 Slavko Rogan1*
Slavko Rogan1* Jan Taeymans1,2
Jan Taeymans1,2
- 1Department of Health, Discipline of Physiotherapy, Bern University of Applied Sciences, Bern, Switzerland
- 2Faculty of Physical Education and Physiotherapy, Free University of Brussels, Brussels, Belgium
Introduction: Due to demographic changes, falls are increasingly becoming a focus of health care. It is known that within six months after a fall, two thirds of fallers will fall again. Therefore, therapeutic procedures to improve balance that are simple and can be performed in a short time are needed. Stochastic resonance whole-body vibration (SR-WBV) may be such a procedure.
Method: An electronic search to assess the effectiveness of SR-WBV on balance in the elderly was conducted using databases that included CINAHL Cochrane, PEDro, and PubMed. Included studies were assessed using the Collaboration Risk of Bias Tool by two independent reviewers.
Results: Nine studies showing moderate methodological quality were included. Treatment parameters were heterogeneous. Vibration frequency ranged from 1 to 12 Hz. Six studies found statistically significant improvements of balance from baseline to post measurement after SR-WBV interventions. One article found clinical relevance of the improvement in total time of the “Expanded Time to Get Up and Go Test”.
Discussion: Physiological adaptations after balance training are specific and may explain some of the observed heterogeneity. Two out of nine studies assessed reactive balance and both indicated statistically significant improvements after SR-WBV. Therefore, SR-WBV represents a reactive balance training.
Introduction
Ageing is associated with sensorimotor deficits resulting in muscular weakness, mobility issues, balance disorders and in gait disorders, and this leads to falls and reduced independence in everyday life (1). The sensorimotor system constantly and unconsciously regulates its movements and postural control based on perceived information to achieve postural stability. Numerous research studies have assessed the effect of stochastic resonance (SR) stimulation to the lower extremity on postural regulation and balance performance in sub-populations such as healthy adults (mean age: 23.04 years, ±6.33 years) (2), elderly individuals (mean age: 73.00 years) (3), or individuals with comprised health suffering from Parkinson (4), or multiple sclerosis (5) or stroke (6, 7), SR has been shown in a variety of physiological systems (8–11), in which the presence of noise below the sensory threshold could enhance the response of the system to weak signals (12–14). Collins et al. (12) postulated that SR could be used to elderly individuals with elevated sensory thresholds.
Whole body vibration (WBV) with stochastic resonance (SR) can easily applied. SR-WBV does not lead to exhaustion and blood pressure and lactate levels are low during vibration training (15). SR-WBV could be easily personalized to the individual's level of fitness (16). For example, elderly with low baseline fitness who want to start an exercise program should start with a program that meets their physical capabilities (16). Older people with frailty or pre-frail condition are advised to undergo a “skilling-up” phase before undertaking more traditional forms of training (17). SR-WBV can be used as a training modality for the “skilling-up” phase (16, 18, 19). Compared to traditional balance training, there are indications on how to design a training regime (sets, rest between sets, session per weeks, etc.) and on the other hand the training protocols are characterized by a short duration between 1 and 5 min of intermittent or continuous WBV application (20). There is no need to change clothes or shoes or to shower afterwards, which might be important in the working world or for adults who do not want to waste time on intensive training (2). Eichelberger et al. (21) were able to determine a decrease in accelerations with increasing distance from the vibrating plate due to damping properties of the involved body structures. However, it is known that a prolonged exposure to vibration (e.g., driving, hammering) may lead to musculoskeletal and neurological disorders (22, 23). Systematic reviews and meta-analysis (24–27) have shown that shorter exposure to vibration have a positive effect on muscle strength and postural control if the training regime (e.g., amplitude, duration and frequency of vibration) is correctly dosed.
SR-WBV differs from sinusoidal WBV in that the stimuli are randomized and amplified using noise (25, 28). This results in a generation of action potentials by the suprathreshold stimuli (29). SR-WBV induces an excitatory stimulus to the alpha motoneuron via mono- and polysynaptic pathways and elicits muscle activation in response, resulting in body stabilization (30). SR-WBV can be understood as reactive balance training that simulates a fall situation itself through the application of unpredictable, random, and multidirectional displacements of the stance surface (31). Reactive balance training means that a person has the ability to react to a loss of balance, because reactive balance is a key factor that ultimately determines whether an individual will sustain a fall (32). Reactive balance can be profoundly impaired in older adult populations (32).
In contrast to SR-WBV, sinusoidal WBV are constant. If the stimulus remains the same, the body adapts very quickly and this slows down the impact of growth stimulus (27). Three WBV devices were used in clinical settings: sinusoidal vertical (SV-WBV), sinusoidal side-alternating (SS-WBV), and stochastic resonance (SR-WBV). While the sinusoidal WBV devices uses a single plate for standing, the SR-WBV device uses two plates for standing (24, 33–36). Due to the different physiological mechanisms of impact and use of equipment, this paper focuses on SR-WBV.
Furthermore, study results demonstrated that whole-body vibration training provides more than physiological effects (2, 37). Animals study showed that daily exposure to WBV over five weeks significantly improved cognition in young mice compared to non-vibrated mice (38, 39). Regterschot et al. (37) could determine that passive WBV could improve executive functions in healthy young adults. They postulated that WBV has the potential as a cognition-enhancing therapy. Chan et al. (40) reported that executive functions are a set of cognitive processes that regulate, manage and control other cognitive processes in order to achieve a goal, such as planning, mental flexibility, multi-tasking etc. Research findings described that cognitive decline and falls are linked (41–43) and that cognitive training improve balance and gait (44).
Aim
A systematic literature review on the effects of SR-WBV on postural control have been conducted previously (27). As the number of publications on SR-WBV has increased significantly in recent years, this present systematic literature review aims to provide an update on the status quo of the efficacy of SR-WBV on postural control in frail elderly individuals. The research question was: could SR-WBV positively influence postural control in individuals with balance disability?
Methods
Study design
This paper is an update of the systematic review by Rogan et al. (27). In advance, a registration on PROSPERO (CRD420203194) was conducted and the guideline “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) was used for reporting. This current systematic review used the same methodological approach as the first study. The inclusion and exclusion criteria were identical. The same search terms were used on the same databases. The data collection process was more comprehensive in this study. Besides the training load, the intervention protocol and the measurement instrument tools were now included. The risk of bias was assessed with the same instrument (The Cochrane Collaboration Cochrane Risk of Bias Tool) as in the first study.
Information sources
Electronic searches were conducted on CINAHL, Cochrane Central Register of Controlled Trials, Physiotherapy Evidence Database (PEDro), and PubMed up to August 2022. In addition, a hand search of the reference lists of included studies, research institution websites, and Google Scholar was conducted.
Search strategy
The PICO model was used in this study. The PICO acronym stands for Population (elderly, frail elderly), Intervention (WBV exercise), Comparator (no treatment, or other balance exercise), Outcomes (postural control, static, dynamic, functional balance). Search terms included: (i) “stochastic resonance whole-body vibration” OR “SR-WBV” OR “stochastic vibration” OR “stochastic training” AND (ii) “balance” OR “postural control* “ OR “postural stability”.
Eligibility criteria
This study included intervention studies and randomized controlled pilot studies. German- and English-language articles with intervention and control groups from the fields of geriatrics were considered. For studies with frail elderly persons, those aged 65 years and older were eligible. Studies with frail elderly persons under 65 years of age, studies with elderly persons with “fit” status, and studies with neurological diseases were excluded.
Data collection process
Two independent study nurses screened and analyzed the title and abstract for inclusion and exclusion criteria. In the next step, the full text was read and included in this systematic literature review if eligible. For each included article, authors, population, intervention protocol, outcome parameters, results, and training load were extracted and electronically recorded by two independent study nurses.
Study risk of bias assessment
The Cochrane Collaboration Cochrane Risk of Bias Tool (RoB) (45) was used to assess the internal validity of the included articles. Two independent reviewers (SR, JT) assessed the methodological quality of the eligible studies with “The Cochrane Collaboration's tool for assessing risk of bias”. The criteria list comprised six items and each item were scored with + for yes, with—for no, and with? if the information was not provided or was unclear. A study was determined as having a low risk of bias if all criteria are fulfilled with yes. A study has a moderate risk of bias when one or more items are scored with unclear, while a study has a high risk of bias if one or more key domains have been rated with no. The level of agreement between the independent reviewers who rated the primary studies was 98%.
Results
Study selection
There were 1,206 matches of studies. Of these, 262 duplicates were removed. A total of 944 titles and abstracts were screened, and 917 articles were removed due to systematic reviews articles (n = 8), application of sinusoidal vibration (n = 898), application of stochastic vibration via the sole of the foot or knee (n = 7), effects of SR-WBV on postural control or pain (n = 2), pelvic floor muscle (n = 2). The remaining 27 full texts were read, of which 9 articles were included in this systematic review (Figure 1). Three articles originated from Germany (4, 46, 47), and six from Switzerland1 (16, 19, 30, 36, 48, 49). Six trials were designed as pilot study (16, 19, 30, 36, 48, 49) and three as randomized controlled trials (4, 46, 47).
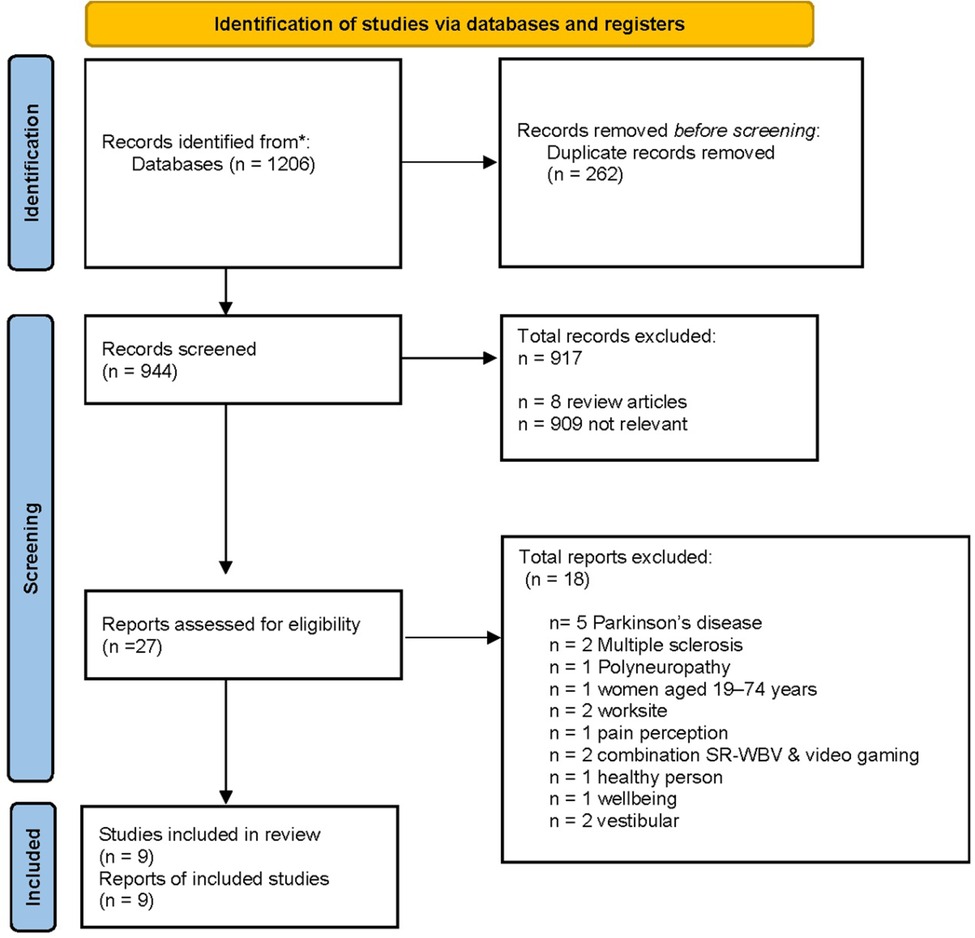
Figure 1. Flow chart of the search.
Balance survey method
A total of six articles examined static balance (16, 19, 30, 47–49), six studies examined dynamic balance (4, 16, 19, 30, 47, 49) while five studies observed functional balance (19, 46–49).
Result overview of the studies
Overall, four of nine studies showed statistically significant balance improvements within the SR-WBV group in the before-after comparison (4, 19, 46, 48). Table 1 summarizes the findings of the individual articles.
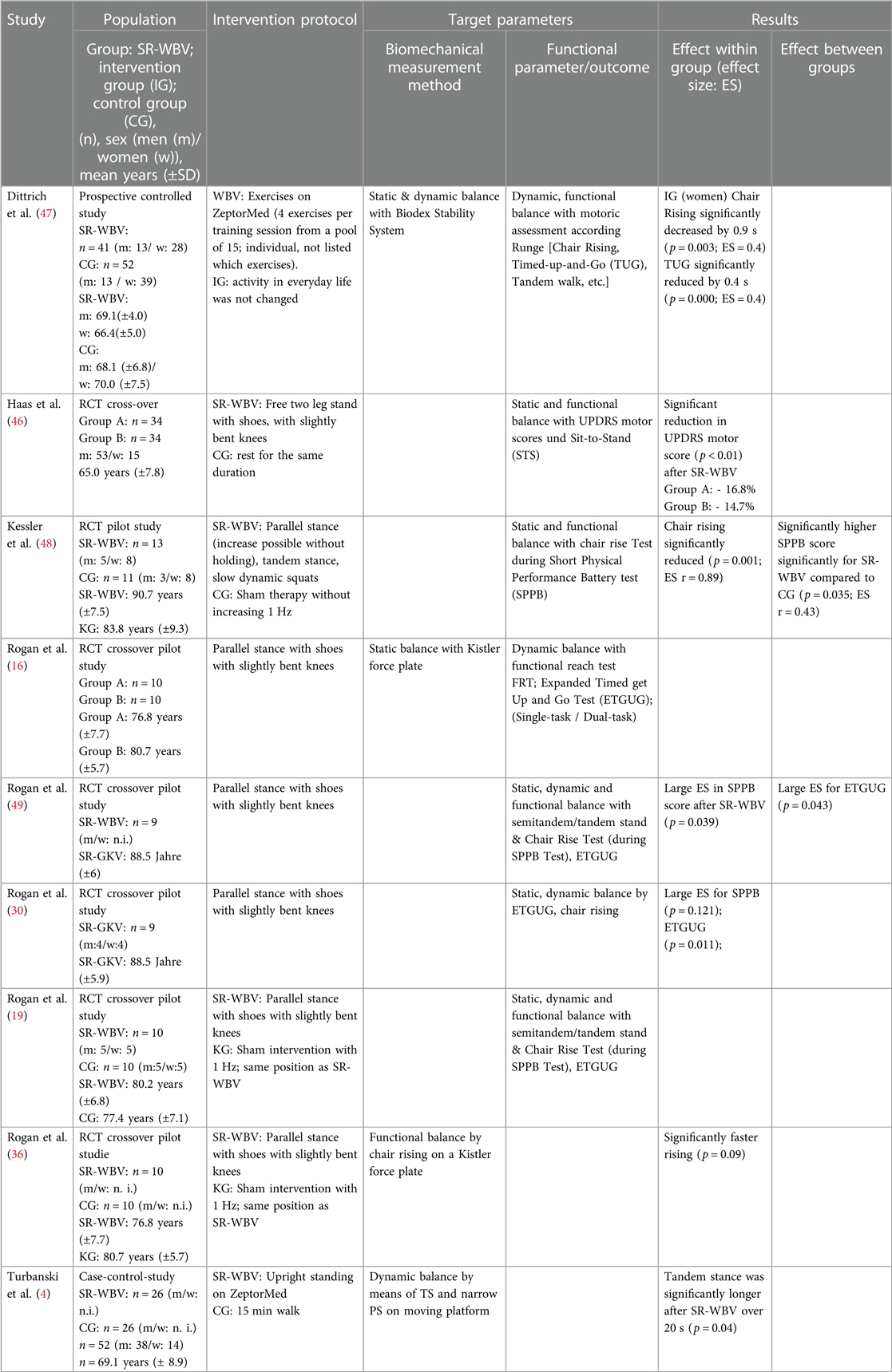
Table 1. Overview of the study characteristics of the included studies.
Training loads
In four of the nine studies, participants received a single training session with SR-WBV (4, 19, 30, 46). The remaining five studies determined the effect of SR-WBV after multiple interventions. The range was 12–36 training sessions (16, 36, 47–49).
In three studies (4, 46, 48), the frequency was increased and the starting position on the vibration device was progressively adjusted to the participants. All three studies use 5 sets and 60 s of vibration. One study did not specify a frequency (47). In three trials, continuous vibration was performed at a frequency of 5 Hz and five series with a duration of 60 s and rest of 60 s (19, 36). Four studies applied a frequency of 6 Hz, with 5–6 series of 60 s duration and 60 s rests (4, 16, 30, 46, 49).
The control group (CG) received no active intervention in four out of nine studies (19, 46, 47, 50). In one study, the CG completed a different intervention (4). Sham intervention was performed in four other studies. Table 2 gives an overview of the training load.
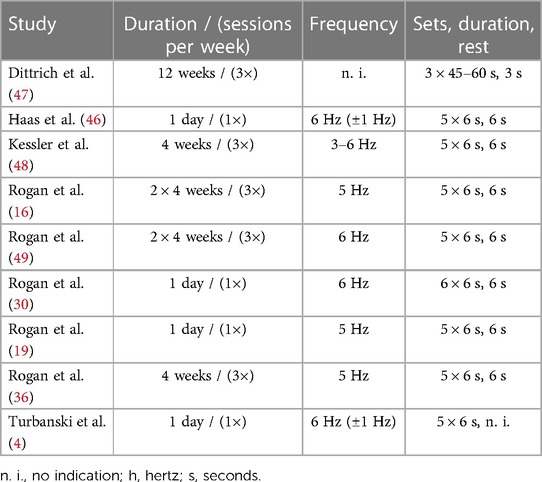
Table 2. SR-WBV training load as used in the different studies under investigation.
The evaluation of the methodological quality was classified as followed (Table 3): one study did not use the method of allocation concealment (47), seven studies (4, 16, 19, 30, 46, 47, 49) did not report the blinded status of the investigator or participant, and four studies (4, 19, 46, 49) showed incomplete outcome data. They presented only change percentage data. They did not give any information about baseline and intervention data and no effect size calculation was used. Table 3 provides an overview of the risk of bias of the included studies.
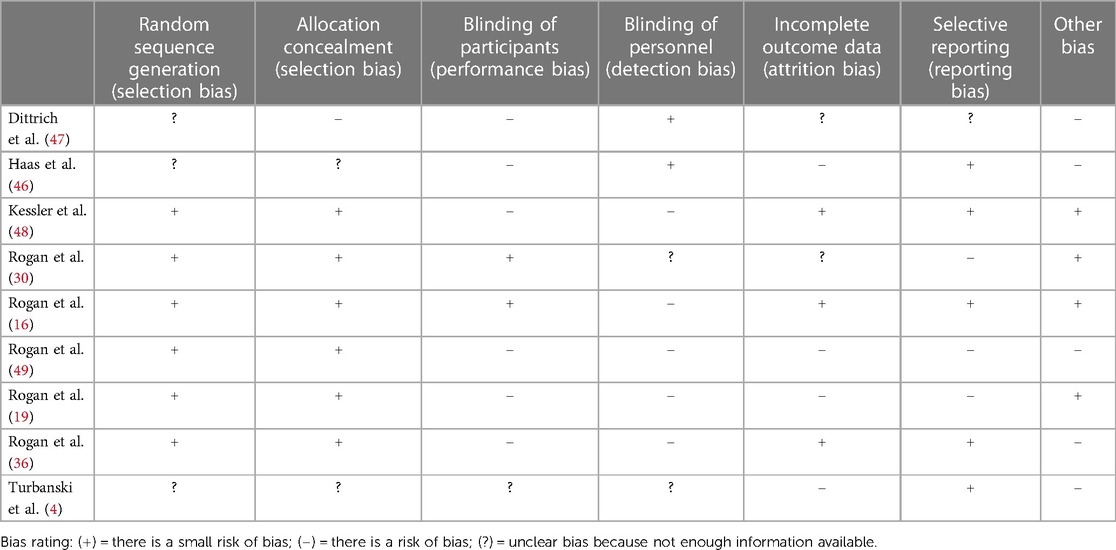
Table 3. Risk of bias of the included studies.
Discussion
During aging, sensory symptoms such as absent reflexes are clinically relevant. They are not only debilitating but also responsible for changes. This systematic literature review addressed the research question “could SR-WBV positively influence postural control in individuals with balance disability?” using published results.
In summary, the effect of SR-WBV on postural control presents a mixed picture. The statistically significant results from four studies were contrasted with five statistically unsound results. However, the effect size was strengthened by Rogan et al.'s (49) indication of clinical relevance. They were able to demonstrate clinical relevance (2.9 s) for the Expanded Timed Get-up-and-Go (ETGUG) test (51) in frail individuals after SR-WBV training. The SR-WBV group was a median of 3 s faster after the intervention period compared with the baseline measurement (P = 0.043; ES: 0.91). This study result has immediate consequences in terms of treatment recommendation for frail individuals with a postural control deficit of dynamic balance (52). It is known that a normal sensory system is necessary for successful postural control and movement. The central nervous system must accurately assess the position of the body in space and the limbs in relation to each other (proprioception). Postural reflexes must be released efficiently when external perturbations are detected. Maintaining balance must be automatic so that it is not impaired by other tasks. During aging, impairments of the sensorimotor system lead to a loss of postural control and to falls. The process of postural control depends on many sensory signals and neurological pathways and maintaining the quality of these systems at their optimal level is fundamental. SR-WBV could play an important role toward addressing postural control, by involving an interaction of different types of neurophysiological sensors and the adaptation of afferent and efferent signals, the SR-WBV likely serves as an exercise for the sensorimotor system. Tan et al. (53) demonstrated in their systematic review a significant positive benefit on postural control (SMD = 0.61, 95% CI: 0.12 to 1.09, P = 0.01) and muscle activity in tibialis anterior (SMD = 0.46, 95% CI: 0.04 to 0.88, P = 0.03) and gastrocnemius (SMD = 0.68, 95% CI: 0.14 to 1.23, P = 0.01) using sinusoidal whole-body vibration in individuals with a sensorimotor deficit after ankle injury. They concluded that whole body vibration has the potential to improve sensorimotor deficits involving balance, strength, joint position sense, and muscle activity in people with chronic ankle instability. However, Lesinski et al. (54) formulated in their systematic review and meta-analysis article a balance training regime for healthy elderly by a training period of 11–12 weeks, a training frequency of three sessions per week, a total number of 36–40 training sessions, a duration of 31–45 min of a single training session, and a total duration of 91–120 min of balance training per week. Comparing these findings with findings from young healthy adults, it seems plausible that almost the same balance protocols are effective in healthy young and older adults and there seems to be no age effect (54). In this current article, no of the included articles reported this amount of training regimes. Fisher et al. were able to illustrate in their meta-analysis, that long-term WBV (between 4 weeks and 32 weeks) could significantly improve functional balance (Timed-up-Go test: SMD = −0.18; 95% CI: −0.32, −0.04; 10 min walking test SMD = −0.28; 95% CI: −0.56, −0.01). However, no significant changes were found in elderly individuals (tinetti gait scores: SMD = 0.04; 95% CI: −0.23, 0.31, 6 min walking test: SMD = 0.37; 95% CI: −0.03, 0.78).
It is known that muscle strength is a potentially important factor contributing to postural control (61). Large effects of strength training could be determined for static and dynamic balance in elderly individuals, but only a small effect was found for dynamic balance in young adults (62). Son et al. (63) were able to demonstrate that strength training increase muscle strength in ankle musculature and improve one-leg-standing balance compared to control situation. It can be concluded that the intensity of strength training is fundamental not only for increasing muscle strength but also for improving postural balance in elderly participants.
Furthermore, Kingwell described that exercise has the potential to improve cognitive function (64). Explanatory models address the fact that WBV stimulate mechanosensory receptors (e.g., tactile corpuscles). These signals are transmitted to the primary somatosensory cortex. These areas have connection with region in the prefrontal cortex that strongly involved in cognitive processing (37, 65). An indirect pathway involves the limbic system (e.g., amygdala and hippocampus, important areas of learning and memory), which can mediate the effects of sensory correlations on the prefrontal cortex (66). The amygdala has projections to non-thalamic nuclei (e.g., the cholinergic nuclei of the basal forebrain) with diffuse connections to several brain regions (65). It can be speculated that mechanosensory receptor stimulation can increase cognitive function. Furthermore, it has been assumed that improvement in cognitive function depends on increased production of neurotrophins [e.g., brain-derived neurotrophic factor (BDNF)] (67). BDNF is recognized as the most significant neurotrophic growth factor related to neuronal plasticity and has a key role in the differentiation and survival of neurons (68). Studies could demonstrate a close correlation between increased BDNF levels and WBV (69, 70). However, so far it is unclear how mechanical vibrations may influence the expression of BDNF (71).
The loss of balance ability is an important risk factor for falls in elderly individuals. Reactive balance is a crucial part of avoiding and adapting to complex environments that threaten postural stability (72). In German-speaking countries, the balance ability is considered to be a coordinative ability (73). We describe this ability as the aggregate understood to maintain and regain balance, taking into account the necessary personal conditions.
Various types of exercises (e.g., airex pad, tilting board, swinging platforms) are used in treatment settings and summarized with the synonym balance training (74–77). The goal is to optimize balance. It is assumed that balance is a skill, and that balance training improves several balance tasks at the same time (29). However, recent studies indicate that only those balance tasks that are trained can also improve (77, 78). Giboin et al. (32) showed that the group which trained in a single-leg stand on the tilting board and the group that trained in a single-leg stand on the swinging board (Posturomed) improved statistically significantly only in the area in which they trained.
Recently, there have been attempts to move away from the term ability towards the definition of skill (73). Taube (78) explained that balance training does not change the behavior of the spinal reflex per se. It seems rather to improve the ability of finding the right reflex settings for specific conditions of postural control. Thus, balance training improves task-specific reflex modulation. Low et al. (55) postulated, that specific balance exercise could be the only one likely to improve postural balance. Slackline training improves postural balance in young and elderly individuals in a one-leg stance (56, 57). However, the impact of slackline training is limited or negligible for standard static and dynamic bipedal stances (58–60). Paillard (79) explains that specific balance training optimizes postural skills, but it is not known whether these skills improve motor skills in all types of physical activity. He further refers to the fact that additional studies are required to address this question accurately. Grabiner et al. (80) indicates that task-specific perturbation training is superior to traditional balance exercise training in improving reactive balance capacity and thus preventing falls. Kim et al. (72) performed a network meta-analysis to specify which exercise method is most effective to improve reactive balance in elderly individuals. They analyzed data of 39 RCTs including 1,388 elderly individuals receiving balance training with reactive components (perturbations training) demonstrated the most amount of improvement in reactive training, followed by power training and gait training. SR-WBV is power training. SR-WBV has the potential to improve race of force development after four weeks SR-WBV training in elderly individuals (48). In relation to gait, SR-WBV can be used as skilling up in elderly not able to perform standard gait training. It is known that SR-WBV could significantly improve gait in older adults (19, 47, 49). In the case of a reactive balance, the better the gait, the sooner gait training can be started.
Limitation
The observed heterogeneity in the individual studies' study quality and findings impede a clear-cut answer to the research question. Furthermore, the study design of the pilot study does not allow a clear conclusion on efficacy because the primary aim of the pilot study is not to assess an exact intervention effect size, but rather to determine the sample sizes and evaluate feasibility of the study protocol (81–83).
Conclusion
We found a heterogeneous situation on effects for balance according to SR-WBV. One study showed clinical relevance for ETGUG. Two studies examined the skill in reactive balance. Since balance is a skill and SR-WBV trains reactive balance, future studies should focus on the parameter reactive balance.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author contributions
This research project was developed by SR. Data collection was undertaken by two independent bachelor students. SR wrote and JT edited the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
We would like to thank Ross Bennie for proofreading the manuscript and the bachelor students Lisa Matthaes and Patric Schnegg.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnote
1These articles are from the authors of this systematic review.
References
1. Muslimović D, Post B, Speelman JD, Schmand B, de Haan RJ. Determinants of disability and quality of life in mild to moderate Parkinson disease. Neurology. (2008) 70(23):2241. doi: 10.1212/01.wnl.0000313835.33830.80
2. Faes Y, Rolli Salathé C, Herlig ML, Elfering A. Beyond physiology: acute effects of side-alternating whole-body vibration on well-being, flexibility, balance, and cognition using a light and portable platform A randomized controlled trial. Front Sports Act Living. (2023) 5. doi: 10.3389/fspor.2023.1090119
3. Priplata AA, Niemi JB, Harry JD, Lipsitz LA, Collins JJ. Vibrating insoles and balance control in elderly people. Lancet. (2003) 362(9390):1123–4. doi: 10.1016/S0140-6736(03)14470-4
4. Turbanski S, Haas CT, Schmidtbleicher D, Friedrich A, Duisberg P. Effects of random whole-body vibration on postural control in Parkinson’s disease. Res Sports Med. (2005) 13(3):243–56. doi: 10.1080/15438620500222588
5. Schuhfried O, Mittermaier C, Jovanovic T, Pieber K, Paternostro-Sluga T. Effects of whole-body vibration in patients with multiple sclerosis: a pilot study. Clin Rehabil. (2005) 19(8):834–42. doi: 10.1191/0269215505cr919oa
6. Herren K, Schmid S, Rogan S, Radlinger L. Effects of stochastic resonance whole-body vibration in individuals with unilateral brain lesion: a single-blind randomized controlled trial: whole-body vibration and neuromuscular function. Rehabil Res Pract. (2018) 2018. doi: 10.1155/2018/9319258
7. Priplata AA, Patritti BL, Niemi JB, Hughes R, Gravelle DC, Lipsitz LA, et al. Noise-enhanced balance control in patients with diabetes and patients with stroke. Ann Neurol. (2006) 59(1):4–12. doi: 10.1002/ana.20670
8. Collins JJ, Imhoff TT, Grigg P. Noise-enhanced information transmission in rat SA1 cutaneous mechanoreceptors via aperiodic stochastic resonance. J Neurophysiol. (1996) 76(1):642–5. doi: 10.1152/jn.1996.76.1.642
9. Cordo P, Inglis JT, Verschueren S, Collins JJ, Merfeld DM, Rosenblum S, et al. Noise in human muscle spindles. Nature. (1996) 383(6603):769–70. doi: 10.1038/383769a0
10. Douglass JK, Wilkens L, Pantazelou E, Moss F. Noise enhancement of information transfer in crayfish mechanoreceptors by stochastic resonance. Nature. (1993) 365(6444):337–40. doi: 10.1038/365337a0
11. Levin JE. Miller JP. Broadband neural encoding in the cricket cereal sensory system enhanced by stochastic resonance. Nature. (1996) 380(6570):165–8. doi: 10.1038/380165a0
12. Collins JJ, Imhoff TT, Grigg P. Noise-enhanced tactile sensation. Nature. (1996) 383(6603):770. doi: 10.1038/383770a0
13. Collins JJ, Chow CC, Imhoff TT. Stochastic resonance without tuning. Nature. (1995) 376:236–8. doi: 10.1038/376236a0
14. Wiesenfeld K, Moss F. Stochastic resonance and the benefits of noise: from ice ages to crayfish and SQUIDs. Nature. (1995) 373(6509):33–6. doi: 10.1038/373033a0
15. Herren K, Hängärtner CH, Oberli A, Radlinger L. Kardiovaskuläre und metabolische Beanspruchung während stochastischer Resonanztherapie bei Schlaganfallpatienten. Physioscience. (2009) 5(01):13–7. doi: 10.1055/s-0028-1109140
16. Rogan S, Radlinger L, Hilfiker R, Schmidtbleicher D, De Bie RA, De Bruin ED. Feasibility and effects of applying stochastic resonance whole-body vibration on untrained elderly: a randomized crossover pilot study. BMC Geriatr. (2015) 15(1):25. doi: 10.1186/s12877-015-0021-4
17. Skelton DA, Dinan SM. Exercise for falls management: rationale for an exercise programme aimed at reducing postural instability. Physiother Theory Pract. (1999) 15(2):105–20. doi: 10.1080/095939899307801
19. Rogan S, Radlinger L, Schmid S, Herren K, Hilfiker R, de Bruin ED. Skilling up for training: a feasibility study investigating acute effects of stochastic resonance whole-body vibration on postural control of older adults. Ageing Res. (2012) 3(1):e5-e. doi: 10.4081/ar.2012.e5
20. Ritzmann R, Kramer A, Bernhardt S, Gollhofer A. Whole body vibration training-improving balance control and muscle endurance. PLoS One. (2014) 9(2):e89905. doi: 10.1371/journal.pone.0089905
21. Eichelberger P, Fankhauser R, Geering R, Radlinger L, Rogan S. Trunk muscle activity and acceleration of the spine during partial-body vibration in a sitting position—a single case study. Physiotherapy. (2015) 101:e347. doi: 10.1016/j.physio.2015.03.556
22. Johanning E. Whole-body vibration-related health disorders in occupational medicine–an international comparison. Ergonomics. (2015) 58(7):1239–52. doi: 10.1080/00140139.2015.1005170
23. Scherrer A. Risikofaktor vibrationen: So schützen sie die gesundheit ihrer mitarbeitenden. SUVA: SUVA- Gesundheitschutz (2012).
24. Rogan S, Taeymans J, Radlinger L, Naepflin S, Ruppen S, Bruelhart Y, et al. Effects of whole-body vibration on postural control in elderly: an update of a systematic review and meta-analysis. Arch Gerontol Geriatr. (2017) 73:95–112. doi: 10.1016/j.archger.2017.07.022
25. Rogan S, de Bruin ED, Radlinger L, Joehr C, Wyss C, Stuck N-J, et al. Effects of whole-body vibration on proxies of muscle strength in old adults: a systematic review and meta-analysis on the role of physical capacity level. Eur Rev Aging Phys Act. (2015) 12(1):1–26. doi: 10.1186/s11556-015-0149-4
26. Rogan S, Hilfiker R, Herren K, Radlinger L, de Bruin ED. Effects of whole-body vibration on postural control in elderly: a systematic review and meta-analysis. BMC Geriatr. (2011) 11(1):1–18. doi: 10.1186/1471-2318-11-72
27. Rogan S, Hilfiker R, Schenk A, Vogler A, Taeymans J. Effects of whole-body vibration with stochastic resonance on balance in persons with balance disability and falls history–a systematic review. Res Sports Med. (2014) 22(3):294–313. doi: 10.1080/15438627.2014.919504
28. Gammaitoni L, Hänggi P, Jung P, Marchesoni F. Stochastic resonance. Rev Mod Phys. (1998) 70(1):223. doi: 10.1103/RevModPhys.70.223
29. Haas CT, Turbanski S, Markitz S, Kaiser I, Schmidtbleicher D. Stochastische Resonanz in der Therapie von Bewegungsstörungen. B&G Bewegungstherapie und Gesundheitssport. (2006d) 22:58–61. doi: 10.1055/s-2006-933388
30. Rogan S, Schmidtbleicher D, Radlinger L. Immediate effects after stochastic resonance whole-body vibration on physical performance on frail elderly for skilling-up training: a blind cross-over randomised pilot study. Aging Clin Exp Res. (2014) 26(5):519–27. doi: 10.1007/s40520-014-0212-4
31. Krause A, Freyler K, Gollhofer A, Stocker T, Brüderlin U, Colin R, et al. Neuromuscular and kinematic adaptation in response to reactive balance training–a randomized controlled study regarding fall prevention. Front Physiol. (2018) 9:1075. doi: 10.3389/fphys.2018.01075
32. Palmer JA, Payne AM, Ting LH, Borich MR. Cortical engagement metrics during reactive balance are associated with distinct aspects of balance behavior in older adults. Front Aging Neurosci. (2021) 13:684743. doi: 10.3389/fnagi.2021.684743
34. De Bruin ED, Baur H, Brülhart Y, Luijckx E, Hinrichs T, Rogan S. Combining stochastic resonance vibration with exergaming for motor-cognitive training in long-term care; A sham-control randomized controlled pilot trial. Front Med (Lausanne). (2020) 7:507155. doi: 10.3389/fmed.2020.507155
35. Rogan S, Radlinger L, Baur H, Schmidtbleicher D, de Bie RA, de Bruin ED. Sensory-motor training targeting motor dysfunction and muscle weakness in long-term care elderly combined with motivational strategies: a single blind randomized controlled study. Eur Rev Aging Phys Act. (2016) 13(1):1–12. doi: 10.1186/s11556-016-0164-0
36. Rogan S, Hilfiker R, Schmid S, Radlinger L. Stochastic resonance whole-body vibration training for chair rising performance on untrained elderly: a pilot study. Arch Gerontol Geriatr. (2012) 55(2):468–73. doi: 10.1016/j.archger.2012.02.011
37. Regterschot GRH, Van Heuvelen MJG, Zeinstra EB, Fuermaier ABM, Tucha L, Koerts J, et al. Whole body vibration improves cognition in healthy young adults. PLoS One. (2014) 9(6):e100506. doi: 10.1371/journal.pone.0100506
38. Timmer M, Van der Zee EA, Riedel G. Whole body vibration and behavior: Investigation of the role of various neurotransmitter systems. Federation of European Neuroscience Societies Abstract. (2006) 3(089.31)
39. Van der Zee EA, Riedel G, Rutgers EH, De Vries C, Postema F, Venema BJ. Enhanced neuronal activity in selective brain regions of mice induced by whole body stimulation. Federation of European Neuroscience Societies Abstract. (2010) 5(024.49):R2.
40. Chan RCK, Shum D, Toulopoulou T, Chen EYH. Assessment of executive functions: review of instruments and identification of critical issues. Arch Clin Neuropsychol. (2008) 23(2):201–16. doi: 10.1016/j.acn.2007.08.010
41. Chen TY, Peronto CL, Edwards JD. Cognitive function as a prospective predictor of falls. J Gerontol B Psychol Sci Soc Sci. (2012) 67(6):720–8. doi: 10.1093/geronb/gbs052
42. Springer S, Giladi N, Peretz C, Yogev G, Simon ES, Hausdorff JM. Dual-tasking effects on gait variability: the role of aging, falls, and executive function. Mov Disord. (2006) 21(7):950–7. doi: 10.1002/mds.20848
43. Tinetti ME. Preventing falls in elderly persons. N Engl J Med. (2003) 348(1):42–9. doi: 10.1056/NEJMcp020719
44. Doumas M, Rapp MA, Krampe RT. Working memory and postural control: adult age differences in potential for improvement, task priority, and dual tasking. J Gerontol B. (2009) 64(2):193–201. doi: 10.1093/geronb/gbp009
45. Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. Br Med J. (2011) 343. doi: 10.1136/bmj.d5928
46. Haas CT, Turbanski S, Kessler K, Schmidtbleicher D. The effects of random whole-body-vibration on motor symptoms in Parkinson’s disease. Neurorehabilitation. (2006b) 21:29–36. doi: 10.3233/NRE-2006-21105
47. Dittrich M, Eichner G, Schmidtbleicher D, Beyer WF. Eine Untersuchung zur Wirkung der Stochastischen Resonanztherapie (SRT-Zeptoring) auf die Knochendichte, Rumpfkraft und Koordination bei Senioren. OUP. (2012) 1(2):60–5. doi: 10.328/oup.2012.0060-0065
48. Kessler J, Radlinger L, Baur H, Rogan S. Effect of stochastic resonance whole body vibration on functional performance in the frail elderly: a pilot study. Arch Gerontol Geriatr. (2014) 59(2):305–11. doi: 10.1016/j.archger.2014.06.005
49. Rogan S, Radlinger L, Schmidtbleicher D, de Bie RA, de Bruin ED. Preliminary inconclusive results of a randomised double blinded cross-over pilot trial in long-term-care dwelling elderly assessing the feasibility of stochastic resonance whole-body vibration. Eur Rev Aging Phys Act. (2015) 12(1):5. doi: 10.1186/s11556-015-0150-y
50. Haas CT, Buhlmann A, Turbanski S, Schmidtbleicher D. Proprioceptive and sensorimotor performance in Parkinson’s disease. Res Sports Med. (2006a) 14. doi: 10.1080/15438620600985902
51. Botolfsen P, Helbostad JL, Moe-nilssen R, Wall JC. Reliability and concurrent validity of the expanded timed up-and-go test in older people with impaired mobility. Physiother Res Int. (2008) 13(2):94–106. doi: 10.1002/pri.394
52. White O, Babič J, Trenado C, Johannsen L, Goswami N. The promise of stochastic resonance in falls prevention. Front Physiol. (2019) 9. doi: 10.3389/fphys.2018.01865
53. Tan J, Wu X, Clark CCT, Barton V, Chen S, Liu S, et al. The effect of whole body vibration on sensorimotor deficits in people with chronic ankle instability: a systematic review and meta-analysis. Clin Rehabil. (2022) 36(8):1016–31. doi: 10.1177/02692155221095
54. Lesinski M, Hortobágyi T, Muehlbauer T, Gollhofer A, Granacher U. Effects of balance training on balance performance in healthy older adults: a systematic review and meta-analysis. Sports Med. (2015) 45(12):1721–38. doi: 10.1007/s40279-015-0375-y
55. Horlings CGC, Van Engelen BG, Allum JHJ, Bloem BR. A weak balance: the contribution of muscle weakness to postural instability and falls. Nat Clin Pract Neurol. (2008) 4(9):504–15. doi: 10.1038/ncpneuro0886
56. Behm DG, Muehlbauer T, Kibele A, Granacher U. Effects of strength training using unstable surfaces on strength, power and balance performance across the lifespan: a systematic review and meta-analysis. Sports Med. (2015) 45:1645–69. doi: 10.1007/s40279-015-0384-x
57. Son SM, Kang KW, Lee NK, Nam SH, Kwon JW, Kim K. Influence of isokinetic strength training of unilateral ankle on ipsilateral one-legged standing balance of adults. J Phys Ther Sci. (2013) 25(10):1313–5. doi: 10.1589/jpts.25.1313
58. Kingwell K. An exercise-linked mediator of memory protection. Nat Rev Drug Discovery. (2019) 18(2):97–8. doi: 10.1038/d41573-019-00006-x
59. Braak H, Braak E, Yilmazer D, Bohl J. Topical review: functional anatomy of human hippocampal formation and related structures. J Child Neurol. (1996) 11(4):265–75. doi: 10.1177/088307389601100402
60. Durgut E, Orengul AC, Algun ZC. Comparison of the effects of treadmill and vibration training in children with attention deficit hyperactivity disorder: a randomized controlled trial. NeuroRehabilitation. (2020) 47(2):121–31. doi: 10.3233/NRE-203040
61. Bonanni R, Cariati I, Tarantino U, D’Arcangelo G, Tancredi V. Physical exercise and health: a focus on its protective role in neurodegenerative diseases. J Funct Morphol Kinesiol. (2022) 7(2):38. doi: 10.3390/jfmk7020038
62. von Bohlen und Halbach O, von Bohlen und Halbach V. BDNF Effects on dendritic spine morphology and hippocampal function. Cell Tissue Res. (2018) 373:729–41. doi: 10.1007/s00441-017-2782-x
63. Ribeiro VGC, Lacerda ACR, Santos JM, Coelho-Oliveira AC, Fonseca SF, Prates ACN, et al. Efficacy of whole-body vibration training on brain-derived neurotrophic factor, clinical and functional outcomes, and quality of life in women with fibromyalgia syndrome: a randomized controlled trial. J Healthc Eng. (2021) 2021. doi: 10.1155/2021/7593802
64. Simão AP, Mendonça VA, Avelar NCP, da Fonseca SF, Santos JM, De Oliveira ACC, et al. Whole body vibration training on muscle strength and brain-derived neurotrophic factor levels in elderly woman with knee osteoarthritis: a randomized clinical trial study. Front Physiol. (2019) 10:756. doi: 10.3389/fphys.2019.00756
65. Bonanni R, Cariati I, Romagnoli C, D’Arcangelo G, Annino G, Tancredi V. Whole body vibration: a valid alternative strategy to exercise? J Funct Morphol Kinesiol. (2022) 7(4):99. doi: 10.3390/jfmk7040099
66. Kim Y, Vakula MN, Bolton DAE, Dakin CJ, Thompson BJ, Slocum TA, et al. Which exercise interventions can most effectively improve reactive balance in older adults? A systematic review and network meta-analysis. Front Aging Neurosci. (2022) 13:992. doi: 10.3389/fnagi.2021.764826
67. Kramer A, Giboin L-S. Gleichgewichtstraining: transfer auf untrainierte Aufgaben? Sportphysio. (2019) 7(01):16–21. doi: 10.1055/a-0818-3129
68. Rogan S, Baur H, Sargent A, Schori M, Taeymans J. Machbarkeit eines Gleichgewichtstrainings auf Matten bei gesunden, moderat sportlichen Frauen im Alter. Z Gerontol Geriat. (2015) 48(2):135–41. doi: 10.1007/s00391-014-0630-0
69. Heitkamp HC, Horstmann T, Mayer F, Weller J, Dickhuth HH. Balance training in men and women: effect on knee extensors and flexors. Isokinet Exerc Sci. (2001) 9(1):41–4. doi: 10.3233/IES-2001-0062
70. Giboin L-S, Gruber M, Kramer A. Task-specificity of balance training. Hum Mov Sci. (2015) 44:22–31. doi: 10.1016/j.humov.2015.08.012
71. Kümmel J, Kramer A, Giboin L-S, Gruber M. Specificity of balance training in healthy individuals: a systematic review and meta-analysis. Sports Med. (2016) 46(9):1261–71. doi: 10.1007/s40279-016-0515-z
72. Taube W. Neurophysiological adaptations in response to balance training. German J Sports Med. (2012) 63(9). doi: 10.5960/dzsm.2012.030
73. Low DC, Walsh GS, Arkesteijn M. Effectiveness of exercise interventions to improve postural control in older adults: a systematic review and meta-analyses of centre of pressure measurements. Sports Med. (2017) 47:101–12. doi: 10.1007/s40279-016-0559-0
74. Thomas M, Kalicinski M. The effects of slackline balance training on postural control in older adults. J Aging Phys Act. (2016) 24(3):393–8. doi: 10.1123/japa.2015-0099
75. Pfusterschmied J, Stöggl T, Buchecker M, Lindinger S, Wagner H, Müller E. Effects of 4-week slackline training on lower limb joint motion and muscle activation. J Sci Med Sport. (2013) 16(6):562–6. doi: 10.1016/j.jsams.2012.12.006
76. Granacher U, Iten N, Roth R, Gollhofer A. Slackline training for balance and strength promotion. Int J Sports Med. (2010) 31(10):717–23. doi: 10.1055/s-0030-1261936
77. Donath L, Roth R, Zahner L, Faude O. Slackline training and neuromuscular performance in seniors: a randomized controlled trial. Scand J Med Sci Sports. (2016) 26(3):275–83. doi: 10.1111/sms.12423
78. Donath L, Roth R, Zahner L, Faude O. Slackline training (balancing over narrow nylon ribbons) and balance performance: a meta-analytical review. Sports Med. (2017) 47(6):1075–86. doi: 10.1007/s40279-016-0631-9
79. Paillard T. Plasticity of the postural function to sport and/or motor experience. Neurosci Biobehav Rev. (2017) 72:129–52. doi: 10.1016/j.neubiorev.2016.11.015
80. Grabiner MD, Crenshaw JR, Hurt CP, Rosenblatt NJ, Troy KL. Exercise-based fall prevention: can you be a bit more specific? Exerc Sport Sci Rev. (2014) 42(4):161–8. doi: 10.1249/JES.0000000000000023
81. Thabane L, Ma J, Chu R, Cheng J, Ismaila A, Rios LP, et al. A tutorial on pilot studies: the what, why and how. BMC Med Res Methodol. (2010) 10(1):1. doi: 10.1186/1471-2288-10-1
82. Thabane L, Cambon L, Potvin L, Pommier J, Kivits J, Minary L, et al. Population health intervention research: what is the place for pilot studies? Trials. (2019) 20(1):309. doi: 10.1186/s13063-019-3422-4
Keywords: stochastic resonance therapy, whole-body vibration (WBV), falls, aged, postural balance [MeSH]
Citation: Rogan S and Taeymans J (2023) Effects of stochastic resonance whole-body vibration on sensorimotor function in elderly individuals—A systematic review. Front. Sports Act. Living 5:1083617. doi: 10.3389/fspor.2023.1083617
Received: 29 October 2022; Accepted: 27 March 2023;
Published: 17 April 2023.
Edited by:
Jaap Van Dieen, VU Amsterdam, NetherlandsReviewed by:
Achim Elfering, University of Bern, SwitzerlandYannik Faes, FernUni Schweiz, Switzerland
© 2023 Rogan and Taeymans. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Slavko Rogan c2xhdmtvLnJvZ2FuQGJmaC5jaA==
Specialty Section: This article was submitted to Biomechanics and Control of Human Movement, a section of the journal Frontiers in Sports and Active Living