 José María Llorente1,2
José María Llorente1,2 Bárbara Oliván-Blázquez1,3,4*
Bárbara Oliván-Blázquez1,3,4* María Zuñiga-Antón5
María Zuñiga-Antón5 Bárbara Masluk1,3,4
Bárbara Masluk1,3,4 Eva Andrés6
Eva Andrés6 Javier García-Campayo1,2,4,7
Javier García-Campayo1,2,4,7 Rosa Magallón-Botaya1,2,4,7
Rosa Magallón-Botaya1,2,4,7- 1Health Research Institute of Aragon, Zaragoza, Spain
- 2Aragones Health Service, Zaragoza, Spain
- 3Department of Psychology and Sociology, University of Zaragoza, Zaragoza, Spain
- 4Primary Care Prevention and Health Promotion Network (RedIAPP), Madrid, Spain
- 5Department of Geography and Territorial Planning, University of Zaragoza, Zaragoza, Spain
- 6Department of Applied Economics, Autonomous University of Madrid, Madrid, Spain
- 7Department of Medicine and Psychiatry, University of Zaragoza, Zaragoza, Spain
Major depression etiopathogenesis is related to a wide variety of genetics, demographic and psychosocial factors, as well as to environmental factors. The objective of this study is to analyze sociodemographic and environmental variables that are related to the prevalence of depression through correlation analysis and to develop a regression model that explains the behavior of this disease from an ecological perspective. This is an ecological, retrospective, cross-sectional study. The target population was 1,148,430 individuals over the age of 16 who were registered in Aragon (Spain) during 2010, with electronic medical records in the community’s primary health care centers. The spatial unit was the Basic Health Area (BHA). The dependent variable was the diagnosis of Depression and the ecological independent variables were: Demographic variables (gender and age), population distribution, typology of the entity, population structure by sex and age, by nationality, by education, by work, by salary, by marital status, structure of the household by number of members, and state of the buildings. The results show moderate and positive correlations with higher rates of depression in areas having a higher femininity index, higher population density, areas with a higher unemployment rate and higher average salary. The results of the linear regression show that aging +75 and rural entities act as protective factors for depression, while urban areas and deficient buildings act as risk factors. In conclusion, the ecological methodology may be a useful tool which, together with the statistical epidemiological analysis, can help in the political decision making process.
Introduction
Depression is a highly prevalent mental disorder in our society, with 10–20% of the population experiencing a depressive disorder during their lives (Üstün et al., 2004; Bromet et al., 2011; Gutiérrez-Fraile et al., 2011). Depression increases the risk for early mortality and has become the second most common cause of disease-induced disability in our developed society (Gabilondo et al., 2010; Stegmann et al., 2010; Ferrari et al., 2013). In addition, it is the most expensive mental disorder in Europe, representing 1% of the total European economy (Sobocki et al., 2006; Mykletun et al., 2009).
Major depression etiopathogenesis is related to a wide variety of genetic (Cervilla et al., 2006, 2007) demographic and psychosocial factors (Patten et al., 2009; Bellón et al., 2011; Hidaka, 2012; Kupfer et al., 2012) as well as to environmental factors (Probst et al., 2006; Annequin et al., 2015; O’Hare et al., 2016). The most frequently studied sociodemographic factors, related to depression are: gender (Weissman and Olfson, 1995; Aragonès Benaiges et al., 2003; Barry et al., 2008); age (Roberts et al., 1997; Weissman and Wickramaratne, 2000; Gum et al., 2009; Kessler et al., 2010; Trainor et al., 2013); ethnic group (Somervell et al., 1989; Kessler, 2003) cultural and educational level (Kempen et al., 1999; Koster et al., 2006; Weich et al., 2007; Bjelland et al., 2008); marital status and relationship (Whisman and Bruce, 1999; Lorant et al., 2007; Plaisier et al., 2008) social relationship and social support (Stansfeld et al., 2003; Leskela et al., 2004; Brugha et al., 2005; Kendler, 2005; Golden et al., 2009; Lino et al., 2013); and socioeconomic level and unemployment (Weich and Lewis, 1998; Lorant et al., 2003, 2007). Other analyzed risk factors are comorbidity with other physical and psychiatric diseases (Sekula et al., 2003; Djernes, 2006), disability (Spijker et al., 2004), experiences of discrimination (Karlsen et al., 2005) and abuse in childhood (Rohde et al., 2008), work demands (Plaisier et al., 2007), stressful life events (Patton et al., 2003; Bos et al., 2007) etc.
In response to these researches, a scarce bibliography exists, that delves into the association between environmental factors and the prevalence and/or etiopathogenesis of depression. The most frequently studied environmental factors have been the influence of the rural or urban residence, the proximity to natural spaces or social interaction, physical environment, climatology, or changes in temperatures. Regarding the rural/urban residence, several studies state that depression rates in rural areas are lower once adjusting for confounding factors (Wang, 2004; Weich et al., 2006). This may be explained by a higher sense of belonging to their community and higher social support (Romans et al., 2011). As for climatology, a relationship has been found between climatic factors such as ambient temperature, light duration and changing and extreme climates, and depression (Jessen et al., 1998; Gaxiola-Robles et al., 2013); other factors such as a favorable environment and the proximity to natural spaces have been related to a better well-being and mood (Regan and Horn, 2005; Ryan et al., 2010; Berman et al., 2012). However, this bibliography does not analyze collective environmental factors and there are few studies that address them from an ecological perspective.
The objective of this study is to analyze sociodemographic and environmental variables that are related to the prevalence of depression through correlation analysis and to develop a regression model that explains the behavior of this disease from an ecological perspective. The hypothesis of this study is that sociodemographic variables are related with the prevalence of depression, with different strength, and direction, as protector or risk factors.
Materials and Methods
Design
This is an ecological, retrospective, cross-sectional study.
Setting and Study Population
The target population was 1,148,430 individuals over the age of 16 who were registered in Aragon (Spain) during 2010, with electronic medical records in the community’s primary health care centers. The autonomous community under study has an area of 47,719 square Km and a population density of 28.20 inhabitants per square kilometer. Its population is over-aged, which is more concentrated in rural areas, with the capitals having a younger population structure. The capital of the community (Zaragoza) contains half of the population and there are only thirteen municipalities that exceed 10,000 inhabitants. Rural nuclei (with less than 2000 inhabitants) represent 86% of the municipalities, where only 16.8% of the population lives.
The population pyramid graph related to Aragon, in Figure 1, shows a contracting structure. On one hand, the main groups by age are 30–49 age people (active population), this age group has been increased by the significant arrival of immigrant population since 2000. On the other hand, the importance of the population over 65 is growing significantly since the beginning of the century. This is a common feature in all developed regions and an element to be taken into account in government and health policies. The origin of this situation is double: an important decrease of fertility rates in the region and an increase of Life expectancy at birth, especially in the older cohorts. The pyramid allows to see that Crude birth rates are low, because the first cohorts (0–4 years old) are a low number, and Crude death rates are low, also.
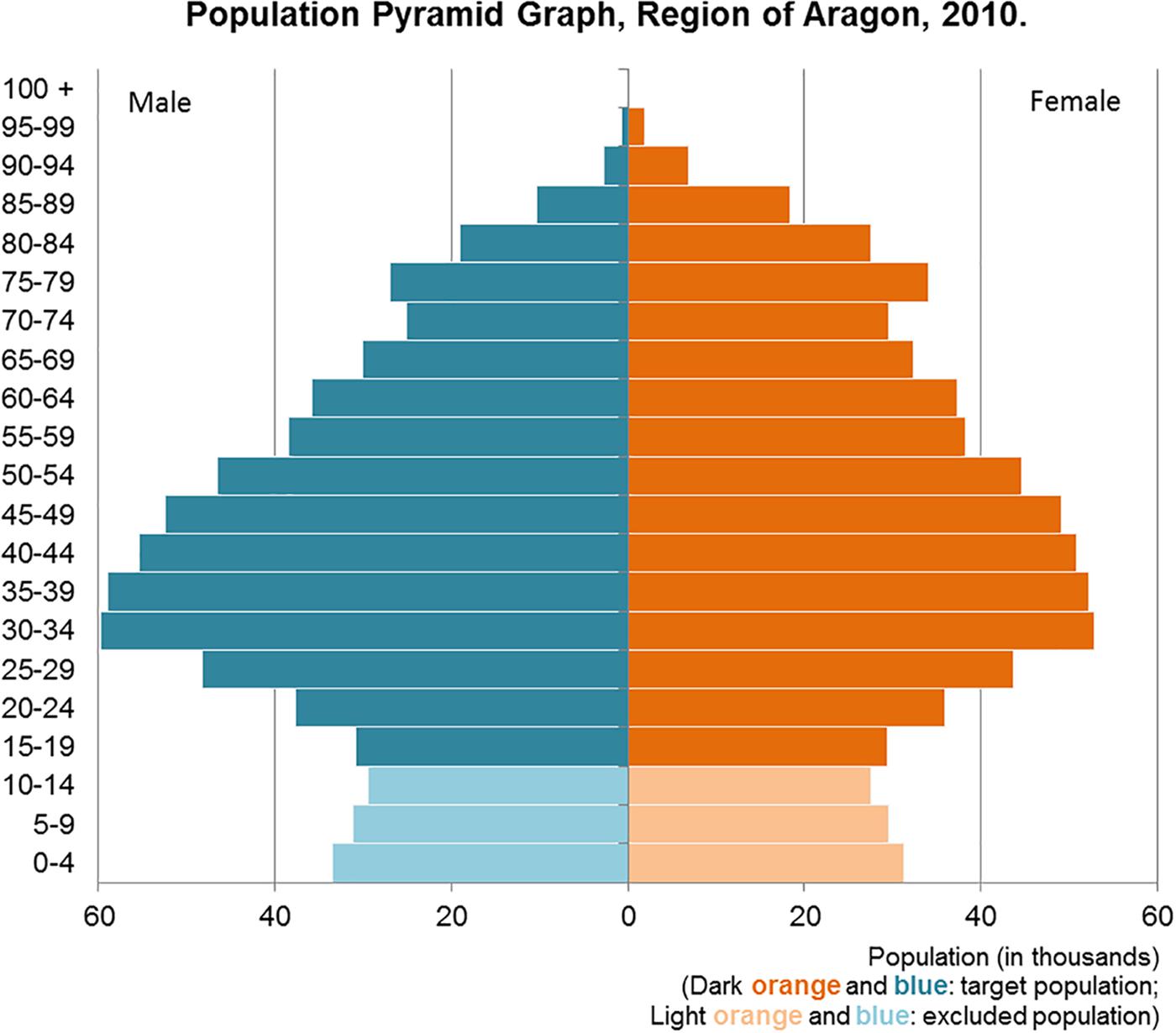
FIGURE 1. Population Pyramid Graph. Region of Aragon. 2010.
The sample of this study consists of all individuals having open electronic medical records in health centers of the autonomous community of Aragon (Spain), for at least 2 years during the time of entry into the study, including patients with an active diagnosis of depression during the year of the study. Records containing inconsistencies in the database were excluded from the study. These were the cases of patients with diagnosis of death and those revealing less than one doctor’s visits during the year of analysis.
Due to the universal nature of the health system and the absence of other primary health care providers, the data obtained in the study is considered to be representative of practically 100% of the population that met the criteria for inclusion in the study.
Outcomes and Instruments
The spatial unit in which both the dependent and independent variables were correlated was the Basic Health Area (BHA).
The dependent variable of the study was the diagnosis of Depression, for which the International Classification in Primary Care (ICPC) of the World Organization of Family Doctors (WONCA) was used. This data was collected from electronic medical records of all primary care patients in the community.
The ecological independent variables of the study were related to the prevalence of depression, which have been found in previous studies in the literature consulted. These variables were: Demographic variables (gender and age), population distribution, typology of the entity, population structure by sex and age, by nationality, by education, by work, by salary, by marital status, structure of the household by number of members, and state of the buildings. For each of these variables, the source of information, the scale of work, and the indicators used are indicated below, in Table 1. These variables were collected from the data for the year 2010.
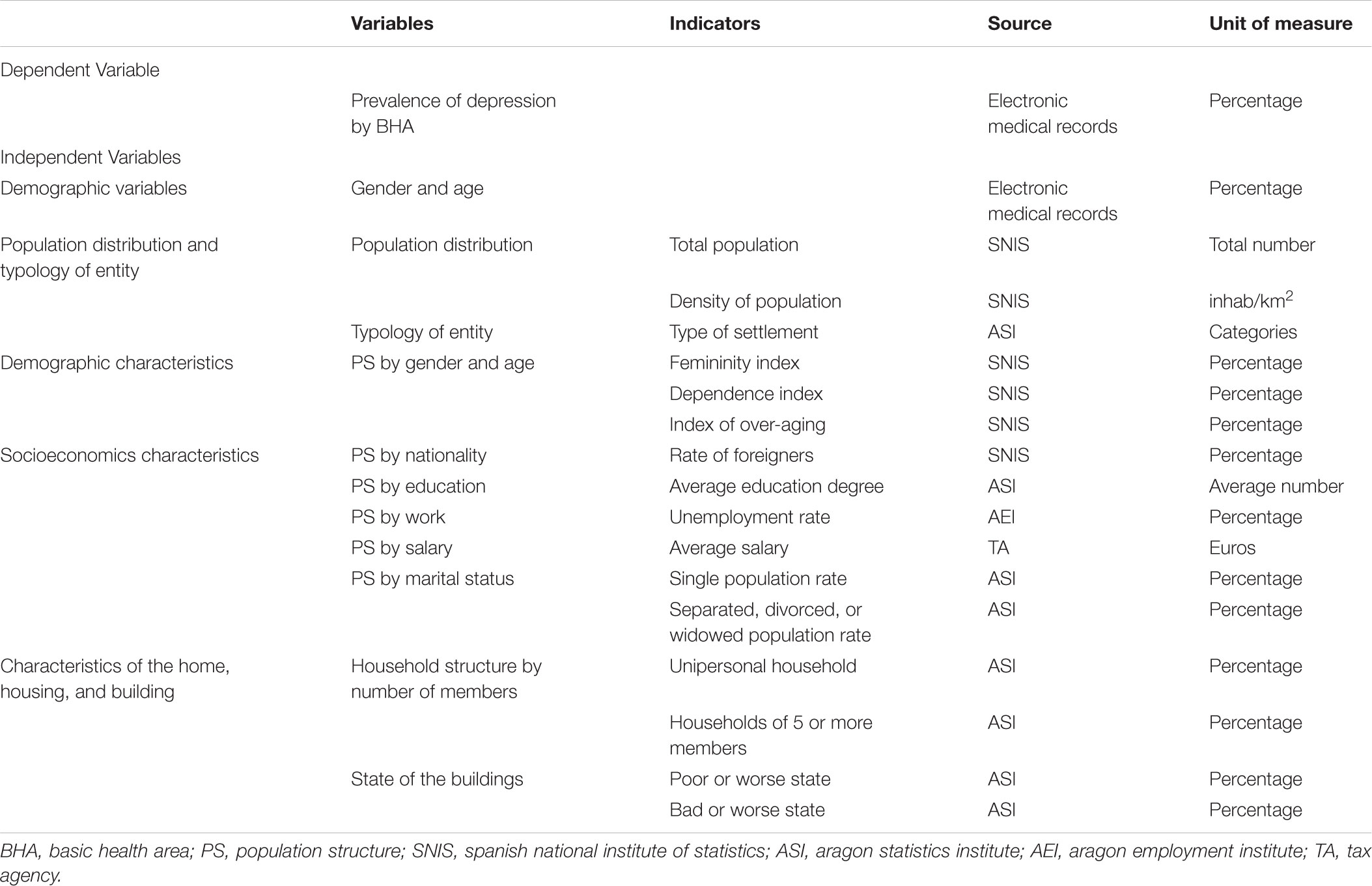
TABLE 1. Variables of the study, indicators, sources, and units of measure.
Analyzed demographic variables were gender and age, collected from electronic medical records.
The population distribution variable was measured with the following indicators: (1) total population, measured by total number; and (2) population density, measured by inhabitants per square kilometer71. This variable was collected according to the official figures of Population of Spanish Municipalities of the Spanish National Institute of Statistics (SNIS).
The Typology of entity variable, following the standard classification collected by the Aragon Statistics Institute (ASI, 2010), was classified as Rural zone: made up of municipalities of up to 2,000 inhabitants; intermediate zone: made up of municipalities from 2,001 to 10,000 inhabitants; and urban area: made up of municipalities with over 10,000 inhabitants. This variable was collected from the official figures of the Aragon Statistics Institute (ASI, 2010).
The variable of population structure by sex and age was measured based on the following indicators: (1) femininity index that is expressed as the number of women per 100 men, expressed as a percentage; (2) dependence index indicating the number of people under 15 and over 64 years old per 100 people between the ages of 15 and 64. It is expressed in percentage; and (3) index of over-aging (75 and 85), which indicates the number of people aged 75 years old and over; and of 85 years old and over, per 100 people aged 65 years and over (Reques Velasco, 2010). These indicators are expressed in percentages. They were obtained from the Official Population Figures from Spanish Municipalities compiled by the SNIS.
The Structure of the population by nationality variable was measured using the rate of foreigners, defined as the number of foreigners out of the total population of a BHA and expressed as the number of foreigners per 100 individuals (percentage). These data were obtained from the Official Population Figures from Spanish Municipalities compiled by the Spanish National Institute of Statistics (SNIS, 2010).
The Structure of the population by education variable was measured using the average grade of education indicator, which is the sum of class marks of the level of studies of people aged 16 and over divided by the total number of people of those ages residing in the studied territory. The class mark is the half-sum of the extremes of the interval and represents a central value of it. It is expressed as a value between 1 and 4 corresponding to (1) Without studies, (2) First grade, (3) Second grade and (4) Third grade. It represents a mean value. These data were obtained from the Population and Housing Censuses of the ASI.
The Structure of the population by work variable was collected using the unemployment rate as an indicator, which is defined as the percentage of the population in an unemployment situation with respect to the total population between 16 and 65 years of age. It is expressed as a percentage. These data were obtained from the Labor, Wages and Labor Relations Statistics of the Aragon Employment Institute (AEI, 2010).
The Structure of the population by salary variable was recollected using the Average Salary as an indicator, which is considered the average salary of each inhabitant in thousands of euros, understood as the relationship between perceptions, and payments. It is therefore quantified in euros. These data were obtained from the labor market database and pensions in the tax sources (Tax Agency based on the Annual Withholding Tax on Labor Income Tax Return (Tax Agency, 2010).
The Structure of the population by marital status variable, was collected according to the following indicators: (1) Single Population rate, understood as the ratio between the number of people with single marital status and the total number of people over 16 years of age; and (2) the rate of a separated, divorced or widowed population, understood as the ratio between the number of persons with a personal status of separated, divorced, or widowed and the total number of persons over 16 years of age. Both indicators are expressed in percentages. The rate of married population was not considered as being complementary to the analyzed rates and as a protective factor against depression, especially in men (Plaisier et al., 2008). This variable was collected from the Population and Housing Census, of the ASI.
The Household structure by number of members variable was collected using the following indicators: (1) unipersonal households, understood as the relationship between the number of households of a single member and the total number of households; and (2) households of 5 or more members, understood as the ratio between the number of households composed of 5 or more members and the total number of households. Both indicators are expressed in percentages. These data were obtained from the Population and Housing Censuses of the ASI.
The state of the buildings variable was collected using the following indicators: (1) Poor or worse state of the buildings, which is the percentage of buildings that, in the last census, were classified as a decaying, bad, or deficient building in relation to the total of buildings, and (2) Buildings in bad or worse condition, which is the percentage of buildings that were classified as decaying or bad in relation to the total number of buildings in the last census. The data was obtained from the Population and Housing Censuses of the ASI.
Accessibility to equipment and services has not been included as a variable in the analysis, since these data were not available for the entire autonomous community.
Statistical Analysis
The unit used to correlate and analyze the studied variables is the BHA, as a delimitation of the territorial framework in which the primary care professionals act. The average population of a BHA in Aragon is 10,622.01 inhabitants (SD: 8,762.522).
For the representation of the initial descriptive study in the model, direct standardization is carried out on the cases observed by age and sex. Age and sex are shown as two confounding factors in relation to morbidity, as confirmed by the literature (Kessler, 2003; Urbina Torija et al., 2007). In order to control their effect, specific prevalence rates are calculated by groups of sex and age by BHA with Epidat 3.1®.
From an ecological epidemiological perspective, the variables are described using average value or percentages, according to the type of variable. Subsequently, correlations are established and a multiple linear regression is performed. A binary dummy variable is created for inclusion in the study, from a qualitative variable such as the type of entity: Urban, Intermediate and Rural. Decomposing the Rural entity as value “0” in the two dummy variables (URB1 = 0, URB2 = 0), the Intermediate entity has the values (URB1 = 0, URB2 = 1) and the Urban entity has the values (URB1 = 1, URB2 = 0).
Results
During 2010, 62,804 people experienced an active process of depression and visited their family physician. This supposes a prevalence of 5.67%, with an average age of 59.50 years and with a greater proportion in women (3 women for each man). The female subgroup revealed a progressive and rapid increase in the prevalence curve of depression up to 55 years, then stabilizing and reaching a plateau up to 65 years of age, with abrupt and decrease occurring between 65 and 74 and then having another equally sharp rise until 80. In the male subgroup, there was a slow progressive increase in the number of prevalent cases of depression until the age of 50; there was a tendency to stabilize until the age of 64, only to descend slowly with a small increase until 77–80 years.
Analyzing by BHAs, the depression prevalence obtained is 4.55% (CI 4.20–4.89), with an interquartile range (Q3–Q1) of 2.97 and a range of 8.36. This gives us an idea of the differences found in the prevalence rates throughout the analyzed territory. A maximum value of 8.79% appears in a BHA in the main nucleus of Aragon (Zaragoza), with a lower prevalence of depression outside the main population centers of Aragon.
The correlations between the adjusted prevalence rates of depression by BHA and the analyzed variables are shown in Table 2. The Pearson P statistic was used for the variables over-aging, widowed/separated/divorced, foreigners and middle-school; whereas in the analysis of the rest of the variables, Spearman’s rho statistic has been used since they are ordinal variables or do not follow a normal distribution. It may be observed that the moderate and positive correlations appear with higher rates of depression in areas having a higher femininity index, higher population density, areas with a higher unemployment rate and higher average salary. And a positive weak correlation is seen in relation to the percentage of singles.
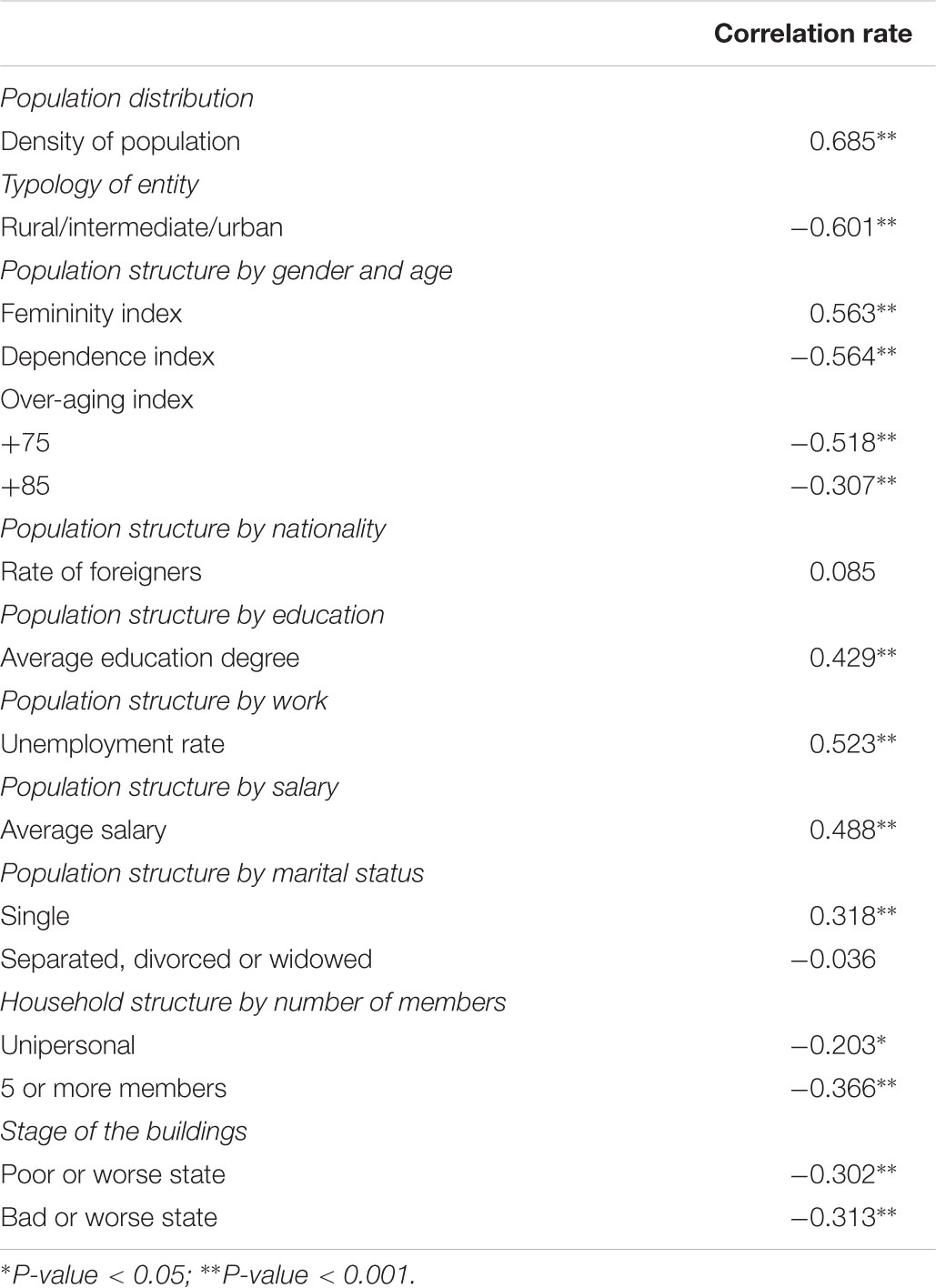
TABLE 2. Correlations between the prevalence of depression and the variables studied.
Weak and negative correlations are found in relation to the state of buildings and the household structure according to the number of people. In relation to the category of BHA, depending on whether they are located in an urban, intermediate or rural environment; a moderate negative correlation has been found. This indicates that there are lower rates of depression in rural areas. Negative and moderate correlations have also been found in relation to the dependency rate and the aging index.
In order to predict the depression prevalence rates of a BHA, an explanatory model was developed based on the following variables: urban/intermediate/rural decomposed into Dummy variables; over-aging-75 and percentage of the state of the building in poor or worse condition. Obtaining a square R = 0.422, which would mean that the model would explain 42.2% of the variability of depression prevalence rates and with a significant linear relationship in ANOVA with a significance coefficient < 0.001.
The coefficients that would make up the equation: over-aging-75 with a coefficient B = -1.646, meaning that each increase by one unit in over-aging corresponds to a decrease of 1.646 in the prevalence rate of depression. A coefficient of URB1 B = 19.436 and URB2 B = 7.804 for the Urban/intermediate/rural entity of the BHA, which implies greater weight, increasing the pressure prevalence rate if the entity is urban and B = -0.438 for buildings in poor or worse condition. That is, aging +75 and rural entities would act as protective factors for depression, while urban areas and deficient buildings act as risk factors. These relationships are shown in Figure 2.
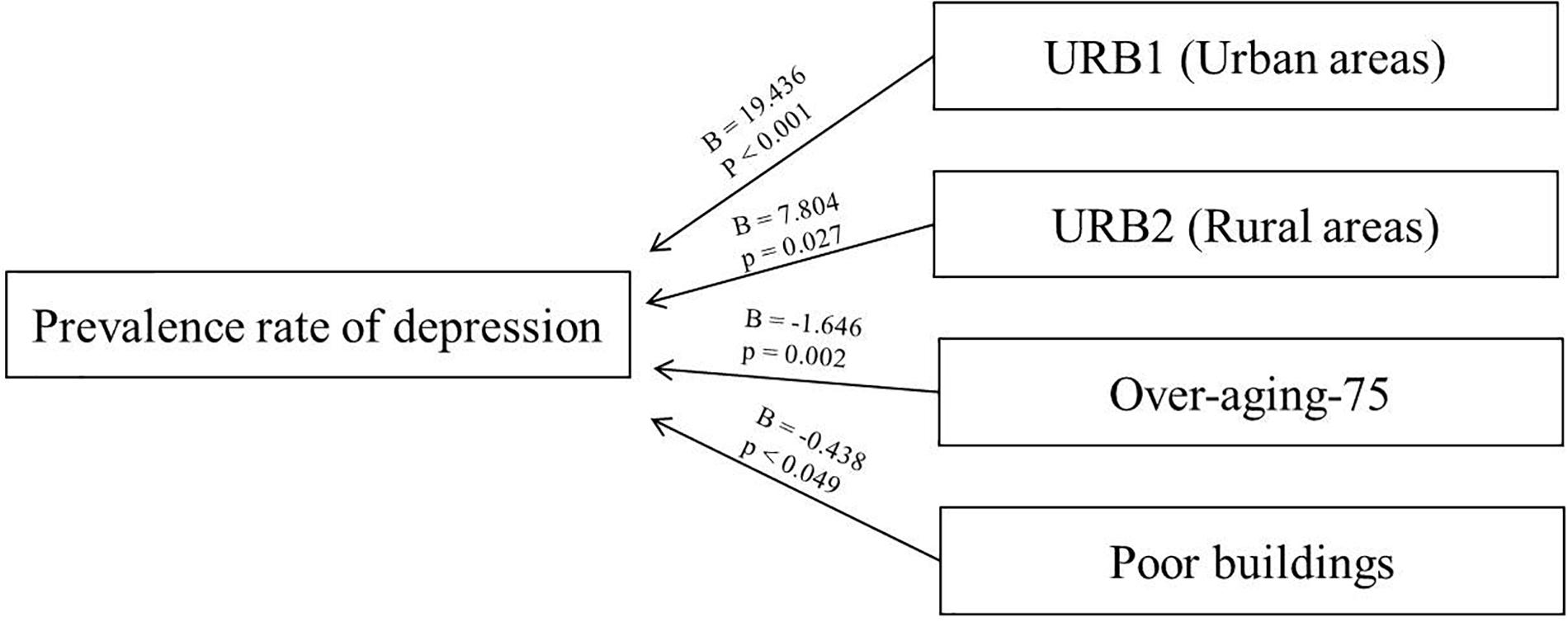
FIGURE 2. Coefficients related to the multiple linear regression.
The equation of the linear regression is as follows: Prevalence rate = 106.96 + 19.436∗URB1-1646∗Over-aging-75 + 7.804∗URB2-0.438∗Poor buildings.
Discussion
This ecological methodology may be a useful tool which, together with the statistical epidemiological analysis, can help in the political decision making process, and in this case, with the specific objective of health and, especially, mental health and depression. Relating diseases with the environment where they are generated may help to improve the health attention in the BHA, since it includes the community care in the day-to-day work. Thus, through a study of correlations, we can observe the association of depression illness with social or demographic determinants. And with a regression model, we can perceive which of the study areas are more likely to have a population that may suffer from depression. Thus, in the predictive regression model of depression, 42.2% of the variability of depression prevalence rates would be explained, whereas the other 57.8% of the variation would be attributable to other causes of a genetic, psychological or family nature. It must be considered that the model shows a key factor such as the type of rural/intermediate/urban environment being an unchangeable factor, so it is up to the public administrations to facilitate dynamics that modify habits, relationships and the day to day of people in the urban environment (Dufouil et al., 1995; Weich et al., 2006). With respect to the variables obtained in the model of over-aging, they should be analyzed with caution in regards to a potential under-diagnosis, and an influence of the rural environment variable, since in the analyzed territory the rural world is very old. The state of the buildings variable could in turn be correlated with over-aging (older people tend to live in old buildings).
If we analyze the obtained results, with respect to the depression rate, we have obtained a total prevalence of depression of 5.67%, which corresponds to a lower prevalence than that offered by the large European studies having a level of 10.55% (ESEMeD in Spain) or the PREDICT study in Spain with a 12.2% depression from primary care consultations (Haro et al., 2006; King et al., 2008). Given that these studies used population samples in which they have passed diagnostic tests and since in this study, the diagnoses were made by the family physician in a real context, the existence of under-diagnosis in Primary Care consultations could be considered in Aragon. This would be in agreement with other studies that affirm that the number of patients with depression diagnosed by the family doctor is between 42 and 72% of the total of depressed patients. Subjects that are not recognized by the family doctor are the least symptomatic (Simon and Von Korff, 1995; Vazquez-Barquero et al., 1997; Simon et al., 1999). The detection is related to the educational level of the patients, the severity of the symptoms, the level of disability and the explicit complaint of psychological depressive symptoms (Aragones et al., 2004).
The infradiagnosis may be influenced by the age of the patients, since there are significant differences when comparing Aragon rates and European rates for adults under and over 65 years; in people older than 65 years, an average that is 4.72 points less than that of European prevalence has been found whereas, on the other hand, it is 2.84 points less for adults under the age of 65. The possible considerable under-diagnosis in the older population is thus reflected in several studies (VanItallie, 2005; Urbina Torija et al., 2007; Kessler et al., 2010). This may be explained by the fact that older people express symptoms of depression as physical ailments or also because they may be confused with symptoms of dementia or long chronic diseases (Gum et al., 2009). But it is also important to analyze the rate of depression prevalence in individuals over 65 while taking account the demographic context, not only adjusting for sex and age, but also for aspects such as rurality or not of populations, because this aspect influences social networks support (Probst et al., 2006).
Regarding the variability obtained in the depression rates in the different BHA in relation to the other environmental factors analyzed, in the correlation analysis obtained, many correlations are supported by the bibliography, but other correlations have also appeared that should be studied in greater depth.
In the anticipated results based on the consulted bibliography, the traditional protective role of the rural environment in mental illnesses has been shown in this study (Vink et al., 2008; McKenzie et al., 2013). Expected results related to higher rates of depression are unemployment (Whooley et al., 2003); the higher population density, which is related to the variable rural/urban environment; and higher rates of femininity, which also correlates with the prevalence rates of depression according to gender (Aragonès Benaiges et al., 2003; Barry et al., 2008); and a lower dependency rate, supported by studies of depression according to the life cycle (Gum et al., 2009; Kessler et al., 2010).
However, as an unexpected result, a higher average salary correlates with an increase in the rate of depression. There are many studies that relate depression to low socioeconomic levels, in fact subjects with a low socioeconomic status have a 2.5 risk of developing depression (Araya et al., 1998; Ostler et al., 2001; Aragones et al., 2004), but the interaction between depression, social classes, and low economic level is complex (Lewis et al., 1998). Some studies reveal that if the degree of social isolation is controlled, the effects of poverty are reduced (Bruce et al., 1991; Bruce and Hoff, 1994) and other studies affirm that the main effect of poverty does not increase the prevalence of mental disorders, but prolongs the duration of the episodes (Weich and Lewis, 1998; Lorant et al., 2007). In this study, we consider that the reason of this unexpected result is the concentration of depression in urban areas, where the inequality is more evident (Fernández Morales, 2003). Anyway following studies should focus in this topic.
Regarding the average education, which it may be considered a protective factor (Koster et al., 2006), as an unexpected result of this study, higher depression rates has been obtained when higher levels of education are achieved. However, when analyzing within the urban environment, it appears that a higher degree of education in a large city exerts a certain protective factor against depression whereas in the intermediate and rural environment, those with higher educational levels encounter worse state of mental health. This may be due to the fact that the work to be done in the intermediate-rural environment does not meet the expectations of the degree that was earned or because it is more difficult to advance in the academic or professional field (Stansfeld et al., 2003; Arslan and Acar, 2013).
There is no significant relationship between depression and the rate of foreigners in this study, as is shown in previous studies that find only a significant relationship in recently immigrated and low-income women (Plant and Sachs-Ericsson, 2004; Smith et al., 2007). There is no significant relationship between depression and the percentage of widowers, separated-divorced, perhaps partly due to the non-disaggregation of data in adequate subgroups. More exhaustive studies with disaggregated data show that the couple’s relationship influences depression rates (Bruce and Kim, 1992; Lorant et al., 2007).
This study has certain limitations that are mainly focused on the data source of the depression rate, since they have been obtained from electronic medical records, and this may be a cause of possible under-diagnosis, especially in those over 65 years. However, it is the data from these electronic medical records that are used in statistical epidemiological analyses and that are also used in decision making on a political scope. Therefore, it is necessary to establish educational and organizational measures in order to correctly diagnose the depression episode, especially in the population group over the age of 65.
Conclusion
When studying depression in its environment, we obtain an ecological analysis for the rates of depression. The variable found to have the greatest weight in the model obtained from the multiple linear regression is the rural/urban environment. Although this factor is unchangeable on its own, it could be compensated with the establishment of dynamics that modify habits, relationships and the daily life of individuals living in urban environments.
Ethics Statement
The authors assert that all procedures contributing to this work comply with the ethical standards of the Clinical Research Ethics Committee of Aragón (belonging to the Department of Health of the Government of Aragon, Spain) and with the Helsinki Declaration of 1975, as revised in 2008. The Study Protocol was approved by the Clinical Research Ethics Committee of Aragón (Spain) (10/2008) and by the Aragones Health Service (2009). Data of prevalence of depression were obtained from clinical records provided in a non-identifiable format by Aragones Health Service.
Author Contributions
JL, MZ-A, and RM-B were responsible for the conception, data collection, and design of the study. JL and EA were responsible for data analysis. JL, BO-B, BM, RM-B, and JC contributed to the interpretation of data. JL, MZ-A and BO-B wrote the article, which was critically revised by all the other authors. All authors have approved the final version of the manuscript.
Funding
This work was supported by the Health Institute Carlos III (grant number Medical research Council (grant number PS09/01378); Research Group B21_R17 of the Department of Research, Innovation and University of the Government of Aragon (Spain); and Feder Funds “Another way to make Europe”.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We wish to thank the Primary Care Prevention and Health Promotion Network (RedIAPP-Health Institute Carlos III, Spain); Research Group B21_R17 of the Department of Research, Innovation and University of the Government of Aragon (Spain); Feder funds “Another way to make Europe”; and the Group of Studies in Territorial Planning (Grupo de Estudios en Ordenación del Territorio – GEOT) for their support in the development of the study.
References
AEI (2010). Aragon Employment Institute. Inst. Aragon. Empl. Available at: http://www.aragon.es/DepartamentosOrganismosPublicos/Institutos/InstitutoAragonesEstadistica. [accessed January 18, 2018]
Annequin, M., Weill, A., Thomas, F., and Chaix, B. (2015). Environmental and individual characteristics associated with depressive disorders and mental health care use. Ann. Epidemiol. 25, 605–612. doi: 10.1016/j.annepidem.2015.02.002
Aragones, E., Pinol, J. L., Labad, A., Masdeu, R. M., Pino, M., and Cervera, J. (2004). Prevalence and determinants of depressive disorders in primary care practice in Spain. Int. J. Psychiatry Med. 34, 21–35. doi: 10.2190/C25N-W4NY-BN8W-TXN2
Aragonès Benaiges, E., Gutiérrez Pérez, M. A., Piñol Moreso, J. L., Mèlich Teruel, N., Folch Pujol, S., and Labad Alquézar, A. (2003). Prevalencia, expresión e impacto de los trastornos depresivos en atención primaria. Atención Primaria 31, 120–125. doi: 10.1016/S0212-6567(03)79149-5
Araya, R., Rojas, G., and Lewis, G. (1998). Common mental disorders, depression and public health. Rev. Med. Chil. 126, 582–589.
Arslan, R., and Acar, B. (2013). A research on academics on life satisfaction, job satisfaction and professional burnout. Suleyman Demirel University. J. Fac. Econ. Adm. Sci. 18, 281–299.
ASI (2010). Aragon Statistics Institute (ASI). Inst. Aragon. Estad. Available at: http://www.aragon.es/DepartamentosOrganismosPublicos/Institutos/InstitutoAragonesEstadistica. [accessed January 12, 2018]
Barry, L. C., Allore, H. G., Guo, Z., Bruce, M. L., and Gill, T. M. (2008). Higher burden of depression among older women: the effect of onset, persistence, and mortality over time. Arch. Gen. Psychiatry 65, 172–178. doi: 10.1001/archgenpsychiatry.2007.17
Bellón, J. Á, De Dios Luna, J., King, M., Moreno-Küstner, B., Nazareth, I., Montón-Franco, C., et al. (2011). Predicting the onset of major depression in primary care: international validation of a risk prediction algorithm from Spain. Psychol. Med. 41, 2075–2088. doi: 10.1017/S0033291711000468
Berman, M. G., Kross, E., Krpan, K. M., Askren, M. K., Burson, A., Deldin, P. J., et al. (2012). Interacting with nature improves cognition and affect for individuals with depression. J. Affect. Disord. 140, 300–305. doi: 10.1016/j.jad.2012.03.012
Bjelland, I., Krokstad, S., Mykletun, A., Dahl, A. A., Tell, G. S., and Tambs, K. (2008). Does a higher educational level protect against anxiety and depression? The HUNT study. Soc. Sci. Med. 66, 1334–1345. doi: 10.1016/j.socscimed.2007.12.019
Bos, E. H., Bouhuys, A. L., Geerts, E., van Os, T. W. D. P., and Ormel, J. (2007). Stressful life events as a link between problems in nonverbal communication and recurrence of depression. J. Affect. Disord. 97, 161–169. doi: 10.1016/j.jad.2006.06.011
Bromet, E., Andrade, L. H., Hwang, I., Sampson, N. A., Alonso, J., de Girolamo, G., et al. (2011). Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 9:90. doi: 10.1186/1741-7015-9-90
Bruce, M., Takeuchi, D., and Leaf, P. (1991). Poverty and psychiatric status: longitudinal evidence from the new haven epidemiologic catchment area study. Arch. Gen. Psychiatry 48, 470–474. doi: 10.1001/archpsyc.1991.01810290082015
Bruce, M. L., and Hoff, R. A. (1994). Social and physical health risk-factors for 1st-onset major depressive disorder in a community sample. Soc. Psychiatry Psychiatr. Epidemiol. 29, 165–171.
Bruce, M. L., and Kim, K. M. (1992). Differences in the effects of divorce on major depression in men and women. Am. J. Psychiatry 149, 914–917. doi: 10.1176/ajp.149.7.914
Brugha, T. S., Weich, S., Singleton, N., Lewis, G., Bebbington, P. E., Jenkins, R., et al. (2005). Primary group size, social support, gender and future mental health status in a prospective study of people living in private households throughout Great Britain. Psychol. Med. 35, 705–714. doi: 10.1017/S0033291704003903
Cervilla, J. A., Molina, E., Rivera, M., Torres-González, F., Bellón, J. A., Moreno, B., et al. (2007). The risk for depression conferred by stressful life events is modified by variation at the serotonin transporter 5HTTLPR genotype: evidence from the Spanish PREDICT-Gene cohort. Mol. Psychiatry 12, 748–755. doi: 10.1038/sj.mp.4001981
Cervilla, J. A., Rivera, M., Molina, E., Torres-González, F., Bellón, J. A., Moreno, B., et al. (2006). The 5-HTTLPR s/s genotype at the serotonin transporter gene (SLC6A4) increases the risk for depression in a large cohort of primary care attendees: the PREDICT-gene study. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 141, 912–917. doi: 10.1002/ajmg.b.30455
Djernes, J. K. (2006). Prevalence and predictors of depression in populations of elderly: a review. Acta Psychiatr. Scand. 113, 372–387. doi: 10.1111/j.1600-0447.2006.00770.x
Dufouil, C., Dartigues, J., and Fuhrer, R. (1995). Symptômes dépressifs chez les personnes âgées: comparaison entre des populations rurales et urbaines. Rev. Epidemiol. Sante Publique 43, 308–315.
Fernández Morales, A. (2003). Inequality and poverty in rural and urban areas in Spain: a parametric approach. Estadística 55, 351–365.
Ferrari, A. J., Charlson, F. J., Norman, R. E., Patten, S. B., Freedman, G., Murray, C. J. L., et al. (2013). Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. PLoS Med. 10:e1001547. doi: 10.1371/journal.pmed.1001547
Gabilondo, A., Rojas-Farreras, S., Vilagut, G., Haro, J. M., Fernández, A., Pinto-Meza, A., et al. (2010). Epidemiology of major depressive episode in a southern European country: results from the ESEMeD-Spain project. J. Affect. Disord. 120, 76–85. doi: 10.1016/j.jad.2009.04.016
Gaxiola-Robles, R., de Jesús, A., Labrada-Martagón, V., Díaz-Castro, S., and Zenteno-Savín, T. (2013). Increase of the enviromental temperatura and its associationto suicide rates in South California 1985-2008. Salud Ment. 36, 421–427. doi: 10.17711/SM.0185-3325.2013.053
Golden, J., Conroy, R., Bruce, I., Denihan, A., Greene, E., Kirby, M., et al. (2009). Loneliness, social support networks, mood and wellbeing in community-dwelling elderly. Int. J. Geriatr. Psychiatr. 24, 694–700. doi: 10.1002/gps.2181
Gum, A., King-Kallimanis, B., and Kohn, R. (2009). Prevalence of mood, anxiety, and substanceabuse disorders for older Americans in the national comorbidity survey-replication. Am. J. Geriatr. Psychiatry 17, 769–781. doi: 10.1097/JGP.0b013e3181ad4f5a
Gutiérrez-Fraile, M., García-Calvo, C., Prieto, R., and Gutiérrez-Garitano, I. (2011). Mental disorders in psychiatric outpatients in Spain. Actas Esp. Psiquiatr. 39, 349–355.
Haro, J. M., Palacin, C., Vilagut, G., Martinez, M., Bernal, M., Luque, I., et al. (2006). Prevalencia y factores asociados de los trastornos mentales en España: resultados del estudio ESEMeD-España. Prevalence of mental disorders and associated factors: results from the ESEMeD-Spain study. Med. Clín. 126, 445–451. doi: 10.1157/13086324
Hidaka, B. (2012). Depression as a disease od modernity: explanations for increasing prevalence. J. Affect. Disord. 140, 205–214. doi: 10.1016/j.jad.2011.12.036
Jessen, G., Steffensen, P., and Jensen, B. (1998). Seasons and meteorological factors in suicidal behaviour. Findings and methodological considerations from a Danish study. Arch. Suicide Res. 4, 263–280. doi: 10.1080/13811119808258301
Karlsen, S., Nazroo, J. Y., McKenzie, K., Bhui, K., and Weich, S. (2005). Racism, psychosis and common mental disorder among ethnic minority groups in England. Psychol. Med. 35, 1795–1803. doi: 10.1017/S0033291705005830
Kempen, G. I., Brilman, E. I., Ranchor, A. V., and Ormel, J. (1999). Morbidity and quality of life and the moderating e € ects of level of education in the elderly. Soc. Sci. Med. 49, 143–149. doi: 10.1016/S0277-9536(99)00129-X
Kendler, K. S. (2005). Sex differences in the relationship between social support and risk for major depression: a longitudinal study of opposite-sex twin pairs. Am. J. Psychiatry 162, 250–256. doi: 10.1176/appi.ajp.162.2.250
Kessler, R. C. (2003). Epidemiology of women and depression. J. Affect. Disord. 2, 5–13. doi: 10.1016/S0165-0327(02)00426-3
Kessler, R. C., Birnbaum, H. G., Shahly, V., Bromet, E., Hwang, I., McLaughlin, K. A., et al. (2010). Age differences in the prevalence and co-morbidity of DSM-IV major depressive episodes: results from the WHO world mental health survey initiative. Depress. Anxiety 27, 351–364. doi: 10.1002/da.20634
King, M., Nazareth, I., Levy, G., Walker, C., Morris, R., Weich, S., et al. (2008). Prevalence of common mental disorders in general practice attendees across Europe. Br. J. Psychiatry 192, 362–367. doi: 10.1192/bjp.bp.107.039966
Koster, A., Bosma, H., Kempen, G., Penninx, B., Beekman, A., Deeg, D., et al. (2006). Socioeconomic differences in incident depression in older adults: the role of psychosocial factors, physical health status, and behavioral factors. J. Psychosom. Res. 61, 619–627. doi: 10.1016/j.jpsychores.2006.05.009
Kupfer, D. J., Frank, E., and Phillips, M. L. (2012). Major depressive disorder: new clinical, neurobiological, and treatment perspectives. Lancet 379, 1045–1055. doi: 10.1016/S0140-6736(11)60602-8
Leskela, U., Melartin, T., Lestela-Mielonen, P., Rytsala, H., Sokero, T., and Heikkinen, M. (2004). Life events, social support, and onset of major depressive episode in Finnish patients. J. Nerv. Ment. Dis. 192, 373–381. doi: 10.1097/01.nmd.0000126705.15497.c9
Lewis, G., Bebbington, P., Brugha, T., Farrell, M., Gill, B., Jenkins, R., et al. (1998). Socioeconomic status, standard of living, and neurotic disorder. Lancet 22, 605–609. doi: 10.1016/S0140-6736(98)04494-8
Lino, V. T. S., Portela, M. C., Camacho, L. A. B., Atie, S., and Lima, M. J. B. (2013). Assessment of social support and its association to depression, self-perceived health and chronic diseases in elderly individuals residing in an area of poverty and social vulnerability in Rio de Janeiro City, Brazil. PLoS One 8:e71712. doi: 10.1371/journal.pone.0071712
Lorant, V., Croux, C., Weich, S., Deliège, D., Mackenbach, J., and Ansseau, M. (2007). Depression and socio-economic risk factors: 7-Year longitudinal population study. Br. J. Psychiatry 190, 293–298. doi: 10.1192/bjp.bp.105.020040
Lorant, V., Deliège, D., Eaton, W., Robert, A., Philippot, P., and Ansseau, M. (2003). Socioeconomic inequalities in depression: a meta-analysis. Am. J. Epidemiol. 157, 98–112. doi: 10.1093/aje/kwf182
McKenzie, K., Murray, A., and Booth, T. (2013). Do urban environments increase the risk of anxiety, depression and psychosis? An epidemiological study. J. Affect. Disord. 150, 1019–1024. doi: 10.1016/j.jad.2013.05.032
Mykletun, A., Bjerkeset, O., Øverland, S., Prince, M., Dewey, M., and Stewart, R. (2009). Levels of anxiety and depression as predictors of mortality: the HUNT study. Br. J. Psychiatry 195, 118–125. doi: 10.1192/bjp.bp.108.054866
O’Hare, C., O’Sullivan, V., Flood, S., and Kenny, R. (2016). Seasonal and meteorological associations with depressive symptoms in older adults: a geo-epidemiological study. J. Affect. Disord. 191, 172–179. doi: 10.1016/j.jad.2015.11.029
Ostler, K., Thompson, C., Kinmonth, A. L., Peveler, R. C., Stevens, L., and Stevens, A. (2001). Influence of socio-economic deprivation on the prevalence and outcome of depresion in primary care. The Hampshire Depression Project. Br. J. Psychiatry 178, 12–17. doi: 10.1192/bjp.178.1.12
Patten, S. B., Kennedy, S. H., Lam, R. W., O’Donovan, C., Filteau, M. J., Parikh, S. V., et al. (2009). Canadian network for mood and anxiety treatments (CANMAT) clinical guidelines for the management of major depressive disorder in adults. I. Classification, burden and principles of management. J. Affect. Disord. 117, S5–S14. doi: 10.1016/j.jad.2009.06.044
Patton, G. C., Coffey, C., Posterino, M., Carlin, J. B., and Bowes, G. (2003). Life events and early onset depression: cause or consequence? Psychol. Med. 33, 1203–1210. doi: 10.1017/S0033291703008626
Plaisier, I., Beekman, A., Bruijn, J., de Graaf, R., Ten Have, M., Smit, J., et al. (2008). The effect of social roles on mental health: a matter of quantity or quality? J. Affect. Disord. Disord. 111, 261–270. doi: 10.1016/j.jad.2008.03.007
Plaisier, I., de Bruijn, J. G., de Graaf, R., ten Have, M., Beekman, A. T., and Penninx, B. W. (2007). The contribution of working conditions and social support to the onset of depressive and anxiety disorders among male and female employees. Soc. Sci. Med. 64, 401–410. doi: 10.1016/j.socscimed.2006.09.008
Plant, E. A., and Sachs-Ericsson, N. (2004). Racial and ethnic differences in depression: the roles of social support and meeting basic needs. J. Consult. Clin. Psychol. 72, 41–52. doi: 10.1037/0022-006X.72.1.41
Probst, J. C., Laditka, S. B., Moore, C. G., Harun, N., Powell, M. P., and Baxley, E. G. (2006). Rural-urban differences in depression prevalence: implications for family medicine. Fam. Med. 38, 653–660.
Regan, C. L., and Horn, S. A. (2005). To nature or not to nature: associations between environmental preferences, mood states and demographic factors. J. Environ. Psychol. 25, 57–66. doi: 10.1016/j.jenvp.2005.01.001
Reques Velasco, P. (2010). Geodemografía. Módulo 2. Fuentes Para el Estudio de la Población: la Importancia Creciente de Internet - BASES TEÓRICAS. Available at: https://ocw.unican.es/pluginfile.php/843/course/section/912/Modulo2-MATERIALDECLASE.pdf
Roberts, R. E., Kaplan, G. A., Shema, S. J., and Strawbridge, W. J. (1997). Does growing old increase the risk for depression? Am. J. Psychiatry 154, 1384–1390. doi: 10.1176/ajp.154.10.1384
Rohde, P., Ichikawa, L., Simon, G. E., Ludman, E. J., Linde, J. A., Jeffery, R. W., et al. (2008). Associations of child sexual and physical abuse with obesity and depression in middle-aged women. Child Abus. Negl. 32, 878–887. doi: 10.1016/j.chiabu.2007.11.004
Romans, S., Cohen, M., and Forte, T. (2011). Rates of depression and anxiety in urban and rural Canada. Soc. Psychiatry Psychiatr. Epidemiol. 46, 567–575. doi: 10.1007/s00127-010-0222-2
Ryan, R. M., Weinstein, N., Bernstein, J., Brown, K. W., Mistretta, L., and Gagné, M. (2010). Vitalizing effects of being outdoors and in nature. J. Environ. Psychol. 30, 159–168. doi: 10.1016/j.jenvp.2009.10.009
Sekula, L., DeSantis, J., and Gianetti, V. (2003). Considerations in the management of the patient with comorbid depression and anxiety. J. Am. Acad. Nurse Pract. 15, 23–33. doi: 10.1111/j.1745-7599.2003.tb00251.x
Simon, G. E., and Von Korff, M. (1995). Recognition, management, and outcomes of depression in primary care. Arch. Fam. Med. 4, 99–105. doi: 10.1001/archfami.4.2.99
Simon, G. E., VonKorff, M., Piccinelli, M., Fullerton, C., and Ormel, J. (1999). An international study of the relation between somatic symptoms and depression. N. Engl. J. Med. 341, 1329–1335. doi: 10.1056/NEJM199910283411801
Smith, K., Glazier, R., Moineddin, R., and Matheson, F. (2007). Gender, income and immigration differences in depression in Canadian Urban centres. Can. J. Public Health 98, 149–153.
SNIS. (2010). Spanish National Institute of Statistics. Available at: www.ine.es [accessed January 18, 2018]
Sobocki, P., Jönsson, B., Angst, J., and Rehnberg, C. (2006). Cost of depression in Europe. J. Ment. Health Policy Econ. 9, 87–98.
Somervell, P., Leaf, P., Weissman, M. M., Blazer, D., and Bruce, M. (1989). The prevalence of major depression in black and white adults in five United States communities. Am. J. Epidemiol. 130, 725–735. doi: 10.1093/oxfordjournals.aje.a115394
Spijker, J., de Graaf, R., Bijl, R. V., Beekman, A. T. F., Ormel, J., and Nolen, W. A. (2004). Functional disability and depression in the general population. results from the netherlands mental health survey and incidence study (NEMESIS). Acta Psychiatr. Scand. 110, 208–214. doi: 10.1111/j.1600-0447.2004.00335.x
Stansfeld, S. A., Head, J., Fuhrer, R., Wardle, J., and Cattell, V. (2003). Social inequalities in depressive symptoms and physical functioning in the Whitehall II study: exploring a common cause explanation. J. Epidemiol. Commun. Heal. 57, 361–367. doi: 10.1136/jech.57.5.361
Stegmann, M. E., Ormel, J., de Graaf, R., Haro, J. M., De Girolamo, G., Demyttenaere, K., et al. (2010). Functional disability as an explanation of the associations between chronic physical conditions and 12-month major depressive episode. J. Affect. Disord. 124, 38–44. doi: 10.1016/j.jad.2009.10.026
Tax Agency. (2010). Agencia Tributaria. Available at: www.agenciatributaria.es [accessed January 15, 2018]
Trainor, K., Mallet, J., and Rushe, T. (2013). Age related differences in mental health scale scores and depression diagnosis: adult responses to the CIDI-SF and MHI-5. J. Affect. Disord. 151, 639–645. doi: 10.1016/j.jad.2013.07.011
Urbina Torija, J. R., Flores Mayor, J. M., García Salazar, M. P., Torres Buisán, L., and Torrubias Fernández, R. M. (2007). Síntomas depresivos en personas mayores. Prevalencia y factores asociados. Gac. Sanit. 21, 37–42. doi: 10.1157/13099119
Üstün, T. B., Ayuso-Mateos, J. L., Chatterji, S., Mathers, C., and Murray, C. J. L. (2004). Global burden of depressive disorders in the year 2000. Br. J. Psychiatry 184, 386–392. doi: 10.1192/bjp.184.5.386
VanItallie, T. B. (2005). Subsyndromal depression in the elderly: underdiagnosed and undertreated. Metabolism 54, 39–44. doi: 10.1016/j.metabol.2005.01.012
Vazquez-Barquero, J., Garcia, J., Simon, J., Iglesias, C., Montejo, J., and Herran, A. (1997). Mental health in primary care. An epidemiológical study of morbidity and use of health resources. Br. J. Psychiatry 170, 529–535.
Vink, D., Aartsen, M. J., and Schoevers, R. A. (2008). Risk factors for anxiety and depression in the elderly: a review. J. Affect. Disord. 106, 29–44. doi: 10.1016/j.jad.2007.06.005
Wang, J. L. (2004). Rural-urban differences in the prevalence of major depression and associated impairment. Soc. Psychiatry Psychiatr. Epidemiol. 39, 19–25. doi: 10.1007/s00127-004-0698-8
Weich, S., and Lewis, G. (1998). Poverty, unemployment, and common mental disorders: population based cohort study. BMJ 317, 115–119. doi: 10.1136/bmj.317.7151.115
Weich, S., Nazareth, I., Morgan, L., and King, M. (2007). Treatment of depression in primary care: socio-economic status, clinical need and receipt of treatment. Br. J. Psychiatry 191, 164–169. doi: 10.1192/bjp.bp.106.032219
Weich, S., Twigg, L., and Lewis, G. (2006). Rural/non-rural differences in rates of common mental disorders in Britain: prospective multilevel cohort study. Br. J. Psychiatry 188, 51–57. doi: 10.1192/bjp.bp.105.008714
Weissman, M., and Wickramaratne, P. (2000). Age of onset and familial risk in major depression. Arch. Gen. Psychiatry 57:511. doi: 10.1001/archpsyc.57.5.513
Weissman, M. M., and Olfson, M. (1995). Depression in women: implications for health care research. Sci. New Ser. 269, 799–801. doi: 10.1126/science.7638596
Whisman, M. A., and Bruce, M. L. (1999). Marital dissatisfaction and incidence of major depressive episode in a community sample. J. Abnorm. Psychol. 108, 674–678. doi: 10.1037//0021-843X.108.4.674
Keywords: depression, variability, prevalence, sociodemographic factors, environmental factors
Citation: Llorente JM, Oliván-Blázquez B, Zuñiga-Antón M, Masluk B, Andres E, Garcia-Campayo J and Magallon-Botaya R (2018) Variability of the Prevalence of Depression in Function of Sociodemographic and Environmental Factors: Ecological Model. Front. Psychol. 9:2182. doi: 10.3389/fpsyg.2018.02182
Received: 11 April 2018; Accepted: 23 October 2018;
Published: 12 November 2018.
Edited by:
Patrik Sörqvist, Gävle University College, SwedenReviewed by:
Arcady A. Putilov, Humboldt-Universität zu Berlin, GermanyCarlos Tomaz, Universidade Ceuma, Brazil
Angela J. Grippo, Northern Illinois University, United States
Copyright © 2018 Llorente, Oliván-Blázquez, Zuñiga-Antón, Masluk, Andrés, Garcia-Campayo and Magallón-Botaya. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bárbara Oliván-Blázquez, Ym9saXZhbkB1bml6YXIuZXM=