 Udeme Samuel Jacob
Udeme Samuel Jacob Jace Pillay
Jace Pillay Ensa Johnson
Ensa Johnson Oluwatomilayo (Tomi) Omoya3
Oluwatomilayo (Tomi) Omoya3- 1South African Research Chair: Education and Care in Childhood, Faculty of Education, University of Johannesburg, Johannesburg, South Africa
- 2Department of Inclusive Education, College of Education, University of South Africa, Pretoria, South Africa
- 3College of Nursing and Health Sciences, Flinders University, Adelaide, Australia
- 4Department of Special Education, Faculty of Education, University of Ibadan, Ibadan, Nigeria
The inactivity of people with intellectual disabilities (PwID) is a major contributor to ill health. Probably because people with intellectual disabilities are not adequately informed about physical activity and intervention programs required to enhance their fitness. This study critically reviewed physical activity: benefits and needs for maintenance of quality of life among adults with intellectual disability. An extensive search of bibliographic databases such as PubMed, PsycINFO, BioMed Central and Medline identified 735 academic papers. The research rigour was evaluated, and the validity of the findings was established. Based on the inclusion criteria, 15 studies were included in the review. Various forms of physical activity were studied as interventions. The results of a critical review indicate that physical activity has a moderate to strong positive impact on weight loss, sedentary behaviour, and disability-related quality of life. Adults with ID may benefit from physical activity as a non-pharmaceutical method of improving their health needs. However, this study's results may only apply to some adults with intellectual disabilities. The sample size needs to be increased in future studies in order to draw generalizable conclusions.
Introduction
Intellectual disability (ID) is associated with considerable impairments in cognitive performance, resulting in the exhibition of maladaptive behaviour that originates before age 22 (1, 2). In addition to affecting the nervous and sensory systems, this disability may lead to metabolic and degenerative disorders, impaired ability to function, and physical disabilities (3). It significantly reduces the ability to comprehend, apply new and complex information. During the developmental period, intellectual and developmental disabilities (IDD) result from impairments in intellectual functioning and adaptive skills that adversely affect domains such as cognitive, functional, and social (4). Intellectual disability begins before adulthood, affects one's ability to function independently, and is detrimental to development on the long run (5). In the United Kingdom, intellectual disability is known as learning disabilities (6, 7), whereas in the United States of America, it is intellectual developmental disorder (7).
It is estimated that 10.37 people out of 1,000 live with this condition (8), affecting their ability to cope independently and affecting their development for the rest of their lives. Inequalities in health and social status are significant problems for many adults with ID (9). The evidence-based benefits of increased physical activity (PA) are also not enjoyed by a third of adults with ID (10). Health and social exclusion are aggravated by the lack of involvement in PA. Adults with ID face a global burden of health and social care costs (8).
Moreover, a person's inability to cope with social demands based on age can be categorized further according to severity (11). Apart from methodological differences between studies, estimates of ID prevalence vary by country (12), level of economic development, and individual characteristics (8). Some characteristics are associated with intellectual disabilities, including poor verbal skills, difficulty grasping the numerical concept, poor personal hygiene, such as using the bathroom, and emotional disorders or behavioural problems (13). Moreover, these individuals have difficulty balancing, separating, and connecting their movements. Their walking speed is noticeably slower the typical, thus restricting their physical or environmental movements, leading to little or no physical activities (14).
Inactive lifestyles or inability to engage in PA contribute significantly to high lifetime costs of health and non-healthcare services associated with diagnoses of ID. In addition to the economic costs associated with ID—or the resources used or lost because of the IDs—people with ID often require lifelong treatment and services (15). Cognitive impairments prevent persons with intellectual disability from actively participating in physical activities. Their appetites tend to be higher than those without intellectual disability, resulting in difficulties maintaining a healthy weight and an increased rate of obesity due to their appetite (13). These disabilities are more expensive to diagnose than other disabilities (such as cerebral palsy and visual and hearing impairments) (16). In some cases, they may be minimised by modifying one's lifestyle (12, 17).
In spite of the considerable health benefits of physical activity, it is believed that individuals with ID engage in relatively fewer PA, which makes it somewhat difficult for them to attain the expected level of health (10, 18). Lin et al., (19) suggested that people with ID should be physically active at least exercise 3 times per week and 30 min per, at a moderate intensity, for thirty minutes to improve their quality of life. The low levels of PA practice in this population have led to several articles focusing on identifying the factors that hinder PA practice in this population. Studies have identified a few factors that limit accessibility to PA practices, including transportation problems, cost, lack of personalized support and choices as well as lack of community PA programs (20–22). In the light of this reality, it is only logical that we should consider various ways PA can be of benefits to adults with ID. Relevant literature provides studies addressing this concern.
In terms of quality of life (QoL), adaptive behaviour is the most significant predictor (23). A person with IDD often has impaired executive function, which affects their ability to perform daily activities (24). Adults with ID have higher morbidity rates and shorter life expectancies (25, 26). As a result, individuals with ID are prone to age-related health problems at an earlier age, thus interventions that promote health status are beneficial for them (27). Most adults with ID do not strictly adhere to PA recommendations (28). Considering the above, promoting PA is essential for adults with ID.
The benefits taking part in PA includes enhances cardiorespiratory fitness as well as muscular strength. It contributes significantly to healthy weight loss (29). Another evidence showed that physical activity enhances performance and reduces the incidence of high blood pressure, weight gain, stroke, and blood sugar levels (13, 30). Adults with ID have a declining PA rate, which means they do not exercise enough to achieve optimal health. Sedentary behaviour resulting from poor physical activity is prevalent among adults with ID (25). Other findings have equally shown that adults with ID tend to experience fatigue-related diseases, low fitness levels, and obesity (25, 26) more than the general population health risks and mortality. PA is vital for healthy living because it reduces cardiovascular disease, hypertension, cancer, diabetes, and weight gain (31).
Every adult between 18 and 64 years old should exercise at least 150 min a week irrespective of their health status (32). Nevertheless, adults with ID have a relatively low prevalence of PA in this population subgroup. Individuals with ID participate in approximately 17.5%–33% of the recommended physical activity levels (33). The prevalence of obesity was higher among adults with ID than in adults without ID (34). Physical fitness and cardiovascular endurance are lower in people with ID than those without ID (35). Recognizing the health-promoting implications of PA on psychological well-being is imperative in determining the type, duration, frequency, and approach interventions that will improve quality of life (36). Based on the foregoing, this study was designed to assess and collate global research evidence on using physical activity among adults with ID. This study also examined gender differences in physical activity among adults with ID. Moreover, the review investigated the effect of physical activity on the experimental group. Hence, this study was guided by the following research questions:
1. What are the benefits of physical activity for adults with ID?
2. Is there a significant effect of physical activity on adults with ID based on gender difference?
3. Did physical activity significantly enhance the performance of adults with ID in the experimental group?
Methodology
A search of PubMed, Scopus, PsychINFO, Cochrane library, and Ebsco databases was conducted using keywords and medical subject headings (MeSH). We used the following keywords in isolation and in combination: “physical activity”, “Adults”, “intellectual disability”, “exercise”, “therapy”, “physical health”, “lifestyle factors”, and “Barriers and facilitators”. Initially, no inclusion or exclusion criteria were applied to the literature search (see PRISMA flow chart below).
Selection criteria
This systematic literature review aimed to conduct a systematic review of physical activity: benefits and needs for maintenance of quality of life among adults with intellectual disability. As explained in the section on data reduction, the search resulted in data sets that were then classified into predetermined categories. PRISMA established screening criteria (37). There was no limit to the location of the search. Vickers and Smith (38) found that excluding dissertations or including them did not affect the conclusion of the systematic literature review. All articles were screened independently based on the research objectives.
Outcome of search
Our search identified 735 publications (PubMed, Scopus, PsychINFO, Cochrane library and Ebsco) (see Figure 1). Before searching, we established criteria for including and excluding records. We removed 510 of the 225 articles due to their type, publication stage, source type, and publication language. We further screened the remaining 225 articles for duplication and relevance to the review, resulting in 51 articles being removed. Twenty-five of the remaining 51 articles were excluded based on access to articles, study participants, the scope of the review, and preliminary findings (39). A total of 15 studies were reviewed in full. The study included only original research articles.
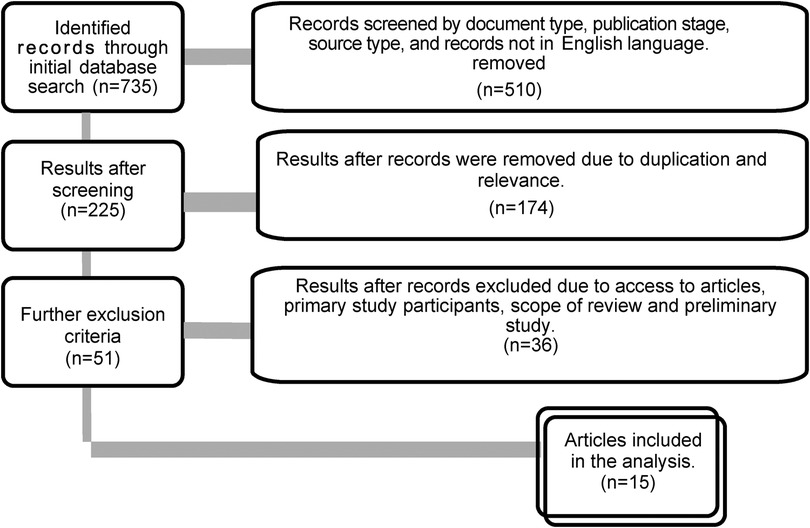
Figure 1. Flowchart of the systematic literature search.
Data extraction
Two raters blind coded the 15 articles using a variety of demographic variables and effects of PA on people with ID (see Table 1 for details). In this study, some measures were coded, including the purpose, sample size (males and females), sampling technique, study design, instrument, and outcomes (pre and post). The information gathered was validated by two experts. All identified studies were evaluated and critiqued by two colleagues with higher degree status.

Table 1. Included studies, sample size, study objectives and major findings.
Description of participants
Table 1 revealed that the included studies were conducted between 2011 and 2022. There were two thousand three hundred and three (2,303) participants in the fifteen (15) studies reviewed. There were 920 participants in the study conducted by Tyrer et al. (50), representing 38.9% of the study participants, which is the study with the highest number of participants. There were 529 respondents in Carbo-Carretéa et al. (40), representing 22.4% of the study participants included in the review. Diz et al. (43) had the least number of participants that is 16 (0.67%), while Kim and Yi (13) had 17 (0.72%) participants. Each other study included less than 1% of the total participants.
The table also showed that the primary participants in 10 (63%) studies were described as adults with ID, while 1 (6%) study participants were young adults with ID. Moreover, four studies used mixed participants. One study (6%) involved adults with ID, their professional service providers, and relatives, while three (19%) involved adults with and without ID. 1 (6%) study had participants with comorbid conditions (adults with intellectual disabilities and obesity).
Study objective
The objectives of the studies included in this review varied significantly. Carbo-Carretéa et al. (40) investigated how perceptions of PA affect the quality of life using eight categories and three higher-level quality-of-life factors. A single-blind, cluster-randomised controlled trial compared a multi-component health education programme to a weight management program (41). Researchers also investigated the impact of physical activities on metabolic syndrome risk factors (13), quality of life, motor proficiency, and fitness levels (43) and fitness levels, self-efficacy, and activity levels (43) among adults with ID.
Melville et al. (42) evaluated the efficacy of TAKE 5, an intervention designed to promote weight loss. The objective of Chow et al. (47) and Oviedo et al. (48) examined the relationship between PA levels and sedentary time, while Hsu et al. (49) examined the correlation between physical fitness and gender, age, degree of ID and sedentary time and PA time. Tyrer et al. (50) and Olsen et al. (51) examined risk factors for multimorbidity, including lifestyle factors. Olsen et al. (51) also considered the relationship between perceptions of health and demographics, degree of ID, weight and PA, and overall health condition. Zwack et al. (52) examined the relationship between reversible risk factors and cardiometabolic profiles. Mitchell et al. (53) examined participants' perceptions of benefits, barriers, and choices in a walking program as part of a study.
Research design
Additionally, the table provides information on the research design used in the studies included in this review. In the review, 7 (43.8%) studies employed a cross-sectional research design (45–51). There are also several other research designs used in the included studies, including accidental, non-randomized sampling (40), randomized controlled studies (41), an open pilot study (42), an experimental study (44), and qualitative studies. It should be noted, however, that 3 (18.8%) of the studies did not specify the research design employed.
Participants gender
Table 1 also showed that 8 (50%) of the included studies indicated the gender of participants while the remaining 8 (50%) did not. 542 (23%) of the participants were identified as male while 424 (18%) were identified as female. The gender of 1,399 (59%) participants was not specified. The number of male participants were more than female by 118. A study had more female that is 32 compare male 22 (42) while another study had the lowest number of female participants that is 4 to male that is 13 (13). It is worth noting that the table also revealed the sampling technique for selection of study participants in the included study and the instrument used for data collection. Two studies collected data on body index mass of participants (42, 46, 48). A study employed semi-structured interviews or focus groups for data collection (53). Self-efficacy scale was used in one study (44). A scale for assessing physical activity known as accelerometers was used in three studies (44, 46, 48). In one study physical activity was monitored for 7 days using an ActiGraph GT3X monitor (49).
Sampling technique
Five studies used convenient sampling technique for the selection of participants in the study (43, 45–47, 53). Purposive sampling technique was adopted in three studies for participants selection (44, 48, 50). However, 5(38%) of the included studies describe the procedure for sampling but did not specify the sampling technique (13, 40–42).
Culminative main findings
Benefits of physical activity
Improved quality of life
The results revealed high values for PA, especially for the well-being factor (Carbo-Carretéa et al. (40) and the relationship between fitness and health was significant (44). The correlation between physical activity and muscular strength, endurance, total cholesterol, low-density lipoprotein cholesterol, and disability rating was confirmed (13). Despite being not statistically significant, Diz et al. (43) found that the PA program appears to have a moderate positive impact on QOL: experimental group participants reported better scores in both versions. Font-Farré (45) results showed that differences in heart rate variability variables between groups were insignificant. According to Hsu et al. (49) flexibility and endurance were associated with more light-intensity PA (LPA).
Weight loss
In persons with ID, disability ratings, glycated haemoglobin, and physical activity levels were correlated by 73.9% (13). Subjects' demographic variables and activity levels differed significantly (P0.001), but not their age or body mass index. The exploratory efficacy analysis by Harris et al. (41) revealed that at 12 months, nearly five times as many participants in TAKE 5 (50·0%) achieved 5%–10% weight loss, compared to Waist Winners Too (20·8%). Adults with ID and obesity can benefit from an energy deficit diet incorporated into a multi-component programme for weight loss. Melville et al. (42) concluded that weight (mean difference) decreased significantly (−4·47), body mass index (−1·82) and waist circumference (−6·29) where P < 0·0001 and participants' daily sedentary behaviour (−41·40) where P = 0·00034. In addition, thirteen participants (36%) lost at least 5% of their original body weight after the intervention. Diz et al. (43) showed that physical activity improved balance and strength. However, the improvement could have been more significant, allowing for enhanced performance in everyday activities like sitting and walking.
Sedentary life
Oviedo et al. (48) reported that the study provides a more comprehensive understanding of PA levels and sedimentary time in groups of active and inactive adults with and without ID. It is consistent with other studies that, regardless of gender or age, adults with ID are more sedentary and perform less light PA (54, 55). Oviedo et al. (46)) found that adults with ID were more physically active than older adults with ID regarding moderate-to-vigorous PA, but there was no difference in ST. The influence of moderate to vigorous PA on total PA was similar in previous studies with the general population and with individuals with ID (56, 57).
A significant difference was not observed in physical activity, sedentary behaviour, and physical fitness variables between non-overweight/nonobese (BMI < 23) or obese (BMI ≥ 23) people, nor was there any difference between those at low and high risks for central obesity (47). Furthermore, Oviedo et al. (48) found that participants with ID tended to engage in more bouts of sedentary behaviour per day, regardless of gender or age, compared to participants without ID. Some underlining factors may contribute to this. Depending on the centre, participants with ID will take similar scheduled breaks, such as tea and lunchtime. It is also important to note that adults with ID have less opportunity to participate in PA after work.
The likelihood of multimorbidity increased with physical inactivity or sedentary behaviour, regardless of age, gender, the severity of ID, ethnicity, or socioeconomic status (50). Researchers found that sedentary behaviour, not physical activity, still negatively affected health (50) even when lifelong conditions were excluded. Additionally, this population's nutrition and physical activity knowledge appear to significantly predict cardiometabolic risk (52). Oviedo et al. (46) found that light PA values were similar to those reported by Philips & Holland (57) but higher than those found by Melville et al. (42). The difference with Melville et al. (42) stems from the fact that the participants in that study were four years older with a BMI ≥ 30 kg/m2.
Effect on physical activity based on gender difference
Oviedo et al. (48) revealed that females from the group without intellectual disability engaged in more physical activity than females from the non-activity group with ID. As a result of the lack of participation in physical activity programs and the low-intensity tasks conducted at centres, the total physical activity of females with ID was lower. Physical fitness variables, except for body fat percentage, did not differ by sex during a 6-minute walk, arm curl, and sit-and-reach test (47). However, Hsu et al. (49) reported that female gender above 39 years old were associated with lower performance in multiple aspects of physical fitness.
According to Oviedo et al. (46), males and females did not have different PA levels or ST. Based on these results, older males and females in Oviedo et al. (46) should engage in activities specific to their age and gender to increase their PA levels. In univariate analyses, the number of PA conditions, lower motor function, and multiple physical activity indicators correlated with poor health ratings (51). Oviedo et al. (46) found that females in the non-ID group performed higher amounts of total PA than those in the non-active group.
There was a significant difference between male and female participants regarding abdominal muscular endurance and grip strength; these results are consistent with research suggesting that men with ID have higher muscular strength and endurance (58). It has been found, however, that women with ID have less cardiorespiratory endurance (59) and greater flexibility (58). Oviedo et al. (46) found no statistically significant differences between genders for the parameters studied. This supported the findings of Gawlik et al. (59) that aerobic capacity calculated per kilogram of body weight did not differ by gender.
Effect of physical activity on experimental group
The experimental group significantly enhanced muscle endurance, self-efficacy, and levels of physical activity (43). Diz et al. (43) observed that controls impair children's physical development, responsibility, and socialisation and negatively affect their interpersonal interactions. A significant difference was found between participants in the experimental group, although effect sizes tended to be moderate, indicating better performance following the program.
Diz et al. (43) reported that after the program, the experimental group participants reported higher levels of satisfaction, despite the higher levels of social inclusion, individual autonomy, intellectual development, and general well-being reported in the control group initially and in the self-report version. The proxy version assumes greater values only for the control group's interpersonal relationships and emotional well-being domains. Neither age nor body mass index was significantly correlated with differences in demographic variables or activity levels (13).
Discussion of finding
This systematic review evaluates the physical activity benefits and needs of adults with ID. The predetermined inclusion criteria were met by 15 of the 1,005 studies identified as potentially relevant. This review has identified various ways physical activity can be of benefit and use to ensure an improved quality of life among persons with ID. The use of physical activity as an intervention group varied significantly between the studies in terms of content, structure, and duration. The studies did not use a single outcome measure. In the studies, intellectual disability was referred to using relatively consistent terminology. Three studies used a purposive sampling technique, while five used a convenient sampling.
The results from the meta-analysis show variation in the effect of PA on quality of life of adults with ID. The prevalence of factors related to well-being and fitness was high (40, 44). It is partially consistent with the results of Calders et al. (60), which showed that exercise improved muscle endurance, strength, and cardiovascular endurance in adults with ID after 20 weeks. Jo et al. (44) reported significantly different results from Wu et al. (61). The exercise intervention in Jo et al. (44) was shorter and less intense than Wu et al. (61), a 6-month exercise intervention. There may also be a difference because previous studies used different measurement tools.
Several factors make it difficult to generalize the participants' PA levels to the general population of adults with ID. This review's data were derived from a selective sample, which doesn't seem to represent the ID community, so their activity levels were likely higher than those of the general ID population. The study design and instruments for data collection varied significantly. Additionally, the duration of the included studies varied widely from as low as 7 days to as long as 12 months. Although, the study by Carbo-Carretéa et al. (40) confirmed that physical activity perceptions and individualized support habits are associated with improved quality of life.
Diz et al. (43) concluded that controls showed a better adaptive profile in most adaptive domains, except for time and numbers, sexual behaviour, and social interaction. This group's scores remained the same over time, while the experimental group's performance improved in most areas. As a result, Kim and Yi (13) advocated for more research on improving and enhancing physical activities in sheltered workshops, where adults with ID receive the most supervision and guidelines for maintaining their health. Physical activity and fitness variables did not differ significantly between mild and moderate ID (47). Carbó-Carretéa et al. (40) show that identifying support needs and providing appropriate strategies in PA is associated with enhanced outcomes for individuals.
The benefits of physical activity include improving strength and reducing the prevalence of chronic diseases, including hypertension, obesity, stroke, and diabetes (30). Physical activity improves strength and reduces chronic diseases such as hypertension, obesity, strokes, and diabetes (30). The difficulty of carrying out daily activities, avoiding movement, and becoming physically inactive is common among individuals with disabilities. Since they cannot participate in the same amount of physical activity as adults without disabilities, their weight and metabolic syndrome frequencies increase (62). If this inactivity continues into adulthood, metabolic syndrome and related chronic diseases will likely develop (13).
It was found that the improvements continued a month after the program ended despite a slight decline in retention assessments (43). Despite this, there were significant improvements in effort items, concentration, and agility. There were four overarching themes identified by Mitchell et al. (53): perceived benefits of participating in the programme, perceived disadvantages, walking options, and resources for walking. Participants reported positive experiences with the programme, despite no significant increase in walking. An integrated weight management programme for adults with intellectual disabilities can be tested in a full-scale trial (41). Researchers recruited adults with all levels of intellectual disabilities using the multi-point recruitment strategy, which overcame barriers to recruitment for adults with ID.
There were no statistically significant differences in testing the homogeneity between the experimental and control groups (44). Consequently, the researchers concluded that there were no initial differences in the data. Font-Farré et al. (45) concluded that differences between groups in heart rate variability were not significant. Results showed that participants without ID had significantly better heart rate kinetics during recovery than those with ID.
Conclusion
This study reviewed PA therapies delivered by different specialists for adults with ID. Further research is needed to determine whether PA programs lead to positive outcomes among adults with ID. The findings of our study cannot be directly compared to those of existing studies. Promoting regular PA engagement among adults with ID should be put forward on national and international agenda and considered non-pharmacological support for a more active life and a healthier lifestyle. As a result of reviewing fifteen studies, the authors found that the treatment had varied significant effects on individuals with intellectual disabilities, including weight loss, sedentary behaviour, and improved quality of life for individuals with intellectual disabilities. Based on physical activity, tests of abdominal muscular endurance and grip strength were also statistically different between males and females.
The findings highlight the importance of actively participating in research and considering the complexities of PA for individuals with ID. In addition, caregivers, stakeholders, and other community members must be informed about PA's benefits for adults with ID. A larger sample size is necessary to establish a generalizable conclusion for future research. Based on an existing review, there is evidence that interventions for individuals with ID are effective. Consequently, our review complements the findings of other reviews and is highly relevant to the needs and benefits of physical activity for adults with ID. Our review has several limitations, which should be noted. We only included open-access publications due to resource limitations. Secondly, we used a reductionist approach, excluding articles that were not about PA interventions for adults with ID.
Additionally, a publication bias remains since we excluded publications in journals and books (excluding studies that are in press). This review did not allow the analysis of possible mediating and moderating factors that may contribute to barriers to PA for adults with ID because of maximizing study homogeneity.
Author contributions
UJ, TO and AA: contributed to the conception and design of the study. UJ: conducted the systematic literature search and study selection and extracted the data. UJ and TO: performed the quality assessment. UJ: wrote the initial draft of the manuscript. EJ and JP: reviewed the manuscript while TO design sections of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the South African Research Chairs Initiative of the Department of Science and Innovation and National Research Foundation of South Africa, South African Research Chair in Education and Care in Childhood, Faculty of Education, University of Johannesburg, South Africa (grant number: 87300, 2017).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Luckasson R, Borthwick-Duffy S, Buntinx WHE, Coulter DL, Craig EM, Reeve A, et al. Mental retardation: Definition, classification, and systems of supports (10th ed.). AAMR. (2002). doi: 10.1016/S0160-2896(03)00012-6
2. Schalock RL, Luckasson R, Tassé MJ. Intellectual disability: Definition, classification, and systems of supports. 12th Edn. Washington, USA: American Association on Intellectual and Developmental Disabilities (2021).
3. Harris JC, Greenspan S. Definition and nature of intellectual disability. In: Singh N, editors. Handbook of evidence-based practices in intellectual and developmental disabilities. Georgia, USA: Springer (2016). p. 11–39.
4. American Psychiatric Association, DSM-5 Task Force. Diagnostic and statistical manual of mental disorders: DSM-5™. 5th ed. American Psychiatric Publishing, Inc (2013). doi: 10.1176/appi.books.9780890425596
5. World Health Organisation W. Health Topics Online (2015) Available at: http://www.euro.who.int/en/health-topics/noncommunicable-diseases/mental-health/news/news/2010/15/childrens-right-to-family-life/definition-intellectual-disability
6. Cowen P, Harrison P, Burns T. Shorter Oxford textbook of psychiatry. 6th ed. Oxford: Oxford University Press (2013).
7. While AE, Clark LL. Overcoming ignorance and stigma relating to intellectual disability in healthcare: a potential solution. J Nurs Manag. (2010) 18:166–72. doi: 10.1111/j.1365-2834.2009.01039.x
8. Maulik PK, Mascarenhas MN, Mathers CD, Dua T, Saxena S. Prevalence of intellectual disability: a meta-analysis of population-based studies. Res Dev Disabil. (2011) 32(2):419–36. doi: 10.1016/j.ridd.2010.12.018
9. Emerson E, Hatton C. Socioeconomic disadvantage, social participation and networks and the self-rated health of English men and women with mild and moderate intellectual disabilities: cross sectional survey. Eur J Public Health. (2008) 18(1):31–7. doi: 10.1093/eurpub/ckm041
10. Temple VA, Frey GC, Stanish HI. Physical activity of adults with mental retardation: review and research needs. Am J Health Promot. (2006) 21(1):2–12. doi: 10.1177/089011710602100103
11. Salvador-Carulla L, Reed GM, Vaez-Azizi LM, Cooper SA, Martinez-Leal R, Bertelli M, et al. Intellectual developmental disorders: towards a new name, definition and framework for “mental retardation/intellectual disability” in ICD-11. World Psychiatry. (2011) 10(3):175–80. doi: 10.1002/j.2051-5545.2011.tb00045.x
12. Doran CM, Einfeld SL, Madden RH, Otim M, Horstead SK, Ellis LA, et al. How much does intellectual disability really cost? First estimates for Australia. J Intellect Dev Disabil. (2012) 37(1):42–9. doi: 10.3109/13668250.2011.648609
13. Kim JY, Yi ES. Analysis of the relationship between physical activity and metabolic syndrome risk factors in adults with intellectual disabilities. J Exerc Rehabil. (2018) 14(4):592–7. doi: 10.12965/jer.1836302.151
14. Frey GC, Stanish HI, Temple VA. Physical activity of youth with intellectual disability: review and research agenda. Adapt Phys Activ Q. (2008) 25(2):95–117. doi: 10.1123/apaq.25.2.95
15. Boyle CA, Yeargin-Allsopp M, Doernberg NS, Holmgreen P, Murphy CC, Schendel D. Prevalence of selected developmental disabilities in children 3–10 years of age: the metropolitan Atlanta developmental disabilities surveillance program, 1991. Morb Mortal Wkly Rep. (1996) 45(SS-2):1–14.
16. National Center on Birth Defects and Developmental Disabilities. Data and statistics for cerebral palsy. Centers for Disease Control and Prevention (2022). https://www.cdc.gov/ncbddd/cp/data.html
17. Honeycutt AA, Grosse SD, Dunlap LJ, Schendel DE, Chen H, Brann E, et al. Economic costs of mental retardation, cerebral palsy, hearing loss, and vision impairment. In: Altman BM, Barnartt SN, Hendershot GE, Larson SA, editors. Using Survey Data to Study Disability: Results from the National Health Survey on Disability (Research in Social Science and Disability, Vol. 3). Bingley: Emerald Group Publishing Limited. (2003) pp. 207–28. doi: 10.1016/S1479-3547(03)03011-2
18. Fernhall B, Pitetti KH. Limitations to physical work capacity in individuals with mental retardation. Clin Exerc Physiol. (2001) 3:176–85.
19. Lin JD, Lin PY, Lin LP, Chang YY, Wu SR, Wu JL. Physical activity and its determinants among adolescents with intellectual disabilities. Res Dev Disabil. (2010) 31(1):263–69. doi: 10.1016/j.ridd.2009.09.015
20. Hsieh K, Heller T, Bershadsky J, Taub S. Impact of adulthood stage and social-environmental context on body mass index and physical activity of individuals with intellectual disability. Intellect Dev Disabil. (2015) 53(2):100–13. doi: 10.1352/1934-9556-53.2.100
21. Howie EK, Pate RR. Physical activity and academic achievement in ahildren: a historical perspective. JSHS. (2012) 1:160–69. doi: 10.1016/j.jshs.2012.09.003
22. Mahy J, Shields N, Taylor NF, Dodd KJ. Identifying facilitators and barriers to physical activity for adults with Down syndrome. J Intellect Disabil Res. (2010) 54(9):795–805. doi: 10.1111/j.1365-2788.2010.01308.x
23. Santos S. Psychomotor therapy and intellectual disability in Portugal: from 0 to 100. Int J Psy Neurosci. (2017) 3:22–37. https://www.peertechzpublications.com/articles/JNPPR-5-160.php
24. Woolf S, Woolf C, Oakland T. Adaptive behaviour among adults with intellectual disabilities and its relationship to community independence. Intellect Dev Disabil. (2010) 48(3):209–15. doi: 10.1352/1944-7558-48.3.209
25. Draheim CC, Williams DP, McCubbin JA. Prevalence of physical inactivity and recommended physical activity in community-based adults with mental retardation. Ment Retard. (2002) 40(6):436–44. doi: 10.1352/0047-6765(2002)040%3C0436:POPIAR%3E2.0.CO;2
26. Grondhuis SN, Aman MG. Overweight and obesity in youth with developmental disabilities: a call to action. J Intellect Disabil Res. (2014) 58(9):787–99. doi: 10.1111/jir.12090
27. Brooker K, van Dooren K, McPherson L, Lennox N, Ware R. A systematic review of interventions aiming to improve involvement in physical activity among adults with intellectual disability. J Phys Act Health. (2015) 12(3):434–44. doi: 10.1123/jpah.2013-0014
28. Peterson JJ, Janz KF, Lowe JB. Physical activity among adults with intellectual disabilities living in community settings. Prev Med. (2008) 47:101–6. doi: 10.1016/j.ypmed.2008.01.007
29. Warburton DE, Nicol C, Bredin SS. Health benefits of physical activity: the evidence. Can Med Assoc J. (2006) 174:801–9. doi: 10.1503/cmaj.051351
30. Taylor D. Physical activity is medicine for older adults. Postgrad Med J. (2014) 90(1059):26–32. doi: 10.1136/postgradmedj-2012-131366
31. U.S. Department of Health and Human Services. Physical activity and health: a report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion (1996). https://profiles.nlm.nih.gov/101584932X106
32. World Health Organization. Global Recommendations on Physical Activity for Health WHO. Geneva (2010). https://www.who.int/publications/i/item/9789241599979
33. Heller T, McCubbin JA, Drum C, Peterson J. Physical activity and nutrition health promotion interventions: what is working for people with intellectual disabilities? Intellect Dev Disabil. (2011) 49(1):26–36. doi: 10.1352/1934-9556-49.1.26
34. Rimmer JH, Chen MD, McCubbin JA, Drum C, Peterson J. Exercise intervention research on persons with disabilities: what we know and where we need to go. Am J Phys Med Rehabil. (2010) 89(3):249. doi: 10.1097/PHM.0b013e3181c9fa9d
35. Lotan M, Isakov E, Kessel S, Merrick J. Physical fitness and functional ability of children with intellectual disability: effects of a short-term daily treadmill intervention. Sci World J. (2004) 4:449–57. doi: 10.1100/tsw.2004.97
36. Ogg-Groenendaal M, Hermans H, Claessens B. A systematic review on the effects of exercise interventions on challenging behaviour for people with intellectual disabilities. Res Dev Disabil. (2014) 35:1507–17. doi: 10.1016/j.ridd.2014.04.003
37. Ghafari M, Baigi V, Cheraghi Z, Doosti-Irani A. Correction: the prevalence of asymptomatic bacteriuria in Iranian pregnant women: a systematic review and meta-analysis. PLoS One. (2016) 11(10):e0165114. doi: 10.1371/journal.pone.0165114
38. Vickers AJ, Smith C. Incorporating data from dissertations in systematic reviews. Int J Technol Assess Health Care. (2000) 16(2):711–3. doi: 10.1017/S0266462300101278
39. Kretzmann M, Shih W, Kasari C. Improving peer engagement of children with autism on the school playground: a randomized controlled trial. Behavioural Therapy. (2015) 46(1):20–8. doi: 10.1016/j.beth.2014.03.006
40. Carbó-Carretéa M, Guàrdia-Olmos J, Giné C, Schalock RL. A structural equation model of the relationship between physical activity and quality of life. Int J Clin Health Psyc. (2016) 16(2):147–56. 0.1016/j.ijchp.2015.11.001
41. Harris L, Hankey C, Jones N, Pert C, Murray H, Tobin J, et al. A cluster randomised control trial of a multi-component weight management programme for adults with intellectual disabilities and obesity. Br J Nutr. (2017) 118(3):229–40. doi: 10.1017/S0007114517001933
42. Melville CA, Boyle S, Miller S, Macmillan S, Penpraze V, Pert C, et al. An open study of the effectiveness of a multi-component weight-loss intervention for adults with intellectual disabilities and obesity. Br J Nutr. (2011) 105(10):1553–62. doi: 10.1017/S0007114510005362
43. Diz S, Gomes F, Santos S. Does physical activity improve adaptive behaviour, fitness, and quality of life of adults with intellectual disability?. Rev Bras Ciênc. (2021) Esporte 4. doi: 10.1590/rbce.43.e001621
44. Jo G, Rossow-Kimball B, Lee Y. Effects of 12-week combined exercise program on self-efficacy, physical activity level, and health related physical fitness of adults with intellectual disability. J Exerc Rehabil. (2018) 14(2):175–82. doi: 10.12965/jer.1835194.597
45. Font-Farré M, Farche A, de Medeiros Takahashi AC, Guerra-Balic M, Figueroa A, Oviedo GR. Cardiac autonomic modulation response before, during, and after submaximal exercise in older adults with intellectual disability. Front Physiol. (2021) 12:702418. doi: 10.3389/fphys.2021.702418
46. Oviedo GR, Travier N, Guerra-Balic M. Sedentary and physical activity patterns in adults with intellectual disability. Int J Environ Res Public Health. (2017) 14(9):1027. doi: 10.3390/ijerph14091027
47. Chow BC, Choi P, Huang W. Physical activity and physical fitness of adults with intellectual disabilities in group homes in Hong Kong. Int J Environ Res Public Health. (2018) 15(7):1370. doi: 10.3390/ijerph15071370
48. Oviedo GR, Tamulevicius N, Guerra-Balic M. Physical activity and sedentary time in active and non-active adults with intellectual disability: a comparative study. Int J Environ Res Public Health. (2019) 16(10):1761. doi: 10.3390/ijerph16101761
49. Hsu PJ, Chou HS, Pan YH, Ju YY, Tsai CL, Pan CY. Sedentary time, physical activity levels and physical fitness in adults with intellectual disabilities. Int J Environ Res Public Health. (2021) 18(9):5033. doi: 10.3390/ijerph18095033
50. Tyrer F, Dunkley AJ, Singh J, Kristunas C, Khunti K, Bhaumik S, et al. Multimorbidity and lifestyle factors among adults with intellectual disabilities: a cross-sectional analysis of a UK cohort. J Intellect Disabil Res. (2019) 63(3):255–65. doi: 10.1111/jir.12571
51. Olsen MI, Halvorsen MB, Søndenaa E, Langballe EM, Bautz-Holter E, Stensland E, et al. How do multimorbidity and lifestyle factors impact the perceived health of adults with intellectual disabilities? J Intellect Disabil Res. (2021) 65(8):772–83. doi: 10.1111/jir.12845
52. Zwack CC, McDonald R, Tursunalieva A, Lambert GW, Lambert EA. Exploration of diet, physical activity, health knowledge and the cardiometabolic profile of young adults with intellectual disability. J Intellect Disabil Res. (2022) 66(6):517–32. doi: 10.1111/jir.12917
53. Mitchell F, Stalker K, Matthews L, Mutrie N, Melling C, McConnachie A, et al. A qualitative exploration of participants’ experiences of taking part in a walking programme: perceived benefits, barriers, choices and use of intervention resources. J Appl Res Intellect Disabil. (2018) 31(Suppl 1):110–21. doi: 10.1111/jar.12326
54. Melville CA, McGarty A, Harris L, Hughes-McCormack L, Baltzer M, McArthur LA, et al. A population-based, cross-sectional study of the prevalence and correlates of sedentary behaviour of adults with intellectual disabilities. J Intellect Disabil Res. (2018) 62(1):60–71. doi: 10.1111/jir.12454
55. Shields N, Synnot AJ, Barr M. Perceived barriers and facilitators to physical activity for children with disability: a systematic review. Br J Sports Med. (2012) 46(14):989–97. doi: 10.1136/bjsports-2011-090236
56. Dixon-Ibarra A, Lee M, Dugala A. Physical activity and sedentary behavior in older adults with intellectual disabilities: a comparative study. Adapt Phys Activ Q. (2013) 30(1):1–19. doi: 10.1123/apaq.30.1.1
57. Phillips AC, Holland AJ. Assessment of objectively measured physical activity levels in individuals with intellectual disabilities with and without Down's syndrome. PLoS One. (2011) 6(12):e28618. doi: 10.1371/journal.pone.0028618
58. Skowronski W, Horvat M, Nocera J, Roswal G, Croce R. Eurofit special: european fitness battery score variation among individuals with intellectual disabilities. Adapt Phys Activ Q. (2009) 26(1):54–67. doi: 10.1123/apaq.26.1.54
59. Gawlik K, Zwierzchowska A, Manowska B, Celebańska D. Aerobic capacity of adults with intellectual disabilities. Ann Agric Environ Med. (2016) 24(1):117–20. doi: 10.5604/12321966.1233999
60. Calders P, Elmahgoub S, Roman De Mettelinge T, Vandenbroeck C, Dewandele I, Rombaut L, et al. Effect of combined exercise training on physical and metabolic fitness in adults with intellectual disability: a controlled trial. Clin Rehabil. (2011) 25(12):1097–108. doi: 10.1177/0269215511407221
61. Wu CL, Lin JD, Hu J, Yen CF, Yen CT, Chou YL, et al. The effectiveness of healthy physical fitness programs on people with intellectual disabilities living in a disability institution: six-month short-term effect. Res Dev Disabil. (2010) 31(3):713–7. doi: 10.1016/j.ridd.2010.01.013
62. Carroll DD, Courtney-Long EA, Stevens AC, et al.. Vital signs: disability and physical activity--United States, 2009-2012. MMWR Morb Mortal Wkly Rep. (2014) 63(18):407–13. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5779402/24807240
Keywords: physical activity, interventions, intellectual disability, benefits, quality of life
Citation: Jacob US, Pillay J, Johnson E, Omoya Oluwatomilayo (Tomi) and Adedokun AP (2023) A systematic review of physical activity: benefits and needs for maintenance of quality of life among adults with intellectual disability. Front. Sports Act. Living 5:1184946. doi: 10.3389/fspor.2023.1184946
Received: 12 March 2023; Accepted: 22 May 2023;
Published: 8 June 2023.
Edited by:
Ricardo Ferraz, University of Beira Interior, PortugalReviewed by:
Bolanle Oyundoyin, Federal University of Agriculture, NigeriaAdigun Timothy Olufemi, University of Zululand, South Africa
Christopher Omoregie, University of Eswatini, Eswatini
© 2023 Jacob, Pillay, Johnson, Omoya and Adedokun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Udeme Samuel Jacob dWRlbWUwMUBnbWFpbC5jb20=