 Øystein Robertsen1
Øystein Robertsen1 Marit Nøst Hegseth1
Marit Nøst Hegseth1 Solveig Føreland1
Solveig Føreland1 Frank Siebler2
Frank Siebler2 Martin Eisemann2
Martin Eisemann2 Hans Christian Bones Vangberg1,2*
Hans Christian Bones Vangberg1,2*- 1Department of Occupational and Environmental Medicine, University Hospital of North Norway, Tromsø, Norway
- 2Department of Psychology, Faculty of Health Sciences, UiT The Arctic University of Norway, Tromsø, Norway
Introduction: The present study investigated the effect of interventions aiming to improve attitudes toward the use of respiratory protective equipment (RPE), knowledge of RPE and the use of RPE in the Norwegian smelter industry.
Method: The surveys received 567 respondents to baseline and 240 respondents 2 weeks after the intervention. Participants were invited to either a fit-testing of respirators [Group 1] or a fit-testing combined with a lecture on exposure [Group 2], health effects and RPE. The control group [Group 3] received no training. Questionnaires containing measures of subjective knowledge, attitudes and behavior regarding RPE use were assessed.
Results: Testing indicated an improvement in knowledge of RPE and a reduction in perceived inconveniences regarding the use of RPE for both intervention groups. Group 1 showed an improvement in attitudes and organizational support, while intervention Group 2 showed an improvement in subjective norms related to RPE use. Intention to use or rate of respirator use was not shown to change significantly for any group using paired testing. Regression analysis indicated that participation in either intervention influenced intention to use respirators. The effect was significant for Group 1 and was marginally significant for intervention Group 2.
Conclusion: The results indicate that interventions can increase workers’ knowledge and attitudes, and reduce perceived inconvenience regarding the use of respiratory protective equipment. However, even though some variables seemed to positively change, reported respirator use did not improve for either groups participating in the study. It may be that physical barriers with regards to using RPE, such as fogging of protective goggles, sweating, breathing and communication issues outweigh individual attitudes, intentions and social pressure to use respirators.
Practical Applications: The tailored course and practical training in RPE use in the current intervention can be applied in the smelting industry to provide up to date information on dust exposure, health effects and protective equipment. Some adjustments may be warranted for the content to fit specific risks and exposures of other industries. However, the general pedagogical framework of the educational material regarding health effects and RPE should be useful for most heavy industries.
Introduction
The presence of respiratory risk factors such as gases, fumes, fibers and dust, including nano-sized particles, in the work atmosphere of smelters in the Norwegian metal alloy industry has been well documented (Ellingsen et al., 2003; Føreland et al., 2008; Berlinger et al., 2015; Kero and Jørgensen, 2016; Kero et al., 2017). Depending on the end product and production processes, these exposure factors vary both qualitatively and quantitatively between smelters, but the respiratory risk they represent is of general concern for the industry. Previous studies conclude that Norwegian smelter workers are more susceptible to develop respiratory diseases such as chronic obstructive pulmonary disorder (COPD) than the general population (Johnsen et al., 2008; Søyseth et al., 2011, 2013, 2015). Although measures have been taken to reduce exposure, there are still areas and work-tasks where exposure is too high and occupational exposure levels are exceeded. Indeed, 98% of the employees at Norwegian smelters reported that they were exposed to one or more respiratory health risk factors more than once a week (Hegseth et al., 2018). According to the hierarchy of controls, the use of personal protective equipment (PPE) should be the final solution to end respiratory challenges. Prior to the use of PPE, removal or substitution of hazardous materials, engineering controls or administrative controls should be considered. Some exposure cannot be controlled by engineering or administrative solutions, making personal protective equipment a necessity. All Norwegian smelters have included the use of respiratory protective equipment (RPE) in their health and safety regulations. Yet, compliance with RPE regulations is sub-optimal. Seventy-eight percent of the workers report that they do not always use RPE in exposed situations (Hegseth et al., 2018). Sub-optimal RPE use has been reported in other professions such as nursing, farming, mining, construction and nuclear energy (Salazar et al., 2001; Carpenter et al., 2002; Bryce et al., 2008; MacFarlane et al., 2008; Mitchell and Schenker, 2008; Tam and Fung, 2008; Han and Kang, 2009; Guseva Canu et al., 2013).
In a review by Graveling et al. (2011), the authors suggested several measures to optimize RPE use and compliance among workers. The role of management with regards to facilitating use, providing the correct equipment and training in addition to aspects of the RPE equipment such as user comfort and technical appropriateness were pointed out. Also, correct RPE use could be facilitated through increasing employee intentions by means of education in addition to administrative measures (Szeinuk et al., 2000). Testing for proper RPE fit is important. Facial structures vary individually, and RPE that fits one person adequately may not do so on another individual. The Health and Safety Executive (HSE) standard for fit-testing recommends quantitative fit-testing and suggests a fit-factor of 100 in order to ensure proper protection. Fit-factor is the ratio between ambient particle count and particle count measured inside RPE. Furthermore, RPE fit testing should be performed yearly in order to ensure protection, i.e., if a person gains or lose weight it may affect fit (HSE, 2012).
According to the theory of planned behavior (TPB) (Ajzen, 1985, 1991), behavior is guided by intention, influenced by the antecedents attitudes toward the behavior, subjective norms and perceived control. Attitudes toward behavior emerge from the affective or cognitive evaluations a subject makes regarding the behavior, e.g., feeling comfortable, regarding it as meaningful. Attitudes also involve evaluations of outcomes of performing behavior. Subjective norms are individual evaluations of how the social norms regarding the behavior, this concept comprise descriptive and injunctive norms. For instance, descriptive norms are individual perceptions of how colleagues behave, while injunctive norms are individual perceptions of what colleagues think about a behavior, i.e., whether colleagues approve or disapprove of the behavior. Perceived control is the extent to which the subject feels in control of the behavior, e.g., belief that they can successfully perform the behavior or whether they feel that they control behavior, or if it is externally occurring. These three structures are related to background factors such as personality, intelligence, values, education, culture etc. Therefore, a change in these factors should influence a behavioral change. The TPB has been shown to be effective in predicting behavior and intentions based on attitudes, subjective norms and perceived behavioral control (Godin and Kok, 1996; Armitage and Conner, 2001). Indeed, interventions based on TPB have previously shown efficacy in increasing intentions with regards to health-related behaviors (Brubaker and Fowler, 1990; Murphy and Brubaker, 1990; Fishbein et al., 1996; Jemmott et al., 1998).
Interventions containing training and/or education to influence the use of RPE have previously been performed in farming and health care (Gjerde et al., 1991; Carrico et al., 2007; Dressel et al., 2007; Donham et al., 2011; Kim et al., 2012; Shamsi et al., 2015). A review by Luong Thanh et al. (2016) revealed that given the current knowledge status, there was not sufficient evidence to conclude that training and education interventions did not have an effect on the use of respirators. The authors also requested more rigorous studies on this topic. Lunt et al. (2011) came to a similar conclusion when reviewing studies using interventions to improve behaviors related to dermal and respiratory hazards. Mullan et al. (2015) reviewed studies investigating the efficacy of various theory-based interventions in the construction business and concluded that interventions employing feedback, monitoring and goal setting were more effective than behavior instruction and information regarding health effects.
Fit-testing respirators in order to assure sufficient protection has been conducted for some time. As previously mentioned, objective fit-testing is done by using instruments that count particle ratios between the atmosphere inside the respirator and outside. There is evidence that RPE efficiency can be increased by fit-testing respirators on end users (Myers et al., 1995; Or et al., 2012; Harber et al., 2013). The purpose of fit-testing is to prevent leakage of hazardous substances into the RPE (HSE, 2012). Fit-testing is normally done in a one-to-one scenario where the participant receives personalized advice and equipment testing (HSE, 2012), interactions where subjects receive information and testing by a professional can to some extent function as tailored interventions. Tailored interventions demonstrably exert a significant impact on health behavior (Noar et al., 2007). Experience from our clinic suggests that fit-testing increases awareness of RPE and its use. This observation supports the hypothesis that fit-testing may function as an intervention to increase positive behavior. Additionally, as Howie (2005) pointed out, informing the workers of the consequence of exposure is of great importance in increasing motivation to use RPE. Hence, education on relevant exposure and potential health effects could improve the effect of the intervention (Szeinuk et al., 2000).
The overall goal of this study was to improve the rate of RPE use in the Norwegian smelter industry through a tailored knowledge-based intervention comprising a seminar on dust exposure and health effects and/or RPE fit-testing. The aim of this research was to determine which of the described interventions, if any, increased the rate of RPE use.
Materials and Methods
Participants
Participants were recruited from the population of smelter workers involved in the DeMaskUs project (Sintef, 2015). Criteria for participation was age of 18 or above and that they had previously worked in or currently were working in jobs where they could encounter respiratory exposure. See Tables 1 and 2 for demographics and plant distribution.
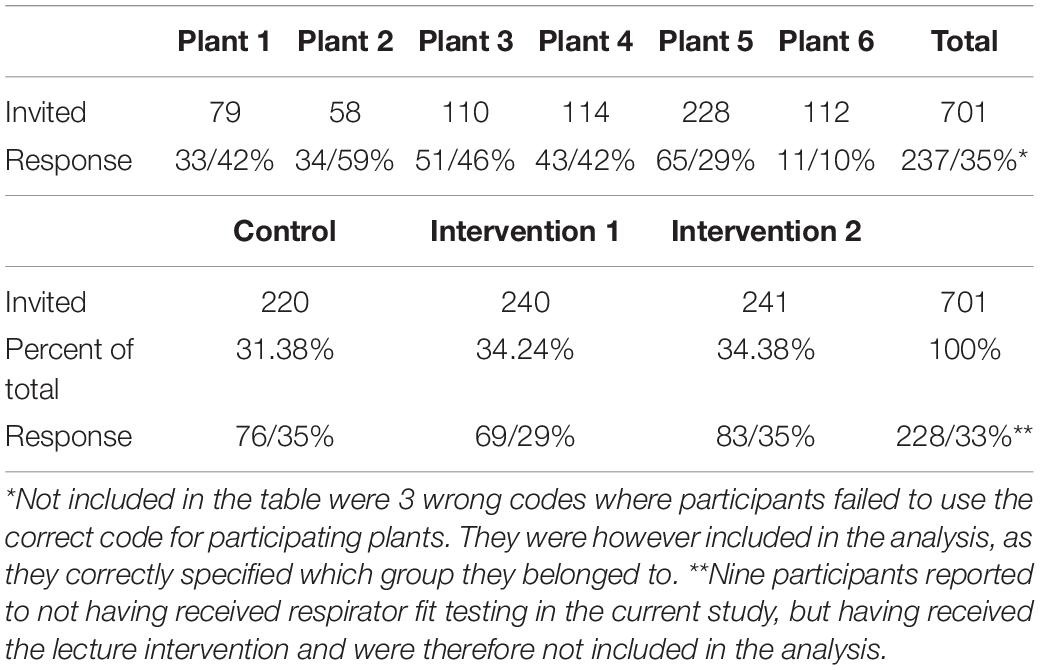
Table 1. Number of participants and response rate (%) by plant and intervention group at post-intervention.
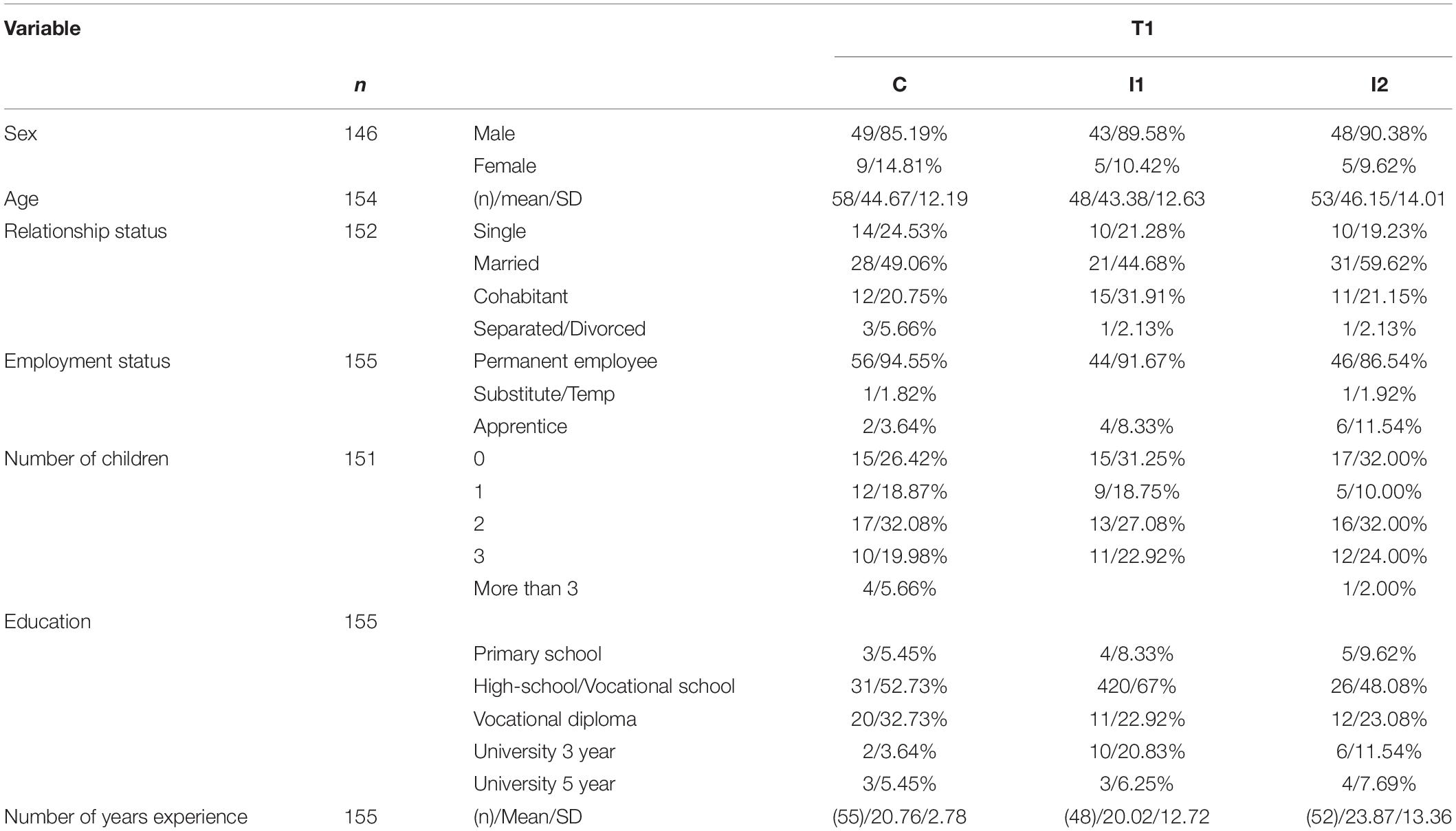
Table 2. Sample demographics, by group for participants who responded to both pre and post-intervention questionnaire.
Design
The presented work was a controlled before-and-after study included in the DeMaskUs project, conducted in the Norwegian smelter industry. The current study described the relationship between intervention participation and intention to use RPE 2 weeks after the intervention, controlling for TPB factors. Furthermore, participants scores on single-item factors were investigated to see if they had changed between baseline and post-intervention.
Randomization
Participants were randomly assigned into three groups, one control group and two intervention groups, using a random number generator. An intra-plant design was adopted to mitigate influence from confounding variables present at the plants. That is, participants were randomized into three groups at each plant. Interventions were implemented at the six participating plants following the baseline data collection (Robertsen et al., 2018). Smelting plants are operational 24 h, 365 days a year, meaning most participants had shift-arrangements working morning, afternoon, night-shifts or off-days on rotation. The period for data collection and intervention implementation had to be scheduled with the plant management to be conducted at an appropriate time. This meant that during intervention, some shifts had off-days. A completely random allocation of all participants at each plant was therefore not practically obtainable. However, as participants were not deliberately assigned to shifts ahead of time, the randomization was as rigorous as possible.
Questionnaires
Questionnaires were used to collect data from participants before and after the intervention. Baseline data had been collected using a questionnaire described in Robertsen et al. (2018), comprising scales measuring TPB variables, safety climate, work experience and items measuring perceived exposure, organizational perception regarding support and communication, knowledge and perceived inconveniences regarding the use of RPE. Follow-up data formed the basis for the current article and was collected 2 weeks post intervention. The follow-up questionnaire was a condensed version of the baseline questionnaire comprised of variables thought to change due to the intervention. Primarily TPB factors and single-item factors. Additional items asking if participants had received fit-testing and/or course were added to determine which group they had been assigned to.
Factors Based on the Theory of Planned Behavior
Questionnaire items representing the TPB (Theory of Planned Behavior) factors (attitudes toward the use of respirators, subjective norms regarding the use of respirators, perceived control in regards of respirator use, intention to use respirators and rate of respirator use) had been developed in several steps following recommendations by Fishbein and Ajzen (2009); see Robertsen et al. (2018) for details. The factors were employed in the follow-up questionnaires to investigate changes between pretest and posttest as a result of the intervention. Factor sample items; Attitudes (e.g., Regularly using a respirator during the next work-week would be. Very harmful vs. Not harmful at all), Subjective norms (e.g., My colleagues always wear respirators during the work-week.), Perceived control (e.g., It’s up to me whether or not I use the respirator during a work-week.), Intention (e.g., I am going to use the respirator in all required situations next work-week).
See Supplementary Appendix Table A2 for a list of TPB factors and items.
Factors Based on Single Items
The single item creation was described in Robertsen et al. (2018). Items aimed at measuring change due to intervention were included in the follow-up. Items were assigned into three factors, see Supplementary Appendix Table A1. Items were scored on a seven point likert-scale from 1,“Completely disagree” to 7, “Completely agree.”
Knowledge
Items in this factor measured perceived knowledge regarding the use of respirators. High scores were favorable and indicated that participants perceived to know more about respirators. Example items; “I know what the respirator protects against,” “I am confident that the respirator works as intended.”
Organization
This factor provided a measure of how participants experienced organizational climate regarding health and safety at work. High scores on these items were considered positive. Example items: “The organization is willing to provide personalized protective equipment,” “Employee suggestions on improvements are taken into consideration properly and discussed openly.”
Inconveniences
The factor measured practical issues regarding the use of respirators, e.g., impractical in certain work-tasks, communication issues or accessibility. Items were negatively worded. A low score indicated that the participants felt less practical obstruction regarding RPE use. Example items: “It is impossible to follow respirator guidelines during some work-task,” “Sometimes I don’t bother changing respirator even though I know I should.”
The single item factors were thought to be linked to the use of RPE. Knowledge of RPE and perceived organizational support were considered important background factors facilitating use of RPE and perceived inconveniences was thought to directly influence RPE use. A confirmatory factor analysis was performed to check for convergent and discriminant validity of the three factors based upon single-items. Self-reported measures were chosen due to potential problems with biases and cost-effectiveness, monetary and timewise.
Data Collection and Preparation
Questionnaires were individually packaged and distributed to the plants by the researchers. Contact personnel at each plant distributed questionnaires to the employees. Envelopes contained questionnaires, information leaflet describing the project, what participation entailed and information about chances to win lottery prizes. Baseline questionnaires were sent out 3 weeks prior to the intervention and handed in before the intervention started. Follow-up questionnaires were sent out 2 weeks after the intervention and the participants had 10 days respond.
Returned questionnaires were optically read at the University Hospital of Northern Norway’s Clinical Research Department.
To increase response rates, participants had a chance to win a gift certificate (6 per plant) of approximately 80 EUR.
Procedures
Participants who had received fit testing prior to the DeMaskUs Project were excluded from the analysis (n = 11). In order to follow participants from baseline to follow-up but still keep their anonymity, they were asked to use a self-generated ID-key (Yurek et al., 2008). Participants were invited to take part in the intervention groups, there was no mandatory or forced participation.
Content of Intervention
Intervention 1 (Group 1)
Fit testing was performed using a TSI Portacount Respirator Fit Tester 8038 (TSI inc, Shoreview, MN, United States). The Portacount generates a ratio between measured ambient particle count and particle count inside the RPE, while the wearer executes a standardized set of exercises (HSE, 2012).
Participants were invited to a testing room where the HSE fit test standard (HSE, 2012) was explained to the participants. They were asked which respirator they normally used, if they liked it and how they perceived performance, and they were asked to don the respirator.
The participants could follow the results on screen and for each task the Portacount calculated the fit-factor and indicated either fail or pass. This allowed participants to observe how different tasks affected the fit of the respirator, and how the respirator performed.
If the respirator failed fit-testing, the participant could test a number of other respirators. If the respirator passed testing, we asked if they wanted to test any other respirators to see if they liked them better, and if so another test was performed. The tests were performed by the research group, all of whom had training in the use of the Portacount Pro + machine and HSE-standard. Personnel performing the tests also provided information about how the respirators function, different types of filters and other relevant information about respirators during the test session.
Intervention 2 (Group 2)
Group 2 received the same fit-testing procedure as group 1 and in addition they were invited to take part in a 45 min lecture on exposure and health effects named “Dust and Health,” tailored to the production and specific exposure risks at their smelting plant. The course included a brief introduction to the following topics:
• What is dust, fumes and gasses? Specific focus on nanosized particles.
• Where and what kind of dust/fumes/gases were located in the plant.
• How exposure affects the respiratory system.
• Mechanisms behind the development of COPD.
• Description of other health risks related to dust/fumes/gases.
• The meaning of increased risk.
• References to recent studies from their industry.
• Measures to reduce exposure.
• Respiratory protective equipment: Design and structure.
• Properties of different types of filters and RPE.
• The importance of fit-testing.
• Visualization of the amount of nano-sized particles that one can breathe in, by showing a used filter from a dust measurement in an actual smelter.
A toxicologist and a specialist physician in work and occupational medicine delivered the course to the participants. Questions were welcomed both during and after the course. Meeting rooms were booked on site at each participating plant for the delivery of the course and fit-testing. Group 1 were invited to receive fit-testing a specific time slots each day the project personnel were present at the site. Participants in Group 2 were invited to participate in the course prior to being scheduled for fit-testing. Approximately 6–10 participants were invited to each course.
Control
The control group was not invited to any activity conducted by the researchers or the project. To our knowledge, none of the participating plants conducted respirator fit-testing during the project period.
Statistical Analyses
Eleven participants stated that they had previously received fit-testing prior to the current study and were excluded. Demographic distributions between groups over time were investigated with Case-control studies odds ratios with Fisher’s exact p.
Confirmatory factor analysis was used to determine psychometric properties of the proposed factors containing single items. Raykov’s Reliability Coefficient was applied to investigate convergent reliability, values should exceed 0.70 (Mehmetoglu and Jakobsen, 2017, p. 304). Furthermore, discriminant validity was assessed by checking that the latent variables’ average variance extracted was larger than the squared correlations between them (Mehmetoglu and Jakobsen, 2017, p. 305). Robust regression was used to investigate the relationship between TPB-factors and groups on the intention to use respirators. Robust regression was used due to issues with heteroskedasticity (Mehmetoglu and Jakobsen, 2017, pp. 334–338). Due to non-normally distributed factors, non-parametric tests were run to investigate differences between groups before and after intervention and differences within groups. Kruskal–Wallis and Mann–Whitney tests were used to investigate differences between groups at T0 and T1. Paired Wilcoxon rank-sum tests were applied to investigate changes before and after intervention for the different groups. Participation in the intervention groups or the control group was dummy coded such that intervention groups could be distinguished from the other intervention group and the control group. All analyses were conducted in STATA 15.0 (64-bit) for Windows.
Ethics
The Regional Committee for Medical and Health Research Ethics declared that the project did not fall under the Norwegian health research legislation. In addition, the Norwegian Center for Research Data approved the method for collecting and storing data.
Results
Demographics
A total of 240 participants completed the post-intervention questionnaire. Reported demographics were based on those who had responded to both baseline and T1 (164/240). There were 146 males and 18 females, average age of 45.12 (SD = 13.05, range 18–69) and 75.15% had high-school or vocational diplomas. The distribution of demographics between groups over time were not significantly different. The distribution of participants from plants did not significantly differ over time.
Confirmatory Factor Analysis
The model achieved the following fit statistics; a comparative fit-index (CFI) of 0.98 and a Root mean squared error of approximation (RMSEA) of 0.06. The Organization factor did not achieve satisfactory levels of discriminant and convergent validity, with average variance extracted of 0.45. Furthermore, the Inconvenience factor achieved a Raykov’s factor reliability coefficient of 0.66. Therefore, items within these factors could not be considered to measure the same underlying structure with confidence nor were they sufficiently different from each other. Even though some of these factors have issues, the researchers argue that the items themselves are of interest and have a subjective value. Therefore, they were not altered. See Supplementary Appendix Table A1 for statistics of the confirmatory factor analysis.
Effects of Intervention
Kruskal–Wallis tests were performed to check for selection bias between those who answered only the baseline questionnaire and those who responded to both baseline and follow-up on all measured variables. No significant differences between groups were found.
Sum-scores of factors for the three groups were analyzed before and after interventions for comparison (Table 3). Both intervention groups (Group 1 and 2) showed an increase in knowledge regarding RPE use while the control group (Group 0) did not change. The median attitude score increased after intervention for both intervention groups, and was significantly higher in Group 2 compared to Group 1 and control after intervention. The subjective norms surrounding the use of RPE increased for group 2. Scores for Perceived behavioral control did not change for any group over time or between groups. Median scores for organizational items increased for Group 1. Both intervention groups showed a significant decrease in how much inconvenience they perceived by using RPE. Two research questions were central to this study, intent to use and rate of respirator use. Intention to use RPEs as well as rate of respirator use did not change over the intervention, nor were there differences between groups in this analysis.
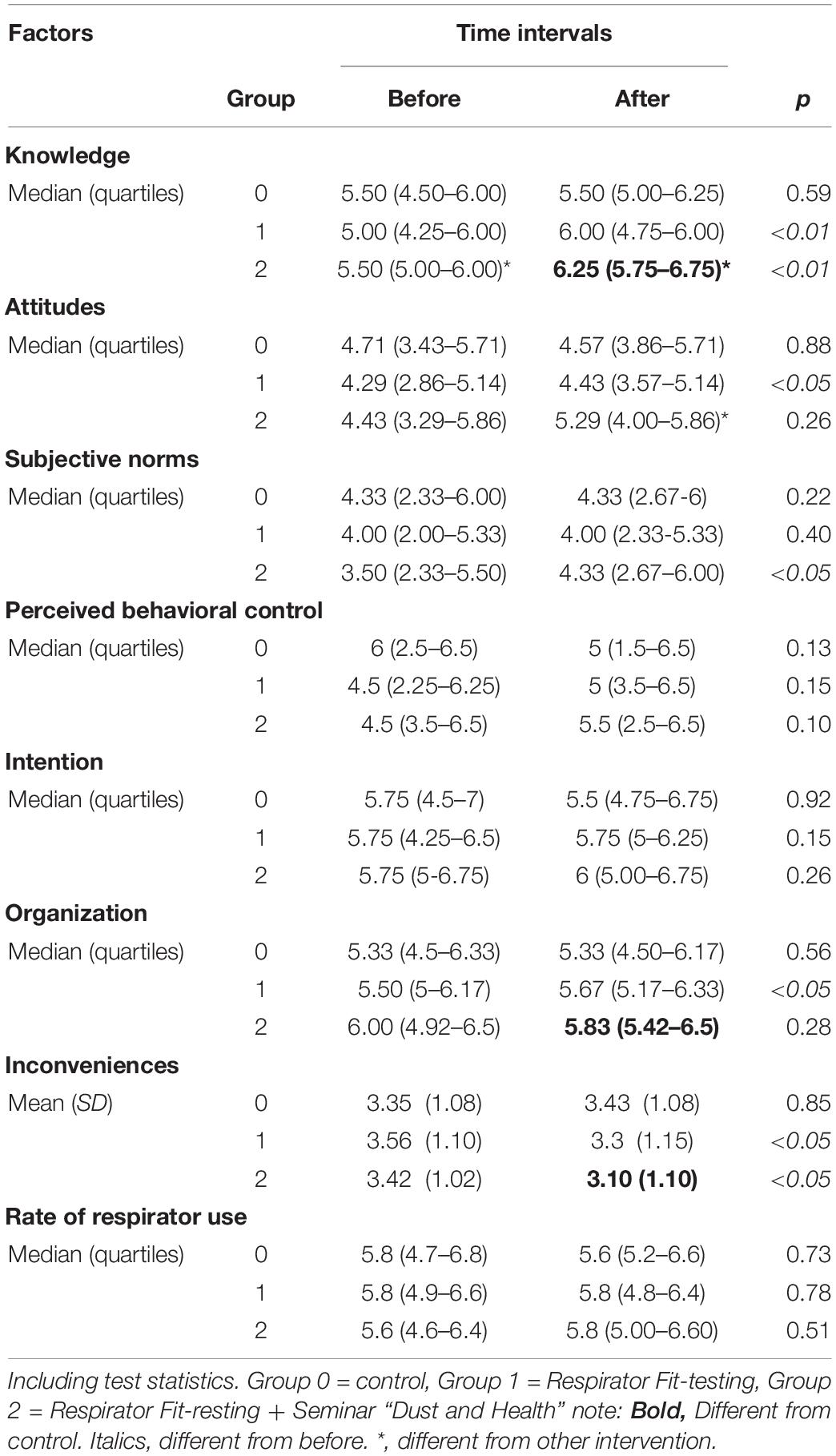
Table 3. Median and Mean scores on measured factors for the three intervention groups before and after intervention.
A multiple linear regression was calculated to predict Intention based on the independent variables; Attitudes, Subjective norms, Perceived control, Rate of respirator use, Group 1 and Group 2. A significant regression equation was found [F(6,228) = 38.75, p < 0.01], with an R2 of 0.55. Participants’ predicted Intention is equal to 1.53 + 0.28 (Attitudes) + 0.10 (Subjective norms) + −0.08 (Perceived control) + 0.30 (Group1) + 0.25 (Group 2), where Group 1 and Group 2 were coded as 0 = not participating and 1 = Participating. Participants Intention increased by 0.30 for participation in Group1 and 0.25 for participation in Group 2. Group 1 was the significant predictor of Intention. See Table 4 for details.
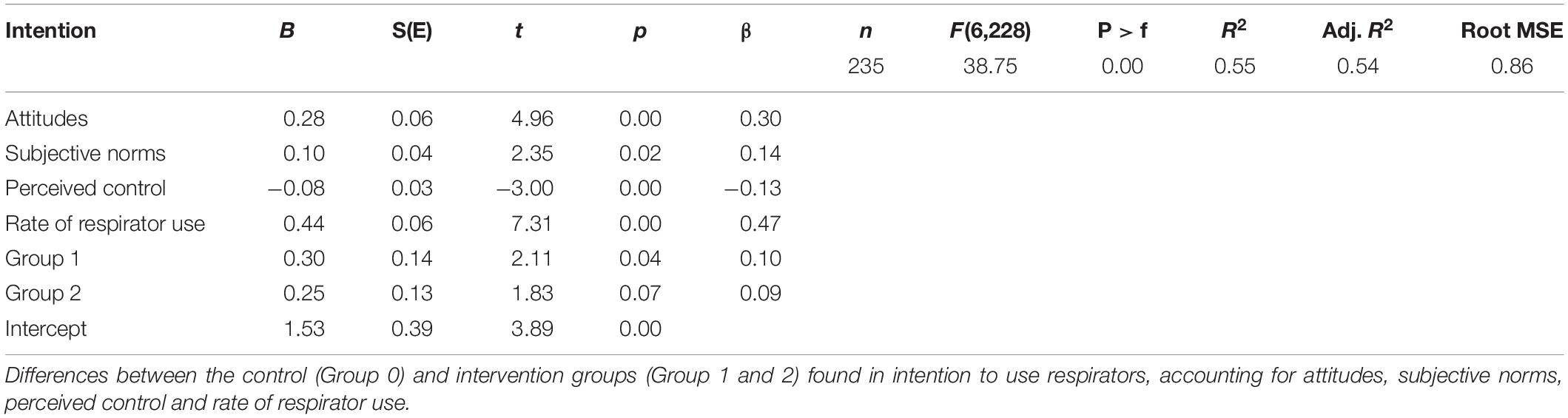
Table 4. Robust regression, after intervention.
Results showed that 54% of the variance in intentions to use RPE was explained by this model. Participation in the intervention (Group 1) significantly increased the intention to use RPE (Group 2 showed a marginally significant increase) over and above the effects of core TPB variables (attitude, subjective norms, perceived behavioral control, and previous behavior).
Discussion
The present study investigated the efficacy of a knowledge-based intervention containing two treatments aimed to increase workers’ knowledge and their general attitudes toward respiratory protective equipment (RPE) and their use. The intervention format was in part chosen because the authors wanted to test how fit-testing as an intervention would compare against a more common lecture-based intervention. As described earlier, Luong Thanh et al. (2016) showed small improvements in RPE use due to, among others, lecture based interventions. In addition, lecture based interventions are relatively easy to construct and perform. A review of the literature yielded no other studies addressing interventions among Norwegian smelter workers. Data was collected before and after intervention at six Norwegian smelting plants.
The design and content of the current intervention was partially based on research by Howie (2005), who provided a list of how to implement a successful program for RPE use. Howie pointed out the necessity of employee grounding in order to ensure the proper motivation for wearing RPE, including information of the consequences for the workers’ health from exposure, the necessity of having correct equipment available, knowledge of correct use and the importance of optimal fit. Graveling et al. (2011) also provided recommendations for proper RPE programs. They stated that all management levels need to understand the importance of, and need for RPE. These managers must also see to that appropriate RPE is supplied in sufficient quantities and that suitable provisions exist in order to clean, store and maintain RPE. Furthermore, they need to ensure that proper training and information is disseminated in the workforce. The RPEs need to fit individual employees, they should be comfortable and compatible with other PPE. The current study attempted to design an intervention intended to be used as a management tool to improve respirator use on employees using the aforementioned principles for RPE programs.
The current study aimed to deliver an efficient and applicable intervention to the smelting industry to optimize RPE use among the workers. The lecture was considered possible for non-scientific staff to implement for later use and course material was made accessible to all the smelters after the project, fit-testing should be performed by trained personnel.
Intervention groups (Group 1 and 2) were invited to RPE fit-testing, aiming to help the participant find a respirator that provided sufficient protection.
A comparable type of interactive training had been attempted in order to influence health workers’ attitudes toward RPEs. Carrico et al. (2007) performed an intervention consisting of classroom training combined with a visual bio-simulation training in order to increase RPE use for nurses working in a hospital. A control group received classroom training only. These authors did not report statistically significant difference between the two groups in respect to appropriate use of RPE for the nurses. However, they did find that nurses in the intervention group more often put a respirator on the patient compared to their control counterparts, suggesting that the intervention did have an effect. In the current study, no increase in rate of respirator use or intention to use respirators was observed. However, an increase in knowledge, attitudes toward RPE, subjective norms and a more positive view on the organization was found in addition to a decrease in the perception of inconvenience associated with RPE. There were no indications that conducting an intervention aiming to increase knowledge and attitudes toward the use of respirators affect smelting workers negatively.
Participants assigned to the control group did not report changes in any of the variables post intervention. Group 2 received the same RPE fit-testing procedure as group 1, in addition to a 45 min long educational lecture on dust, gas and fumes, health effects and protection. It was expected that the more comprehensive intervention given to group 2 would have a stronger effect. Both intervention groups showed increased scores on the Attitudes factor, although not statistically significant for group 2. Chatzisarantis and Hagger (2005) found that persuasive communications increased attitudes and intentions, but not reported behavior. However, there were some inconsistencies in the results of the current study. Group 1 increased their scores significantly on the organization factor, while group 2 did not, and vice versa for subjective norms. This indicated that going through RPE fit-testing resulted in a more positive view on the way the organization handled and administered RPE related issues. Since this effect was not observed in Group 2 it is possible that the content in the lecture may have modified the effect from the RPE fit-testing. It may also be a random effect. The increase on subjective norms in Group 2 may have indicated that participation in both fit-testing and the course increased perception of how colleagues evaluated RPE use. Accordingly, the content of the lecture may have altered perception of how people around them expect them to act. However, despite the described inconsistencies, the overall changes detected in the intervention groups compared to the control group suggest that the intervention was effective.
The clearest findings were increased knowledge scores for intervention groups. Knowledge increased for both intervention groups, and there were significantly higher scores in Group 2, as expected. Participants reported to know more about respirators, what they protected against and how they worked, after the intervention. The fact that the control group did not significantly change in knowledge score, indicated that the intervention measures were effective. Indeed, knowledge is considered an important precursor of behavior (Glanz and Bishop, 2010), although the causal relationship might not be a direct one. For instance, Fisher et al. (1996, p. 400) note that “knowledgeable individuals are not necessarily motivated to change their behavior, and motivated individuals are not necessarily well informed.” Donham et al. (2011) employed an intervention system (Certified Safe Farm) over a five-year period to e.g., increase the use of RPE, the knowledge of which type of RPE to use, understanding symptoms and possible health effects of exposure. These authors concluded that post intervention, farmers in the intervention group used RPEs more often than those in the control group, in addition, they suffered less acute symptoms of organic dust toxic syndrome. Dressel et al. (2007) reported similar results when measuring symptoms of asthma before and after educational interventions performed on farmers.
Perhaps the two most important outcome measures were participants’ intention to use RPE and rate of respirator use. Several studies have concluded that the use of respiratory protective equipment is not optimal in construction, manufacturing, health care, nuclear industry, farming and hazardous waste management (Salazar et al., 2001; Carpenter et al., 2002; Bryce et al., 2008; MacFarlane et al., 2008; Mitchell and Schenker, 2008; Tam and Fung, 2008; Han and Kang, 2009; Guseva Canu et al., 2013). Our own results indicated that most respondents in the current study had a high level of intent to use respirators at baseline and that they used respirators most of the time spent in exposed areas. The scores on Intention and RPE use did not change significantly post intervention, although regression analyses showed that allocation to an intervention group would predict an increased intention to use RPE. Given an average response rate of 34%, selection bias may have influenced the high baseline scores. Individuals who were more aware of health- and safety issues might have been more likely to participate. Non-responder analysis was not performed in this study, ergo this assumption will remain unanswered. Furthermore, the items included in the Intention factor were generated for the purpose of the current study and had not been validated elsewhere. It is possible that an optimized and more accurate instrument to measure intention would have been able to detect more subtle changes with greater accuracy. Nevertheless, the results are in line with existing literature reporting small increases in attitudes, knowledge and behavior after conducting similar interventions (Luong Thanh et al., 2016).
An observation often discussed at the plants with employees and management was that the observed non-compliance of respirator use was mostly a practical issue. In fact, previous analyses showed that only 4% of the respondents reported “laziness” or “bad excuses” as explanations to why they did not always wear RPE in exposed situations (Hegseth et al., 2018). However, comfort issues were reported as major reasons not to use RPE. Training in correct donning and finding a properly fitted respirator was expected to reduce discomfort and accommodate practical difficulties associated with RPE use. Indeed, the results showed that both intervention groups perceived significantly fewer practical challenges (Inconveniences) related to RPE use after the intervention compared to the control group. Improved knowledge of RPE and the possible health effects caused by exposure might have resulted in increased awareness of benefits of RPE use, which may have moderated the perception of practical disadvantages related to RPE use. However, this effect may be small, as indicated by previous findings, suggesting that beliefs about health benefits resulting from RPE influence use less than discomfort and inconvenience (White et al., 1988). The interventions may have provided participants with knowledge that they subsequently used to justify that RPEs are not as impractical or uncomfortable as previously experienced. It might therefore be that they do not experience less perceived inconveniences, but the knowledge they gained justified changes resulting in the measured decrease.
As reported from a study in a swine barn environment, the use of respirators can reduce negative acute health-effects in subjects not previously exposed to such environments (Dosman et al., 2000). There is no reason to assume that respirators would not help prevent non-acute issues as well. However, non-acute health issues that develop slowly over time are often considered less threatening than immediate and direct effects. Motivation to use RPE in order to prevent slowly progressing diseases such as COPD may therefore be moderate.
While implementation of interventions with an increase in awareness, attitudes, use of protective equipment and proper use of protective equipment are well documented in previous literature, proper randomization, use of controls and large samples are sometimes not well described or performed (Becker and Morawetz, 2004; Kim et al., 2012; Fu et al., 2013; Casalino et al., 2015; Navidian et al., 2015). Indeed, performing experimental procedures in applied settings where production is prioritized, can be impractical. Nevertheless, use of controls and random allocation into groups should be possible. Perry and Layde (2003) demonstrated that educational intervention sessions had an effect on participants’ knowledge, attitudes and use of protective equipment. Moreover, they noted that future interventions studies should ideally involve more than single-interventions.
Knowledge based interventions based on TPB have previously proven effective in increasing intentions and behavior, however no TPB-based intervention studies were found implemented in the Norwegian smelter industry. In the present study, one group received a single intervention, while the second group received two. Results did not show that either intervention were substantially superior to the other. Despite methodological short-comings, there seems to be a trend toward increased knowledge, attitudes and perceived inconveniences after the intervention. Future studies should investigate how comfort issues affect the use of RPE.
Conclusion
The intervention, consisting of a lecture and/or respirator fit-testing, significantly improved the participants’ knowledge of RPE, attitudes toward RPE use, perceptions of their organization and the perception of how their surroundings considered their RPE use. Additionally, less hassle and practical issues were associated with RPE use after the intervention. Whereas mean comparisons between prior and post-intervention did not show changes in intention to use RPE or rate of RPE use over the intervention, regression analysis of post-intervention data revealed significantly greater intention to use RPE in each intervention group. Our findings indicate that knowledge-based interventions are useful to optimize workers’ motivations and attitudes toward RPE use in terms of increased knowledge and customization of the equipment, but that innate practical issues with RPE use are major reasons for non-compliance with regulations and have to be addressed through other measures.
Practical Applications
The study intervention can be used as a framework for future health and safety work in industries where respiratory exposure represents a potential hazard. The current intervention was tailored for specific Norwegian smelting plants. The education package was based on exposure data from Norwegian smelters and addressed specific exposure scenarios for different plants, work-tasks and areas. To use the course in other industries, adjustments would be warranted to include specific exposure scenarios relevant to the designated work place. However, for most particle, gas and dust exposures, respiratory risks will be comparable, and the content of the course addressing this topic is employable in environments similar to smelters. The objective respirator fit-testing is applicable for all scenarios where employees are required to use respiratory protective equipment.
Limitations
The data used in the study was founded on self-reports of attitudes, perceived coworker behavior, intention and rate of RPE use. Biases such as social desirability must always be taken into account when assessing data based on self-reports. Furthermore, the self-reports were cross-sectional in time. Meaning that there might be a difference in reported intention and actual intention in the specific situation of interest. The randomization method applied in this study could have influenced measures in that the three groups were present at all plants, meaning that the participants in reality were free to converse and share information out of the control of the researchers.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
ØR: design, data collection, analysis, and writing. MH and SF: design, data collection, editing, and writing. FS: editing and writing. ME: editing and writing. HV: design, data collection, editing, and writing.
Funding
Project funding was granted by The Research Council of Norway (grant number: 245216), The Norwegian Ferroalloy Producers Research Association and the silicon carbide producers St. Gobain and Washintgon Mills.
Conflict of Interest
We wish to draw the attention to the following facts which may be considered as potential conflicts of interest and to significant financial contributions to this work. Funding for this research was received from The Research Council of Norway (NOK 12 million, grant number: 245216) and The Norwegian Ferroalloy Producers Research Association and the SiC producers Washington Mills and Saint Gobain (NOK 6 million). SF worked for Elkem from August 2013 to August 2014 as Corporate advisor in occupational hygiene and toxicology. However, SF was not working for Elkem during the project.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We wish to extend our gratitude to Simen Oscar Bø Wie, Marte Renate Thomassen, and Anna Aminoff for their invaluable help in conducting the intervention.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2020.00270/full#supplementary-material
References
Ajzen, I. (1985). “From intentions to actions: a theory of planned behavior,” in Action Control, eds J. Khul, and J. Beckmann (Berlin: Springer), 11–39. doi: 10.1007/978-3-642-69746-3_2
Ajzen, I. (1991). The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 50, 179–211. doi: 10.1016/0749-5978(91)90020-T
Armitage, C. J., and Conner, M. (2001). Efficacy of the theory of planned behaviour: a meta-analytic review. Br. J. Soc. Psychol. 40, 471–499. doi: 10.1348/014466601164939
Becker, P., and Morawetz, J. (2004). Impacts of health and safety education: comparison of worker activities before and after training. Am. J. Ind. Med. 46, 63–70. doi: 10.1002/ajim.20034
Berlinger, B., Bugge, M. D., Ulvestad, B., Kjuus, H., Kandler, K., and Ellingsen, D. G. (2015). Particle size distribution of workplace aerosols in manganese alloy smelters applying a personal sampling strategy. Environ. Sci. Process. Impacts 17, 2066–2073. doi: 10.1039/c5em00396b
Brubaker, R. G., and Fowler, C. (1990). Encouraging college males to perform testicular self-examination: evaluation of a persuasive message based on the revised theory of reasoned action. J. Appl. Soc. Psychol. 20, 1411–1422. doi: 10.1111/j.1559-1816.1990.tb01481.x
Bryce, E., Forrester, L., Scharf, S., and Eshghpour, M. (2008). What do healthcare workers think? A survey of facial protection equipment user preferences. J. Hosp. Infect. 68, 241–247. doi: 10.1016/j.jhin.2007.12.007
Carpenter, W. S., Lee, B. C., Gunderson, P. D., and Stueland, D. T. (2002). Assessment of personal protective equipment use among Midwestern farmers. Am. J. Ind. Med. 42, 236–247. doi: 10.1002/ajim.10103
Carrico, R. M., Coty, M. B., Goss, L. K., and LaJoie, A. S. (2007). Changing health care worker behavior in relation to respiratory disease transmission with a novel training approach that uses biosimulation. Am. J. Infect. Control 35, 14–19. doi: 10.1016/j.ajic.2005.12.013
Casalino, E., Astocondor, E., Sanchez, J. C., Díaz-Santana, D. E., Del Aguila, C., and Carrillo, J. P. (2015). Personal protective equipment for the Ebola virus disease: a comparison of 2 training programs. Am. J. Infect. Control 43, 1281–1287. doi: 10.1016/j.ajic.2015.07.007
Chatzisarantis, N. L., and Hagger, M. S. (2005). Effects of a brief intervention based on the theory of planned behavior on leisure-time physical activity participation. J. Sport Exerc. Psychol. 27, 470–487. doi: 10.1123/jsep.27.4.470
Donham, K. J., Lange, J. L., Kline, A., Rautiainen, R. H., and Grafft, L. (2011). Prevention of occupational respiratory symptoms among certified safe farm intervention participants. J. Agromedicine 16, 40–51. doi: 10.1080/1059924X.2011.532761
Dosman, J. A., Senthilselvan, A., Kirychuk, S. P., Lemay, S., Barber, E. M., Willson, P., et al. (2000). Positive human health effects of wearing a respirator in a swine barn. Chest 118, 852–860. doi: 10.1378/chest.118.3.852
Dressel, H., Gross, C., De la Motte, D., Sültz, J., Jörres, R., and Nowak, D. (2007). Educational intervention decreases exhaled nitric oxide in farmers with occupational asthma. Eur. Respir. J. 30, 545–548. doi: 10.1183/09031936.00023807
Ellingsen, D. G., Hetland, S. M., and Thomassen, Y. (2003). Manganese air exposure assessment and biological monitoring in the manganese alloy production industry. J. Environ. Monitor. 5, 84–90. doi: 10.1039/B209095C
Fishbein, M., and Ajzen, I. (2009). Predicting and Changing Behavior: The Reasoned Action Approach. New York, NY: Taylor & Francis.
Fishbein, M., Guenther-Grey, C., Johnson, W. D., and Wolitski, R. J. (1996). “Using a theory-based community intervention to reduce AIDS risk behaviors: the CDC’s AIDS community demonstration projects,” in The Claremont Symposium on Applied Social Psychology. Understanding and preventing HIV Risk Behavior: Safer Sex and Drug Use, eds S. Oskamp, and S. C. Thompson (Thousand Oaks, CA: Sage Publications, Inc), 177–206.
Fisher, J. D., Fisher, W. A., Misovich, S. J., Kimble, D. L., and Malloy, T. E. (1996). Changing AIDS risk behavior: effects of an intervention emphasizing AIDS risk reduction information, motivation, and behavioral skills in a college student population. Health Psychol. 15, 114–123. doi: 10.1037/0278-6133.15.2.114
Føreland, S., Bye, E., Bakke, B., and Eduard, W. (2008). Exposure to fibres, crystalline silica, silicon carbide and sulphur dioxide in the Norwegian silicon carbide industry. Ann. Occup. Hyg. 52, 317–336. doi: 10.1093/annhyg/men029
Fu, C., Zhu, M., Yu, T. S. I., and He, Y. (2013). Effectiveness of participatory training on improving occupational health in small and medium enterprises in China. Int. J. Occup. Environ. Health 19, 85–90. doi: 10.1179/2049396713Y.0000000021
Gjerde, C., Ferguson, K., Mutel, C., Donham, K., and Merchant, J. (1991). Results of an educational intervention to improve the health knowledge, attitudes and self-reported behaviors of swine confinement workers. J. Rural Health 7, 278–286. doi: 10.1111/j.1748-0361.1991.tb00728.x
Glanz, K., and Bishop, D. B. (2010). The role of behavioral science theory in development and implementation of public health interventions. Annu. Rev. Public Health 31, 399–418. doi: 10.1146/annurev.publhealth.012809.103604
Godin, G., and Kok, G. (1996). The theory of planned behavior: a review of its applications to health-related behaviors. Am. J. Health Promot. 11, 87–98. doi: 10.4278/0890-1171-11.2.87
Graveling, R., Sánchez-Jiménez, A., Lewis, C., and Groat, S. (2011). Protecting respiratory health: what should be the constituents of an effective RPE programme? Ann. Occup. Hyg. 55, 230–238. doi: 10.1093/annhyg/meq098
Guseva Canu, I., Faust, S., Canioni, P., Collomb, P., Samson, E., and Laurier, D. (2013). Attitude towards personal protective equipment in the French nuclear fuel industry. Arch. Ind. Hyg. Toxicol. 64, 285–292. doi: 10.2478/10004-1254-64-2013-2289
Han, D.-H., and Kang, M.-S. (2009). A survey of respirators usage for airborne chemicals in Korea. Ind. Health 47, 569–577. doi: 10.2486/indhealth.47.569
Harber, P., Boumis, R. J., Su, J., Barrett, S., and Alongi, G. (2013). Comparison of three respirator user training methods. J. Occup. Environ. Med. 55, 1484–1488. doi: 10.1097/JOM.0000000000000010
Hegseth, M. N., Robertsen, Ø., Aminoff, A., Vangberg, H. C. B., and Føreland, S. (2018). “Reasons for not using respiratory protective equipment and suggested measures to optimize use in the Norwegian silicon carbide, ferro- and silicon-alloy industry,” in Paper Presented at the Infacon XV: International Ferro-Alloys Congress, Cape Town.
Howie, R. (2005). Respiratory protective equipment. Occup. Environ. Med. 62, 423–428. doi: 10.1136/oem.2002.004424
HSE (2012). Fit Testing of Respiratory Protective Equipment facepieces. London: Health and Safety Executive.
Jemmott, J. B. III, Jemmott, L. S., and Fong, G. T. (1998). Abstinence and safer sex HIV risk-reduction interventions for African American adolescents: a randomized controlled trial. JAMA 279, 1529–1536. doi: 10.1001/jama.279.19.1529
Johnsen, H. L., Kongerud, J., Hetland, S. M., Benth, J. Š., and Søyseth, V. (2008). Decreased lung function among employees at Norwegian smelters. Am. J. Ind. Med. 51, 296–306. doi: 10.1002/ajim.20557
Kero, I., Grådahl, S., and Tranell, G. (2017). Airborne emissions from Si/FeSi production. JOM 69, 365–380. doi: 10.1007/s11837-016-2149-x
Kero, I. T., and Jørgensen, R. B. (2016). Comparison of three real-time measurement methods for airborne ultrafine particles in the silicon alloy industry. Int. J. Environ. Res. Public Health 13:871. doi: 10.3390/ijerph13090871
Kim, J., Arrandale, V., Kudla, I., Mardell, K., Lougheed, D., and Holness, D. (2012). Educational intervention among farmers in a community health care setting. Occup. Med. 62, 458–461. doi: 10.1093/occmed/kqs129
Lunt, J., Sheffield, D., Bell, N., Bennett, V., and Morris, L. (2011). Review of preventative behavioural interventions for dermal and respiratory hazards. Occup. Med. 61, 311–320. doi: 10.1093/occmed/kqr099
Luong Thanh, B. Y., Laopaiboon, M., Koh, D., Sakunkoo, P., and Moe, H. (2016). Behavioural interventions to promote workers’ use of respiratory protective equipment. Cochrane Database Syst. Rev. 12:CD010157. doi: 10.1002/14651858.CD010157.pub2
MacFarlane, E., Chapman, A., Benke, G., Meaklim, J., Sim, M., and McNeil, J. (2008). Training and other predictors of personal protective equipment use in Australian grain farmers using pesticides. Occup. Environ. Med. 65, 141–146. doi: 10.1136/oem.2007.034843
Mehmetoglu, M., and Jakobsen, T. G. (2017). Applied Statistics Using Stata: A Guide for The Social Sciences. London: Sage Publications ltd.
Mitchell, D. C., and Schenker, M. B. (2008). Protection against breathing dust: behavior over time in Californian farmers. J. Agric. Saf. Health 14, 189–203. doi: 10.13031/2013.24350
Mullan, B., Smith, L., Sainsbury, K., Allom, V., Paterson, H., and Lopez, A.-L. (2015). Active behavior change interventions in the construction industry: a systematic review. Saf. Sci. 79, 139–148. doi: 10.1016/j.ssci.2015.06.004
Murphy, W. G., and Brubaker, R. G. (1990). Effects of a brief theory-based intervention on the practice of testicular self-examination by high school males. J. Sch. Health 60, 459–462. doi: 10.1111/j.1746-1561.1990.tb05977.x
Myers, W. R., Jaraiedi, M., and Hendricks, L. (1995). Effectiveness of fit check methods on half mask respirators. Appl. Occup. Environ. Hyg. 10, 934–942. doi: 10.1080/1047322X.1995.10387716
Navidian, A., Rostami, Z., and Rozbehani, N. (2015). Effect of motivational group interviewing-based safety education on Workers’ safety behaviors in glass manufacturing. BMC Public Health 15:929. doi: 10.1186/s12889-015-2246-8
Noar, S. M., Benac, C. N., and Harris, M. S. (2007). Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol. Bull. 133, 673–693. doi: 10.1037/0033-2909.133.4.673
Or, P., Chung, J., and Wong, T. (2012). Does training in performing a fit check enhance N95 respirator efficacy? Workplace Health Saf. 60, 511–515. doi: 10.3928/21650799-20121128-76
Perry, M. J., and Layde, P. M. (2003). Farm pesticides: outcomes of a randomized controlled intervention to reduce risks. Am. J. Prev. Med. 24, 310–315. doi: 10.1016/S0749-3797(03)00023-0
Robertsen, Ø., Siebler, F., Eisemann, M., Hegseth, M. N., Føreland, S., and Vangberg, H. C. B. (2018). Predictors of respiratory protective equipment use in the norwegian smelter industry. The role of the theory of planned behavior, safety climate and work experience in understanding protective behavior. Front. Psychol. 9:1366. doi: 10.3389/fpsyg.2018.01366
Salazar, M. K., Connon, C., Takaro, T. K., Beaudet, N., and Barnhart, S. (2001). An evaluation of factors affecting hazardous waste workers’ use of respiratory protective equipment. AIHAJ 62, 236–245. doi: 10.1080/15298660108984627
Shamsi, M., Pariani, A., Shams, M., and Soleymani-Nejad, M. (2015). Persuasion to use personal protective equipment in constructing subway stations: application of social marketing. Inj. Prev. 22, 149–152. doi: 10.1136/injuryprev-2014-041461
Sintef (2015). DeMaskUs. Available at: https://www.sintef.no/en/projects/demaskus/ (accessed January 24, 2019).
Søyseth, V., Johnsen, H. L., Bugge, M. D., Hetland, S. M., and Kongerud, J. (2011). Prevalence of airflow limitation among employees in Norwegian smelters: a longitudinal study. Occup. Environ. Med. 68, 24–29. doi: 10.1136/oem.2009.049452
Søyseth, V., Johnsen, H. L., Henneberger, P. K., and Kongerud, J. (2015). Increased decline in pulmonary function among employees in Norwegian smelters reporting work-related asthma-like symptoms. J. Occup. Environ. Med. 57, 1004–1008. doi: 10.1097/JOM.0000000000000518
Søyseth, V., Johnsen, H. L., and Kongerud, J. (2013). Respiratory hazards of metal smelting. Curr. Opin. Pulm. Med. 19, 158–162. doi: 10.1097/MCP.0b013e32835ceeae
Szeinuk, J., Beckett, W. S., Clark, N., and Hailoo, W. L. (2000). Medical evaluation for respirator use. Am. J. Ind. Med. 37, 142–157. doi: 10.1002/(sici)1097-0274(200001)37:1<142::aid-ajim11>3.0.co;2-k
Tam, V., and Fung, I. (2008). A study of knowledge, awareness, practice and recommendations among Hong Kong construction workers on using personal respiratory protective equipment at risk. Open Constr. Build. Technol. J. 2, 69–81. doi: 10.2174/1874836800802010069
White, M. C., Baker, E. L., Larson, M. B., and Wolford, R. (1988). The role of personal beliefs and social influences as determinants of respirator use among construction painters. Scand. J. Work Environ. Health 14, 239–245. doi: 10.5271/sjweh.1926
Keywords: intervention, respiratory protective equipment, theory of planned behavior, industry, smelting
Citation: Robertsen Ø, Hegseth MN, Føreland S, Siebler F, Eisemann M and Vangberg HCB (2020) The Effect of a Knowledge-Based Intervention on the Use of Respirators in the Norwegian Smelter Industry. Front. Psychol. 11:270. doi: 10.3389/fpsyg.2020.00270
Received: 07 November 2019; Accepted: 04 February 2020;
Published: 20 February 2020.
Edited by:
Carlos María Alcover, Rey Juan Carlos University, SpainReviewed by:
Patrick O’Shaughnessy, The University of Iowa, United StatesLi Lin, The University of Oklahoma, United States
Copyright © 2020 Robertsen, Hegseth, Føreland, Siebler, Eisemann and Vangberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hans Christian Bones Vangberg, aGFucy5jaHJpc3RpYW4udmFuZ2JlcmdAdW5uLm5v