 Kristine Gustavsen Madsø
Kristine Gustavsen Madsø Elisabeth Flo-Groeneboom
Elisabeth Flo-Groeneboom Nancy A. Pachana
Nancy A. Pachana Inger Hilde Nordhus
Inger Hilde Nordhus- 1Department of Clinical Psychology, Faculty of Psychology, University of Bergen, Bergen, Norway
- 2NKS Olaviken Gerontopsychiatric Hospital, Bergen, Norway
- 3School of Psychology, The University of Queensland, Brisbane, QLD, Australia
- 4Department of Behavioral Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway
Optimizing the possibility to lead good lives is at the core of treatment and care for people with dementia. This may be monitored by assessing well-being and quality of life. However, cognitive impairment following dementia may complicate recall-based assessment with questionnaires, and proxy-ratings from family-caregivers do not correspond well to self-reports. Thus, using observational measures represents a potentially advanced option. Systematic reviews evaluating measurement properties, interpretability and feasibility of observational instruments assessing well-being in people living with dementia are lacking. Thus, this review performed systematic searches to find peer reviewed validated instruments of relevance in the databases MEDLINE, EMBASE, PsycINFO, Web of Science, CINAHL and ProQuest. Twenty-two instruments assessing well-being were included for evaluation of measurement properties based on the systematic approach of the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN). The evaluation included risk of bias on study level, and assessment of measurement properties on instrument level including content validity, construct validity, structural validity, internal consistency, measurement invariance, cross-cultural validity, measurement error and inter-rater/intra-rater/test–retest reliability and responsiveness. Additionally, the feasibility and interpretability of the measures were evaluated. No single instrument could be recommended based on existing publications. Thus, we provide general recommendations about further assessment and development of these instruments. Finally, we describe the most promising instruments and offer guidance with respect to their implementation and use in clinical and research contexts.
Introduction
Well-being and quality of life (QoL) are identified as core outcomes for psychosocial interventions by people living with dementia (Øksnebjerg et al., 2018; Reilly et al., 2020), in public health initiatives (World Health Organization [WHO], 2017), national guidelines (National Institute for Health and Care Excellence [NICE], 2018), and research recommendations (Dröes et al., 2016). World-wide, dementia is estimated to affect 50 million people (Livingston et al., 2017). Dementia is defined as a public health priority, causing disability and increasing dependency on help from others in the people affected (World Health Organization [WHO], 2017). However, increasing evidence highlights how people with dementia may live good lives in environments adapted to their physical, social, emotional, and psychological needs (Livingston et al., 2017).
To be able to ascertain whether the dementia care and interventions implemented actually promote individual well-being, valid measurement approaches reflecting well-being as it is described by the target group are needed (Madsø and Nordhus, 2021). In a recent scoping review, relevant well-being domains close to the experiences of people living with dementia were defined. These domains include positive emotions, experiencing meaning, a positive sense of self and a sense of agency, having rewarding relationships with significant others, and experiencing life satisfaction (Clarke et al., 2020). Well-being and QoL originate from separate research fields (Skevington and Böhnke, 2018), but have also been used synonymously in the dementia literature (Bowling et al., 2015). In this review, the term well-being is used when the domains are in line with Clarke et al. (2020).
In other populations, well-being is often measured by self-report (Ferring and Boll, 2010). It is well established that people in the earlier stages of dementia can provide valid self-reports of their well-being (Stoner et al., 2019; Clarke et al., 2020). Unfortunately, relying on self-report only may exclude people with more severe dementia, and reduce the possibility of longitudinal assessment throughout the degenerative course of the disease (Algar et al., 2016; Kaufmann and Engel, 2016). With increasing cognitive impairment, well-being is frequently assessed through proxy-reports. Proxy-reports refer to assessment of an individual based on the evaluations of informants other than the person themself. Studies have consistently found proxy-evaluations by family and professional caregivers to rate well-being lower as compared to self-reports (Sands et al., 2004; Kolanowski et al., 2007; Ferring and Boll, 2010; Schulz et al., 2013). The low correspondence between proxy-reports and self-report implies that well-being in dementia should be measured in face-to-face interviews for individuals able to give valid self-reports, together with observational measures by independent and neutral observers in those from whom self-reports may not be obtained (Ferring and Boll, 2010; Bowling et al., 2015).
It is well known that a measurement that relies on retrospective self-reports evaluating longer time-intervals is prone to bias because our autobiographical recall can be inaccurate and influenced by for example current mood (Shiffman et al., 2008). This may particularly be a source of bias in the dementia population due to impairments in memory, attention, insight, and communication skills (Ettema et al., 2007; Trigg et al., 2011). During retrospective self-report, the current emotional state may interfere with the judgment of the past (Kolanowski et al., 2014). Thus, the risk of substantial measurement error from self-reports is increased by the fluctuating nature of neuropsychiatric symptoms (Kales et al., 2015), as well as attention or awareness (Clare et al., 2012). Consequently, an alternative is to use Ecological Momentary Assessment (EMA) and assess well-being within a momentary timeframe that can detect clinically relevant variations occurring over short time intervals (Shiffman et al., 2008). EMA consists of several approaches - direct observation is one of them. Assessing well-being in dementia through observing behavior as it occurs is one approach that can omit several of the problems and sources of bias related to measurement in dementia as mentioned above (Ferring and Boll, 2010). In sum, observational methods are advantageous because (1) they can be used to assess subjects that struggle with self-report, (2) neutral observers may provide more accurate evaluations than proxies, (3) it is not dependent on memory of the past, and (4) it is sensitive to changes in state.
However, the well-being domains identified as central in dementia by Clarke et al. (2020) are not all available for assessment through observation. Assessing well-being through observation implies coding or rating behavioral expressions, bodily positions, verbal or non-verbal expressions, or facial expressions that are all assumed to indicate the inner state of the observed person. Thus, we suggest observable aspects in line with the model of Clarke et al. (2020) are operationalized expressions of well-being in terms of positive behavioral expressions, balance between positive and negative emotions, level of engagement, expressions of satisfaction, and quality of social relationships. These aspects reflect central domains from the perspective of people living with dementia (Clarke et al., 2020) and central theories of well-being (Diener, 1984) and well-being in dementia (Lawton et al., 1996; Kitwood, 1997). The remaining domains of Clarke et al. (2020) related to experiencing meaning, having a positive sense of self and a sense of agency, may better be assessed through self-report. Still, accessing these domains and describing them may be difficult for people with more moderate and severe dementia.
Former reviews have reported on a variety of observational measures for people living with dementia (Curyto et al., 2008), including observational instruments specific for well-being and QoL in dementia (Algar et al., 2016), and measurements of emotional expressions in dementia (Lee et al., 2019). However, there is a lack of systematic reviews evaluating measurement instruments assessing momentary well-being in dementia that includes an evaluation against quality criteria and risk of bias. The COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) initiative is a relevant systematic approach for reviewing health related outcome instruments (Prinsen et al., 2018). COSMIN is developed through extensive Delphi-studies with experts and in concordance with well-established systematic approaches for conducting reviews such as the Cochrane Handbook, the PRISMA statement, and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) principles (Mokkink et al., 2017; Prinsen et al., 2018; Terwee et al., 2018).
Our objective is to systematically review the literature and inform researchers and practitioners about the current state of knowledge and clinical utility of observational instruments assessing momentary well-being, to support care and interventions for people living with dementia. Guided by the COSMIN-framework, this systematic review aims to:
1. Identify observational instruments assessing momentary well-being in people with dementia.
2. Evaluate study specific methodological quality of the included publications through risk of bias (RoB) ratings.
3. Evaluate and compare measurement properties against quality criteria at instrument level.
4. Summarize and grade the trustworthiness of the body of evidence for each instrument.
5. Assess feasibility and interpretability of the instruments.
Methods
The protocol for this review was pre-registered in the international register of systematic reviews, PROSPERO (RRID:SCR_019061, ID: 176160). Figure 1 describes the COSMIN-guideline for conducting systematic reviews on health-related outcome measures that was utilized in this review.
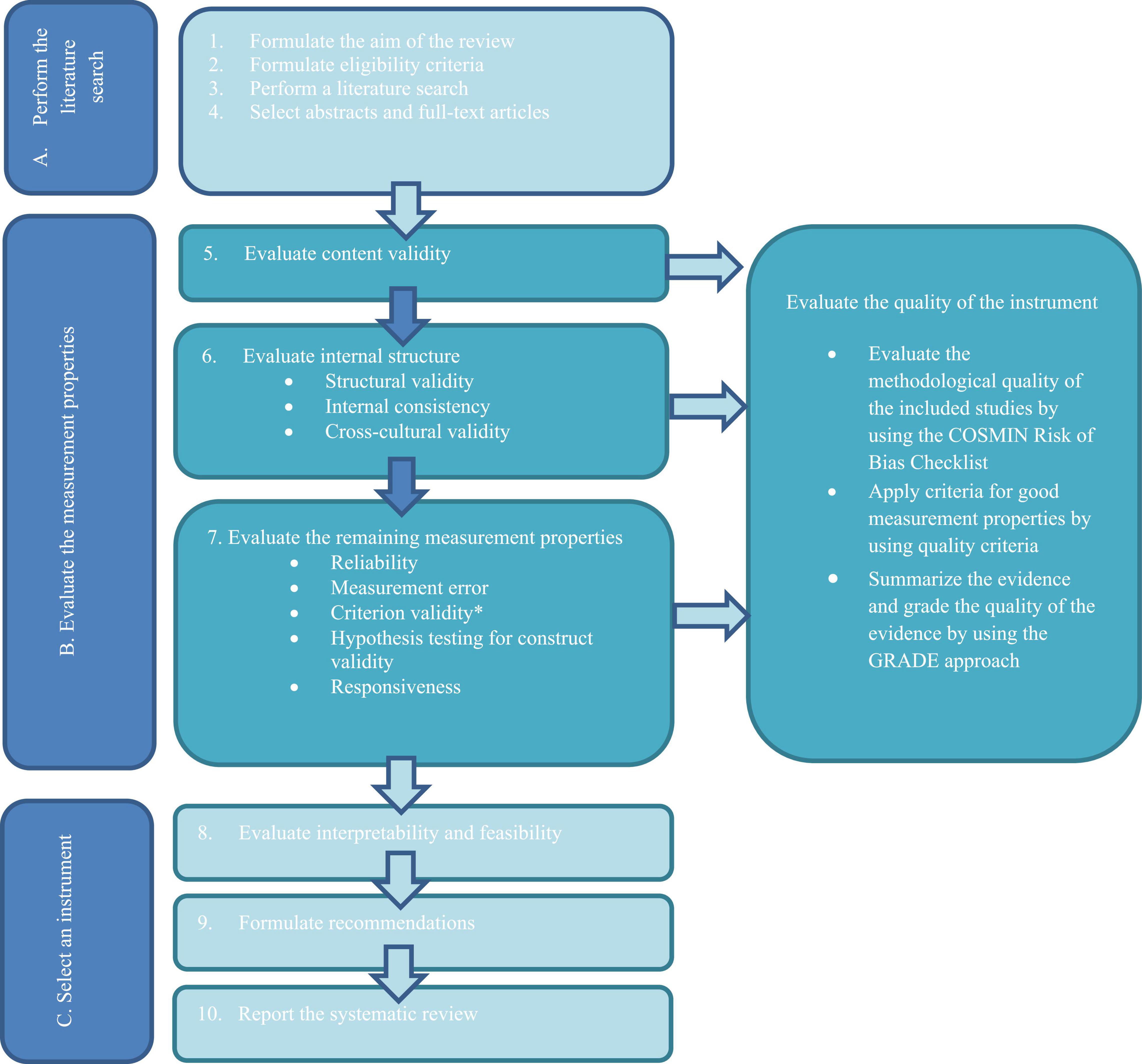
Figure 1. COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) guideline for systematic reviews of health-related measurement instruments. Reprint of this figure from Prinsen et al. (2018) is permitted under the Creative Commons Attribution 4.0. (http://creativecommons.org/licenses/by/4.0/). The acronym PROM (Patient Rated Outcome Instrument) is changed to “instrument” in this reprint. *Criterion validity was not assessed in this review, as no gold-standard instrument for comparison was identified.
Inclusion and Exclusion Criteria
Criteria for inclusion were (a) observational measures of momentary well-being (b) assessed by independent observers (c) during direct observation or video-recordings, containing (d) observable operationalizations of well-being such as positive and negative emotions/affect, or behavioral displays of satisfaction or engagement. Instruments should assess well-being (e) before, during and/or after psychosocial interventions over (f) short time intervals (minutes or hours). At least one psychometric property should be reported, and g) instruments not exclusively assessing well-being could be included, but only the well-being domain would be assessed. Instruments developed for the general population could be included if they also were specifically tested in people with dementia. Only English peer-reviewed journal articles were included.
Exclusion criteria were observational instruments (a) focusing merely on ill-being, such as negative emotions, anxiety, depression or neuropsychiatric symptoms, and instruments measuring (b) observable physiological indicators of well-being only (such as biomarkers or startle reflex).
Search Strategy
Searches were performed on April 21st, 2020, and repeated on April 06th, 2021, in the databases MEDLINE, EMBASE, PsycINFO (all via OVD), Web of ScienceTM, CINAHL (via EBSCOhost) and ProQuest® (Psychology and Nursing and Allied Health). A combination of the words “well-being,” “dementia,” “observation,” “measurement,” and “psychometric properties” were searched for, using both Boolean operators and truncations. We utilized the published search filter with words describing measurement properties of outcome instruments from Terwee et al. (2009). The full search strategy corresponding to the databases is available in Supplementary Appendix A.
The search was limited to peer-reviewed journal articles, searching in title, abstract and subject headings. In addition, we hand-searched reference lists of relevant reviews, investigated reference lists and forward chained citations of the included publications. Authors of relevant articles were contacted when the publication did not provide the full observation tool. Other publication types, such as conference proceedings, editorials and books were excluded (Prinsen et al., 2018), as were articles where the instrument was not accessible and lacked a full description of the operationalizations of the items in the publication.
Selection of Studies
The first author (KM) carried out the searches in the databases, imported the results to Endnote® (RRID:SCR_014001) where the results were checked, and duplicates removed. Next, KGM screened the titles and imported the records eligible for screening of abstract to Rayyan QCRI® (RRID:SCR_017584). KM also conducted hand searches of relevant records and imported these to Rayyan. The first (KM) and last (IN) author independently screened the records in Rayyan based on the eligibility criteria. Next, the results from the independent screening were compared, and all conflicts and their solutions of abstract screening were logged to ensure transparency. The next step was to evaluate the included publication based on full text. KM and IN read the full text independently and evaluated the publications against eligibility criteria in team meetings.
Data Extraction
Extraction was conducted by the first author (KM) and reviewed by a team including three of the authors (KM, EF-G, and IN). 20% of the data was extracted twice by the first author (KM) to ensue correct extraction. The extraction procedure was predefined and based on the COSMIN extraction tables (Prinsen et al., 2018). The first category addressed conceptualization (overarching conceptualization of well-being, population the instrument was developed in, and well-being domains assessed). The second category addressed central study characteristics (population, setting, methods, and results) for publications reporting on any of the measurement properties “content validity,” “structural validity,” “internal consistency,” “cross-cultural validity/measurement invariance,” “reliability,” “measurement error,” “construct validity” through hypothesis testing, and “responsiveness” (Mokkink et al., 2017; Prinsen et al., 2018; Terwee et al., 2018). The third category addressed feasibility (procedure, granularity, concreteness, training, requirements) and interpretability (measurement level and scoring, primary recording units, distribution, and sensitivity; Bakeman and Quera, 2012; Mokkink et al., 2017; Prinsen et al., 2018; Terwee et al., 2018).
Granularity refers to how fine grained and detailed the instrument is. Concreteness refers to how physically based the items are, where high concreteness involves bodily movement and low concreteness allows for interpretation of inner states. Measurement level defines which research questions may be asked, from nominal and ordinal to continuous output. Lastly, the primary recording unit defines how you sample the observations, from counting specific events in continuous or pre-specified intervals, to continuous recordings of duration (Bakeman and Quera, 2012; Chorney et al., 2015).
An overview of the COSMIN-definitions of central measurement properties of health-related instruments are provided in Table 1.
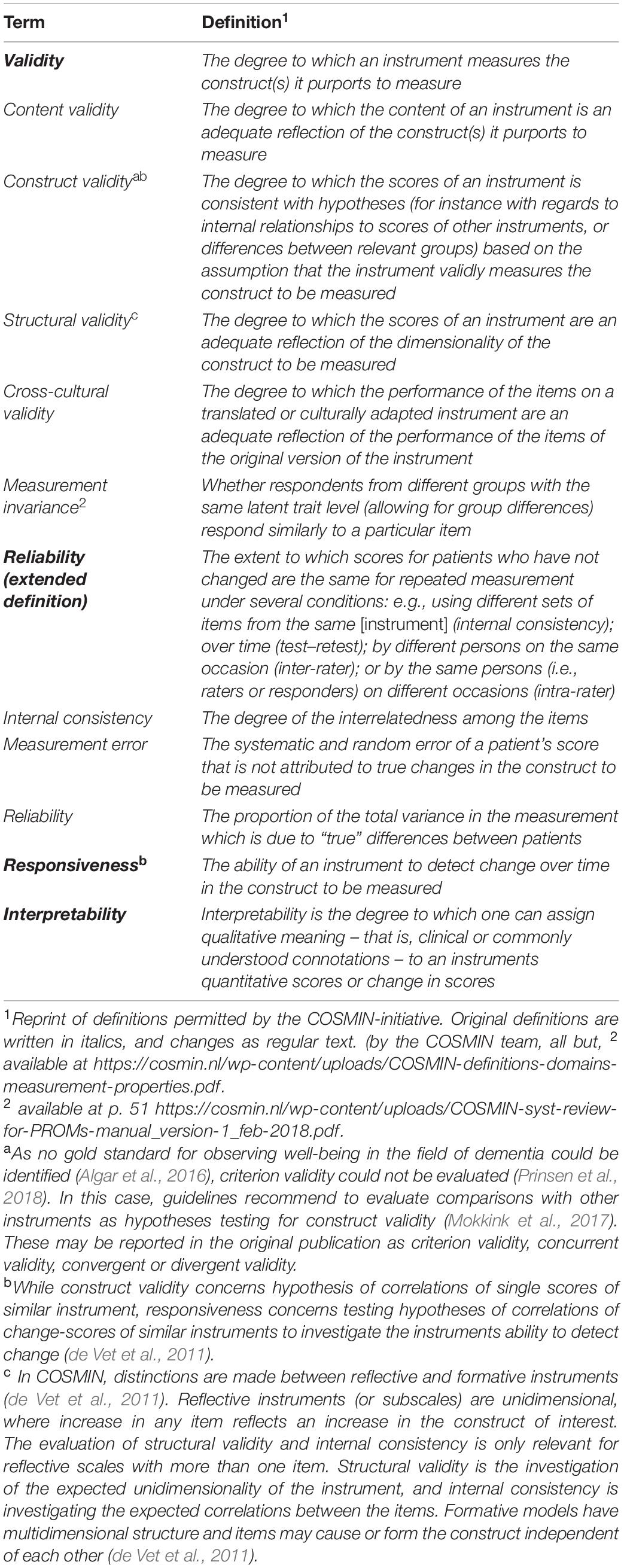
Table 1. COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) definitions of central terms.
Evaluating Methodological Quality
Study specific RoB-ratings from multiple sources per instrument were ranked with the categories “very good,” “adequate,” “doubtful,” “inadequate,” and “not applicable.” RoB-ratings were conducted by KM and IN in collaboration. Conflicting ratings were discussed with EF-G or NP. Rating criteria were based on the COSMIN RoB Checklist (Mokkink et al., 2017; Prinsen et al., 2018). The COSMIN-framework is created for patient-reported measurement instruments. To fit the COSMIN evaluations to the specific requirements for observational measures, some adaptations to the COSMIN-criteria were necessary. These mainly regarded the evaluation of content validity of the instruments. Our adaptations were based on recommendations from Bakeman and Quera (2011) and Bakeman and Quera (2012), and can be found in the Supplementary Material (Supplementary Table 1).
Consensus-based Standards for selection of health Measurement Instruments (COSMIN)-criteria for the content validity of self-reported measures are strongly based on feedback from the target group to assess relevance, comprehensiveness, and comprehensibility of the content of an instrument. Criteria for “relevance” requires items to be relevant for the construct of interest, the target population, and the context of use. To be “comprehensive,” the items need to cover all key aspects of the construct (Terwee et al., 2018). We adapted the evaluations of content validity to observational measures based on Bakeman and Quera (2012); Chorney et al. (2015); and Perugia et al. (2018b). To get an “adequate” or “good” rating of content validity, our team decided at least two of the following approaches were required: theoretical approaches with literature reviews, qualitative field work and development of coding scheme or ethogram, and quantitative survey or qualitative interviews including the target group (people with dementia or their close care givers and/or experts from all relevant disciplines). In addition, lack of pilot field testing followed by evaluation and revision of the “comprehensibility” of the instrument lead to a rating of “inadequate.”
Content validity is context- and population specific, implying that in this review the instruments’ content validity is evaluated for the specific construct (well-being) in the specific context of evaluating psychosocial interventions for persons living with dementia (Terwee et al., 2018). Thus, evidence of content validity in other populations or contexts may not be generalizable and are not included.
As lack of a priori hypotheses is a common bias in health-related measurement development, we used a recommended generic hypothesis from COSMIN for evaluating construct validity and responsiveness (Prinsen et al., 2018, Table 4, p. 1154). COSMIN recommends similar constructs to be evaluated against a threshold of ± ≥ 0.5, and related but dissimilar constructs to be evaluated against a threshold of ± ≥ 0.3. Defining constructs as similar or only related a priori is a complex task. Relevant sources of measurement error identified in previous reviews are: (1) comparisons between state or trait dimensions (Curyto et al., 2008); (2) comparing self-, proxy- and observer-rated measures (Ferring and Boll, 2010); and (3) comparing instruments with different timeframes (Shiffman et al., 2008). Thus, we chose to use the recommended threshold of ± ≥ 0.3 as our threshold of comparison.
In addition, we did not expect decreasing well-being-scores to correlate with increasing dementia severity or cognitive impairment, as these constructs are found to be independent in several reviews (e.g., Missotten et al., 2008; Martyr et al., 2018).
Inter-rater reliability and agreement are particularly important properties of observational measures, and the new COSMIN-consensus regarding ratings of reliability and measurement error for clinician rated instruments was incorporated (Mokkink et al., 2020). The principle for overall quality scorings is ‘the worst score counts’, and one uses the lowest rating of the measurement property to indicate RoB (Mokkink et al., 2017; Prinsen et al., 2018; Terwee et al., 2018). COSMIN guidelines are available at www.cosmin.nl.
Data Synthesis
After the initial study specific evaluation, the total evidence provided for each instrument was rated against adapted COSMIN quality criteria using the ratings “good” (+), “unclear” (?), “inadequate” (-), = “conflicting” (±), “not evaluated” (NE), and “not applicable” (NA). Table 2 provides an overview of the quality criteria. As most instruments were investigated in one publication only, no quantitative data synthesis was obtainable except for construct validity. For construct validity, the summarized number of hypotheses supporting the construct was divided by the sum of hypotheses (Prinsen et al., 2018).
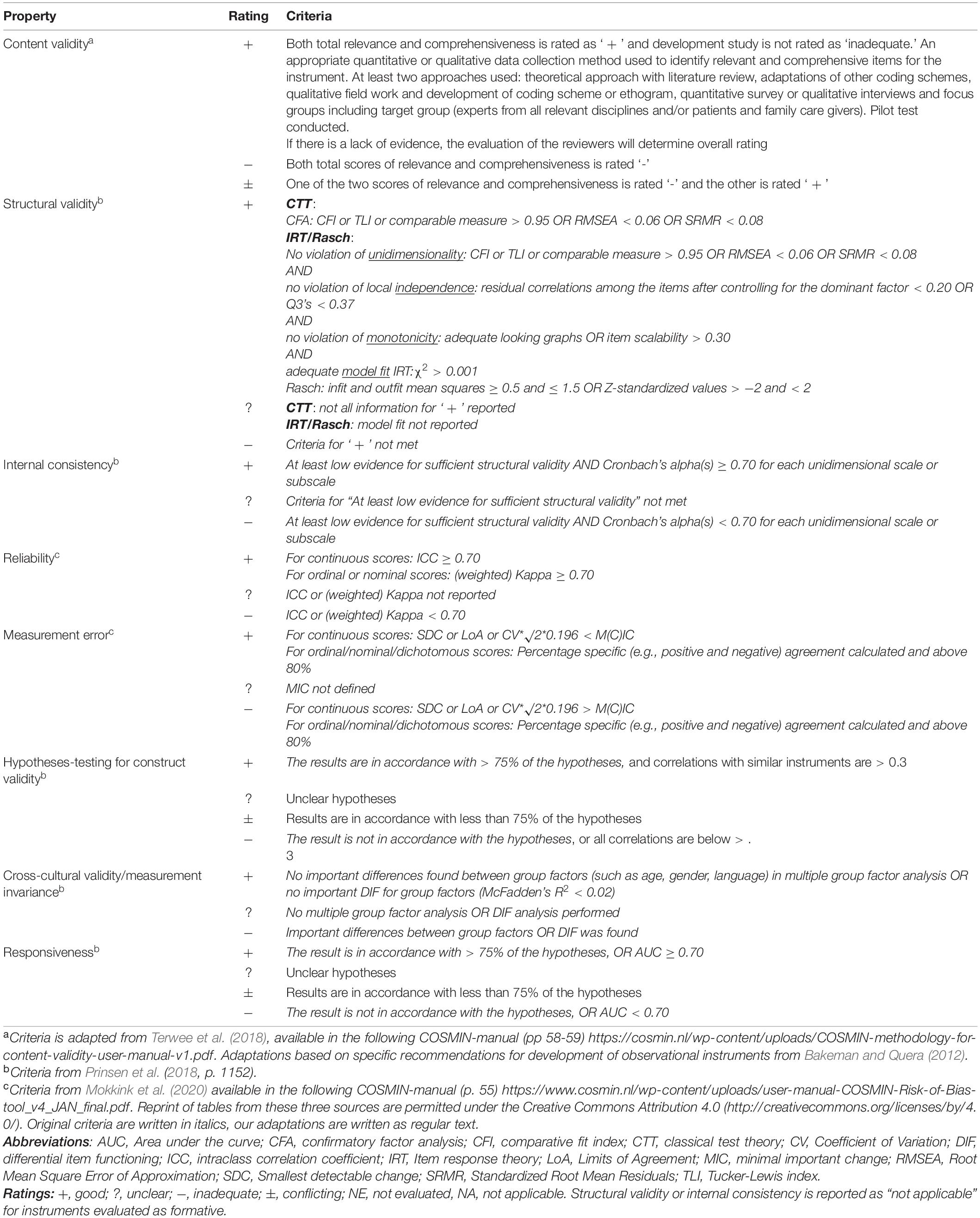
Table 2. Adapted COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN)-quality criteria.
The trustworthiness of the summarized quality criteria rating was ranked with Grading of Recommendations Assessment, Development and Evaluation (GRADE) principles (GRADE Handbook, 2013), modified in the COSMIN approach for the context of health-related outcome measures (Prinsen et al., 2018). Four factors are assessed on instrument level: “risk of bias,” “inconsistency,” “imprecision,” and “indirectness” of the evidence, graded as “high,” “moderate,” “low,” or “very low”. Ratings were conducted in team meetings with KM and IN, including EF-G if consensus was not met.
Results
Search Results
Search results and reasons for exclusion is presented in Figure 2. After removing duplicates, KM screened 4309 records by title. Then, the 255 publications eligible for evaluation of abstracts was blind screened for inclusion by KM and IN (82% agreement). Additionally, 25 publications were added through hand search of relevant records. After full-text review of 87 records by KM and IN, 36 articles describing a total of 22 instruments were included, of which three originated from the hand-search.
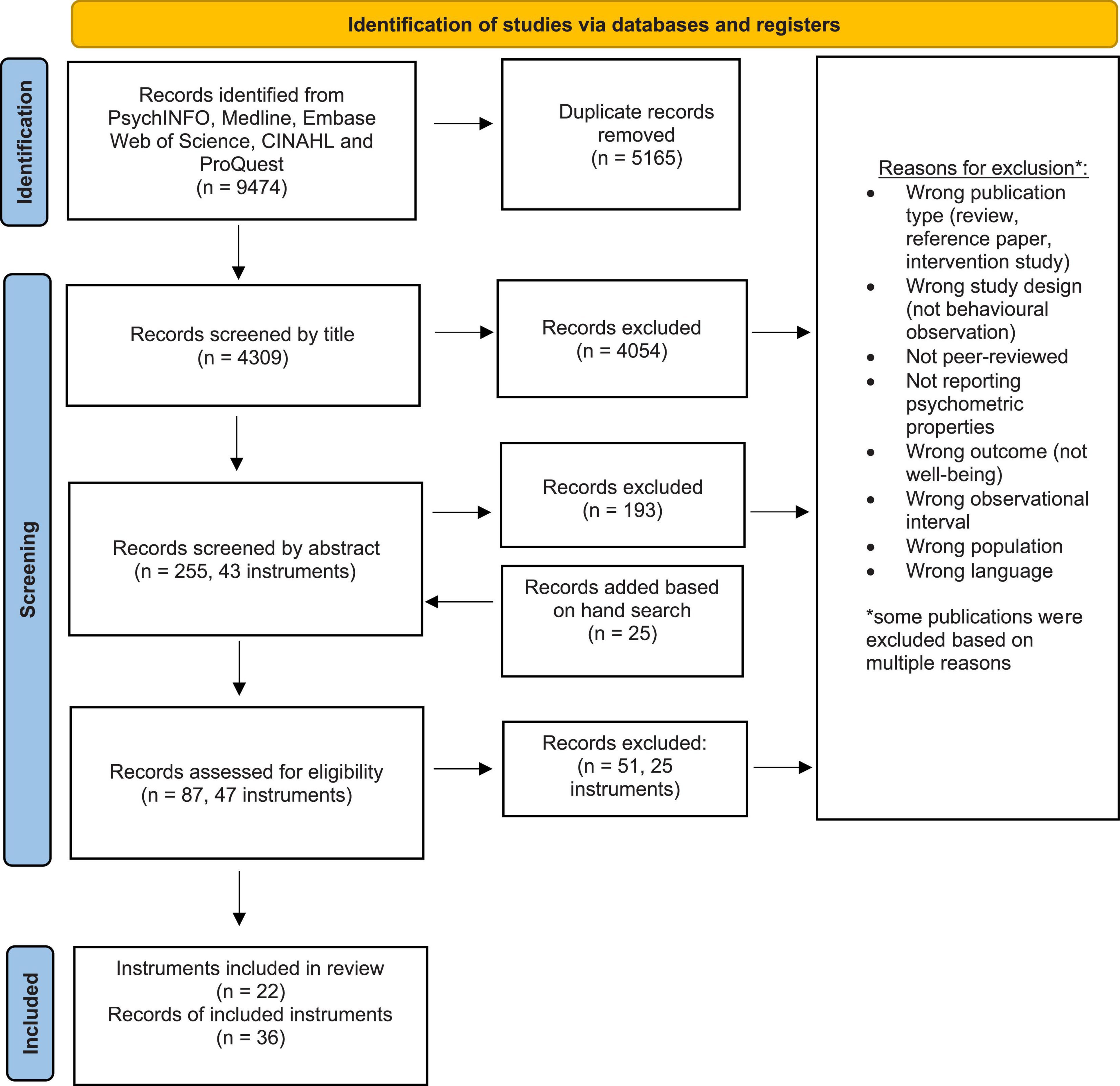
Figure 2. PRISMA Flow chart of search results.
Conceptualizations of the Included Instruments
Key characteristics of the instrument, target population and domains are presented in Table 3. The included instruments are sorted in the three (not mutually exclusive) categories (a) observations of emotions, (b) observations of positive behavioral expressions, and (c) observations of engagement. Instruments are presented in chronological order within each category.
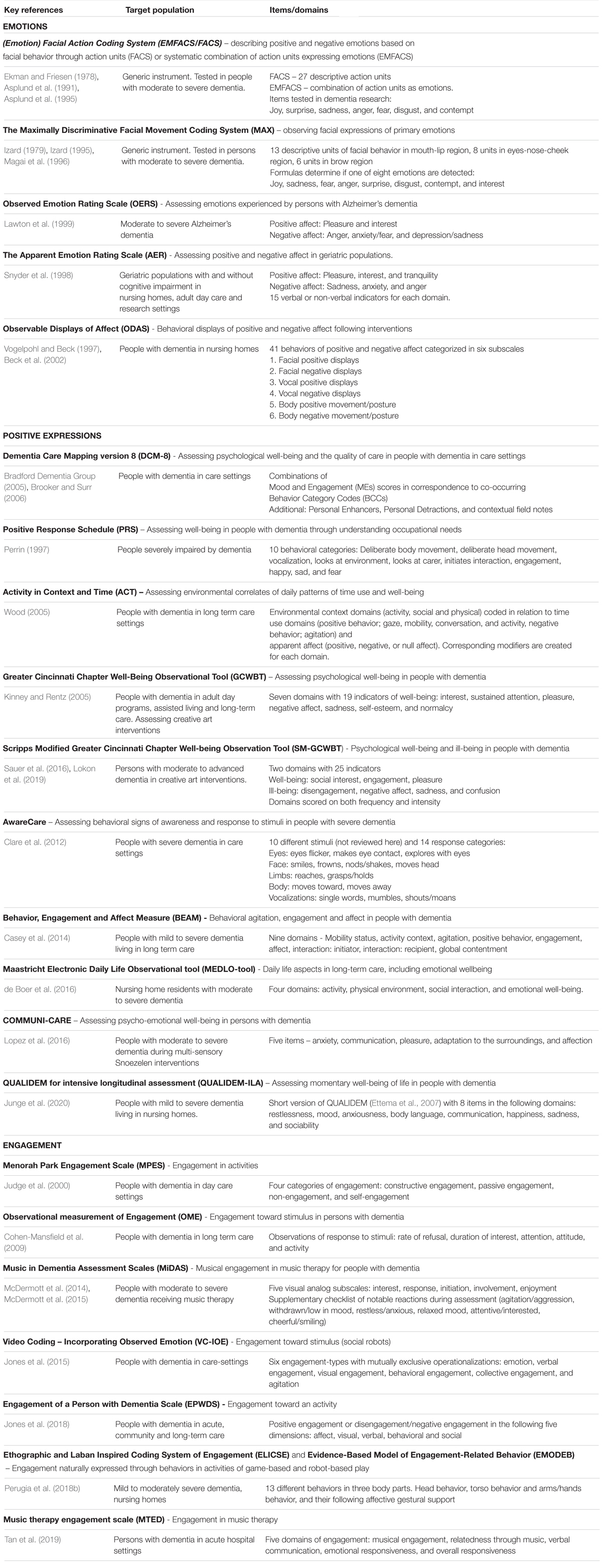
Table 3. Characteristics of the included instruments.
Observations of Emotions
Five instruments were identified assessing emotion through operationalizations of facial, bodily, and behavioral expressions; The Facial Action Coding System (FACS, Ekman and Friesen, 1978; Ekman et al., 2002), The Maximally Discriminative Facial Movement Coding System (MAX, Izard, 1979, 1995), The Observed Emotion Rating Scale1 (OERS, Lawton et al., 1996, 1999), Observable Displays of Affect Scale (ODAS, Vogelpohl and Beck, 1997), and The Apparent Emotion Rating Instrument (AER; Snyder et al., 1998). Two instruments employed generic approaches for emotion detection (FACS and MAX), two were dementia specific (OERS and ODAS), and one was developed to observe emotions in geriatric populations (AER).
Observations of Positive Expressions
Ten dementia-specific instruments that operationalized well-being as positive and negative expressions or responses to stimuli were identified; Dementia Care Mapping (DCM, Kitwood and Bredin, 1992), The Positive Response Schedule (PRS, Perrin, 1997), Activity in Context and Time (ACT; Wood, 2005), Greater Cincinnati Chapter Well-Being Observational Tool (GCC-WOT, Rentz, 2002), a revision of the former, named Scripps Modified Greater Cincinnati Chapter Well-Being Observational Tool (SM-GWW-WOT, Sauer et al., 2016), AwareCare (Clare et al., 2012), The Behavior, Engagement and Affect Measure (BEAM, Casey et al., 2014), Maastricht Electronic Daily Life Observation tool (MEDLO-tool, de Boer et al., 2016), COMMUNI-CARE (Lopez et al., 2016) and QUALIDEM-ILA (Junge et al., 2020).
Observations of Engagement
Seven instruments measuring engagement in dementia met the inclusion criteria; Menorah Park Engagement Scale2 (MPES, Judge et al., 2000), Observational Measurement of Engagement (OME, Cohen-Mansfield et al., 2009), Music in Dementia Assessment Scales (MiDAS, McDermott et al., 2015), Video coding – Incorporating Observed Emotion (VC-IOE, Jones et al., 2015), Engagement of a Person with Dementia Scale (EPWDS, Jones et al., 2018), Ethographic and Laban-Inspired Coding System of Engagement (ELICSE, Perugia et al., 2018b), and Music Therapy Engagement Scale for Dementia (MTED, Tan et al., 2019).
Evaluating Measurement Properties
Extracted data on measurement properties and study characteristics are reported in Supplementary Table 2 together with the study specific RoB-ratings. As most publications use data from repeated observations of the same subjects, both number of participants and number of observations are reported when available. Measurement properties are presented under three headings: (a) content validity, (b) construct validity, including structural validity, measurement invariance and hypothesis testing (for construct validity), and (c) reliability, including internal consistency, inter-rater, intra-rater or test–retest reliability, and measurement error. None of the included publications reported cross-cultural validity and responsiveness, using the methodological definition and criteria of COSMIN (see Tables 1, 2).
The ratings against quality criteria for the available evidence of the measurement properties on instrument level are presented in Table 4. Ten of 22 instruments had only one publication describing the development and measurement properties. More than half of the instruments were developed or tested in small samples [11 of 36 studies have n < 20, mean n = 89.4 (SD = 102)]. The trustworthiness of the summarized result per property evaluated by the GRADE approach (GRADE Handbook, 2013; Prinsen et al., 2018) are presented in Table 4.
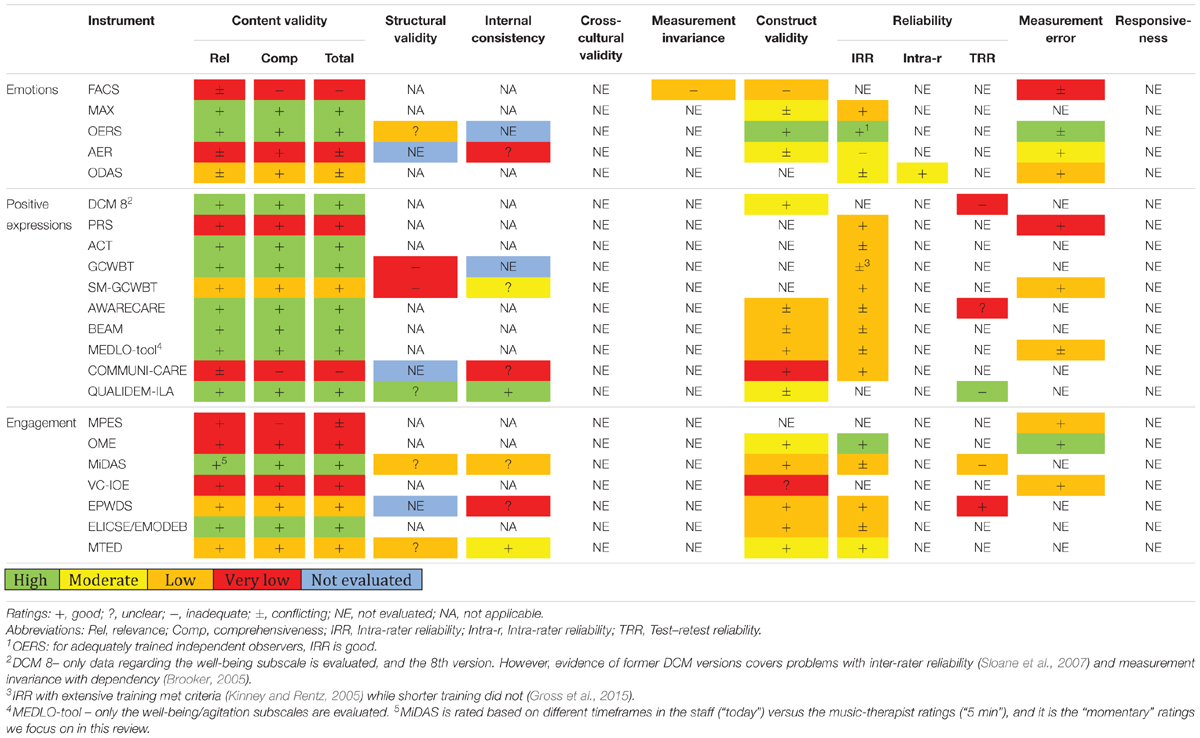
Table 4. Rating against quality criteria and GRADE.
Content Validity
Seventeen of 22 instruments were rated as “good” when evaluated against quality criteria (MAX, OERS, PRS, DCM, ACT, GCWBT, SM-GCWBT, AwareCare, BEAM, MEDLO-tool, QUALIDEM-ILA, OME, MiDAS, VC-IOE, EPWDS, ELICSE/EMODEB, and MTED). Three instruments were rated as “conflicting” (ODAS, AER, and MPES), and two were rated as “inadequate” (FACS and COMMUNI-CARE). The study specific methodological approach for establishing content validity is presented in Supplementary Table 2.
As presented in Table 4,11 of the 17 instruments meeting quality criteria, were supported with high quality ratings of evidence of content validity according to GRADE (MAX, OERS, DCM 8, ACT, GCWBT, AwareCare, BEAM, MEDLO-tool, QUALIDEM-ILA, MiDAS, and ELICSE/EMODEB). Inviting people with dementia and/or family caregivers to include their view on the content of the instruments is an advantage, but was only conducted for AwareCare, QUALIDEM-ILA, MiDAS, and EPWDS.
Structural Validity and Internal Consistency
Statistical methods to investigate structural validity are only developed for unidimensional and reflective instruments or subscales and require independent observations and large samples (de Vet et al., 2011). We identified nine scales as reflective (OERS, AER, GCWBT, SM-GCWBT, COMMUNI-CARE, QUALIDEM ILA, EPWDS, and MTED). Six of the nine scales used factor analysis to investigate structural validity. Except for OERS (Lawton et al., 1996) and QUALIDEM-ILA (Junge et al., 2020), all scales are at risk of bias due to small samples (<100, GCWBT; Gross et al., 2015; SM-GWWBT; Lokon et al., 2019; MiDAS; McDermott et al., 2014; MTED; Tan et al., 2019). Use of repeated (dependent) observations of the same individuals violates statistical assumptions of these methods as well (MiDAS; McDermott et al., 2014). As Table 4 shows, no instruments have higher than “unclear”-rating of structural validity. This is mainly due to a lack of reporting model fit (OERS, QUALIDEM-ILA, MiDAS, and MTED). Investigations of structural validity for GCWBT (Gross et al., 2015) and SM-GCWBT (Lokon et al., 2019) did not confirm the theoretical factor structure.
Internal consistency was sometimes reported when no evidence of unidimensionality was provided (EPWDS; Jones et al., 2018; COMMUNI-CARE; Lopez et al., 2016; AER; Snyder et al., 1998). These results are rated as “unclear,” as internal consistency is a reliability parameter relevant for reflective instruments known to be unidimensional only (Prinsen et al., 2018).
Cross-Cultural Validity
No instruments reported cross-cultural validity. Nevertheless, instruments were developed in several different countries (see Supplementary Table 2), and eight reported the ethnicity of the included participants (BEAM; Casey et al., 2014; AwareCare; Clare et al., 2012; OME; Cohen-Mansfield et al., 2009; GCWBT; Kinney and Rentz, 2005; MAX; Magai et al., 2002; MiDAS; McDermott et al., 2014; MTED; Tan et al., 2019; ACT; Wood et al., 2005).
Measurement Invariance
Little evidence of measurement invariance was reported, when using COSMIN criteria. Only multiple group factor analysis and regression analysis are applicable approaches (Prinsen et al., 2018). An exception was FACS, where apathy explained lower frequency of facial emotions in people with mild to moderate dementia (Seidl et al., 2012).
Measurement invariance has important implications for interpretations of the scores of an instrument. Typical relevant covariates investigated were dementia severity, assessed with Pearson’s or Spearman’s correlations. Due to the methodological approach employed, these are reported under “construct validity” (Cfr. Supplementary Table 2). Lower well-being was correlated with dementia severity in MAX (Magai et al., 1997), AER (Snyder et al., 1998) and AwareCare (Clare et al., 2012). Evidence from earlier DCM-versions have shown well-being scores to vary due to level of cognitive impairment or dependency in the observed persons (Brooker and Surr, 2006; Chaudhury et al., 2013). QUALIDEM-ILA (Junge et al., 2020) and MTED (Tan et al., 2019) did not vary with dementia severity. Apathy correlated negatively with engagement in EPWDS (Jones et al., 2018).
Hypothesis Testing for Construct Validity
Sixteen of 22 instruments investigated construct validity through hypothesis testing. Nine instruments were thus rated as “good” (> 75% of hypotheses supported; OERS, DCM 8, MEDLO-tool, COMMUNI-CARE, OME, MiDAS, EPWDS, ELICSE/EMODEB, and MTED). Five instruments were rated as “conflicting” (MAX, AER, AwareCare, BEAM, and QUALIDEM-ILA), and one as “inadequate” (FACS). Only OERS provided evidence rated as high quality according to GRADE.
A frequently detected risk of bias was lack of specific hypotheses about the strengths of correlations with similar or divergent measures, postulated a priori (Prinsen et al., 2018). According to our quality criteria, significant correlations ≤ 0.3 were discarded. Weak statistically significant correlations with instruments measuring similar constructs are not adequate evidence of construct validity (Mokkink et al., 2017), but were reported as evidence supporting construct validity in AER, BEAM, and QUALIDEM-ILA.
In three of the instruments with “conflicting” evidence (AwareCare, BEAM and QUALIDEM-ILA), proxy-reported long-term QoL ratings by staff and/or family members and momentary observations by independent observers did not correlate and consequently did not support construct validity (Clare et al., 2012; Casey et al., 2014; Junge et al., 2020). Overall, further investigation of construct validity with specific and a priori hypotheses is required for all instruments, except OERS.
Inter-Rater Reliability and Measurement Agreement
As Table 4 demonstrates, some evidence of agreement between coders were reported in all but DCM 8 and QUALIDEM-ILA. Eight of 22 instruments (MAX, OERS, PRS, SM-GCWBT, COMMUNI-CARE, OME, EPWDS, and MTED) met quality criteria of inter-rater reliability (IRR, > 0.70). Of these, only two (OERS and OME) were evaluated with high quality evidence according to GRADE. Some report IRR using invalid methods according to Prinsen et al. (2018) such as Spearman’s Rho (BEAM; Casey et al., 2014) or Pearson’s correlations (GCWOT; Gross et al., 2015). For instruments concerned about item levels, the items’ specific Kappa values are the relevant parameters (Prinsen et al., 2018), but some report Kappa values on instrument level rather than an item-specific Kappa (GCWBT; Kinney and Rentz, 2005; COMMUNI-CARE; Lopez et al., 2016; SM-GCWBT; Sauer et al., 2016; PRS; Schall et al., 2015).
If the total sum of the scale is to be used, IRR should be assessed with intra class correlations (ICC), as the agreement of the total sum is the relevant reliability parameter (Prinsen et al., 2018). For most health measurement instruments, the preferred ICC formula is absolute agreement for random models with single measurements. This reflects whether different observers consistently reach the same conclusions (see de Vet et al., 2011; chapter 5). However, the formulae were often not reported and suboptimal calculations were often used.
For ordinal, nominal and dichotomous level scores, measurement error is defined as measurement agreement between raters. This was reported for 10 instruments, where seven met the quality criteria (> 80%, AER, ODAS, PRS, SM-GCWBT, MPES, OME, and VC-IOE). Of these, only one was evaluated with high quality evidence (OME).
Low inter-rater agreement (IRR and measurement agreement) may reflect both lack of training and problems with content validity/poor operationalizations of the items. The amount of training will affect the level of inter-rater agreement, for instance as shown in OERS (Lawton et al., 1999) and when comparing inter-rater reliability for GCWBT with extensive training (Kinney and Rentz, 2005) and 30 min training (Gross et al., 2015). For MiDAS, the varying timeframes of the staff- and music-therapist ratings (“today” versus 5 min) may account for the low inter-rater reliability of the staff-ratings (McDermott et al., 2014). This may well reflect lower relevance of the items in the prolonged timeframe, and potentially issues concerning content validity.
Test–Retest Reliability and Measurement Error
Test–retest reliability was rarely investigated, and of the five scales reporting on this property, EPWDS was the only scale meeting the quality criteria. To validly evaluate test–retest reliability, the subjects need to be stable in the interim-period to ensure that any difference is caused by random measurement error (de Vet et al., 2011). In general, several studies showed fluctuating well-being scores (AwareCare; Clare et al., 2012; QUALIDEM-ILA; Junge et al., 2020; MiDAS; McDermott et al., 2014). Competing explanations of low test–retest reliability may include too long an interval between comparison measurements or may simply reflect qualities of the construct.
The low test–retest reliability detected for DCM 8 is prone to bias, as the assessments were three months apart (Villar et al., 2015).
For continuous level scores, measurement error is related to the test–retest reliability, and we need to know the smallest detectable change (SDC) or limits of agreement (LoA), as well as the minimal important change (MIC) defined by the target group, to apply the quality criteria (Prinsen et al., 2018). None of the instruments reported these outcomes.
Responsiveness
No instruments reported evidence of responsiveness.
Feasibility and Interpretability
Extracted data regarding feasibility and interpretability are reported in Supplementary Table 3. Additional publications from the search process describing use of the instrument in clinical settings or research were extracted here.
Feasibility
Four instruments require video-recordings (FACS, ODAS, VC-IOE, and ELICSE) and the latter may be used for direct observation. Several instruments allow for observing people simultaneously or sequentially (DCM, ACT, GCWBT, SM-GCWBT, BEAM, MEDLO-tool, MiDAS, and MTED). Some instruments were developed mainly as research tools (FACS, MAX, ODAS, PRS, ACT, VC-IOE, and ELICSE). Two instruments appear best suited for evaluation in care settings only (DCM 8 and MTED). Several instruments appear feasible for evaluating psychosocial interventions (FACS, MAX, ODAS, OERS, AER, PRS, ACT, MPES, BEAM, and QUALIDEM-ILA), and some are suited for care settings as well (OERS, AER, ACT, BEAM, QUALIDEM-ILA, DCM 8, AwareCare and MEDLO-tool). Some instruments are developed for specific interventional approaches, including art-interventions and other creative interventions (GCWBT and SM-GCWBT), multi-sensory interventions (COMMUNI-CARE), interaction with social robots (ELICSE, VC-IOE, and EPWDS), and music interventions (MiDAS and MTED). Most instruments are feasible for persons with mild, moderate, and severe dementia, but two instruments were specifically developed for very severe dementia (PRS and AwareCare). Personalized stimuli can be incorporated in two instruments (AwareCare and OME), and six instruments are easily adapted to other environmental contexts (OERS, GCWBT, SM-GCWBT, BEAM, MEDLO-tool, and ACT).
Interpretability
Skewed distributions of the negative expressions were commonly reported (FACS/EMFACS; Asplund et al., 1995; ODAS; Beck et al., 2002; Beerens et al., 2016; BEAM; Casey et al., 2014; MEDLO-tool; de Boer et al., 2016; MPES; Judge et al., 2000; GCWOT; Kinney and Rentz, 2005; OERS; Lawton et al., 1999; SM-GCWOT; Lokon et al., 2019; MAX; Magai et al., 1996, 2002; PRS; Perrin, 1997; Phillips et al., 2010; ACT; Wood, 2005). For AwareCare, infrequent items were removed during fieldwork to avoid skewness (Clare et al., 2012).
Sensitivity to detect statistically significant changes were demonstrated for FACS/EMFACS (in people with mild to moderate dementia; Seidl et al., 2012; but not for people with severe dementia; Asplund et al., 1995), MAX (Magai et al., 1996), OERS (when aggregating positive and negative affect; Hammar et al., 2011; except anger; Lawton et al., 1999), AER (Snyder et al., 2001), ODAS (for two of three subscales, Beck et al., 2002, or when aggregating scores to positive and negative affect; Lee et al., 2013, 2014, 2017), DCM 8 (Brooker, 2005), PRS (Hadley et al., 1999; Schall et al., 2015), ACT (Wood et al., 2005; Lassell et al., 2021), GCWBT (positive items only, Kinney and Rentz, 2005) and SC-GWBT (Sauer et al., 2016; Lokon et al., 2019), AwareCare (Clare et al., 2012, 2014), BEAM (for “happiness” and “agitation”, Low et al., 2014), MEDLO-tool (“mood”; Beerens et al., 2016, 2018), MPES (Lee et al., 2007), OME (Cohen-Mansfield et al., 2011, 2012), MiDAS (Garrido et al., 2020) and EPWDS (Feng et al., 2020).
To ease interpretation, available sources for means and standard deviations of scores are reported in Supplementary Table 3. However, guidelines for interpretation of clinically significant scores or change scores are not identified in most instruments. DCM 8 offers calculating an individual or group level well-being profile. PRS gives a ratio, where higher ratios imply the setting triggers more well-being. AwareCare offers calculation of a “Responsiveness Index” for stimuli or for the individual, enabling the assessment of both individual processes and comparisons on group-level (Clare et al., 2012). COMMUNI-CARE provides a cut-off score of positive, indifferent, and negative effects of an intervention (Lopez et al., 2016). For ACT and EPWDS, creating an individual baseline is recommended to interpret change-scores.
Discussion
In this review we investigated observational instruments assessing momentary well-being in the context of research, interventions and care for people living with dementia. We identified 22 instruments, and evaluated RoB on study level, and measurement properties, feasibility, and interpretability on instrument level. The content validity of many of the instruments reviewed was sound and supported by high quality evidence for 11 instruments. Meanwhile, the presence of high-quality evidence of other central psychometric aspects was sparse. This may in part be explained historically by the more recent development of stringent quality criteria. Hence, several instruments have the potential to meet these quality criteria if further investigated. To guide and advise further use of these instruments in care and research, we provide a general discussion of the most common methodological problems. Finally, we present instrument-specific recommendations.
Issues Regarding Measurement Properties, Feasibility, and Interpretability
Problems with skewed distributions or low frequencies of negative emotions, behaviors or expressions are reported for the majority of the instruments (Cfr. Supplementary Table 3). This complicates parametric approaches assuming a normal distribution of items. We suggest that assessing psychosocial interventions for people living with dementia should mainly focus on increases in well-being. Negative symptoms in dementia have a diversity of causes, some of which will necessarily be less modifiable by psychosocial interventions (Kales et al., 2015; Kolanowski et al., 2017; Livingston et al., 2017). However, momentary well-being is particularly achievable through modifying environmental factors (Lawton, 1994; Kolanowski et al., 2020). Moving the focus from ill-being (such as agitation or apathy) to well-being, has three advantages. First, it will decrease the labor intensiveness of the observational assessment because less items are assessed. Second, it will bring about data better fitted for statistical approaches because the distribution of ill-being items in the clinical studies using these instruments often were skewed and not normally distributed (see Asplund et al., 1995; Magai et al., 1996, 2002; Perrin, 1997; Lawton et al., 1999; Judge et al., 2000; Beck et al., 2002; Kinney and Rentz, 2005; Wood, 2005; Phillips et al., 2010; Casey et al., 2014; Beerens et al., 2016; de Boer et al., 2016; Lokon et al., 2019). Lastly, it will increase the likelihood of correct conclusions about the positive effects of the psychosocial interventions because this is operationally defined as an increase in positive expressions and not as a decrease in negative expressions. Ill-being should still be monitored during psychosocial interventions, but the absence of ill-being is not synonymous with well-being (Martyr et al., 2018).
While 15 of 22 instruments could detect statistically significant changes, definitions to guide interpretation of these change-scores were not provided. An option for future studies is to calculate MIC and the SDC or LoA (de Vet et al., 2011) for continuous level instruments. MIC is important because it is defined as the smallest clinical meaningful change as evaluated by patients or clinicians (de Vet and Terwee, 2010). SDC indicates whether change scores are reflecting a “true” change in the construct, as opposed to expected random error or natural fluctuation. Test–retest values may be used to calculate SDC for continuous scores (Prinsen et al., 2018; Mokkink et al., 2020). Several instruments were operationalized at a nominal or ordinal level, while using total score as continuous in statistical analyses. However, using the total score implies that the score reflects, predicts, or describes well-being validly. Although several instruments claim the total score to reflect level of well-being or engagement, adequate evidence of this relationship is rarely provided. Specifically, the formative instruments are hampered by unclear clinical interpretation.
Test–retest reliability reflects the instrument’s measurement error in repeated measurement of stable constructs (de Vet et al., 2011). This required “stability” may be unattainable for fluctuating phenomena such as pain. In this review, several instruments provide evidence suggesting momentary well-being in dementia is a fluctuating phenomenon (Clare et al., 2012; McDermott et al., 2014; Junge et al., 2020). Fluctuations in the construct of interest between measurements creates an ambiguous reliability estimate (Jensen, 2003) and discarding instruments with a cut-off score < 0.70 (Prinsen et al., 2018) is not necessarily useful in this context. It is reasonable to assume test–retest scores reflect a natural fluctuation or variability in well-being in people with dementia, as the presence of neuropsychiatric symptoms such as apathy are episodic and fluctuating as well (Kales et al., 2015). Examining the natural variation of the construct by investigating test–retest reliability is nevertheless important, as the range of variation in fluctuating constructs influence the accuracy when interpreting scores of an instrument. Thus, a clinically significant score needs to be larger than the measurement error inflicted by this natural variation (de Vet et al., 2011). If test–retest reliability is not investigated, we cannot know if the measure can detect change in the observed persons beyond measurement error (Mokkink et al., 2020). This is a significant problem, that may lead to erroneous conclusions in both research and care. In addition, adjusting the interval of the repeated measurements to increase the likelihood of stability is essential, as longer time intervals may reflect the degenerative path of dementia and not instrument reliability.
Developing fine grained instruments used for ecological momentary sampling requires repeated assessment of the same subjects (Shiffman et al., 2008). Investigating behavior as it unfolds over time is labor intensive, and naturally includes smaller samples, often with numerous repeated observations. Standard approaches to develop self-rated instruments require large samples to investigate structural validity with factor analysis (N > 100), or scalability through for example Mokken analysis (N > 2000; Prinsen et al., 2018). Investigating large samples in labor intensive instruments is in many cases unrealistic. Additionally, using serially dependent repeated observations in the same subjects to increase the sample size violates basic assumptions required for these methods (Manolov and Moeyaert, 2017).
Most instruments in this review require further investigations of construct validity to ensure that the output is consistent with the underlying theoretical constructs. Comparisons with global rating scales are recommended when investigating the construct-validity of new instruments (de Vet et al., 2011). While developing COMMUNI-CARE, a validated clinician-rated global scale was used for this purpose (Lopez et al., 2016), but the same non-blinded investigator was rating both scales, contributing to a considerable risk of bias. In OME (Cohen-Mansfield et al., 2009), a similar approach is used, only with blinded ratings of a non-validated global engagement-scale. Thus, investigating construct validity through correlations with similar instruments is a challenge in the face of a lack of a “gold standard measure,” as one must rely on existing instruments with their respective limitations (de Vet et al., 2011). Sometimes the hypothesized correlations included comparisons of well-being levels from long-term versus momentary instruments (Clare et al., 2012). Well-being states and traits do not necessary correlate (Curyto et al., 2008; Cohen-Mansfield, 2011). Therefore, investigating correlations with other momentary assessment approaches is recommended.
When assessing momentary well-being in dementia, two domains seem important to control for to interpret changes in well-being scores more accurately. Several of the instruments included in this review have a well-being score that is associated with (1) dementia severity or (2) level of function. However, research suggests that these constructs are not expected to be systematically related (Missotten et al., 2008; Barca et al., 2011; Cohen-Mansfield, 2011; Martyr et al., 2018). This has implications for how we interpret changes in well-being scores over time. If well-being scores of a particular instrument are lowered as a consequence of the dementia progressing, is this reflecting lack of treatment effect, poorer dementia care, or neurodegenerative development? Future studies assessing the measurement properties of these instruments should assess if a relationship between well-being and dementia severity or level of function is present. Such covariance may indicate that the instrument is tapping both cognitive functioning as well as well-being (for example if the score is relying on verbal expression). Understanding these relationships is required to accurately interpret changes in well-being scores during psychosocial interventions.
Personal well-being refers to a subjective evaluation, and observational measures use behavioral expressions to infer about an inner state. Hence, the most crucial property of a measurement instrument is content validity. Content validity will vary with the context, population, and construct to be measured, and affects all other psychometric properties of an instrument (Terwee et al., 2018). Together with agreement between observers, these two aspects are considered the most important for observational instruments (Bakeman and Quera, 2012; Chorney et al., 2015). Moreover, evidence of structural validity or construct validity, ensuring that an increase in the score reflects an increase in the construct, is important when making inferences about inner states. Cross-validating scores with other instruments, particularly self-report instruments, will strengthen this.
As no evidence of cross-cultural validity or responsiveness was detected, special attention to investigating this knowledge-gap and establishing these properties are important in future studies using any of the instruments in this review. In relation to cross-cultural validity, we make the following recommendation: Behavioral expressions of momentary well-being are likely to differ across cultures (Lim, 2016). Thus, securing cross cultural validity by establishing content validity in new cultural contexts is in our evaluation an alternative to statistical evaluation of cross-cultural validity for observational measures. This can be achieved through the recommended qualitative approaches involving clinical expertise from people with dementia, family- and professional caregivers, as well as clinical experts and field testing (Terwee et al., 2018).
In relation to the lack of responsiveness, we make the following recommendation: Several instruments have provided evidence of their capacity to statistically detect changes in intervention studies (Conf. Supplementary Table 3). However, this is not adequate evidence of responsiveness, as we do not know if the lack of detecting change is due to lack of responsiveness or lack of intervention effect. Responsiveness of these instruments needs to be investigated through correlations with change-scores in similar instruments (de Vet et al., 2011).
The clinical utility of an instrument is specific to the context and aims of the user, and is influenced by its feasibility, interpretability, benefits, and shortcomings (Smart, 2006; Terwee et al., 2018). To recommend a specific instrument to assess observed well-being is not our intention. However, we generally recommend identifying instruments with proper conceptualizations, which are feasible for the specific purpose, context, and target population (Terwee et al., 2018). Choosing instruments with acceptable content validity should be followed by investigation or adaptation to solve the additional instrument-specific issues addressed in this review. An overview of the issues of each instrument is provided in Table 4, Supplementary Tables 2, 3. Establishing or evaluating if the instrument has good content validity in the applied context is vital, especially in securing relevance and comprehensiveness (Chorney et al., 2015).
A final note worth commenting regards the large number of instruments identified in the hand search, of which three were included in this review. This suggests that researchers may not be choosing appropriate keywords when publishing articles relating to observational measures for people living with dementia.
Recommendations of Instruments
Of the instruments measuring emotions with acceptable content validity (OERS and MAX), OERS is the most frequently used (Lee et al., 2019) instrument with the most extensively documented psychometric properties (Lawton et al., 1996, 1999). MAX (and FACS) requiring a close view of the face; problems with interpreting facial movement in persons wearing glasses, having facial hair, or facing more than 45 degrees away from the camera (Cohn et al., 2007) reduces the clinical utility of these instruments in people living with dementia. Thus, the feasibility of instruments relying on facial expressions and excluding bodily expressions may decrease the instruments’ sensitivity to detect expressions of well-being in the dementia population (Seidl et al., 2012). However, as negative emotions are infrequent, the feasibility of the full OERS scale in research and clinical setting is limited (Algar et al., 2016). Thus, for investigating well-being in people with dementia, the positive emotions in OERS may be best suited. However, from these findings, emotions in people with mild to moderate dementia seem to be best measured through self-report (instruments are reviewed in Ferring and Boll, 2010; Stoner et al., 2019; and Clarke et al., 2020).
Users looking for instruments investigating positive expressions are recommended to consider any instruments with acceptable content validity (DCM 8, PRS, ACT, GCWBT, SM-GCWBT, AwareCare, BEAM, MEDLO-tool and QUALIDEM ILA). PRS and MEDLO-tool are instruments with high granularity, detecting changes on micro-levels that offer interval-sampling from 30 s to 2 min. While DCM, ACT, GCWBT, SM-GCWBT offers somewhat fine-grained observations (5-10 min), AwareCare offers fine-grained observations as they unfold over time, and BEAM consists of both fine-grained and aggregated scores. QUALIDEM-ILA is best suited for total evaluations of interventions (30-45 min). Users looking for behavioral or movement-anchored operationalizations of positive expressions with high levels of concreteness may look at PRS, ACT and AwareCare. DCM, GCWBT, SM-GCWBT, BEAM, MEDLO-tool and QUALIDEM-ILA offer more contextual cues and social interpretations.
AwareCare appears clinically useful for people with very severe dementia, and BEAM is feasible for moderate dementia. AwareCare detected signs of awareness in all participants and suggests a clinically useful index for interpretation as well (Clare et al., 2012). PRS needs to be investigated in a larger sample but is a promising tool in very severe dementia (Perrin, 1997). BEAM covers behavior, engagement, and affect, through direct observation in various settings without being very labor intensive and while avoiding observer’s fatigue (Casey et al., 2014). Further investigation of its construct validity may, however, be required, in addition to an improved evaluation of inter-rater reliability. The clinical sensitivity of DCM has been questioned (Cooke and Chaudhury, 2013), and the well-being (ME-score) of DCM 8 is probably not sensitive enough to detect clinical change reliably in intervention studies on a group level. DCM 8 seems better suited for clinical practice (Villar et al., 2015) on an individual level (Brooker and Surr, 2006). MEDLO-tool’s mood score is based on DCM as well, and shows the same problems (Beerens et al., 2016; de Boer et al., 2016), lowering the utility of this instrument for assessing well-being. ACT is based on a thorough development (Wood, 2005), and seems like a feasible and clinically useful instrument, but needs further investigation of construct validity. GCWBT should be omitted due to evidence of low structural validity (Gross et al., 2015), but the revised SM-GCWBT needs further modification and investigation of a proposed two-factor structure, as well as exclusion of some unrelated items (Lokon et al., 2019). Further investigation of QUALIDEM-ILA, in terms of both inter-rater reliability and use in clinical/research contexts are required (Junge et al., 2020). Still, QUALIDEM-ILA is one of the most recent instruments included in this review, and further publications are expected.
Of the instruments assessing engagement with acceptable content validity (OME, VC-IOE, EPWDS, ELICSE, MiDAS, and MTED), users searching for instruments with high granularity may look at VC-IOE or ELICSE (both continuous sampling), EPWDS or MiDAS (5-min intervals), or OME (15 min including both duration-based and aggregated scores). MTED provides an aggregated score based on the intervention-session. ELICSE and VC-IOE offers the highest level of concreteness, and EPWDS, OME, MiDAS, and MTED is less concrete and more interpretative. However, higher levels of concreteness will often increase labor intensiveness (Bakeman and Quera, 2011) and offer broader generalizability, at the cost of lower sensitivity to individual variations. In clinical contexts, allowing for interpreting idiographic expressions of well-being may sometimes be an advantage.
Ethographic and Laban Inspired Coding System of Engagement (ELICSE) is based on an exemplary solid development-phase with subsequent theoretical and conceptual development (Perugia et al., 2018a,b, 2020). Nevertheless, the system is highly context specific to the manipulation of objects when sitting down and may not be as easily adaptable to other activities or clinical contexts. Developers of OME describe a need for further work on increasing the clinical utility of the scale (Cohen-Mansfield et al., 2011, 2012), and it is critiqued for lack of interpretability (Jones et al., 2015, 2018; Perugia et al., 2018b). VC-IOE needs further evaluation of reliability and construct validity (Jones et al., 2015). MiDAS strength is the inclusion of the target group in the development (McDermott et al., 2015), but needs further investigation of psychometric properties and is hampered by low intra-rater reliability (McDermott et al., 2014). MTED appear to be a good option when evaluating engagement in clinical music therapy processes, but the scale is not intended for evaluating intervention effect (Tan et al., 2019).
Engagement of a Person with Dementia Scale (EPWDS) stands out as a feasible, easily administered scale that may allow for assessing engagement in contexts other than robot-based play (Jones et al., 2018). Formal evaluation of its structural validity is required, but indications of test–retest reliability are promising given the common problems of low stability between assessments in this population.
Strengths and Limitations
The first strength of this review is that the protocol was pre-registered in PROSPERO. The second strength is that we used the most relevant systematic approach, the COSMIN-guidelines (Prinsen et al., 2018; Terwee et al., 2018; Mokkink et al., 2020). The third strength is that when required, these guidelines were adapted for evaluating observational instruments based on relevant literature (Bakeman and Quera, 2011, 2012; Chorney et al., 2015; Perugia et al., 2018b). The fourth strength is the extensive review of study-specific and instrument-specific evaluation and overarching methodological issues that provides relevant knowledge to both researchers and practitioners.
A first limitation of this review is that by including instruments reporting at least one psychometric property, instruments describing promising content validity only were not evaluated (such as Morse and Chatterjee, 2018). A second limitation is that the COSMIN-criteria of construct validity requires at least 75% of hypotheses to be supported. This may lead to somewhat unbalanced ratings, as publications reporting only one or two supportive correlations may be given a more positive rating than studies examining multiple correlations. However, testing several hypotheses provides more detailed knowledge about construct validity. A third limitation is the use of correlations of > 0.3 as the cutoff for supporting construct validity. This cutoff may seem low, and less conservative than the original suggestion of correlations ≥ 0.5 with instruments measuring similar constructs (Prinsen et al., 2018). However, the majority of the correlated instruments were assessing related and not similar constructs, indicating that correlations > 0.3 are an adequate expectation. Finally, the blinding procedure within our team of raters could have been more extensive, as completely blinded ratings are considered the gold standard (Mokkink et al., 2017).
Conclusion
Several instruments may validly assess well-being through observation in people with dementia. Evaluating their context specific clinical utility and content validity are more important than choosing the instrument with the best ratings or psychometric properties. However, piloting the instruments, investigating the effects of cultural context and study-specific inter-rater agreement and measurement error is advised. Moreover, utilizing an instrument in a clinical study provides the opportunity to investigate hypotheses that may further inform the construct validity. All measurement approaches come with some strengths and some weaknesses, and observational measures are vulnerable to misinterpretation when they are used to infer about inner states. Nevertheless, observations offer unique opportunities to investigate associations between external stimuli and well-being that can provide important knowledge of the usefulness of various interventions for people living with dementia.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
KM conducted the literature searches, initial screening of records and imported these to the data-management-tools, extracted data, assessed RoB, evaluated against quality criteria, and conducted GRADE-ratings, and wrote methods and result-section, with ideas and commentaries from EF-G and IN. IN and KM blind-screened the abstracts for inclusion and adapted the COSMIN guidelines to observational measures. These were consecutively reviewed in consensus-meetings with KM and IN. EF-G were included in discussions if consensus was not met. KM, EF-G, and IN reviewed and consolidated extracted data into the current tables and wrote the introduction and discussion in collaboration. NP edited the document for conceptual clarity and discussed methodological and quantitative considerations regarding the measures. All authors contributed to the article and approved the submitted version.
Funding
This research was funded by the University of Bergen, Norway.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We wish to acknowledge librarian Kjersti Aksnes-Hopland at the University of Bergen Library for her important advice about search strategies, databases and tools for deduplication and management of references. We appreciate the COSMIN-initiative that offers freely available tools with high standards for reviewing and assessing health related measurement instruments.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2021.742510/full#supplementary-material
Footnotes
- ^ Variations of the name of the OERS are Philadelphia Geriatric Center Affect Scales, Apparent Affect Rating Scale, Lawton’s Modified Behavior Stream, Affect Rating Scale, and Observed Affect Scale (Lee et al., 2019).
- ^ MPES is also referred to as Myers Research Institute Engagement Scale (Lee et al., 2007).
References
Algar, K., Woods, R. T., and Windle, G. (2016). Measuring the quality of life and well-being of people with dementia: a review of observational measures. Dementia 15, 832–857. doi: 10.1177/1471301214540163
Asplund, K., Jansson, L., and Norberg, A. (1995). Facial expressions of patients with dementia: a comparison of two methods of interpretation. Int. Psychogeriatr. 7, 527–534. doi: 10.1017/S1041610295002262
Asplund, K., Norberg, A., Adolfsson, R., and Waxman, H. M. (1991). Facial expressions in severely demented patients: a stimulus-response study of four patients with dementia of the Alzheimer type. Int. J. Geriatr. Psychiatry 6, 599–606. doi: 10.1002/gps.930060809
Bakeman, R., and Quera, V. (2011). Sequential Analysis and Observational Methods for the Behavioral Sciences. Cambridge: Cambridge University Press.
Bakeman, R., and Quera, V. (2012). “Behavioral observation,” in APA Handbook of Research Medhods in Psychology, eds H. Cooper, M. Paul, L. L. Debra, A. T. Panter, D. Rindskopf, and K. J. Sher (Washington: American Psychological Association), 207–225. doi: 10.1037/13619-013
Barca, M. L., Engedal, K., Laks, J., and Selbæk, G. (2011). Quality of Life among elderly patients with dementia in institutions. Dement. Geriatr. Cogn. Disord. 31, 435–442. doi: 10.1159/000328969
Beck, C. K., Vogelpohl, T. S., Rasin, J. H., Uriri, J. T., O’sullivan, P., Walls, R., et al. (2002). Effects of behavioral interventions on disruptive behavior and affect in demented nursing home residents. Nurs. Res. 51, 219–228. doi: 10.1097/00006199-200207000-00002
Beerens, H. C., De Boer, B., Zwakhalen, S. M. G., Tan, F. E. S., Ruwaard, D., Hamers, J. P. H., et al. (2016). The association between aspects of daily life and quality of life of people with dementia living in long-term care facilities: a momentary assessment study. Int. Psychogeriatr. 28, 1323–1331. doi: 10.1017/S1041610216000466
Beerens, H. C., Zwakhalen, S. M. G., Verbeek, H., E.S. Tan, F., Jolani, S., Downs, M., et al. (2018). The relation between mood, activity, and interaction in long-term dementia care. Aging Ment. Health 22, 26–32. doi: 10.1080/13607863.2016.1227766
Bowling, A., Rowe, G., Adams, S., Sands, P., Samsi, K., Crane, M., et al. (2015). Quality of life in dementia: a systematically conducted narrative review of dementia-specific measurement scales. Aging Ment. Health 19, 13–31. doi: 10.1080/13607863.2014.915923
Bradford Dementia Group. (2005). DCM 8 User’s Manual: The DCM Method. Bradford: University of Bradford.
Brooker, D. (2005). Dementia care mapping: a review of the research literature. Gerontologist 45, 11–18. doi: 10.1093/geront/45.suppl_1.11
Brooker, D., and Surr, C. (2006). Dementia Care Mapping (DCM): initial validation of DCM 8 in UK field trials. Int. J. Geriatr. Psychiatry 21, 1018–1025. doi: 10.1002/gps.1600
Casey, A.-N., Low, L.-F., Goodenough, B., Fletcher, J., and Brodaty, H. (2014). Computer-assisted direct observation of behavioral agitation, engagement, and affect in long-term care residents. J. Am. Med. Dir. Assoc. 15, 514–520. doi: 10.1016/j.jamda.2014.03.006
Chaudhury, H., Cooke, H., and Frazee, K. (2013). “Developing a physical environmental evaluation component of the Dementia Care Mapping (DCM) tool,” in Environmental Gerontology: Making Meaningful Places in Old Age, eds G. D. Rowles and M. Bernard (New York: Springer Publishing Company), 153–172.
Chorney, J. M., Mcmurtry, C. M., Chambers, C. T., and Bakeman, R. (2015). Developing and modifying behavioral coding schemes in pediatric psychology: a Practical Guide. J. Pediatr. Psychol. 40, 154–164. doi: 10.1093/jpepsy/jsu099
Clare, L., Quinn, C., Hoare, Z., Whitaker, R., and Woods, R. T. (2014). Care staff and family member perspectives on quality of life in people with very severe dementia in long-term care: a cross-sectional study. Health Qual. Life Outcomes 12, 175–175. doi: 10.1186/s12955-014-0175-3
Clare, L., Whitaker, R., Quinn, C., Jelley, H., Hoare, Z., Woods, B., et al. (2012). AwareCare: development and validation of an observational measure of awareness in people with severe dementia. Neuropsychol. Rehabil. 22, 113–133. doi: 10.1080/09602011.2011.640467
Clarke, C., Woods, B., Moniz-Cook, E., Mountain, G., Øksnebjerg, L., Chattat, R., et al. (2020). Measuring the well-being of people with dementia: a conceptual scoping review. Health Qual. Life Outcomes 18:249. doi: 10.1186/s12955-020-01440-x
Cohen-Mansfield, J. (2011). “The shifting baseline theory of well-being: Lessons from across the aging spectrum,” in Understanding Well-Being In The Oldest Old, eds L. W. Poon and J. Cohen-Mansfield (New York: Cambridge University Press), 46–64.
Cohen-Mansfield, J., Dakheel-Ali, M., Jensen, B., Marx, M. S., and Thein, K. (2012). An analysis of the relationships among engagement, agitated behavior, and affect in nursing home residents with dementia. Int. Psychogeriatr. 24, 742–752. doi: 10.1017/S1041610211002535
Cohen-Mansfield, J., Dakheel-Ali, M., and Marx, M. S. (2009). Engagement in persons with dementia: the concept and its measurement. Am. J. Geriatr. Psychiatry 17, 299–307. doi: 10.1097/JGP.0b013e31818f3a52
Cohen-Mansfield, J., Marx, M., Freedman, L., Murad, H., Regier, N., Thein, K., et al. (2011). The Comprehensive Process Model of Engagement. Am. J. Geriatr. Psychiatry 19, 859–870. doi: 10.1097/JGP.0b013e318202bf5b
Cohn, J. F., Ambadar, Z., and Ekman, P. (2007). “Observer-Based Measurement of Facial Expression With The Facial Action Coding System,” in Handbook of Emotion Elicitation and Assessment, eds J. A. Coan and J. J. B. Allen (New York: Oxford University Press), 203–221.
Cooke, H. A., and Chaudhury, H. (2013). An examination of the psychometric properties and efficacy of Dementia Care Mapping. Dementia 12, 790–805. doi: 10.1177/1471301212446111
Curyto, K., Haitsma, K., and Vriesman, D. (2008). Direct ob servation of behavior: a review of current measures for use with older adults with dementia. Res. Gerontol. Nurs. 1, 52–76. doi: 10.3928/19404921-20080101-02
de Boer, B., Beerens, H. C., Zwakhalen, S. M. G., Tan, F. E. S., Hamers, J. P. H., and Verbeek, H. (2016). Daily lives of residents with dementia in nursing homes: development of the Maastricht electronic daily life observation tool. Int. Psychogeriatr. 28, 1333–1343. doi: 10.1017/S1041610216000478
de Vet, H. C. W., and Terwee, C. B. (2010). The minimal detectable change should not replace the minimal important difference. J. Clin. Epidemiol. 63, 804–805. doi: 10.1016/j.jclinepi.2009.12.015
de Vet, H. C. W., Terwee, C. B., Mokkink, L. B., and Knol, D. L. (2011). Measurement in Medicine: A Practical Guide. Cambridge: Cambridge University Press.
Dröes, R. M., Chattat, R., Diaz, A., Gove, D., Graff, M., Murphy, K., et al. (2016). Social health and dementia: a European consensus on the operationalization of the concept and directions for research and practice. Aging Ment. Health 21, 4–17. doi: 10.1080/13607863.2016.1254596
Ekman, P., and Friesen, W. V. (1978). Facial Action Coding System (FACS): Manual. Palo Alto: Consulting Psychologist Press.
Ekman, P., Friesen, W. V., and Hager, J. C. (2002). Facial Action Coding System: The Manual on CD ROM. Salt Lake City: A Human Face.
Ettema, T. P., Dröes, R.-M., De Lange, J., Mellenbergh, G. J., and Ribbe, M. W. (2007). QUALIDEM: development and evaluation of a dementia specific quality of life instrument—-validation. Int. J. Geriatr. Psychiatry 22, 424–430. doi: 10.1002/gps.1692
Feng, Y., Barakova, E. I., Yu, S., Hu, J., and Rauterberg, G. W. M. (2020). Effects of the level of interactivity of a social robot and the response of the augmented reality display in contextual interactions of people with dementia. Sensors 20:3771. doi: 10.3390/s20133771
Ferring, D., and Boll, T. (eds) (2010). Subjective Well-Being in Older Adults: Current State and Gasp of Research. London: Palgrave Macmillan.
Garrido, S., Dunne, L., Stevens, C. J., and Chang, E. (2020). Music playlists for people with dementia: trialing a guide for caregivers. J. Alzheimers Dis. 77, 219–226. doi: 10.3233/JAD-200457
GRADE Handbook (2013). Handbook for Grading the Quality of Eidence and the Strength of Reccomendations Using the GRADE Approach. Available online at: http://gdt.guidelinedevelopment.org/app/handbook/handbook.html (Accessed April 21, 2020)
Gross, S. M., Danilova, D., Vandehey, M. A., and Diekhoff, G. M. (2015). Creativity and dementia: does artistic activity affect well-being beyond the art class? Dementia 14, 27–46. doi: 10.1177/1471301213488899
Hadley, C., Brown, S., and Smith, A. (1999). Evaluating interventions for people with severe dementia: using the Positive Response Schedule. Aging Ment. Health 3, 234–240. doi: 10.1080/13607869956190
Hammar, L. M., Gotell, E., and Engstrom, G. (2011). Singing while caring for persons with dementia. Arts Health 3, 39–50. doi: 10.1080/17533015.2010.481289
Izard, C. E. (1979). The Maximally Discriminative Facial Movement Coding System (MAX). Newark: University of Delaware.
Izard, C. E. (1995). The Maximally Discriminative Facial Movement Coding System (MAX) (Rev. ed). Newark: University of Delaware.
Jensen, M. P. (2003). Questionnaire validation: a brief guide for readers of the research literature. Clin. J. Pain 19, 345–352. doi: 10.1097/00002508-200311000-00002
Jones, C., Sung, B., and Moyle, W. (2015). Assessing engagement in people with dementia: a new approach to assessment using video analysis. Arch. Psychiatr. Nurs. 29, 377–382. doi: 10.1016/j.apnu.2015.06.019
Jones, C., Sung, B., and Moyle, W. (2018). Engagement of a Person with Dementia Scale: establishing content validity and psychometric properties. J. Adv. Nurs. 74, 2227–2240. doi: 10.1111/jan.13717
Judge, K. S., Camp, C. J., and Orsulic-Jeras, S. (2000). Use of Montessori-based activities for clients with dementia in adult day care: effects on engagement. Am. J. Alzheimers Dis. Other Demen. 15, 42–46. doi: 10.1177/153331750001500105
Junge, S., Gellert, P., O’sullivan, J. L., Moller, S., Voigt-Antons, J.-N., Kuhlmey, A., et al. (2020). Quality of life in people with dementia living in nursing homes: validation of an eight-item version of the qualidem for intensive longitudinal assessment. Qual. Life Res. 29, 1721–1730. doi: 10.1007/s11136-020-02418-4
Kales, H. C., Gitlin, L. N., and Lyketsos, C. G. (2015). Assessment and management of behavioral and psychological symptoms of dementia. BMJ 350:h369. doi: 10.1136/bmj.h369
Kaufmann, E. G., and Engel, S. A. (2016). Dementia and well-being: a conceptual framework based on Tom Kitwood’s model of needs. Dementia 15, 774–788. doi: 10.1177/1471301214539690
Kinney, J. M., and Rentz, C. A. (2005). Observed well-being among individuals with dementia: memories in the Making, an art program, versus other structured activity. Am. J. Alzheimers Dis. Other Demen. 20, 220–227. doi: 10.1177/153331750502000406
Kitwood, T. (1997). Dementia Reconsidered: The Person Comes First. Buckingham: Open University Press.
Kitwood, T., and Bredin, K. (1992). A new approach to the evaluation of dementia care. J. Adv. Health Nurs. Care 1, 41–60.
Kolanowski, A., Behrens, L., Lehman, E., Oravecz, Z., Resnick, B., Boltz, M., et al. (2020). Living well with dementia: factors associated with nursing home residents’ affect balance. Res. Gerontol. Nurs. 13, 21–30. doi: 10.3928/19404921-20190823-01
Kolanowski, A., Boltz, M., Galik, E., Gitlin, L. N., Kales, H. C., Resnick, B., et al. (2017). Determinants of behavioral and psychological symptoms of dementia: a scoping review of the evidence. Nurs. Outlook 65, 515–529. doi: 10.1016/j.outlook.2017.06.006
Kolanowski, A., Hoffman, L., and Hofer, S. M. (2007). Concordance of self-report and informant assessment of emotional well-being in nursing home residents with dementia. J. Gerontol. B Psychol. Sci. Soc. Sci. 62, 20–27. doi: 10.1093/geronb/62.1.P20
Kolanowski, A., Van Haitsma, K., Meeks, S., and Litaker, M. (2014). Affect balance and relationship with well-being in nursing home residents with dementia. Am. J. Alzheimers Dis. Other Demen. 29, 457–462. doi: 10.1177/1533317513518657
Lassell, R., Wood, W., Schmid, A. A., and Cross, J. E. (2021). A comparison of quality of life indicators during two complementary interventions: adaptive gardening and adaptive riding for people with dementia. Complement. Ther. Med. 57:102658. doi: 10.1016/j.ctim.2020.102658
Lawton, M. P. (1994). Quality of life in Alzheimer’s disease. Alzheimer Dis. Assoc. Disord. 8, 138–150. doi: 10.1097/00002093-199404000-00015
Lawton, M. P., Van Haitsma, K., and Klapper, J. (1996). Observed affect in nursing home residents with Alzheimer’s disease. J. Gerontol. B Psychol. Sci. Soc. Sci. 51:3. doi: 10.1093/geronb/51b.1.p3
Lawton, M. P., Van Haitsma, K., Perkinson, M., and Ruckdeschel, K. (1999). Observed affect and quality of life in dementia: further affirmations and problems. Aging Ment. Health 5, 69–81.
Lee, K. H., Algase, D. L., and Mcconnell, E. S. (2013). Daytime observed emotional expressions of people with dementia. Nurs. Res. 62, 218–225. doi: 10.1097/NNR.0b013e31829999d7
Lee, K. H., Algase, D. L., and Mcconnell, E. S. (2014). Relationship between observable emotional expression and wandering behavior of people with dementia. Int. J. Geriatr. Psychiatry 29, 85–92. doi: 10.1002/gps.3977
Lee, K. H., Boltz, M., Lee, H., and Algase, D. L. (2017). Is an engaging or soothing environment associated with the psychological well-being of people with dementia in long-term care? J. Nurs. Scholarsh. 49, 135–142. doi: 10.1111/jnu.12263
Lee, K. H., Lee, J. Y., Boltz, M., and Mcconnell, E. S. (2019). Emotional expression of persons with dementia: an integrative review with implications for evidence-based practice. Worldviews Evid. Based Nurs. 16, 344–351. doi: 10.1111/wvn.12395
Lee, M. M., Camp, C. J., and Malone, M. L. (2007). Effects of intergenerational Montessori-based activities programming on engagement of nursing home residents with dementia. Clin. Interv. Aging 2, 477–483.
Lim, N. (2016). Cultural differences in emotion: differences in emotional arousal level between the East and the West. Integr. Med. Res. 5, 105–109. doi: 10.1016/j.imr.2016.03.004
Livingston, G., Sommerlad, A., Orgeta, V., Costafreda, S. G., Huntley, J., Ames, D., et al. (2017). Dementia prevention, intervention, and care. Lancet 390, 2673–2734. doi: 10.1016/S0140-6736(17)31363-6
Lokon, E., Sauer, P. E., and Li, Y. (2019). Activities in dementia care: a comparative assessment of activity types. Dementia 18, 471–489. doi: 10.1177/1471301216680890
Lopez, J. J. B., Bolivar, J. C. C., and Perez, M. S. (2016). COMMUNI-CARE: assessment tool for reactions and behaviours of patients with dementia in a multisensory stimulation environment. Dementia 15, 526–538. doi: 10.1177/1471301214528346
Low, L.-F. P., Goodenough, B. P., Fletcher, J. P., Xu, K. P., Casey, A.-N. B., Chenoweth, L. R. N. P., et al. (2014). The effects of humor therapy on nursing home residents measured using observational methods: the SMILE cluster randomized trial. J. Am. Med. Dir. Assoc. 15, 564–569. doi: 10.1016/j.jamda.2014.03.017
Madsø, K. G., and Nordhus, I. H. (2021). Implementation of quality of life assessment in long-term care. Int. Psychogeriatr. 33, 861–863. doi: 10.1017/S1041610221000983
Magai, C., Cohen, C., Gomberg, D., Malatesta, C., and Culver, C. (1996). Emotional expression during mid- to late-stage dementia. Int. Psychogeriatr. 8, 383–395. doi: 10.1017/S104161029600275X
Magai, C., Cohen, C. I., Culver, C., Gomberg, D., and Malatesta, C. (1997). Relation between premorbid personality and patterns of emotion expression in mid- to late-stage dementia. Int. J. Geriatr. Psychiatry 12, 1092–1099. doi: 10.1002/(SICI)1099-1166(199711)12:11<1092::AID-GPS690<3.0.CO2-X
Magai, C., Cohen, C. I., and Gomberg, D. (2002). Impact of training dementia caregivers in sensitivity to nonverbal emotion signals. Int. Psychogeriatr. 14, 25–38. doi: 10.1017/S1041610202008256
Manolov, R., and Moeyaert, M. (2017). How can single-case data be analyzed? Software resources, tutorial, and reflections on analysis. Behav. Modif. 41, 179–228. doi: 10.1177/0145445516664307
Martyr, A., Nelis, S. M., Quinn, C., Wu, Y.-T., Lamont, R. A., Henderson, C., et al. (2018). Living well with dementia: a systematic review and correlational meta-analysis of factors associated with quality of life, well-being and life satisfaction in people with dementia. Psychol. Med. 48, 2130–2139. doi: 10.1017/S0033291718000405
McDermott, O., Orgeta, V., Ridder, H. M., and Orrell, M. (2014). A preliminary psychometric evaluation of Music in Dementia Assessment Scales (MiDAS). Int. Psychogeriatr. 26, 1011–1019. doi: 10.1017/S1041610214000180
McDermott, O., Orrell, M., and Ridder, H. M. (2015). The development of Music in Dementia Assessment Scales (MiDAS). Nord. J. Music Ther. 24, 232–251. doi: 10.1080/08098131.2014.907333
Missotten, P., Squelard, G., Ylieff, M., Di Notte, D., Paquay, L., De Lepeleire, J., et al. (2008). Relationship between quality of life and cognitive decline in dementia. Dement. Geriatr. Cogn. Disord. 25, 564–572. doi: 10.1159/000137689
Mokkink, L. B., Boers, M., Van Der Vleuten, C. P. M., Bouter, L. M., Alonso, J., Patrick, D. L., et al. (2020). COSMIN Risk of Bias tool to assess the quality of studies on reliability or measurement error of outcome measurement instruments: a Delphi study. BMC Med. Res. Methodol. 20:293. doi: 10.1186/s12874-020-01179-5
Mokkink, L. B., De Vet, H. C. W., Prinsen, C. A. C., Patrick, D. L., Alonso, J., Bouter, L. M., et al. (2017). COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. Qual. Life Res. 27, 1171–1179. doi: 10.1007/s11136-017-1765-4
Morse, N., and Chatterjee, H. (2018). Museums, health and wellbeing research: co-developing a new observational method for people with dementia in hospital contexts. Perspect. Public Health 138, 152–159. doi: 10.1177/1757913917737588
National Institute for Health and Care Excellence [NICE] (2018). Dementia: Assessment, management and support for people living with dementia and their carers. London: National Institute for Health and Care Excellence.
Øksnebjerg, L., Diaz-Ponce, A., Gove, D., Moniz-Cook, E., Mountain, G., Chattat, R., et al. (2018). Towards capturing meaningful outcomes for people with dementia in psychosocial intervention research: a pan-European consultation. Health Expect. 21, 1056–1065. doi: 10.1111/hex.12799
Perrin, T. (1997). The Positive Responses Schedule for severe dementia. Aging Ment. Health 1, 184–191. doi: 10.1080/13607869757290
Perugia, G., Diaz-Boladeras, M., Catala-Mallofre, A., Barakova, E. I., and Rauterberg, M. (2020). “ENGAGE-DEM: A Model of engagement of people with dementia,” in IEEE Transactions on Affective Computing, (Piscataway: IEEE). doi: 10.1109/TAFFC.2020.2980275
Perugia, G., Van Berkel, R., Díaz-Boladeras, M., Català-Mallofré, A., Rauterberg, M., and Barakova, E. (2018b). Understanding engagement in dementia through behavior. The ethographic and Laban-inspired coding system of engagement (ELICSE) and the Evidence-based Model of Engagement-related Behavior (EMODEB). Front. Psychol. 9:690. doi: 10.3389/fpsyg.2018.00690
Perugia, G., Roíguez-Martín, D., Díaz-Boladeras, M., Català-Mallofré, A., Barakova, E. I., and Rauterberg, G. W. M. (2018a). Quantity of movement as a measure of engagement for dementia : the influence of motivational disorders. Am. J. Alzheimers Dis. Other Demen. 33, 112–121. doi: 10.1177/1533317517739700
Phillips, L. J., Reid-Arndt, S. A., and Pak, Y. (2010). Effects of a Creative Expression Intervention on Emotions, Communication, and Quality of Life in Persons With Dementia. Nurs. Res. 59, 417–425. doi: 10.1097/NNR.0b013e3181faff52
Prinsen, C. A. C., Mokkink, L. B., Bouter, L. M., Alonso, J., Patrick, D. L., De Vet, H. C. W., et al. (2018). COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual. Life Res. 27, 1147–1157. doi: 10.1007/s11136-018-1798-3
Reilly, S. T., Harding, A. J. E., Morbey, H., Ahmed, F., Williamson, P. R., Swarbrick, C., et al. (2020). What is important to people with dementia living at home? A set of core outcome items for use in the evaluation of non-pharmacological community-based health and social care interventions. Age Ageing 49, 664–671. doi: 10.1093/ageing/afaa015
Rentz, C. A. (2002). Memories in the Making© : outcome-based evaluation of an art program for individuals with dementing illnesses. Am. J. Alzheimers Dis. Other Demen. 17, 175–181. doi: 10.1177/153331750201700310
Sands, L. P., Ferreira, P., Stewart, A. L., Brod, M., and Yaffe, K. (2004). What explains differences between dementia patients’ and their caregivers’ ratings of patients’ quality of life? Am. J. Geriatr. Psychiatry 12, 272–280. doi: 10.1097/00019442-200405000-00006
Sauer, P. E., Fopma-Loy, J., Kinney, J. M., and Lokon, E. (2016). “It makes me feel like myself”: person-centered versus traditional visual arts activities for people with dementia. Dementia 15, 895–912. doi: 10.1177/1471301214543958
Schall, A., Haberstroh, J., and Pantel, J. (2015). Time series analysis of individual music therapy in dementia: effects on communication behavior and emotional well-being. GeroPsych 28, 113–122. doi: 10.1024/1662-9647/a000123
Schulz, R., Cook, T. B., Beach, S. R., Lingler, J. H., Martire, L. M., Monin, J. K., et al. (2013). Magnitude and causes of bias among family caregivers rating Alzheimer disease patients. Am. J. Geriatr. Psychiatry 21, 14–25. doi: 10.1016/j.jagp.2012.10.002
Seidl, U., Lueken, U., Thomann, P. A., Kruse, A., and Schröder, J. (2012). Facial Expression in Alzheimer’s Disease: impact of Cognitive Deficits and Neuropsychiatric Symptoms. Am. J. Alzheimers Dis. Other Demen. 27, 100–106. doi: 10.1177/1533317512440495
Shiffman, S., Stone, A. A., and Hufford, M. R. (2008). Ecological Momentary Assessment. Annu. Rev. Clin. Psychol. 4, 1–32. doi: 10.1146/annurev.clinpsy.3.022806.091415
Skevington, S. M., and Böhnke, J. R. (2018). How is subjective well-being related to quality of life? Do we need two concepts and both measures? Soc. Sci. Med. 206, 22–30. doi: 10.1016/j.socscimed.2018.04.005
Sloane, P. D., Brooker, D., Cohen, L., Douglass, C., Edelman, P., Fulton, B. R., et al. (2007). Dementia care mapping as a research tool. Int. J. Geriatr. Psychiatry 22, 580–589. doi: 10.1002/gps.1721
Smart, A. (2006). A multi-dimensional model of clinical utility. Int. J. Qual. Health Care 18, 377–382. doi: 10.1093/intqhc/mzl034
Snyder, M., Ryden, M. B., Shaver, P., Wang, J.-J., Savik, K., Gross, C. R., et al. (1998). The Apparent Emotion Rating Instrument: assessing affect in cognitively impaired elders. Clin. Gerontol. 18, 17–29. doi: 10.1300/J018v18n04_03
Snyder, M., Tseng, Y.-H., Brandt, C., Croghan, C., Hanson, S., Constantine, R., et al. (2001). A glider swing intervention for people with dementia. Geriatr. Nurs. 22, 86–90. doi: 10.1067/mgn.2001.115197
Stoner, C. R., Stansfeld, J., Orrell, M., and Spector, A. (2019). The development of positive psychology outcome measures and their uses in dementia research: a systematic review. Dementia 18, 2085–2106. doi: 10.1177/1471301217740288
Tan, J., Wee, S.-L., Yeo, P. S., Choo, J., Ritholz, M., and Yap, P. (2019). A new music therapy engagement scale for persons with dementia. Int. Psychogeriatr. 31, 49–58. doi: 10.1017/S1041610218000509
Terwee, C. B., Jansma, E. P., Riphagen, I. I., and De Vet, H. C. W. (2009). Development of a methodological PubMed search filter for finding studies on measurement properties of measurement instruments. Qual. Life Res. 18:1115. doi: 10.1007/s11136-009-9528-5
Terwee, C. B., Prinsen, C., Chiarotto, A., Westerman, M., Patrick, D., Alonso, J., et al. (2018). COSMIN methodology for evaluating the content validity of patient-reported outcome measures: a Delphi study. Qual. Life Res. 27, 1159–1170. doi: 10.1007/s11136-018-1829-0
Trigg, R., Watts, S., Jones, R., and Tod, A. (2011). Predictors of quality of life ratings from persons with dementia: the role of insight. Int. J. Geriatr. Psychiatry 26:83. doi: 10.1002/gps.2494
Villar, F., Vila-Miravent, J., Celdran, M., Fernandez, E., and D’arcy, L. (2015). Assessing the well-being of patients with dementia: validity and reliability of the Spanish version of the Dementia Care Mapping (DCM) tool. Estud. Psicol. 36, 389–412. doi: 10.1080/02109395.2015.1026124
Vogelpohl, T. S., and Beck, C. K. (1997). Affective responses to behavioral interventions. Semin. Clin. Neuropsychiatry 2, 102–112. doi: 10.1053/SCNP00200102
Wood, W. (2005). Toward developing new occupational science measures: an example from dementia care research. J. Occup. Sci. 12, 121–129. doi: 10.1080/14427591.2005.9686555
Wood, W., Harris, S., Snider, M., and Patchel, S. A. (2005). Activity situations on an Alzheimer’s disease special care unit and resident environmental interactions, time use, and affect. Am. J. Alzheimers Dis. Other Demen. 20, 105–118. doi: 10.1177/153331750502000210
Keywords: well-being, dementia, observation, emotion, systematic review, psychometric properties, engagement
Citation: Madsø KG, Flo-Groeneboom E, Pachana NA and Nordhus IH (2021) Assessing Momentary Well-Being in People Living With Dementia: A Systematic Review of Observational Instruments. Front. Psychol. 12:742510. doi: 10.3389/fpsyg.2021.742510
Received: 16 July 2021; Accepted: 26 October 2021;
Published: 23 November 2021.
Edited by:
Peter ten Klooster, University of Twente, NetherlandsReviewed by:
Jannis Kraiss, University of Twente, NetherlandsKatherine Algar-Skaife, Norwegian University of Science and Technology, Norway
Copyright © 2021 Madsø, Flo-Groeneboom, Pachana and Nordhus. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kristine G. Madsø, a3Jpc3RpbmUubWFkc29AdWliLm5v