 Sanne Koops
Sanne Koops Hilde van den Brink
Hilde van den Brink Iris E. C. Sommer
Iris E. C. Sommer- Psychiatry Department, Brain Center Rudolf Magnus, University Medical Center Utrecht, Utrecht, Netherlands
Auditory hallucinations (AH) are a symptom of several psychiatric disorders, such as schizophrenia. In a significant minority of patients, AH are resistant to antipsychotic medication. Alternative treatment options for this medication resistant group are scarce and most of them focus on coping with the hallucinations. Finding an alternative treatment that can diminish AH is of great importance. Transcranial direct current stimulation (tDCS) is a safe and non-invasive technique that is able to directly influence cortical excitability through the application of very low electric currents. A 1–2 mA direct current is applied between two surface electrodes, one serving as the anode and the other as the cathode. Cortical excitability is increased in the vicinity of the anode and reduced near the cathode. The technique, which has only a few transient side effects and is cheap and portable, is increasingly explored as a treatment for neurological and psychiatric symptoms. It has shown efficacy on symptoms of depression, bipolar disorder, schizophrenia, Alzheimer’s disease, Parkinson’s disease, epilepsy, and stroke. However, the application of tDCS as a treatment for AH is relatively new. This article provides an overview of the current knowledge in this field and guidelines for future research.
Hallucinations in Psychotic Disorders
Auditory hallucinations (AH) are a frequent symptom of schizophrenia which occurs in about 60–80% of patients (Andreasen and Flaum, 1991). The content of these hallucinations is mostly negative, often conveying anger (McCarthy-Jones et al., 2014), or terms of abuse (Nayani and David, 1996) and increasing the risk for suicidal behavior (Harkavy-Friedman et al., 2003). Furthermore, AH also occur in other diagnostic groups such as borderline personality disorder, anxiety disorders, affective disorders, posttraumatic stress disorder, autism, and significant hearing loss (Sommer et al., 2012b).
In approximately 70–75% of these cases, antipsychotic medication and/or cognitive behavioral therapy sufficiently suppress AH. However, the remaining 25–30% continues to suffer from AH despite optimal therapy (Shergill et al., 1998). Alternative treatment options are scarce for this group of patients, and often focus on coping with the hallucinations and accepting their presence instead of reducing them (Bentall et al., 1994). Due to the distressing impact AH have on the patients’ quality of life, their ability to concentrate and their social and professional functioning, finding an effective treatment option to reduce AH in this treatment-resistant group would be of great value.
Transcranial Direct Current Stimulation
Transcranial direct current stimulation (tDCS) is a non-invasive focal neurostimulation technique that involves the application of a low intensity electric current between two surface electrodes, an anode and a cathode (Nitsche et al., 2008). A 1–2 mA direct current is applied between two electrodes, often with a size of 35 cm2 (5 cm × 7 cm), which are placed on the scalp. The current flows between the anode and the cathode, some of it being diverted through the scalp and another part moving through the brain where brain activity is modulated. Although the exact mechanisms of action of tDCS have yet to be completely elucidated, there are two mechanisms by which tDCS modulates brain activity that are currently widely accepted in the field (Brunoni et al., 2012). The first proposes that the current that passes through the brain modulates levels of cortical excitability in a polarity dependent manner (Miranda et al., 2006). Cortical excitability is thought to be increased in the vicinity of the anode and reduced near the cathode. The anodal and cathodal effects of tDCS on cortical excitability are thought to be explained by shifts in the resting membrane potential (depolarization and hyperpolarization). The second proposes that prolonged effects of tDCS can be explained by modifications of N-methyl-D-aspartate (NMDA) receptor efficacy, changes in gamma-aminobutyric acid-ergic activity and modulation of interneurons, resulting in prolonged synaptic efficacy changes (Nitsche et al., 2008; Stagg and Nitsche, 2011). However, most of what we know about the effects of tDCS on a neural level is derived from studies of the primary motor cortex (Nitsche et al., 2008). Questions can be raised concerning the generalizability of these underlying mechanisms to other cortical areas (Horvath et al., 2015).
In the 1960s, tDCS was studied extensively, but never gained much popularity in clinical practice (Priori, 2003). Currently, this seems to be changing as tDCS is increasingly explored for the treatment of both neurologic and psychiatric symptoms (Boggio et al., 2008). It has shown efficacy on the clinical symptoms of depression, on both depressive and manic symptoms of bipolar disorder, cognitive functioning in schizophrenia, episodic memory in Alzheimer’s disease, motor symptoms and working memory in Parkinson’s disease, on the amount of insults in epilepsy, on rehabilitation of motor function, and language disorder after stroke and on tinnitus (Floel, 2014; Kuo et al., 2014). tDCS is a safe treatment with few, if any, side effects (Nitsche et al., 2008). Some mild side effects of a transient nature that have been mentioned in association with tDCS are a slight headache, an itching or tingling sensation at the location of the electrodes and redness of the skin at the location of the electrodes. However, such side effects are also reported after placebo (sham) treatment (Brunoni et al., 2014). Other advantages of this technique are that tDCS equipment is relatively cheap, the treatment can be given after a short training course, and it is easily portable.
Compared to transcranial magnetic stimulation (TMS), another form of focal stimulation that has often been used as an alternative treatment option for AH (Slotema et al., 2014), tDCS has some explicit benefits when using it for research. It is easier to apply an identical placebo treatment, as less physical sensations occur compared to TMS. The itching or tingling sensation that is sometimes mentioned by participants is often only present at the start of treatment and disappears quickly. To mimic this in a placebo treatment, it helps to start with a short period of active stimulation (30–40 s) after which stimulation slowly regresses. During the rest of the treatment period, no active stimulation takes place. This short active stimulation period does not have modulating effects on the brain, but it properly mimics the physical sensations of active treatment. Furthermore, it is possible to preprogram tDCS equipment to apply placebo treatment, which makes it easier to perform double blind sham-controlled trials (Nitsche et al., 2008).
Transcranial Direct Current Stimulation in AH
The use of tDCS as a treatment option for medication resistant AH is relatively new and has till now only been tested in patients with AH in the context of psychotic disorders. Homan et al. (2011) were the first to explore this in a case study. For 10 consecutive days, the patient received daily treatment of 15 min tDCS at an intensity of 1 mA. The cathode was placed on the left temporoparietal cortex (TPC), a location that has been linked to the experience of AH (Silbersweig et al., 1995; Shergill et al., 2000). The anode was placed on the right supraorbital area. Using this method, they were able to ameliorate medication resistant AH. Moreover, this effect was still present 6 weeks after treatment. A more recent case study reported a reduction of 90% in AH severity after 2 months of daily 20 min tDCS at an intensity of 1 mA (Andrade, 2013). After this, treatment was increased to twice daily and an intensity of 3 mA, which led to increased improvement in AH severity. This improvement was still present after 3 years of daily maintenance treatment, but when treatment frequency was reduced to once per 2 days the ameliorating effects disappeared. In this study, the cathode was also placed on the left TPC, but the anode was placed on the left dorsolateral prefrontal cortex (DLPFC). This is an area that is often used in studies investigating the effects of tDCS on cognitive functioning (Hoy et al., 2014). These two tDCS locations have been used in several other case studies reporting positive effects of tDCS on AH severity after multiple sessions of 20 min tDCS at an intensity of 2 mA (Rakesh et al., 2013; Shiozawa et al., 2013; Shivakumar et al., 2013; Nawani et al., 2014). However, all these studies were open-label without a control condition, meaning that non-specific effects (i.e., placebo-effects) may have been of large influence. Brunelin et al. (2012) were the first to publish a tDCS study in AH in which a control group was included. In this study, 15 patients received a 20 min tDCS treatment twice daily at an intensity of 2 mA, for 5 consecutive days and an equal number of patients received sham. In this study, the cathode was also placed on the left TPC and the anode on the left DLPFC. They found a robust decrease in AH severity of 30% compared to a placebo group of equal size. Furthermore, a significant decrease was found in other symptoms as measured by the Positive and Negative Syndrome Scale (PANSS), such as negative symptoms. These positive effects were still present after 3 months. A more recent study by the same group, using a partially overlapping sample of 28 patients and identical methods, reported a decrease of 46% in AH frequency in medication resistant patients after active treatment, whereas no such effect occurred in the placebo group (Mondino et al., 2014). A recent open label study including 21 patients with schizophrenia and the same stimulation parameters and locations as Brunelin et al. (2012) found a similar improvement of 32% in AH severity. However, this study did not include a placebo condition (Bose et al., 2014). Up till now, one pilot study has been published that reports no beneficial effect of tDCS treatment on AH (Fitzgerald et al., 2014). This study tested the effects of both unilateral (N = 13) and bilateral (N = 11) tDCS on AH compared to placebo. In total, patients underwent 15 treatments in 3 weeks time. The AH did not respond to either treatment method. However, it is important to note that this study had a very small sample size and rated AH severity based on the PANSS only. This scale does not measure AH in much detail and the different severity scores of the hallucination item are found to be hard to differentiate (Santor et al., 2007). Other studies mostly use the Auditory Hallucination Rating Scale (AHRS) to measure AH severity. See Table 1 for a summary of all included studies.
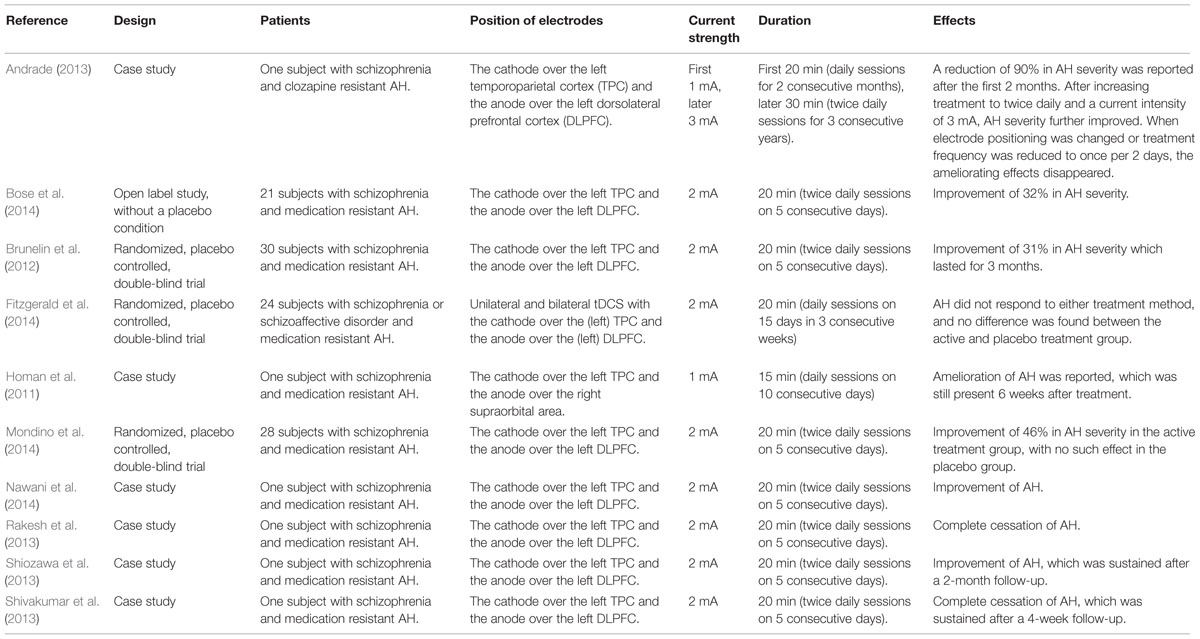
TABLE 1. Studies using tDCS for the treatment of auditory hallucinations (AH).
It is still unclear in what way tDCS might influence AH. As all studies that report positive results up till now have used the left TPC as the location for the cathode, it appears that the inhibiting action of tDCS on that specific location is important for the beneficial effects. It is unclear if excitation on the left DLPFC also influences AH severity. Brunelin et al. (2012) associated excitation on this location with a decrease of negative symptoms. However, Andrade (2013) found that using a more neutral position for the anode, namely the left mastoid, caused the beneficial effects on AH to vanish. This implicates that the excitatory effect of the anode on the DLPFC is important to induce a beneficial effect on AH. Possibly this can be explained by a positive effect from anodal stimulation of the left DLPFC on working memory. This hypotheses is mainly derived from literature on tinnitus, for which tDCS has also been reported to be effective. Like schizophrenia, tinnitus has been associated with reduced executive control (Heeren et al., 2014). Besides, tinnitus has been found to be alleviated by tDCS over the DLPFC (Frank et al., 2012). These authors hypothesized that improved executive control, as induced by tDCS over the DLPFC, acts as a mediator for the impact from tDCS on tinnitus (Heeren et al., 2014). It may be that a similar therapeutic mechanism is involved in the therapeutic effect of tDCS for AH. Reduced inhibition of irrelevant verbal information may be an important underlying mechanism of AH, speculatively AH could result from misattribution of self-generated information to an external source (Daalman et al., 2011). Application of anodal tDCS over de left DLPFC has been found to enhance working memory, which plays an important role in the executive control of information (Brunoni and Vanderhasselt, 2014). It could therefore be speculated that anodal tDCS over the left DLPFC induces the ameliorating effects on AH by improving the inhibition of irrelevant verbal information. Whether this excitation must take place at the left DLPFC is, however, yet unclear, as the first case study in this field used the right supraorbital area for the anode and still showed a positive result (Homan et al., 2011). Moreover, tDCS does not only produce focal effects but also indirect effects on surrounding brain areas and their connections (Keeser et al., 2011). The more distal effects of tDCS could also be of influence on the ameliorating effects on AH. Imaging studies combined with tDCS in AH could provide more insight in the exact neurological underpinnings of the effects of this treatment.
Taken together, the results of tDCS as an alternative treatment option for AH are preliminary and so far mostly positive. However, a note of caution may be in place here. When new treatment strategies are introduced, the initial reports tend to feature relatively small sample sizes and favorable results, whereas small studies with negative findings do not tend to be published (Emerson et al., 2010; Sommer et al., 2012a). With an increase of studies with larger sample sizes over time, negative findings tend to become published as well. Such trends have led effect sizes to decrease per year of publication (Munafo and Flint, 2010). This effect has also been visible in the application of TMS for AH (Slotema et al., 2012). As tDCS in the treatment of AH is a young treatment method, future studies may well show less favorable results. In the University Medical Center Utrecht, we have started a large randomized double blind trial to investigate the effects of tDCS on AH. We plan to include 62 patients and expect to be able to report results in autumn 2015. It is important to await such studies with large sample sizes before conclusions are drawn about the efficacy of tDCS. This also means that there is a large responsibility for scientific periodic journals to also publish negative findings of such treatments, to help reduce publication bias for positive results.
Moreover, it is of importance that placebo treatments in double blind trials are hard to distinguish from active tDCS treatment. At this point, all placebo-controlled trials in this field have used tDCS at an intensity of 2 mA (Brunelin et al., 2012; Fitzgerald et al., 2014; Mondino et al., 2014). For 1 mA tDCS, it has been reported that placebo treatment is highly identical to active treatment. Both participants and investigators were not able to distinguish between the two (Gandiga et al., 2006). This provides confidence that both participants and investigators will remain well blinded throughout the duration of a double blind trial. However, it is yet unsure if the same applies for tDCS stimulation at 2 mA, as the physical sensations at this intensity are more pronounced and redness of the skin may occur. Although the literature is still unclear if participants themselves are able to differentiate between 2 mA active stimulation and placebo treatment, it has been found that redness of the skin is a possible clue for researchers to differentiate between the two (O’Connell et al., 2012; Palm et al., 2013). However, it is important that these results stem from crossover studies, in which subtle differences between treatments and the effects on each individual participant attract more attention. Brunoni et al. (2014) investigated tDCS blinding of 2 mA stimulation in a large sample of patients with a depression disorder, using a parallel design. Each patient received either active or placebo treatment. They found that patients were able to identify 2 mA active treatment above chance level, but this appeared to be related to the occurrence of clinical response. Patients who did not show clinical response to treatment were not able to identify active treatment. However, this study did not mention results about the accuracy of blinding in tDCS operators, which were different investigators than the assessors of the clinical effect of the treatment. Knowing if a parallel design has advantages for the accuracy of blinding in tDCS operators is important to assess the reliability of results from double blind studies using placebo-controlled tDCS in parallel designs.
At this time, studies using tDCS in AH have highly similar methods, using 15–20 min of treatment at 1–2 mA and mostly placing the electrodes over the left TPC and left DLPFC. Future research could further investigate if these are indeed the most optimal parameters and locations for tDCS in AH. In TMS, the left TPC is also the most used brain area for inhibitory stimulation as a treatment for AH. Multiple attempts at other locations for TMS did not lead to positive results compared to placebo (Slotema et al., 2014). Considering that, the choice for the left TPC as a location for the cathode in tDCS seems logical. However, it may be worth the effort to test the efficacy of both cathodal and anodal tDCS on other brain areas that have been associated with AH.
Furthermore, the precision of the treatment in influencing the targeted brain areas could possibly be optimized. In most studies, relatively large electrodes are used with a surface size of 35 cm2. However, it is also possible to use smaller electrodes with a surface size of 25 cm2 or even so called ‘high definition’ tDCS in which electrodes are used with a diameter of 12 mm or less (Minhas et al., 2010). Such a method may increase the precision of treatment by decreasing the amount of electricity that is lost due to distribution over the scalp. But using smaller electrodes should be investigated thoroughly, as the neuromodulating effects of small electrodes can strongly differ from those of big electrodes (Nitsche et al., 2008). It is possible that the desired effects are eliminated instead of increased using small electrodes, as they are designed for more focal effects and will have less effect on surrounding brain areas and their connections. The use of small electrodes also increases the need for more precision in placing the electrodes on the scalp. Currently, electrode placement is mostly done using the international 10–20 system for EEG electrode placement (Jasper, 1958), but it is unclear whether this offers enough precision when using smaller electrodes. A stereotactic neuronavigation technique based on an individual’s structural MRI image may be a suitable option to offer more reliability that the focus of tDCS treatment is targeted at the right brain area (Neggers et al., 2004; Fitzgerald et al., 2009; Sack et al., 2009).
Conclusion
At this moment, tDCS appears to be a possible new treatment option to help reduce treatment-resistant AH. However, as currently only three randomized controlled trials have been published with relatively small sample sizes, two of which reporting positive results and one with non-significant results, insufficient data is available to determine if tDCS treatment is indeed effective in AH. Future placebo-controlled trials in large samples will have to assess if the mainly positive results up till now can be replicated. Furthermore, different methods and parameters for stimulation, localization, and precision of tDCS should be investigated in more detail to further optimize this treatment.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This work was supported by ZonMW (Dutch Scientific Research Organization), Innovation Impulse (VIDI): ‘where the voices come from, and how to get rid of them,’ a grant to IECS (nr. 017.106.301).
References
Andrade, C. (2013). Once- to twice-daily, 3-year domiciliary maintenance transcranial direct current stimulation for severe, disabling, clozapine-refractory continuous auditory hallucinations in schizophrenia. J. ECT. 29, 239–242. doi: 10.1097/YCT.0b013e3182843866
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Andreasen, N. C., and Flaum, M. (1991). Schizophrenia: the characteristic symptoms. Schizophr. Bull. 17, 27–49. doi: 10.1093/schbul/17.1.27
Bentall, R. P., Haddock, G., and Slade, P. D. (1994). Cognitive-behavior therapy for persistent auditory hallucinations – from theory to therapy. Behav. Ther. 25, 51–66. doi: 10.1016/S0005-7894(05)80145-5
Boggio, P. S., Rigonatti, S. P., Ribeiro, R. B., Myczkowski, M. L., Nitsche, M. A., Pascual-Leone, A.,et al. (2008). A randomized, double-blind clinical trial on the efficacy of cortical direct current stimulation for the treatment of major depression. Int. J. Neuropsychopharmacol. 11, 249–254. doi: 10.1017/S1461145707007833
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Bose, A., Shivakumar, V., Narayanaswamy, J. C., Nawani, H., Subramaniam, A., Agarwal, S. M.,et al. (2014). Insight facilitation with add-on tDCS in schizophrenia. Schizophr. Res. 156, 63–65. doi: 10.1016/j.schres.2014.03.029
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Brunelin, J., Mondino, M., Gassab, L., Haesebaert, F., Gaha, L., Suaud-Chagny, M. F.,et al. (2012). Examining transcranial direct-current stimulation (tDCS) as a treatment for hallucinations in schizophrenia. Am. J. Psychiatry 169, 719–724. doi: 10.1176/appi.ajp.2012.11071091
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Brunoni, A. R., Nitsche, M. A., Bolognini, N., Bikson, M., Wagner, T., Merabet, L.,et al. (2012). Clinical research with transcranial direct current stimulation (tDCS): challenges and future directions. Brain Stimul. 5, 175–195. doi: 10.1016/j.brs.2011.03.002
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Brunoni, A. R., Schestatsky, P., Lotufo, P. A., Bensenor, I. M., and Fregni, F. (2014). Comparison of blinding effectiveness between sham tDCS and placebo sertraline in a 6-week major depression randomized clinical trial. Clin. Neurophysiol. 125, 298–305. doi: 10.1016/j.clinph.2013.07.020
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Brunoni, A. R., and Vanderhasselt, M. (2014). Working memory improvement with non-invasive brain stimulation of the dorsolateral prefrontal cortex: a systematic review and meta-analysis. Brain Cogn. 86, 1–9. doi: 10.1016/j.bandc.2014.01.008
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Daalman, K., Van Zandvoort, M., Bootsman, F., Boks, M., Kahn, R., and Sommer, I. (2011). Auditory verbal hallucinations and cognitive functioning in healthy individuals. Schizophr. Res. 132, 203–207. doi: 10.1016/j.schres.2011.07.013
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Emerson, G. B., Warme, W. J., Wolf, F. M., Heckman, J. D., Brand, R. A., and Leopold, S. S. (2010). Testing for the presence of positive-outcome bias in peer review: a randomized controlled trial. Arch. Intern. Med. 170, 1934–1939. doi: 10.1001/archinternmed.2010.406
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Fitzgerald, P. B., Hoy, K., Mcqueen, S., Maller, J. J., Herring, S., Segrave, R.,et al. (2009). A randomized trial of rTMS targeted with MRI based neuro-navigation in treatment-resistant depression. Neuropsychopharmacology 34, 1255–1262. doi: 10.1038/npp.2008.233
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Fitzgerald, P. B., Mcqueen, S., Daskalakis, Z. J., and Hoy, K. E. (2014). A negative pilot study of daily bimodal transcranial direct current stimulation in schizophrenia. Brain Stimul. 7, 813–816. doi: 10.1016/j.brs.2014.08.002
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Floel, A. (2014). tDCS-enhanced motor and cognitive function in neurological diseases. Neuroimage 85(Pt 3), 934–947. doi: 10.1016/j.neuroimage.2013.05.098
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Frank, E., Schecklman, M., Landgrebe, M., Burger, J., Kreuzer, P., Poeppl, T. B.,et al. (2012). Treatment of chronic tinnitus with repeated sessions of prefrontal transcranial direct current stimulation: outcomes from an open-label pilot study. J. Neurol. 259, 327–333. doi: 10.1007/s00415-011-6189-4
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Gandiga, P. C., Hummel, F. C., and Cohen, L. G. (2006). Transcranial DC stimulation (tDCS): a tool for double-blind sham-controlled clinical studies in brain stimulation. Clin. Neurophysiol. 117, 845–850. doi: 10.1016/j.clinph.2005.12.003
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Harkavy-Friedman, J. M., Kimhy, D., Nelson, E. A., Venarde, D. F., Malaspina, D., and Mann, J. J. (2003). Suicide attempts in schizophrenia: the role of command auditory hallucinations for suicide. J. Clin. Psychiatry 64, 871–874. doi: 10.4088/JCP.v64n0803
Heeren, A., Maurage, P., Perrot, H., De Volder, A., Renier, L., Araneda, R.,et al. (2014). Tinnitus specifically alters the top-down executive control sub-component of attention: evidence from the attention network task. Behav. Brain Res. 269, 147–154. doi: 10.1016/j.bbr.2014.04.043
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Homan, P., Kindler, J., Federspiel, A., Flury, R., Hubl, D., Hauf, M.,et al. (2011). Muting the voice: a case of arterial spin labeling-monitored transcranial direct current stimulation treatment of auditory verbal hallucinations. Am. J. Psychiatry 168, 853–854. doi: 10.1176/appi.ajp.2011.11030496
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Horvath, J. C., Forte, J. D., and Carter, O. (2015). Evidence that transcranial direct current stimulation (tDCS) generates little-to-no reliable neurophysiologic effect beyond MEP amplitude modulation in healthy human subjects: a systematic review. Neuropsychologia 66, 213–236. doi: 10.1016/j.neuropsychologia.2014.11.021
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Hoy, K. E., Arnold, S. L., Emonson, M. R., Daskalakis, Z. J., and Fitzgerald, P. B. (2014). An investigation into the effects of tDCS dose on cognitive performance over time in patients with schizophrenia. Schizophr. Res. 155, 96–100. doi: 10.1016/j.schres.2014.03.006
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Jasper, H. H. (1958). Report of the committee on methods of clinical examination in electroencephalography. Electroencephalogr. Clin. Neurophysiol. 10, 370–375. doi: 10.1016/0013-4694(58)90053-1
Keeser, D., Meindl, T., Bor, J., Palm, U., Pogarell, O., Mulert, C.,et al. (2011). Prefrontal transcranial direct current stimulation changes connectivity of resting-state networks during fMRI. J. Neurosci. 31, 15284–15293. doi: 10.1523/JNEUROSCI.0542-11.2011
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Kuo, M. F., Paulus, W., and Nitsche, M. A. (2014). Therapeutic effects of non-invasive brain stimulation with direct currents (tDCS) in neuropsychiatric diseases. Neuroimage 85(Pt 3), 948–960. doi: 10.1016/j.neuroimage.2013.05.117
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
McCarthy-Jones, S., Trauer, T., Mackinnon, A., Sims, E., Thomas, N., and Copolov, D. L. (2014). A new phenomenological survey of auditory hallucinations: evidence for subtypes and implications for theory and practice. Schizophr. Bull. 40, 225–235. doi: 10.1093/schbul/sbs156
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Minhas, P., Bansal, V., Patel, J., Ho, J. S., Diaz, J., Datta, A.,et al. (2010). Electrodes for high-definition transcutaneous DC stimulation for applications in drug delivery and electrotherapy, including tDCS. J. Neurosci. Methods 190, 188–197. doi: 10.1016/j.jneumeth.2010.05.007
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Miranda, P. C., Lomarev, M., and Hallett, M. (2006). Modeling the current distribution during transcranial direct current stimulation. Clin. Neurophysiol. 117, 1623–1629. doi: 10.1016/j.clinph.2006.04.009
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Mondino, M., Haesebaert, F., Poulet, E., Suaud-Chagny, M. F., and Brunelin, J. (2014). Fronto-temporal transcranial direct current stimulation (tDCS) reduces source-monitoring deficits and auditory hallucinations in patients with schizophrenia. Schizophr. Res. 161, 515–516 doi: 10.1016/j.schres.2014.10.054
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Munafo, M. R., and Flint, J. (2010). How reliable are scientific studies? Br. J. Psychiatry 197, 257–258. doi: 10.1192/bjp.bp.109.069849
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Nawani, H., Kalmady, S. V., Bose, A., Shivakumar, V., Rakesh, G., Subramaniam, A.,et al. (2014). Neural basis of tDCS effects on auditory verbal hallucinations in schizophrenia: a case report evidence for cortical neuroplasticity modulation. J. ECT. 30, e2–e4. doi: 10.1097/YCT.0b013e3182a35492
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Nayani, T. H., and David, A. S. (1996). The auditory hallucination: a phenomenological survey. Psychol. Med. 26, 177–189. doi: 10.1017/S003329170003381X
Neggers, S. F., Langerak, T. R., Schutter, D. J., Mandl, R. C., Ramsey, N. F., Lemmens, P. J.,et al. (2004). A stereotactic method for image-guided transcranial magnetic stimulation validated with fMRI and motor-evoked potentials. Neuroimage 21, 1805–1817. doi: 10.1016/j.neuroimage.2003.12.006
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Nitsche, M. A., Cohen, L. G., Wassermann, E. M., Priori, A., Lang, N., Antal, A.,et al. (2008). Transcranial direct current stimulation: state of the art 2008. Brain Stimul. 1, 206–223. doi: 10.1016/j.brs.2008.06.004
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
O’Connell, N. E., Cossar, J., Marston, L., Wand, B. M., Bunce, D., Moseley, G. L.,et al. (2012). Rethinking clinical trials of transcranial direct current stimulation: participant and assessor blinding is inadequate at intensities of 2mA. PLoS ONE 7:e47514. doi: 10.1371/journal.pone.0047514
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Palm, U., Reisinger, E., Keeser, D., Kuo, M. F., Pogarell, O., Leicht, G.,et al. (2013). Evaluation of sham transcranial direct current stimulation for randomized, placebo-controlled clinical trials. Brain Stimul. 6, 690–695. doi: 10.1016/j.brs.2013.01.005
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Priori, A. (2003). Brain polarization in humans: a reappraisal of an old tool for prolonged non-invasive modulation of brain excitability. Clin. Neurophysiol. 114, 589–595. doi: 10.1016/S1388-2457(02)00437-6
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Rakesh, G., Shivakumar, V., Subramaniam, A., Nawani, H., Amaresha, A. C.,et al. (2013). Monotherapy with tDCS for schizophrenia: a case report. Brain Stimul. 6, 708–709. doi: 10.1016/j.brs.2013.01.007
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Sack, A. T., Cohen, K. R., Schuhmann, T., Moerel, M., Walsh, V., and Goebel, R. (2009). Optimizing functional accuracy of TMS in cognitive studies: a comparison of methods. J. Cogn. Neurosci. 21, 207–221. doi: 10.1162/jocn.2009.21126
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Santor, D. A., Ascher-Svanum, H., Lindenmayer, J. P., and Obenchain, R. L. (2007). Item response analysis of the positive and negative syndrome scale. BMC Psychiatry 7:66. doi: 10.1186/1471-244X-7-66
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Shergill, S. S., Brammer, M. J., Williams, S. C., Murray, R. M., and Mcguire, P. K. (2000). Mapping auditory hallucinations in schizophrenia using functional magnetic resonance imaging. Arch. Gen. Psychiatry 57, 1033–1038. doi: 10.1001/archpsyc.57.11.1033
Shergill, S. S., Murray, R. M., and Mcguire, P. K. (1998). Auditory hallucinations: a review of psychological treatments. Schizophr. Res. 32, 137–150. doi: 10.1016/S0920-9964(98)00052-8
Shiozawa, P., Da Silva, M. E., Cordeiro, Q., Fregni, F., and Brunoni, A. R. (2013). Transcranial direct current stimulation (tDCS) for the treatment of persistent visual and auditory hallucinations in schizophrenia: a case study. Brain Stimul. 6, 831–833. doi: 10.1016/j.brs.2013.03.003
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Shivakumar, V., Bose, A., Rakesh, G., Nawani, H., Subramaniam, A., Agarwal, S. M.,et al. (2013). Rapid improvement of auditory verbal hallucinations in schizophrenia after add-on treatment with transcranial direct-current stimulation. J. ECT. 29, e43–e44. doi: 10.1097/YCT.0b013e318290fa4d
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Silbersweig, D. A., Stern, E., Frith, C., Cahill, C., Holmes, A., Grootoonk, S.,et al. (1995). A functional neuroanatomy of hallucinations in schizophrenia. Nature 378, 176–179. doi: 10.1038/378176a0
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Slotema, C. W., Aleman, A., Daskalakis, Z. J., and Sommer, I. E. (2012). Meta-analysis of repetitive transcranial magnetic stimulation in the treatment of auditory verbal hallucinations: update and effects after one month. Schizophr. Res. 142, 40–45. doi: 10.1016/j.schres.2012.08.025
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Slotema, C. W., Blom, J. D., Van, L. R., Hoek, H. W., and Sommer, I. E. (2014). Review of the efficacy of transcranial magnetic stimulation for auditory verbal hallucinations. Biol. Psychiatry 76, 101–110. doi: 10.1016/j.biopsych.2013.09.038
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Sommer, I. E., Aleman, A., Slotema, C. W., and Schutter, D. J. (2012a). Transcranial stimulation for psychosis: the relationship between effect size and published findings. Am. J. Psychiatry 169, 1211. doi: 10.1176/appi.ajp.2012.12060741
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Sommer, I. E. C., Koops, S., and Blom, J. D. (2012b). Comparison of auditory hallucinations across different disorders and syndromes. Neuropsychiatry 2, 57–68. doi: 10.2217/npy.12.2
Stagg, C. J., and Nitsche, M. A. (2011). Physiological basis of transcranial direct current stimulation. Neuroscientist 17, 37–53. doi: 10.1177/1073858410386614
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Keywords: auditory hallucinations, focal stimulation, tDCS, psychosis, voices
Citation: Koops S, van den Brink H and Sommer IEC (2015) Transcranial direct current stimulation as a treatment for auditory hallucinations. Front. Psychol. 6:244. doi: 10.3389/fpsyg.2015.00244
Received: 02 January 2015; Accepted: 17 February 2015;
Published online: 06 March 2015.
Edited by:
Anna Abraham, Leeds Beckett University, UKReviewed by:
Alexandre Heeren, Univesité Catholique de Louvain,BelgiumPeter Moseley, Durham University, UK
Copyright © 2015 Koops, van den Brink and Sommer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Iris E. C. Sommer, Psychiatry Department, Brain Center Rudolf Magnus, University Medical Center Utrecht, Heidelberglaan 100, 3584 CX Utrecht, NetherlandsaS5zb21tZXJAdW1jdXRyZWNodC5ubA==