 Åsa Hammar1,2,3*
Åsa Hammar1,2,3* Guro Årdal1
Guro Årdal1- 1Department of Biological and Medical Psychology, University of Bergen, Bergen, Norway
- 2Division of Psychiatry, Haukeland University Hospital, University of Bergen, Bergen, Norway
- 3Moodnet Research Group, Haukeland University Hospital, University of Bergen, Bergen, Norway
The aim of the present study was to investigate verbal memory performance in a group of patients with remitted and partial remitted major depressive disorder. Thirty-one patients and 31 healthy matched controls were included in the study. Results from the California Verbal Learning Test show intact verbal memory performance in the patient group regarding learning, recall and recognition. However, patients had significantly poorer performance compared to healthy controls in immediate recall of the first trial in the verbal memory test. In conclusion, the patient group showed intact memory performance, when material is presented more than once. These findings indicate that memory performance in MDD patients with partial remission and remission benefit from repetition of material.
Introduction
Depressed patients often report generalized memory problems, however it has been shown that they estimate their actual performance worse than objective measures (Kalska et al., 1999; Wong et al., 2000). Indeed, several studies show intact memory functioning in depression (Egeland et al., 2003; Porter et al., 2003; Smith et al., 2005; Wang et al., 2006; Hammar et al., 2011). In contrast, others report memory impairments during acute phase of the disorder (for overview se Austin et al., 2001; Fossati et al., 2002, 2004; Neu et al., 2005; Bearden et al., 2006). Hence, the literature regarding acute depression and memory impairment is divergent and inconclusive. Consequently, the long term course of verbal memory functioning during phases of symptom recovery is still unclear.
Nevertheless, in the comprehensive review conducted by Douglas and Porter (2009) it was concluded that whilst some cognitive functions remain impaired during symptom improvement it seems as functioning in verbal memory recovers. Still, the number of published reports that investigates verbal memory in a long term course are few.
In a recent study by Hammar et al. (2011), a group of patients diagnosed with unipolar recurrent major depression was investigated in verbal memory. All patients were in an acute phase of depression with severe symptom load. We found intact verbal learning and memory, however the patient group reported significantly fewer words compared to the healthy control group on the first immediate recall trial in the verbal learning test. Performance of the patients were normalized during the remaining trials. In order to pursue the finding regarding first trial impairment, we conducted a study including patients previously diagnosed with recurrent major depressive disorder and currently in remission or partial remission.
Based on the previous literature we hypothesized that patients with recurrent MDD would show normal performance on the verbal memory test and that the impaired performance regarding the first trial would be normalized.
Methods
Subjects
Data from 31 patients (11 males, 20 females) who formerly met the DSM-IV criteria (DSM-IV, 2000) for a unipolar recurrent MDD diagnosis, using MINI - International Psychiatric Structural Interview (Leiknes et al., 1999) and 31 healthy matched controls were included in the present study. Severity of depression was assessed using the Hamilton Depression Rating Scale (HDRS), (Hamilton, 1960). For demographic data see Table 2.
The patient group had experienced a minimum of two previous episodes of MDD, with at least one episode scoring a minimum of 18 on HDRS and at testing the patients had experienced improvement in symptoms of depression. Patients have been excluded from the study if known; history of brain damage, alcohol and/or substance abuse.
The control group was matched to the patient group ± a 2 year limit on age, and completed years of education. Exclusion criteria on control subjects were alcohol or any other substance abuse, brain damage, or a history of any mental disorder.
Procedure
All participants were assessed regarding their learning and memory capacity using the California Verbal Learning Test (CVLT) (Delis et al., 1987). CVLT is a verbal learning and memory test, which permits examination of acquisition, retrieval, and retention processes (Basso and Bornstein, 1999).The CVLT-II measures both recall and recognition over five immediate trials and five delayed memory trials, using two word lists consisting of 16 words each. See Table 1 for an overview of obtained variables.
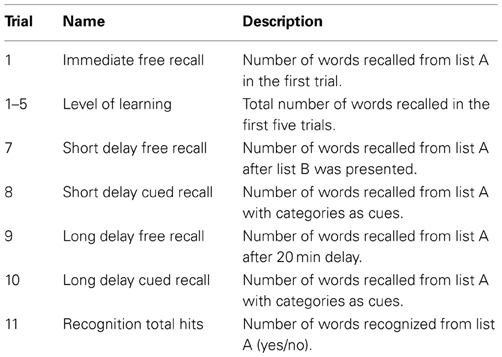
Table 1. CVLT-II variables.
Informed consent was obtained from all participants. The study was performed in accordance with the Helsinki Declaration of the World Medical Association Assembly. The study was approved by the Regional Committee for Medical Research Ethics and The Norwegian Data Inspectorate.
Data Scoring and Analysis
The statistical analysis of the data was carried out using the statistical package SPSS (20.0 for Windows). Group comparison analyses were carried out using a one way ANOVA. Group comparison analyses were carried out using a one way ANOVA. An alpha level of < 0.05 was used for statistical tests. Age and level of education were controlled for through the matched control group. Preliminary assumption testing was conducted to check for normality, linearity and outliers. In order to check for equal variance, Levine's test of homogeneity of variance was conducted. To measure effect sizes for significant differences partial eta square was calculated. Data were analyzed as number of words recalled in the different conditions or as number of words correctly recognized. An independent samples t-test was conducted to compare the IQ scores for the patient and control group. Correlations were calculated with Pearson's coefficients.
Results
CVLT: Immediate recall (trial 1): The patient group recalled significant fewer words compared to the control group on immediate recall, trial 1 F(1, 60) = 6.183, p = 0.016. Partial eta squared = 0.09. There were no significant differences between the two groups in the other conditions (see Table 2).
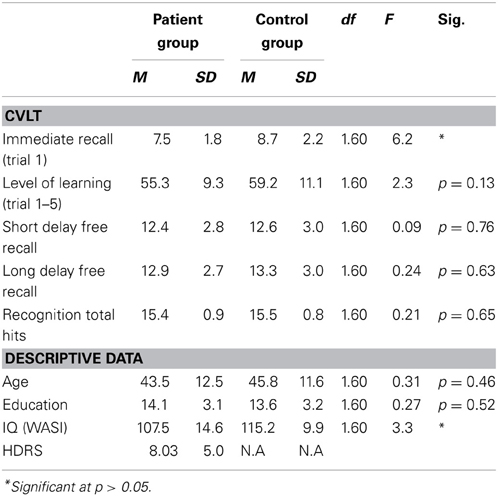
Table 2. Test performance and descriptive data for both groups.
There was no correlation between current symptoms of depression (as measured by HDRS) and performance on immediate recall, trial 1. There was a significant difference between the patient and the control group on WASI total IQ score t(60) = −2,43, p = 0.018. Further there was a significant correlation in the patient group r = 0.575, n = 31, p > 0.01 between WASI total IQ score and scores on immediate recall, trial 1. There was no correlation between WASI total IQ score and immediate recall, trial 1 in the control group. See Figure 1.
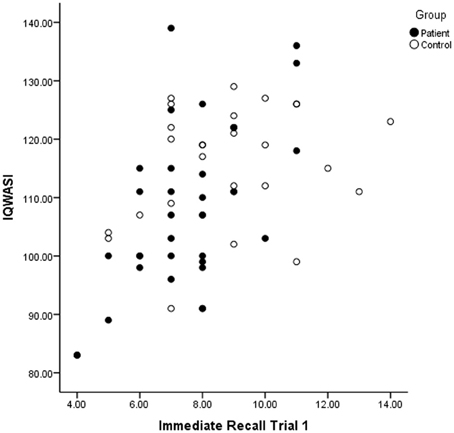
Figure 1. The correlation between IQ and Immediate Recall for patients and controls.
To further explore the possible link between current depressive symptoms and performance on immediate recall, trial 1 the patient group was divided into two groups: remitted (N = 13) and partial remitted (N = 18) based on HDRS scores. Remission was defined as a HDRS score of ≥ 7 and partial remission was defined as ≤ 8 and improvement from baseline inclusion.
There were no significant difference in immediate recall, trial 1 between patients in remission and patients with partial remission (see Table 3).
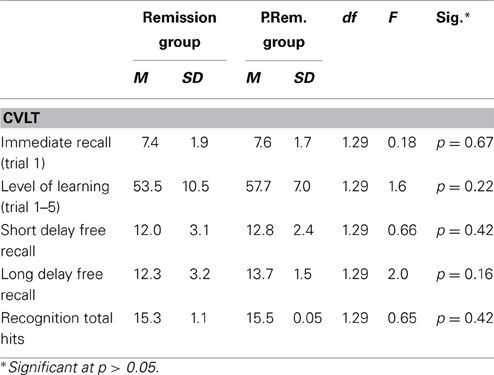
Table 3. Test performance and descriptive data for the remission group (N = 18) and the partial remission group (P.Rem. group) (N = 13).
Discussion
Patients with remitted and partial remitted major depression show intact verbal memory performance regarding learning, recall and recognition in the present study. The patient group had significantly poorer performance compared to the control group in immediate recall of the first trial in verbal memory.
Thus, the hypothesis that patients with recurrent MDD would show normal performance on the verbal memory test was confirmed, however, the expectation of normalized performance on immediate recall of the first trial was not supported. Severity of depression did not have any effects of the results.
There are various possible explanations for the findings in the present study. As described in the CVLT manual (Delis et al., 1987) depressed patients might struggle on the first learning trial because they feel overwhelmed, thus performance will normalize trough the test. Such an explanation is in accordance with previous findings in acutely depressed patients (Hammar et al., 2011). According to Delis et al. (2000) the first immediate recall trial on the CVLT-II is thought to be especially dependent on auditory attention span. Individuals with impaired attention, but normal learning and memory may perform poorly on the first immediate recall trial, but perform adequately on subsequent trials (Delis et al., 2000). This is a plausible explanation for the findings in the present study, since attention is a domain which often is impaired in depressed patients (Hammar and Årdal, 2009). Deficits in attention have been reported in studies of remitted patients (Weiland-Fiedler et al., 2004; Paelecke-Habermann et al., 2005; Preiss et al., 2009).
The patient group was divided into patients in remission or partially remission in order to investigate if performance was related to symptom load. There was no difference in performance on immediate recall of the first trial between the two groups. Moreover, there was no correlation between symptom load and performance on the first learning trial. Thus, the results in the present report could not be explained by the presence of depressive symptoms.
In a clinical perspective the finding reflects the often self-reported experience of poor memory functioning in this patient group (Kalska et al., 1999; Wong et al., 2000), since daily life memory functioning often requires immediate recall without repetition. When disseminating these results, it is of importance to communicate both the cognitive strengths in verbal memory in this patient group, but at the same time not underestimate the dysfunction found in immediate recall of the first trial.
A correlation between IQ scores and immediate recall was observed in immediate recall of the first trial in the patient group, indicating that higher IQ is associated with better performance on immediate recall. There was no correlation between these measures in the control group. This finding was not evident in a previous study of patients in the acute phase of depression (Hammar et al., 2011). High IQ seems to benefit improved performance in immediate recall, when patients are in remission or partial remission. However this seems not to be the case in the acute phase of illness (Hammar et al., 2011). It is important to note that IQ was average in the patient group, thus low IQ could not explain the result in general.
Little research is published showing cognitive strengths in depressed patients. Following the reasoning by Delis et al. (2000), the present finding of impairment in immediate recall in the patient group might reflect impaired attention span rather than memory impairment. However, it is important to highlight the intact learning performance when repetitions are provided, and further the intact short and long-term memory. This knowledge is important for clinicians and the patients themselves in order to plan rehabilitation and interventions. Future research should aim to clarify the impact of attention span on memory functioning with subjective and objective measures in this patient group.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Austin, M.-P., Mitchell, P., and Goodwin, G. M. (2001). Cognitive deficits in depression: possible implications for functional neuropathology. Br. J. Psychiatry 178, 200–206. doi: 10.1192/bjp.178.3.200
Basso, M. R., and Bornstein, R. A. (1999). Relative memory deficits in recurrent versus first-episode major depression on a word learning task. J. Neuropsychol. 13, 557–563. doi: 10.1037/0894-4105.13.4.557
Bearden, C. A., Glahn, D. C., Monkul, E. S., Barret, J., Najt, P., Villareal, V., et al. (2006). Patterns of memory impairment in bipolar disorder, and unipolar major depression. Psychiatry Res. 142, 139–150. doi: 10.1016/j.psychres.2005.08.010
Delis, D. C., Kramer, J. H., Kaplan, E., and Ober, B. A. (2000). California Verbal Learning Test 2nd Edition: Adult Version Manual. San Antonio, TX: The Psychological Corporation.
Delis, D. C., Kramer, J. H., Kaplan, E., and Ober, B. A. (1987). California Verbal Learning Test: Adult Version Manual. San Antonio, TX: The Psychological Corporation.
Douglas, K. M., and Porter, R. J. (2009). Longitudinal assessment of neuropsychological function in major depression. Aust. N.Z. J. Psychiatry 43, 1105–1117. doi: 10.3109/00048670903279887
DSM-IV. (2000). Diagnostic and Statistical Manual of Mental Disorders: DSM-IV TR. Washington, DC: American Psychiatric Association.
Egeland, J., Sundet, K., Rund, B. R., Asbjørnsen, A., Hugdahl, K., Landrø, N. I., et al. (2003). Sensitivity and specificity of memory dysfunction in schitzophrenia: a comparison with major depression. J. Clin. Exp. Neuropsychol. 25, 79–93. doi: 10.1076/jcen.25.1.79.13630
Fossati, P., Coyette, F., Ergis, A.-M., and Alliaire, J.-F. (2002). Influence of age and executive functioning on verbal memory of inpatients with depression. J. Affect. Disord. 68, 261–271. doi: 10.1016/S0165-0327(00)00362-1
Fossati, P., Harvey, P.-O., Le Bastard, G., Ergis, A.-M., Jouvent, R., and Allilaire, J.-F. (2004). Verbal memory performance of patients with a first depressive episode, and patients with unipolar and bipolar recurrent depression. J. Psychiatr. Res. 38, 137–144. doi: 10.1016/j.jpsychires.2003.08.002
Hammar, Å. Isaksen, L., Schmid, M., Årdal, G., Strand, M. (2011) MDD patients show intact memory performance when given optimal conditions. Appl. Neuropsychol. 18, 191–196.
Hammar, Å. Årdal, G. (2009). Cognitive functioning in major depression-a summary. Front. Hum. Neurosci. 3:26. doi: 10.3389/neuro.09.026.2009
Hamilton, M. (1960). A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 23, 56–62. doi: 10.1136/jnnp.23.1.56
Kalska, H., Punamäki, R.-L., Mäkinen-Pelli, T., and Saarinen, M. (1999). Memory and metamemory functioning among depressed patients. Appl. Neuropsychol. 6, 96–107. doi: 10.1207/s15324826an0602_5
Leiknes, K. A., Leganger, S., Malt, E. A., and Malt, U. (1999). “Mini internasjonalt neuropsykiatrisk intervju,” in Mini International Neuropsychiatric Interview, eds D. Sheehan, J. Janavs, J. Baker, K. Harnett-Sheenan, E. Knapp and M. Sheehan (0Tampa, FL: University of South Florida).
Neu, P., Bajbouj, M., Schilling, A., Godeman, F., Berman, R., and Schlattman, P. (2005). Cognitive function over the treatment course of depression in middle aged patients: correlation with brain MRI signal hyperintensities. J. Psychiatr. Res. 39, 129–135. doi: 10.1016/j.jpsychires.2004.06.004
Paelecke-Habermann, Y., Pohl, J., and Leplow, B. (2005). Attention and executive functions in remitted major depression patients. J. Affect. Disord. 89, 125–135. doi: 10.1016/j.jad.2005.09.006
Porter, R. J., Gallagher, P., Thompson, J. M., and Young, A. (2003). Neurocognitive impairment in drug-free patients with major depressive disorder. Br. J. Psychiatry 182, 214–220. doi: 10.1192/bjp.182.3.214
Preiss, M., Kucerova, H., Lukavsky, J., Stepankova, H., Sos, P., and Kawaciukova, R. (2009). Cognitive deficits in the euthymic phase of unipolar depression. Psychiatry Res. 169, 235–239. doi: 10.1016/j.psychres.2008.06.042
Smith, D. J., Harrison, N., Muir, W., and Blackwood, D. H. R. (2005). High prevalence of bipolar spectrum disorders in young adults with recurrent depression: toward an innovative diagnostic framework. J. Affect. Disord. 84, 167–178. doi: 10.1016/j.jad.2004.02.005
Wang, C. E., Halvorsen, M., Sundet, K., Steffensen, A. L., Holte, A., and Waterloo, K. (2006). Verbal memory performance of mildly to moderately depressed outpatient younger adults. J. Affect. Disord. 92, 283–286. doi: 10.1016/j.jad.2006.02.008
Weiland-Fiedler, P., Erickson, K., Waldeck, T., and Luckenbaugh, D, A. Pike, D., Bonne, O. et al. (2004). Evidence for continuing neuropsychological impairments in depression. J. Affect. Disord. 82, 253–258. doi: 10.1016/j.jad.2003.10.009
Keywords: verbal memory, depression, cognitive function, partial remission, remission
Citation: Hammar Å and Årdal G (2013) Verbal memory functioning in recurrent depression during partial remission and remission-Brief report. Front. Psychol. 4:652. doi: 10.3389/fpsyg.2013.00652
Received: 11 March 2013; Accepted: 03 September 2013;
Published online: 08 October 2013.
Edited by:
Marit Schmid, University of Bergen, NorwayReviewed by:
Karen L. Bales, University of California Davis, USASven-Erik Fernaeus, Karolinska Institutet, Sweden
Copyright © 2013 Hammar and Årdal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Åsa Hammar, Department of Biological and Medical Psychology, University of Bergen, Jonas Lies vei 91, 5009 Bergen, Norway e-mail:YWFzYS5oYW1tYXJAcHN5YnAudWliLm5v