 Liliana Lorettu1
Liliana Lorettu1 Giuseppe Mastrangelo2†
Giuseppe Mastrangelo2† Joanna Stepien3
Joanna Stepien3 Jakub Grabowski4
Jakub Grabowski4 Roberta Meloni1Davide Piu1Tomasz Michalski5
Roberta Meloni1Davide Piu1Tomasz Michalski5 Przemyslaw M. Waszak6
Przemyslaw M. Waszak6 Saverio Bellizzi7
Saverio Bellizzi7 Luca Cegolon8,9*†
Luca Cegolon8,9*†
- 1Department of Medical, Surgical and Experimental Sciences, University of Sassari, Sassari, Italy
- 2Department of Cardiac, Thoracic, Vascular Sciences and Public Health, University of Padua, Padua, Italy
- 3Department of Socio-Economic Geography, Faculty of Social Sciences, University of Gdańsk, Gdańsk, Poland
- 4Department of Developmental Psychiatry, Psychotic and Geriatric Disorders, Medical University of Gdańsk, Gdańsk, Poland
- 5Department of Regional Development, Faculty of Social Sciences, University of Gdańsk, Gdańsk, Poland
- 6Department of Hygiene and Epidemiology, Medical University of Gdańsk, Gdańsk, Poland
- 7Independent Consultant, Geneva, Switzerland
- 8Department of Medical, Surgical & Health Sciences, University of Trieste, Trieste, Italy
- 9University Health Authority Giuliano-Isontina (ASUGI), Public Health Department, Trieste, Italy
Background: During the first wave of the COVID-19 pandemic (April to May 2020), 6,169 Polish and 939 Italian residents were surveyed with an online questionnaire investigating socio-demographic information and personality traits (first section) as well as attitudes, position, and efficacy perceptions on the impact of lockdown (second section) and various health protection measures enforced (third section).
Methods: The “health protection attitude score” (HPAS), an endpoint obtained by pooling up the answers to questions of the third section of the survey tool, was investigated by multiple linear regression models, reporting regression coefficients (RC) with 95% confidence intervals (95% CI).
Results: Concerns for business and health due to COVID-19 were associated with a positive attitude toward risk reduction rules. By contrast, male sex, concerns about the reliability of information available online on COVID-19 and its prevention, along with the feeling of not being enough informed on the transmissibility/prevention of SARS-CoV-2 were associated with a negative attitude toward risk mitigation measures.
Discussion: A recent literature review identified two social patterns with different features in relation to their attitude toward health protection rules against the spread of COVID-19. Factors positively associated with adherence to public health guidelines were perceived threat of COVID-19, trust in government, female sex, and increasing age. Factors associated with decreased compliance were instead underestimation of the COVID-19 risk, limited knowledge of the pandemic, belief in conspiracy theories, and political conservativism. Very few studies have tested interventions to change attitudes or behaviors.
Conclusion: To improve attitude and compliance toward risk reduction norms, a key intervention is fostering education and knowledge on COVID-19 health risk and prevention among the general population. However, information on COVID-19 epidemiology might be user-generated and contaminated by social media, which contributed to creating an infodemic around the disease. To prevent the negative impact of social media and to increase adherence to health protection, stronger content control by providers of social platforms is recommended.
Introduction
On 11st March 2020 the World Health Organization (WHO) declared the COVID-19 pandemic, officially starting the so-called phase 1 (World Health Organization, 2021). Before then, on February 21, 2020 the first COVID-19 clusters in Northern Italy burst out, affecting 11 municipalities in the regions of Lombardy and Veneto (Reuters, 2021). Tougher social restrictions on the general population were progressively imposed in Italy until 9 March 2020, when a national lock down was declared. Several European countries enforced more or less similar social restrictions, with the aim of curbing the spread of SARS-CoV-2. Supplementary Table 1 “Urgent nationwide measures to prevent and control the COVID-19 emergency” lists the main regulations introduced in Italy (Italian Government, 2021). Similar coercive health protection measures were introduced also in Poland (Pinkas et al., 2020). These social limitations began to be lifted on 16th May 2020, marking the beginning of phase 2 of the pandemic.
Whilst isolation and quarantine are long-standing health protection measures against the spread of dangerous communicable diseases, a country lock-down entails a number of extraordinary interventions limiting the social freedom of the general population to protect the entire community against the risk of contagion (Official Gazzette of the Italian Republic, 2021). The only movements permitted during a country lock-down are those justified by work, health and primary needs (e.g., purchasing food) and return home. Moreover, a curfew is imposed from 6 pm on, social events (team sports, gyms, religious events, funerals, cinemas, museums, etc.) are suspended and smart working is encouraged. Activities of schools, including nurseries and universities are also suspended. Bars and restaurants, initially permitted to open between 6 am and 6 pm, were eventually allowed to continue their business only as take away or domiciliary delivery (Official Gazzette of the Italian Republic, 2021).
Social restrictions are somehow in contrast with the ethical and juridical principles of European countries, which are centered around liberty and autonomy of the individual. Nobody can be obliged to follow a health treatment unless imposed by law, in full respect of human rights (Benelhocine, 2021). Nonetheless, health protection measures against COVID-19 should take into account the principle of solidarity and the good of the entire community. The solidarity principle implies that the actions of the individual should be directed at protecting not only his/her own health, but also the general population. Therefore, the principle of solidarity recalls the principle of individual responsibility to adopt social behaviors protecting other people from SARS-CoV-2 contagion (Davies and Savulescu, 2019).
A survey on Albanian residents and expats reported a high satisfactory rate (88.0%) on infection prevention and control measures against COVID-19 (Kamberi, 2020). Likewise, an Indian survey from Kerala region revealed that 95% respondents were respectful of social restrictions imposed by the local government to tackle the current pandemic (Saji, 2020). By contrast, United Kingdom residents were less satisfied with risk reduction measures implemented against COVID-19, especially with bans affecting business activities, with 31.1% interviewees convinced that quarantine could cause health problems, independently from the country of residence (Saji, 2020).
Concerns for work and business are not the only factors influencing the perceptions of health protection measures against the spread of COVID-19. Misinformation, fake news and conspiracy theories inundating social media since the beginning of the COVID-19 pandemic have generated a worrisome “infodemic,” undermining the credibility of health institutions, at least in some sectors of the general population (The Lancet Infectious Disease, 2020).
Furthermore, attitude and compliance with health protection measures against the spread of COVID-19 could vary between and within countries.
In view of the above we investigated the attitude and perception of health protection measures against COVID-19 during the first pandemic wave in Italy and Poland, to inform public health policy makers on the respective determinants. Despite Italy being more heavily hit than Poland during the first COVID-19 wave, social restrictions in the latter two countries were in fact similar (Dong et al., 2020; Roser et al., 2020; Grabowski et al., 2021).
Materials and Methods
During the first wave of COVID-19 pandemic (April – May 2020) Polish and Italian (Sardinian) residents were approached and surveyed by national/local media, regional websites, social media and university newsletters using an online questionnaire. A convenience snow-balling sampling was employed to approach as many respondents as possible from both countries. The survey instrument was posted online, participation to the survey was voluntary and all respondents returning a filled-up questionnaire were included in the study. A cross-sectional study design was adopted. Polish and Italian version of the survey tool were distributed.
The first section of the questionnaire collected socio-demographic information (Table 1). The second part investigated various perceptions/attitudes/positions (Table 2), using a Likert-type scale based upon four possible options (Grabowski et al., 2021). The last section included 7 questions (Table 3) on the attitude/perception of health protection rules, using pre-classified responses based on a Likert-type scale. The Cronbach alpha test for the seven outcome items displayed in Table 3 was calculated with Stata 14.2 and equaled 0.8141 for the overall sample, 0.8019 for the Italian version and 0.8164 for the Polish version.
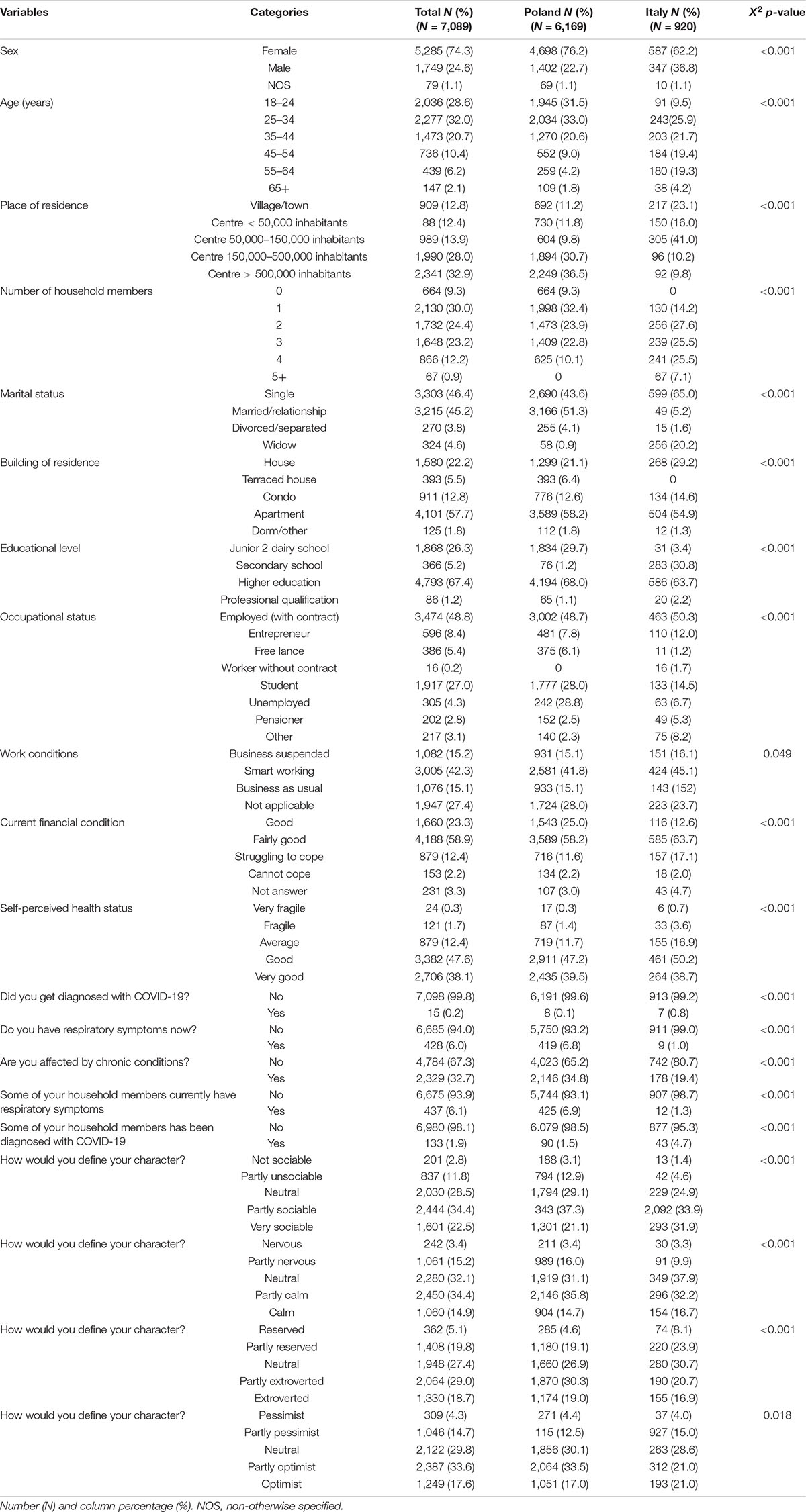
Table 1. Distributions of socio-demographic information collected by the survey.
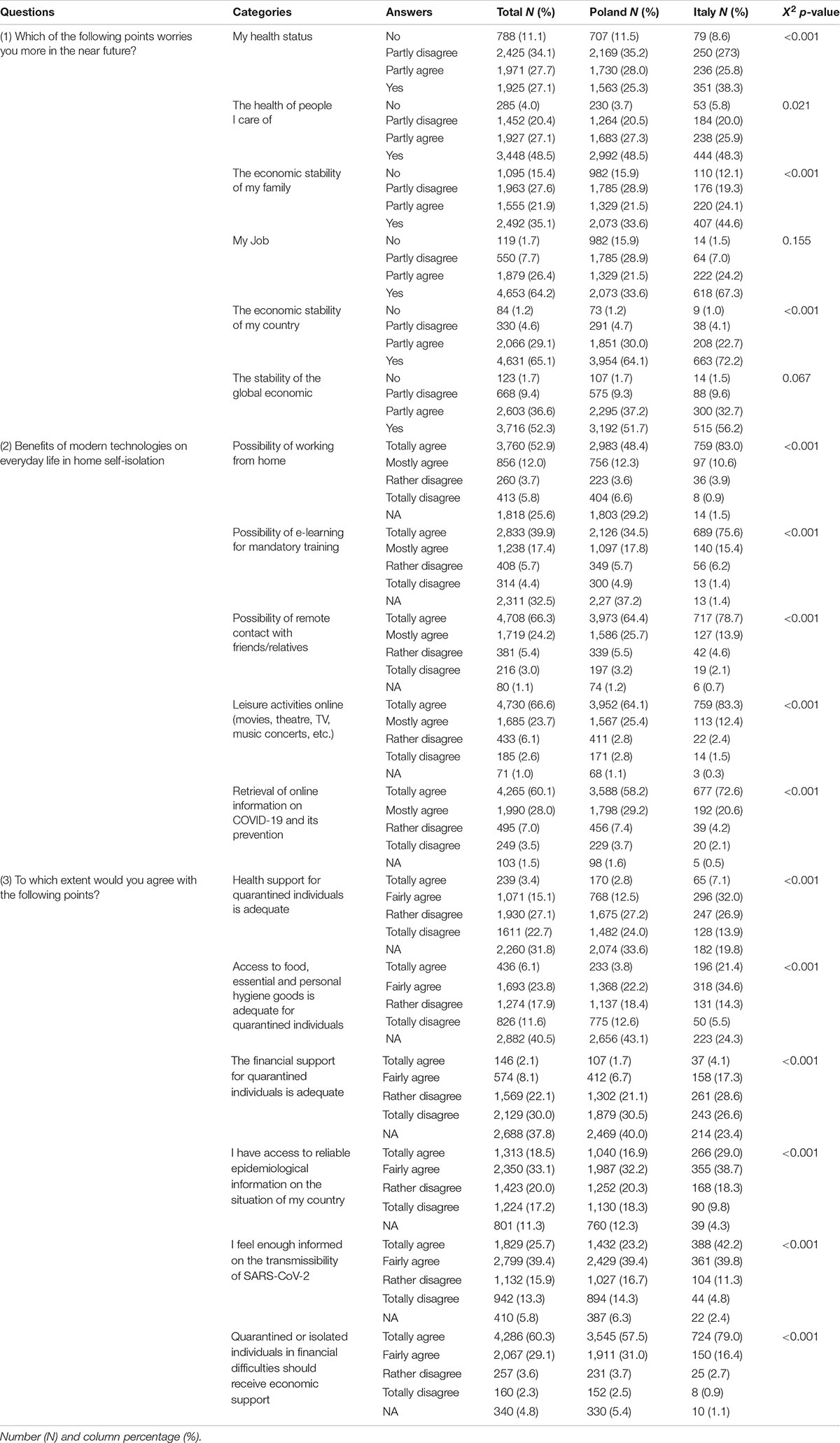
Table 2. Distributions of attitudes/perceptions on health protection measures against the spread of COVID-19 during the first epidemic wave by country.
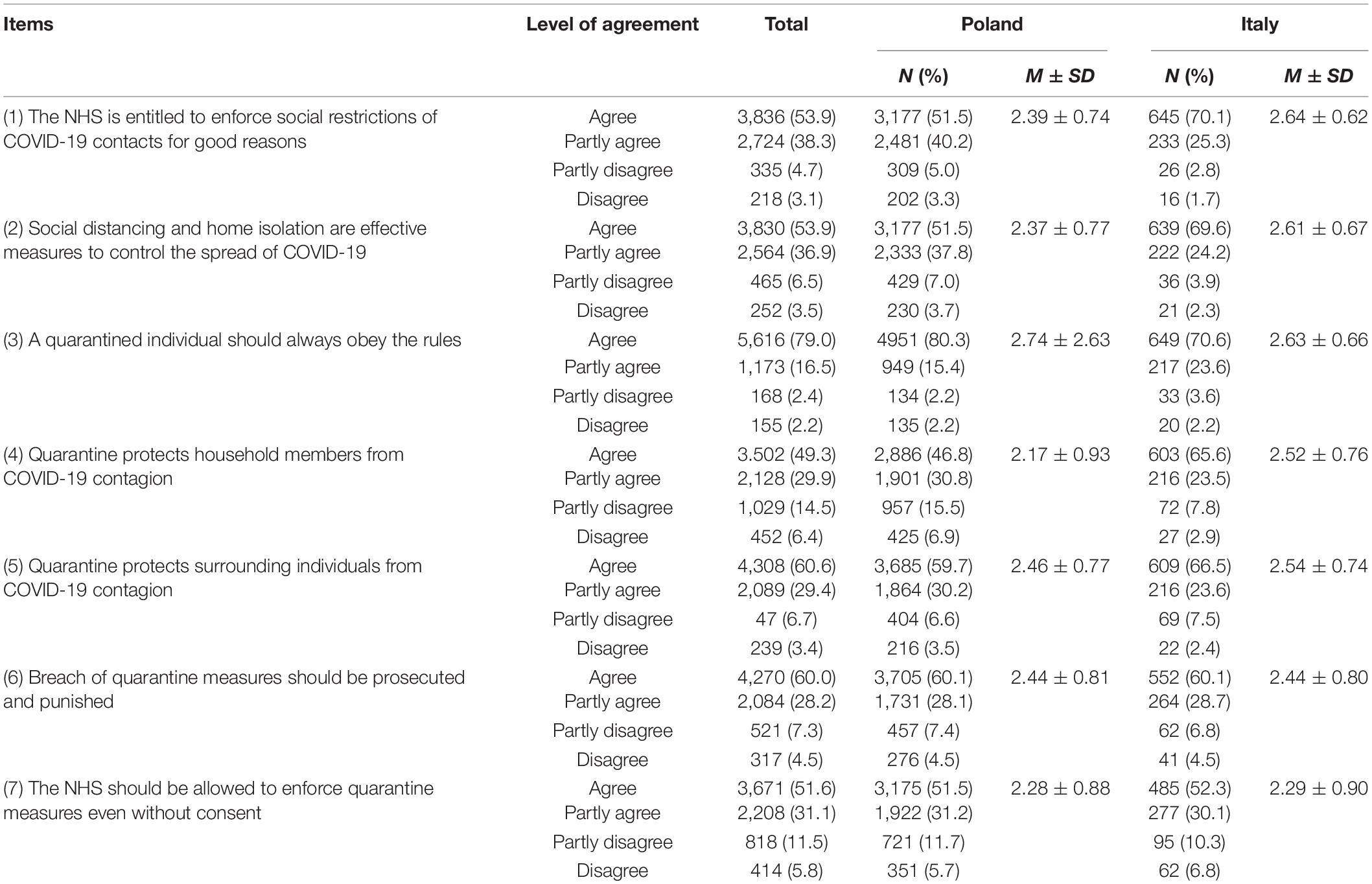
Table 3. Attitudes/perceptions on health protection measures against the spread of COVID-19 by level of agreement and country of residence (Number, N and percentage, %); and Health Protection Attitude Score (Mean, M ± standard deviation, SD) by country.
National laws and ethical guidelines for studies involving human subjects were observed. Ethics approval was obtained from the Independent Bioethical Commission for Issues of Scientific Research at the University of Gdańsk (Resolution Number NKBBN/144/2021). In particular, interviewees provided an electronic informed consent before completing the questionnaire (Supplementary Files 1, 2). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Statistical Analysis
Variables
All answers to questions displayed in Table 1 were considered categorical variables. Pre-classified answers to questions listed in Table 2 were Likert-type items which were coded as follows: “No = 0, Partly disagree = 1, Partly agree = 2, Yes = 3” (question 1); and “Totally agree = 0, Fairly agree = 1, Rather disagree = 2, Totally disagree = 3 and NA = 4” (questions 2 and 3). The latter were considered as factor variables (i.varname, according to STATA syntax) in the statistical analysis.
The answers to questions related to attitude and perception of health protection rules (Table 3) were assigned the following values: “Agree = 3; Partly agree = 2; Partly disagree = 1; and Disagree = 0.” The scores developed for each of the above 7 questions (ranging from 0 to 3) were summed up to obtain a pooled linear indicator, which we defined “health protection attitude score” (HPAS). Attitude/efficacy perception toward health protection rules increased with HPAS, which could reach a maximum value of 21 (=7 × 3).
Analysis
Numbers and percentage were calculated for each available term.
A multiple linear regression was fitted, where the outcome was HPAS and predictors were the above variables included in Tables 1, 2. The independent variables included in the multiple regression model were selected by using an automated stepwise procedure. Results were expressed as regression coefficients (RC) with 95% confidence interval (95% CI). We used the procedure of Benjamini–Hochberg (BH) to control for the false discovery rate when conducting multiple comparisons (Benjamini and Hochberg, 1995). Finally, using the values returned by the computer program, the predicted values of HPAS were calculated (Y = a + b1x1 + b2x2) for different values of predictors, using the Stata command “predict,” after fitting the final multivariable linear regression model, adding also the constant term to the predicted value estimated.
Stata 14.2 (Stata corporation, College Station, TX, United States) was used for the analysis.
Results
A total number of 7,108 questionnaires were returned: 6,169 from Poland (77% females vs. 23% males) and 939 from Sardinia (62,8% females vs. 37,1% males).
Table 1 shows the distribution of socio-demographic variables. As can be seen, interviewees were predominantly Polish residents (N = 6,169; 87.0%) than Italians (N = 920) and 74.3% were females. The age groups more represented were 25–34 years old (32.0%), followed by 18–24 years old (28.6%) and 35–44 years old (20.7%). Most respondents were living in centers with >500,000 (32.9%) or 150,000–500,000 (28.0%) inhabitants and were either single (46.4%) or married/in a relationship (45.2%) and were living with 1 (30.0%) or 2 (24.4%) household members. The vast majority of interviewees were living in apartments (57.7%) followed by condos (12.8%) and were students (27.0%), with higher education (67.4%) and were doing smart-working (42.3%). Most interviewees were in fairly good (58.9%) or good (23.3%) financial conditions and perceived their health conditions as good (47.6%) or very good (38.1%). About 32.7% of individuals were affected by co-morbidities, with 0.2% of those diagnosed with COVID-19 and 6% with respiratory symptoms at the time of the interview. Respondents predominantly had a “partly social” (34.4%), “partly calm” (34.4%), “partly extroverted” (29.0%) or “partly optimist” (33.6%) character trait.
Table 2 shows the distribution of variables expressing the perceptions as well as attitudes on health protection measures during the first pandemic wave of COVID-19. There were three main questions, each including several sub-questions (categories) with the corresponding pre-classified options (answers). The main results are the following:
Higher concerns were reported for “the economic stability of my country” (Yes = 65.1%), “my job” (Yes = 64.2%), “stability of the global economic” (Yes = 52.3), and “health of people I care of” (Yes = 48.5%).
Regarding benefits of modern technologies, “Totally agree” was expressed by 66.6% interviewees (on leisure activities online), 66.3% (on remote contact with friends/relatives), 60.1% (on retrieval of information online) and 52.9% (working from home); the corresponding percentage was, however, 39.9% for the “Possibility of e-learning for mandatory training.”
For three questions asking “is … adequate for quarantined individuals?”, the more common answer was “NA,” with a percentage equal to 40.5% (regarding access to food and essential goods), 37.8% (on financial support), and 31.8% (on health support). Obviously, for 60.3% of interviewees, quarantined individuals “should receive economic support.”
Regarding access to reliable epidemiological information, there was not a sharp contrast in beliefs but a set of opinions. The sum of “Totally agree” and “Fairly agree” is always higher than 50%, but “Totally disagree” is 17.2% for one question and 13.3% for the other.
Table 3 shows the personal positions on norms to control the spread of COVID-19 by country and level of agreement (number and percentage of respondents); and the value (mean ± standard deviation) of HPAS by country. The main interest of this table is the chance of estimating the weight of different groups. “Agree” with the 7 questions was expressed by 58% (min-max: 49%; 79%), while “Disagree” was reported by 4% (min–max: 2%; 6%) of interviewees.
As can be seen there was a highly significant cross-country variability in the distribution of all factors displayed in Tables 1–3, with the exception of occupational status of interviewees (p = 0.049) and “concerns for my job” (p = 0.155) and “stability of the global economy” (p = 0.067) in the near future (Table 3).
Table 4 displays the results of the multiple linear regression model, fitted onto 6,992 complete observations, on the attitude/perception toward health protection norms. It can be seen that, apart from sex, socio-demographic factors (shown in Table 1) were not significantly associated with HPAS. The three questions listed in Table 2 were the main drivers. Each of the latter had Likert-type items as pre-classified answers. If one or more Likert items showed non-significant RCs, the whole cluster was dropped from Table 4. Otherwise, if all RCs were significant according to BH procedure, their signs were consistent (always positive or negative) and their values displayed a monotonic trend. The sign of RC specifies the direction of association (positive sign indicating higher attitude/perception of health protection rules, and vice versa); the value of RC and the statistical significance expresses the strength of association; the monotonic trend of predicted values of HPAS displays an exposure-effect relationship. Furthermore, since they were adjusted for all other variables, RCs were devoid of confounding effect, fulfilling Hill’s criteria of causality.
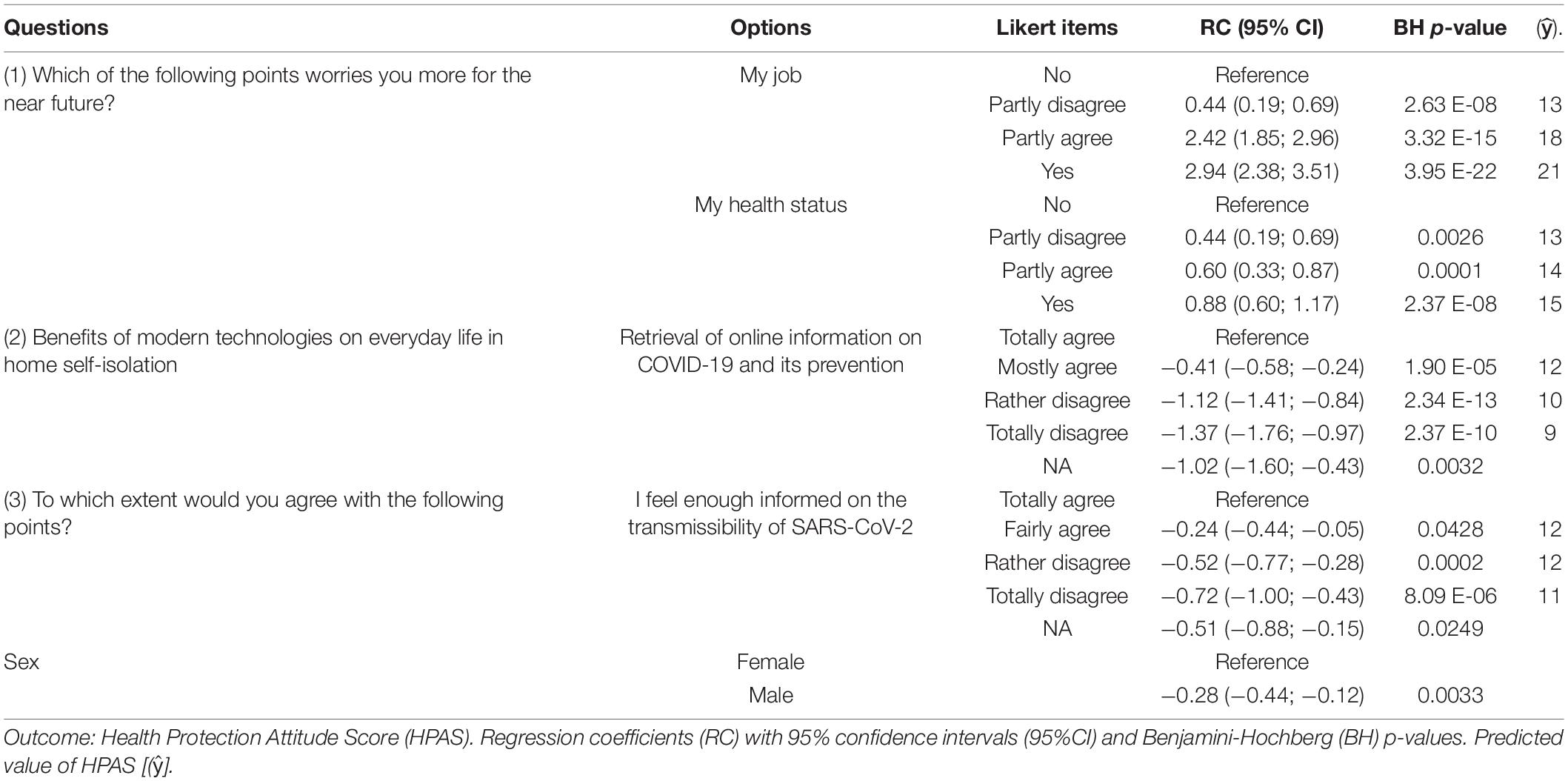
Table 4. Multiple linear regression model.
Therefore, as can be seen in Table 4, concerns for business and health due to COVID-19 were associated with a positive attitude/perception toward health protection rules. By contrast, male subjects, concerns about reliability of information available online on COVID-19 and its prevention as well as feeling of not being enough informed on the transmissibility of SARS-CoV-2 were associated with a negative attitude for risk reduction measures.
Discussion
Key Findings
A relevant finding of the present study was that, albeit significant cross-country variability between Poland and Italy in the distribution of information collected, apart from sex, socio-demographic factors (displayed in Table 1) were not significantly associated with the endpoint HPAS, whereas perceptions and positions (listed in Table 2) were its main drivers. Despite future concerns for their work and health, individuals positively perceived the social restrictions imposed in Italy and Poland to control the spread of COVID-19. However, a negative attitude toward these measures was expressed by interviewees undervaluing the reliability of the available information on the transmissibility of SARS-CoV-2 and the benefits of modern technology to mitigate the inconveniences caused by home isolation.
Study Limitations
This survey, relied on data collected via internet, cannot be considered representative of the respective general populations of Italy and Poland. In fact, our convenience sample was mainly composed of females, Polish respondents, <44 years of age. Thus, a selection bias cannot be excluded. However, the relatively large sample size, the wide range of explanatory variables and the employment of the BH criterium for statistical significance to filter possible false associations empowered this study to draw some relevant conclusions from this study.
Generalizability
Two groups of interviewees could be distinguished from the present investigation, based upon the final multiple regression model: one that, due to the threat posed by COVID-19 on health and business activities, and despite present and future hardships, accept social restrictions imposed by the government with the goal of decreasing the circulation of SARS-CoV-2; a second group not accepting limitations of liberty under the justification that the current epidemiologic information on COVID-19 is not reliable (Table 4).
Likewise, in a review of recent studies, two groups of individual characteristics were identified in relation to their attitude/compliance with public health measures against the spread of COVID-19 (Vanhove et al., 2015; Moran et al., 2021):
• GROUP 1 (“Eudaimonic”): perceiving the threat of COVID-19, trusting governments, more likely to be female and older, consistently showing a positive attitude/adherence with public health guidelines. Factors positively related to adherence though less frequently mentioned were higher socio-economic status, accessing traditional media sources, trust in science or medicine, perceived effectiveness of risk reduction measures, ability to follow guidelines.
• GROUP 2 (“Hedonic”): characterized by decreased adherence to public health guidelines, political conservatism and belief in conspiracy theories. Those with limited knowledge of the pandemic, those who felt that COVID-19 posed a low risk, and those who were unconvinced of the efficacy of health protection measures to contrast the spread of SARS-CoV-2 were consistently more likely to exhibit poor adherence.
In a study carried out in representative samples across eight countries (N = 7,568), the additional mortality rate over a 3-month period (June–August 2020) following the enforcement of lock-down against the spread of COVID-19 was 10 times higher in countries with low adherence against risk mitigation measures (United States, Sweden, Poland, and Russia) than in those with high compliance (Germany, France, Spain, and United Kingdom) (Margraf et al., 2021). Cross-country discrepancies in the adherence with health protection measures correlated with subsequent increase of mortality (correlation coefficient = −0.91) (Margraf et al., 2021). Cross-country modeling of social restrictions showed that implementing non-pharmaceutical interventions (NPIs) determines an instantaneous reduction of the base reproduction number (Rt)−an indicator of new infections of SARS-CoV-2 (Brauner et al., 2021). Brauner et al. (2021) gathered chronological data on the implementation of NPIs for 41 European and non-European countries between January and end of May 2020. The effectiveness of these NPIs was estimated by linking their enforcement dates with national case and death counts. Shutting down all educational institutions, limiting social gatherings to 10 people or less and suppressing face-to-face businesses considerably reduced the transmission of SARS-CoV-2. The additional effect of the stay-at-home policy on the transmissibility of SARS-CoV-2 was instead comparatively marginal (Brauner et al., 2021). Finally, mathematical modeling suggested that while delaying the imposition of social restrictions by 1 or 2 weeks had a negligible effect on the circulation of SARS-CoV-2, an earlier relaxation of these measures by 1 or 2 weeks translated into a marked increase of the respective infection rate (Gevertz et al., 2021).
There is a gap in the literature between the important scientific advances in COVID-19 knowledge and the strategies to promote adherence with health protection measures to contain this disease. In fact, according to the above-mentioned review (Moran et al., 2021), very few interventional studies or quasi-experimental studies have been published to date. Authors generally offered logical suggestions based on inferential findings from convenience sample surveys, rather than evidence from evaluations of interventions implemented to change attitudes and social behaviors (Moran et al., 2021).
Several people use social media platforms such as Facebook, Youtube, and Twitter as a source of information on COVID-19 (Allington et al., 2020; Brailovskaia et al., 2021; Moran et al., 2021). Differently from other sources (scientific journals, newspapers, television, reports, and official sites of governments and health authorities), the content available on social media is user-generated, hence each user can freely create, modify and share this content (Brailovskaia et al., 2021). As a consequence, social media often provide a huge amount of unfiltered (mis-) information and fake news (Allington et al., 2020; Cuello-Garcia et al., 2020; Pennycook et al., 2020; Brailovskaia et al., 2021). Previous research showed that the absorption of such information can have a major influence on the perceived burden of COVID-19, its related emotional overload, stress symptoms associated and poor adherence to urgent risk mitigation measures (Brailovskaia et al., 2021). To prevent the negative impact of social media use and to increase adherence to NPIs, a stronger content control on social platforms by the respective providers is urgently recommended. To further develop and disseminate solutions and resilience against mis- and disinformation, as requested in a “Joint Statement” by WHO, UN, UNICEF, UNDP, UNESCO, UNAIDS, ITU, UN Global Pulse and IFRC, all stakeholders – including media and social media, researchers, technologists capable to design and build effective strategies and tools to respond to the so called “infodemic,” civil society leaders and influencers – should cooperate with the UN system, with Member States and with each other (UNICEF, 2021).
Conclusion
To improve attitude and compliance with risk reduction norms, a key intervention is fostering education and knowledge on the COVID-19 risk among the general population. However, a considerable proportion of information on COVID-19 epidemiology is user-generated and contaminated by social media, contributing to create an “infodemic” around this disease. It is therefore urgent to set up interventions to contain the mis- and disinformation disseminated online by users of social media. In addition, governmental communication should stress the responsibility of users for the contents they spread via social media and the need for the respective providers to verify all information posted online, before sharing it.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Independent Bioethical Commission for Issues of Scientific Research at the Medical University of Gdańsk (NKBBN/144/2021). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
LL, JG, JS, TM, and PW: study concept. LC and GM: study design, data analysis, and data interpretation. RM, LL, and JG: survey translation. RM, DP, SB, JG, JS, TM, and PW: data collection. LC, GM, LL, and DP: literature search. LC, GM, SB, and LL: manuscript drafting. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2021.805790/full#supplementary-material
References
Allington, D., Duffy, B., Wessely, S., Dhavan, N., and Rubin, J. (2020). Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psycholog. Med. 2020, 1–7. doi: 10.1080/08870446.2021.1974861
Benelhocine, C. (2021). European Social Charter. - Council of Europe. Available from: https://rm.coe.int/168048b05a (accessed on 4 August 2021).
Benjamini, Y., and Hochberg, Y. (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. 57, 289–300.
Brailovskaia, J., Cosci, F., Mansueto, G., and Margraf, J. (2021). The relationship between social media use, stress symptoms and burden caused by Coronavirus (Covid-19) in Germany and Italy: A cross-sectional and longitudinal investigation. J. Affect. Dis. Rep. 3:100067. doi: 10.1016/j.jadr.2020.100067
Brauner, J. M., Mindermann, S., and Mrinank Sharma, M. (2021). Inferring the effectiveness of government interventions against COVID-19. Science 371:eabd9338. doi: 10.1126/science.abd9338
Cuello-Garcia, C., Perez-Gaxiola, G., and van Amelsvoort, L. (2020). Social media can have an impact on how we manage and investigate the COVID-19 pandemic. J. Clin. Epidemiol. 2020:32603686. doi: 10.1016/j.jclinepi.2020.06.028
Davies, B., and Savulescu, J. (2019). Solidarity and Responsibility in Health Care. Public Health Ethics 12, 133–144. doi: 10.1093/phe/phz008
Dong, E., Du, H., and Gardner, L. (2020). An interactive web-based dashboard to track COVID-19 in real 352 time. Lancet Infect. Dis. 20, 533–534. doi: 10.1016/S1473-3099(20)30120-1
Gevertz, J. L., Greene, J. M., Sanchez-Tapia, C. H., and Sontag, E. D. (2021). A novel COVID-19 epidemiological model with explicit susceptible and asymptomatic isolation compartments reveals unexpected consequences of timing social distancing. J. Theoret. Biol. 510:110539. doi: 10.1016/j.jtbi.2020.110539
Grabowski, J., Stepien, J., Waszak, P., Michalski, T., Meloni, R., Grabkowska, M., et al. (2021). Social Isolation During COVID-19 Pandemic. Perceived Stress and Containment Measures Compliance Among Polish and Italian Residents. Front. Psychol. 12:673514. doi: 10.3389/fpsyg.2021.673514
Italian Government (2021). Coronavirus Covid-19. Available from: www.governo.it/it/coronavirus misure del governo (accessed on 4 August 2021)
Kamberi, F. (2020). Effect of Covid-19 pandemic on mental health among Albanian people residing in the country and abroad – Implications for mental care. Archiv. Psychiat. Nurs. 34, 507–512. doi: 10.1016/j.apnu.2020.08.003
Margraf, J., Brailovskaia, J., and Schneider, S. (2021). Adherence to behavioral Covid-19 mitigation measures strongly predicts mortality. PLoS One 16:e0249392. doi: 10.1371/journal.pone.0249392
Moran, C., Campbell, D. J., Campbell, T. S., Roach, P., Bourassa, L., Collins, Z., et al. (2021). Predictors of attitudes and adherence to COVID-19 public health guidelines in Western countries: a rapid review of the emerging literature. J. Public Health 2021:70. doi: 10.1093/pubmed/fdab070
Official Gazzette of the Italian Republic (2021). Decree of the President of the Council of the Ministries 8 march 2020. Available from: www.gazzettaufficiale.it/eli/id/2020/03/08/20A01522/sg (accessed on 4 August 2021)
Pennycook, G., McPhetres, J., Zhang, Y., Lu, J. G., and Rand, D. G. (2020). Fighting COVID-19 misinformation on social media: Experimental evidence for a scalable accuracy-nudge intervention. Psycholog. Sci. 31, 770–780. doi: 10.1177/0956797620939054
Pinkas, J., Jankowski, M., Szumowski, L., Lusawa, A., and Zgliczynski, W. S. (2020). Filip Raciborski Waldemar Wierzba Mariusz Gujski. Public Health Interventions to Mitigate Early Spread of SARS-CoV-2 in Poland. Med. Sci. Monit. 26:e924730. doi: 10.12659/MSM.924730
Reuters (2021). Coronavirus outbreak grows in northern Italy, 16 cases reported in one day. Avialble from: https://www.reuters.com/article/us-china-health-italy-outbreak-idUSKBN20F2GF (accessed on 4 August 2021)
Roser, M., Ritchie, H., Ortiz-Ospina, E., and Hasell, J. (2020). Coronavirus Pandemic (COVID-19). OurWorldInData. Org. 4:355.
Saji, J. A. (2020). Social influence of COVID-19: An observational study on the social impact of post-COVID-19 lockdown on everyday life in Kerala from a community perspective. J. Educ. Health Promot. 2020:29. doi: 10.4103/jehp.jehp_650_20
UNICEF (2021). Managing the COVID-19 infodemic: Promoting healthy behaviours and mitigating the harm from misinformation and disinformation Joint statement by WHO, UN, UNICEF, UNDP, UNESCO, UNAIDS, ITU, UN Global Pulse, and IFRC. Available from: https://www.unicef.org/press-releases/managing-covid-19-infodemic-promoting-healthy-behaviours-and-mitigating-harm (last accessed on 4 August 2021)
Vanhove, A. J., Herian, M. N., Harms, P. D., Luthans, F., and DeSimone, J. A. (2015). Examining psychosocial well-being and performance in isolated, confined, and extreme environments. Washington, DC: National Aeronautics and Space Administration.
World Health Organization (2021). WHO Director-General’s opening remarks at the media briefing on COVID-19 - 11 March 2020. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020 (accessed on 3 August 2021)
Keywords: COVID-19, health protection, lock down, risk reduction, risk perception, attitude, adherence, social restrictions
Citation: Lorettu L, Mastrangelo G, Stepien J, Grabowski J, Meloni R, Piu D, Michalski T, Waszak PM, Bellizzi S and Cegolon L (2021) Attitudes and Perceptions of Health Protection Measures Against the Spread of COVID-19 in Italy and Poland. Front. Psychol. 12:805790. doi: 10.3389/fpsyg.2021.805790
Received: 31 October 2021; Accepted: 07 December 2021;
Published: 24 December 2021.
Edited by:
Dian Veronika Sakti Kaloeti, Diponegoro University, IndonesiaReviewed by:
Arif Ansori, Airlangga University, IndonesiaCaleb Cornaby, University of North Carolina Hospitals, United States
Copyright © 2021 Lorettu, Mastrangelo, Stepien, Grabowski, Meloni, Piu, Michalski, Waszak, Bellizzi and Cegolon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luca Cegolon, bC5jZWdvbG9uQGdtYWlsLmNvbQ==, bHVjYS5jZWdvbG9uQHVuaXRzLml0
†These authors have contributed equally to this work