 Maren Nyer1,2*
Maren Nyer1,2* Sofia Montinola3
Sofia Montinola3 Samantha Pegg2,3Yousif Alsaadi3Zainab O. Soetan4Simmie Foster1,2Dustin J. Rabideau4,5Juliana Peacock1Yian Wu1Anna Kinnas1
Samantha Pegg2,3Yousif Alsaadi3Zainab O. Soetan4Simmie Foster1,2Dustin J. Rabideau4,5Juliana Peacock1Yian Wu1Anna Kinnas1 David Mischoulon1,2Louisa G. Sylvia2,3
David Mischoulon1,2Louisa G. Sylvia2,3- 1Depression Clinical and Research Program, Massachusetts General Hospital, Boston, MA, United States
- 2Department of Psychiatry, Harvard Medical School, Boston, MA, United States
- 3Dauten Family Center for Bipolar Treatment Innovation, Massachusetts General Hospital, Boston, MA, United States
- 4Biostatistics, Massachusetts General Hospital, Boston, MA, United States
- 5Department of Medicine, Harvard Medical School, Boston, MA, United States
The present study surveyed predominantly heated yoga users (N = 2,514) from CorePower Yoga, the largest U.S. yoga studio brand, to explore: (1) demographic characteristics and (2) facilitators and barriers to class participation. The sample was predominantly white (78%), at least 4-year college educated (90%), and female (87%). Twenty-three percent of participants (n = 587) self-reported being diagnosed with clinical depression. Most participants practiced yoga several days a week, and for at least 2 years, predominantly heated yoga classes. Out of a list of options, participants selected facilitators to heated yoga practice and barriers to yoga practice. Physical and mental health benefits of heated yoga facilitated their practice, whereas being around others, improved sleep, and reduction of physical pain were ranked as the lowest facilitators. Scheduling and expense related concerns were the highest ranked barriers to yoga classes, while not liking class participants, administrative issues, and discomfort with exercising around others were the lowest ranked barriers. Overall, these barriers and facilitators were generally consistent across subgroups (e.g., age, gender, race, ethnicity). Participants with self-reported diagnosed clinical depression reported improvement in mood as a more important facilitator than improvement in physical health, and barriers were consistent with the general survey population. Further research is needed to characterize facilitators and barriers to practice and strategies for improved usage.
1 Introduction
The rates of individuals practicing yoga in the U.S. are increasing. According to the 2022 National Health Interview Survey (NHIS), which examined trends in complementary medicine use over a 20-year period, the percentage of U.S. adults practicing yoga tripled from 5% in 2002 to 15.8% in 2022 (NCCIH, 2022). In the U.S., heated yoga originated in the 1970s with the introduction of Bikram yoga, a standardized sequence of 26 postures and two breathing exercises practiced in a heated environment (Fish, 2006; Singleton, 2010). After that, other forms of heated yoga were established in the U.S., such as CorePower Yoga, Baptiste Power Yoga, and heated vinyasa flow. To date, there are no known published reports specifically on heated yoga practice rates in the U.S.
In terms of the mental health benefits of heated yoga, studies have shown (1) improvements in self-reported and clinician-rated depressive symptoms in those with depression (Nyer et al., 2019, 2023; La Rocque et al., 2021); (2) reductions in cortisol reactivity and self-reported measures of binge and affective eating in women at risk for obesity-related illness (Hopkins et al., 2016); (3) improvements in wellbeing, life satisfaction, general health, mindfulness, peace of mind, and eudaimonic wellbeing in healthy yoga-naïve adults (Hui et al., 2022); (4) improvements in mindfulness, perceived stress, cardiorespiratory endurance, flexibility, and balance in healthy yoga-naïve adults (Hewett et al., 2011); and (5) improvements in self-efficacy, perceived stress, quality of life, general health, and energy/fatigue in sedentary, stressed adults (Hewett et al., 2018).
Heated yoga may also improve physical health. Heated yoga has been associated with cardiovascular fitness in terms of (1) improving arterial stiffness in overweight/obese participants (Hewett et al., 2018); (2) improving arterial stiffness in young adults (Hunter et al., 2013); and (3) improving vascular endothelial function in middle and older-aged adults (Hunter et al., 2017). Heated yoga in young healthy adults has been associated with improvements in measures of musculoskeletal fitness, such as deadlift strength, lower back/hamstring flexibility, and shoulder flexibility, and modestly decreased body fat compared to controls (Tracy and Hart, 2013). Additionally, heated yoga has been associated with increased aerobic fitness when compared to normal temperature yoga, with some evidence for cellular thermotolerance adaptations (Bourbeau et al., 2021).
These mental and physical health benefits could be related to each of the three main components of heated yoga, namely exercise, heat, and yoga. For example, one study that explored the contribution of yoga when compared to walking for those with depression in a 12-week trial, found that Iyengar yoga was associated with greater mood improvement and reduction in anxiety compared to a metabolically matched walking control condition (Streeter et al., 2010). Heat may also play a unique role; in a study in which heated yoga users performed the same posture sequence in heated and non-heated conditions, only the heated group showed acute IL-6 elevations (Lambert et al., 2020). This could potentially indicate that the heat may be associated with mental health benefits given that acute IL-6 spikes have been linked to antidepressant effects in other contexts [e.g., following whole-body hyperthermia (Flux et al., 2023)]. Finally, in women with depression, both heated yoga and aerobic exercise outperformed a waitlist control condition in reducing depressive symptoms, though the two exercise conditions did not differ from each other likely due to small sample size and limited power (La Rocque et al., 2021).
There remains a lack of targeted research exploring the demographics, practice patterns, and motivations of heated yoga users. This gap is important, as understanding who participates in heated yoga—and why—can inform more accessible and effective interventions. To address this, the present study surveyed the characteristics of predominantly heated yoga users, as well as facilitators and barriers to practice, across CorePower Yoga studios—the largest yoga studio brand in the U.S.
2 Method
2.1 Procedure
All study procedures were approved by the Mass General Brigham Institutional Review Board. An email inviting users of CorePower Yoga to complete a public survey link was distributed through CorePower Yoga's commercial mailing lists on November 21, 2024. The email was sent to a targeted group of users who visited CorePower Yoga studios at least twice in 2024 and had opted into email marketing, which was a total of 225,872 student profiles. Individuals answered screening questions to assess eligibility—i.e., 18 years or older, not currently pregnant, able to read and understand English, and users of CorePower Yoga. Eligible participants were then presented with a brief description of the study, contact information of study staff, and then the survey. The survey was designed to take approximately 5–10 min and consisted of questions related to participant demographics, non-heated and heated yoga experience, whether participants had ever been diagnosed with clinical depression, and facilitators and barriers to practicing classes at CorePower Yoga. Upon completion of the survey, participants were thanked for their time. Participants did not receive compensation for completing the survey. See Supplementary Figure 1 for the full survey questions.
2.2 CorePower Yoga
CorePower Yoga is the largest yoga studio brand (by studio count) in the U.S. with over 220 studios nationwide and offers a range of classes with varying heat, intensity levels, and duration. Its predominant and most popular formats are heated yoga classes and a heated “Yoga Sculpt” class practiced with light weights. The temperatures range from non-heated (residual heat can be present) to 105°F. According to CorePower Yoga, their most popular yoga class is a 60-min heated Power Yoga or “vinyasa” class practiced in 95°F called CorePower 2.
2.3 Data analysis
For the facilitator analysis, participants were analyzed if they provided at least one facilitator. For the barrier analysis, participants were analyzed if they provided at least one facilitator and at least one barrier. Descriptive statistics were reported for participant demographics and yoga experience and preferences, including facilitators and barriers. Participants also chose their top five facilitators out of 9 options (including “other”) to practicing heated yoga. Participants also chose their top five barriers to practicing yoga classes at CorePower Yoga out of 18 options. Facilitators and barriers were ranked by importance (1 = most important facilitator/barrier; 5 = least important facilitator/barrier). Please see Supplementary Figure 1 for the full survey for an exhaustive list of all facilitators and barriers. Facilitators were scored 6—chosen rank (i.e., on a scale from 0 to 5). Specifically, facilitators ranked as most important (i.e., first on the survey) were given the score of 5 for the participant. Facilitators ranked second most important were given the score of 4. This continued to the facilitator ranked least important out of 5 (i.e., their 5th choice), which was given a score of 1. If a participant did not rank a facilitator, the facilitator would get a score of 0. Scores for each facilitator were then averaged across participants. Higher mean scores indicate that more participants ranked that facilitator highly, while lower mean scores indicate that participants ranked the facilitator lower or did not rank the facilitator at all. The same scoring procedure was followed for barriers.
We also examined potential differences in reported facilitators and barriers based on demographic variables, depression diagnosis, years of experience, frequency of yoga practice, and heated vs. non-heated class preference (i.e., those who chose a heated yoga class as their first choice compared to those who chose a non-heated yoga class as their first choice). For some variables, categories were collapsed to examine differences in facilitators and barriers between two groups (see footnote1). We report on the three highest and three lowest ranked facilitators and barriers in these group-specific comparisons.
3 Results
3.1 Demographics
A total of 3,019 respondents were eligible, reviewed the study information sheet, and began the survey. There were 2,514 survey responses from participants who indicated at least one facilitator on the survey and included in study results. Participants were allowed to skip questions, thus, not all questions included responses from all participants. Participant demographics of the 2,514 participant sample are presented in Table 1. The median age of participants was 39 years. Most participants were female (87%) and White (78%). Regarding ethnicity, 11% of participants were Hispanic or Latino/a. Most participants had a household income above $125,000 (53%), were employed full-time (71%), and held a Bachelor's level degree or higher (90%). Regarding depression diagnosis, 23% reported having ever been diagnosed with clinical depression and 74% reported that they had not. Most participants reported practicing yoga (either heated or non-heated) for 5 years or more (64%), practicing more than 2 days per week (55%), and that practicing yoga improves their mental health (98%). Experience with yoga is reported in Table 2. Regarding heated yoga practice preference between heated vs. non-heated yoga, 87% selected a heated yoga class as their first choice of class, and 7% selected a non-heated yoga class as their first choice of class.
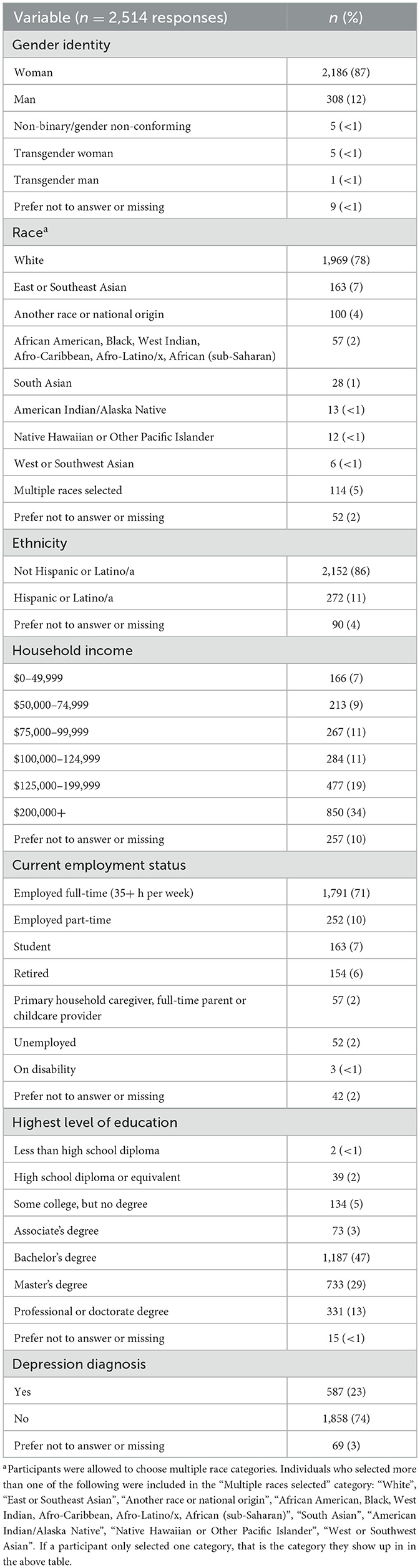
Table 1. Demographics of the sample.
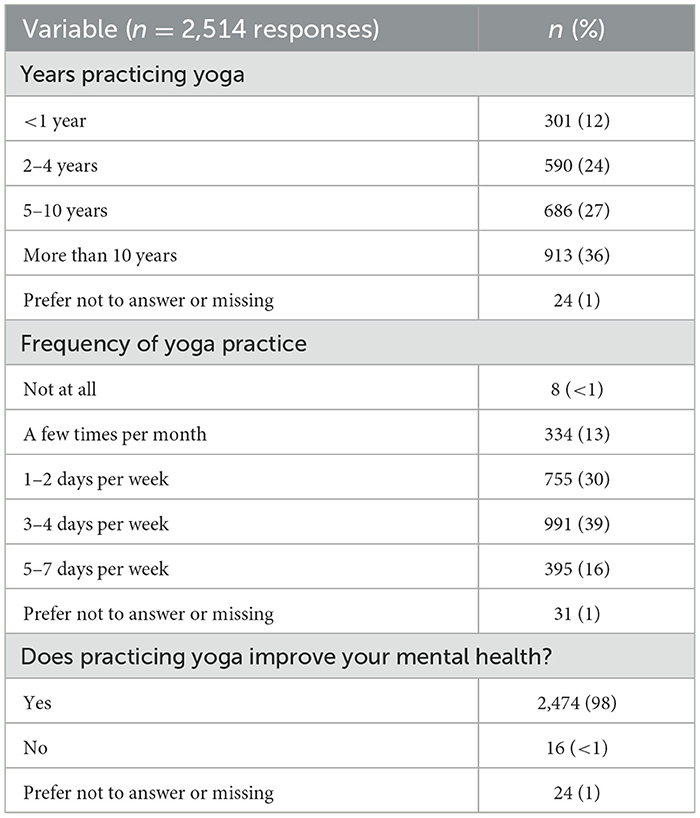
Table 2. Yoga experience of the sample.
3.2 Barriers and facilitators to yoga participation
Ranked facilitators to heated yoga participation and barriers to yoga classes at CorePower Yoga across the sample are presented in Table 3.
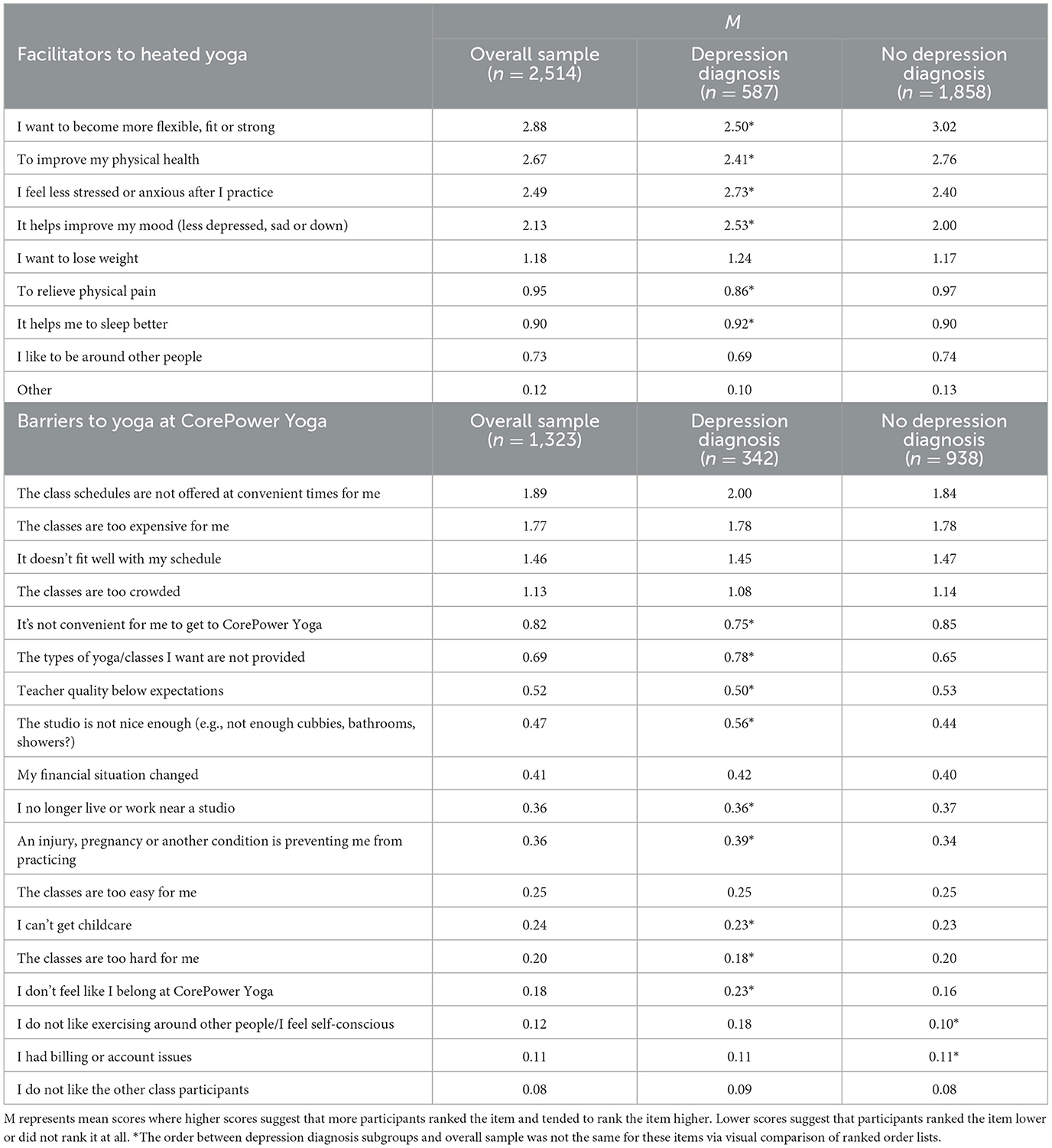
Table 3. Facilitators to heated yoga and barriers to yoga classes at corepower yoga across the sample.
3.2.1 Facilitators
As reported in Table 3, across the sample of 2,514 respondents, the highest three ranked facilitators (in order of highest ranked to lowest ranked) to taking heated yoga classes were: (1) “I want to become more flexible, fit or strong”; (2) “To improve my physical health”; and (3) “I feel less stressed or anxious after I practice”. The three highest ranked facilitators differed for those with a depression diagnosis (n = 587): (1) “I feel less stressed or anxious after I practice”; (2) “It helps improve my mood (less depressed, sad or down)”; and (3) and “I want to become more flexible, fit, or strong” (see Table 3). For participants without a depression diagnosis (n = 1,858), the highest three ranked facilitators and their order did not differ from the overall sample. The highest three ranked facilitators generally did not differ by gender, race, ethnicity, age, income, years of yoga experience, yoga practice frequency, and yoga class preference, although the order varied in some cases.
Across the sample of 2,514 respondents, the lowest three ranked facilitators (in order of least ranked/lowest on the list to higher ranked) (besides an open-ended “other” response) were: (1) “I like to be around other people”; (2) “It helps me sleep better”; and (3) “To relieve physical pain”. These differed by age, years of yoga experience, and yoga class preference. Specifically, the lowest ranked facilitator was “I want to lose weight” for participants who were 39 years or older, those with 5 or more years of yoga experience, and those who preferred non-heated yoga as their first choice (vs. heated yoga classes) (see Table 3). The lowest three ranked facilitators generally did not differ by gender, race, ethnicity, income, yoga practice frequency, and depression diagnosis, although the order varied in some cases.
3.2.2 Barriers
Across the sample of 1,323 respondents included in barrier analyses (i.e., those who provided at least one facilitator and at least one barrier), the highest three ranked barriers (out of the 18 options available) for taking yoga classes at CorePower Yoga were: (1) “The class schedules are not offered at convenient times for me”; (2) “The classes are too expensive for me”; and (3) “It doesn't fit well with my schedule”. These barriers differed by age, income, years of yoga experience, and preference for heated yoga classes. Specifically, the third highest ranked barrier was “The classes are too crowded” for participants younger than 39 years old, with an income less than $125,000, and with less than 5 years of yoga experience. The highest three ranked barriers generally did not differ by gender, race, ethnicity, yoga practice frequency, yoga class preference, and depression diagnosis, although the order varied in some cases (see Table 3).
Across the sample of 1,323 respondents included in barrier analyses, the lowest three ranked barriers (out of the 18 available options; in order of least ranked/lowest on the list to higher ranked) were: (1)“I do not like other class participants”; (2) “I had billing or account issues”; and (3) “I do not like exercising around other people/I feel self-conscious”. These differed by gender, ethnicity, age, income, years of yoga experience, and yoga class preference (see Table 3). Specifically, the third lowest ranked barrier was “I can't get childcare” for men and participants who preferred non-heated yoga as their first choice (vs. heated yoga classes). This barrier was also the second lowest ranked barrier for participants who were younger than 39 years old, had an income less than $125,000, and had less than 5 years of yoga experience. The second lowest ranked barrier was “An injury, pregnancy, or another condition is preventing me from practicing” for participants who identified as Hispanic or Latino/a. The lowest three ranked barriers generally did not differ by race, yoga practice frequency, and depression diagnosis, although the order varied in some cases.
4 Discussion
The present study examined participant demographics, as well as facilitators of and barriers to predominantly heated yoga participation, among users of CorePower Yoga, the largest brand of community-based yoga studios in the U.S. Among the 2,514 participants who ranked at least one facilitator, the majority of respondents (87%) selected a heated yoga class as their first-choice class. This was expected, given that most classes offered at CorePower Yoga are heated.
Regarding demographic characteristics of this predominantly heated yoga sample, the majority of participants were female, white, and highly educated, and reported higher income levels. This is consistent with multiple reports that have demonstrated that the typical yoga users in the U.S. are female, college educated, younger, and white (Birdee et al., 2008; Zhang et al., 2021; Yoga Among Adults Age 18 Older: United States, 2022) and with higher incomes (Cramer et al., 2016). These studies did not differentiate heated and non-heated yoga. The only known larger study of heated yoga (N = 700) that reported on demographic characteristics also reported a predominantly female (60%) and white (78%) sample (Firebaugh and Eggleston, 2017). Our study had a median age of 39 years, and the above study had a similar age range with the average age of 32.6 years (Firebaugh and Eggleston, 2017).
Regarding yoga use, the majority reported practicing yoga for at least 2 years, at least several days per week. Additionally, the email link to the survey was sent to a group of CorePower Yoga users who visited their studios at least twice in the year the survey was distributed. It is possible that within this group that those who care most about their practice at CorePower Yoga were more likely to take the time to fill out this uncompensated survey. Thus, this may not be a complete reflection of the overall populations of yoga users at CorePower Yoga.
Across the general sample, the highest ranked facilitators to participating in heated yoga classes were related to improving physical health and fitness as well as reducing stress or anxiety. These results may suggest that participants are interested in the physical and mental health benefits of heated yoga as described in the literature (Hunter et al., 2016, 2013, 2017; Tracy and Hart, 2013; Lambert et al., 2020; Hewett et al., 2015). These highly ranked facilitators of heated yoga were generally consistent between subgroups of participants, with one notable exception being participants who had been diagnosed with clinical depression. These participants identified reducing stress or anxiety and improving mood as higher ranked facilitators—i.e., mental health facilitators were ranked higher than physical health in the depressed sample when compared to the non-depressed sample. This, too, aligns with previous work identifying psychological benefits of heated yoga for depressive symptoms (Nyer et al., 2019, 2023; La Rocque et al., 2021) and perceived stress and cortisol reactivity in the face of a lab-based stressor (Hopkins et al., 2016).
The lowest ranked facilitators to participating in heated yoga classes (i.e., factors that were ranked the lowest if at all) across the sample were being around others, helping with sleep, and relieving physical pain. This was a surprising finding, as prior literature has shown that heated yoga (Kudesia and Bianchi, 2012), and to a much greater extent non-heated yoga (Turmel et al., 2022; Zhu et al., 2023; Wang et al., 2020; Bankar et al., 2013; Alghosi et al., 2025), may provide benefits for sleep. In addition, non-heated yoga has also been shown to reduce pain in chronic pain conditions (Wren et al., 2011; Büssing et al., 2012; Anheyer et al., 2022). It is possible, given that the study did not specifically recruit a population with physical pain or sleep concerns, that the benefits may not be noticeable for this general population.
The highest ranked barriers to participating in yoga at CorePower Yoga across the sample were related to class scheduling conflicts and expense. These ranked barriers differed slightly for those who were comparatively younger, had lower income, and had less yoga experience. Specifically, these subgroups ranked that the classes were too crowded as a barrier more so than the schedule-related concerns. It is possible that post the COVID-19 pandemic, there are concerns with infection in crowded enclosed spaces. These results highlight the importance of having many classes across different days and times to increase access and reduce crowdedness in classes. In addition, yoga classes are expensive for many. There are many classes available online; however, heated yoga is difficult to do at home without a heated space, and thus, is only accessible to those who live near heated studios. There are no trials to date comparing heated and non-heated yoga directly for mental health benefits. If heated yoga is associated with greater effectiveness in large-scale trials, accessibility for lower income populations and rural populations or those in places without heated yoga studios will need to be considered. For example, if it is determined that there is a need for heated yoga in lower income communities, one option could be that heated yoga could be added to YMCAs or other community centers to increase access. Considerations for making yoga more accessible to lower income populations can include things like location, cost, and childcare (Nagaswami et al., 2024). Additional research is needed to understand who is more likely to attend and benefit from heated yoga.
There are a several limitations of the present study worth noting. Responses were limited to options and questions included in the survey, and participants were not required to answer each question or complete all rankings. While this reduced burden and allowed participants to respond to questions more comfortably, response rates varied across questions. The response rate was particularly low for barriers. This could also be due to the order of survey questions, as barriers were amongst the last questions on the survey, or it is possible that participants may not have identified with the barrier choices listed in the survey and opted not to respond. Since the survey was accessible via a public link, there is the possibility that the same individual could have taken the survey multiple times. However, this is unlikely as there was no renumeration offered for the survey and therefore no benefit to producing multiple entries. The survey did not separate heated and non-heated yoga in some of the questions—e.g., the survey listed facilitators of “heated yoga” and barriers to “yoga”, which was an oversight in survey design. There are likely several sources of selection bias in this data. This is only a survey of CorePower Yoga users and also only a subsample of those who filled out the survey. This means that they are (1) likely highly motivated, and (2) have the time to fill out the survey. The sample had notably higher income, which could suggest that CorePower Yoga serves a higher income population and/or those with higher incomes had more leisure time to participate in the survey. Thus, the information on barriers and benefits of heated yoga may not be generalizable to lower income population. Special considerations may be needed for low-income populations (see Nagaswami et al., 2024 for a review). The participants in the survey also may be more invested in this form of yoga as their survey responses reflected that they practiced yoga for at least 2 years and more than 2 days per week.
Future research using qualitative methods is needed to more fully improve our understanding of participant experiences, including facilitators, barriers, and benefits/risks of practice. Furthermore, participants were all recruited only through CorePower Yoga studios in the U.S., and thus, the sample cannot be considered representative of all yoga users generally in the U.S. Although the sample, and the community from which it was drawn, was quite large and is a strength of this study, we had a low response rate (i.e., < 5% of CorePower Yoga patrons), suggesting possible selection bias. Future research could survey participants from other heated yoga studios outside of the CorePower Yoga network and pay participants to respond, thus improving the generalizability of the sample. Finally, responses were based on self-report, including lifetime clinical depression diagnosis, which would ideally be confirmed via clinician-rated assessment. Larger scale studies with more rigorous diagnostic methods are needed to more fully explore implications of depression and potential influence of comorbidities, such as sleep disorders and chronic pain conditions, in results. Additionally, as this is a group who practices predominantly a relatively rigorous form of heated yoga frequently and for a long period of time, they may be healthier on average than the general population, and as such, heated yoga as an intervention for specific conditions cannot be drawn from this sample.
Despite these limitations, the present study is the first known large-scale survey of predominantly heated-yoga users. As such, it adds to the literature-base in characterizing the sample and also identifies facilitators and barriers for a sample of predominantly heated yoga users. As heated yoga use increases in the U.S., the present study represents a first step in examining experiences and motivations of heated yoga users. Additional research building on this work has the potential to impact the development of interventions using heated yoga to improve physical and mental health.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Mass General Brigham Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants' legal guardians/next of kin because consent was implied by the decision to click on the survey link and complete the survey questions.
Author contributions
MN: Project administration, Resources, Writing – review & editing, Methodology, Conceptualization. SM: Investigation, Data curation, Writing – review & editing, Writing – original draft. SP: Data curation, Writing – original draft, Writing – review & editing. YA: Investigation, Data curation, Writing – review & editing, Writing – original draft. ZS: Formal analysis, Data curation, Writing – review & editing. SF: Methodology, Supervision, Writing – review & editing, Resources. DR: Writing – review & editing, Formal analysis, Data curation. JP: Writing – review & editing. YW: Writing – review & editing. AK: Writing – review & editing. DM: Writing – review & editing, Supervision, Resources. LS: Methodology, Writing – review & editing, Resources, Conceptualization, Project administration.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was partially funded by the Dauten Family Foundation.
Acknowledgments
We thank CorePower Yoga for their collaboration in designing and distributing the survey. We are also grateful to Sarah Choi, Chief Marketing and Commercial Officer at CorePower Yoga, and Karolina Kielbowicz, Vice President of Brand Marketing at CorePower Yoga, for their valuable contributions to survey development and coordination. We are grateful to CorePower Yoga for giving us access to their students for this survey.
Conflict of interest
DM has received research support from Nordic Naturals and Heckel Medizintechnik GmbH. He has received honoraria for speaking from the Massachusetts General Hospital Psychiatry Academy. He also works with the MGH Clinical Trials Network and Institute (CTNI), which has received research funding from multiple pharmaceutical companies and NIMH. LS reports receiving grant funding from PCORI, NIH, HRSA Tiny Blue Dot Foundation and AFSP. She has also received funding as a member of the Milken Institute's Scientific Advisory Board as well as royalties from New Harbinger for her two published books on bipolar disorder. MN reports receiving grant funding from NIH, Osher Center for Integrative Medicine, and the Tiny Blue Dot Foundation.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2025.1655405/full#supplementary-material
Footnotes
1. ^Gender was collapsed into men (including transgender men; facilitator n = 309; barrier n = 122) and women (including transgender women; facilitator n = 2,191; barrier n = 1,194). Race was collapsed into White (facilitator n = 1,969; barrier n = 985) and any other race (facilitator n = 376; barrier n = 238). Ethnicity was defined as Hispanic or Latino/a (facilitator n = 272; barrier n = 158) and not (facilitator n = 2,152; barrier n = 1,122). Age was divided into those who were younger than the median age of 39 (facilitator n = 1,162; barrier n = 718), and those who were at least 39 (facilitator n = 1,263; barrier n = 551). Income was collapsed into annual household income less than $125,000 (facilitator n = 930; barrier n = 551) and at least $125,000 (facilitator n = 1,327; barrier n = 658). Years of yoga practice experience were collapsed into less than 5 years of experience (facilitator n = 891; barrier n = 499) and 5 or more years of experience (facilitator n = 1,599; barrier n = 811). Yoga frequency was divided into 0-2 times per week (facilitator n = 1,097; barrier n = 698) and more than 2 times a week (facilitator n = 1,386; barrier n = 611). Yoga class preference was divided into those who chose heated yoga as their first choice (facilitator n = 2,196; barrier n = 1,126) and those who chose non-heated yoga as their first choice (facilitator n = 182; barrier n = 127). Depression diagnosis history was defined as having a self-reported diagnosis (facilitator n = 587; barrier n = 342) and not (facilitator n = 1,858; barrier n = 938).
References
Alghosi, M., Sharifi, M., Namavari, S., Rajamand, N., Bamorovat, F., Norouzi, N., et al. (2025). The effect of chronic yoga interventions on sleep quality in people with sleep disorders: a scoping review. Front Neurol. 16:1566445. doi: 10.3389/fneur.2025.1566445
Anheyer, D., Haller, H., Lauche, R., Dobos, G., and Cramer, H. (2022). Yoga for treating low back pain: a systematic review and meta-analysis. Pain 163, e504–e517. doi: 10.1097/j.pain.0000000000002416
Bankar, M. A., Chaudhari, S. K., and Chaudhari, K. D. (2013). Impact of long term Yoga practice on sleep quality and quality of life in the elderly. J. Ayurveda Integr. Med. 4, 28–32. doi: 10.4103/0975-9476.109548
Birdee, G. S., Legedza, A. T., Saper, R. B., Bertisch, S. M., Eisenberg, D. M., Phillips, R. S., et al. (2008). Characteristics of yoga users: results of a national survey. J. Gen. Intern. Med. 23, 1653–1658. doi: 10.1007/s11606-008-0735-5
Bourbeau, K. C., Moriarty, T. A., Bellovary, B. N., Bellissimo, G. F., Ducharme, J. B., Haeny, T. J., et al. (2021). Cardiovascular, cellular, and neural adaptations to hot yoga versus normal-temperature yoga. Int. J. Yoga. 14, 115–126. doi: 10.4103/ijoy.IJOY_134_20
Büssing, A., Ostermann, T., Lüdtke, R., and Michalsen, A. (2012). Effects of yoga interventions on pain and pain-associated disability: a meta-analysis. J. Pain 13, 1–9. doi: 10.1016/j.jpain.10, 001.
Cramer, H., Ward, L., Steel, A., Lauche, R., Dobos, G., Zhang, Y., et al. (2016). Prevalence, patterns, and predictors of yoga use: results of a U.S. nationally representative survey. Am. J. Prev. Med. 50, 230–235. doi: 10.1016/j.amepre.2015.07.037
Firebaugh, C. J. M., and Eggleston, B. (2017). Hydration and Hot Yoga: Encouragement, Behaviors, and Outcomes. Int J Yoga. 10, 107. doi: 10.4103/ijoy.IJOY_8_17
Fish, A. (2006). The commodification and exchange of knowledge in the case of transnational commercial yoga. Int. J. Cult. Prop. 13, 189–206. doi: 10.1017/S0940739106060127
Flux, M. C., Smith, D. G., Allen, J. J. B., Mehl, M. R., Medrano, A., Begay, T. K., et al. (2023). Association of plasma cytokines and antidepressant response following mild-intensity whole-body hyperthermia in major depressive disorder. Transl. Psychiatry. 13:132. doi: 10.1038/s41398-023-02402-9
Hewett, Z., Ransdell, L., Gao, Y., Petlichkoff, L., and Lucas, S. (2011). An examination of the effectiveness of an 8-week bikram yoga program on mindfulness, perceived stress, and physical fitness. J. Exerc. Sci. Fit. 9, 87–92. doi: 10.1016/S1728-869X(12)60003-3
Hewett, Z. L., Cheema, B. S., Pumpa, K. L., and Smith, C. A. (2015). The effects of bikram yoga on health: critical review and clinical trial recommendations. Evid. Based Complement. Alternat. Med. 2015:428427. doi: 10.1155/2015/428427
Hewett, Z. L., Pumpa, K. L., Smith, C. A., Fahey, P. P., and Cheema, B. S. (2018). Effect of a 16-week Bikram yoga program on perceived stress, self-efficacy and health-related quality of life in stressed and sedentary adults: a randomised controlled trial. J Sci Med Sport. 21, 352–357. doi: 10.1016/j.jsams.2017.08.006
Hopkins, L. B., Medina, J. L., Baird, S. O., Rosenfield, D., Powers, M. B., Smits, J. A. J., et al. (2016). Heated hatha yoga to target cortisol reactivity to stress and affective eating in women at risk for obesity-related illnesses: A randomized controlled trial. J. Consult. Clin. Psychol. 84, 558–564. doi: 10.1037/ccp0000091
Hui, B. P. H., Parma, L., Kogan, A., and Vuillier, L. (2022). Hot yoga leads to greater well-being: a six-week experience-sampling RCT in healthy adults. Psychosoc Interv. 31, 67–82. doi: 10.5093/pi2022a4
Hunter, S. D., Dhindsa, M. S., Cunningham, E., Tarumi, T., Alkatan, M., Nualnim, N., et al. (2013). The effect of Bikram yoga on arterial stiffness in young and older adults. J Altern Complement Med N Y N. 19, 930–934. doi: 10.1089/acm.2012.0709
Hunter, S. D., Dhindsa, M. S., Cunningham, E., Tarumi, T., Alkatan, M., Nualnim, N., et al. (2016). Impact of hot yoga on arterial stiffness and quality of life in normal and overweight/obese adults. J. Phys. Act. Health. 13, 1360–1363. doi: 10.1123/jpah.2016-0170
Hunter, S. D., Dhindsa, M. S., Cunningham, E., Tarumi, T., Alkatan, M., Nualnim, N., et al. (2017). The effect of Bikram yoga on endothelial function in young and middle-aged and older adults. J. Bodyw. Mov. Ther. 21, 30–34. doi: 10.1016/j.jbmt.2016.06.004
Kudesia, R. S., and Bianchi, M. T. (2012). Decreased nocturnal awakenings in young adults performing bikram yoga: a low-constraint home sleep monitoring study. ISRN Neurol. 2012, 1–7. doi: 10.5402/2012/153745
La Rocque, C. L., Mazurka, R., Stuckless, T. J. R., Pyke, K., and Harkness, K. L. (2021). Randomized controlled trial of bikram yoga and aerobic exercise for depression in women: Efficacy and stress-based mechanisms. J. Affect Disord. 280, 457–66. doi: 10.1016/j.jad.10.067
Lambert, B. S., Miller, K. E., Delgado, D. A., Chaliki, K., Lee, J., Bauza, G., et al. (2020). Acute physiologic effects of performing yoga in the heat on energy expenditure, range of motion, and inflammatory biomarkers. Int. J. Exerc. Sci. 13, 802–817. doi: 10.70252/AKMZ9424
Nagaswami, M. V., Saper, R. B., Streeter, C. C., Uebelacker, L., Ding, G., Dalvie, A., et al. (2024). Yoga-based interventions in low-income populations: a scoping review. J. Integr. Complement. Med. 30, 735–752. doi: 10.1089/jicm.2023.0479
NCCIH (2022). National Health Interview Survey. Available online at: https://www.nccih.nih.gov/research/national-health-interview-survey-2022 (Accessed 14 April, 2025)
Nyer, M., Hopkins, L. B., Farabaugh, A., Nauphal, M., Parkin, S., McKee, M. M., et al. (2019). Community-delivered heated hatha yoga as a treatment for depressive symptoms: an uncontrolled pilot study. J. Altern. Complement Med. N Y N. 25, 814–823. doi: 10.1089/acm.2018.0365
Nyer, M. B., Hopkins, L. B., Nagaswami, M., Norton, R., Streeter, C. C., Hoeppner, B. B., et al. (2023). A randomized controlled trial of community-delivered heated hatha yoga for moderate-to-severe depression. J. Clin. Psychiatry. 84:14621. doi: 10.4088/JCP.22m14621
Singleton, M. (2010). Yoga Body: The Origins of Modern Posture Practice. Oxford ; New York: Oxford University Press, 272p.
Streeter, C. C., Whitfield, T. H., Owen, L., Rein, T., Karri, S. K., Yakhkind, A., et al. (2010). Effects of yoga versus walking on mood, anxiety, and brain gaba levels: a randomized controlled MRS study. J. Altern. Complement Med. 16, 1145–1152. doi: 10.1089/acm.2010.0007
Tracy, B. L., and Hart, C. E. F. (2013). Bikram yoga training and physical fitness in healthy young adults. J. Strength Cond. Res. 27:822. doi: 10.1519/JSC.0b013e31825c340f
Turmel, D., Carlier, S., Bruyneel, A. V., and Bruyneel, M. (2022). Tailored individual Yoga practice improves sleep quality, fatigue, anxiety, and depression in chronic insomnia disorder. BMC Psychiatry. 22:267. doi: 10.1186/s12888-022-03936-w
Wang, W. L., Chen, K. H., Pan, Y. C., Yang, S. N., and Chan, Y. Y. (2020). The effect of yoga on sleep quality and insomnia in women with sleep problems: a systematic review and meta-analysis. BMC Psychiatry. 20:195. doi: 10.1186/s12888-020-02566-4
Wren, A. A., Wright, M. A., Carson, J. W., and Keefe, F. J. (2011). Yoga for persistent pain: new findings and directions for an ancient practice. Pain. 152, 477–480. doi: 10.1016/j.pain.2010.11.017
Yoga Among Adults Age 18 and Older: United States (2022). Available online at: https://stacks.cdc.gov/view/cdc/156474 (Accessed 10 April, 2025)
Zhang, Y., Lauche, R., Cramer, H., Munk, N., and Dennis, J. A. (2021). Increasing trend of yoga practice among U.S. adults from 2002 to 2017. J. Altern. Complement Med. N Y N. 27, 778–85. doi: 10.1089/acm.2020.0506
Keywords: yoga, heated yoga, survey, depression, facilitators, barriers, mental health
Citation: Nyer M, Montinola S, Pegg S, Alsaadi Y, Soetan ZO, Foster S, Rabideau DJ, Peacock J, Wu Y, Kinnas A, Mischoulon D and Sylvia LG (2025) Demographics, facilitators, and barriers among predominantly heated yoga users: a survey of the largest U.S. yoga studio brand. Front. Psychol. 16:1655405. doi: 10.3389/fpsyg.2025.1655405
Received: 27 June 2025; Accepted: 30 September 2025;
Published: 04 November 2025.
Edited by:
R. K. Roshni Raj Lakshmi, Manipur University, IndiaReviewed by:
Apar Avinash Saoji, Swami Vivekananda Yoga Anusandhana Samsthana, IndiaSally Sherman, University of Pittsburgh, United States
Copyright © 2025 Nyer, Montinola, Pegg, Alsaadi, Soetan, Foster, Rabideau, Peacock, Wu, Kinnas, Mischoulon and Sylvia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maren Nyer, bW55ZXJAbWdoLmhhcnZhcmQuZWR1