 Annarosa Cipriano
Annarosa Cipriano Stefania Cella
Stefania Cella Paolo Cotrufo
Paolo Cotrufo- Observatory on Eating Disorders, Department of Psychology, University of Campania “Luigi Vanvitelli”, Caserta, Italy
Objective: Nonsuicidal self-injury (NSSI) refers to the intentional self-inflicted destruction of body tissue without suicidal intention and for purposes not socially sanctioned. Our paper presents an up-to-date overview on nonsuicidal, self-injurious behaviors.
Method: In accordance with PRISMA guidelines, a systematic literature search was conducted across two databases, PubMed and PsycARTICLES, regarding the main features of NSSI with a focus on epidemiological and etiologic data, diagnostic criteria, and functions. All English articles, published between 1998 and 2016, were considered, and screened against a priori inclusion/exclusion criteria. The search terms include: self-harm, self-injury, NSSI, epidemiology, comorbidity, gender, functions and DSM. We also examined the references of the retrieved articles.
Results: NSSI is most common among adolescents and young adults, and the age of onset is reported to occur between 12 and 14 years. Comorbidity with borderline personality disorder (BPD) and eating disorders is often reported. DSM-5 includes NSSI as a condition requiring further study. This review gives an overview of the prevalence rates (7.5–46.5% adolescents, 38.9% university students, 4–23% adults) and main causes that appear to stem from childhood trauma, comorbidity with many other disorders and several functions of NSSI, and the potential independence of a NSSI disorder.
Conclusion: Over the years, interest in NSSI grew to such an extent that an ongoing debate was instigated on whether NSSI should be considered as a diagnosis in its own right and given its own category. This paper provides an up-to-date overview on self-injury, what is known about it and what remains to be done. Clearly, our understanding of the main issues of NSSI has increased in last two decades. However, future researches is needed to examine the developmental trajectories, cultural backgrounds and shed light on the risk factors and functions as well as clarify its role as an independent diagnostic entity.
Introduction
Nonsuicidal Self-Injury (NSSI) behavior is a growing clinical and public health problem. NSSI is defined as the direct and deliberate destruction of one's own bodily tissue in the absence of lethal intent and for reasons not socially sanctioned (Favazza, 1996; Nock, 2010). Common forms of NSSI include behaviors such as cutting, burning, scratching, and self-hitting (Briere and Gil, 1998; Laye-Gindhu and Schonert-Reichl, 2005; Whitlock et al., 2006; Klonsky and Muehlenkamp, 2007) and most self-injurers report using multiple method (Favazza and Conterio, 1988; Favazza, 1992). Evidences focused on the psychological intentions underlying NSSI demonstrated that the behavior serves a variety of function, both interpersonal and intrapersonal, that are not mutually exclusive (Suyemoto, 1998; Nock and Prinstein, 2004; Klonsky, 2007). Initial research on self-injurious behavior focused on studies in clinical settings (Pattison and Kahan, 1983), primarily with female subjects (Favazza and Conterio, 1989; Favazza et al., 1989; Herpertz, 1995; Suyemoto and MacDonald, 1995).
Epidemiological studies have endured due to the over-inclusive definition of behavior, with and without suicidal intent, as well as the dearth of consistent assessment measures. Earlier estimates ranged from 40 to 82% among adolescents in psychiatric inpatient settings (Darche, 1990; DiClemente et al., 1991) and stated that ~4% of the general population have a history of NSSI (Briere and Gil, 1998). Most recently researchers noticed that self-injurious behavior is more prevalent even among adolescents and young adults. The first attempt to describe this behavior can be seen in the book “Man against himself” by Menninger (1938), in which the author defined self-injurious behavior as a sort of “partial suicide.” There has been an absence of generally agreed upon terminology and, over the years, several different terms to define self-injurious behaviors have appeared in literature: syndrome of delicate self-cutting (Pao, 1969), deliberate self-harm (Pattison and Kahan, 1983), self-wounding (Tantam and Whittaker, 1992), moderate self-mutilation (Favazza and Rosenthal, 1993), self-mutilation (Ross and Heath, 2002); some of which include suicidal behaviors, risk taking, and an indirect form of self-harm (Favazza, 1996). The lack of consensus regarding terminology and definition has made the understanding of such behaviors very difficult. Self-injury is a common but—as yet—poorly understood phenomenon (Klonsky and Muehlenkamp, 2007).
Self-injury has long been linked to other disorders as well, including post-traumatic stress disorder (Briere and Gil, 1998; Bolognini et al., 2003), depressive disorders (Darche, 1990), obsessive-compulsive disorder (Bolognini et al., 2003), anxiety disorder (Darche, 1990; Simeon and Favazza, 2001), borderline personality disorder (BPD) (Klonsky et al., 2003; Nock et al., 2006), and eating disorder (Iannaccone et al., 2013). Many researchers and clinicians have argued for the adoption of a NSSI disorder: some of the earliest attempts to define such a syndrome being made by Graff and Mallin (1967); Pao (1969), and Rosenthal et al. (1972). Those first attempted failed (Favazza and Rosenthal, 1990) due to the inclusion of suicide attempts in the definitions. Kahan and Pattison (1984) differentiated self-harming behaviors from suicide and proposed a separate diagnostic disorder: the deliberate self-harm syndrome (DSH). Later, Favazza and Rosenthal (1990) suggested that habitual and repetitive self-injurious behavior could be considered as an impulse control disorder: the repetitive self-mutilation syndrome. Muehlenkamp (2005) also proposed that repetitive NSSI should be regarded as a separate diagnostic disorder. More recently, Wilkinson and Goodyer (2011) proposed that giving NSSI its own diagnostic category would improve communication and increase research on etiology, its treatment and outcome. There have been many arguments over NSSI, but given the high prevalence of self-injurious behaviors among clinical and community samples of adolescents (Muehlenkamp et al., 2012; Swannell et al., 2014), and associated clinical and functional impairment, the Childhood and Mood Disorders work-group of the DSM-5 proposed the inclusion of NSSI as a separate diagnostic disorder (Shaffer and Jacobson, 2009). Despite its criteria undergoing several revisions, due to a lack of research on the full set proposed criteria, inadequate sample size and unacceptably low inter-rater reliability results in the DSM-5 field trials (Regier et al., 2013), the NSSI disorder (NSSID) was only included as a condition requiring further study, in section 3 of DSM-5, and it represents an important step forward in recognizing NSSI as a disorder in its own right (Selby et al., 2015) and in promoting further research. Given the contrasts and conflicting data present in literature on NSSI, the aim of the present study is to systematize this broad field of research, focusing on (1) proposed diagnostic criteria for the DSM-5, (2) epidemiology, (3) comorbidity, (4) etiology, and (5) functions.
Materials and Methods
Data Source and Search Strategy
The present study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA, Liberati et al., 2009). PubMed and PsycARTICLES databases were searched for eligible studies published in English between 1998 and 2016. The following combinations of search terms were employed: 1. self-harm OR, self-injury OR, nonsuicidal self-injury OR, NSSI, 2. epidemiology, 3. comorbidity, 4. gender, 5. Functions, 6. DSM. Additionally, we also examined the references of the articles identified in the search.
Study Selection
Figure 1 shows the selection of included studies. In total, the initial database search yielded 12340 abstract, of which 6356 duplicate were removed. Articles were first screened by title and abstract by two independent reviewers. Of the remaining studies, the full text was obtained and inspected independently by the same two authors to ensure that the inclusion/exclusion criteria were met.
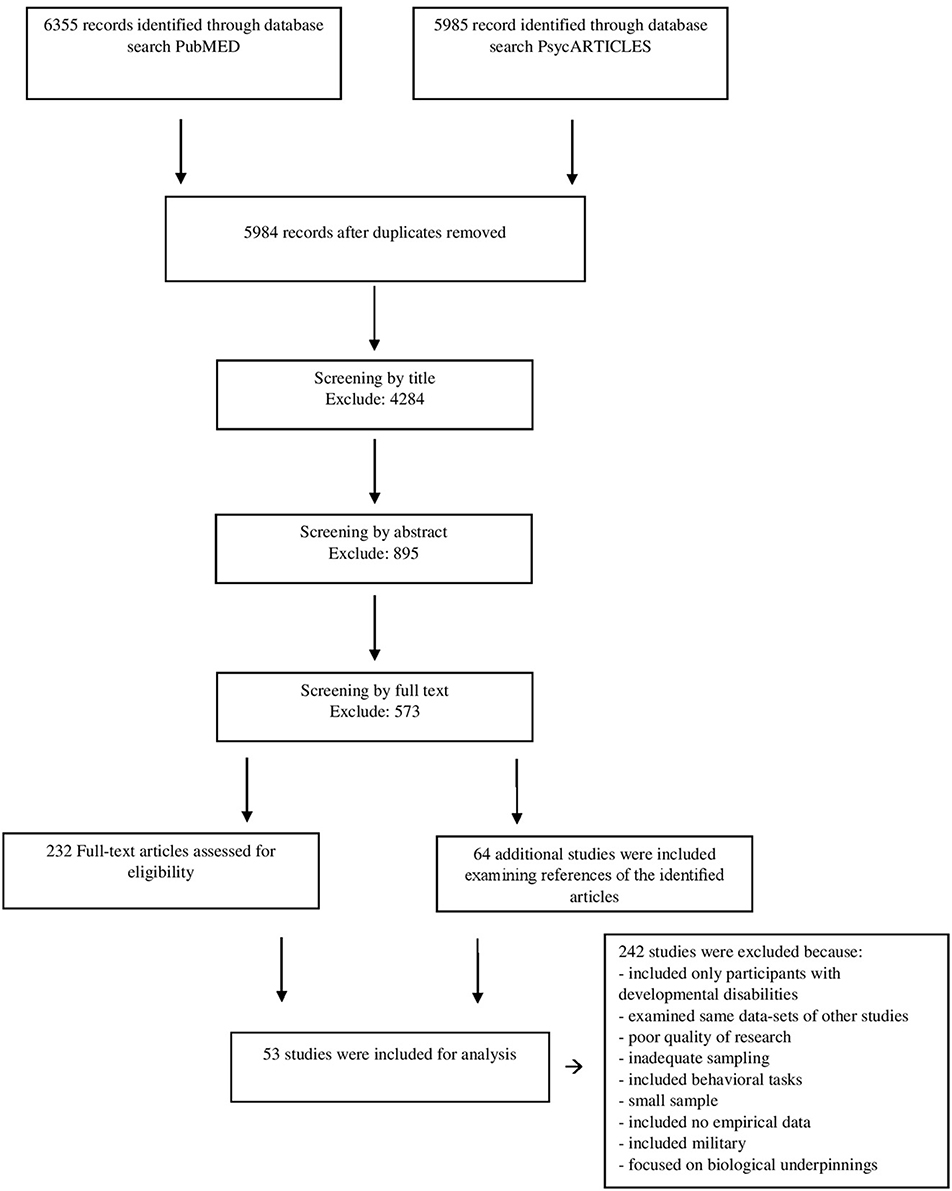
Figure 1. PRISMA flow diagram of study selection.
Inclusion/Exclusion Criteria
To be included in this review, studies had to: (a) be published between 1998 and 2016, (b) reported empirical data, (c) provide a definition of self-injury and of their method of assessment, (d) not focus on treatment for NSSI, (e) be published in the English language. There were no restrictions on participant.
Reason for exclusion were: (a) samples could be not categorized as universal, (b) studies were based on the same results already found in another publication, (c) the full text was not available.
Results
We identified 53 studies that met the inclusion criteria for this review. Table 1 provide a summary of the data obtained from each study.

Table 1. Study characteristics.
Diagnostic Criteria
Recent research on NSSI disorder (American Psychiatric Association, 2013) found that a high percentage of those who self-injure met the DSM-5 proposed criteria (Glenn and Klonsky, 2013; Washburn et al., 2015). In a community sample of 3,097 Swedish adolescents, Zetterqvist et al. (2013) found that 6.7% met the criteria, whereas in a sample of adolescent impatients prevalence was 50% (Glenn and Klonsky, 2013). Empirical data on a potential NSSI disorder have collected among clinical and community samples of adolescents and adults, using different version of proposed criteria (Shaffer and Jacobson, 2009; American Psychiatric Association, 2012, 2013). In a combination samples of inpatient and intensive outpatient subjects 85.5% met Criterion A (Washburn et al., 2015). Two hundred and five of adolescents reported frequent and multiple forms of NSSI (Zetterqvist et al., 2013). For Criterion B, high endorsement was found in clinical sample of adolescents and adults (In-Albon et al., 2013; Zetterqvist et al., 2013; Washburn et al., 2015), as well as in general adult samples (Andover, 2014; Gratz et al., 2015). Almost all of adolescents (99.5%) who fulfilled criteria for NSSI disorder reported engaging NSSI to relieve both intrapersonal and interpersonal difficulties (Zetterqvist et al., 2013), likewise most patients engaged in NSSI with the expectation to lead relief from either a negative feeling or cognitive state (82.0%) or resolution of an interpersonal problem (57.1%) (Washburn et al., 2015). Automatic functions are reported significantly more often than social functions, in adolescents and adults (Zetterqvist et al., 2013; Andover, 2014). In Washburn et al. (2015), it was also rare to meet Criterion B without also meeting Criterion C: C1 (American Psychiatric Association, 2013) was the most commonly endorsed symptom, but patients also reported high endorsement (62.4%) for all three symptoms.
Clinicians and expert NSSI researchers described experiencing negative feeling or through prior to the NSSI behavior as a prototypic symptom, following by preoccupation and urge to engage with a less agreement (Lengel and Mullins-Sweatt, 2013). Criterion D—behavior act for purposes not socially sanctioned—had an agreement of 88% as being relevant characteristic to the disorder (Lengel and Mullins-Sweatt, 2013). The presence of clinically significant distress or impairment (Criterion E) is considered difficult to assess, NSSI behavior would lead relief rather than impairing. NSSID group reported more distress and impairment in functioning than non-NSSID group (Zetterqvist et al., 2013; Andover, 2014; Gratz et al., 2015). Several studies have assessed Criterion F using indirect methods (e.g., In-Albon et al., 2013; Andover, 2014).
Epidemiology
Prevalence rates of NSSI in adolescents fall between 7.5 and 46.5%, rising to 38.9% among university students and 4–23% among adults (Briere and Gil, 1998; Gratz et al., 2002; Whitlock et al., 2006; Lloyd-Richardson et al., 2007; Hilt et al., 2008a; Plener et al., 2009; Cerutti et al., 2012; Andover, 2014). Although self-injurious behavior is a widespread phenomenon, data vary considerably across samples. The age onset of NSSI most often occurs in early adolescence, between 12 and 14 years (Nock et al., 2006; Muehlenkamp and Gutierrez, 2007; Cerutti et al., 2011), but findings have also reported NSSI behavior in children under the age of 12 (Barrocas et al., 2012). The most common method was self-cutting (over 70%) followed by head banging, scratching, hitting and burning (Briere and Gil, 1998; Laye-Gindhu and Schonert-Reichl, 2005; Gratz, 2006; Whitlock et al., 2006). However, most individuals who engage in NSSI employ more than one method (e.g., Whitlock et al., 2011) acting on the arms, legs, wrists and stomach (Whitlock et al., 2006; Lloyd-Richardson et al., 2007; Klonsky, 2011; Sornberger et al., 2012). The results from some studies suggested that women displayed more NSSI behaviors than males, in both clinical and non-clinical samples (Ross and Heath, 2002; Laye-Gindhu and Schonert-Reichl, 2005; Whitlock et al., 2006, 2011; Claes et al., 2007; Muehlenkamp and Gutierrez, 2007; Yates et al., 2008; Plener et al., 2009; Sornberger et al., 2012; Muehlenkamp et al., 2013). A meta-analysis by Bresin and Schoenleber (2015) demonstrated that women are slightly more likely than men to engage in NSSI.
Differences concern also the type of method chosen: self-cutting is most common among women, that were more likely than men to engage in methods of NSSI that generally involve blood (Sornberger et al., 2012), whereas hitting, burning and banging are most common among men (Laye-Gindhu and Schonert-Reichl, 2005; Claes et al., 2007). On the other hand, equal rates of NSSI between the genders have been reported within samples of adolescents, college students, and adults (Briere and Gil, 1998; Nock et al., 2006; Lloyd-Richardson et al., 2007; Hilt et al., 2008a; Cerutti et al., 2011, 2012; Kirchner et al., 2011; Kaess et al., 2013), as well as clinical samples of adults (Briere and Gil, 1998). Although no race differences were noted in NSSI rate among adolescents and university samples (Gratz et al., 2002; Hilt et al., 2008a), data on ethnic/minority groups are scarce. Within ethnically diverse sample, multiracial college students reported high prevalence rates (20.8%), followed by Caucasian (16.8) and Hispanic (17%) (Kuentzel et al., 2012). However, research on non-Caucasian subjects was limited to few countries. Among Chinese students prevalence rates of NSSI ranged 24.9–29.2% (Wan et al., 2015; Tang et al., 2016), likewise Zoroglu et al. (2003) reported that 21.4% of Turkish adolescents engage NSSI.
NSSI and Other Disorders
According to research literature, NSSI is often associated with several maladaptive outcomes. Most notably, there is an association between NSSI and the diagnosis of BPD (Briere and Gil, 1998; Nock et al., 2006; Glenn and Klonsky, 2013; Gratz et al., 2015). Although listed as a diagnostic criterion for BPD (DSM-5, American Psychiatric Association, 2013), NSSI may also occur in individuals who do not receive BPD diagnosis, and not every individual who receives BPD diagnosis engages in self-harm behaviors (e.g., In-Albon et al., 2013). Differences between NSSI-group and BPD-group would suggest to define NSSI as syndrome in its own right (Selby et al., 2012; Turner et al., 2015). Even though NSSI and suicidal behavior are distinct, suicide attempts and suicide ideation were found in both clinical and non-clinical samples of adolescents (Nock et al., 2006; Plener et al., 2009).
Exploring the association between NSSI and psychiatric diagnoses, several researchers have reported self-injurious behavior in a wide range of other disorders, such as post-traumatic stress disorder (PTSD), dissociative disorder, conduct disorder, obsessive-compulsive disorder, intermittent explosive disorder, anxiety and mood disorder, substance use disorder, bulimia, and dissociative identity disorder (Briere and Gil, 1998; Nock et al., 2006; Claes et al., 2007; Selby et al., 2012; Glenn and Klonsky, 2013; In-Albon et al., 2013; Gratz et al., 2015; Jenkins et al., 2015; Turner et al., 2015). Furthermore, in a study on DSH behavior among young Italian adults, individuals with a history of DSH, compared with individuals with no history of DSH, reported higher levels of dissociations and depersonalization (Cerutti et al., 2012). In addition, a relationship between NSSI and eating disorders often appears (Claes et al., 2001; Iannaccone et al., 2013; Eichen et al., 2016), although not all researchers confirm such an association (Selby et al., 2012). Cerutti et al. (2012) found that adults with NSSI history reported negative attitudes toward the body and lower levels of body protection. In both clinical and non-clinical samples, those who self-injury were more likely to report depressive symptomatology and anxiety (Ross and Heath, 2002; Muehlenkamp and Gutierrez, 2007; Giletta et al., 2012; Selby et al., 2012). Moreover, results provided significantly higher rates of both internalizing (Nock et al., 2006; Glenn and Klonsky, 2013; In-Albon et al., 2013) and externalizing disorders (Nock et al., 2006). Adolescents who engage in NSSI were more likely to present several health-risk behaviors, such as substance abuse, risky sexual behaviors, and maladaptive eating habits (Hilt et al., 2008a; Giletta et al., 2012). In a study that assess potential NSSI disorder (Gratz et al., 2015) participants who met the proposed criteria for NSSID (DSM-5, American Psychiatric Association, 2013) differed from NSSI-group and reported significantly more depression, anxiety and stress symptoms, and BPD disorder.
Etiology
The potential etiologic factors of NSSI may be divided into two major categories: individual (e.g., emotional dysregulation, psychiatric disorders) and environmental (e.g., childhood maltreatments, attachment disruption). Most research focused on early childhood traumatic experiences found that childhood maltreatments emerged as a predictor of NSSI within adolescents and college students (Paivio and McCulloch, 2004; Gratz, 2006; Arens et al., 2012; Auerbach et al., 2014; Wan et al., 2015). Exploration of environmental contributors revealed that childhood sexual abuse would present a strong link with NSSI development (Briere and Gil, 1998; Gratz et al., 2002; Gratz, 2006; Gratz and Chapman, 2007; Yates et al., 2008; Auerbach et al., 2014). However, other researchers have not found a strong association with sexual abuse (Zoroglu et al., 2003; Whitlock et al., 2006; Goldstein et al., 2009). In their study among college female students, Gratz (2006) found that both environmental and individual factors were strongly associated with NSSI, as well their interaction. Gratz et al. (2002) emphasized the role of parental relationship in the etiology of self-injurious behaviors: insecure paternal attachment and both maternal and paternal emotional neglect were significant predictors of NSSI within women, whereas NSSI in men was primarily predicted by childhood separation (usually from father). Furthermore, maternal rejection appeared the only significant predictor among psychiatric inpatients sample (Kaess et al., 2013).
Most recent studies have investigated the role of stress-full life events in the etiology of NSSI (Cerutti et al., 2011; Tang et al., 2016). Among Chinese adolescents, Tang et al. (2016) found that adverse life experiences were associated with moderate and severe NSSI and a lesser risk of engaging NSSI in those who had a good emotional regulation. Examining individual factors, results reported that NSSI frequency was strongly predicted by emotion dysregulation and affect intensity/reactivity within men (Gratz and Chapman, 2007), and by emotional inexpressivity within women (Gratz, 2006). Low emotional expressiveness would have a role in engagement in NSSI (Jacobson et al., 2015). Results of a regression analysis showed that difficulties to identify and express emotional experience appropriately (i.e., alexithymia) mediated the relation between childhood trauma (except sexual abuse) and NSSI (Paivio and McCulloch, 2004).
Functions
Engage in NSSI may serves several functions that are not mutually exclusive (Nock and Prinstein, 2004; Klonsky, 2011). The most common function seems to be the affect regulation (Nock and Prinstein, 2004; Laye-Gindhu and Schonert-Reichl, 2005; Claes et al., 2007; Muehlenkamp et al., 2013). Indeed, negative emotions, such as anger, anxiety, depression, and loneliness, tend to occur before the NSSI behavior, whereas an increase in positive emotions and a decrease in negative emotions would follow as well (e.g., Laye-Gindhu and Schonert-Reichl, 2005; Claes et al., 2007). Moreover, Giletta et al. (2012) found that engaging NSSI were strongly associated with depressive feelings among Italian, USA and Dutch samples. NSSI may represent a strategy for affect regulation (Laye-Gindhu and Schonert-Reichl, 2005). Nock and Prinstein (2004) proposed a functional model of NSSI, known as the Four Factor Model (FFM). FFM is grounded on behavioral theory, which focus on the antecedent and consequent influences that produce and maintain the behavior.
The FFM delineates two dichotomous dimensions of functional processes: contingencies interpersonal/social vs. intrapersonal/automatic, and reinforcement positive vs. negative. The four processes proposed by the model include: automatic negative reinforcement when NSSI serves to reduce aversive internal states, automatic positive reinforcement, when NSSI serves to generate positive feelings, social negative reinforcement, when NSSI serves to avoid interpersonal demands, and social positive reinforcement, when NSSI serves to gain attention, or increase social support (Nock and Prinstein, 2004). Much of the studies on the psychological reasons underlying the NSSI behavior has mainly focused on emotion regulation and tension reduction, but social functions of NSSI have also been described in both adolescents (Nock and Prinstein, 2004; Lloyd-Richardson et al., 2007; Hilt et al., 2008a,b; Turner et al., 2012; Muehlenkamp et al., 2013; Zetterqvist et al., 2013) and adults samples (Turner et al., 2012, 2016). Engaging NSSI “to stop bad feelings” was endorsed by 56.8% of German inpatients sample, in which automatic functions were predicted by adverse childhood experiences (Kaess et al., 2013). Self-punishment function was commonly endorsed by adolescents and adult among community and clinic samples (Briere and Gil, 1998; Laye-Gindhu and Schonert-Reichl, 2005; Lloyd-Richardson et al., 2007; Turner et al., 2012; Glenn and Klonsky, 2013; Kaess et al., 2013). Although males were more likely to engage NSSI for social reasons (Claes et al., 2007) and females to relieve negative emotional states and self-punishment (Briere and Gil, 1998; Glenn and Klonsky, 2013), no significant gender differences emerged about NSSI functions among adolescents samples (e.g., Lloyd-Richardson et al., 2007; Calvete et al., 2015). Zetterqvist et al. (2013) found that about 90% of adolescents those met proposed criteria for NSSI disorder most commonly reported automatic negative functions, followed by automatic positive ones, and about 27% reported social functions. Greater endorsement of intrapersonal functions than social was also found among adult with NSSI Disorder (Andover, 2014).
Discussion
The purpose of this study was to review the existing literature on NSSI by providing a preliminary understanding of the main features. There is general consensus that NSSI begins in early adolescence, with a main age onset of 12 years old. Even though only few studies have investigated NSSI within children younger than 12 years old (Kirchner et al., 2011; Barrocas et al., 2012; Sornberger et al., 2012). Prevalence is even high among adult, mostly in samples of university students. Studies have demonstrated a high variability on prevalence rates. Some of this variability may partially explain by a growing interest in NSSI behavior. Nevertheless, the assessment methods chosen appears to heavily influence the estimates of prevalence: checklists would seem to provide higher estimates than single item questions (Muehlenkamp et al., 2012).
In order to overcome the mentioned assessment bias, future research will have to accurately investigate perceptions and interpretations of participants which may not reflect NSSI definition provided. NSSI is generally assumed to be more common among females than men. This assumption is not fully supported by existing literature. Self-injury is popularly associated with “cutting” and this could have influenced data, as females are more likely to self-cut than men. Literature has primarily focused on women samples and higher prevalence on NSSI among females could be due to an over representation of women (Claes et al., 2007). Data on non-Caucasian samples are scarce, but it may be due to an ethnocentric bias that tend to underestimate the culture impact on NSSI. Indeed, similar rates of prevalence among female adolescent and methods used, in Chinese samples, could be consider a reflection of Western culture's influence, and NSSI in minorities group, such as Native Americans (e.g., Kuentzel et al., 2012), could be related to culturally sanctioned rituals (ceremonial or religious). Due to paucity of studies on racial/ethnic differences in NSSI, its distribution and prevalence remain unclear.
Regarding etiology, the relation between sexual abuse and NSSI remains still contentious. Evidence suggests that additional risk factors, both environmental and individual, may play a role in the etiology of NSSI: a history of child maltreatment and stressful life experiences could represent a vulnerability that disrupt emotional regulation function. Therefore, several forms of maltreatment appear to be related to engaging NSSI in both clinical and non-clinical samples (e.g., Briere and Gil, 1998; Gratz et al., 2002; Gratz, 2006; Yates et al., 2008; Arens et al., 2012; Auerbach et al., 2014), whereas individual factors might play a role in the maintenance of the behavior (e.g., Gratz and Chapman, 2007; Jacobson et al., 2015). So, a potential interaction between risk factors should be explored. Emotional regulation was the most common reason for NSSI behavior: individuals who self-injury commonly reported negative experiences, such as depression, anxiety, and angry, before NSSI. To further support automatic function, NSSI would result in a negative emotions reduction. Although interpersonal functions have not received as much attention, both adolescents and adult endorsed social reasons to engage NSSI (e.g., Nock and Prinstein, 2004; Lloyd-Richardson et al., 2007; Hilt et al., 2008b; Zetterqvist et al., 2013). Moreover, lower prevalence of social functions could be explained by the fact that NSSI is a private act and who self-injury may be socially isolated and experience negative emotions that increase the likelihood of further acts to reduce tension state. The inclusion of a potential NSSI disorder in the DSM-5 is justified by the clinical benefits that would ensue from a better understanding of the behavior.
Empirical research on NSSI disorder has recently begun to provide relevant data. It is however limited by the use of the different methods employed in assessing NSSI, and not originally envisaged for this purpose. There are several important obstacles regarding diagnostic validity of NSSID. Firstly, delimitation from other disorders. Self-injurious behavior primarily existed in the DSM as a symptom of BPD but, although NSSI and BPD can co-occur, they also present themselves independently (In-Albon et al., 2013). Most studies, focused on NSSI disorder rather than BPD, have highlighted that NSSI is not indicative of BPD and that the diagnostic coincidence of NSSI disorder and BPD was similar to existed to a lesser degree than BPD and other disorders (Glenn and Klonsky, 2013). Moreover, the introduction of NSSI disorder recognizes the importance of differentiating NSSI from attempted suicide. Although both suicide attempts and NSSI conform to a continuum of self-harming behaviors, there are important clinically differences among behaviors in etiology, psychiatric impairment, functions, methods and course. The use of diverse criteria, different assessment methodologies and the absence of studies employing all the criteria as proposed in the DSM-5, have deterred advancement in this field.
Strengths and Limitations
The current review not only includes women engaged in self-injury but also men, and goes some way to addressing the misrepresentation present in previous literature, which could be explained by the fact that men behave differently to women in this context. This study only addresses the links between NSSI and biological roots and developmental\intellectual disabilities in part, and does not address NSSI treatment. Our review attempted to understand the main causes and functions of NSSI through studies on clinical and non-clinical populations but many aspects remain unclear, especially as regard NSSI etiology. Finally, we must consider the secretive nature of self-injury due to which prevalence rates may be seen to be ambiguous. Studies on NSSI treatment were not included.
Implications for Future Research
Despite the behavior is more likely to present in adolescence, the variation in age of onset and in prevalence rates among adolescents and adults suggest that there may be different developmental trajectories in NSSI and a lack of knowledge regarding the course of NSSI: further exploration should employ a longitudinal approach aimed at examining the risk factors and progression of a potential NSSI disorder. This implication is directly related to the need for additional research using a variety of adult group to obtain accurate prevalence rates, as data on adult samples have mostly collected in educational institutions.
Findings on gender differences provided contradictory data that could benefit from future research that also consider other variables, such as culture, school, and social contagion. More research would be helpful in understanding the course and patterns of NSSI and exploring NSSI among gender. Research should be extended to other cultures and ethnicities, in order to recognize the influence of cultural factors on these behaviors. Self-injurious behavior for culturally sanctioned purposes (e.g., religious ritual, tattoos and piercings) was not considered in the research field nor included among the proposed diagnostic criteria for NSSID in the DSM-5. The contextualization of behavior is required, as is an exploration of the similarities and differences in prevalence rates, methods and functions across cultures. Although findings suggest the role of abuse, neglect and disruption in attachment in the potential development of NSSI behavior, future research could explore other characteristics of maltreatment experiences, such as frequency, perpetrator, bond type between child, and abuser, and cumulative effects.
There may be several reasons for engaging in NSSI and future research should investigate the mechanism underlying NSSI, the role of gender differences and whether functions change during development in order to a more complete understanding of the behavior. Moreover, there are still several areas that require further investigation to give credence to NSSI as a disorder in its own right: it would be pertinent to provide a valid, clinical delineation of the disorder and develop a standardized tool for its assessment in order to improve research, to conduct longitudinal studies and cross-cultural and ethnic studies, but there is still further work to be done.
Conclusions
NSSI is a common phenomenon among adolescents and adults, associated with significant impairment. Over the years, interest in NSSI grew to such an extent that an ongoing debate was instigated on whether NSSI should be considered as a diagnosis in its own right and given its own category. As a result, it was included in section 3 of the DSM-5 as a condition requiring further studies. This paper provides an up-to-date overview on self-injury, what is known about it and what remains to be done.
Author Contributions
AC and SC conducted the study, AC writes the first draft of the paper, PC designed the study and supervise the procedure and the paper.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
American Psychiatric Association (2012). Suggested Criteria for DSM-5 Non-Suicidal Self-injury Disorder. Washington, DC: American Psychiatric Association.
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Washington, DC: American Psychiatric Association.
Andover, M. S. (2014). Non-suicidal self-injury disorder in a community sample of adults. Psychiatry Res. 219, 305–310. doi: 10.1016/j.psychres.2014.06.001
Arens, A. M., Gaher, R. M., and Simons, J. S. (2012). Child maltreatment and deliberate self-harm among college students: testing mediation and moderation models for impulsivity. Am. J. Orthopsychiatry 82, 328–337. doi: 10.1111/j.1939-0025.2012.01165.x
Auerbach, R. P., Kim, J. C., Chango, J. M., Spiro, W. J., Cha, C., Gold, J., et al. (2014). Adolescent nonsuicidal self-injury: examining the role of child abuse, comorbidity, and disinhibition. Psychiatry Res. 220, 579–584. doi: 10.1016/j.psychres.2014.07.027
Barrocas, A. L., Hankin, B. L., Young, J. L., and Abela, J. R. (2012). Rates of nonsuicidal self- injury in youth: age, sex, and behavioural methods in a community sample. Pediatrics 130, 39–45. doi: 10.1542/peds.2011-2094
Bolognini, M., Plancherel, B., Laget, J., Stephan, P., and Halfon, O. (2003). Adolescents' self-mutilation – relationship with dependent behaviour. Swiss J. Psychol. 62, 241–249. doi: 10.1024/1421-0185.62.4.241
Bresin, K., and Schoenleber, M. (2015). Gender differences in the prevalence of nonsuicidal self-injury: a meta-analysis. Clin. Psychol. Rev. 38, 55–64. doi: 10.1016/j.cpr.2015.02.009
Briere, J., and Gil, E. (1998). Self-mutilation in clinical and general population samples: prevalence, correlates, and functions. Am. J. Orthopsychiatry 68, 609–620. doi: 10.1037/h0080369
Calvete, E., Orue, I., Aizpuru, L., and Brotherton, H. (2015). Prevalence and functions of non-suicidal self-injury in Spanish adolescents. Psychotema 27, 223–228. doi: 10.7334/psicothema2014.262
Cerutti, R., Manca, M., Presaghi, F., and Gratz, K. L. (2011). Prevalence and clinical correlates of deliberate self-harm among a community sample of Italian adolescents. J. Adolesc. 34, 337–347. doi: 10.1016/j.adolescence.2010.04.004
Cerutti, R., Presaghi, F., Manca, M., and Gratz, K. L. (2012). Deliberate self-harm behavior among italian young adults: correlations with clinical and nonclinical dimensions of personality. Am. J. Orthopsychiatry 82, 298–308. doi: 10.1111/j.1939-0025.2012.01169
Claes, L., Vandereycken, W., and Vertommen, H. (2001). Self-injurious behaviors in eating-disordered patients. Eat. Behav. 2, 263–272. doi: 10.1016/S1471-0153(01)00033-2
Claes, L., Vandereycken, W., and Vertommen, H. (2007). Self-injury in female versus male psychiatric patients: a comparison of characteristics, psychopathology and aggression regulation. Pers. Indiv. Dif. 42, 611–621. doi: 10.1016/j.paid.2006.07.021
Darche, M. A. (1990). Psychological factors differentiating self-mutilating and non-self-mutilating adolescent inpatient females. Psychiatr. Hosp. 21, 31–35.
DiClemente, R. J., Ponton, L. E., and Hartley, D. (1991). Prevalence and correlates of cutting behavior: risk for HIV transmission. J. Am. Acad. Child Adolesc. Psychiatry 30, 735–739. doi: 10.1016/S0890-8567(10)80007-3
Eichen, D. M., Kass, A. E., Fitzsimmons-Craft, E. E., Gibbs, E., Trockel, M., Taylor, B., et al. (2016). Non-suicidal self-injury and suicidal ideation in relation to eating and general psychopathology among college-age women. Psychiatr. Res. 235, 77–82. doi: 10.1016/j.psychres.2015.11.046
Favazza, A. R. (1992). Repetitive self-mutilation. Psychiatr. Ann. 22, 60–63. doi: 10.4236/health.2010.24055
Favazza, A. R. (1996). Bodies under Siege: Self-mutilation and Body Modification in Culture and Psychiatry, 2nd Edn. Baltimore, MD: John Hopkins University Press.
Favazza, A. R., and Conterio, K. (1988). The plight of chronic self-mutilators. Commun. Ment. Health J. 24, 22–30. doi: 10.1007/BF00755050
Favazza, A. R., and Conterio, K. (1989). Female habitual self-mutilators. Acta Psychiatr. Scand. 79, 283–289. doi: 10.1111/j.1600-0447.1989.tb10259.x
Favazza, A. R., DeRosear, L., and Conterio, K. (1989). Self-mutilation and eating disorders. Suicide Life Threat. Behav. 19, 352–361.
Favazza, A. R., and Rosenthal, R. J. (1990). Varieties of pathological self-mutilation. Behav. Neurol. 3, 77–85. doi: 10.3233/BEN-1990-3202
Favazza, A. R., and Rosenthal, R. J. (1993). Diagnostic issue in self-mutilation. Hosp. Commun. Psychiatry 44, 134–139. doi: 10.1176/ps.44.2.134
Giletta, M., Scholte, R. H., Engels, R. C., Ciairano, S., and Prinstein, M. J. (2012). Adolescent non-suicidal self-injury: a cross-national study of community samples from Italy, the Netherlands and the United States. Psychiatry Res. 197, 66–72. doi: 10.1016/j.psychres.2012.02.009
Glenn, C. R., and Klonsky, E. D. (2013). Nonsuicidal self-injury disorder: an empirical investigation in adolescent psychiatric patients. J. Clin. Child Adolesc. Psychol. 42, 496–507. doi: 10.1080/15374416.2013.794699
Goldstein, A. L., Glett, G. L., Wekerle, C., and Wall, A. (2009). Personality, child maltreatment, and substance use: examining correlates of deliberate self-harm among university students. Can. J. Behav. Sci. 41, 241–251. doi: 10.1037/a0014847
Graff, H., and Mallin, R. (1967). The syndrome of the wrist cutter. Am. J. Psychiatry 124, 74–80. doi: 10.1176/ajp.124.1.36
Gratz, K. L. (2006). Risk factors for deliberate self-harm among female college students: the role and interaction of childhood maltreatment, emotional inexpressivity, and affect intensity/reactivity. Am. J. Orthopsychiatry 76, 238–250. doi: 10.1037/0002-9432.76.2.238
Gratz, K. L., and Chapman, A. L. (2007). The role of emotional responding and childhood maltreatment in the development and maintenance of deliberate self-harm among male undergraduates. Psychol. Men Masculinity 8, 1–14. doi: 10.1037/1524-9220.8.1.1
Gratz, K. L., Conrad, S. D., and Roemer, L. (2002). Risk factors for deliberate self-harm among college students. Am. J. Orthopsychiatry 1, 128–140. doi: 10.1037/0002-9432.72.1.128
Gratz, K. L., Dixon-Gordon, K. L., Chapman, A. L., and Tull, M. T. (2015). Diagnosis and characterization of DSM-5 nonsuicidal self-injury disorder using the clinician administered nonsuicidal self-injury disorder index. Assessment 22, 527–539. doi: 10.1177/1073191114565878
Herpertz, S. (1995). Self-injurious behavior: psychopathological and nosological characteristics in subtypes of self-injurers. Acta Psychiatr. Scand. 91, 57–68. doi: 10.1111/j.1600-0447.1995.tb09743.x
Hilt, L. M., Cha, C. B., and Nolen-Hoeksema, S. (2008b). Nonsuicidal self-injury in young adolescent girls: moderators of the distress-function relationship. J. Consult. Clin. Psychol. 76, 63–71. doi: 10.1037/0022-006X.76.1.63
Hilt, L. M., Nock, M. K., Lloyd-Richardson, E. E., and Prinstein, M. J. (2008a). Longitudinal study of nonsuicidal self-injury among young adolescents: rates, correlates, and preliminary test of an interpersonal model. J. Early Adolesc. 28, 455–469. doi: 10.1177/0272431608316604
Iannaccone, M., Cella, S., Manzi, S. A., Visconti, L., Manzi, F., and Cotrufo, P. (2013). My body and me: self-injurious behaviors and body modifications in eating disorders—preliminary results. Eat. Disord. 21, 130–139. doi: 10.1080/10640266.2013.761087
In-Albon, T., Ruf, C., and Schmid, M. (2013). Proposed diagnostic criteria for the DSM-5 of nonsuicidal self-injury in female adolescents: diagnostic and clinical correlates. Psychiatry J. 2013:159208. doi: 10.1155/2013/159208
Jacobson, C. M., Hill, R. M., Pettit, J. W., and Grozeva, D. (2015). The association of interpersonal and intrapersonal emotional experiences with non-suicidal self-injury in young adults. Arch. Suicide Res. 19, 401–413. doi: 10.1080/13811118.2015.1004492
Jenkins, A. L., McCloskey, M. S., Kulper, D., Berman, M. E., and Coccaro, E. F. (2015). Self-harm behavior among individuals with intermittent explosive disorder and personality disorders. J. Psychiatr. Res. 60, 125–131. doi: 10.1016/j.jpsychires.2014.08.013
Kaess, M., Parzer, P., Mattern, M., Plener, P. L., Bifulco, A., Resch, F., et al. (2013). Adverse childhood experiences and their impact on frequency, severity, and the individual function of nonsuicidal self-injury in youth. Psychiatry Res. 206, 265–272. doi: 10.1016/j.psychres.2012.10.012
Kahan, J., and Pattison, E. M. (1984). Proposal for a distinctive diagnosis: the deliberate self-harm syndrome (DSH). Suicide Life Threat. Behav. 14, 17–35. doi: 10.1111/j.1943-278X.1984.tb00334.x
Kirchner, T., Ferrer, L., Forns, M., and Zanini, D. (2011). Self-harm behavior and suicidal ideation among high school students. Gender differences and relationship with coping strategies. Actas Esp. Psiquiatr. 39, 226–235.
Klonsky, E. D. (2007). The functions of deliberate self-injury: a review of the evidence. Clin. Psychol. Rev. 27, 226–239. doi: 10.1016/j.cpr.2006.08.002
Klonsky, E. D. (2011). Non-suicidal self-injury in United States adults: prevalence, sociodemographics, topography and functions. Psychol. Med. 41, 1981–1986. doi: 10.1017/S0033291710002497
Klonsky, E. D., and Muehlenkamp, J. J. (2007). Self-injury: a research review for the practitioner. J. Clin. Psychol. 63, 1045–1056. doi: 10.1002/jclp.20412
Klonsky, E. D., Oltmanns, T. F., and Turkheimer, E. (2003). Deliberate self-harm in a nonclinical population: prevalence and psychological correlates. Am. J. Psychiatry 160, 1501–1508. doi: 10.1176/appi.ajp.160.8.1501
Kuentzel, J. G., Arble, E., Boutros, N., Chugani, D., and Barnett, D. (2012). Nonsuicidal self-injury in an ethnically diverse college sample. Am. J. Orthopsychiatry 82, 291–297. doi: 10.1111/j.1939-0025.2012.01167.x
Laye-Gindhu, A., and Schonert-Reichl, K. A. (2005). Nonsuicidal self-harm among community adolescents: understanding the whats and whys of self-harm. J. Youth Adolesc. 34, 447–457. doi: 10.1007/s10964-005-7262-z
Lengel, G. J., and Mullins-Sweatt, S. N. (2013). Nonsuicidal self-injury disorder: clinician and expert ratings. Psychiatry Res. 210, 940–944. doi: 10.1016/j.psychres.2013.08.047
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P. A., et al. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Br. Med. J. 339:b2700. doi: 10.1136/bmj.b2700
Lloyd-Richardson, E. E., Perrine, N., Dierker, L., and Kelley, M. L. (2007). Characteristics and functions of non-suicidal self-injury in a community sample of adolescents. Psychol. Med. 37, 1183–1192. doi: 10.1017/S003329170700027X
Muehlenkamp, J. J. (2005). Self-injurious behavior as a separate clinical syndrome. Am. J. Orthopsychiatry 75, 324–333. doi: 10.1037/0002-9432.75.2.324
Muehlenkamp, J. J., Brausch, A., Quigley, K., and Whitlock, J. (2013). Interpersonal features and functions of nonsuicidal self-injury. Suicide Life Threat. Behav. 2013, 43–67. doi: 10.1111/j.1943-278X.2012.00128.x
Muehlenkamp, J. J., Claes, L., Havertape, L., and Plener, P. L. (2012). International prevalence of adolescent non-suicidal self-injury and deliberate self-harm. Child Adolesc. Psychiatry Ment. Health 6, 1–9. doi: 10.1186/1753-2000-6-10
Muehlenkamp, J. J., and Gutierrez, P. M. (2007). Risk for suicide attempts among adolescents who engage in non-suicidal self-injury. Arch. Suicide Res. 11, 69–82. doi: 10.1080/13811110600992902
Nock, M. K. (2010). Self-injury. Annu. Rev. Clin. Psychol. 6, 339–363. doi: 10.1146/annurev.clinpsy.121208.131258
Nock, M. K., Joiner, T. E., Gordon, K. H., Lloyd-Richardson, E., and Prinstein, M. J. (2006). Nonsuicidal self-injury among adolescents: diagnostic correlates and relation to suicide attempts. Psychiatry Res. 144, 65–72. doi: 10.1016/j.psychres.2006.05.010
Nock, M. K., and Prinstein, M. J. (2004). A functional approach to the assessment of self mutilative behavior. J. Clin. Consult. Psychol. 72, 885–890. doi: 10.1037/0022-006X.72.5.885
Paivio, S. C., and McCulloch, C. R. (2004). Alexithymia as a mediator between childhood trauma and self-injurious behaviours. Child Abuse Negl. 28, 339–354. doi: 10.1016/j.chiabu.2003.11.018
Pao, P. (1969). The syndrome of delicate self cutting. Br. J. Med. Psychol. 42, 213–221. doi: 10.1111/j.2044-8341.1969.tb02071.x
Pattison, E. M., and Kahan, J. (1983). The deliberate self-harm syndrome. Am. J. Psychiatry 140, 867–872. doi: 10.1176/ajp.140.7.867
Plener, P. L., Libal, G., Keller, F., Fegert, J. M., and Muehlenkamp, J. J. (2009). An international comparison of non-suicidal self-injury (NSSI) and suicide attempts: Germany and the USA. Psychol. Med. 39, 1549–1558. doi: 10.1017/S0033291708005114
Regier, D. A., Narrow, W. E., Clarke, D. E., Kraemer, H. C., Kuramoto, S. J., Kuhl, E. A., et al. (2013). DSM-5 field trials in the United States and Canada, part II: test–retest reliability of selected categorical diagnoses. Am. J. Psychiatry 170, 59–70. doi: 10.1176/appi.ajp.2012.12070999
Rosenthal, R., Rinzler, C., Wallsch, R., and Klausner, E. (1972). Wrist-cutting syndrome: the meaning of a gesture. Am. J. Psychiatry 128, 1363–1368. doi: 10.1176/ajp.128.11.1363
Ross, S., and Heath, N. (2002). A study of the frequency of self-mutilation in a community sample of adolescents. J. Youth Adolesc. 31, 67–77. doi: 10.1023/A:1014089117419
Selby, E. A., Bender, T. W., Gordon, K. H., Nock, M. K., and Joiner, T. E. (2012). Non-suicidal selfinjury (NSSI) disorder: a preliminary study. Personal. Disord. 3, 167–175. doi: 10.1037/a0024405
Selby, E. A., Kranzler, A., Fehling, K. B., and Panza, E. (2015). Nonsuicidal self-injury disorder: the path to diagnostic validity and final obstacles. Clin. Psychol. Rev. 38, 79–91. doi: 10.1016/j.cpr.2015.03.003
Shaffer, D., and Jacobson, C. (2009). Proposal to the DSM-V Childhood Disorder and Mood Disorder Work Groups to Include Non-Suicidal Self-Injury (NSSI) as a DSM-V disorder. Washington, DC: American Psychiatric Association.
Simeon, D., and Favazza, A. R. (2001). “Self-injurious behaviors: Phenomenology and assessment,” in Self-Injurious Behaviors: Assessment and Treatment, eds D. Simeon and E. Hollander (Washington, DC: American Psychiatric Publishing), 1–28.
Sornberger, M. J., Heath, N. L., Toste, J. R., and McLouth, R. (2012). Nonsuicidal self-injury and gender: patterns of prevalence, methods, and locations among adolescents. Suicide Life Threat. Behav. 42, 266–278. doi: 10.1111/j.1943-278X.2012.0088.x
Suyemoto, K. L. (1998). The functions of self-mutilation. Clin. Psychol. Rev. 18, 531–554. doi: 10.1016/S0272-7358(97)00105-0
Suyemoto, K. L., and MacDonald, M. L. (1995). Self-cutting in female adolescents. Psychotherapy 32, 162–171. doi: 10.1037/0033-3204.32.1.162
Swannell, S. V., Martin, G. E., Page, A., Hasking, P., and St John, M. J. (2014). Prevalence of nonsuicidal self-injury in nonclinical samples: systematic review, meta-analysis and meta-regression. Suicide Life Threat. Behav. 44, 273–303. doi: 10.1111/sltb.12070
Tang, J., Yang, W., Ahmed, N. I., Ma, Y., Liu, H., Wang, J., et al. (2016). Stressful life events as a predictor for nonsuicidal self-injury in southern Chinese adolescence. Medicine 95:e2637. doi: 10.1097/MD.0000000000002637
Tantam, D., and Whittaker, J. (1992). Personality disorder and self-wounding. Br. J. Psychiatry 161, 451–464. doi: 10.1192/bjp.161.4.451
Turner, B. J., Chapman, A. L., and Layden, B. K. (2012). Intrapersonal and interpersonal functions of non-suicidal self-injury: associations with emotional and social functioning. Suicide Life Threat. Behav. 42, 36–55. doi: 10.1111/j.1943-278X.2011.00069.x
Turner, B. J., Cobb, R. J., Gratz, K. L., and Chapman, A. L. (2016). The role of interpersonal conflict and perceived social support in nonsuicidal self-injury in daily life. J. Abnorm. Psychol. 125, 588–598. doi: 10.1037/abn0000141
Turner, B. J., Dixon-Gordon, K. L., Austin, S. B., Rodriguez, M. A., Rosenthal, M. Z., and Chapman, A. L. (2015). Non-suicidal self-injury with and without borderline personality disorder: differences in self-injury and diagnostic comorbidity. Psychiatry Res. 230, 28–35. doi: 10.1016/j.psychres.2015.07.058
Wan, Y., Chen, J., Sun, Y., and Tao, F. B. (2015). Impact of childhood abuse on the risk of non-suicidal self-injury in mainland Chinese adolescents. PLoS ONE 10:e0131239. doi: 10.1371/journal.pone.013123
Washburn, J. J., Potthoff, L. M., Juzwin, K. R., and Styer, D. M. (2015). Assessing DSM-5 nonsuicidal self-injury disorder in a clinical sample. Psychol. Assess. 27, 31–41. doi: 10.1037/pas0000021
Whitlock, J., Eckenrode, J., and Silverman, D. (2006). Self-injurious behaviors in a college population. Pediatrics 117, 1939–1948. doi: 10.1542/peds.2005-2543
Whitlock, J., Muehlenkamp, J. J., Purington, A., Eckenrode, J., Barreira, J., Abrams, G. B., et al. (2011). Non-suicidal self-injury in a college population: general trends and sex differences. J. Am. College Health 59, 691–698. doi: 10.1080/07448481.2010.529626
Wilkinson, P., and Goodyer, I. (2011). Non-suicidal self-injury. Eur. Child Adolesc. Psychiatry 20, 103–108. doi: 10.1007/s00787-010-0156-y
Yates, T. M., Tracy, A. J., and Luthar, S. S. (2008). Nonsuicidal self-injury among “privileged” youths: longitudinal and cross-sectional approaches to developmental process. J. Consult. Clin. Psychol. 76, 52–62. doi: 10.1037/0022-006X.76.1.52
Zetterqvist, M., Lundh, L. G., Dahlström, Ö., and Svedin, C. G. (2013). Prevalence and function of non-suicidal self-injury (NSSI) in a community sample of adolescents, using suggested DSM-5 criteria for a potential NSSI disorder. J. Abnorm. Child Psychol. 41, 759–773. doi: 10.1007/s10802-013-9712-5
Keywords: deliberate self-harm, self-injury, nonsuicidal self-injury, NSSI, DSM-5
Citation: Cipriano A, Cella S and Cotrufo P (2017) Nonsuicidal Self-injury: A Systematic Review. Front. Psychol. 8:1946. doi: 10.3389/fpsyg.2017.01946
Received: 24 May 2017; Accepted: 23 October 2017;
Published: 08 November 2017.
Edited by:
Yossi Levi-Belz, Ruppin Academic Center, IsraelReviewed by:
Timo Partonen, National Institute for Health and Welfare, FinlandDiane Carol Gooding, University of Wisconsin-Madison, United States
Copyright © 2017 Cipriano, Cella and Cotrufo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paolo Cotrufo, cGFvbG8uY290cnVmb0B1bmljYW1wYW5pYS5pdA==