 Stephan Becker*
Stephan Becker* Steven Simon*
Steven Simon* Josefine HayerJana Heidger
Josefine HayerJana Heidger Wjatscheslaw Koltschin
Wjatscheslaw Koltschin Carlo Dindorf
Carlo Dindorf Jonas Dully
Jonas Dully Michael Fröhlich
Michael Fröhlich
- Department of Sports Science, RPTU University of Kaiserslautern-Landau, Kaiserslautern, Germany
Background: Sensorimotor foot orthoses (SMFO) may be a helpful intervention to improve balance by enhancing proprioceptive input within the sensorimotor control loop. SMFO intervention could have beneficial effects on reducing risk of ankle sprains and falls.
Methods: A total of 57 healthy adults (age: 48.5 ± 11.8 years) completed a static balance test (30 s) on a force plate, with open eyes (OE) and closed eyes (CE). Balance performance was assessed by using posturography to measure the sway area (mm2), under SMFO and no foot orthoses (NFO) conditions.
Results: Descriptive statistics show a reduced median of 1.9 cm2 (29.6%) for SMFO with CE. No interaction was found, while main effects showed significant differences (vision: p < 0.001, sole: p = 0.004). post-hoc tests underlined these results and static balance improved by a median 0.8 cm2 (14.5%) with SMFO compared to NFO.
Conclusion: The SMFO seems to support static balance and sensorimotor system, which could help to avoid falls and injuries as ankle sprains. Further age groups, long-term effects and the impact on dynamic balance must be studied.
1 Introduction
Balance is a fundamental ability, involved in almost all human movements and plays a central role in regulating of our posture (1). As a human being is not a rigid structure, gravitational forces and natural internal fluctuations, which can be generated by breathing, for example, must be compensated for by adequate muscle reactions while standing (2). Owing to the human bipedal stance and relatively high center of gravity, humans already have demanding prerequisites for maintaining balance (3).
Balance is also considered to be of great importance in injury prevention (4). A poor sense of balance can increase the risk of injury (5) and functional ankle instability (6). Older people are also more likely to fall because of poorer vestibular sense, among other factors (7). One explanation for the importance of balance with regard to injury prevention and fall prevention is that balance is controlled by the sensorimotor control circuit in addition to the vestibular organs (8). In addition to the visual and vestibular senses, the sensorimotor control circuit also includes various exteroceptors and proprioceptors that inform the CNS via afferent pathways regarding the sensory signals that are received, for example, via the sole of the foot or changes in muscle tension (4). The sum of the incoming feedback is processed subconsciously in the CNS, and the body reacts muscularly to achieve the desired state, by comparing the predicted and actual states (9, 10). The better the sense of balance, the faster the processing sensory information (4).
Balance training is a proven method to improve balance (1, 11) and reduce injuries (12) and functional ankle stability (13). However, not all people get to train regularly. Therefore, the potential added value of sensorimotor foot orthoses (SMFO) is increasingly coming into focus (14). The primary aim of SMFO is to change the foot kinetics and kinematics in a defined manner (tonus increase or tonus decrease) via specific elements at a certain point in the step cycle (15–17). The insole utilizes the exteroceptors and proprioceptors, which are stimulated by the SMFO elements. From the authors’ point of view, the combination of a toe bar and retrocapital could have a positive influence on balance. Combining both elements supposedly increases plantar flexor tension (15). The plantar flexors are the central control elements for static balance (7). In addition, the toe bar causes the toes to lay down, particularly if a person tends to curl their toes, which can increase the contact surface of the toes. With an increased contact area, the input of sensory information from exteroceptors in the skin could increase, which would be beneficial for balance (4, 14). SMFO has been used in practice for many years and was investigated for the first time in 2013 by a research group from Japan (18). Even though its use in practice has generated a lot of positive feedback, there is a need for evidence-based research into the postulated effect of the combination of the two elements.
To date, no studies have investigated the effects of SMFO on balance. However, some studies have investigated the influence of textured insoles on balance (19) and demonstrated that balance can be positively affected by changing afferent information from the foot sole (20).
Several validated methods exist for assessing balance, with computer-assisted posturography being a recognized static procedure, commonly referred to as the postural stability test (21, 22). Using a force plate, changes in the center of mass (COM) can be assessed using the center of pressure (COP), which is also observed in healthy individuals while standing completely still (23). A common issue seen in individual balance abilities, both static and dynamic, is the over-reliance on the visual sense (24–26). Without input from the visual receptors in the sensorimotor control circuit, many individuals struggle to attain similar balance measurement values (4, 27).
This study aimed to investigate the influence of SMFO on static balance in healthy adults. Using a randomized cross-over design, participants completed a posturographic balance measurement with SMFO and with no foot orthosis (NFO). We tested the following hypotheses:
• Wearing SMFO improves static balance during a 30 s measurement with open eyes (OE) and with closed (CE) compared to NFO.
The literature shows that, to date, there has been no study on balance with SMFO, which seems to be a promising intervention method that has been on the market for many years. Demographic changes, the growing number of elderly people, and the increasing social importance of injury prevention in general also support the value of such supportive measures. However, the necessary evidence must first be provided, which is why the first step should be to look at whether there are general effects of the SMFO on the balance in healthy people, regardless of a specific indication, being the next step.
2 Methods
2.1 Participants
A sample size was prior calculated using G*power (Version 3.1.9.6 for Macintosh, University of Kiel, Germany) for t-tests between two dependent means (matched pairs; effect size d = 0.5, 2 ToMs, α error probability = 0.05, power: 0.95). A minimum group size of 45 individuals was calculated. To account for potential dropouts, a total of 57 participants (sex: 28♀, 29 ♂; age: 48.5 ± 11.8 years; height: 1.73 ± 0.1 m; weight: 79.1 ± 15.2 kg; body mass index: 26.3 ± 4.0 kg/m2) were included in this crossover randomized controlled study. This study was conducted in accordance with the current guidelines of Declaration of Helsinki and was approved by the responsible ethics commission (No. 55). All participants provided written informed consent after receiving a full explanation of the study and agreeing to the participation and publication of the results.
The inclusion criterion was age >30 years, when postural balance starts declining (28, 29). The youngest participant was 30 years old, and the oldest participant was 68 years old. The exclusion criteria were diabetes mellitus, rheumatic diseases, and neurological disorders of the musculoskeletal system. Additionally, individuals with an acute foot or ankle injury in the past eight weeks were excluded. These exclusion criteria were selected because of their potential influence on balance. As this is the first study on SMFO and balance, a healthy sample was selected in order to check whether effects can already be seen here.
2.2 Foot orthoses
SMFOs were manufactured according to the Woltring/Springer and built using ethylene-vinyl acetate (EVA) material with a shore hardness of 35 by the same and experienced orthopedic shoe technician. The medial and lateral elements were grounded to prevent muscle activation or stabilization. In contrast, the toe bar (7.5–8.1 mm) and retrocapital pad (8.7–9.5 mm) were constructed in relation to the shoe size and not individually manufactured. The exact structure and the height ranges of the elements are given in Figure 1.
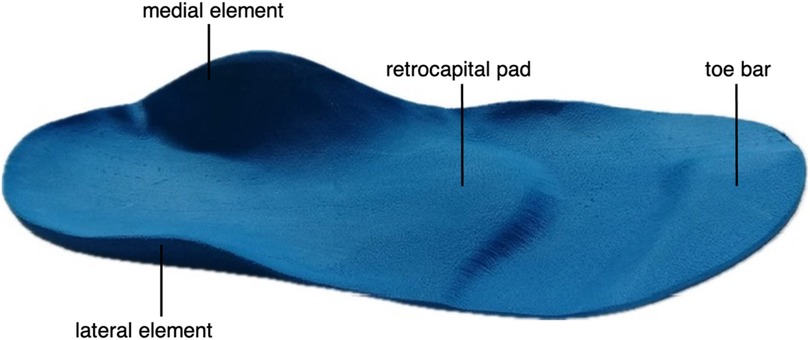
Figure 1. The SMFOs used in this study.
2.3 Procedure
First, we randomly determined whether a person started an SMFO or NFO. Next, we randomly determined whether static balance was measured with OE or CE. Figure 2 illustrates the exact procedure followed after randomization. Measurements were conducted in the private setting for each participant using neutral shoes (model: Samba, Adidas AG, Herzogenaurach, Germany) with flat soles and without arch support. Static balance was analyzed using a posturographic measurement of 3 × 30 s (OE and CE) on a mobile force plate (model: GP Multisens, version: MS4, go-tec GmbH, Münster, Germany). The plate features 2.304 resistance sensors over a 39 × 39 cm surface (2 sensors per cm²) with a sampling rate of 200 Hz. Data processing and visualization were performed using the GP Manager (version 7, Go-tec GmbH, Münster, Germany) to derive the movement of the center of pressure, known as the area of the ellipse of the sway area (cm2). Out of the three tests performed for each of the conditions [SMFO (OE, CE); NFO (OE, CE)] mean value was used for the statistical analysis. The pressure plate was positioned facing the wall to reduce distraction. The measurements were performed without acoustic disturbances. The participants positioned themselves in a hip-width stance with the same stand width between the tests. The head was in an upright position, looking straight ahead, and the arms were relaxed on their sides. The participants were instructed to stand as still as possible and to visually fixate on a point on a wall during the tests with OE. The investigator and the display were outside of the field of view to ensure that there was no distraction and, in particular, no visual feedback on the movements of the COP.
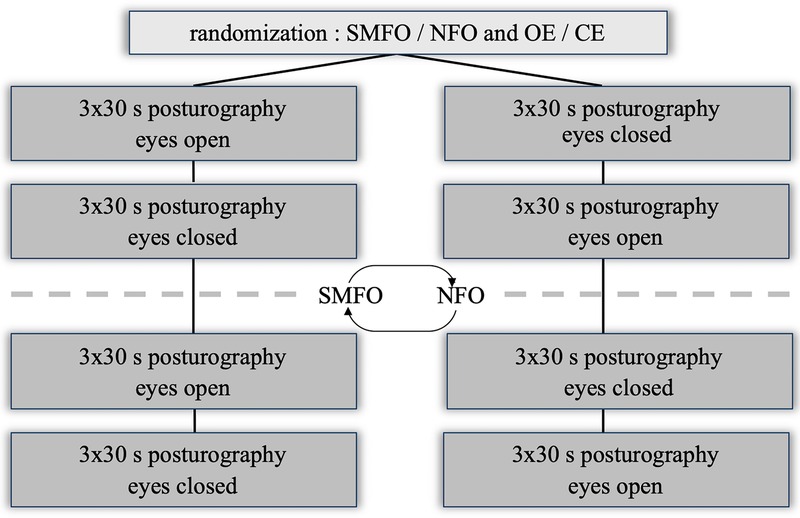
Figure 2. Study design. Test procedure (SMFO, sensorimotor foot orthoses; NFO, no foot orthoses; OE, open eyes; CE, closed eyes).
2.4 Statistics
Statistical analyses were performed in R (version 4.4.2). The results are expressed as mean values ± standard deviations and 95% confidence intervals. Both, the orthoses (SMFO, NFO) and the setting (OE, CE) were seen as repeated measures factors. The various conditions were calculated in one model based common procedure in this discipline (30). Since the data violated normal distribution (31), a LD-F2 design with ANOVA-Type statistics was calculated using the R package nparLD (32) with effect sizes eta². Significant effects were post-hoc tested with a Wilcoxon signed-rank test with Pearson's r effect size. Statistical significance was set at p < 0.05. The outliers were evaluated by experts and found to be systematic. This was also confirmed by the methodological procedure, which always included the best of three attempts for all conditions in the statistics.
3 Results
The descriptive statistics showed a reduction in the sway area while wearing SMFOs compared to NFO for OE and CE (Figure 3; Table 1).
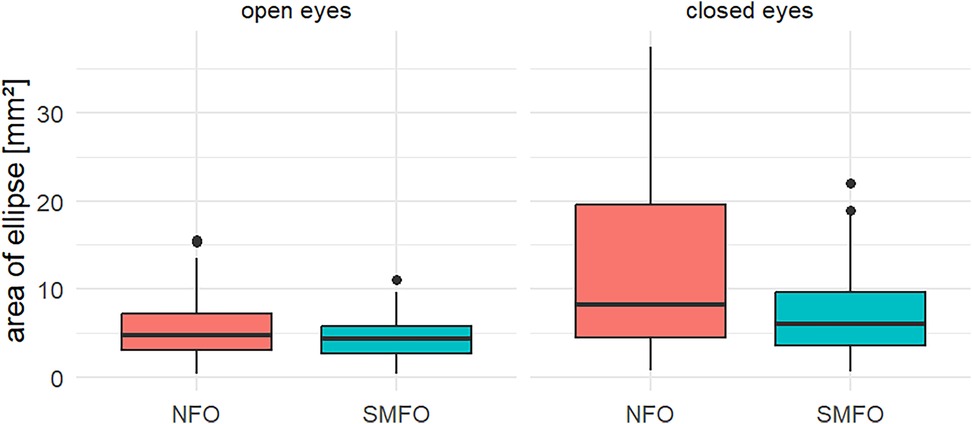
Figure 3. Boxplots representing descriptive statistics of both conditions (open eyes, closed eyes) for both type of soles (NFO, SMFO). Some of the outliers were removed to improve presentation with consistent scaling.

Table 1. Descriptive data of the results (median, interquartile range).
The results of the non-parametric ANOVA are presented in Table 2. Since sole (SMFO, NFO) and vision (OE, CE) both showed significant effects, Table 3 shows the post-hoc Wilcoxon tests for both effects.
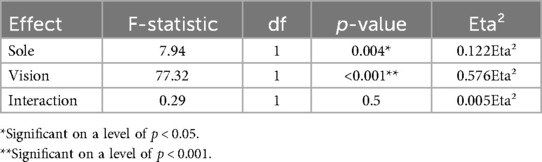
Table 2. Results of the non-parametric ANOVA.
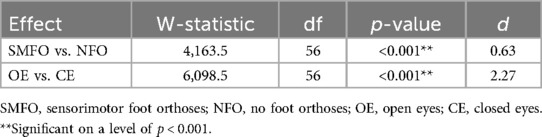
Table 3. Post-hoc-Wilcoxon test for both main effects.
4 Discussion
The results of the present study showed no interaction between the conditions sole and vision but two significant main effects (sole: p = 0.004, vision: p < 0.001). The significant difference for the vision is an additional result of the inferential statistics which can be expected and does not differentiate between SMFO vs. NFO and is therefore negligible. post-hoc tests underlined these results, where static balance improved by a median of 0.8 cm2 (14.5%) with SMFO compared to NFO (p < 0.001, d = 0.6).
Due to the lack of an interaction effect, no inference statistical differentiation is made between SMFO OE vs. NFO OE and SMFO CE and NFO CE. The descriptive statistics indicate that participants in particular benefited from the SMFO with CE (median: 1.9 cm2, 29.6%) compared to NFO.
The results support the hypothesis that the SMFO might be a helpful foot orthosis for improving balance regulation. This could be a helpful support for our sensorimotor system to avoid injuries or falls.
4.1 Possible neurophysiological explanations
From the authors’ perspective, there are several possible explanations for the positive influence of SMFO on balance regulation. The first explanation is based on a changed proprioception do to the fact that the combination and arrangement of the two elements (see Figure 1) causes the toe flexors to stretch, as the metatarsal heads fall into the gap between the toe bar and the retrocapital pad. Consequently, an increased muscle tone resolved via Ia afferents triggered by the muscle spindles (33). This indicated that the activation frequency of these muscular tension sensors increased in the afferent signal chain (33). The neuromuscular consequence is a contraction of the plantar foot muscles to protect them from further increases in stretch (33). In this case, however, as the participants were standing statically on the SMFO, it is probably only an isometric contraction and an increase in tension, as a concentric shortening of the muscle probably cannot be achieved mechanically due to the standing position. Nevertheless, an increase in the tension of the toe flexors may be beneficial for balance regulation. It is known that the toe flexors play an important role here (34), particularly while standing (35). In a further explanatory approach, it is conceivable that this increase in tension on the plantar aponeurosis could pull the calcaneus into a slight retroversion that transmits a similar supportive toning effect via the Ia afferents to the m. gastrocnemius and m. soleus (36), which also play an important role in balance regulation (37, 38).
The following explanation focuses on the toe bar and its primarily effects on mechanoception. This element of the SMFO is said to be beneficial for the pre-tension of the toe flexors and leads to a greater area of contact between toes and SMFO because of its shape. The increased contact surface can increase afferent information density via known mechanoceptors in the skin (20, 39), such as the Pacini corpuscles, Ruffini corpuscles, and Merkel cells. An increase in sensory information to the CNS seems to be a helpful factor, ashas been shown in other studies (19, 20). Furthermore, the toe bar might improve toe grip strength and standing balance, as Nakano et al. have already revealed for a slightly different toe grip bar (40).
Another explanation is the mechanical stimulus by the elements, which is altered by the surface profile compared to the NFO and causes new joint positioning, which could unconsciously have a greater impact on the afferent information from this area (41–43), which having a unspecific but somehow positive effect on balance regulation, in this case, COP control (19, 44).
The last explanation is a combination of the previous approaches. In conclusion, it should be emphasized that the results demonstrate the positive change with the present experimental design and methodology. Other studies are needed to answer this complex neurophysiological question and thus provide an evidence-based explanation. Nonetheless though the exact neurophysiological processes of the SMFO are unclear, this first study confirms the assumption that the SMFO positively influences balance.
4.2 Comparable investigations
To the best of our knowledge, this is the first study on SMFO and their effects on balance. Therefore, further studies must examine other forms of balance and participants. Nevertheless, previous studies have shown that balance can be influenced by the surface texture of the insole (19). These forms of insoles also influence the afferent information within the sensorimotor system. While the SMFO consists of four central elements, all of which have specific and targeted functions (toning and detoning of muscle tension) (15, 16) this form consists of flat, industrially manufactured insoles that only have a very small und unspecific textured surface that is the same at all points of the insole (19). However, based on the design in these cases, primarily via a change in mechanoception through the non-specific surface texture (spikes, pyramids and granulations) of the insole, there were no fundamental changes to the profile with specific and predefined objectives (19). Compared with other reference values for the area of the ellipse (45), the present values are higher on average, which is presumably due to the methodical approach: average value from three attempts, instead of the best value per condition (46).
Kalron, Pasitselsky (47) showed that in 25 patients with MS with an insole containing miniature square pyramids, CE led to immediate improvements in static balance (sway path length and sway rate). A significant observation was also confirmed after a wearing period of 4 weeks. As in the present study, Kalron, Pasitselsky (47) did not find any significant improvements with OE. Hatton, Dixon (48) made similar observations in 50 healthy adults. With OE, static balance (medio-lateral sway) improved significantly, by 9.2% when wearing an insole with pyramidal peaks. The same authors also found a significant improvement in balance (sway velocity) in patients with diabetic neuropathy (49). A textured insole with a nodule design was used, whereby the intervention group with the textured insole improved significantly, by 5%, after a wearing duration of 4 weeks in the static test with OE. Qiu, Cole (50) showed that patients with Parkinson disease significantly improved their static balance (medio-lateral sway) by wearing textured insoles with granulations across the upper surface. Other studies with a similar designs also demonstrated the positive influence of textured insoles with significant results, particularly with CE (51).
All of them are only partially comparable with the present study, as these types of mainly industrially manufactured insoles must be distinguished from the SMFO by their variation of specific manufactured elements. The insoles used in these studies primarily work with an unspecific and consistently structured surface texture, whereas the SMFO uses different elements that lead to mechanical position changes in the feet and lower extremities via a specific profile with the respective objectives (18, 52–54). Treatment with an SMFO is usually based on a specific indication that is also known from biomechanical foot orthosis treatment and is an individual, handcrafted product. For SMFO, the improvement in balance can therefore, be described as a positive side effect, which can make sense in several clinical cases that affect balance regulation, such as multiple sclerosis (47, 55), Parkinson disease (56), or polyneuropathy (49). However, a comparison with the studies presented shows that balance can be influenced by the sole of the foot and the afferent information to the CNS (20). Furthermore, the findings show that even if the heterogeneity of the collected parameters and participants weakens the comparability, that people seem to benefit from the insoles, especially when their eyes are closed.
Nevertheless, some studies have not shown significant improvements in static balance (57–59). However, it is important to note that, thus far, there have not been any opposing trends that would worsen the balance via these approaches (19).
4.3 Relevance
Although the connection between SMFO and balance requires further confirmatory studies, this topic is highly relevant in practice. Demographic changes and the resulting increase in the proportion of older people are some of the reasons for this. The sense of balance declines continuously from middle age onwards (60, 61). This contributes to an increased number of falls among the elderly population (7). In this population group, the declining visual sense also plays a role (62), so that SMFO could presumably be particularly helpful for these people, as the results with CE show. Consequently, SMFOs could support fall prevention in the elderly population, even though improved balance has a positive side effect in the majority of SMFO treatments. The actual reason for SMFO treatment will probably be a specific indication [e.g., pes planovalgus (63)] or corresponding kinematic abnormalities that justify preventive action.
Furthermore, SMFO may be more important in the context of rehabilitation. Owing to its muscle-activating properties (63, 64), it may be of increased interest to clients anyway. Proprioceptive training, which is basically a type of balance training, is also an essential component of many post-traumatic or post-operative rehabilitation programs, as proprioceptive abilities have a stabilizing and therefore protective effect on joint kinematics (4, 12). This training effect might be enhanced by using SMFO.
Since the ability to maintain balance is often functionally limited because the sensorimotor status is deficient (8), SMFO could make a positive contribution to minimizing the risk of functional ankle instability, as the static balance is considered a predictor for ankle injuries (6). Especially if the SMFO is equipped with the lateral and medial spot in an individually adapted form. Ludwig and colleagues (64) have already been able to demonstrate that the lateral spot of a SMFO significantly increases the muscle activity of the m. peroneus longus. As a main foot pronator, the m. peroneus plays an important role in securing the ankle joint against supination strains. Ludwig and colleagues showed that both the integrated electromyographic output increased and that earlier activation of the same muscle was initiated. No lateral and medial spot were used for this study, as the focus was on the two anterior elements (toe bar and retrocapital pad). Nevertheless, the toe bar and the retrocapital pad already appear to improve the sensorimotor status and improving the static balance, which could be beneficial for the ankle stability.
Although there are evidence-based positive correlations between balance and, for example, the likelihood of injury (5, 6, 65), we must await further research to better assess the clinical relevance of a improved sway area for everyday life. Similarly, further research is needed to explicitly assess the difference between OE and CE of the different conditions (e.g., SMFO OE vs. NFO OE). This step was not taken due to the lack of an interaction effect (Table 2). The general difference between OE and CE, as applied here due to the statistical procedure used, is negligible from the authors’ point of view. The primary argument is the difference that the visual sense as one of the most important supporters of the sense of balance is absent (26). Nevertheless, both parts of the study are important, as they reflect everyday life on the one hand (OE) and reduce the focus on internal sensorimotor control circuits on the other (CE) (45).
4.4 Limitations
Despite these positive results, there are some limitations that restrict their generalizability. This is the first study on balance in combination with SMFO. The sample size was appropriate and healthy, but the results cannot be applied to younger people or older people, or to people with specific diseases. It is questionable whether SMFO would be useful for younger people, as their sense of balance might still be sufficiently developed. Balance has several dimensions. Whether these effects can be positively transferred to a dynamic balance needs to be investigated. Furthermore, this study analyzed only short-term effects, and no statements about the long-term effects can be made. Moreover, to calculate the group differences, the mean values of three measurements per condition were determined. This step results in a high coefficient of variation for all groups (46), which should be noted for future studies and interpretation. Limiting yourself to the respective best value could also be a suitable approach. Posturography is often only used with one measurement per condition in practical screenings.
It should be noted that the SMFOs in this study were prefabricated for all shoe sizes by an experienced master craftsman. This means that the retrocapital pads and the toe bars were adjusted to an average shape in relation to the foot size. However, they were not individually manufactured for each participant. However, from the authors’ point of view, however, this should be seen as a positive rather than a negative aspect, as an individual fitting should be more precise.
Follow-up studies should also compare BMFO as a control variable or target the influence of fatigue (66) as a confounding variable in combination with SMFO. It is conceivable that in the case of intentional neuromuscular fatigue, the support of the SMFO could lead to even better effects. Furthermore future studies should add self-reported ankle stability questionnaires to combine the objective results with the subjective perception.
5 Conclusion
SMFO may be a helpful intervention for improving static balance (sway area) and supporting our sensorimotor system to avoid injuries (e.g., ankle sprains) or falls. Further research is needed to determine the extent to which the combination of a retrocapital pad and a toe bar effectively supports different dimensions of balance, its long-term effects and clinical relevance. Also, to include natural variation and therefore a more ecologically valid measure, future investigations should consider analyzing more trials per condition.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by RPTU Social Sciences Ethics Commission. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SB: Supervision, Methodology, Software, Writing – review & editing, Writing – original draft, Conceptualization. SS: Conceptualization, Supervision, Software, Writing – review & editing, Writing – original draft, Methodology. JHa: Writing – review & editing, Data curation, Investigation. JHe: Writing – review & editing, Data curation, Investigation. WK: Writing – review & editing, Investigation. CD: Writing – review & editing, Methodology. JD: Writing – review & editing, Formal analysis, Visualization. MF: Resources, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
SB has a freelance collaboration and Steven Simon has a part-time job at Springer Aktiv AG.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Horak FB. Postural compensation for vestibular loss and implications for rehabilitation. Restor Neurol Neurosci. (2010) 28(1):57–68. doi: 10.3233/RNN-2010-0515
2. Kuczynski MP, Wieloch M. Effects of accelerated breathing on postural stability. Human Movement. (2008) 9:107–10. doi: 10.2478/v10038-008-0012-9
3. Sekulic S, Podgorac J, Kekovic G, Žarkov M, Kopitović A. Significance of adequate postural control in the appearance of habitual upright bipedal locomotion. Med Hypotheses. (2012) 79(5):564–71. doi: 10.1016/j.mehy.2012.07.019
4. Etty Griffin LY. Neuromuscular training and injury prevention in sports. Clin Orthop Relat Res. (2003) 409:53–60. doi: 10.1097/01.blo.0000057788.10364.aa
5. Larsen LR, Kristensen PL, Junge T, Møller SF, Juul-Kristensen B, Wedderkopp N. Motor performance as risk factor for lower extremity injuries in children. Med Sci Sports Exerc. (2016) 48(6):1136–43. doi: 10.1249/mss.0000000000000877
6. Ross S, Guskiewicz KM, Gross MT, Yu B. Balance measures for discriminating between functionally unstable and stable ankles. Med Sci Sports Exerc. (2009) 41(2):399–407. doi: 10.1249/MSS.0b013e3181872d89
7. Ema R, Saito M, Ohki S, Takayama H, Yamada Y, Akagi R. Association between rapid force production by the plantar flexors and balance performance in elderly men and women. Age (Omaha). (2016) 38:475–83. doi: 10.1007/s11357-016-9949-3
8. Khan S, Chang R. Anatomy of the vestibular system: a review. NeuroRehabilitation. (2013) 32(3):437–43. doi: 10.3233/NRE-130866
9. van Beers RJ, Baraduc P, Wolpert DM. Role of uncertainty in sensorimotor control. Philos Trans R Soc Lond B Biol Sci. (2002) 357(1424):1137–45. doi: 10.1098/rstb.2002.1101
10. Vetter P, Wolpert DM. Context estimation for sensorimotor control. J Neurophysiol. (2000) 84(2):1026–34. doi: 10.1152/jn.2000.84.2.1026
11. Martínez-Amat A, Hita-Contreras F, Lomas-Vega R, Caballero-Martínez I, Alvarez PJ, Martínez-López E. Effects of 12-week proprioception training program on postural stability, gait, and balance in older adults: a controlled clinical trial. J Strength Cond Res. (2013) 27(8):2180–8. doi: 10.1519/JSC.0b013e31827da35f
12. Malliou P, Gioftsidou A, Pafis G, Beneka A, Godolias G. Proprioceptive training (balance exercises) reduces lower extremity injuries in young soccer players. J Back Musculoskelet Rehabil. (2004) 17(3–4):101–4. doi: 10.3233/bmr-2004-173-403
13. Al Attar WSA, Khaledi EH, Bakhsh JM, Faude O, Ghulam H, Sanders RH. Injury prevention programs that include balance training exercises reduce ankle injury rates among soccer players: a systematic review. J Physiother. (2022) 68(3):165–73. doi: 10.1016/j.jphys.2022.05.019
14. de Morais Barbosa C, Bertolo MB, Gaino JZ, Davitt M, Sachetto Z, de Paiva Magalhaes E. The effect of flat and textured insoles on the balance of primary care elderly people: a randomized controlled clinical trial. Clin Interv Aging. (2018) 13:277–84. doi: 10.2147/CIA.S149038
15. Becker S, Ludwig O, Woltring S, Simon S, Fröhlich M. Sensomotorische Einlagen. Grundlagen Und Funktionen. Berlin, Heidelberg: Springer (2024).
16. Becker S, Simon S, Mühlen J, Dindorf C, Fröhlich M. Assessing the subjective effectiveness of sensorimotor insoles (smis) in reducing pain: a descriptive mulitcenter pilot study. J Funct Morphol Kinesiol. (2023) 8(66):1–9. doi: 10.3390/jfmk8020066
17. Simon S, Dully J, Ludwig O, Dindorf C, Bartaguiz E, Fröhlich M, et al. Kinematic effects of sensorimotor foot orthoses on the gait of patients with patellofemoral pain—a randomized controlled trial. Front Sports Act Living. (2025) 7:1546821. doi: 10.3389/fspor.2025.1546821
18. Mabuchi A, Kitoh H, Inoue M, Hayashi M, Ishiguro N, Suzuki N. The biomechanical effect of the sensomotor insole on a pediatric intoeing gait. Int Sch Res Notices. (2012) 2012:396718. doi: 10.5402/2012/396718
19. Azhar A N, Bergin SM, Munteanu SE, Menz HB. Footwear, orthoses, and insoles and their effects on balance in older adults: a scoping review. Gerontology. (2024) 70(8):801–11. doi: 10.1159/000539591
20. Strzalkowski NDJ, Peters RM, Inglis JT, Bent LR. Cutaneous afferent innervation of the human foot sole: what can we learn from single-unit recordings? J Neurophysiol. (2018) 120(3):1233–46. doi: 10.1152/jn.00848.2017
21. Christensen IK, Deilami SSJ, Amiri S, Nissen MH, Devantier L, Ovesen T. Validation of posturographic measurements in adolescents. Otol Neurotol. (2018) 39(7):e568–74. doi: 10.1097/MAO.0000000000001870
22. Yoon JJ, Yoon TS, Shin BM, Na EH. Factors affecting test results and standardized method in quiet standing balance evaluation. Ann Rehabil Med. (2012) 36:112–8. doi: 10.5535/arm.2012.36.1.112
23. Pomarino D, Nawrath A, Beyer J. Age-dependent measurements of postural stability in healthy individuals. Oxford Univ Press. (2013) 2(9):420–5. doi: 10.3238/oup.2013.0420_0425
24. Magnusson M, Enbom H, Johansson R, Pyykkö I. Significance of pressor input from the human feet in anterior-posterior postural control. The effect of hypothermia on vibration-induced body-sway. Acta Otolaryngol. (1990) 110(3–4):182–8. doi: 10.3109/00016489009122535
25. Lipowicz A, Bugdol M, Graja K, Nowakowska-Lipiec K, Jochymczyk-Woźniak K, Fryc D, et al. Relationship between body sway and body build in healthy adult men and women. Anthropol Rev. (2023) 86:45–61. doi: 10.18778/1898-6773.86.4.04
26. Ludwig O, Mazet C, Mazet D, Hammes A, Schmitt E. Changes in habitual and active sagittal posture in children and adolescents with and without visual input—implications for diagnostic analysis of posture. J Clin Diagn Res. (2016) 10(2):Sc14–7. doi: 10.7860/jcdr/2016/16647.7283
27. Palazzo F, Nardi A, Tancredi V, Caronti A, Scalia Tomba G, Lebone P, et al. Effect of textured insoles on postural control during static upright posture following lower limb muscle fatigue. J Sports Med Phys Fitness. (2019) 59(2):246–52. doi: 10.23736/S0022-4707.17.08029-X
28. Franz JR, Francis CA, Allen MS, O’Connor SM, Thelen DG. Advanced age brings a greater reliance on visual feedback to maintain balance during walking. Hum Mov Sci. (2015) 40:381–92. doi: 10.1016/j.humov.2015.01.012
29. Era P, Sainio P, Koskinen S, Haavisto P, Vaara M, Aromaa A. Postural balance in a random sample of 7,979 subjects aged 30 years and over. Gerontology. (2006) 52(4):204–13. doi: 10.1159/000093652
30. Palazzo F, Nardi A, Lamouchideli N, Caronti A, Alashram A, Padua E, et al. The effect of age, sex and a firm-textured surface on postural control. Exp Brain Res. (2021) 239(7):2181–91. doi: 10.1007/s00221-021-06063-2
31. Bortz J, Schuster C. Statistik Für Human- Und Sozialwissenschaftler. Berlin, Heidelberg: Springer (2010).
32. Noguchi K, Gel YR, Brunner E, Konietschke F. Nparld: an R software package for the nonparametric analysis of longitudinal data in factorial experiments. J Stat Softw. (2022) 50(12):1–23. doi: 10.32614/CRAN.package.nparLD
33. Macefield VG, Knellwolf TP. Functional properties of human muscle spindles. J Neurophysiol. (2018) 120(2):452–67. doi: 10.1152/jn.00071.2018
34. Quinlan S, Fong Yan A, Sinclair P, Hunt A. The evidence for improving balance by strengthening the toe flexor muscles: a systematic review. Gait Posture. (2020) 81:56–66. doi: 10.1016/j.gaitpost.2020.07.006
35. Otake Y, Yozu A, Fukui T, Sumitani M, Haga N. Relationship between toe flexion movement and center of pressure position. Int J Foot Ankle. (2018) 2(2):1–6. doi: 10.23937/ijfa-2017/1710015
36. Schwarz M, Sontag KH, Wand P. Sensory-motor processing in substantia nigra pars reticulata in conscious cats. J Physiol. (1984) 347:129–47. doi: 10.1113/jphysiol.1984.sp015057
37. Maritz CA, Silbernagel KG. A prospective cohort study on the effect of a balance training program, including calf muscle strengthening, in community-dwelling older adults. J Geriatr Phys Ther. (2016) 39(3):125–31. doi: 10.1519/JPT.0000000000000059
38. Bano M, Sharma T, Gujral T, Rai RH, Mandal S, Mandal S. Effects of calf muscle fatigue and postural control on balance and functional test among adults: a quasi experimental study. J Datta Meghe Inst Med Sci Univ. (2024) 19(4):806–12. doi: 10.4103/jdmimsu.jdmimsu_505_24
39. Shin JY, Ryu YU, Yi CW. Effects of insoles contact on static balance. J Phys Ther Sci. (2016) 28(4):1241–4. doi: 10.1589/jpts.28.1241
40. Nakano H, Murata S, Abiko T, Sakamoto M, Matsuo D, Kawaguchi M, et al. Effect of insoles with a toe-grip bar on toe-grip strength and body sway in middle-aged and elderly women. Top Geriatr Rehabil. (2019) 35:125–8. doi: 10.1097/TGR.0000000000000221
41. Zimny ML. Mechanoreceptors in articular tissues. Am J Anat. (1988) 182(1):16–32. doi: 10.1002/aja.1001820103
42. Forth KE, Layne CS. Neuromuscular responses to mechanical foot stimulation: the influence of loading and postural context. Aviat Space Environ Med. (2008) 79(9):844–51. doi: 10.3357/asem.2176.2008
43. Palluel E, Olivier I, Nougier V. The lasting effects of spike insoles on postural control in the elderly. Behav Neurosci. (2009) 123(5):1141–7. doi: 10.1037/a0017115
44. Preszner-Domjan A, Nagy E, Szíver E, Feher-Kiss A, Horvath G, Kranicz J. When does mechanical plantar stimulation promote sensory Re-weighing: standing on a firm or compliant surface? Eur J Appl Physiol. (2012) 112(8):2979–87. doi: 10.1007/s00421-011-2277-5
45. Becker S, Thomas A, Ulrich L, Becker L, Dindorf C, Berger J, et al. Reference values for static posturography of sportive and healthy adults aged 18–30 years. BMC Sports Sci Med Rehabil. (2025) 17(1):94. doi: 10.1186/s13102-025-01128-z
46. Chaudhry H, Bukiet B, Ji Z, Findley TW. Measurement of balance in computer posturography: comparison of methods–a brief review. J Bodyw Mov Ther. (2011) 15(1):82–91. doi: 10.1016/j.jbmt.2008.03.003
47. Kalron A, Pasitselsky D, Greenberg-Abrahami M, Achiron A. Do textured insoles affect postural control and spatiotemporal parameters of gait and plantar sensation in people with multiple sclerosis? Phys Med Rehabil J. (2015) 7(1):17–25. doi: 10.1016/j.pmrj.2014.08.942
48. Hatton AL, Dixon J, Rome K, Martin D. Standing on textured surfaces: effects on standing balance in healthy older adults. Age Ageing. (2011) 40(3):363–8. doi: 10.1093/ageing/afr026
49. Hatton AL, Chatfield MD, Gane EM, Maharaj JN, Cattagni T, Burns J, et al. The effects of wearing textured versus smooth shoe insoles for 4-weeks in people with diabetic peripheral neuropathy: a randomised controlled trial. Disabil Rehabil. (2025) 47(3):751–61. doi: 10.1080/09638288.2024.2360658
50. Qiu F, Cole MH, Davids KW, Hennig EM, Silburn PA, Netscher H, et al. Effects of textured insoles on balance in people with parkinson’s disease. PLoS One. (2013) 8(12):e83309. doi: 10.1371/journal.pone.0083309
51. Kenny RPW, Eaves DL, Martin D, Hatton AL, Dixon J. The effects of textured insoles on quiet standing balance in four stance types with and without vision. BMC Sports Sci Med Rehabil. (2019) 11(1):1–8. doi: 10.1186/s13102-019-0117-9
52. Laštovička O, Klein T, Abrantes J, Janura M. Immediate effect of individual bars of insoles and their combination on gait parameters in asymptomatic healthy adults. Somatosens Mot Res. (2020) 37(2):125–31. doi: 10.1080/08990220.2020.1753686
53. Wegener C, Wegener K, Smith R, Schott K-H, Burns J. Biomechanical effects of sensorimotor orthoses in adults with charcot–marie–tooth disease. Prosthet Orthot Int. (2016) 40(4):436–46. doi: 10.1177/0309364615579318
54. Klein T, Lastovicka O, Janura M, Svoboda Z, Chapman GJ, Richards J. The immediate effects of sensorimotor foot orthoses on foot kinematics in healthy adults. Gait Posture. (2021) 84:93–101. doi: 10.1016/j.gaitpost.2020.11.022
55. Hatton AL, Williams K, Chatfield MD, Hurn S, Maharaj JN, Gane EM, et al. Effects of wearing textured versus smooth shoe insoles for 12 weeks on gait, foot sensation and patient-reported outcomes, in people with multiple sclerosis: a randomised controlled trial. Brain Impair. (2023) 24(2):148–67. doi: 10.1017/BrImp.2022.33
56. Maurer LK, Maurer H, König M, van Munster M, Haen S, Pedrosa DJ. Do sensorimotor insoles improve gait safety in patients with Parkinson’s disease on a short scale? Clin Park Relat Disord. (2024) 11:100290. doi: 10.1016/j.prdoa.2024.100290
57. Dixon J, Hatton AL, Robinson J, Gamesby-Iyayi H, Hodgson D, Rome K, et al. Effect of textured insoles on balance and gait in people with multiple sclerosis: an exploratory trial. Physiotherapy. (2014) 100(2):142–9. doi: 10.1016/j.physio.2013.06.003
58. Kenny RP, Eaves DL, Martin D, Behmer LP, Dixon J. The effects of textured insoles on cortical activity and quiet bipedal standing with and without vision: an eeg study. J Mot Behav. (2020) 52(4):489–501. doi: 10.1080/00222895.2019.1648237
59. Qu X. Impacts of different types of insoles on postural stability in older adults. Appl Ergon. (2015) 46(Pt A):38–43. doi: 10.1016/j.apergo.2014.06.005
60. Roman-Liu D. Age-related changes in the range and velocity of postural sway. Arch Gerontol Geriatr. (2018) 77:68–80. doi: 10.1016/j.archger.2018.04.007
61. Colledge NR, Cantley P, Peaston I, Brash H, Lewis S, Wilson JA. Ageing and balance: the measurement of spontaneous sway by posturography. Gerontology. (1994) 40(5):273–8. doi: 10.1159/000213596
62. Lord SR, Smith ST, Menant JC. Vision and falls in older people: risk factors and intervention strategies. Clin Geriatr Med. (2010) 26(4):569–81. doi: 10.1016/j.cger.2010.06.002
63. Schmitt AP-L, Liebau K-H, Hamm A, Hacke C, Mittelmeier W, Schulze C. Comparison of the influence of supportive and sensorimotor insoles in the muscle activity of tibialis anterior and peroneus longus in combat boots. Foot. (2022) 52:101910. doi: 10.1016/j.foot.2022.101910
64. Ludwig O, Kelm J, Frohlich M. The influence of insoles with a peroneal pressure point on the electromyographic activity of tibialis anterior and peroneus longus during gait. J Foot Ankle Res. (2016) 9(1):33. doi: 10.1186/s13047-016-0162-5
65. Johansson J, Jarocka E, Westling G, Nordström A, Nordström P. Predicting incident falls: relationship between postural sway and limits of stability in older adults. Hum Mov Sci. (2019) 66:117–23. doi: 10.1016/j.humov.2019.04.004
Keywords: SMFO, insoles, proprioception, center of pressure (COP), posturography, postural sway, fall prevention
Citation: Becker S, Simon S, Hayer J, Heidger J, Koltschin W, Dindorf C, Dully J and Fröhlich M (2025) Effects of sensorimotor foot orthoses on static balance in healthy adults: a crossover randomized controlled trial. Front. Sports Act. Living 7:1616696. doi: 10.3389/fspor.2025.1616696
Received: 23 April 2025; Accepted: 16 July 2025;
Published: 31 July 2025.
Edited by:
Jia Han, Shanghai University of Medicine and Health Sciences, ChinaReviewed by:
Roger David Adams, University of Canberra, AustraliaRatakorn Aimkosa, Shanghai University of Sport, China
Xiaoyue Hu, Shanghai University of Medicine and Health Sciences, China
Copyright: © 2025 Becker, Simon, Hayer, Heidger, Koltschin, Dindorf, Dully and Fröhlich. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stephan Becker, c3RlcGhhbi5iZWNrZXJAcnB0dS5kZQ==; Steven Simon, c3RldmVuLnNpbW9uQHJwdHUuZGU=