 Bruno Luis Schaab1*
Bruno Luis Schaab1* Lara Finkler Cunha2Desiree Cordoni Silveira1Pamela Carvalho da Silva1
Lara Finkler Cunha2Desiree Cordoni Silveira1Pamela Carvalho da Silva1 Kellen Greff Ballejos3Gabriela Bertoletti Diaz3Vanessa Kaiser1Prisla Ücker Calvetti1Sílvio César Cazella2
Kellen Greff Ballejos3Gabriela Bertoletti Diaz3Vanessa Kaiser1Prisla Ücker Calvetti1Sílvio César Cazella2 Helena Maria Tannhauser Barros4Caroline Tozzi Reppold1
Helena Maria Tannhauser Barros4Caroline Tozzi Reppold1- 1Psychological Assessment Laboratory, Health Sciences Program, Federal University of Health Sciences of Porto Alegre (UFCSPA), Porto Alegre, Brazil
- 2Department of Exact Sciences and Social Applied Science, Health Sciences Program, Federal University of Health Sciences of Porto Alegre (UFCSPA), Porto Alegre, Brazil
- 3Psychological Assessment Laboratory, Rehabilitation Sciences Program, Federal University of Health Sciences of Porto Alegre (UFCSPA), Porto Alegre, Brazil
- 4Department of Pharmacosciences, Health Sciences Program, Federal University of Health Sciences of Porto Alegre (UFCSPA), Porto Alegre, Brazil
Introduction: Epidemiological data suggest substantial issues on the mental health of university students worldwide. Self-compassion is associated with lower rates of psychological distress and better positive mental health. Thus, we have developed a app-based intervention based on self-compassion principles targeting the prevention and promotion of mental health in college students. The current pilot study assessed adherence to intervention, preliminary mental health benefits, and satisfaction and acceptability with the app among Brazilian college students.
Methods: The study employed a pre-experimental single-group design along with pre-test and post-test assessments (n = 23). A mixed methods approach was utilized to comprehensively assess the outcomes of the intervention.
Results: The overall adherence rate for the intervention was 37.87%, with 26.26% of participants successfully completing all modules. Among the 21 outcomes assessed, 15 exhibited statistically significant results. Notably, there was a substantial increase in self-compassion, demonstrating a large effect size (d = 1.15), and a moderate effect size reduction in stress (d = 0.62) and anxiety (d = 0.52). All satisfaction indicators for the intervention received scores above 7. The intervention was well-received by participants who completed it, although a potential barrier identified was the volume of text within the app and the need to adopt a more playful and concise format for the intervention.
Discussion: Despite a notable participant dropout, the adherence to intervention aligns with patterns observed in other online interventions conducted in real-world settings. The observed mental health benefits, high satisfaction levels, and positive acceptance underscore the rationale for pursuing a subsequent randomized clinical trial.
1 Introduction
In developed countries and some developing countries, such as Brazil, university life typically spans the period between the end of adolescence and early adulthood. Emotional conflicts typical of this developmental phase, along with the demanding and competitive academic environment, are associated with the onset of mental health disorders and psychopathological symptoms before the professional life of adults (Pedrelli et al., 2019; Broglia et al., 2021; Campbell et al., 2022). Therefore, even before COVID-19, mental health issues of college students were a concern in both educational and health segments. Epidemiological data prior to COVID-19 suggested that up to 35% of college students met criteria for a common mental disorder (Auerbach et al., 2018). In Brazil, between 34 and 49% of college students reported experiencing emotional distress (Graner and Cerqueira, 2019). Since the onset of the COVID-19 pandemic and the necessity for lockdowns, there has been a decline in the mental health status of university students worldwide (Buizza et al., 2022; Lemyre et al., 2023).
Nowadays, even with the end of the social isolation and the return to normal life globally, recent estimates still suggest a high prevalence of mental disorders and psychopathology symptoms among college students, especially depression, anxiety, and stress (Estrada-Araoz et al., 2023; Farfán-Latorre et al., 2023; Liverpool et al., 2023; Dave et al., 2024). These mental health issues are not just a personal burden; they also contribute to several challenges in daily life, such as poor academic performance, impairments in academic adherence (Mboya et al., 2020), difficulties in peers relationships (Dachew et al., 2015), substance use (Mboya et al., 2020), self-harm, risky sexual behaviors, and negative impacts on physical health. In addition, suicide is a significant concern, ranking as the fourth leading cause of death among individuals aged 15 to 29 (World Health Organization, 2019).
Given this, there is a recognized urgency for worldwide policies addressing the mental health of university students, especially for those students from low-income countries or without regular access to mental health care, as in Brazil. Beyond pharmacological interventions, it is crucial the development and offering of programs for fostering psychological resources (Worsley et al., 2022). These psychological programs may contribute to positive mental health and alleviate psychological distress through cultivating emotion regulation skills, that is, the capacity to intentionally manage and control emotions occurrence, intensity and duration through attitudes, behaviors, and thoughts (Leahy et al., 2011).
In recent years, typical dimensions of Positive Psychology (PP) have emerged as promising strategies for emotion regulation, notably self-compassion skills (Inwood and Ferrari, 2018). Self-compassion encompasses attitudes of kindness, tolerance, and support towards oneself during challenging times or when confronted with feelings of failure and inadequacy (Neff, 2023). Also, self-compassion entails recognizing our own suffering with the intention of healing it (Neff, 2011). This involves directing towards ourselves the same compassion that we might extend to a person experiencing distress, pain or facing life challenges (Neff and Germer, 2018; Neff, 2023).
According to seminal author Neff (2023), self-compassion encompasses three interrelated components: self-kindness versus self-judgment, which involves being kind and understanding towards oneself during moments of inadequacy, suffering, or failure instead of being self-critical or neglecting one’s suffering; common humanity versus isolation, which involves recognizing that mistakes and failures are part of the human condition and that we should not feel isolated; and mindfulness versus over-identification, which involves seeing oneself in a balanced and realistic way, without suppressing or exaggerating one’s thoughts or emotions, rather than over-identifying with them (Neff, 2011; Neff and Germer, 2018). Evidence suggests that higher rates of psychological distress among undergraduate students are associated with higher rates of self-criticism (McIntyre et al., 2018) and loneliness (Yang et al., 2023). Self-compassion interventions may cultivate skills that allow individuals to treat themselves with more kindness and less self-criticism; feel less lonely and more connected to others; and recognize their own thoughts and emotions and being mindfulness.
Cross-sectional studies have consistently indicated an association between self-compassion with lower rates of distress and higher rates of positive mental health, including optimism (Zhao et al., 2022), positive affect and life satisfaction (Stoeber et al., 2020), hope (Yang et al., 2016), compassion (López et al., 2018) and emotion regulation (Rech et al., 2023). Self-compassion appears to be particularly effective in alleviating the impacts of self-criticism and self-demand among university students (Wakelin et al., 2022), which are typically linked to poorer mental health (McIntyre et al., 2018). Since self-compassion skills may be learned and applied in everyday life, it’s been suggested to develop and implement self-compassion programs for promoting emotional well-being among university students and young people (Egan et al., 2022; Neff, 2023).
Different therapeutic approaches have focused on cultivating self-compassionate skills, including Compassion Focused Therapy (CFT) (Gilbert, 2010) and Mindful Self-Compassion (MSC) program (Neff and Germer, 2018). Despite specific differences in techniques, format and length of interventions, all these approaches have in common the promotion of self-compassionate skills. Systematic reviews of randomized clinical trials with meta-analysis suggests the efficacy of self-compassion interventions in enhancing self-compassion and, consequently, reducing depression, anxiety, and stress among the general population with moderate effect size (Kirby et al., 2017; Ferrari et al., 2019).
Despite the efficacy of these interventions, the most of them are still provided in a face-to-face format, potentially limiting access to their benefits. Recently, some studies have aimed to adapt these interventions into the online format to university students (Andersson et al., 2021; Serlachius et al., 2021; Beaumont et al., 2022), circumventing barriers present in face-to-face contexts, such as professional costs, service location, privacy and anonymity. The purpose of this app is to cultivate self-compassion skills among Brazilian university students for use in university life, which can reduce their psychological distress and improve positive mental health.
To the best of our knowledge, no digital intervention based on self-compassion specifically targeting Brazilian college students has been previously developed. Furthermore, only one app in Portuguese was found for cultivating self-compassion, which is the app 29K FJN from Portugal. Consequently, we created a new app called “Eu + Compassivo” (translated in English as “Me More Compassionate”) featuring a self-compassion-based intervention delivered through a smartphone app to prevent issues and promote better mental health of Brazilian college students. Thus, the purpose of this new app is to cultivate self-compassion skills among Brazilian university students for use in university life, which can reduce their psychological distress and improve positive mental health. Since this is a population with a high prevalence of common mental disorders, it is believed that college students can benefit from a self-compassion intervention.
As a pilot study, the research aims to identify indicators for conducting a randomized clinical trial (Lancaster, 2015; Lowe, 2019). The objectives include assessing the adherence to app and its preliminary benefits on mental health, along with the assessment of satisfaction and acceptability of the intervention.
2 Materials and methods
2.1 Eu + Compassivo app
The app constitutes an asynchronous psychoeducational intervention designed for the prevention and promotion of mental health among Brazilian college students. The content of the app primarily draws upon the principles of self-compassion as proposed by Neff (2011), as well as on the literature concerning the mental health of college students (Mofatteh, 2021).
The first step of app development involved drafting an intervention protocol in a PDF format. This protocol comprehensively outlined all facets of the app, including textual elements and psychological exercises aimed at cultivating self-compassion. Subsequently, the intervention protocol was assessed by six psychologists specialized in Positive Psychology and Clinical Psychology, who assessed the suitability of its contents and active components. Following this phase, the app’s coding and design processes commenced, culminating in the creation of version 1.0 of the app (Schaab et al., 2024).
The app comprises eight thematic modules that must be completed within a maximum 45-day timeframe. These modules consist of texts, audios, and videos that connect the principles of self-compassion with university life. Each module also includes exercises within the app to foster self-compassion, encouraging students to integrate these practices into their daily lives. The exercises encompass diverse tasks, such as writing and meditation, and focus on the dimensions outlined in the Self-Compassion Scale — specifically, self-kindness, self-judgment, common humanity, isolation, mindfulness, and over-identification (Neff, 2016). Table 1 presents the structure of the intervention. Below is a summary of each of the eight modules:
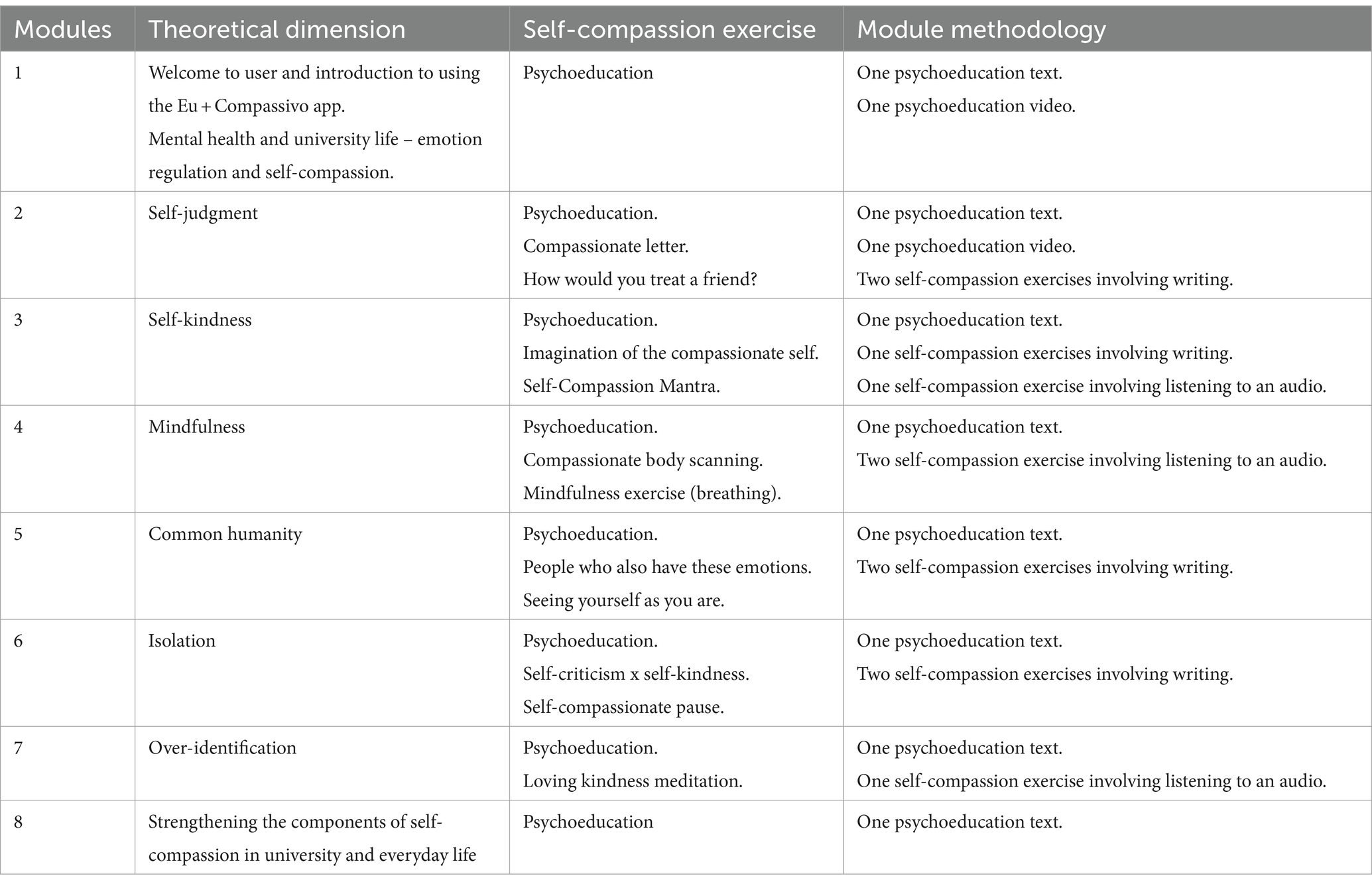
Table 1. Summary of app modules.
Module 1 – This module aims to teach college students about psychological distress, highlighting how these symptoms are associated with academic life stressors such as pressure for results and deadlines, competitiveness among classmates, separation from family, and beliefs about academic performance. It introduces the role of self-compassion as an emotional self-regulation mechanism. Additionally, it provides guidelines on using the app, including how the app works, the length of exercises, and how to prepare the personal environment for using the app.
Module 2 – This module introduces the self-judgment component. The authors considered it more viable to start with self-judgment because it is a common issue among college students. The module discusses the reasons behind self-criticism, such as beliefs about academic performance and self-efficacy. Module 2 highlights the importance of self-compassion in mitigating the harmful effects of self-criticism and teaches exercises to reduce self-criticism.
Module 3 – Module 3, as it addresses the component of self-kindness, highlights the importance of being kind, understanding and tolerant of oneself in the face of difficulties that arise in university life, such as not getting an internship or performing insufficiently on a task. Module 2 teaches two exercises for practicing self-kindness.
Module 4 – This module addresses the importance of mindfulness in university life and provides mindfulness exercises focusing on self-compassion. It is more practical than the previous modules. The reason it was presented in the middle of the intervention is that the researchers believed it was initially more appropriate to introduce the components of “self-judgment × self-kindness,” as this prior knowledge would facilitate the understanding of mindfulness in self-compassion.
Module 5 – This module addresses the common humanity component. Essentially, it emphasizes the importance of college students understanding that their perceived difficulties and suffering are shared experiences that other students also face. The exercises taught in this module aim to reinforce the sense of common humanity.
Module 6 – This module extends the discussion from Module 5, emphasizing the potential harmful effects of isolation. It proposes exercises designed to help college students feel less isolated while also encouraging self-kindness.
Module 7 – The seventh module addresses the remaining dimension of self-compassion, which is overidentification. This module highlights the importance of learning to recognize the thoughts and emotions that may occur in university life without neglecting or overestimating them. It teaches another mindfulness practice to cultivate this skill and is more practical compared to the other modules.
Module 8 – The last module provides a brief summary of the key points of the intervention and encourages college students to practice self-compassion on a daily basis to deal with the suffering arising from university life.
The app was developed in the JavaScript language and was based on principles of the user-centered approach. The app prioritizes features such as anonymity, confidentiality, and data security. It is currently accessible on both Android and iOS platforms. A prior study highlighted excellent usability and acceptability of the tool among Brazilian college students and informatic workers (Schaab et al., 2024). Figure 1 presents some screenshots of the app.
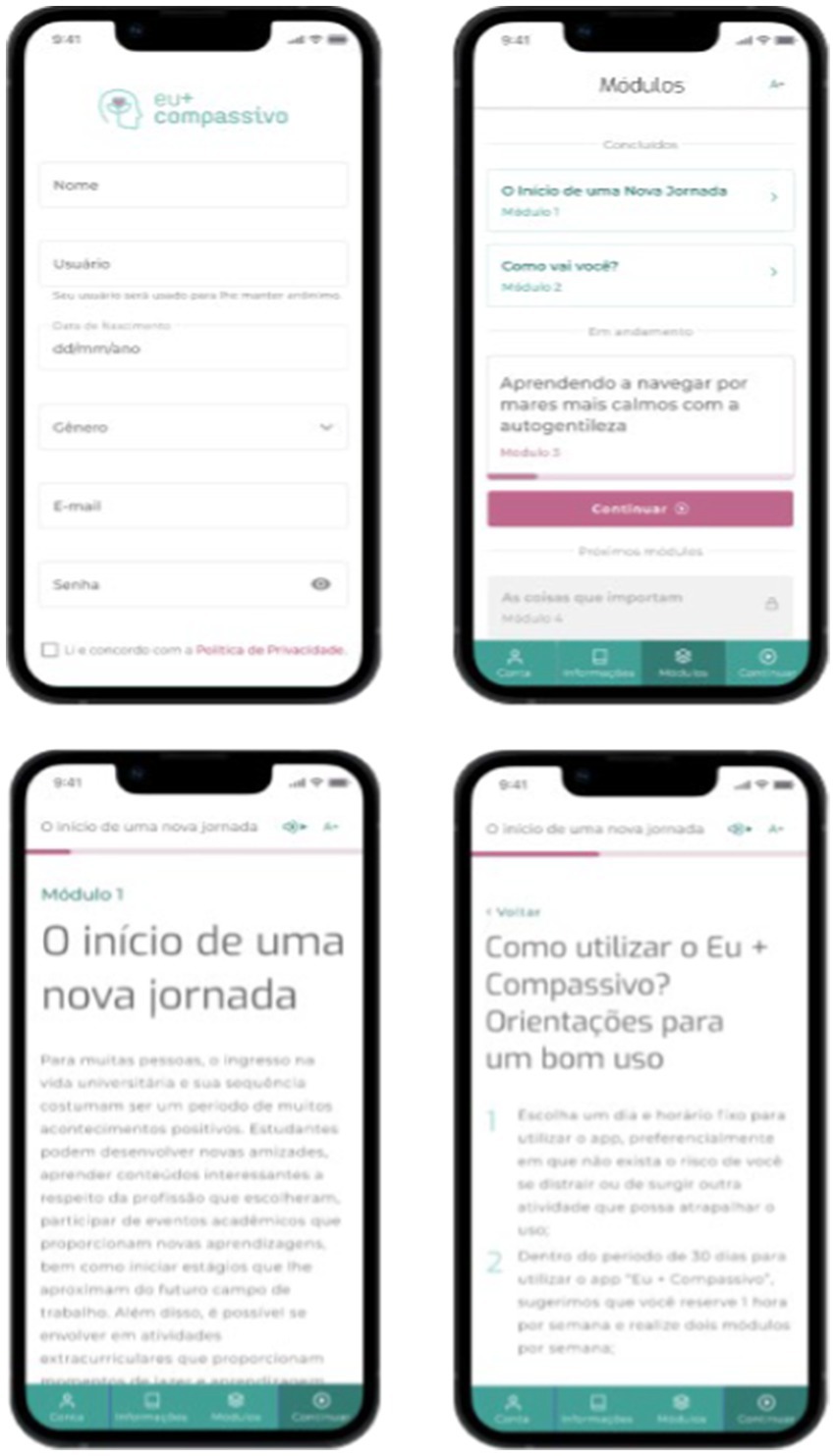
Figure 1. Screens of Eu + Compassivo.
2.2 Design
This pilot study used a pre-experimental design, involving a single group with both pre-test and post-test assessments (Shaughnessy et al., 2015). We assessed the intervention results using mixed methods (Creswell and Clark, 2011). The study protocol was previously registered on the Brazilian Clinical Trials platform1.
2.3 Participants
Initially, 99 undergraduate college students were recruited, surpassing the minimum requirement of 18 participants suggested by the sample calculation (Viechtbauer et al., 2015) and the minimum of 12 participants recommended in the scientific literature (Julious, 2005). The participants constituted a non-probabilistic and convenience sample (Shaughnessy et al., 2015). To be eligible, students had to declare at least mild symptoms of anxiety, stress, or depression due to issues in university life (as indicated through qualitative feedback from potential participants to researchers), be enrolled in an undergraduate course at a Brazilian university, possess a smartphone with Android and internet access, and declare proficiency in using a smartphone.
The participants’ mean age was 27.53 years (SD = 8.55 years). The majority of students originated from the southern region of Brazil (85.9%) and were enrolled in a public university (94.9%). Regarding smartphone usage patterns, 97% of participants reported using their smartphone more than 1 h daily, while 84.8% reported routinely using more than 3 apps on their cell phones. A significant portion of participants were in psychotherapy in parallel with the study (51.5%), and 47.5% were utilizing psychotropic medicines. Detailed demographic data are presented in Table 2.

Table 2. Sample characteristics.
2.4 Measurements and instruments
2.4.1 Mental health outcomes
2.4.1.1 Primary outcomes
Depression, Anxiety, and Stress – 21– item Depression, Anxiety and Stress Scale (DASS-21): Originally developed by Lovibond and Lovibond (1995), the DASS-21 assesses symptoms of depression, anxiety, and stress. Responses to its items are recorded on a Likert scale ranging from 0 to 3 (“strongly disagree” to “strongly agree,” respectively). In Brazil, adaptation and validation for the adult population were conducted by Vignola and Tucci (2014), demonstrating satisfactory internal consistency, with Cronbach’s alpha values of 0.92 for the depression subscale, 0.86 for anxiety, and 0.90 for stress. To obtain the score for each dimension, the sum of all items should be calculated and then multiplied by 2, resulting in a score ranging from 0 to 42.
Emotional well-being – WHO-5: this generic measure evaluates emotional well-being over the preceding 14 days (Topp et al., 2015). Comprising five items rated on a Likert scale from 0 to 5, it yields a score ranging from 0 to 25. Higher scores indicate greater emotional well-being. The WHO-5 exhibits satisfactory reliability.
Self-compassion – Self-Compassion Scale: originally proposed by Neff (2003) and validated in Brazil by Souza and Hutz (2016), this scale comprises six factors: self-kindness, self-judgment, mindfulness, over-identification, common humanity, and isolation. With 26 items scored on a Likert scale from “almost never” (1) to “almost always” (5). The study reported a Cronbach’s alpha value of 0.92 for the overall scale and values ranging between 0.66 and 0.81 for each factor, indicating adherence to the original factorial structure and confirming the instrument’s validity. After reversing the punctuation of specific items, the score for each dimension is determined by calculating the average of all its items. The overall self-compassion score is then computed as the average across self-kindness, self-judgment, mindfulness, over-identification, common humanity, and isolation.
Compassion – Santa Clara Brief Compassion Scale: developed by Hwang et al. (2008), this unidimensional scale aims to succinctly measure compassion with five items on a Likert scale ranging from “not at all true for me” (1) to “very true for me” (7). In validation among the Brazilian population, the scale demonstrated satisfactory internal consistency, with a Cronbach’s alpha of 0.84 (Marchetti et al., 2018). Each item should be summed, resulting in a total compassion score ranging from 5 to 35.
Emotion Regulation – Emotional Dysregulation Scale – Adults (EDEA): we employed a condensed version of the Emotional Self-Regulation Scale (EARE). Comprising 15 items rated on a 4-point Likert scale, with endpoints labeled as “none of the times/not at all” (0) and “always” (3) (Cremasco et al., 2020), this scale encompasses four factors: adequate coping strategies, externalization of aggression, pessimism, and paralysis. Validation in Brazil demonstrated consistent internal validity, with values ranging from 0.68 to 0.96 for each factor (Cremasco et al., 2020). The score for each subscale is the sum of its respective items. The total score for the subscales of adequate coping strategies, pessimism, and paralysis ranges from 0 to 12, while for externalizing aggression, it varies between 0 and 9. Higher scores indicate increased emotion dysregulation.
2.4.1.2 Secondary outcomes
Positive and Negative Affects – Positive and Negative Affect Schedule (PANAS): PANAS is a succinct two-dimensional self-report measure that assesses negative and positive affects (Watson et al., 1988). With 10 items in each affective dimension, respondents evaluate their experiences using a Likert scale that ranges from “not at all” (1) to “extremely” (5). In its Brazilian adult version, the instrument underwent validation and adaptation by Zanon et al. (2013), exhibiting satisfactory Cronbach’s alpha values. The total scores for negative affect and positive affect range from 5 to 50 and are obtained by summing the 10 items in each construct. Higher scores indicate greater intensity of the respective affects.
Satisfaction with Life – Life Satisfaction Scale (LSS): developed by Diener et al. (1985), this unidimensional measure assesses the cognitive facet of subjective well-being. LSS consists of 5 items on a Likert scale with anchors 1 and 7 denoting “strongly disagree” and “strongly agree.” Validated in Brazil by Zanon et al. (2014), LSS exhibited evidence of validity and satisfactory Cronbach’s alpha. The sum of item scores yields a total score between 5 and 35, with higher values indicating greater life satisfaction.
Hope – Cognitive Hope Scale (CHS): originating from Staats (1989), this measure focuses on the cognitive dimension of hope rooted in the Beckian theory of depression. Comprising 21 items arranged in a two-dimensional structure (self-centered hope and altruistic hope), responses are recorded on a two-column 5-point Likert scale. The scale captures both the desire and expectation aspects for each item (0 = do not want to; 5 = really want to; 0 = do not believe; 5 = believe a lot). In Brazil, the Cognitive Hope Scale underwent adaptation and validation by Pacico and Bastianello (2014) and demonstrated Cronbach’s alpha values of 0.86 for self-centered hope and 0.80 for altruistic hope. Expectation and desire scores for each item must be multiplied. The total cognitive hope score is the sum of these multiplied items, resulting in a score between 0 and 525. A higher total score indicates a higher level of cognitive hope.
Optimism – Life Orientation Test-Revised (LOT-R): developed by Scheier et al. (1994), this instrument assesses dispositional optimism through a unidimensional structure. Comprising 10 items, with 3 measuring optimism, 3 measuring pessimism, and 4 serving as “filter” items whose scores are not computed (Bastianello et al., 2014), responses are scored on a scale from 1 to 5, with anchors “strongly disagree” and “strongly agree.” The total scale score results from adding its six items, with three negative items being inverted. The LOT-R provides a total score between 6 and 30, with a higher score indicating a greater level of optimism. In Brazil, the LOT-R underwent validation and adaptation by Bastianello et al. (2014), demonstrating internal validity and a Cronbach’s alpha value of 0.80.
2.4.2 Other outcomes
Adherence – Determined by the ratio between the scheduled intervention modules and those effectively achieved by the participants.
Satisfaction – Intervention Satisfaction: an ad hoc measure was devised to evaluate satisfaction and acceptability of the intervention. This instrument comprises 6 items, assessed on a Likert-type scale ranging from 1 to 10 (“strongly disagree” and “strongly agree”).
Acceptability and Impressions Regarding the Intervention – Intervention and App Impressions and Perceptions Questionnaire: a qualitative questionnaire was formulated to encompass impressions, perceptions and acceptability regarding both the intervention and the app.
2.5 Procedures
Firstly, the study was shared on the authors’ social networks and within public and private universities in Brazil. Prospective participants expressed their interest by reaching out to the study’s main author (BLS) through email or WhatsApp. Upon contact, they received comprehensive information about the research procedures and made a voluntary decision to participate. All students who consented to join the study were placed on a waiting list for approximately 3 weeks to ensure simultaneous initiation of app usage.
Seven days prior to starting using the app, participants were provided with the Consent Form (CF) and the pre-test form through Google Forms. All participants provided their consent by clicking on option “yes, I have read the terms and agree to participate in the research” before responding to research forms. Subsequently, participants received a link for accessing the Play Store, allowing them to download and utilize the app on their personal smartphones. The app usage occurred within a natural context, granting students the flexibility to choose the day, time, and location for engaging in the activities that best suited their routines. Participants were advised to use the app for a minimum period of 30 days, completing two modules per week, with an additional 15 days provided to accommodate any potential interruptions to the intervention.
Seven days later, after completion of the intervention, participants were provided with the post-test questionnaire and a satisfaction and acceptability measure, administered through a Google Forms survey. Also, all participants provided their consent by clicking on option “yes, I have read the terms and agree to participate in the research.” Additionally, they were invited to respond to qualitative questions regarding their experience with the app. This step was facilitated by a trained research (DCS) assistant using either Google Meet or WhatsApp, based on the participant’s preference. Figure 2 displays a comprehensive view of the research procedures.

Figure 2. Procedures steps.
2.6 Data analysis procedures
All quantitative and categorical data were analyzed in the Statistical Package for the Social Sciences (SPSS), version 28.0 (SPSS® Inc., Chicago, IL, United States). Quantitative sociodemographic data, outcomes, and cross-sectional measures of the intervention were summarized using mean, minimum, and maximum values, along with standard deviation. Categorical data were summarized using frequency.
Initially, the data normality was verified using the Shapiro–Wilk test (Field, 2017), which suggested a normal distribution. Therefore, the paired Student’s T-test (Field, 2017) was employed with a p-value of <0.05 in order to evaluate the benefits of the intervention. Effect sizes for each assessed outcome were computed using Cohen’s d. For interpreting effect sizes, Cohen’s (1998) guidelines were considered: scores between 0 and 0.2 indicate a null effect size; scores between 0.2 and 0.5 indicate a small effect size; scores between 0.5 and 0.8 indicate a medium effect size; finally, scores above 0.8 indicate a large effect size.
Qualitative data were analyzed using Thematic Analysis (Braun and Clarke, 2006). Initially, the audios from interviews were transcribed into text format, creating a document in docx format. Two researchers (BLS and DCS) independently reviewed this content and identified themes, adhering strictly to guidelines proposed for Braun and Clarke (2006). We adopted a data-driven approach, abstaining from a priori categories and theories in the interpretation of the qualitative data (Braun and Clarke, 2022). The steps undertaken included: (1) data familiarization, comprising repetitive and in-depth reading of qualitative data; (2) generation of initial codes, involving the identification of meaningful cores capable of generating themes; (3) theme identification, wherein these codes evolve into broader themes; (4) themes review, verifying the accurate representation of the qualitative database by the identified themes; (5) themes defining, which also involves assessing the presence of sub-themes. After these steps, the two authors met to deliberate and define the final thematic.
2.7 Ethical procedures
This research rigorously adhered to all ethical procedures as outlined in the Declaration of Helsinki for research involving human beings. Prior to commencing the study, approval was obtained from the Research Ethics Committee of the Federal University of Health Sciences of Porto Alegre (CAAE: 43804621.8.0000.5345). All participants provided their consent both in pre-test and post-test by reading the consent form and choosing the option “yes, I have read the terms and agree to participate in the research.”
3 Results
3.1 Adherence to the intervention
Since 99 participants were expected to utilize each of eight modules of the app, a total of 792 app usage modules were anticipated. Three hundred of the total 792 intervention modules were achieved, representing a 37.87% overall adherence. Approximately 68.69% of participants finished at least one module, with 26.26% completing all eight modules. The number of participants decreased by 50% between the first and fourth modules but remained relatively stable from the fifth to the eighth (11.35% decrease). Module four took the longest time (M = 1116.06 s; SD = 992.49 s) to be finished, while module eight was completed the fastest (M = 370.77 s; SD = 183.43 s). Table 3 provides an overview of the intervention’s adherence metrics.
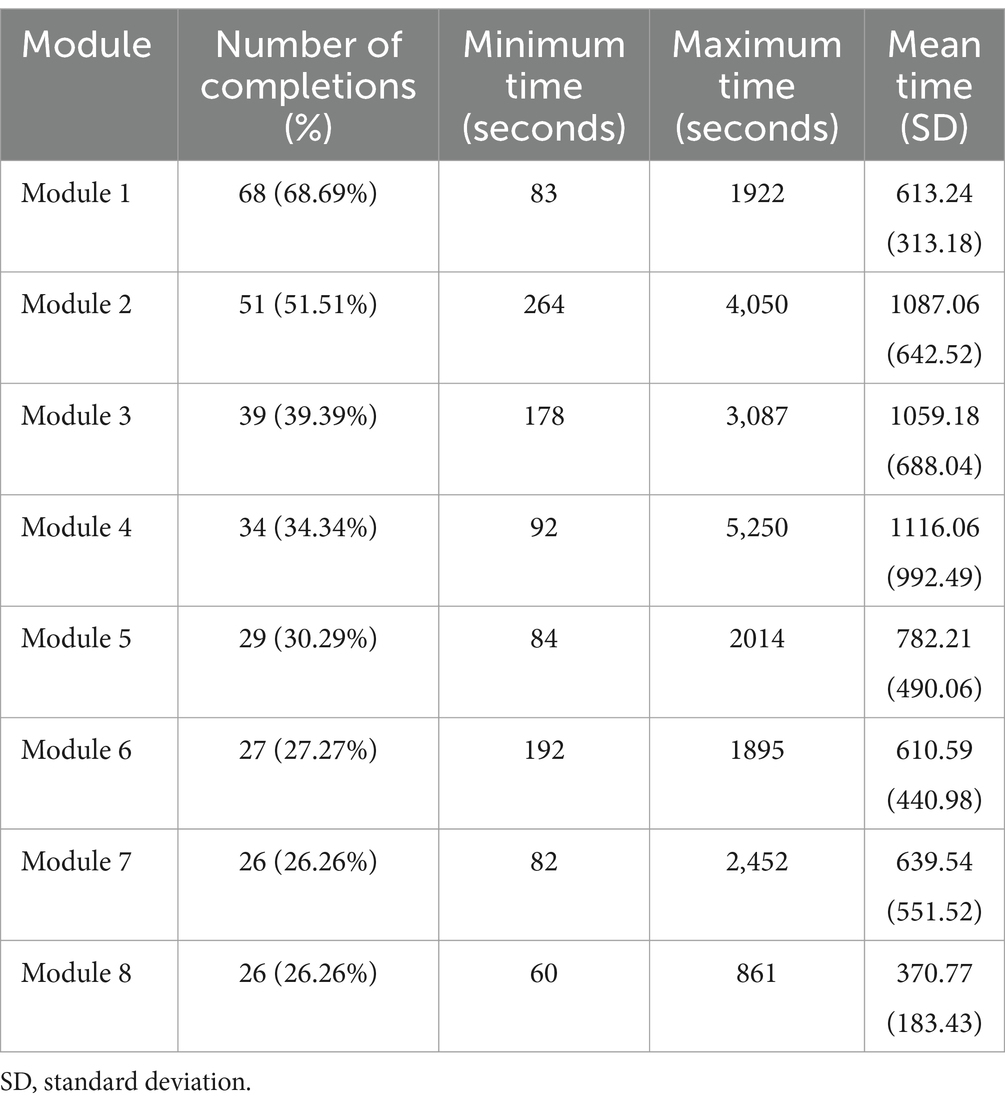
Table 3. Adherence to intervention.
3.2 Benefits of the intervention
Only participants who responded to both the pre-test and post-test and completed all eight modules of the intervention were included in the analysis of the app’s benefits. Thus, the benefits of the intervention were analyzed using data from 23 out of the initial 99 participants. Improvements in mental health scores were observed across all 21 assessed outcomes, as the reduction of psychopathological symptoms (e.g., depression) or the enhancement of positive mental health (e.g., positive affects). In 15 of these outcomes, the results were statistically significant, demonstrating a small, medium or large effect size. Anxiety (d = 0.52), stress (d = 0.62), negative affects (d = 0.66), and pessimism (d = 0.77) exhibited a decrease in scores with a medium effect size. Conversely, self-compassion demonstrated improvement with a large effect size (d = 1.15). Additionally, there was a large effect size increase in self-kindness (d = 0.95), common humanity (d = 1.05), and mindfulness scores (d = 0.94), accompanied by a large effect size decrease in self-judgment (d = 0.85), isolation (d = 0.97), and a medium effect size in over-identification (d = 0.76) scores. Positive affects (d = 0.45), optimism (d = 0.44) and life satisfaction (d = 0.48) also exhibited score improvements with a small effect size. Finally, emotional well-being exhibited score improvement with a medium effect size (d = 0.54). Table 4 provides a comprehensive presentation of intervention’s benefits.
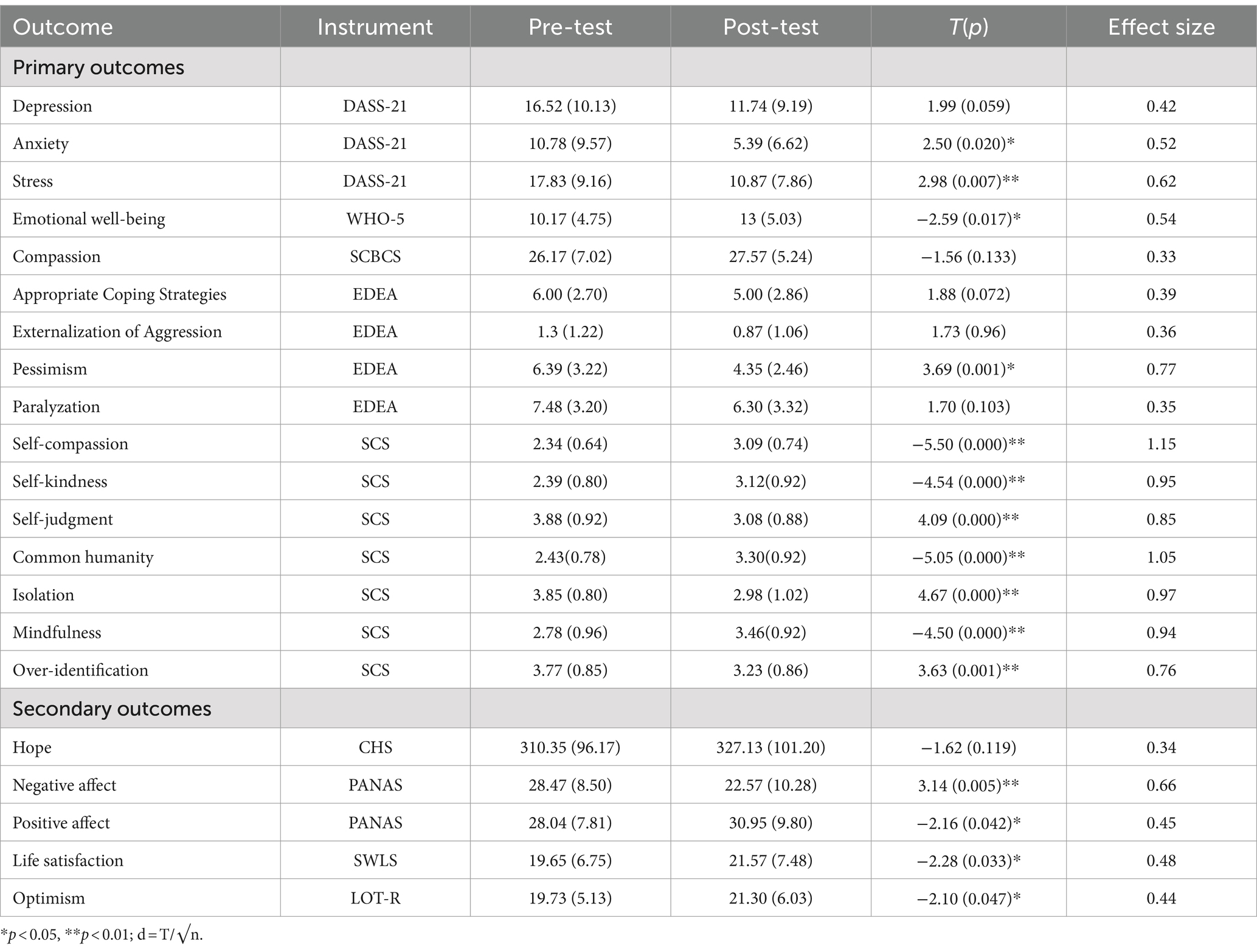
Table 4. Benefits of app on mental health indicators (n = 23).
3.3 Satisfaction and acceptability of the intervention
All six indicators assessing the satisfaction and acceptability of the intervention had an average score above seven, with five indicators averaging above eight. The statement “I think the app can help with the emotional well-being of college students “received the highest rating (M = 8.87; SD = 1.42), while the statement “I will continue using the app if I do not feel good” received the lowest rating (M = 7.30; SD = 2.58). Table 5 presents a comprehensive overview of the global assessment of satisfaction.
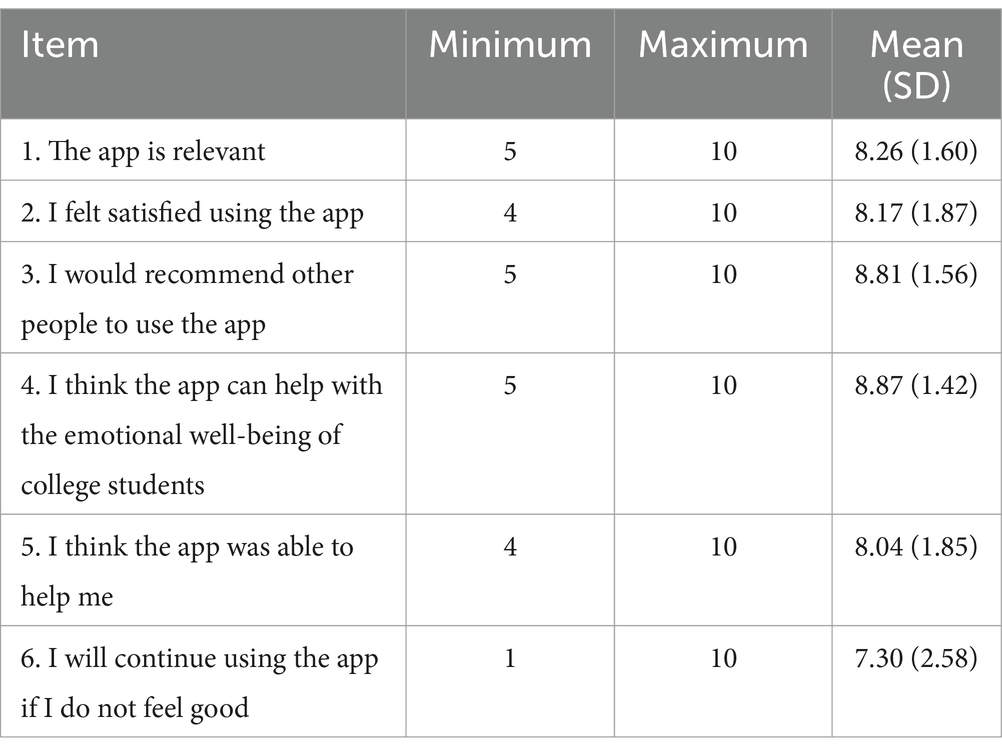
Table 5. Measure of acceptability and satisfaction with the intervention (n = 23).
3.4 Qualitative assessment
Nineteen participants agreed to participate in the qualitative research step. The qualitative analysis revealed two main themes. They are, respectively, named “perceptions about the app and the intervention,” and “perceptions of personal benefits.” The theme perceptions about the app and the intervention captures feedback patterns concerning the format and presentation of the app. It comprises four subthemes: ease of use, reflecting on the app’s user-friendliness; intervention acceptance, indicating participants’ receptiveness to the intervention; length of the texts, suggesting participants’ perceptions of extensive textual content; and organization of the routine, pointing to potential barriers in executing the intervention, such as the demands of classes, internships or work.
The theme perceptions of personal benefits address the perceived advantages by participants, categorized into three subthemes: self-knowledge, demonstrating that the app may have contributed to participants’ enhanced self-awareness; emotional well-being, focusing on the perceived mental health benefits of the app; and self-compassion, indicating participants’ acquired self-compassion skills. Table 6 presents these themes, subthemes, and some excerpts exemplifying the analyses.

Table 6. Thematic analysis.
4 Discussion
Before conducting randomized clinical trials, which may demand considerable time, financial funds, and high specialized staff, pilot studies are recommended to assess key variables that may affect the success of these interventions (Lancaster, 2015; Lowe, 2019). Consequently, methodological guidelines propose the prior evaluation of indicators, such as the initial benefits of the intervention, its acceptability, interest, and participant’s satisfaction (Lancaster, 2015; Teresi et al., 2022). The evidence assessed in pilot studies facilitates adjustments in the presentation, format, and active ingredients of interventions (Schaab and Remor, 2023). This adjustment aims to enhance personalization and attractiveness, ultimately increasing the likelihood of achieving effectiveness in the targeted outcomes (Lowe, 2019; Schaab and Remor, 2023). In line with these considerations, this pilot study assessed the adherence to the intervention, its preliminary benefits, user satisfaction, acceptability, and general qualitative impressions regarding the app. Each of these topics is expounded upon in the subsequent sections.
4.1 Adherence to intervention
The final intervention adherence rate of 26.26% aligns with scores identified in digital intervention studies in natural contexts addressing psychological distress. Evidence suggests that only between 0.5 and 28.6% of users complete interventions or persist in using them after 6 weeks (Fleming et al., 2018). Regarding mindfulness apps, the user retention rate is just 4.7% after 30 days of use (Baumel et al., 2019). The observed trend of a gradual decrease in app usage or module completion over time in the present study is also consistent with findings in similar research (i.e., Fleming et al., 2018; Baumel et al., 2019; Linardon and Fuller-Tyszkiewicz, 2020). Several factors are associated with the decline in app usage in natural contexts, including the absence of immediate benefits, competition with other smartphone apps, and a lack of user motivation and engagement (Giebel et al., 2023).
Regarding barriers to completing the modules, we formulated two hypotheses: the module size and the mental health status of individuals in the sample. Initially, we believe that the length of texts and information in app may have impacted adherence to the intervention. Some users qualitatively suggested that engaging in the intervention involved reading or listening to an extensive amount of information, and this could be a barrier. Evidence on adherence to digital interventions indeed suggests that information overload can pose a potential barrier to intervention adherence (Giebel et al., 2023). Therefore, it is important that interventions are also attractive, especially to people experiencing depressive symptoms.
It is plausible that the mental health status of the sample is associated with adherence to the app modules. Individuals with higher levels of depressive symptoms tend to exhibit lower engagement in app-based interventions (Zeng et al., 2020; Molloy and Anderson, 2021), as well as in face-to-face psychological services and psychological resources programs (Zeng et al., 2020). This behavior may be attributed to the depressive symptoms themselves, which encompass disinterest, lack of energy, motivation, tiredness, and apathy (Molloy and Anderson, 2021). Given that the majority of the sample in this research manifested severe symptoms of depression and anxiety, it is conceivable that these symptoms influenced adherence.
In the future, gamification could be a strategy to increase user adherence and retention rates, as it has been associated with better engagement rates in app-based interventions (Jakob et al., 2022). Furthermore, another promising strategy is the creation of a forum within the app. Users could anonymously share their experiences with self-compassion practices, making the experience of using the app more collective and even more attractive, since several app-based interventions have adopted social media elements as a way to become more attractive (Wei et al., 2020).
For the implementation of the clinical trial, we will consider a potential sample attrition of approximately 75% by the conclusion of the intervention. To enhance engagement and adherence, an augmented strategy will involve the implementation of more reminders and weekly notifications for participants. These reminders aim to encourage continued utilization of the app.
4.2 Intervention benefits
The intervention results indicate that the app may be effective in promoting the mental health of Brazilian college students, demonstrating a reduction in psychopathological symptoms and an improvement in positive mental health indicators. These findings align with evidence from interventions conducted in face-to-face settings, which have also shown medium effect sizes in decreasing self-judgment (Wakelin et al., 2022), anxiety and depression (Kirby et al., 2017), and enhancing self-compassion, mindfulness and subjective well-being (Kirby et al., 2017).
The identified benefits are consistent with findings from two known digital self-compassion interventions targeting college students (Andersson et al., 2021; Serlachius et al., 2021). The Whitu app designed for New Zealand university students demonstrated effectiveness in decreasing anxiety and stress, while enhancing subjective well-being over a six-week period, with observed medium effect sizes (Serlachius et al., 2021). Similarly, a digital intervention grounded in self-compassion principles, delivered to Swedish university students, proved effective, exhibiting a large effect size in stress reduction and self-compassion improvement within the experimental group as compared to the control group (Andersson et al., 2021).
Regarding self-compassion interventions among college students delivered in a face-to-face format and online format, the present research presented a higher effect size (d = 1.15) than the synthesis of other studies (g = 0.49) (Póka et al., 2024). Also, the effect size of self-compassion in the present study (d = 1.15) is similar to that of the synthesis of face-to-face interventions (g = 0.80) (Póka et al., 2024). However, it is important to highlight that the results of behavioral interventions may vary depending on the characteristics of the audience, psychological instruments, and, mainly, the intervention itself, including psychological techniques, experience and previous training of facilitators, and intervention length.
Studies employing structural equation modeling have underscored the association between self-compassion and mental health. An investigation assessing the advantages of a guided Positive Psychology intervention delivered via email for adult mental health, using a mediation model, revealed that self-compassion emerged as the most proficient construct in elucidating the decrease in anxiety and depression and the enhancement of emotional well-being (Schotanus-Dijkstra et al., 2019). Similarly, an eight-week mindfulness-based intervention demonstrated that self-compassion mediated the direct effects of the intervention on stress (Sevel et al., 2020). These mediation effects provide insights into how the app may have positively influenced Brazilian college students.
Self-compassion and self-judgment yielded the most substantial effect sizes in the current study. The improvement in self-compassion is likely associated with a decrease in psychological distress, along with improvements in emotion regulation dimensions, such as pessimism. Given that emotion regulation serves as a mediator in the connection between self-compassion and mental health (Fong and Loi, 2016), it is plausible that college students utilized learned self-compassion strategies to manage the intensity and frequency of negative emotions linked to university life. A central emphasis of the intervention was to introduce and cultivate a set of self-compassionate skills specifically helpful to academic stressors, with a primary focus on fostering self-kindness, cultivating a sense of common humanity, and practicing mindfulness.
It is important to note that the development of the app strictly adhered to the self-compassion literature, which contributes to the positive outcomes of the study. The level of compassion content in psychological interventions is linked to its enhancement (Jazaieri et al., 2013). Thus, before creating the prototype, psychologists specializing in Positive Psychology reviewed the intervention to ensure that the content and techniques used were scientifically appropriate and could be effective among college students. A recent qualitative review evidenced on Android and iOS platforms 24 apps to promote compassion, but only nine of which are properly based on scientific evidence (Krijger et al., 2023), which reinforce the importance of solid theoretical foundations.
The observed benefits in the current study are promising and indicate the feasibility of conducting a randomized clinical trial in the near future. The incorporation of a control group, randomization, and follow-up procedures will enable a comprehensive assessment of the app’s effectiveness, ensuring both robust evaluation and the examination of result consistency over time.
Finally, it is important to note that the results cannot yet be generalized, primarily due to the study’s sample size and the fact that it was only conducted in Brazil. However, the positive results obtained, especially in the self-compassion components, encourage further studies to evaluate the benefits of practicing self-compassion among university students, particularly in Latin America. Most studies of app-based self-compassion interventions are currently concentrated in Europe.
4.3 Intervention’s satisfaction
All satisfaction indicators for the intervention were positive, with scores consistently exceeding the established cutoff of 7 in previous pilot studies (Schaab and Remor, 2023). The satisfaction observed is likely linked to perceived benefits, as participants recognized the potential advantages for both them and other college students. This satisfaction is highlighted in responses to the item, “I think the app can help with the emotional well-being of college students,” which garnered the highest average score.
Conversely, the item “I will continue using the app if I do not feel good” received the lowest rating. This lower score can be attributed to the fact that some users, upon completing the intervention, may not be inclined to revisit the same activities. Consequently, implementing app modifications becomes crucial to sustain ongoing user interest in the tool.
Additionally, it is noteworthy that there is a substantial score variation between each item, ranging from 1 to 10 in certain instances and, more commonly, between 5 and 10. These findings indicate that a minority of participants expressed dissatisfaction with the intervention. Such discrepancies were expected, considering individual preferences regarding the content and format of the app.
In summary, the satisfaction measure indicated favorable outcomes for the app. However, it is essential to acknowledge that the satisfaction assessment was conducted solely among the 23 participants who completed the entire intervention. This potential bias could have influenced the positive evaluation of the intervention. Next, it is crucial to gather data from participants who did not complete all the modules to discern whether the dropout is associated with the app itself or arises from personal issues.
4.4 Acceptability and qualitative impressions
The qualitative data suggests the acceptance of the app by participants, as confirmed through the identified subthemes “ease of use” and “mental health.” It was expected that participants would encounter no difficulties on app use, which aligns with a previous study that indicated the excellent usability of Eu + Compassivo. Furthermore, earlier data on participants’ smartphone use revealed that almost 97% of them spent more than an hour a day on their cell phones and 84% used more than 3 apps, highlighting their digital literacy. The widespread use of mobile technologies among university students positions them as an opportune audience for the administration of digital interventions (Kern et al., 2018).
Conversely, it is crucial to acknowledge that, for at least some participants, the volume of text in the intervention was a potential barrier. Usability research involving other mental health apps has indicated a preference for more direct information presented in a playful manner (Jessen et al., 2018). Future versions of the app will aim to modify the presentation format and the extent of information, especially because playful elements such as gamification have been recommended in the development of online interventions (Jakob et al., 2022). Furthermore, participants identified a challenge in integrating the use of the app into their study, internship, and work routine, underscoring the importance of a more concise and attractive intervention.
Also, it is crucial to highlight that studies’ participants perceived benefits from using the app on their mental health aligning with the quantitative data. The specific enhancement in emotional well-being may stem from acquiring self-compassion strategies for emotion regulation and self-knowledge, as suggested by these subthemes. As reflected in the results, many participants appear to have broadened their sense of shared humanity, a component of self-compassion, acknowledging that other college students also experience suffering, which means they are not alone. Additionally, some university college students reported a reduced tendency for self-criticism, aligning with the self-judgment dimension of self-compassion.
The evidence regarding personal benefits aligns with findings from other digital self-compassion interventions. A study qualitatively assessed the effects of the Self-Compassion app on British university students (Beaumont et al., 2022). After 6 weeks of use, students reported an increased ability to feel and practice self-compassion in their daily lives.
In summary, the present evidence indicates that app is accepted, easy to use, and can provide benefits to the emotional well-being of college students. Changes to the format and presentation of the app may be necessary in the future in order to make its content more succinct and objective.
4.5 Limitations
The first limitation is the significant dropout in the intervention. Although dropout rates are in line with app-based intervention studies in natural contexts, the small number of participants who completed the intervention and responded to the pre-test and post-test (n = 23) suggests caution in interpreting the benefits of the intervention.
The second limitation of the study pertains to the substantial number of participants concurrently engaging in psychotherapy or utilizing psychotropic drugs while utilizing the app, particularly antidepressants and benzodiazepines. While this introduces a confounding variable, it is crucial to acknowledge that both the average duration of psychotherapy and the usage of psychopharmaceuticals exceed 3 years, potentially mitigating the impact of these variables.
Finally, the last potential limitation is the absence of a control group. Although control groups are not deemed obligatory in pilot studies, the inclusion of a control group could have aided in mitigating experimental biases.
4.6 Strengths
To the best of our knowledge, our app stands as one of the initial app-based intervention based on self-compassion principles designed to enhance the mental well-being of college students worldwide. Additionally, in the context of Brazil, digital interventions based on self-compassion are not currently prevalent, which highlights the innovative nature of our study. Conducting this research in a natural setting allows us to comprehend the anticipated user engagement and real-world benefits of the app.
5 Conclusion
The results of this pilot study suggest that the app may be beneficial for Brazilian college students and is accepted and well-received by at least those who have completed all intervention. However, despite adherence rates falling within the expected range for studies conducted in natural contexts, there is a need for activities to enhance intervention adherence, such as weekly usage reminders and increased dynamism in content presentation and exercises. The next step involves conducting a randomized clinical trial, comparing participants using this Brazilian self-compassion app with those on a waiting list. We expect still in 2024 to distribute the app free of charge among Brazilian college students facing mental health impairments.
Data availability statement
The dataset generated during the current study are not publicly available due nature of the information provided by the research participants. Requests to access the dataset should be directed to the corresponding author BS, YnJ1bm8uc2NoYWFiQHVmY3NwYS5lZHUuYnI=.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of the Federal University of Health Sciences of Porto Alegre (CAAE: 43804621.8.0000.5345). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
BS: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. LC: Investigation, Resources, Visualization, Writing – review & editing. DS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Visualization, Writing – review & editing. PS: Data curation, Investigation, Methodology, Software, Visualization, Writing – review & editing. KB: Investigation, Methodology, Validation, Visualization, Writing – review & editing. GD: Conceptualization, Investigation, Methodology, Validation, Writing – review & editing. VK: Conceptualization, Investigation, Validation, Visualization, Writing – review & editing. PC: Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SC: Validation, Visualization, Writing – review & editing, Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision. HB: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing. CR: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001. Also, this study was supported in part by a research grant from the National Counsel of Technological and Scientific Development (CNPq) conceded to CR and HB and a research grant from CAPES conceded to BS.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
Andersson, C., Bergsten, K. L., Lilliengren, P., Norbäck, K., Rask, K., Einhorn, S., et al. (2021). The effectiveness of smartphone compassion training on stress among Swedish university students: a pilot randomized trial. J. Clin. Psychol. 77, 927–945. doi: 10.1002/jclp.23092
Auerbach, R. P., Mortier, P., Bruffaerts, R., Alonso, J., Benjet, C., Cuijpers, P., et al. (2018). WHO world mental health surveys international college student project: prevalence and distribution of mental disorders. J. Abnorm. Psychol. 127, 623–638. doi: 10.1037/abn0000362
Bastianello, M. R., Pacico, J. C., and Hutz, C. S. (2014). Optimism, self-esteem and personality: adaptation and validation of the Brazilian version OS the revised life orientation test (LOT-R). Psico USF 19, 523–531. doi: 10.1590/1413-827120140190030
Baumel, A., Muench, F., Edan, S., and Kane, J. M. (2019). Objective user engagement with mental health apps: systematic search and panel-based usage analysis. J. Med. Intern. Res. 21:e14567. doi: 10.2196/14567
Beaumont, E. A., Irons, C., and McAndrew, S. L. (2022). A qualitative study exploring the impact the self-compassion app has on levels of compassion, self-criticism, and wellbeing. OBM Integr. Complement. Med. 7, 1–24. doi: 10.21926/obm.icm.2203045
Braun, V., and Clarke, V. (2006). Using thematic analysis in psychology. Qual. Res. Psychol. 3, 77–101. doi: 10.1191/1478088706qp063oa
Broglia, E., Millings, A., and Barkham, M. (2021). Student mental health profiles and barriers to help seeking: when and why students seek help for a mental health concern. Couns. Psychother. Res. 21, 816–826. doi: 10.1002/capr.12462
Buizza, C., Bazzoli, L., and Ghilardi, A. (2022). Changes in college students mental health and lifestyle during the COVID-19 pandemic: a systematic review of longitudinal studies. Adolesc. Res. Rev. 7, 537–550. doi: 10.1007/s40894-022-00192-7
Campbell, F., Blank, L., Cantrell, A., Baxter, S., Blackmore, C., Dixon, J., et al. (2022). Factors that influence mental health of university and college students in the UK: a systematic review. BMC Public Health 22:1778. doi: 10.1186/s12889-022-13943-x
Cohen, J. (1998). Statistical power analysis for the behavioural sciences. Hillsdale, NJ: Lawrence Erlbaum Associates.
Cremasco, G., Pallini, A. C., Bonfá-Araujo, B., Noronha, A. P. P., and Baptista, M. N. (2020). Emotional dysregulation scale – adults (EDEA): validity evidence. Psicol. Teor. Prat. 22, 161–178. doi: 10.5935/1980-6906/psicologia
Creswell, J. W., and Clark, V. L. (2011). Designing and conducting mixed methods research. Los Angeles, CA: Sage.
Dachew, B. A., Bisetegn, T. A., and Gebremariam, R. B. (2015). Prevalence of mental distress and associated factors among undergraduate students of University of Gondar, Northwest Ethiopia: a cross-sectional institutional based study. PLoS One 10:e0119464. doi: 10.1371/journal.pone.0119464
Dave, S., Jaffe, M., and O'Shea, D. (2024). Navigating college campuses: the impact of stress on mental health and substance use in the post COVID-19 era. Curr. Probl. Pediatr. Adolesc. Healt. Care 54:101585. doi: 10.1016/j.cppeds.2024.101585
Diener, E., Emmons, R. A., Larsen, R. J., and Griffin, S. (1985). The satisfaction with life scale. J. Pers. Assess. 49, 71–75. doi: 10.1207/s15327752jpa4901_13
Egan, S. J., Rees, C. S., Delalande, J., Greene, D., Fitzallen, G., Brown, S., et al. (2022). A review of self-compassion as an active ingredient in the prevention and treatment of anxiety and depression in young people. Admin. Pol. Ment. Health 49, 385–403. doi: 10.1007/s10488-021-01170-2
Estrada-Araoz, E. G., Bautista Quispe, J. A., Córdova-Rojas, L. M., Ticona Chayña, E., Mamani Coaquira, H., and Huaman Tomanguilla, J. (2023). Mental health of university students when returning to face-to-face classes: a cross-sectional study. Behav. Sci. 13:438. doi: 10.3390/bs13060438
Farfán-Latorre, M., Estrada-Araoz, E. G., Lavilla-Condori, W. G., Ulloa-Gallardo, N. J., Calcina-Álvarez, D. A., Meza-Orue, L. A., et al. (2023). Mental health in the post-pandemic period: depression, anxiety, and stress in Peruvian university students upon return to face-to-face classes. Sustain. For. 15:11924. doi: 10.3390/su151511924
Ferrari, M., Hunt, C., Harrysunker, A., Abbott, M. J., Beath, A. P., and Einstein, D. A. (2019). Self-compassion interventions and psychosocial outcomes: a meta-analysis of RCTs. Mindfulness 10, 1455–1473. doi: 10.1007/s12671-019-01134-6
Field, A. (2017). Discovering statistics using IBM SPSS statistics. North American Edn. London: SAGE Publications Ltd.
Fleming, T., Bavin, L., Lucassen, M., Stasiak, K., Hopkins, S., and Merry, S. (2018). Beyond the trial: systematic review of real-world uptake and engagement with digital self-help interventions for depression, low mood, or anxiety. J. Med. Internet Res. 20:e199. doi: 10.2196/jmir.9275
Fong, M., and Loi, N. M. (2016). The mediating role of self-compassion in student psychological health. Aust. Psychol. 51, 431–441. doi: 10.1111/ap.12185
Giebel, G. D., Speckemeier, C., Abels, C., Plescher, F., Börchers, K., Wasem, J., et al. (2023). Problems and barriers related to the use of digital health applications: scoping review. J. Med. Internet Res. 25:e43808. doi: 10.2196/43808
Gilbert, P. (2010). Compassion focused therapy: The CBT distinctive features series. London: Routledge.
Graner, K. M., and Cerqueira, A. T. (2019). Integrative review: psychological distress among university students and correlated factors. Ciênc. Saúde Colet. 24, 1327–1346. doi: 10.1590/1413-81232018244.09692017
Hwang, J. Y., Plante, T., and Lackey, K. (2008). The development of the Santa Clara brief compassion scale: an abbreviation of Sprecher and Fehr’s compassionate love scale. Pastoral Psychol. 56, 421–428. doi: 10.1007/s11089-008-0117-2
Inwood, E., and Ferrari, M. (2018). Mechanisms of change in the relationship between self-compassion, emotion regulation, and mental health: a systematic review. Appl. Psychol. Health Well Being 10, 215–235. doi: 10.1111/aphw.12127
Jakob, R., Harperink, S., Rudolf, A. M., Fleisch, E., Haug, S., Mair, J. L., et al. (2022). Factors influencing adherence to mHealth apps for prevention or management of non-communicable diseases: systematic review. J. Med. Internet Res. 24:e35371. doi: 10.2196/35371
Jazaieri, H., Jinpa, G. T., McGonigal, K., Rosenberg, E. L., Finkelstein, J., Simon-Thomas, E., et al. (2013). Enhancing compassion: a randomized controlled trial of a compassion cultivation training program. J. Happiness Stud. 14, 1113–1126. doi: 10.1007/s10902-012-9373-z
Jessen, S., Mirkovic, J., and Ruland, C. M. (2018). Creating gameful design in mhealth: a participatory co-design approach. JMIR Mhealth Uhealth 6:e11579. doi: 10.2196/11579
Julious, S. A. (2005). Sample size of 12 per group rule of thumb for a pilot study. Pharm. Stat. 4, 287–291. doi: 10.1002/pst.185
Kern, A., Hong, V., Song, J., Lipson, S. K., and Eisenberg, D. (2018). Mental health apps in a college setting: openness, usage, and attitudes. Mhealth 4:20. doi: 10.21037/mhealth.2018.06.01
Kirby, J. N., Tellegen, C. L., and Steindl, S. R. (2017). A meta-analysis of compassion-based interventions: current state of knowledge and future directions. Behav. Ther. 48, 778–792. doi: 10.1016/j.beth.2017.06.003
Krijger, E., Bohlmeijer, E. T., Geuze, E., and Kelders, S. M. (2023). Compassion apps for better mental health: qualitative review. BJPsych Open 9:e141. doi: 10.1192/bjo.2023.537
Lancaster, G. A. (2015). Pilot and feasibility studies come of age! Pilot Feasibility Stud. 1, 1–4. doi: 10.1186/2055-5784-1-1
Leahy, R. L., Tirch, D., and Napolitano, L. A. (2011). Emotion regulation in psychotherapy: a practitioner's guide. Washington, DC: American Psychological Association.
Lemyre, A., Palmer-Cooper, E., and Messina, J. P. (2023). Wellbeing among university students during the COVID-19 pandemic: a systematic review of longitudinal studies. Public Health 222, 125–133. doi: 10.1016/j.puhe.2023.07.001
Linardon, J., and Fuller-Tyszkiewicz, M. (2020). Attrition and adherence in smartphone-delivered interventions for mental health problems: a systematic and meta-analytic review. J. Consult. Clin. Psychol. 88, 1–13. doi: 10.1037/ccp0000459
Liverpool, S., Moinuddin, M., Aithal, S., Owen, M., Bracegirdle, K., Caravotta, M., et al. (2023). Mental health and wellbeing of further and higher education students returning to face-to-face learning after Covid-19 restrictions. PLoS One 18:e0280689. doi: 10.1371/journal.pone.0280689
López, A., Sanderman, R., Ranchor, A. V., and Schroevers, M. J. (2018). Compassion for others and self-compassion: levels, correlates, and relationship with psychological well-being. Mindfulness 9, 325–331. doi: 10.1007/s12671-017-0777-z
Lovibond, P. F., and Lovibond, S. H. (1995). The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behav. Res. Ther. 33, 335–343. doi: 10.1016/0005-7967(94)00075-U
Lowe, N. K. (2019). What is a pilot study? J. Obstet. Gynecol. Neonatal. Nurs. 48, 117–118. doi: 10.1016/j.jogn.2019.01.005
Marchetti, E., Bertolino, C. D. O., Schiavon, C. C., Gurgel, L. G., Kato, S. K., Menezes, C. B., et al. (2018). Santa Clara brief compassion scale: psychometric properties for the Brazilian context. Aval. Psicol. 17, 371–377. doi: 10.15689/ap.2018.1703.15208.10
Mboya, I. B., John, B., Kibopile, E. S., Mhando, L., George, J., and Ngocho, J. S. (2020). Factors associated with mental distress among undergraduate students in northern Tanzania. BMC Psychiatry 20, 28–27. doi: 10.1186/s12888-020-2448-1
McIntyre, R., Smith, P., and Rimes, K. A. (2018). The role of self-criticism in common mental health difficulties in students: a systematic review of prospective studies. Ment. Health Prev. 10, 13–27. doi: 10.1016/j.mhp.2018.02.003
Mofatteh, M. (2021). Risk factors associated with stress, anxiety, and depression among university undergraduate students. AIMS Public Health 8, 36–65. doi: 10.3934/publichealth.2021004
Molloy, A., and Anderson, P. L. (2021). Engagement with mobile health interventions for depression: a systematic review. Internet Interv. 26:100454. doi: 10.1016/j.invent.2021.100454
Neff, K. D. (2003). The development and validation of a scale to measure self-compassion. Self Identity 2, 223–250. doi: 10.1080/15298860309027
Neff, K. D. (2011). Self-compassion: the proven power of being kind to yourself. New York: William Morrow.
Neff, K. D. (2016). The self-compassion scale is a valid and theoretically coherent measure of self-compassion. Mindfulness 7, 264–274. doi: 10.1007/s12671-015-0479-3
Neff, K. D. (2023). Self-compassion: theory, method, research, and intervention. Annu. Rev. Psychol. 74, 193–218. doi: 10.1146/annurev-psych-032420-031047
Neff, K. D., and Germer, C. K. (2018). The mindful self-compassion workbook: a proven way to accept yourself, find inner strength, and thrive. New York: Guilford Press.
Pacico, J. C., and Bastianello, M. R. (2014). “Instruments for assessing hope: dispositional hope scale and cognitive hope scale” in Assessment in positive psychology. ed. C. S. Hutz (Porto Alegre: ArtMed), 101–110.
Pedrelli, P., Nyer, M., Yeung, A., Zulauf, C., and Wilens, T. (2019). College students: mental health problems and treatment considerations. Acad. Psychiatry 39, 503–511. doi: 10.1007/s40596-014-0205-9
Póka, T., Fodor, L. A., Barta, A., and Mérő, L. (2024). A systematic review and meta-analysis on the effectiveness of self-compassion interventions for changing university students’ positive and negative affect. Curr. Psychol. 43, 6475–6493. doi: 10.1007/s12144-023-04834-4
Rech, M., Diaz, G. B., Schaab, B. L., Rech, C. G., Calvetti, P. Ü., and Reppold, C. T. (2023). Association of Emotional Self-Regulation with psychological distress and positive functioning dimensions in Brazilian university students during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 20:6428. doi: 10.3390/ijerph20146428
Schaab, B. L., and Remor, E. (2023). Development, feasibility testing and perceived benefits of a new app to help with adherence to antiretroviral therapy in people living with HIV in Brazil. Pilot Feasibility Stud. 9:130. doi: 10.1186/s40814-023-01370-7
Schaab, B. L., Santos, L. B., Calvetti, P. Ü., Cazella, S. C., Barros, H. T., and Reppold, C. T. (2024). Development and evaluation of a mobile app-based intervention based on self-compassion for the prevention and promotion of mental health of university students.
Scheier, M. F., Carver, C. S., and Bridges, M. W. (1994). Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): a reevaluation of the life orientation test. J. Pers. Soc. Psychol. 67, 1063–1078. doi: 10.1037/0022-3514.67.6.1063
Schotanus-Dijkstra, M., Pieterse, M. E., Drossaert, C. H. C., Walburg, J. A., and Bohlmeijer, E. T. (2019). Possible mechanisms in a multicomponent email guided positive psychology intervention to improve mental well-being, anxiety and depression: a multiple mediation model. J. Posit. Psychol. 14, 141–155. doi: 10.1080/17439760.2017.1388430
Serlachius, A., Boggiss, A., Lim, D., Schache, K., Wallace-Boyd, K., Brenton-Peters, J., et al. (2021). Pilot study of a well-being app to support New Zealand young people during the COVID-19 pandemic. Internet Interv. 26:100464. doi: 10.1016/j.invent.2021.100464
Sevel, L. S., Finn, M. T., Smith, R. M., Ryden, A. M., and McKernan, L. C. (2020). Self-compassion in mindfulness-based stress reduction: an examination of prediction and mediation of intervention effects. Stress. Health 36, 88–96. doi: 10.1002/smi.2917
Shaughnessy, J. J., Zechmeister, E. B., and Zechmeister, J. S. (2015). Research methods in psychology. 10th Edn. Boston: McGraw-Hill.
Souza, L. K., and Hutz, C. S. (2016). Adaptation of the self-compassion scale for use in Brazil: evidences of construct validity. Trends Psychol. 24, 159–172. doi: 10.9788/TP2016.1-11
Staats, S. (1989). Hope: a comparison of two self-report measures for adults. J. Pers. Assess. 53, 366–375. doi: 10.1207/s15327752jpa5302_13
Stoeber, J., Lalova, A. V., and Lumley, E. J. (2020). Perfectionism, (self-)compassion, and subjective well-being: a mediation model. Pers. Individ. Dif. 154:109708. doi: 10.1016/j.paid.2019.109708
Teresi, J. A., Yu, X., Stewart, A. L., and Hays, R. D. (2022). Guidelines for designing and evaluating feasibility pilot studies. Med. Care 60, 95–103. doi: 10.1097/MLR.0000000000001664
Topp, C. W., Østergaard, S. D., Søndergaard, S., and Bech, P. (2015). The WHO-5 well-being index: a systematic review of the literature. Psychother. Psychosom. 84, 167–176. doi: 10.1159/000376585
Viechtbauer, W., Smits, L., Kotz, D., Budé, L., Spigt, M., Serroyen, J., et al. (2015). A simple formula for the calculation of sample size in pilot studies. J. Clin. Epidemiol. 68, 1375–1379. doi: 10.1016/j.jclinepi.2015.04.014
Vignola, R. C. B., and Tucci, A. M. (2014). Adaptation and validation of the depression, anxiety and stress scale (DASS) to Brazilian Portuguese. J. Affect. Disord. 155, 104–109. doi: 10.1016/j.jad.2013.10.031
Wakelin, K. E., Perman, G., and Simonds, L. M. (2022). Effectiveness of self-compassion-related interventions for reducing self-criticism: a systematic review and meta-analysis. Clin. Psychol. Psychother. 29, 1–25. doi: 10.1002/cpp.2586
Watson, D., Clark, L. A., and Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: the PANAS scales. J. Pers. Soc. Psychol. 54, 1063–1070. doi: 10.1037/0022-3514.54.6.1063
Wei, Y., Zheng, P., Deng, H., Wang, X., Li, X., and Fu, H. (2020). Design features for improving mobile health intervention user engagement: systematic review and thematic analysis. J. Med. Internet Res. 22:e21687. doi: 10.2196/21687
World Health Organization . (2019). Suicide. Available at: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed March 01, 2024).
Worsley, J. D., Pennington, A., and Corcoran, R. (2022). Supporting mental health and wellbeing of university and college students: a systematic review of review-level evidence of interventions. PLoS One 17:e0266725. doi: 10.1371/journal.pone.0266725
Yang, M., Wei, W., Ren, L., Pu, Z., Zhang, Y., Li, Y., et al. (2023). How loneliness linked to anxiety and depression: a network analysis based on Chinese university students. BMC Public Health 23:2499. doi: 10.1186/s12889-023-17435-4
Yang, Y., Zhang, M., and Kou, Y. (2016). Self-compassion and life satisfaction: the mediating role of hope. Pers. Individ. Dif. 98, 91–95. doi: 10.1016/j.paid.2016.03.086
Zanon, C., Bardagi, M. P., Layous, K., and Hutz, C. S. (2014). Validation of the satisfaction with life scale to Brazilians: evidences of measurement non-invariance across Brazil and US. Soc. Indic. Res. 119, 443–453. doi: 10.1007/s11205-013-0478-5
Zanon, C., Bastianello, M. R., Pacico, J. C., and Hutz, C. S. (2013). Development and validation of a positive and negative affect scale. Psico USF 18, 193–201. doi: 10.1590/S1413-82712013000200003
Zeng, Y., Guo, Y., Li, L., Hong, Y. A., Li, Y., Zhu, M., et al. (2020). Relationship between patient engagement and depressive symptoms among people living with HIV in a Mobile health intervention: secondary analysis of a randomized controlled trial. JMIR Mhealth Uhealth 8:e20847. doi: 10.2196/20847
Keywords: positive psychology, self-compassion, app, students, mental health, intervention
Citation: Schaab BL, Cunha LF, Silveira DC, da Silva PC, Ballejos KG, Diaz GB, Kaiser V, Calvetti PÜ, Cazella SC, Barros HMT and Reppold CT (2024) A pilot study of a new app based on self-compassion for the prevention and promotion of mental health among Brazilian college students. Front. Psychol. 15:1414948. doi: 10.3389/fpsyg.2024.1414948
Edited by:
Cristina Torrelles-Nadal, University of Lleida, SpainReviewed by:
Michaela Swee, McLean Hospital, United StatesSandiléia Pfeiffer, Pontifical Catholic University of Rio Grande do Sul, Brazil
Ming Yu Claudia Wong, The Education University of Hong Kong, Hong Kong SAR, China
Copyright © 2024 Schaab, Cunha, Silveira, da Silva, Ballejos, Diaz, Kaiser, Calvetti, Cazella, Barros and Reppold. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bruno Luis Schaab, YnJ1bm8uc2NoYWFiQHVmY3NwYS5lZHUuYnI=