Abstract
With the rising popularity of mindfulness practice, it is necessary and crucial to evaluate mindfulness using comprehensive and objective measures. The instruments to assess mindfulness in China mainly evaluate mindfulness as a state or trait mode. Few process measures have been developed to clarify effective therapy benefits of the alterations obtained using mindfulness practice. Therefore, this study aims to adapt the Applied Mindfulness Process Scale (AMPS) into Mandarin and explore in detail the reliability and validity of this novel-translated measure. Following cross-cultural modification for original AMPS into Mandarin as per established guidelines, psychometric evaluation was performed on a cohort of 234 Chinese adults. Construct validity was analyzed through exploratory factor analysis (n = 115), together with confirmatory factor analysis (n = 119). Reliability was assessed by internal consistency together with test-retest reliability. Findings indicated that the internal consistency was high, with Cronbach’s alpha being 0.936. The principal component analysis led to a three-factor structure that explained 67.374% of all variations. The three-factor model was consistent with the original scale model. Based upon confirmatory factor analyses, all fitting indices satisfied the standard, which showed a close fit to the data. Therefore, the newly multi-culturally modified AMPS has sufficient validity, test-retest reliability, together with internal consistency. Chinese AMPS may offer researchers and clinicians a psychometrically optimized tool for evaluating the application of mindfulness and change process within mindfulness-based interventions (MBIs) in Mainland China.
Introduction
Mindfulness was typically described as the awareness that emerges by intentionally bringing one’s attention, in a non-judgmental manner, to the internal and external experiences that exist in the present moment (Kabat-Zinn, 2003). With the advances in standardized mindfulness-based interventions (MBIs) and its proper implementation, mindfulness has been recognized and spread rapidly in Western psychology (Gu et al., 2015). MBIs consist of a mixture of mind-body practices applied for enhancing mindfulness consciousness, represented through the momentary-based non-judging attention being freed from the abstraction and focus of cognitive emotions (Kabat-Zinn, 2003). Considerable research has shown that MBIs are highly therapeutic for multiple conditions/wellbeing states among diverse populations (Hofmann et al., 2010; Eberth and Sedlmeier, 2012; Khoury et al., 2013), including anxiety (Hofmann et al., 2010; Green and Bieling, 2012; Hinton et al., 2013), depressive relapsing risks (Teasdale et al., 2000; Kuyken et al., 2009), depression (Strauss et al., 2014), stress (Chiesa and Serretti, 2009), chronic pain (Grossman et al., 2007), quality of life (Kuyken et al., 2009; Godfrin and Van Heeringen, 2010), together with psychological/emotional distress (Ledesma and Kumano, 2009; Xu et al., 2016). Furthermore, MBIs have demonstrated to be effective through specific psychopathological alterations, including cognitive biases, affective dysregulation, and interpersonal effectiveness (Brown et al., 2007; Bullis et al., 2014; Curtiss et al., 2017).
Due to the rising popularity of MBIs, proper assessment of mindfulness is essential. The development of reliable, validated instruments gives trainers the possibility to evaluate their interventions, together with researchers being able to analyze potential psychological processing mechanisms using mindfulness. Some self-report state and trait measures are already established, including the Mindful Attention Awareness Scale (MAAS) (Brown and Ryan, 2003), Freiburg Mindfulness Inventory (FMI) (Walach et al., 2006), Kentucky Inventory of Mindfulness Skills (KIMS) (Baer et al., 2004), Five-Facet Mindfulness Questionnaire (FFMQ) (Baer et al., 2006), Cognitive and Affective Mindfulness Scale (CAMS) (Feldman et al., 2007), together with the Toronto Mindfulness Scale (TMS) (Lau et al., 2006). Notwithstanding the proliferation of instruments for mindfulness evaluation, all the tools mentioned above cater for mindfulness assessment through an outcome perspective, not from a processing perspective. Such a methodology kept limited understanding of how mindfulness-based skills and practices were applied in daily life when encountering life stressors. For the purpose of elucidating treatment mechanisms for alterations obtained using mindfulness practice, it was essential to develop a process measure. Measuring the process of mindfulness practice would enable researchers to recognize more effectively the specific mechanistic pathways by which mindfulness and corollary advantages are attained within those involved in MBIs, together with its implementations in day-to-day living situations (Chiesa et al., 2014). The existing scales used to measure the process of mindfulness practice mainly consist of the 7-item Mindfulness Process Questionnaire (MPQ) developed in 2012 and the Applied Mindfulness Process Scale (AMPS), developed in 2016. The MPQ identifies situations in which an individual shifts to a higher mindful state and guides the participant to note how they focus on the process of becoming mindful, instead of the “success” in achieving mindfulness (Erisman and Roemer, 2012). However, the MPQ did not emphasize the application of mindfulness practice. It was difficult for researchers to use this instrument to explore the mechanism of mindfulness practice, which could limit their design of MBI programs. The AMPS is a 15-item process measure developed by Michael J. Li and colleagues (Li et al., 2016). Compared with the MPQ, the AMPS contextualized the application of mindfulness. Every individual AMPS entry was designed to reflect the application of mindfulness in coping with negative states, challenging times, and daily stresses through positive/negative emotional regulation and decentering. The newly well-designed AMPS can be applied to evaluate not only the application of mindfulness but also the change process within mindfulness practice.
In recent years, research on mindfulness practice or MBIs has shown an increasing trend in China. Although several self-report state and trait measures, such as MAAS, FFMQ and FMI, had been validated in Chinese culture (Chen et al., 2012; Chen and Zhou, 2013; Meng et al., 2019), few process measures on the application of mindfulness practice have been developed in the Chinese context. Consequently, the development and psychometric adaptation of a Chinese AMPS can offer a novel angle for identifying a spectrum of therapy-aimed facets of MBIs for Chinese researchers and further lay the foundation for research on applying MBIs in China. In this study, we cross-culturally adapted the AMPS as a psychometric process measure in China to capture the implementation of practical, daily-life mindfulness practice and consequently evaluated its psychometric properties.
Materials and Methods
Procedure and Participants
Psychometric properties for the translated scale were evaluated using a cross-sectional survey. Two hundred thirty-four residents were recruited using convenience sampling from multiple (5) districts of Xi’an, the capital of Shaanxi Province in Northwest China. The city was selected because it is the largest designated central city in Northwest China and is accessible to the investigators. Participant inclusion criteria included: (a) reaching the age of 18; (b) possessing household registration in Xi’an or the permanent residence is Xi’an; (c) possessing the ability of reading and communication; (d) willing to participate in the study. All participants had signed informed consent following a detailed description of the investigation goals and methodologies involved. Meanwhile, all members of the study cohort were advised that withdrawal from the investigation could be performed at any point during the trial, without any repercussions. Anonymity and confidentiality were assured. Written informed consent was taken from all participants before the study. All procedures performed in studies involving human participants were in accordance with the Ethics Committees of Xi’an Jiaotong University and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Instruments
Applied Mindfulness Process Scale
The original Applied Mindfulness Process Scale (AMPS) was developed in 2016 and comprised three subscales: positive emotion regulation (5 items), negative emotion regulation (5 items), and decentering (5 items). Positive Emotion Regulation consisted of items reflecting mindfulness-based coping mechanisms through re-focusing onto positive emotional experiences and positive re-appraisal of challenging life situations. Negative Emotion Regulation included items reflecting mindfulness-based coping mechanisms through reducing negative emotion. Decentering consisted of items reflecting mindfulness-based coping mechanisms by the separation from negative feelings/thoughts through the consideration of individual mental experience as lacking absolute authenticity (Li et al., 2016). Each item was scored from 0 to 4 (0 = never; 1 = rarely; 2 = sometimes; 3 = often; 4 = almost always). According to psychometric properties testing, the overall AMPS had good internal consistency with Cronbach’s alpha coefficient of 0.91. Comparative fit index (CFI) for the three-factor model was 0.97, Tucker-Lewis index was 0.94, and the root-mean-square-error-approximation (RMSEA) was 0.06, indicating it had a valid psychometric parameter (Li et al., 2016).
General Information Questionnaire
We generated the General Information Questionnaire to investigate sociological, demographics-based and health-related status. The questionnaire included age, gender, educational background, health condition, etc.
Translation Process
After receiving permission to use this instrument from the copyright holders, the Chinese translation process for AMPS was completed in two steps using a clear guideline (Beaton et al., 2000). Firstly, in line with Brislin’s translation procedure (Brislin, 1970), a committee of two collaborators who were fluent in Chinese/English and proficient in medical psychology separately accomplished their own version of the first AMPS draft. Consequently, a third individual was required to combine both draft versions while also referring to the original scale. This third, combined draft was consequently and blindly back-translated separately by two translators into English, as accuracy assurance.
Experts’ Reviewing Process
A total of seven experts were recruited for the reviewers’ board, consisting of psychologists, mental health workers, nursing professors, and managers, all with a Master’s degree or higher and with expertise in clinical psychology and scale development. This board assessed the source scale together with all subsequent translated AMPS drafts, verifying the equivalence of phrases within both the initial AMPS and the finalized back-translated AMPS draft. The review board members continued discussing all AMPS items at each stage of reviewing until a consensus was reached. Joint rating for the finalized AMPS was then performed in order to assess the content validity index (CVI), for individual scale items (I-CVIs), together with full scale (S-CVI).
Pilot-Study
A total of 20 residents recruited through convenience sampling in Northwest China were informed to fill in the Chinese AMPS questionnaire together with delineating any unclear/incorrect items and propose alternatives. The completion timeframe was approximately 5–10 min. An interview was performed to evaluate participant perspectives for each entry and register their suggestions for optimizing the Chinese AMPS. Following the discussion between researchers and participants, all ambiguous issues were fixed. One typical issue concerned the improvement of response rate of the questionnaires and participant fear reduction by changing the order of item 1 (Observe thoughts in a non-attached manner.) and item 2 (Relax my body when I was tense.). Moreover, the translations of some phrases were changed to adapt to the Chinese context. Following this process, the final Chinese version was developed. The 20 participants were asked to complete the scale again after 2 weeks, for assessing test-retest reliability.
Data Analysis
Statistical Package for the Social Sciences (SPSS) version 20.0 was employed. Statistical description for demographic variables was performed using means, standard deviations (SD), and frequency tables. Content validity index (CVI) was conducted for score quantification on each entry and the total AMPS. The CVI was generated through expert-opinion on relevance ratings for each entry, through a 4-point scale, from 1 (highly invalid) to 4 (highly valid). Any item being designated a 3 or 4 on this 4-point scale indicated that experts have reached a consensus on the relevance of this item. Individual item CVI was consequently generated, with a score of above 0.8 denoted validity (Polit et al., 2007). Internal consistency was generated via Cronbach alpha coefficient, whereby values ≥0.7 were deemed to be sufficient (Osburn, 2000). Split-half coefficient reliability was generated through the employment of 50% of all odd/even items. Test-retest reliability was generated through intra-class correlation coefficient (ICC) for AMPS items (Giavarina, 2015), whereby values of 0.60–0.80 were accepted as reliable, with values above 0.80 having excelled in reliability (Chavance, 2008). Individual item validity was identified using item analysis. Unfavorable floor/ceiling influences were deemed to exist if more than 15% of survey-participants achieved the highest/lowest score. Exploratory factor analysis employing principal component analysis (PCA) with oblique rotation was performed for assessing AMPS factor structure (Pryse et al., 2015). Scree plot, Kaiser Criterion (eigenvalue), combined with clinical interpretation, were all used to recognize factor solution. Items were considered relevant if factor-loading coefficients were above 0.40/gathered factors obtained an eigenvalue ≥1.0 (Sapountzi-Krepia et al., 2016). Confirmatory factor analysis (CFA) was also done for verifying factor structure. Expected values of proposed indices were (Batista-Foguet et al., 2004): (a) Chi-squared divided by the degrees of freedom ≤ 3; (b) the root mean squared error of approximation (RMSEA) < 0.08; (c) the comparative fit index (CFI) > 0.90 and goodness-of-fit index (GFI) > 0.90.
Results
Sample Characteristics
Table 1 summarizes the participant characteristics. In summary, 234 residents participated in our study, including 128 (54.7%) females and 106 (45.3%) males. The mean age was 38.56 years (SD = 10.575). Participants were well-educated, with more than 44% having a bachelor’s degree or higher. The main occupations of the participants included: Peasantry (10.7%), Worker (8.5%), Staff (32.5%), Cadre (8.5%), Retired or unemployed (30.8%), and other (9.0%). There were 141 (60.2%) participants whose monthly household income was more than 3,000 yuan, though 59.0% of the participants were in a state of illness (indicating 59.0% of the participants had acute or chronic diseases) at the time of the investigation.
TABLE 1
| Characteristics | Respondents | n | % |
| Age (years) | 18–40 | 149 | 63.7 |
| Mean: 38.56 | 41–60 | 85 | 36.3 |
| SD: 10.575 | |||
| Gender | Male | 106 | 45.3 |
| Female | 128 | 54.7 | |
| Ethnicity | Han | 229 | 97.9 |
| Minorities | 5 | 2.1 | |
| Education | Elementary school or lower | 40 | 17.1 |
| Junior middle school | 39 | 16.7 | |
| High school/Vocational School | 52 | 22.2 | |
| College or higher | 103 | 44.0 | |
| Employment | Peasantry | 25 | 10.7 |
| Worker | 20 | 8.5 | |
| Staff | 76 | 32.5 | |
| Cadre | 20 | 8.5 | |
| Retired or unemployed | 72 | 30.8 | |
| Other | 21 | 9.0 | |
| Marital status | Married | 132 | 56.4 |
| Unmarried | 99 | 42.3 | |
| Other | 3 | 1.3 | |
| Monthly household income per person (yuan) | <1,000 | 37 | 15.8 |
| 1,000–2,999 | 56 | 24.0 | |
| 3,000–4,999 | 53 | 22.6 | |
| ≥5,000 | 88 | 37.6 | |
| Illness | No | 96 | 41.0 |
| Yes | 138 | 59.0 |
Demographic characteristics of sample (n = 234).
Item Analysis
First, we sorted AMPS items within high-/low-scoring subgroups, whereby the highest-scoring 27% formed the high subgroup, and the least-scoring 27% formed the low subgroup. Consequently, a comparative analysis of the mean individual-item score for both subgroups was performed. Item analysis (Table 2) confirmed variation between the two subgroups with statistical significance (p < 0.001). Item analysis was additionally conducted on the subscale. For the high subgroup, the mean scores for decentering, positive emotion regulation, and negative emotion regulation were 21.850 (SD = 1.039), 22.383 (SD = 1.354), and 21.550 (SD = 1.567), respectively. For the low subgroup, the mean scores for decentering, positive/negative emotion regulation were 12.167 (SD = 2.203), 13.650 (SD = 2.364), and 12.300 (SD = 2.036), respectively. These results demonstrated that each item had solid discrimination properties exempted from floor/ceiling effects and, consequently, no entry was excluded.
TABLE 2
| Subscale | Low score group (N = 59) | High score group (N = 69) | t | p |
| Decentering | 12.167 ± 2.203 | 21.850 ± 1.039 | –30.797 | <0.001 |
| Positive Emotion Regulation | 13.650 ± 2.364 | 22.383 ± 1.354 | –24.833 | <0.001 |
| Negative Emotion Regulation | 12.300 ± 2.036 | 21.550 ± 1.567 | –27.888 | <0.001 |
| Total | 38.683 ± 6.072 | 64.700 ± 3.475 | –28.806 | <0.001 |
Item analysis of the Chinese version of AMPS (n = 234).
Reliability
The summaries for internal consistency, together with split-half reliability for AMPS are illustrated in Table 3. The Cronbach’s alpha on the total questionnaire was 0.936, with the three subscales having a Cronbach’s alpha of 0.887 (decentering), 0.860 (positive emotion regulation), and 0.922 (negative emotion regulation). Split-half reliability for all items of the scale was 0.902, with subscale values ranging between 0.823 and 0.931. Test-retest reliability through ICC was 0.861 for the total scale and 0.841 to 0.860 for the three subscales, which showed a good stability.
TABLE 3
| Subscale | No. of items | Cronbach’s α | Split-half | Test-retest |
| Decentering | 5 | 0.887 | 0.888 | 0.841 |
| Positive Emotion Regulation | 5 | 0.860 | 0.823 | 0.855 |
| Negative Emotion Regulation | 5 | 0.922 | 0.931 | 0.860 |
| Total | 15 | 0.936 | 0.902 | 0.861 |
Reliability of the Chinese version of AMPS (n = 234).
Content Validity
All experts agreed that the AMPS was mainly developed to evaluate how participants apply mindfulness practices for coping with stressors and hassles in everyday life. All items had been reviewed by the reviewer board to be “very relevant”/“quite relevant.” Item-level CVI ranged from 0.88 to 1.0. Scale-level CVI reached 0.984, indicating excellent content validity.
Construct Validity
Exploratory Factor Analysis
In this study, the data was divided into two parts randomly. The first 115 samples (SPSS marked as “0” subgroup automatically) were used for exploratory factor analysis. Principle component analysis (PCA) with oblique rotation was employed to assess the factorial structure of the 15-item AMPS. The Kaiser-Meyer-Olkin (KMO) recording of sampling adequacy was 0.881, and Bartlett’s test of sphericity was statistically significant (p < 0.01), indicating that such data were appropriate for factor analyses. Following Kaiser’s criterion of extracting factors having eigenvalues >1 (Factor 1 = 7.144, Factor 2 = 1.619, Factor 3 = 1.344) and the scree plot (Figure 1), a three-factor structure that explained 67.374% of the total data variance was revealed through pattern matrix. The communalities of all items ranged from 0.475 to 0.761, which were more than 0.4. Therefore, all items were reserved. Exploratory factor analysis for all items generated factor loading that ranged between 0.615 and 0.823. Item-15 (“see alternate views of a situation”) can correspond to either factor 2 (factor loading: 0.515) or factor 3 (factor loading: 0.665). According to the professional judgment of its content and factor loading, it was finally included in factor 3, the Decentering subscale. The final exploratory factor analysis (EFA) results are illustrated in Table 4.
FIGURE 1
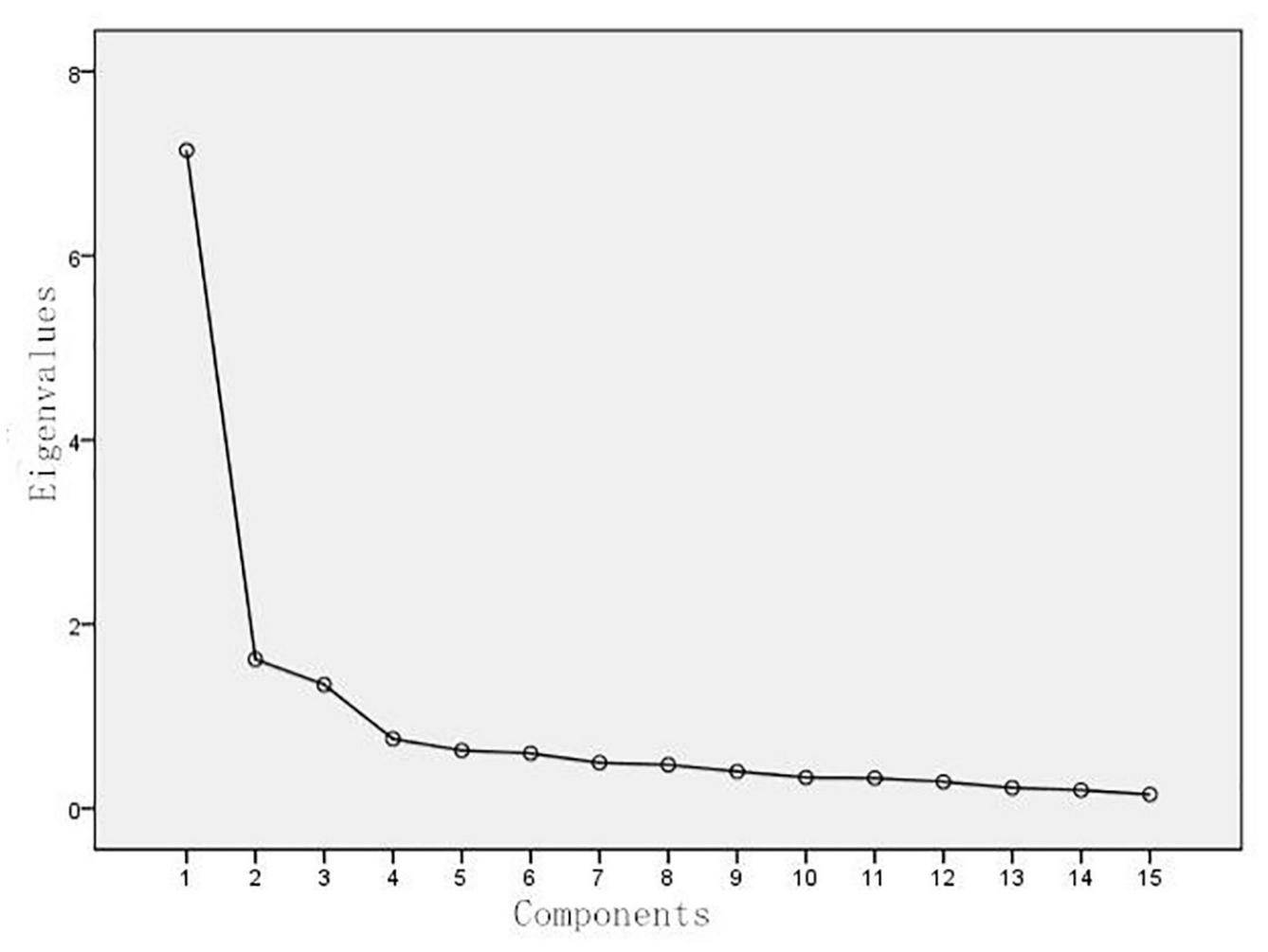
Scree plot of the Chinese version of AMPS.
TABLE 4
| Item No. | Dimension | Item | Factor 1 | Factor 2 | Factor 3 | Communalities |
| 2 | D | Observe my thoughts in a non-attached manner | 0.727 | 0.678 | ||
| 3 | D | See that my thoughts were not necessarily true | 0.823 | 0.742 | ||
| 12 | D | Let go of unpleasant thoughts and feelings | 0.693 | 0.675 | ||
| 13 | D | Realize that my thoughts were not facts | 0.758 | 0.696 | ||
| 15 | D | See alternate views of a situation | 0.515 | 0.665 | 0.719 | |
| 4 | P | Enjoy the little things in life more fully | 0.615 | 0.475 | ||
| 7 | P | See the positive side of difficult circumstances | 0.759 | 0.639 | ||
| 9 | P | Realize that I can grow stronger from difficult circumstances | 0.733 | 0.597 | ||
| 11 | P | Be aware of and appreciating pleasant events | 0.728 | 0.580 | ||
| 14 | P | Notice pleasant things in the face of difficult circumstances | 0.752 | 0.703 | ||
| 1 | N | Relax my body when I was tense | 0.791 | 0.747 | ||
| 5 | N | Calm my emotions when I was upset | 0.805 | 0.761 | ||
| 6 | N | Stop reacting to my negative impulses | 0.793 | 0.726 | ||
| 8 | N | Reduce tension when I was stressed | 0.703 | 0.688 | ||
| 10 | N | Stop my unhelpful reactions to situations | 0.745 | 0.680 | ||
| Eigenvalues | 7.144 | 1.619 | 1.344 | |||
| Variance (%) | 47.624 | 10.790 | 8.960 | |||
| Cumulative (%) | 47.624 | 58.414 | 67.374 | |||
Factor loadings on items of the Chinese version of AMPS (n = 115).
D represents Decentering subscale, P represents Positive Emotion Regulation subscale, N represents Negative Emotion Regulation subscale; Responses are on a 5-point Likert scale from 1 never to 5 almost always.
Confirmatory Factor Analysis
A total of 119 samples (SPSS marked as “1” subgroup automatically) were used for confirmatory factor analyses. A three-factor model was established according to exploratory factor analytical outcomes (see Figure 2 and Table 5). Prior to modification, individual item factor loading ranged between 0.83 and 1.27, all above 0.7. All fit indices, except the p-value and GFI within the initial model, complied with suggested parameters for satisfactory model fitting. The fit indexes were excellent in the modified model: the p-value was 0.093, exceeding 0.05. The indices for GFI (0.902 for the modified model) and CFI (0.987 for the modified model) exceeded 0.90. The RMSEA was 0.042, less than 0.08. Consequently, the correlated three-factor structure contributed an ideal model fit as previously predicted, and its application seems appropriate for the population survey.
FIGURE 2
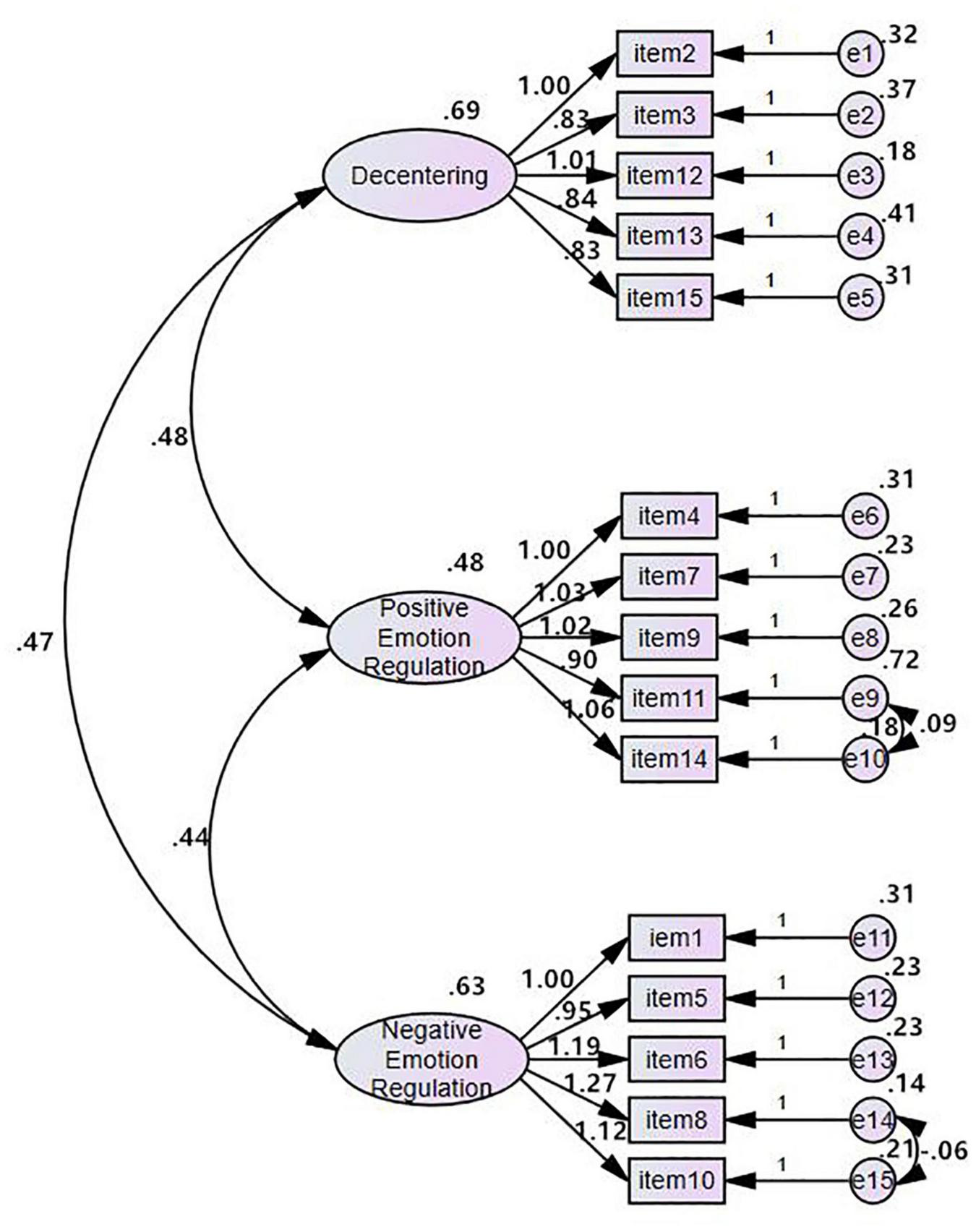
A schematic diagram of standardized model fitting of the Chinese version of AMPS.
TABLE 5
| Index | Benchmark | Initial model | Modified model |
| χ2/df | <3 | 1.297 | 1.208 |
| p | >0.05 | 0.033 | 0.093 |
| GFI | >0.90 | 0.890 | 0.902 |
| CFI | >0.90 | 0.981 | 0.987 |
| RMSEA | <0.08 | 0.050 | 0.042 |
| NFI | >0.90 | 0.924 | 0.931 |
| IFI | >0.90 | 0.982 | 0.987 |
The fitting indexes of confirmatory factor analysis of the Chinese version of AMPS (n = 119).
Discussion
In the present study, we cross-cultural adapted the AMPS into standard Mandarin and explored the reliability/validity for such a novel-translated instrument in China. It was meaningful for Chinese researchers to use the Chinese version of AMPS for analyzing how people employ mindfulness for coping with stress throughout life. All preliminary efforts we conducted ensured AMPS to be designed in compliance with the rules of Standard Mandarin. For this purpose, the forward-backward translating methodology was implemented. In addition, the draft was given to 20 participants for assessing the complexity level in reading and interpretations. According to the pilot results, we had a heated discussion on the translation of some English words and finally reached a consensus. Following these changes, the participants were re-queried, and they claimed they would answer the same way for both items, but the latter construction made more sense in Chinese. Such provisions lead to a semantically, idiomatically, experientially, and conceptually equivalent scale to the original.
Our project also played a crucial role regarding reliability/validity for cross-cultural AMPS. Reliability represents the stability, accuracy and consistency of a measurement (Zhen-qiu, 2011). The Cronbach’s alpha was 0.936 in our 234 residents sample in the northwest of China, indicating a good internal consistency. This result was higher than the result shown in the original version (Li et al., 2016). One reason may be the cultural sensitivity of translation. Mindfulness originated from Southeast Asia and influenced by the regional culture, where the scale is suitable for Chinese citizens. Alternately, such enhanced reliability could be stemming from an increased sample size in this study (234 within our investigation vs. 134 within the original research). Test-retest intra-class correlation was 0.861 for the overall scale, demonstrating that the AMPS is stable over time (across 2 weeks in this study). This adds further information on the reliability of this scale, since test-retest reliability was not measured within the original AMPS validation trial.
Evaluating the validity of the scale can verify the level of compliance between the measured and expected outcomes (Zhen-qiu, 2011). Both content and construct validity were measured for this Chinese AMPS. CVI was employed for content validity analysis. All experts were asked to make comments or suggestions on any items in the inquiry letter of the scale, whereby we would modify any concern only if at least two experts voiced such a concern. The results revealed the majority of items attained 3–4 points. The scale-level CVI reached 0.984, and the CVI for each item was reportedly higher than 0.78, suggesting a satisfactory degree of content validity for the measurement. Both factor analysis and structural equation modeling confirmed the construct validity in the study. Exploratory factor analysis suggested that the extracted three principal components were theoretically equivalent to the initial AMPS structure, accounting for 67.374% of all variance, providing appropriate indices for analyzing the validity of this scale. There were good corresponding relations between Items 1–14 and the expected dimension. Item-15 (“see alternate views of a situation”) can correspond to either factor-2 (Positive Emotion Regulation) or factor-3 (Decentering). This is probably since Chinese people often use the strategy of “look at problems from different angles” to deal with disadvantageous things. By finding the positive aspects in the adverse environment, they change their self-awareness and enhance their positive emotions. However, mindfulness is about attention. We are all mindful to some extent, in each moment. It is an innate capacity. Mindfulness emphasizes simple and efficient routes for cultivating and refining such a capacity and apply it to all aspects of life, not only under adverse circumstances (Kabat-Zinn, 2003). Therefore, According to the professional judgment of its content and factor loading, it was finally included in factor 3.
As an additional study, we conducted CFA to investigate the fit of all three subscales with the overall AMPS structure. The goodness of fit indices in the CFA model was almost achieved, and all fit indices satisfied the standard. Data outcomes of the exploratory/confirmatory factor analyses were consistent; demonstrating the data in our study were consistent with the intrinsic hypothesis. Considering such obtained results, the AMPS consisted of three factors: decentering, positive emotion regulation and negative emotion regulation. It was different from MAAS. The MAAS contained a single factor described as awareness of and attention to the present moment. However, Brown and Ryan found MAAS scores were negatively correlated with negative emotion and positively correlated with psychological wellbeing (Brown and Ryan, 2003), which to some extent supported our findings. Additionally, the decentering dimension was similar to the facets such as “non-judging of inner experience” or “non-reactivity to inner experience” which were presented in other measures (R. A. Baer et al., 2006). This is partly because decentering is identified as an essential component of mindfulness. Our three-factor model is consistent with the original scale model, indicating the Chinese AMPS to have appropriate construct validity. Studies have shown that mindfulness may enable a practitioner to recognize that his/her thoughts might not always be true and that the self might not be consistent with mental experience. Consequently, he/she could apply increasingly accurate situational appraisals, reducing bias caused by cognitive distortions (Mathews and MacLeod, 2005). Simultaneously, modern psychological theories hold that mindfulness can promote positive emotional status. Similarly, Buddhist academics endorsed using mindfulness for promoting a “cultivation of happiness, the genuine inner transformation by deliberately selecting and focusing on positive mental states” (Garland et al., 2010). Furthermore, when facing negative emotions sparked by stressful events, practitioners may use mindfulness to calm themselves down and thereby rein the impulse to react negatively when under stress (Jain et al., 2007). These results also provide a theoretical basis for the construction of the three-factor model of AMPS.
We present the first Chinese version of the AMPS to be developed and psychometrically evaluated. The newly developed Chinese version of AMPS is concise and is a user-centered tool for self-reporting. This scale was designated as easy for users to complete and required minimal/no explanation from the investigator. Completion of the questionnaire took less than 10 min (mean timeframe). Compared with other instruments for measuring mindfulness, AMPS is a process analysis tool that can be adept for use in MBI trials, and can be employed to ascertain how mindfulness will be applied to various therapeutic processes and predict a range of clinical outcomes.
Limitations
Although the result of the cross-cultural adaption of the AMPS is satisfied, a few limitations were present. Firstly, participants were gathered through convenience sampling in Northwest China, which may have impacted the generalizability of the findings to some degree. However, the sample in our study had a broad range of education levels, employment status, and age range, suggesting that AMPS is understandable and acceptable by the general Chinese population. Secondly, the study did not measure the criterion validity. A psychometric evaluation of AMPS concerning criterion validity should be taken into consideration within future validation studies.
Conclusion
The Chinese version of AMPS is expressly developed as a process measure to assess how individuals employ mindfulness for MBIs or within daily life. It has important value and can be easily implemented. Our results indicated that the Chinese version of AMPS is a reliable and valid instrument and may thus be used as a process measure to evaluate the application of mindfulness practice in the Chinese context.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Statements
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committees of Xi’an Jiaotong University. The patients/participants provided their written informed consent to participate in this study.
Author contributions
Y-PZ and YJ performed the study design and manuscript preparation. YJ and YY performed the data collection and analysis. W-XS, GM, and XZ drafted and edited the manuscript. All authors read and approved the final manuscript.
Funding
This work was partly supported by the grants from Shaanxi Province (SGH140537) and Xi’an Jiaotong University Fund.
Acknowledgments
We thank all participants who voluntarily contributed to this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2022.848787/full#supplementary-material
References
1
BaerR. A.SmithG. T.AllenK. B. (2004). Assessment of mindfulness by self-report: the Kentucky inventory of mindfulness skills.Assessment11191–206. 10.1177/1073191104268029
2
BaerR. A.SmithG. T.HopkinsJ.KrietemeyerJ.ToneyL. (2006). Using self-report assessment methods to explore facets of mindfulness.Assessment1327–45. 10.1177/1073191105283504
3
Batista-FoguetJ. M.CoendersG.AlonsoJ. (2004). [Confirmatory factor analysis. Its role on the validation of health related questionnaires].Med. Clin.122(Suppl. 1) 21–27. 10.1157/13057542
4
BeatonD. E.BombardierC.GuilleminF.FerrazM. B. (2000). Guidelines for the process of cross-cultural adaptation of self-report measures.Spine (Phila Pa 1976)253186–3191. 10.1097/00007632-200012150-00014
5
BrislinR. W. (1970). Back-translation for cross-cultural research.J. Cross Cult. Psychol.1185–216. 10.1177/135910457000100301
6
BrownK. W.RyanR. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being.J. Pers. Soc. Psychol.84822–848.
7
BrownK. W.RyanR. M.CreswellJ. D. (2007). Mindfulness: theoretical foundations and evidence for its salutary effects.Psychol. Inq.18211–237. 10.1080/10478400701598298
8
BullisJ. R.BøeH. J.AsnaaniA.HofmannS. G. (2014). The benefits of being mindful: trait mindfulness predicts less stress reactivity to suppression.J. Behav. Ther. Exp. Psychiatry4557–66. 10.1016/j.jbtep.2013.07.006
9
ChavanceM. (2008). A review of: “quality of life: the assessment. analysis and interpretation of patient-reported outcomes, second edition, by P. M. Fayers and D. Machin”.J. Biopharm. Stat.18399–401. 10.1080/10543400701697265
10
ChenS. Y.ZhouR. L. (2013). Validation of a Chinese version of the Freiburg mindfulness inventory–short version.Mindfulness5529–535.
11
ChenS. Y.CuiH.ZhouR. L. (2012). Revision of mindful attention awareness scale (MAAS).Chin. J. Clin. Psychol.20148–151. 10.16128/j.cnki.1005-3611.2012.02.024
12
ChiesaA.SerrettiA. (2009). Mindfulness-based stress reduction for stress management in healthy people: a review and meta-analysis.J. Altern. Complement. Med.15593–600. 10.1089/acm.2008.0495
13
ChiesaA.AnselmiR.SerrettiA. (2014). Psychological mechanisms of mindfulness-based interventions: what do we know?Holist. Nurs. Pract.28124–148. 10.1097/hnp.0000000000000017
14
CurtissJ.KlemanskiD. H.AndrewsL.ItoM.HofmannS. G. (2017). The conditional process model of mindfulness and emotion regulation: an empirical test.J. Affect. Disord.21293–100. 10.1016/j.jad.2017.01.027
15
EberthJ.SedlmeierP. (2012). The effects of mindfulness meditation: a meta-analysis.Mindfulness3174–189. 10.1007/s12671-012-0101-x
16
ErismanS. M.RoemerL. (2012). A preliminary investigation of the process of mindfulness.Mindfulness330–43. 10.1007/s12671-011-0078-x
17
FeldmanG.HayesA.KumarS.GreesonJ.LaurenceauJ. P. (2007). Mindfulness and emotion regulation: the development and initial validation of the cognitive and affective mindfulness scale-revised (CAMS-R).J. Psychopathol. Behav. Assess.29:177. 10.1007/s12671-021-01784-5
18
GarlandE. L.FredricksonB.KringA. M.JohnsonD. P.MeyerP. S.PennD. L. (2010). Upward spirals of positive emotions counter downward spirals of negativity: insights from the broaden-and-build theory and affective neuroscience on the treatment of emotion dysfunctions and deficits in psychopathology.Clin. Psychol. Rev.30849–864. 10.1016/j.cpr.2010.03.002
19
GiavarinaD. (2015). Understanding Bland Altman analysis.Biochem. Med. (Zagreb)25141–151. 10.11613/bm.2015.015
20
GodfrinK. A.Van HeeringenC. (2010). The effects of mindfulness-based cognitive therapy on recurrence of depressive episodes, mental health and quality of life: a randomized controlled study.Behav. Res. Ther.48738–746. 10.1016/j.brat.2010.04.006
21
GreenS. M.BielingP. J. (2012). Expanding the scope of mindfulness-based cognitive therapy: evidence for effectiveness in a heterogeneous psychiatric sample.Cogn. Behav. Pract.19174–180.
22
GrossmanP.Tiefenthaler-GilmerU.RayszA.KesperU. (2007). Mindfulness training as an intervention for fibromyalgia: evidence of postintervention and 3-year follow-up benefits in well-being.Psychother. Psychosom.76226–233. 10.1159/000101501
23
GuJ.StraussC.BondR.CavanaghK. (2015). How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies.Clin. Psychol. Rev.371–12. 10.1016/j.cpr.2015.01.006
24
HintonD. E.VuthP.HofmannS. G.OttoM. W. (2013). Acceptance and mindfulness techniques as applied to refugee and ethnic minority populations with PTSD: examples from “culturally adapted CBT”.Cogn. Behav. Pract.2033–46. 10.1016/j.cbpra.2011.09.001
25
HofmannS. G.SawyerA. T.WittA. A.OhD. (2010). The effect of mindfulness-based therapy on anxiety and depression: a meta-analytic review.J. Consult. Clin. Psychol.78169–183. 10.1037/a0018555
26
JainS.ShapiroS. L.SwanickS.RoeschS. C.MillsP. J.BellI.et al (2007). A randomized controlled trial of mindfulness meditation versus relaxation training: effects on distress, positive states of mind, rumination, and distraction.Ann. Behav. Med.3311–21. 10.1207/s15324796abm3301_2
27
Kabat-ZinnJ. (2003). Mindfulness-based interventions in context: past, present, and future.Clin. Psychol. Sci. Pract.10144–156.
28
KhouryB.LecomteT.FortinG.MasseM.TherienP.BouchardV.et al (2013). Mindfulness-based therapy: a comprehensive meta-analysis.Clin. Psychol. Rev.33763–771. 10.1016/j.cpr.2013.05.005
29
KuykenW.ByfordS.TaylorR. S.WatkinsE. R.TeasdaleJ. D. (2009). Mindfulness-based cognitive therapy to prevent relapse in recurrent depression.J. Consult. Clin. Psychol.76966–978. 10.1037/a0013786
30
LauM. A.BishopS. R.SegalZ. V.BuisT.AndersonN. D.CarlsonL.et al (2006). The Toronto mindfulness scale: development and validation.J. Clin. Psychol.621445–1467. 10.1002/jclp.20326
31
LedesmaD.KumanoH. (2009). Mindfulness-based stress reduction and cancer: a meta-analysis.Psychooncology18571–579. 10.1002/pon.1400
32
LiM. J.BlackD. S.GarlandE. L. (2016). The applied mindfulness process scale (AMPS): a process measure for evaluating mindfulness-based interventions.Pers. Individ. Dif.936–15. 10.1016/j.paid.2015.10.027
33
MathewsA.MacLeodC. (2005). Cognitive vulnerability to emotional disorders.Annu. Rev. Clin. Psychol.1167–195. 10.1146/annurev.clinpsy.1.102803.143916
34
MengY.MaoK.LiC. (2019). Validation of a short-form five facet mindfulness questionnaire instrument in China.Front. Psychol.10:3031. 10.3389/fpsyg.2019.03031
35
OsburnH. G. (2000). Coefficient alpha and related internal consistency reliability coefficients.Psychol. Methods5343–355. 10.1037/1082-989x.5.3.343
36
PolitD. F.BeckC. T.OwenS. V. (2007). Is the CVI an acceptable indicator of content validity? Appraisal and recommendations.Res. Nurs. Health30459–467. 10.1002/nur.20199
37
PryseY.McdanielA.SchaferJ. (2015). Psychometric analysis of two new scales: the evidence-based practice nursing leadership and work environment scales.Worldviews Evid. Based Nurs.11240–247. 10.1111/wvn.12045
38
Sapountzi-KrepiaD.ZygaS.PrezerakosP.MalliarouM.EfstathiouC.ChristodoulouK.et al (2016). Kuopio university hospital job satisfaction scale (KUHJSS): its validation in the Greek language.J. Nurs. Manag.2513–21. 10.1111/jonm.12418
39
StraussC.CavanaghK.OliverK.PettmanD.LaksJ. (2014). Mindfulness-based interventions for people diagnosed with a current episode of an anxiety or depressive disorder: a meta-analysis of randomised controlled trials.PLoS One9:e96110. 10.1371/journal.pone.0096110
40
TeasdaleJ. D.SegalZ. V.WilliamsJ. M.RidgewayV. A.SoulsbyJ. M.LauM. A. (2000). Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy.J. Consult. Clin. Psychol.68615–623.
41
WalachH.BuchheldN.ButtenmüllerV.KleinknechtN.SchmidtS. (2006). Measuring mindfulness—the Freiburg mindfulness inventory (FMI).Pers. Individ. Dif.401543–1555. 10.1016/j.paid.2005.11.025
42
XuW.JiaK.LiuX.HofmannS. G. (2016). The effects of mindfulness training on emotional health in Chinese long-term male prison inmates.Mindfulness (N Y)71044–1051. 10.1007/s12671-016-0540-x
43
Zhen-qiuS. (2011). Medical Statistics.Beijing: People’s Medical Publishing House.
Summary
Keywords
mindfulness, applied mindfulness process scale, reliability, validity, scale
Citation
Jia Y, Yan Y, Shi W-X, Meng G, Zhuang X and Zhang Y-P (2022) Development of the Applied Mindfulness Process Scale as a Process Evaluation Measure for Mindfulness Practice in a Chinese Context. Front. Psychol. 13:848787. doi: 10.3389/fpsyg.2022.848787
Received
05 January 2022
Accepted
17 February 2022
Published
11 March 2022
Volume
13 - 2022
Edited by
Rebecca Shankland, Lumière University Lyon 2, France
Reviewed by
Emmanuelle Le Barbenchon, Aix-Marseille Université, France; Florence Spitzenstetter, Université de Strasbourg, France
Updates
Copyright
© 2022 Jia, Yan, Shi, Meng, Zhuang and Zhang.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yin-Ping Zhang, cathyzh@mail.xjtu.edu.cn
This article was submitted to Positive Psychology, a section of the journal Frontiers in Psychology
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.