Salgado, C. Y. K., Andrade, P. P., Hernández, G. A., González-Arriata, L. F. N. A., Díaz Loving, R., and Velasco, R. Á. E. (2024). Validación de la escala de depresión geriátrica de Yesavage en adultos mayores mexicanos. Inf. Psicol. 24, 123–135. doi: 10.18566/infpsic.v24n1a08
Simkin, H. (2017). Adaptación al español de la Escala de Espiritualidad y Sentimientos Religiosos (ASPIRES). Univ. Psychol. 16, 1–12. doi: 10.11144/Javeriana.upsy16-2.aeee
Soósová, M. S., Timková, V., Dimunová, L., and Mauer, B. (2021). Spirituality as a mediator between depressive symptoms and subjective well-being in older adults. Clin. Nurs. Res. 30, 707–717. doi: 10.1177/1054773821991152
Soriano, G., Calong, K., Martinez, R., and Locsin, R. (2021). Religiosity, spirituality and death anxiety among older adults living at home and in institutional facilities: a comparative study. J. Relig. Spiritual. Aging 34, 284–296. doi: 10.1080/15528030.2021.1948948
Stone, A. A., Broderick, J. E., Wang, D., and Schneider, S. (2020). Age patterns in subjective well-being are partially accounted for by psychological and social factors associated with aging. PLoS One 15:e0242664. doi: 10.1371/journal.pone.0242664
Tabatabaei, S. Z., and Ebrahimi, F. (2023). Religion and subjective well-being among the female elderly people: a focused ethnography. Middle East J. Rehabil. Health 10:e129593. doi: 10.5812/mejrh-129593
Tov, W., Wirtz, D., Kushlev, K., Biswas-Diener, R., and Diener, E. (2022). Well-being science for teaching and the public. Perspect. Psychol. Sci. 17, 1452–1471. doi: 10.1177/17456916211046946
Triyuliasari, A., Irfani, A. D., and Zuliani, S. (2024). What keeps older adults happy? A systematic review of subjective well-being. Eur. J. Psychol. Educ. Res. 7, 225–232. doi: 10.12973/ejper.7.4.225
United Nations. (2022). World population prospects 2022: summary of results. Available online at: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/undesa_pd_2022_wpp_key-messages.pdf (Accessed May 17, 2025).
Vicente, A. R. T., Castro-Costa, É., Firmo, J. D. O. A., Lima-Costa, M. F., and Loyola Filho, A. I. D. (2018). Religiousness, social support and the use of antidepressants among the elderly: a population-based study. Ciênc. Saúde Colet. 23, 963–971. doi: 10.1590/1413-81232018233.05922016
Watkins, P., Frederick, M., and Davis, D. (2022). Gratitude to god predicts religious well-being over time. Religion 13:675. doi: 10.3390/rel13080675
Yesavage, J. A., Brink, T. L., Rose, T. L., and Lum, O. (1983). Development and validation of a geriatric depression scale: a preliminary report. J. Psychiatr. Res. 17, 37–49. doi: 10.1016/0022-3956(82)90033-4
Zapata, N. L. F. (2017). La espiritualidad como factor de bienestar psicológico en el proceso de envejecimiento. Tesis de Doctorado. Bogotá (Col): Corporación Universitaria Minuto de Dios.
Zhang, Y., and Sun, L. (2024). The health status, social support, and subjective well-being of older individuals: evidence from the Chinese general social survey. Front. Public Health 12:1312841. doi: 10.3389/fpubh.2024.1312841
Keywords: religion, health, spiritual, aging, wellbeing
Citation: González-González A, Andrade Palos P, García-Chanes RE, Sánchez Hernández ME and Betancourt Ocampo D (2025) Spirituality and religiosity as predictors of subjective wellbeing in older Mexican adults. Front. Psychol. 16:1663757. doi: 10.3389/fpsyg.2025.1663757
Edited by:
José Aparecido Da Silva, University of Brasilia, BrazilReviewed by:
Lia Araujo, Polytechnic Institute of Viseu, PortugalHelena Chui, Charles Darwin University, Australia
Copyright © 2025 González-González, Andrade Palos, García-Chanes, Sánchez Hernández and Betancourt Ocampo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diana Betancourt Ocampo, ZGlhbmEuYmV0YW5jb3VydEBhbmFodWFjLm14