Abstract
Objectives:
To identify latent profiles and influencing factors of toxic leadership behaviors of nurse managers experienced by staff nurses.
Design:
Cross-sectional study.
Setting:
A total of 12 public hospitals in Guiyang and Zunyi city, Guizhou Province, China.
Methods:
From May 7, 2024 to December 31, 2024, a total of 900 nurses participated, and 868 valid questionnaires were collected with a validity rate of 96.44%. Data was collected via the Toxic Leadership Behaviors of Nurse Managers scale and a demographic questionnaire. Using latent profile analysis (LPA), distinct profiles of toxic leadership behaviors among nurse managers were identified. Univariate and multiple logistic regression analyses were performed to identify the factors associated with the toxic leadership behavior of nurse managers.
Results:
The toxic leadership behaviors suffered by nurses were divided into four profiles: low toxic leadership behavior group (55.07%), moderate toxic leadership behavior group (16.71%), high toxic leadership behavior group (13.36%), and high Intemperate behavior group (14.86%). The results of multiple logistic regression analysis showed that nurses who are male, employed as non-permanent staff, or working in general hospitals are more susceptible to toxic leadership behaviors.
Conclusions:
This study used latent profile analysis to identify four distinct subgroups and found that male nurses, non-permanent staff, and nurses in general hospitals are more susceptible to toxic leadership behaviors. These results emphasize the need for developing strategies to address toxic leadership behaviors in order to promote nurses' wellbeing.
Introduction
As the coordinator of the nursing team, nursing managers should create a favorable professional environment for nurses by making sound management decisions and effectively allocating resources (Alanazi et al., 2023). The effective performance of these important management functions depends on the pattern of leadership behaviors adopted by managers. Leadership behaviors of nurse managers have a profound impact on nursing team effectiveness, staff wellbeing, and quality of patient care (Zhou et al., 2024). In recent years, as healthcare environments grow increasingly complex and nursing workloads intensify, toxic leadership has emerged as a critical issue (Labrague, 2021; Özkan et al., 2022).
Toxic leadership is a negative style that usually manifests itself in the form of demeaning, jealous, authoritarian, intimidating, and manipulative subordinates, which can be harmful to employees and organizations (The Lancet, 2019; Yang et al., 2020). Labrague et al. (2020) categorized toxic leadership behaviors of nurse managers into intemperate behavior, narcissistic behavior, self-promoting behavior, and humiliating behavior. A qualitative study (Guo et al., 2022) further revealed specific manifestations such as negative feedback, neglecting subordinates, unfair treatment, self-centeredness, excessive pressure, and inaction. These behaviors may negatively impact nursing teams in multiple ways, including reduced job satisfaction, heightened professional burnout, increased turnover intentions, and nursing human resource attrition (Ofei et al., 2023). They may also foster organizational silence and deteriorate departmental morale (Hossny et al., 2023). According to a systematic review (Labrague, 2023), toxic leadership can trigger a chain of detrimental effects. It heightens nurses' organizational alienation, impairs their mental health, and diminishes work efficiency, ultimately jeopardizing patient clinical outcomes. Therefore, toxic leadership behaviors are not only detrimental to the psychological health of nurses, but also pose a threat to the quality of service and patient safety in healthcare organizations.
In the field of nursing management, research on leadership behaviors has undergone a more pronounced evolution. Early nursing leadership research centered on positive models like transformational and servant leadership, highlighting how leaders enhance team performance through motivation and personalized care (Wang et al., 2019; Yang et al., 2019). However, with the paradigm shift from positive to negative behavioral research, scholars have begun to focus on the phenomenon of negative leadership in the workplace. The high-intensity and emotionally charged nature of nursing may lead managers to adopt aggressive measures, underscoring the necessity of this research shift.
Currently, most of the research on toxic leadership behavior is concentrated in Western countries, focusing on its formation mechanisms and negative impacts. Estes (2013) surveyed 6,500 nurses in the United States found that 46.6% indicated that they had experienced toxic leadership behaviors by nurse leaders. Results of a survey of 943 nurses from a multi-center in Ghana revealed that nurses perceived toxic leadership behaviors of nurse managers at a moderate level (Ofei et al., 2022). In addition, several studies have found that nurse managers' toxic leadership behaviors can reduce nurses' work engagement and organizational performance levels, and increase nurses' propensity to leave and job stress (Semedo et al., 2022; Ahmed et al., 2024). There are fewer studies on toxic leadership behaviors in China. Zheng et al. (2024) investigated 1,310 nurses and concluded that toxic leadership behaviors of nurse managers can have a negative impact on clinical nurses' work engagement. Another survey (Yao et al., 2023) showed that 43.71% of nurses believed that nurse managers had mild toxic leadership behavior, suggesting that some nurses in China also faced the status quo of toxic leadership behavior.
The toxic leadership behaviors of nurse managers scale (ToxBH-NM) has been applied across regions, and currently stands as the sole instrument (Labrague et al., 2020). Despite advances in toxic leadership research, most scholars treat it solely as a continuous variable, overlooking potential qualitative differences and subgroup characteristics. In addition, research on the heterogeneity of exposure to toxic leadership behaviors across different nursing populations remains severely inadequate. These limitations not only constrain our deep understanding of toxic leadership behaviors but also hinder the development of targeted intervention measures.
Latent Profile Analysis (LPA) is a person-centered approach that uses model fitting to categorize individuals into unobserved (latent) subgroups based on their responses to a set of observed variables (Yang et al., 2022). Traditional clustering methods rigidly partition samples and rely on metrics like scatter plots and contour coefficients for model selection, resulting in inconsistent standards. In contrast, LPA emphasizes membership probabilities, transcending simple data grouping. It provides fit indices based on statistical tests to select appropriate models (Liu et al., 2022). This ultimately achieves grouping effects characterized by intergroup heterogeneity and intragroup homogeneity. It also exhibits high correlation with the precise identification of subgroup characteristics within distinct feature groups. This method aids in revealing qualitative differences and distribution patterns of toxic leadership behaviors within nursing contexts. It also enables in-depth analysis of the “targeted” patterns of toxic leadership behaviors and their underlying formation mechanisms.
In summary, exploring the group heterogeneity of toxic leadership behaviors among nursing managers holds significant value. Therefore, this study aimed to identify subgroups of toxic leadership behaviors among nursing managers, and investigate their influencing factors.
Methods
Design
An online survey was employed in this cross-sectional study to collect relevant data from the target population. Convenience sampling was utilized as the sampling method, aiming to enhance the feasibility and efficiency of the research by allowing access to readily available participants under limited resources. This study was designed and reported in accordance with the guidelines for Strengthening the Reporting of Observational Studies in Epidemiology (von Elm et al., 2014).
Sample size estimation
Latent profile analysis (LPA) requires a sample size of 500 cases, therefore the minimum sample size for this study was 500 (Kassab et al., 2023).
Participants
From May to December 2024, nurses in Guiyang City and Zunyi City, Guizhou Province were invited to conduct the survey. Inclusion criteria: age ≥ 18 years; ≥1 year in nursing; full-time registered nurses; informed consent to this survey and signed an informed consent form. Exclusion criteria: further training, regulation training or internship nurses.
Measurements
Demographic and sociological information
A general information questionnaire was developed by the researchers, including basic demographic data such as age, gender, education level, professional title, employment types, nursing experience, hospital types, and department.
Toxic leadership behaviors of nurse managers scale (ToxBH-NM)
The scale was developed by Labrague et al. (2020). This study used the Chinese version translated by Yao et al. (2023), which was tested for reliability and validity and culturally debugged in China, and has good reliability and validity. The scale includes four dimensions of intemperate behavior, narcissistic behavior, self-promoting behavior, and humiliating behavior. This scale consists a total of 30 items. For the Chinese version of the scale, the Cronbach's α, split-half reliability, and test-retest reliability coefficients were 0.951, 0.831, and 0.959, respectively. The total score ranges from 30 to 150 points, with higher scores indicating more severe toxic leadership behaviors.
Data collection
Wenjuanxing (www.wjx.cn) was used to develop a web-based questionnaire and two researchers reviewed the online questionnaire for rigor. We also created a poster to display the link and QR code, on which the inclusion and exclusion of the population in this study was clearly indicated. We distributed the questionnaire within Guiyang City and Zunyi City. The researcher contacted general nurses to distribute the questionnaires. WeChat was used to send posters and information letters. Participants could access and complete the survey by clicking a link or scanning a QR code. Once submitted, their responses were directly returned to the web page. After the data collection period, two researchers manually reviewed all responses to exclude invalid questionnaires.
Statistical analyses
Mplus 8.3 software was used for LPA to test the model fitness by gradually increasing the profiles based on the fit index. The following fit indices were employed to evaluate the models: Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and adjusted BIC (aBIC). For these indices, smaller values indicate a better model fit. Additionally, entropy was used to assess classification accuracy. It ranges from 0 to 1, with values closer to 1 representing higher accuracy. Lo-mendell-rubin likelihood ratio test (LMRT) and Bootstrapped likeli-hood ratio test (BLRT) are used to evaluate model fit, with a significant P-value (P < 0.05) suggesting that the k-class model fits better than the (k-1)-class model. Although these evaluation indices provide a reference for profile decision-making, the interpretability and theoretical justification of each profile should also be considered when determining the best model.
Data were statistically analyzed using SPSS29.0 software. Count data were expressed as frequencies and percentages or percentages, and comparisons between groups were made using chi-square test or rank-sum test. A multiple logistic regression was performed with the LPA classification as the dependent variable and the variables significant in univariate analysis as independent variables. The significance threshold was set at α = 0.05.
Ethics considerations
The Ethics Committee of the Third Affiliated Hospital of Zunyi Medical University approved this study (2024-1-746). Informed consent was obtained from all participants after disclosure of the study's purpose. Participation was voluntary, with immediate termination of data collection upon refusal. Anonymity is guaranteed through aggregated reporting of results.
Results
Common method bias test
Since the research data is self-reported, common method bias may exist. During the survey process, we emphasized the anonymity and confidentiality of the questionnaire. We explicitly stated that the data would be used solely for academic research to minimize sources of common method bias. Additionally, the Harman single-factor test was employed to assess common method bias. Results revealed three unrotated factor loadings exceeding 1. The first factor explained 33.382% of variance (<40%), indicating that common method bias does not constitute a significant issue.
Demographic characteristics
A total of 900 nurses were invited to participate in the survey, 9 refused, 15 filled out incorrectly, 8 filled out incomplete. Finally, 868 valid questionnaires were recovered, with an effective recovery rate of 96.44%. The ages of the 868 nurses were categorized into four groups: 18–25 (n = 58), 26–35 (n = 633), 36–45 (n = 154), and ≥46 (n = 23). Of the participants, 51 (5.9%) were male and 817 (94.1%) were female.
Model fit indices of LPA
A model-fitting analysis was conducted to estimate profiles of nurses' toxic leadership, based on the dimension scores of the Chinese version of the ToxBH-NM. In this study, the model was fitted and estimated from an initial latent profile model, and then the number of profiles was gradually increased to determine the optimal model. Table 1 shows the fit indices of the latent profile models with different numbers of profiles. As the number of profiles increases, the values of AIC, BIC and aBIC decrease, indicating that the latent profile model is becoming more optimized. The Class 4 model demonstrated the highest classification accuracy, with a maximum entropy value of 0.925. Furthermore, the number of nurses in each of the four classes was 478, 145, 116, and 129, all of which exceeded the recommended threshold of 5% of the total sample size. Based on a comprehensive evaluation of the model fit indices, theoretical justification, and practical interpretability, the Class 4 model was selected as the optimal solution. To test the sensitivity of the results, a separate LPA was conducted on the female subgroup. The results also supported the previously identified Class 4 model (see Table A1). Consequently, the Class 4 model was selected as the final model for this study.
Table 1
| Model | AIC | BIC | aBIC | Entropy | LMRT (P) | BLRT (P) | Category probability |
|---|---|---|---|---|---|---|---|
| 1 | 22778.316 | 22816.445 | 22791.039 | – | – | – | 1 |
| 2 | 21711.942 | 21773.902 | 21732.618 | 0.920 | <0.001 | <0.001 | 0.692/0.308 |
| 3 | 21497.841 | 21583.632 | 21526.469 | 0.828 | 0.0001 | <0.001 | 0.215/0.522/0.263 |
| 4 | 21174.237 | 21283.860 | 21210.817 | 0.925 | <0.001 | <0.001 | 0.551/0.134/0.167/0.149 |
| 5 | 21105.415 | 21238.868 | 21149.947 | 0.861 | 0.0156 | <0.001 | 0.454/0.122/0.134/0.132/0.158 |
Fit statistics for profile structure (n = 868).
AIC, Akaike Information Criterion; BIC, Bayesian Information Criterion; aBIC, adjusted BIC; LMRT, Lo Mendell-Ruben adjusted likelihood ratio test; BLRT, bootstrap likelihood ratio test.
The scale and dimension scores of different profiles
Based on the LPA results, this study identified four distinct profiles of nurses' exposure to toxic leadership behaviors by nurse managers. Profile 1 (C1) was labeled the “Low Toxic Leadership Behavior Group.” Nurses in this profile scored low across all dimensions of toxic leadership, with a total score of 50 (42, 68). This group comprised 478 nurses, accounting for 55.07% of the total sample. Profile 2 (C2) was categorized as the “Moderate Toxic Leadership Behavior Group,” with a total score of 80 (61, 96). It included 145 nurses, representing 16.71% of the sample. Profile 3 (C3) was identified as the “High Toxic Leadership Behavior Group,” exhibiting a high total score of 106 (95, 116). This group consisted of 116 nurses, making up 13.36% of the sample. Profile 4 (C4) was termed the “High Intemperate Behavior Group,” characterized by high scores specifically on the Intemperate Behavior dimension and low scores on all other dimensions. It contained 129 nurses, accounting for 14.86% of the total sample. The LPA results is presented in Figure 1.
Figure 1
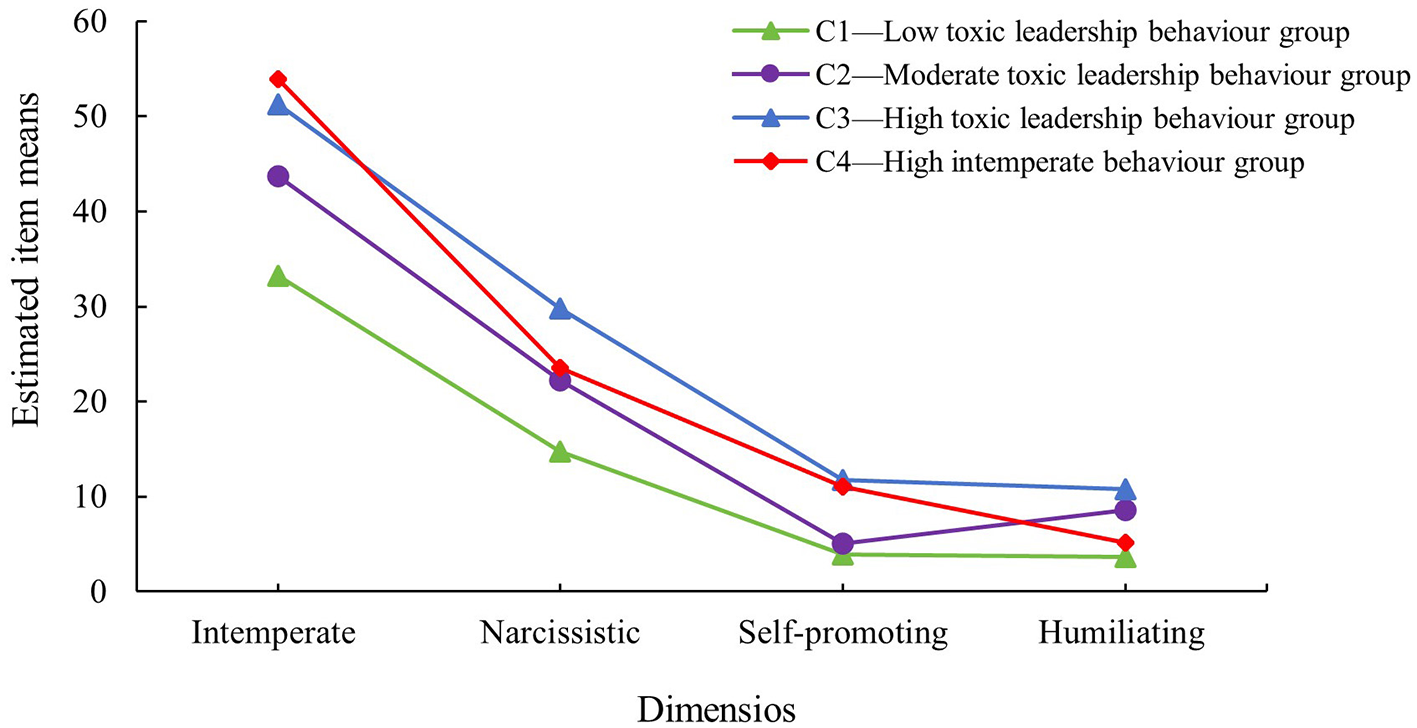
Latent profiles of toxic leadership behaviors of nurse managers.
Demographic and related characteristics of each profile
Following the identification of distinct nurse profiles via LPA, chi-square tests were used to assess for significant differences in demographic characteristics across the profiles. The results revealed statistically significant differences in gender, employment type, hospital type, and department across the profiles. The remaining variables did not show significant associations. The results are presented in the Table 2.
Table 2
| Variables | Lowly toxic leadership behavior group (n = 478) | Moderately toxic leadership behavior group (n = 145) | Highly toxic leadership behavior group (n = 116) | Highly intemperate behavior group (n = 129) | χ2 | P value |
|---|---|---|---|---|---|---|
| Age | 6.524 | 0.687 | ||||
| 18–25 | 32 (6.69) | 8 (5.52) | 13 (11.21) | 5 (3.88) | ||
| 26–35 | 345 (72.18) | 109 (75.17) | 82 (70.69) | 97 (75.19) | ||
| 36–45 | 88 (18.41) | 24 (16.55) | 19 (16.38) | 23 (17.83) | ||
| 46~ | 13 (2.72) | 4 (2.76) | 2 (1.72) | 4 (3.10) | ||
| Gender | 12.608 | 0.006 | ||||
| Male | 17 (3.56) | 14 (9.66) | 12 (10.34) | 8 (6.20) | ||
| Female | 461 (96.44) | 131 (90.34) | 104 (89.66) | 121 (93.80) | ||
| Education | 1.192 | 0.755 | ||||
| College diploma | 94 (19.67) | 28 (19.31) | 26 (22.41) | 30 (23.26) | ||
| Bachelor's degree and above | 384 (80.33) | 117 (80.69) | 90 (77.59) | 99 (76.74) | ||
| Professional title | 11.898 | 0.064 | ||||
| Junior-level | 304 (63.60) | 87 (60.00) | 75 (64.66) | 77 (59.69) | ||
| Intermediate-level | 164 (34.31) | 48 (33.10) | 39 (33.62) | 44 (34.11) | ||
| Senior-level | 10 (2.09) | 10 (6.90) | 2 (1.72) | 8 (6.20) | ||
| Employment types | 27.928 | <0.001 | ||||
| Non-permanent staff | 319 (66.74) | 114 (78.62) | 104 (89.66) | 94 (72.87) | ||
| Permanent employee | 159 (33.26) | 31 (21.38) | 12 (10.34) | 35 (27.13) | ||
| Nursing experience (years) | 19.046 | 0.087 | ||||
| <5 | 87 (18.20) | 26 (17.93) | 15 (12.93) | 27 (20.93) | ||
| 5–10 | 196 (41.00) | 73 (50.34) | 51 (43.97) | 52 (40.31) | ||
| 10–15 | 151 (31.59) | 37 (25.52) | 40 (34.48) | 32 (24.81) | ||
| 15–20 | 27 (5.65) | 1 (0.69) | 6 (5.17) | 8 (6.20) | ||
| 20~ | 17 (3.56) | 8 (5.52) | 4 (3.45) | 10 (7.75) | ||
| Hospital types | 44.789 | <0.001 | ||||
| General hospital | 367 (76.78) | 136 (93.79) | 106 (91.38) | 122 (94.57) | ||
| Specialty hospital | 111 (23.22) | 9 (6.21) | 10 (8.62) | 7 (5.43) | ||
| Department | 51.264 | <0.001 | ||||
| Internal medicine system | 133 (27.82) | 57 (39.31) | 31 (26.72) | 26 (20.16) | ||
| Surgical system | 131 (27.41) | 29 (20.00) | 41 (35.34) | 33 (25.58) | ||
| Gynecology and obstetrics system | 45 (9.41) | 10 (6.90) | 10 (8.62) | 16 (12.40) | ||
| Pediatric system | 41 (8.58) | 17 (11.72) | 9 (7.76) | 20 (15.50) | ||
| Outpatient and emergency system | 38 (7.95) | 15 (10.34) | 18 (15.52) | 10 (7.75) | ||
| Critical care system | 33 (6.90) | 5 (3.45) | 2 (1.72) | 15 (11.63) | ||
| Nursing department | 38 (7.95) | 6 (4.14) | 2 (1.72) | 4 (3.10) | ||
| Function department | 19 (3.97) | 6 (4.14) | 3 (2.59) | 5 (3.88) |
Demographic and related characteristics of each profile (n = 868).
Results of multiple logistic regression analysis
Multiple logistic regression was performed using the four profiles as dependent variables, incorporating the significant univariate predictors of gender, employment type, hospital type, and department. Using C1 as the reference group, the results indicated that nurses who were male, employed as non-permanent staff, and working in general hospitals were more likely to be classified into C2. Similarly, male nurses and those working in general hospitals were more likely to belong to C3. Furthermore, nurses in general hospitals were also more likely to be categorized into C4. The results are presented in the Table 3.
Table 3
| Variables | Class 2 vs. class 1 | Class 3 vs. class 1 | Class 4 vs. class 1 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | OR (95% CI) | P | β | OR (95% CI) | P | β | OR (95% CI) | P | |
| Gender (ref: female) | 1.004 | 2.729 (1.211, 6.148) | 0.015 | 0.892 | 2.440 (1.129, 5.277) | 0.023 | 0.510 | 1.665 (0.679, 4.085) | 0.266 |
| Male | |||||||||
| Employment types (ref: permanent staff) | 1.448 | 4.235 (2.247, 8.050) | <0.001 | 0.638 | 1.893 (1.2, 2.986) | 0.006 | 0.317 | 1.374 (0.877, 2.150) | 0.165 |
| Non-permanent staff | |||||||||
| Hospital types (ref: specialty hospital) | 1.324 | 3.759 (1.828, 7.730) | <0.001 | 1.608 | 4.993 (2.394, 10.414) | <0.001 | 1.832 | 6.246 (2.718, 14.355) | <0.001 |
| General hospital | |||||||||
| Department (ref: function department) | 0.213 | 1.237 (0.333, 4.599) | 0.751 | 0.126 | 1.134 (0.416, 3.09) | 0.805 | −0.470 | 0.625 (0.209, 1.873) | 0.402 |
| Internal medicine system | 0.562 | 1.755 (0.477, 6.451) | 0.397 | −0.479 | 0.620 (0.22, 1.743) | 0.364 | −0.175 | 0.840 (0.284, 2.481) | 0.752 |
| Surgical system | 0.625 | 1.868 (0.442, 7.904) | 0.396 | −0.013 | 0.987 (0.3, 3.245) | 0.983 | 0.651 | 1.917 (0.587, 6.265) | 0.281 |
| Gynecology and obstetrics system | 0.061 | 1.063 (0.249, 4.542) | 0.935 | 0.017 | 1.017 (0.334, 3.097) | 0.976 | 0.360 | 1.433 (0.454, 4.526) | 0.539 |
| Pediatric system | 0.830 | 2.293 (0.577, 9.118) | 0.239 | −0.055 | 0.946 (0.306, 2.927) | 0.924 | −0.283 | 0.753 (0.22, 2.582) | 0.652 |
| Outpatient and emergency system | −1.350 | 0.259 (0.038, 1.755) | 0.167 | −1.139 | 0.320 (0.083, 1.232) | 0.098 | 0.165 | 1.180 (0.36, 3.865) | 0.785 |
| Critical care system | −0.832 | 0.435 (0.065, 2.933) | 0.393 | −0.548 | 0.578 (0.158, 2.113) | 0.407 | −0.848 | 0.428 (0.1, 1.833) | 0.253 |
Results of multiple logistic regression analysis.
Ref, reference.
Discussion
The purpose of this study was to determine the characteristics of toxic leadership behaviors of nurse managers. In this study, we surveyed 868 nurses. The results identified four subgroups, low toxic leadership behavior group, moderate toxic leadership behavior group, high toxic leadership behavior group, and high intemperate behavior group. Our study showed that most of the nurse managers had moderate or low toxic leadership behavior, which is consistent with the results of most studies (Ofei et al., 2022; Yao et al., 2023; Nonehkaran et al., 2023). It is suggested that there is significant heterogeneity in the toxic leadership behaviors suffered by nurses. This heterogeneity may be closely related to nurses' personal characteristics, work environment, and leader characteristics, among others (Labrague et al., 2021; Guo et al., 2023; Farghaly Abdelaliem and Abou Zeid, 2023).
Our study found that male nurses are at higher risk of experiencing toxic leadership behaviors. This finding is highly consistent with Gender Role Theory (GRT; Li et al., 2021). Nursing is often viewed as a “female” profession characterized by empathy and collaboration, which can place male nurses at risk of role conflict for challenging gender norms (Yu et al., 2025). This conflict can be compounded by managerial bias, as some managers may attribute male nurses' career choices to competence issues (Wong et al., 2025), resulting in stricter supervision or negative feedback, aligning with Beck's findings (Baker et al., 2023). In addition, in gender imbalanced workplaces, men are more likely to be “targeted” and their behavioral biases may be amplified (Guy et al., 2022). This cognitive bias may lead to the accumulation of negative evaluations of male nurses by managers, which may eventually evolve into toxic behaviors. Concurrently, establishing male nursing unions or mutual support groups could promote fairness and inclusivity in the workplace environment (Manzi and Heilman, 2021; Morgenroth et al., 2020).
The findings suggest that non-permanent staff nurses are a group that suffers from toxic leadership behaviors. Non-permanent staff nurses lack stable contracts, benefits, and career paths, leading managers to view them as easily replaceable (Galbany-Estragués et al., 2022). This power imbalance can encourage exploitative behaviors. Moreover, Conservation of Resources theory (Bakker and Demerouti, 2024), suggests that these nurses' limited bargaining power forces them to accept unreasonable workloads. The resulting high-pressure environment gradually erodes their willingness to resist, perpetuating a “silence-exploitation” loop (Majeed and Fatima, 2020). The high percentage of non-permanent employee nurses in this study validates this view. This suggests that a more inclusive and equitable nursing workplace ecosystem is still needed to address toxic leadership behaviors (Abdelrahman et al., 2025).
This study revealed that nurses in general hospitals were at significantly higher risk than nurses in specialized hospitals, especially in the group with a high incidence of uncontrolled behavior. This phenomenon stands in stark contrast to the safe, supportive, and empowering work environment advocated by the Magnet Hospital Concept (Yang et al., 2021). General hospitals have high patient flow, frequent examinations of various types, complex interpersonal relationships, and long decision-making chains. Managers under prolonged intense work pressure may resort to unconventional means to maintain work efficiency, which may lead to toxic behaviors, and Sexton's report confirms our findings (Sexton et al., 2022; Beaulieu et al., 2023). Therefore, leveraging the Magnet Hospital initiative's principles flat decision-making structures, open communication cultures, and substantive professional autonomy for nurses can foster a positive atmosphere (Abdelrahman et al., 2025; Harolds and Miller, 2022).
This study examined the relationship between other variables and toxic leadership behavior. First, the findings did not support the predictive role of age and educational attainment on toxic leadership behavior proposed by Guo et al. (2023), suggesting that the explanatory power of these demographic variables may vary across different contexts. Second, neither nurses' professional titles nor work experience significantly influenced toxic leadership behaviors. This indicates that individual-level professional credentials play a limited role in the formation of toxic leadership, suggesting its origins may stem more from organizational environments or leaders' inherent traits. Additionally, department affiliation did not demonstrate significant predictive power in this study, contradicting the findings of Guo et al. (2023). However, the observed distribution differences across departments suggest their potential influence should not be overlooked. These variations may stem from context-specific factors unique to each department, such as distinct work pressures, team cultures, or management styles. Consequently, further studies should aim to disentangle the precise mechanisms through which these factors interact, utilizing more detailed contextual analyses.
This study has some theoretical and practical implications for future research on toxic leadership behavior of nurse managers. First, nurses' gender, employment types and hospital types are the most significant factors affecting nurse managers' toxic leadership behaviors. Meanwhile, we should pay more attention to the degree of influence of these three factors and explore the mechanism of their effects from the theoretical level. Secondly, at the leadership level, hospitals must actively address toxic leadership behaviors faced by clinical nurses by implementing profile-specific countermeasures. This approach is essential for cultivating a healthy work atmosphere and boosting job satisfaction among nurses.
Limitations
This study has several limitations. First, as the sample was recruited from a single province, and using convenience sampling results in a non-representative sample, the findings may lack generalizability to the broader national or global nursing population. Second, the cross-sectional design precludes the establishment of causal relationships. Finally, the use of self-reported data may introduce the potential for response biases.
Conclusion
This study used LPA to identify subgroups of toxic leadership behaviors in nurse managers. The results showed that there were four subgroups: low toxic leadership behavior group, moderate toxic leadership behavior group, high toxic leadership behavior group, and high intemperate behavior group. This study suggests that hospital administrators should pay attention to the prevalence of toxic leadership behaviors among nurse managers. More importantly, targeted interventions based on the distinct profiles identified should be adopted, ultimately fostering a healthier work environment and improving nurse retention.
Statements
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the Third Affiliated Hospital of Zunyi Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
XueyY: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. XuelY: Investigation, Writing – original draft. LT: Investigation, Writing – original draft. HJ: Conceptualization, Formal analysis, Writing – original draft, Writing – review & editing.
Funding
The author(s) declared that financial support was received for this work and/or its publication. This study was supported by Guizhou Provincial Health Commission (gzwkj2023-086).
Conflict of interest
The author(s) declared that this work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declared that generative AI was not used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1
Abdelrahman M. M. Nashwan A. J. El-Boudy D. F. (2025). Nurse managers ‘toxic leadership: its relation to nurses' internal and external intentions to whistleblowing. J. Nurs. Manag.2025:1734502. doi: 10.1155/jonm/1734502
2
Ahmed A. K. Atta M. H. R. El-Monshed A. H. Mohamed A. I. (2024). The effect of toxic leadership on workplace deviance: the mediating effect of emotional exhaustion, and the moderating effect of organizational cynicism. BMC Nurs.23:669. doi: 10.1186/s12912-024-02308-x
3
Alanazi N. H. Alshamlani Y. Baker O. G. (2023). The association between nurse managers' transformational leadership and quality of patient care: a systematic review. Int. Nurs. Rev.70, 175–184. doi: 10.1111/inr.12819
4
Baker M. J. Fisher M. J. Pryor J. (2023). Male nurse practice in inpatient rehabilitation. Finding a safe way: a grounded theory. Int. J. Nurs. Stud.143:104506. doi: 10.1016/j.ijnurstu.2023.104506
5
Bakker A. B. Demerouti E. (2024). Job demands-resources theory: frequently asked questions. J. Occup. Health Psychol.29, 188–200. doi: 10.1037/ocp0000376
6
Beaulieu N. D. Chernew M. E. McWilliams J. M. Landrum M. B. Dalton M. Gu A. Y. et al . (2023). Organization and performance of US health systems. JAMA329, 325–335. doi: 10.1001/jama.2022.24032
7
Estes B. C. (2013). Abusive supervision and nursing performance. Nurs. Forum48, 3–16. doi: 10.1111/nuf.12004
8
Farghaly Abdelaliem S. M. Abou Zeid M. A. G. (2023). The relationship between toxic leadership and organizational performance: the mediating effect of nurses' silence. BMC Nurs.22:4. doi: 10.1186/s12912-022-01167-8
9
Galbany-Estragués P. Millán-Martínez P. Casas-Baroy J. C. Subirana-Casacuberta M. Ramon-Aribau A. (2022). High hiring rate of nurses in Catalonia and the rest of Spain hides precarious employment from 2010 to 2019: a quantitative study. J. Nurs. Manag.30, 1337–1344. doi: 10.1111/jonm.13632
10
Guo X. Li X. Wang Y. Wang Y. Jin H. Xiao F. et al . (2023). Status and influencing factors of nurses' perception of toxic leadership behavior: a cross-sectional study. J. Nurs. Manag.2023:7711237. doi: 10.1155/2023/7711237
11
Guo X. Xiong L. Wang Y. Li X. Wang Y. Xiao F. et al . (2022). Chinese nurses' perceptions on toxic leadership behaviours of nurse managers: a qualitative study. J. Nurs. Manag.30, 3256–3263. doi: 10.1111/jonm.13758
12
Guy M. Hughes K. A. Ferris-Day P. (2022). Lack of awareness of nursing as a career choice for men: a qualitative descriptive study. J. Adv. Nurs.78, 4190–4198. doi: 10.1111/jan.15402
13
Harolds J. A. Miller L. B. (2022). Quality and safety in healthcare, part LXXVI: the value of magnet® hospital recognition. Clin. Nucl. Med.47, e218–e220. doi: 10.1097/RLU.0000000000003223
14
Hossny E. K. Alotaibi H. S. Mahmoud A. M. Elcokany N. M. Seweid M. M. Aldhafeeri N. A. et al . (2023). Influence of nurses' perception of organizational climate and toxic leadership behaviors on intent to stay: a descriptive comparative study. Int. J. Nurs. Stud. Adv.5:100147. doi: 10.1016/j.ijnsa.2023.100147
15
Kassab S. E. Taylor D. Hamdy H. (2023). Student engagement in health professions education: AMEE Guide No. 152. Med. Teach.45, 949–965. doi: 10.1080/0142159X.2022.2137018
16
Labrague L. J. (2021). Influence of nurse managers' toxic leadership behaviours on nurse-reported adverse events and quality of care. J. Nurs. Manag.29, 855–863. doi: 10.1111/jonm.13228
17
Labrague L. J. (2023). Toxic leadership and its relationship with outcomes on the nursing workforce and patient safety: a systematic review. Leadersh. Health Serv.37, 192–214. doi: 10.1108/LHS-06-2023-0047
18
Labrague L. J. Lorica J. Nwafor C. E. Cummings G. G. (2021). Predictors of toxic leadership behaviour among nurse managers: a cross-sectional study. J. Nurs. Manag.29, 165–176. doi: 10.1111/jonm.13130
19
Labrague L. J. Lorica J. Nwafor C. E. van Bogaert P. Cummings G. G. (2020). Development and psychometric testing of the toxic leadership behaviors of nurse managers (ToxBH-NM) scale. J. Nurs. Manag.28, 840–850. doi: 10.1111/jonm.13008
20
Li Y. Mou J. Ye L. Long J. Huang W. W. (2021). An empirical investigation of the utilitarian, social benefits in LBS information disclosure-the moderating effect of the gender based social role theory. Int. J. Inf. Manag.56:102243. doi: 10.1016/j.ijinfomgt.2020.102243
21
Liu F. Yang D. Liu Y. Zhang Q. Chen S. Li W. et al . (2022). Use of latent profile analysis and k-means clustering to identify student anxiety profiles. BMC Psychiatry22:12. doi: 10.1186/s12888-022-04066-z
22
Majeed M. Fatima T. (2020). Impact of exploitative leadership on psychological distress: a study of nurses. J. Nurs. Manag.28, 1713–1724. doi: 10.1111/jonm.13127
23
Manzi F. Heilman M. E. (2021). Breaking the glass ceiling: for one and all?J. Pers. Soc. Psychol.120, 257–277. doi: 10.1037/pspa0000260
24
Morgenroth T. Kirby T. A. Ryan M. K. Sudkämper A. (2020). The who, when, and why of the glass cliff phenomenon: a meta-analysis of appointments to precarious leadership positions. Psychol. Bull.146, 797–829. doi: 10.1037/bul0000234
25
Nonehkaran E. A. Mozaffari N. Iranpour S. Soola A. H. (2023). Identifying the predictors of turnover intention based on nurse managers' toxic leadership behaviors among nurses in Iran: a cross-sectional correlational study. BMC Health Serv. Res.23:1201. doi: 10.1186/s12913-023-10046-0
26
Ofei A. M. A. Paarima Y. Barnes T. Poku C. A. (2022). Toxic leadership behaviour of nurse managers on perceived job satisfaction and productivity of nursing workforce in sub-Saharan Ghana: a multi-centre cross-sectional study. J. Nurs. Manag.30, 2733–2742. doi: 10.1111/jonm.13741
27
Ofei A. M. A. Poku C. A. Paarima Y. Barnes T. Kwashie A. A. (2023). Toxic leadership behaviour of nurse managers and turnover intentions: the mediating role of job satisfaction. BMC Nurs.22:374. doi: 10.1186/s12912-023-01539-8
28
Özkan A. Çamlica T. Kartal H. (2022). An analysis of the effect of nurse managers ‘toxic leadership behaviours on nurses' perceptions of professional values: a cross-sectional survey. J. Nurs. Manag.30, 973–980. doi: 10.1111/jonm.13597
29
Semedo C. S. Salvador A. Dos Santos N. R. Pais L. Mónico L. (2022). Toxic leadership and empowering leadership: relations with work motivation. Psychol. Res. Behav. Manag.15, 1885–1900. doi: 10.2147/PRBM.S340863
30
Sexton J. B. Adair K. C. Proulx J. Profit J. Cui X. Bae J. et al . (2022). Emotional exhaustion among US health care workers before and during the COVID-19 pandemic, 2019-2021. JAMA Netw. Open5:e2232748. doi: 10.1001/jamanetworkopen.2022.32748
31
The Lancet (2019). Silence in the face of abuse of power: UN leadership lacking. Lancet392:2656. doi: 10.1016/S0140-6736(18)33247-1
32
von Elm E. Altman D. G. Egger M. Pocock S. J. Gøtzsche P. C. Vandenbroucke J. P. et al . (2014). The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int. J. Surg.12, 1495–1499. doi: 10.1016/j.ijsu.2014.07.013
33
Wang Y. X. Yang Y. J. Wang Y. Su D. Li S. W. Zhang T. et al . (2019). The mediating role of inclusive leadership: work engagement and innovative behaviour among Chinese head nurses. J. Nurs. Manag.27, 688–696. doi: 10.1111/jonm.12754
34
Wong M. L. L. Koh S. L. S. Teo W. Z. Eng K. W. Shorey S. (2025). Discrimination faced by male nurses and male midwives: a systematic review and meta-synthesis. J. Clin. Nurs.34, 2431–2446. doi: 10.1111/jocn.17679
35
Yang K. Zhou L. Wang Z. Lin C. Luo Z. (2019). Humble leadership and innovative behaviour among Chinese nurses: the mediating role of work engagement. J. Nurs. Manag.27, 1801–1808. doi: 10.1111/jonm.12879
36
Yang L. Q. Zheng X. Liu X. Lu C. Q. Schaubroeck J. M. (2020). Abusive supervision, thwarted belongingness, and workplace safety: a group engagement perspective. J. Appl. Psychol.105, 230–244. doi: 10.1037/apl0000436
37
Yang Q. Zhao A. Lee C. Wang X. Vorderstrasse A. Wolever R. Q. (2022). Latent profile/class analysis identifying differentiated intervention effects. Nurs. Res.71, 394–403. doi: 10.1097/NNR.0000000000000597
38
Yang W. Liu Y. Zeng T. Wang Y. Hao X. Yang W. et al . (2021). Research focus and thematic trends in magnet hospital research: a bibliometric analysis of the global publications. J. Adv. Nurs.77, 2012–2025. doi: 10.1111/jan.14757
39
Yao Q. Wang X. Jiang H. (2023). Translation and reliability test of the toxic leadership behaviour scale for nursing managers. J. Nurs. Sci.38, 80–84. doi: 10.3870/j.issn.1001-4152.2023.18.080
40
Yu H. Y. Tseng I. H. Chin Y. F. Li R. H. Shen Y. C. Lee L. H. et al . (2025). Development and initial validation of a role strain scale for male nursing students. Nurse Educ. Today147:106607. doi: 10.1016/j.nedt.2025.106607
41
Zheng D. Wang Y. Liu N. Ma P. Wu Y. Ma F. (2024). The impact of nursing managers ‘toxic leadership behaviours on clinical nurses' work engagement. J. Nurs. Sci.39, 48–51. doi: 10.3870/j.issn.1001-4152.2024.23.048
42
Zhou Y. Lin J. Liu X. Gao S. Yang F. Xu H. (2024). Validity and reliability of the toxic leadership behaviors of nurse managers scale among Chinese nurses. Front. Psychol.15:1363792. doi: 10.3389/fpsyg.2024.1363792
APPENDIX A
Table A1
| Model | AIC | BIC | aBIC | Entropy | LMR (P) | BLRT (P) | Category probability |
|---|---|---|---|---|---|---|---|
| 1 | 21396.651 | 21434.296 | 21408.891 | – | – | – | 1 |
| 2 | 21404.550 | 20475.723 | 20434.440 | 0.911 | <0.001 | <0.001 | 0.697/0.303 |
| 3 | 20193.517 | 20278.218 | 20221.057 | 0.833 | 0.0001 | 0.0002 | 0.221/0.526/0.253 |
| 4 | 19904.519 | 20012.749 | 19939.710 | 0.925 | <0.001 | <0.001 | 0.152/0.164/0.558/0.127 |
| 5 | 19831.251 | 19963.009 | 19874.092 | 0.864 | 0.0174 | 0.0197 | 0.464/0.125/0.131/0.145/0.136 |
Fit statistics for profile structure of female nurse.
Summary
Keywords
clinical nurse, cross-sectional study, latent profile analysis, nurse managers, toxic leadership behaviors
Citation
Yan X, Yan X, Tan L and Jiang H (2026) Staff nurses' perceptions of toxic leadership behaviors in nurse managers: a latent profile analysis. Front. Psychol. 17:1663057. doi: 10.3389/fpsyg.2026.1663057
Received
10 July 2025
Revised
12 December 2025
Accepted
27 January 2026
Published
18 February 2026
Volume
17 - 2026
Edited by
Luis Felipe Dias Lopes, Federal University of Santa Maria, Brazil
Reviewed by
Yusnaini Yusnaini, Universitas Nurul Hasanah Kutacane, Indonesia
Sisca Mayang Phuspa, Universitas Darussalam Gontor, Indonesia
Updates
Copyright
© 2026 Yan, Yan, Tan and Jiang.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hu Jiang, jianghuchn@163.com
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.