Abstract
Introduction:
Forced displacement constitutes a global crisis impacting millions of people especially in the Middle East, leaving them impacted by traumatic history. Humanitarian aid workers (HAWs) who support displaced individuals are exposed to high risk of burnout and secondary traumatic stress (STS).
Methods:
This study aimed to identify the prevalence of compassion satisfaction (CS) and compassion fatigue (CF), referring to burnout and STS, respectively, using the Professional Quality of Life Scale (ProQOL). The study explored the relationships between these factors and personal variables that are related to shared trauma, as well as coping mechanisms assessed using the Brief-COPE questionnaire among Middle Eastern HAWs working with displaced individuals.
Results:
The study involved 78 HAWs supporting displaced individuals in the Middle East. The mean age was 25.81 years (SD = ± 5.54); 55% were females, and the majority (88%) were Syrians. Approximately 90% of participants were engaged in Turkey and Syria. The most prevalent coping mechanisms were religion and planning. Being a graduate predicted burnout, whereas older age, previous mental diagnosis, and shared trauma predicted higher STS levels. Compassion satisfaction was predicted by active coping, and compassion fatigue was predicted by negative coping.
Conclusion:
HAWs require education to recognize CF signs and psychological training to promote effective coping mechanisms, mitigate CF, and enhance higher levels of CS. More research is needed on the psychology of HAWs and the role of shared trauma and coping mechanisms.
Introduction
Forced displacement is an escalating global phenomenon that disrupts the lives of millions of individuals and communities, profoundly impacting their wellbeing and stability. In 2023, the United Nations High Commissioner for Refugees (UNHCR) estimated that more than one in 73 people worldwide were forcibly displaced, totalling approximately 110 million globally, and this number is expected to increase to 130.8 million (UNHCR, 2024; UNHCR, 2023). Individuals often face displacement due to exposure to a diverse array of traumatic events that jeopardize their safety, including torture, violence, kidnapping, and the loss of loved ones, compelling them to seek essential needs outside their homes. Even if they depart from their traumatizing homes, they carry the burden of trauma with them, which adds new layers of distress to the challenges of relocating and adapting to new circumstances (Henry, 2012; Theisen-Womersley, 2021). Moreover, the departure trajectory itself presents inherent risks, encompassing potential threats such as trafficking, forced labor, and the risk of financial or sexual exploitation (IOM, 2024).
In this context, the role of humanitarian aid workers (HAWs) is paramount because they provide vital support and assistance for displaced individuals and offer various resources to help alleviate their suffering. The occupational duties of HAWs involve conducting needs assessments and formulating plans based on individuals’ vulnerabilities, which requires hearing the traumatic details and challenges faced by their clients. This necessitates empathy and the provision of care for the clients, especially in times of crisis (Walkup, 1997). In addition, HAWs might operate in environments marked by risks related to political instability, poverty, and natural disasters, which could entail the risk of death, injury, or witnessing violence against loved ones (Curling and Simmons, 2010). These environments pose threats of death or injury, and the potential for witnessing violence against loved ones. This reality implies that Humanitarian Aid Workers (HAWs), as trauma helpers, may themselves become trauma survivors as they both suffer from the same collective trauma. The dual exposure to trauma at the personal and professional level is often referred to as shared trauma (Tosone, 2011).
This challenging environment in which humanitarian aid workers (HAWs) operate, combined with their continual exposure to traumatized casualties, makes them vulnerable to the development of various psychological disorders (Lopes Cardozo et al., 2012). Research has shown that HAWs have a greater prevalence of depression, anxiety and posttraumatic stress disorder (PTSD), compared to the general population (Strohmeier and Scholte, 2015).
Additionally, increasing attention has been directed toward the prevalence of secondary traumatic stress and burnout among HAWs (Apostolidou, 2016; Jachens et al., 2016; Jones and Williamson, 2014). Secondary traumatic stress (STS), also known as vicarious trauma, was initially introduced in 1990 by McCann and Pearlman as a framework for understanding the response to working with traumatized individuals (McCann and Pearlman, 1990). STS entails cognitive, behavioral, and emotional responses due to indirect exposure to trauma, which elicits responses similar to those observed in PTSD patients. These shared symptoms include hyperarousal, re-experiencing the traumatic events, social withdrawal, depression, and anxiety (Akinsulure-Smith et al., 2018; Connorton et al., 2012; Figley, 2002). Burnout is referred to in the International Classification of Diseases 11th Revision (ICD-11) as “a syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed. It is characterized by three dimensions: (1) feelings of energy depletion or exhaustion; (2) increased mental distance from one’s job or feelings of negativism or cynicism related to one’s job; and (3) a sense of ineffectiveness and lack of accomplishment” (WHO, 2019). Both STS and burnout are regarded as negative consequences of working in the humanitarian aid field.
Occupation-related psychological consequences have been the subject of research interest, and multiple frameworks have been proposed. In the context of aid work, Stamm (Ano and Vasconcelles, 2005; Ozcan et al., 2021; Stamm, 2009) conceptualized professional quality of life as a construct encompassing both positive and negative aspects of professions involving caregiving. Compassion fatigue (CF) comprises two subdomains, namely, STS and burnout, while compassion satisfaction (CS) refers to the feelings of pleasure and meaning derived from providing care (Geiling et al., 2022; Sagaltici et al., 2022).
The levels of CF and CS among HAWs have been demonstrated to vary widely across studies, as they are influenced by various factors, including the work environment, client factors, and personal characteristics (Roberts et al., 2021). Some personal factors related to age, sex, and previous mental diagnosis could influence the levels of CF and CS (Ager et al., 2012). In addition, shared trauma, in which victims and aid workers experience a traumatic event, may play a pivotal role (Hamid et al., 2020). Moreover, the variations in the levels could be explained in part by the adoption of different coping mechanisms. Coping mechanisms refer to adjusting cognitive and behavioral responses to fulfil challenging demands or stressful events and are considered one of the main factors in stress management (Collins, 2008; Folkman and Moskowitz, 2004). Some coping mechanisms are deemed positive and linked to positive mental outcomes, while maladaptive coping mechanisms might accelerate burnout and STS (Kirby et al., 2011; Maresca et al., 2022).
It is crucial for aid organizations and individuals to understand these factors to enhance CS and mitigate CF. Unaddressed CF among HAWs can lead to negative consequences, including a decline in overall quality of life, diminished work performance, strained social relationships, reduced empathy toward care recipients, and feelings of withdrawal and isolation (Adams et al., 2006). To our knowledge, there is limited research on the relationship between professional quality of life, coping mechanisms, and shared trauma among humanitarian aid workers (HAWs) supporting displaced individuals (Foo et al., 2023; Young et al., 2018). Therefore, this preliminary study aims to identify different factors associated with CF and CS and their relationship with different coping mechanisms as a step toward building supportive recommendations for HAWs aiding displaced individuals specifically and aid workers overall.
Methods
Study population and data collection
HAWs work with displaced individuals due to natural and man-made disasters. This study was conducted in January 2024 as part of an online psychoeducational workshop on stress relief, conducted by Shezlong, an Arabic online platform for mental health, to 98 nongovernmental organization (NGO) workers. After the workshops, all the registered participants received an email containing a link to the questionnaire. The email explained the study details and requested consent before proceeding with the questions. After completing the questionnaire, the participants received an automatic email with their scores, interpretations, and additional guidance on stress management tailored to the context of humanitarian aid work. Each participant had the choice to withdraw from the study at any point. The response rate was 79.5%. To minimize potential desirability bias and encourage candid responses, we ensured complete anonymity and confidentiality in the data collection, with no identifying information recorded.
The assessed NGO is a nonprofit humanitarian organization with international reach, primarily operating in Syria, Turkey, Jordan, and Lebanon. While it functions as a national NGO, it has international influence, with a focus on emergency relief efforts, educational support, medical assistance, and shelter programs for displaced individuals. Its financial resources rely on public donations, international crowdfunding campaigns, and community fundraising initiatives. There were no formal mental health support programs for its workers or volunteers. The authors are unable to provide further details about the NGO for reasons of the security of the people involved.
Study measures
Personal characteristics: to measure sex, age, education, marital status, nationality, country of work, nature of work, fieldwork (including contact with displaced individuals, office-based or both), and years of experience. Participants were asked whether they had been previously diagnosed with a mental health condition using a single yes or no question. Individuals were asked about shared trauma using a single yes or no question to determine whether they had experienced an event similar to that experienced by the individuals they assisted. The questions assessing personal characteristics were designed by the authors specifically for this study.
The Professional Quality of Life Questionnaire (ProQOL 5) is a 30-item self-report survey that assesses three subscales among helping professionals: CS, burnout, and STS. Example items include “I am preoccupied with more than one person I help” and “I get satisfaction from being able to help people.” Each item is rated on a Likert scale where 1 = never, 2 = rarely, 3 = sometimes, 4 = often, and 5 = very often. For each subscale, the scoring system denotes the level experienced by the worker: 22 or less is low, between 23 and 41 is moderate, and 42 or more is considered high. The translated Arabic versions were used (Stamm, 2010) and had accepted psychometric analysis for CS (Cronbach’s α = 0.84), burnout (Cronbach’s α = 0.73), and STS (Cronbach’s α = 0.78) (Hamid et al., 2021).
Brief-COPE: a self-reported questionnaire comprising 28 items that is specifically used to evaluate both healthy and unhealthy coping mechanisms employed in response to stressful life events. Each item is scored on a Likert scale ranging from 1 = I have not been doing this at all to 2 = A little bit, 3 = A medium amount, and 4 = I have been doing this a lot. With 2 items for each, 14 coping mechanisms were assessed: active coping, use of informational support, positive reframing, planning, emotional support, venting, humor, acceptance, religion, self-blame, self-distraction, denial, substance use, and behavioral disengagement (Carver, 1997). Example items include “I’ve been criticizing myself.” and “I’ve been looking for something good in what is happening.” The Arabic valid translation tool was used to reveal 3 main subscales based on exploratory factor analysis: active coping, passive coping, and support seeking, with composite reliability scores of 0.84, 0.75, and 0.81, respectively (Alghamdi, 2020). In this study, we evaluated the 14 specific coping mechanisms, and the three general subscales identified in the Arabic translation. The active coping subscale consists of active coping, planning, positive reframing, acceptance, humor, religion, self-distraction, and venting. The passive coping subscale includes the denial, substance use, behavioral disengagement, and self-blame subscales, along with one item each from the self-distraction and venting subscales. Finally, the seeking support subscale included items on emotional and instrumental support.
Ethical approval
Ethics approval was obtained from the Ethics Committee of Al-Azhar Faculty of Medicine with the registry number of “sych.74 Med.Research.prevalence” Depression/Pts.-MS.0000007. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee of Al-Azhar Faculty of Medicine and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Statistical analysis
The collected data were coded and analysed using SPSS software (Armonk, NY: IBM Corp, version 25). Quantitative variables are presented as the mean ± SD, while the categorical variables are expressed as counts (%). Normality was assessed using the Kolmogorov––Smirnov test (KS). Based on the results of the KS test, the relationships between continuous variables and ProQOL outcomes were examined using independent t-tests, Mann–Whitney tests, one-way ANOVA, and Kruskal-Wallis tests. Pearson correlation analysis was used to investigate the relationship between coping mechanisms and ProQOL. Linear regression models were constructed using significant personal characteristics (Model I), Ghamdi coping strategies (Model II), and 14 coping strategies, with p < 0.1 according to the Pearson correlation (Model III). Statistical significance was set at p < 0.05.
Results
Personal characteristics
The study included 78 participants, 55.1% of whom were female. Participants’ ages ranged from 17 to 36 years, with a mean age of 25.81 years (SD = ± 5.54). In terms of education levels, university students comprised 43.6%, followed by graduates (41.0%) and secondary students (15.4%). Most participants reported never being married (65.4%), while 34.6% were married, including 26 currently married and one divorced. The sample was dominated by Syrian (88.4%), with smaller percentages of Turkish (1.3%), Syrian-Turkish (6.4%), Egyptian (1.3%), and Omani (2.6%). Work locations were primarily in Turkey (61.5%), followed by Syria (28.2%) and other regions (10.3%). Among the participants, 39.7% were exclusively office based, 23.1% engaged in fieldwork with direct contact with displaced individuals, and 37.2% performed both office and field duties. The mean years of experience was 4.31 (SD = 3.3). A minority of participants reported a previous diagnosis of a mental health disorder (12.8%), while a large proportion reported shared traumatic experiences with their clients (83.3%) (Table 1).
Table 1
| Study sample (N = 78) | N (%) |
|---|---|
| Sex | |
| Male | 35 (44.9) |
| Female | 43 (55.1) |
| Age | |
| Min. – Max. | 17.0–36.0 |
| Mean ± SD | 25.81 ± 5.54 |
| Education | |
| Secondary student | 12 (15.4) |
| University student | 34 (43.6) |
| Graduate | 32 (41.0) |
| Marital status | |
| Never married | 51 (65.4) |
| Ever married | 27 (34.6) |
| Nationality | |
| Syrian | 69 (88.4) |
| Turkish | 1 (1.3) |
| Syrian – Turkish | 5 (6.4) |
| Egyptian | 1 (1.3) |
| Omani | 2 (2.6) |
| Country of work | |
| Turkey | 48 (61.5) |
| Syria | 22 (28.2) |
| Other | 8 (10.3) |
| Nature of work | |
| Office work only | 31 (39.7) |
| Field work and direct contact with victims only | 18 (23.1) |
| Both office and field work | 29 (37.2) |
| Years of experience | |
| Min. – Max. | 0.16–12.0 |
| Mean ± SD | 4.31 ± 3.3 |
| Previous mental diagnosis | |
| Yes | 10 (12.8) |
| No | 68 (87.2) |
| Shared Trauma | |
| Yes | 65 (83.3) |
| No | 13 (16.7) |
| Compassion satisfaction (CS) | |
| Low | 0 (0.0) |
| Moderate | 47 (60.3) |
| High | 31 (39.7) |
| Min. – Max. | 25.0–50.0 |
| Mean ± SD. | 39.54 ± 5.88 |
| Burnout | |
| Low | 29 (37.2) |
| Moderate | 49 (62.8) |
| High | 0 (0.0) |
| Min. – Max. | 13.0–37.0 |
| Mean ± SD | 24.73 ± 5.25 |
| Secondary traumatic stress (STS) | |
| Low | 18 (23.1) |
| Moderate | 59 (75.6) |
| High | 1 (1.3) |
| Min. – Max. | 11.0–42.0 |
| Mean ± SD | 28.31 ± 7.22 |
Personal characteristics and professional quality of life.
Professional quality of life
Regarding ProQoL of life, none of the participants had low levels of CS. A total of 60.3% reported moderate levels of CS, while 39.7% reported high levels of CS. Regarding burnout, 37.2% exhibited low levels, 62.8% reported moderate levels, and none of the participants reported high levels. In terms of STS, approximately one-quarter of the participants (23.1%) reported low levels, three-quarters (75.6%) reported moderate levels, and only 1.3% reported high levels of STS (Table 1).
Coping mechanisms
With respect to the subscales of the general coping mechanism, Figure 1 shows that the most prevalent coping was active coping, with a mean percentage of 68.41%, followed by seeking support (66.13%), while passive coping had a mean percentage of 53.657% (Supplementary Table 1). Among the 14 coping mechanisms analyzed, Figure 2 shows that the leading four were religion (84.0%), planning (77.8%), active coping (73.8%), and acceptance (76%). Conversely, the four least utilized mechanisms included behavioral disengagement (53.4%), denial (49.9%), venting (42%), and substance use (38.3%) (Supplementary Table 2).
Figure 1
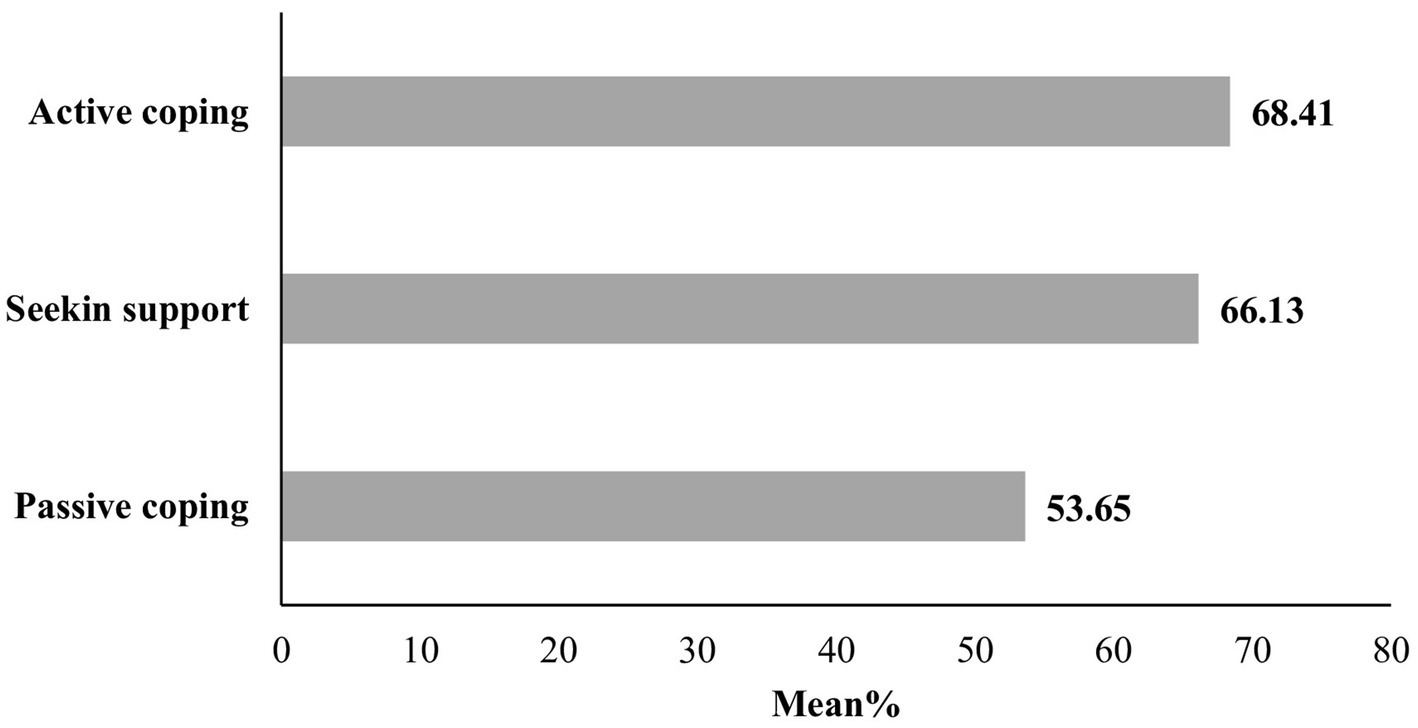
Mean percentage of the general coping mechanisms.
Figure 2
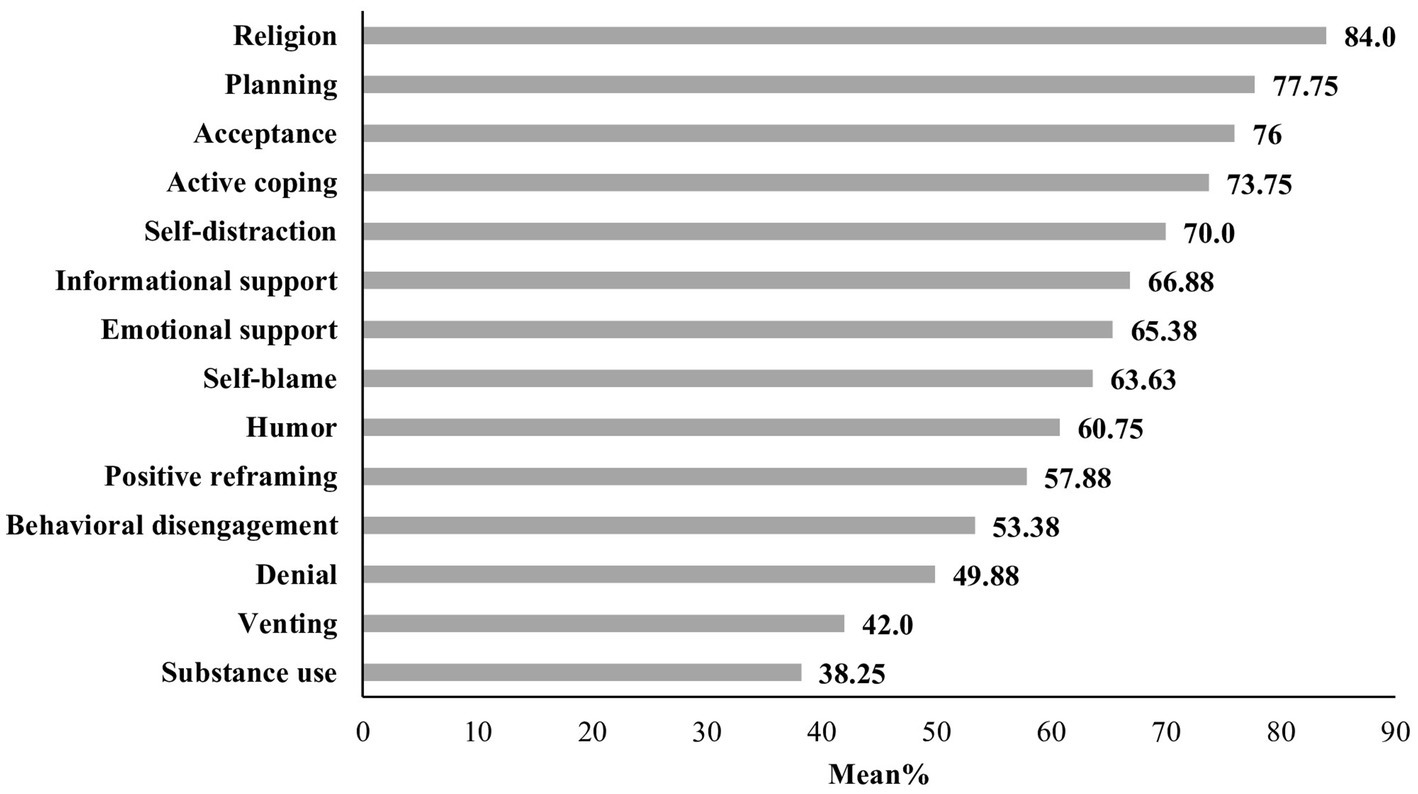
Mean percentage of the specific coping mechanisms.
ProQoL and personal factors
This study explored the relationship between the ProQoL and personal factors. No statistically significant associations were observed between CS and the personal factors examined. However, males exhibited significantly higher levels of burnout (p = 0.004); older age and years of experience demonstrated a positive correlation with burnout (r = 0.437, p < 0.001; r = 0.349, p = 0.002, respectively). A statistically significant difference in education was noted regarding burnout (p = 0.025), particularly among graduates compared with university students. Additionally, being ever married (p = 0.049) and the nature of work (p = 0.049) were significant factors, as pairwise comparisons revealed that individuals involved in both office and fieldwork exhibited greater burnout levels than those solely engaged in fieldwork. However, for STS, males also exhibited significantly increased levels (p = 0.024). Additionally, a positive correlation was observed between age and years of experience in relation to burnout (r = 0.405, p < 0.001; r = 0.278, p = 0.014, respectively). Furthermore, a significant association was found between STS and previous mental diagnosis (p = 0.038), and between STS and shared trauma (p = 0.002) (Table 2).
Table 2
| CS | p | Burnout | p | STS | p | |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Male | 39.83 ± 6.0 | 0.697 | 26.57 ± 4.77 | 0.004* | 30.34 ± 6.15 | 0.024* |
| Female | 39.3 ± 5.83 | 23.23 ± 5.19 | 26.65 ± 7.66 | |||
| Age | r = 0.063 | 0.584 | r = 0.437 | <0.001* | r = 0.405 | <0.001* |
| Education | ||||||
| Secondary student | 39.33 ± 5.76 | 0.919 | 25.25 ± 5.07 | 0.025* | 27.08 ± 6.07 | 0.212 |
| University student | 39.85 ± 5.96 | 22.97 ± 4.83 | 27.15 ± 7.93 | |||
| Graduate | 39.28 ± 6.0 | 26.41 ± 5.3$ | 30.0 ± 6.67 | |||
| Marital status | ||||||
| Never married | 38.82 ± 5.89 | 0.141 | 23.88 ± 5.02 | 0.049* | 27.16 ± 7.16 | 0.052 |
| Ever married | 40.89 ± 5.71 | 26.33 ± 5.39 | 30.48 ± 6.95 | |||
| Nationality | ||||||
| Single nationality | 39.3 ± 5.89 | 0.181 | 24.7 ± 5.27 | 0.919 | 28.14 ± 7.38 | 0.353 |
| Double nationality | 43.0 ± 4.95 | 25.2 ± 5.36 | 30.80 ± 3.70 | |||
| Country of work | ||||||
| Turkey | 38.71 ± 6.0 | 0.136 | 23.96 ± 5.15 | 0.228 | 27.19 ± 6.88 | 0.103 |
| Syria | 41.59 ± 5.44 | 26.36 ± 5.65 | 31.32 ± 6.99 | |||
| Other | 38.88 ± 5.59 | 24.88 ± 4.05 | 26.75 ± 8.29 | |||
| Nature of work | ||||||
| Office work only | 39.19 ± 5.73 | 0.364 | 24.61 ± 5.35 | 0.049* | 27.81 ± 7.04 | 0.360 |
| Field work and direct contact with victims only | 38.28 ± 6.27 | 22.44 ± 3.93 | 29.76 ± 7.51 | |||
| Both office and field work | 40.69 ± 5.78 | 26.28 ± 5.46& | 28.31 ± 7.22 | |||
| Years of experience | r = 0.101 | 0.383 | r = 0.349 | 0.002* | 0.278 | 0.014* |
| Previous mental diagnosis | ||||||
| Yes | 41.5 ± 4.01 | 0.261 | 26.3 ± 5.5 | 0.314 | 32.7 ± 6.18 | 0.038* |
| No | 39.25 ± 6.07 | 24.5 ± 5.21 | 27.66 ± 7.17 | |||
| Shared trauma | ||||||
| Yes | 39.92 ± 5.86 | 0.3 | 24.91 ± 5.26 | 0.656 | 29.49 ± 6.98 | 0.002* |
| No | 38.0 ± 5.88 | 24.17 ± 5.39 | 22.83 ± 5.34 | |||
Professional quality of life and personal factors.
The data are expressed as the mean ± SD, r; Pearson correlation $significant with university students, &significant with field work, *Statistically significant p < 0.05.
Since no personal factors were significantly related to CS, we only performed a linear regression model between personal factors and burnout, and between personal factors and STS. The model for burnout was significant, with F = 3.259 and p = 0.003, and explained 27.7% of the variance; only graduation was the only predictor of burnout. For STS, the linear regression model was also significant (F = 9.669, p < 0.001) and explained a wide range of variability with R2 = 45.7%. Age, previous mental diagnosis and shared trauma predicted STS (Table 3).
Table 3
| Predictors | Unstandardized coefficients B std. error |
Standardized coefficients Beta |
t | Individual predictors sig | 95% Confidence interval | |
|---|---|---|---|---|---|---|
| Burnout# | ||||||
| Constant | 17.586 | 5.369 | 3.276 | 0.002* | 6.874–28.299 | |
| Age | 0.276 | 0.193 | 0.239 | 1.430 | 0.157 | −0.109 – 0.662 |
| Femalea | −1.154 | 1.438 | −0.110 | −0.803 | 0.425 | −4.023 – 1.715 |
| Field workb | −1.562 | 1.562 | −0.124 | −1.000 | 0.321 | −4.679 – 1.556 |
| Office and field workb | 0.418 | 1.432 | 0.039 | 0.292 | 0.771 | −2.440 – 3.276 |
| Ever marriedc | −0.736 | 1.390 | −0.067 | −0.530 | 0.598 | −3.509 – 2.037 |
| Education (secondary students)d | 2.025 | 1.641 | 0.140 | 1.234 | 0.222 | −1.250 – 5.299 |
| Education (Graduate)d | 3.033 | 1.259 | 0.285 | 2.408 | 0.019* | 0.520–5.546 |
| Years of experience | 0.161 | 0.268 | 0.101 | 0.600 | 0.551 | −0.375 – 0.697 |
| Secondary traumatic stress$ | ||||||
| Constant | 8.262 | 6.502 | 1.271 | 0.208 | −4.705 – 21.229 | |
| Age | 0.641 | 0.223 | 0.407 | 2.882 | 0.005* | 0.197–1.085 |
| Femalea | −1.047 | 1.727 | −0.073 | −0.606 | 0.546 | −4.491 – 2.397 |
| Years of experience | −0.143 | 0.331 | −0.066 | −0.431 | 0.668 | −0.802 – 0.517 |
| Previous mental diagnosise | 4.506 | 2.100 | 0.213 | 2.146 | 0.035* | 0.319–8.694 |
| Shared traumae | 6.213 | 1.958 | 0.317 | 3.174 | 0.002* | 2.308–10.117 |
Linear regression model of personal factors predicting affecting professional quality of life (Model I).
aref (Male), bref (other work nature), cref (never married), dref (other education), eref (no).
# F = 3.259, p = 0.003*, R2 = 27.7%, $F = 6.542, p < 0.001*, R2 = 31.8%.
ProQOL and coping mechanisms
With respect to the correlation between ProQOL and coping mechanisms, among the three subscales, active coping exhibited a positive correlation with CS (r = 0.317, p = 0.005), and passive coping demonstrated a positive correlation with STS (r = 0.406, p = 0.001). Among the 14 coping mechanisms, statistically significant correlations with CS were found for planning (r = 0.354, p = 0.001) and acceptance (r = 0.279, p = 0.013). For burnout, significant positive correlations were found with venting (r = 0.257, p = 0.023) and substance use (r = 0.432, p < 0.001), while significant negative correlations were observed with acceptance (r = −0.231, p = 0.042) and religion (r = −0.399, p < 0.001). For STS, significant positive correlations were found with venting (r = 0.256, p = 0.023), denial (r = 0.299, p = 0.008), self-blame (r = 0.339, p = 0.002), substance use (r = 0.351, p = 0.002), and behavioral disengagement (r = 0.379, p = 0.001) (Table 4).
Table 4
| Compassion satisfaction | Burnout | Secondary traumatic stress | ||||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| General copinng mechanisms | ||||||
| Active coping | 0.317 | 0.005* | −0.100 | 0.384 | 0.130 | 0.255 |
| Passive coping | −0.075 | 0.514 | 0.206 | 0.070 | 0.406 | <0.001* |
| Seeking support | 0.151 | 0.186 | −0.043 | 0.705 | 0.158 | 0.166 |
| Specific coping mechanisms | ||||||
| Active coping | 0.167 | 0.144 | 0.005 | 0.963 | 0.199 | 0.081 |
| Informational support | 0.180 | 0.115 | −0.044 | 0.699 | 0.160 | 0.160 |
| Positive reframing | 0.080 | 0.484 | 0.047 | 0.684 | 0.180 | 0.115 |
| Planning | 0.354 | 0.001* | 0.067 | 0.560 | 0.160 | 0.162 |
| Emotional support | 0.100 | 0.383 | −0.036 | 0.754 | 0.133 | 0.247 |
| Venting | 0.130 | 0.256 | 0.257 | 0.023* | 0.256 | 0.023* |
| Humor | −0.091 | 0.431 | 0.007 | 0.950 | −0.073 | 0.525 |
| Acceptance | 0.279 | 0.013* | −0.231 | 0.042* | −0.221 | 0.052 |
| Religion | 0.208 | 0.068 | −0.399 | <0.001* | −0.052 | 0.652 |
| Self-blame | 0.026 | 0.824 | 0.114 | 0.319 | 0.339 | 0.002* |
| Self-distraction | 0.009 | 0.938 | −0.115 | 0.315 | 0.113 | 0.324 |
| Denial | −0.120 | 0.296 | 0.046 | 0.687 | 0.299 | 0.008* |
| Substance use | 0.054 | 0.636 | 0.432 | <0.001* | 0.351 | 0.002* |
| Behavioral disengagement | −0.069 | 0.551 | 0.204 | 0.074 | 0.379 | 0.001* |
Correlations between professional quality of life and coping mechanisms.
*Statistically significant p < 0.05.
According to the linear regression analysis of the general coping mechanisms, active coping emerged as a predictor of CS, whereas negative coping predicted both burnout and STS. In terms of specific coping mechanisms, planning was associated with a higher CS, substance use positively predicted burnout, and religion was a negative predictor. However, no specific coping mechanism was found to predict STS (Table 5).
Table 5
| Predictors | Unstandardized coefficients B std. error |
Standardized coefficients Beta |
t | Individual predictors sig | 95% Confidence interval | |
|---|---|---|---|---|---|---|
| Compassion satisfaction&1,&2 | ||||||
| Constant | 27.235 | 5.526 | 4.928 | <0.001* | 16.223–38.246 | |
| Active coping | 0.357 | 0.123 | 0.314 | 2.903 | 0.005* | 0.112–0.603 |
| Passive coping | −0.238 | 0.159 | −0.175 | −1.493 | 0.140 | −0.555 – 0.079 |
| Seeking support | 0.351 | 0.216 | 0.190 | 1.626 | 0.108 | −0.079 – 0.782 |
| Constant | 23.419 | 4.417 | 5.301 | <0.001* | 14.617–32.221 | |
| Planning | 1.270 | 0.624 | 0.260 | 2.035 | 0.045* | 0.026–2.513 |
| Acceptance | 0.516 | 0.487 | 0.134 | 1.058 | 0.294 | −0.456 – 1.487 |
| Religion | 0.758 | 0.475 | 0.171 | 1.596 | 0.115 | −0.188 – 1.704 |
| Burnout#1,#2 | ||||||
| Constant | 24.401 | 5.129 | 4.757 | <0.001* | 14.181–34.621 | |
| Active coping | −0.112 | 0.114 | −0.110 | −0.977 | 0.332 | −0.339 – 0.116 |
| Passive coping | 0.326 | 0.148 | 0.268 | 2.203 | 0.031* | 0.031–0.620 |
| Seeking support | −0.225 | 0.200 | −0.137 | −1.123 | 0.265 | −0.625 – 0.174 |
| Constant | 32.192 | 4.322 | 7.448 | <0.001* | 23.576–40.808 | |
| Venting | 0.099 | 0.466 | 0.023 | 0.212 | 0.833 | −0.830 – 1.028 |
| Acceptance | −0.461 | 0.336 | −0.134 | −1.370 | 0.175 | −1.131 – 0.210 |
| Religion | −1.610 | 0.375 | −0.407 | −4.291 | <0.001* | −2.358 – −0.862 |
| Substance use | 1.915 | 0.543 | 0.405 | 3.524 | 0.001* | 0.832–2.999 |
| Behavioral disengagement | −0.011 | 0.360 | −0.003 | −0.031 | 0.975 | −0.729 – 0.706 |
| Secondary traumatic stress$1,$2 | ||||||
| Constant | 8.861 | 6.659 | 1.331 | 0.187* | −4.408 – 22.130 | |
| Active coping | 0.136 | 0.148 | 0.097 | 0.916 | 0.363 | −0.160 – 0.432 |
| Passive coping | 0.668 | 0.192 | 0.399 | 3.479 | 0.001* | 0.285–1.050 |
| Seeking support | −0.009 | 0.260 | −0.004 | −0.033 | 0.974 | −0.527 – 0.510 |
| Constant | 10.369 | 5.638 | 1.839 | 0.070 | −0.875 – 21.613 | |
| Active coping | 1.071 | 0.608 | 0.195 | 1.763 | 0.082 | −0.141 – 2.283 |
| Venting | 0.725 | 0.725 | 0.124 | 1.000 | 0.321 | −0.721 – 2.172 |
| Acceptance | −0.708 | 0.519 | −0.150 | −1.364 | 0.177 | −1.742 – 0.327 |
| Self-blame | 0.846 | 0.859 | 0.124 | 0.985 | 0.328 | −0.867 – 2.558 |
| Denial | 0.417 | 0.579 | 0.083 | 0.720 | 0.474 | −0.738 – 1.573 |
| Substance use | 0.963 | 0.809 | 0.148 | 1.190 | 0.238 | −0.651 – 2.577 |
| Behavioral disengagement | 1.070 | 0.660 | 0.221 | 1.620 | 0.110 | −0.247 – 2.386 |
Linear regression model of coping mechanisms predicting professional quality of life (Model II, III).
&1 F = 4.065, p = 0.010*, R2 = 14.1%, &2F = 4.875, p = 0.004*, R2 = 16.5%,#1F = 1.916, p = 0.134, R2 = 7.2%, #2F = 8.586, p < 0.001*, R2 = 37.4%, $1F = 5.190, p = 0.003*, R2 = 17.4%, $2F = 4.419, p < 0.001*, R2 = 30.6%.
Discussion
HAWs face various psychosocial stressors due to their work conditions and interactions with the traumatized individuals they aid, leading to indirect exposure to traumatic events. Consequently, many HAWs may experience distressing symptoms associated with personal factors or maladaptive coping mechanisms (Chen et al., 2020). Unmanaged CF might result in increased levels of absenteeism, impaired productivity, and work commitment, as well as complete cessation of aid work (Curling and Simmons, 2010). Therefore, studying CF, CS, and their association with other factors is crucial for improving the mental well-being of those working in the humanitarian aid field.
Despite most of our sample working in the Middle East, which is known for its geopolitical instabilities, the HAWs in our study exhibited high levels of CS. The absence of low CS levels has been reported in Hispanic caregivers serving Hispanic-displaced refugees in El Paso, Texas, a border region between the United States and Mexico (Lusk and Terrazas, 2015). This aligns with findings from other studies demonstrating elevated CS levels among professionals working with traumatized people (Burnett and Wahl, 2015; Craig and Sprang, 2010; Thieleman and Cacciatore, 2014). With respect to the CF subscales, our study revealed that nearly two-thirds of the participants exhibited a moderate level of burnout, while three-quarters demonstrated a moderate level of STS. Surprisingly, no participants reported high degrees of burnout, and only 1% exhibited high levels of STS. This could be justified by the high levels of CS, as CS is shown to negatively correlate with CF (Gonzalez-Mendez et al., 2020; Tessitore et al., 2023). Heightened CS may stem from the gratitude received from displaced people, a sense of accomplishment, and the valuable gained experience (Apostolidou, 2016). Working with displaced individuals can foster feelings of hope and inspiration, strengthen social connections, and enhance self-image (Barrington and Shakespeare-Finch, 2013).
In our study, male sex, older age, and more years of experience were associated with CF (both burnout and STS). These findings diverge from those of several studies on HAWs. A meta-analysis indicated that CF was either not associated with sex or was more prevalent among females (Cieslak et al., 2014). Other studies have suggested that older and more experienced workers exhibit lower levels of distress and CF, possibly due to their adoption of coping strategies or the quitting of individuals already experiencing significant distress.(Eriksson et al., 2009; Lopes Cardozo et al., 2005) Noticeably, some studies conducted on internal and external displaced refugees from Syria have indicated that men are often exposed to more traumatic events and are at a greater risk of developing PTSD (Tekeli-Yesil et al., 2018). This may imply differing gender roles in non-Western contexts, leading to variable exposures to traumatic experiences. Similarly, the observed associations in our study between CF and older age, male sex, and increased experience could be due to higher job responsibilities and increased workload (Hensel et al., 2015; Ogińska-Bulik et al., 2021).
This may imply differing gender roles in non-Western contexts, leading to variable prevalence rates for these issues. The observed correlations between older age, male sex, and increased experience with higher job responsibilities and workload could offer further insights into these associations.
A history of mental diagnosis was associated with STS in our study. Of the 41 possible variables, a systematic review revealed that a previous psychiatric diagnosis was one of three reliable predictors of psychiatric disorders, including secondary trauma and PTSD symptoms (Opie et al., 2020). A previous study proposed that this process is linked to adopting a negative coping mechanism (Foo et al., 2023).
In our study, shared trauma was significantly associated with higher STS scores and served as a predictor of STS according to linear regression analysis. Working in crisis situations renders HAWs both helpers and survivors themselves, exposing them to trauma directly and indirectly, and increasing their vulnerability to traumatic stress reactions (Lindsay, 2007; Tosone et al., 2011). Shared trauma involves a combination of symptoms of PTSD and STS due to the double exposure to trauma personally and professionally (Tosone et al., 2015), and such exposure makes it difficult to distinguish symptoms related to personal traumatic exposure from those related to professional work (Ehring et al., 2011). On the other hand, the qualitative analysis of shared exposure revealed that shared reality for workers with displaced individuals could be an additive advantage, as it creates a common background with regard to language and cultural barriers, allowing for more empathy and understanding, and in turn enhancing the levels of compassion satisfaction (Hamid et al., 2020). Another study reported that the experience of trauma could be a motive to work in the relief field as a source of meaning and life purpose (Wang et al., 2013).
The findings from our linear regression analysis revealed that heightened levels of active coping were indicative of greater CS, whereas increased negative coping was linked to higher levels of burnout and STS. For the specific coping mechanisms in the linear regression, planning demonstrated a positive correlation with CS; substance use was identified as a positive predictor of burnout, whereas religion emerged as a negative predictor. Religion and planning were the most prevalent coping mechanisms in the sample. Few studies have examined the coping mechanisms among HAWs, therefore, understanding the role of coping mechanisms in the lives of HAWs is crucial; in response to distress, HAWs use maladaptive coping mechanisms such as social isolation, anger, unhealthy eating, and alcohol or smoking (Jachens et al., 2016; Young et al., 2018).
Religion was the most prevalent coping mechanism among participants in this study. In the Middle East, religion and spirituality constitute central frameworks in people’s daily lives, serving as active components of identity and being widely utilized as a resource to overcome life difficulties (Koenig and Al Shohaib, 2023). These values highly prioritize charity and aiding those in need, underscoring the significance of compassion and altruism in religious teachings (Abo El Nasr and Eltaiba, 2016; Chaney and Church, 2017; Soliman, 2017). Religiosity and spirituality were found to be significant protective factors and linked to mental wellbeing, as perceived divine support can mitigate the effects of burnout, negatively correlate with different aspects of burnout, (Shin et al., 2014) and contribute to posttraumatic growth (Cardozo et al., 2013; Eriksson et al., 2015). These findings align with our results, in which religion exhibited a negative correlation with burnout. Although religion is perceived as a coping mechanism against stress, certain forms of religious coping are associated with adverse mental outcomes, including spiritual discontent, passive religious deferral, reassessment of God’s powers, and punitive God’s reappraisal (Ano and Vasconcelles, 2005; Grey et al., 2024). However, the Brief-COPE scale used in our study did not include distinctive items for assessing the different types of religious coping.
Planning was the second most prevalent coping mechanism and was positively linked to compassion satisfaction; it involves actively determining the best approach to address a stressor by considering appropriate actions to take as stress increases (Carver et al., 1989). It may serve as a strategy for those facing emergencies and are experiencing crisis situations regularly in their jobs (Yeşil and Polat, 2023). Such insights could be leveraged at the organizational level to establish effective plans for both organizational and personal growth. Substance use was the least-reported coping mechanism and was associated with higher rates of burnout. This is considered a form of passive coping. The low prevalence of substance use, such as alcohol use, among HAWs can be attributed to cultural beliefs (Lopes Cardozo et al., 2005).
Our study has some limitations. First, its cross-sectional design prevented the establishment of causal relationships. Second, the use of self-report questionnaires introduces the potential for recall or social desirability bias. Furthermore, the relatively small sample size and restriction to a single organization might limit the generalizability of our findings due to possible sampling bias and geographical restrictions. However, prior research has indicated that organizational type may not have a significant impact on mental health symptoms (Strohmeier and Scholte, 2015). Moreover, no specific data were collected on the nature of prior mental health diagnoses due to the sensitivity of the question and the relatively small sample size, which limited the potential for further analysis. This factor could be important in understanding predispositions to CF within our population. Therefore, further research with a larger sample is needed to explore the impact of mental health diagnoses on mental health outcomes in similar populations.
On the other hand, this study highlighted the frequency of CF and CS among a specific group of HAWs who work with displaced communities and shed light on the role of shared trauma and general and specific coping mechanisms in the prevalence of CS and CF. The study findings could be used for further training and education regarding the impact of CS and CF on mental well-being and working abilities. As recommended by the UNHCR (Antares Foundation, 2012), HAWs should be educated on alarming signs that require seeking mental health help, as many altruistic tendencies and a sense of obligation toward work might impede seeking help, thereby perpetuating CF (Gemignani and Giliberto, 2020). Organizations can contribute to empowering humanitarian aid workers (HAWs) by recognizing the threshold at which increased workload may lead to heightened mental distress (Posselt et al., 2020). Additionally, organizations can help provide training and education on the effective management of negative emotions and provide insights into the role of coping mechanisms, as previous psychological training is associated with less burnout, increased levels of well-being, and individual (Young and Pakenham, 2021). Moreover, organizations are advised to have an organizational approach to mental symptoms and to consider psychological wellbeing prior to recruiting workers (Shah et al., 2007).
Further research
Given the preliminary nature of our findings, further studies with larger, more representative sample sizes across different organizations are needed. Future research should focus more on the nature of work and levels of responsibility in relation to mental health outcomes, as well as emphasize the role of shared trauma and different types of coping mechanisms among HAWs. We hope this study serves as a catalyst for longitudinal studies, inspiring more comprehensive research in this critical area.
Conclusion
This study aimed to address key gaps in the literature about the psychology of HAWs in the Middle East. A significant frequency of CS and CF among HAWs supporting displaced communities. Factors such as sex, age, years of experience, and shared trauma were associated with burnout and STS. Specific coping mechanisms, such as religion and planning, positively impact HAWs’ mental well-being of HAWs, while substance use is linked to higher burnout rates. The authors have identified several recommendations including providing education on recognizing signs of mental distress among HAWs, implementing coherent organizational approaches to support their mental health, offering psychosocial training at the point of recruitment and at regular intervals thereafter, and fostering emotional caring and supportive leadership within aid organizations. Moreover, further research is needed to explore the role of shared trauma and coping mechanisms on the psychology of HAWs.
Statements
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of Al-Azhar Faculty of Medicine with the registry number of “sych.74 Med.Research.prevalence” Depression/Pts.-MS.0000007. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MA: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. NA: Conceptualization, Writing – review & editing. IS: Investigation, Writing – review & editing. ME: Conceptualization, Investigation, Methodology, Project administration, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
MA, NA were employed by Shezlong Inc.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2025.1522092/full#supplementary-material
References
1
Abo El Nasr M. Eltaiba N. (2016). Social work in Egypt: experiences and challenges. Br. J. Educ. Soc. Behav. Sci.16, 1–11. doi: 10.9734/BJESBS/2016/25882
2
Adams R. E. Boscarino J. A. Figley C. R. (2006). Compassion fatigue and psychological distress among social workers: a validation study. Am. J. Orthopsychiatry76, 103–108. doi: 10.1037/0002-9432.76.1.103
3
Ager A. Pasha E. Yu G. Duke T. Eriksson C. Cardozo B. L. (2012). Stress, mental health, and burnout in national humanitarian aid workers in Gulu, northern Uganda. J. Trauma. Stress.25, 713–720. doi: 10.1002/jts.21764
4
Akinsulure-Smith A. M. Espinosa A. Chu T. Hallock R. (2018). Secondary traumatic stress and burnout among refugee resettlement workers: the role of coping and emotional intelligence. J. Trauma. Stress.31, 202–212. doi: 10.1002/jts.22279
5
Alghamdi M. (2020). Cross-cultural validation and psychometric properties of the arabic brief cope in Saudi population. Med. J. Malays.75, 502–509
6
Ano G. G. Vasconcelles E. B. (2005). Religious coping and psychological adjustment to stress: a meta-analysis. J. Clin. Psychol.61, 461–480. doi: 10.1002/jclp.20049
7
Antares Foundation , (2012). Managing stress in humanitarian workers guidelines for good practice. Antares Foundation. Available at: https://www.antaresfoundation.org/filestore/si/1164337/1/1167964/managing_stress_in_humanitarian_aid:workers_guidelines_for_good_practice.pdf?etag=4a88e3afb4f73629c068ee24d9bd30d9
8
Apostolidou Z. (2016). The notion of professional identity among practitioners working with asylum seekers. A discursive analysis of practitioners’ experience of clinical supervision and working context in work with asylum seekers. Eur J Psychother Couns18, 4–18. doi: 10.1080/13642537.2015.1130073
9
Barrington A. J. Shakespeare-Finch J. (2013). Working with refugee survivors of torture and trauma: an opportunity for vicarious post-traumatic growth. Couns. Psychol. Q.26, 89–105. doi: 10.1080/09515070.2012.727553
10
Burnett H. J. Wahl K. (2015). The compassion fatigue and resilience connection: a survey of resilience, compassion fatigue, burnout, and compassion satisfaction among trauma responders. Int. J. Emerg. Ment. Health17, 318–326. doi: 10.4172/1522-4821.1000165
11
Cardozo B. L. Sivilli T. I. Crawford C. Scholte W. F. Petit P. Ghitis F. et al . (2013). Factors affecting mental health of local staff working in the Vanni region, Sri Lanka. Psychol. Trauma5, 581–590. doi: 10.1037/a0030969
12
Carver C. S. (1997). You want to measure coping but your protocol’s too long: consider the brief COPE. Int. J. Behav. Med.4, 92–100. doi: 10.1207/s15327558ijbm0401_6
13
Carver C. S. Scheier M. F. Weintraub K. J. (1989). Assessing coping strategies: a theoretically based approach. J. Pers. Soc. Psychol.56, 267–283. doi: 10.1037/0022-3514.56.2.267
14
Chaney C. Church W. T. (2017). Islam in the 21st century: can the Islamic belief system and the ethics of social work be reconciled?J. Relig. Spirit. Social Work36, 25–47. doi: 10.1080/15426432.2017.1311246
15
Chen J. Li J. Cao B. Wang F. Luo L. Xu J. (2020). Mediating effects of self-efficacy, coping, burnout, and social support between job stress and mental health among young Chinese nurses. J. Adv. Nurs.76, 163–173. doi: 10.1111/jan.14208
16
Cieslak R. Shoji K. Douglas A. Melville E. Luszczynska A. Benight C. C. (2014). A meta-analysis of the relationship between job burnout and secondary traumatic stress among workers with indirect exposure to trauma. Psychol. Serv.11, 75–86. doi: 10.1037/a0033798
17
Collins S. (2008). Statutory social work: stress, job satisfaction, coping, social support, and individual differences. Br. J. Soc. Work38, 1173–1193. doi: 10.1093/bjsw/bcm047
18
Connorton E. Perry M. J. Hemenway D. Miller M. (2012). Humanitarian relief workers and trauma-related mental illness. Epidemiol. Rev.34, 145–155. doi: 10.1093/epirev/mxr026
19
Craig C. D. Sprang G. (2010). Compassion satisfaction, compassion fatigue, and burnout in a national sample of trauma treatment therapists. Anxiety Stress Coping23, 319–339. doi: 10.1080/10615800903085818
20
Curling P. Simmons K. B. (2010). Stress and staff support strategies for international aid work. Intervention8, 93–105. doi: 10.1097/WTF.0b013e32833c1e8f
21
Ehring T. Razik S. Emmelkamp P. M. G. (2011). Prevalence and predictors of posttraumatic stress disorder, anxiety, depression, and burnout in Pakistani earthquake recovery workers. Psychiatry Res.185, 161–166. doi: 10.1016/j.psychres.2009.10.018
22
Eriksson C. B. Bjorck J. P. Larson L. C. Walling S. M. Trice G. A. Fawcett J. et al . (2009). Social support, organisational support, and religious support in relation to burnout in expatriate humanitarian aid workers. Ment. Health Relig. Cult.12, 671–686. doi: 10.1080/13674670903029146
23
Eriksson C. B. Holland J. M. Currier J. M. Snider L. M. Ager A. K. Kaiser R. E. R. et al . (2015). Trajectories of spiritual change among expatriate humanitarian aid workers: a prospective longitudinal study. Psycholog. Relig. Spiritual7, 13–23. doi: 10.1037/a0037703
24
Figley C. R. (2002). Compassion fatigue: psychotherapists’ chronic lack of self care. J. Clin. Psychol.58, 1433–1441. doi: 10.1002/jclp.10090
25
Folkman S. Moskowitz J. T. (2004). Coping; pitfalls and promise. Annu. Rev. Psychol.55, 745–774. doi: 10.1146/annurev.psych.55.090902.141456
26
Foo C. Y. S. Tay A. K. Yang Y. Verdeli H. (2023). Psychosocial model of burnout among humanitarian aid workers in Bangladesh: role of workplace stressors and emotion coping. Confl. Heal.17, 1–12. doi: 10.1186/s13031-023-00512-1
27
Geiling A. Böttche M. Knaevelsrud C. Stammel N. (2022). A comparison of interpreters’ wellbeing and work-related characteristics in the care of refugees across different work settings. BMC Public Health22. doi: 10.1186/s12889-022-14034-7
28
Gemignani M. Giliberto M. (2020). Constructions of burnout, identity, and self-Care in Professionals Working toward the psychosocial Care of Refugees and Asylum Seekers in Italy. J. Constr. Psychol.34, 56–78. doi: 10.1080/10720537.2019.1700853
29
Gonzalez-Mendez R. Díaz M. Aguilera L. Correderas J. Jerez Y. (2020). Protective factors in resilient volunteers facing compassion fatigue. Int. J. Environ. Res. Public Health17. doi: 10.3390/ijerph17051769
30
Grey I. Thomas J. Mansour Jamaleddine J. Yaktine T. Cheung Chung M. (2024). Religious coping and levels of posttraumatic stress disorder symptomatology after the Beirut explosion. Psychol. Trauma16, 39–48. doi: 10.1037/tra0001529
31
Hamid A. Scior K. Abdul-Hamid W. Williams A. C. De C. (2021). Displaced Syrian mental health workers: an investigation of professional quality of life. J. Refug. Stud.34, 2394–2405. doi: 10.1093/jrs/feaa068
32
Hamid A. Scior K. Williams A. C. D. C. (2020). Qualitative accounts from Syrian mental health professionals: shared realities in the context of conflict and forced displacement. BMJ Open10:e034291. doi: 10.1136/bmjopen-2019-034291
33
Henry H. M. (2012). African refugees in Egypt: trauma, loss, and cultural adjustment. Death Stud.36, 583–604. doi: 10.1080/07481187.2011.553330
34
Hensel J. M. Ruiz C. Finney C. Dewa C. S. (2015). Meta-analysis of risk factors for secondary traumatic stress in therapeutic work with trauma victims. J. Trauma. Stress.28, 83–91. doi: 10.1002/jts.21998
35
IOM , (2024). On this journey, no one cares if you live or die: Abuse, protection and justice along routes between east and West Africa and Africa’s Mediterranean coast – Volume 2 | IOM publications platform [WWW document]. IOM Publications Platform. Available online at: https://publications.iom.int/books/journey-no-one-cares-if-you-live-or-die
36
Jachens L. Houdmont J. Thomas R. (2016). Effort–reward imbalance and heavy alcohol consumption among humanitarian aid workers. J. Stud. Alcohol Drugs77, 904–913. doi: 10.15288/jsad.2016.77.904
37
Jones C. Williamson A. E. (2014). Volunteers working to support migrants in Glasgow: a qualitative study. Int J Migr Health Soc Care10, 193–206. doi: 10.1108/IJMHSC-10-2013-0034
38
Kirby R. Shakespeare-Finch J. Palk G. (2011). Adaptive and maladaptive coping strategies predict Posttrauma outcomes in ambulance personnel. Traumatology (Tallahass Fla)17, 25–34. doi: 10.1177/1534765610395623
39
Koenig H. G. Al Shohaib S. (2023). Religious involvement and psychological well-being in the Middle East. Int. J. Psychiatry Med.59, 341–359. doi: 10.1177/00912174231197548
40
Lindsay J. (2007). The impact of the 2ND intifada: an exploration of the experiences of Palestinian psychosocial counselors and social workers. Illness Crisis Loss15, 137–153. doi: 10.1177/105413730701500206
41
Lopes Cardozo B. Gotway Crawford C. Eriksson C. Zhu J. Sabin M. Ager A. et al . (2012). Psychological distress, depression, anxiety, and burnout among international humanitarian aid workers: a longitudinal study. PLoS One7:e44948. doi: 10.1371/journal.pone.0044948
42
Lopes Cardozo B. Holtz T. H. Kaiser R. Gotway C. A. Ghitis F. Toomey E. et al . (2005). The mental health of expatriate and Kosovar Albanian humanitarian aid workers. Disasters29, 152–170. doi: 10.1111/j.0361-3666.2005.00278.x
43
Lusk M. Terrazas S. (2015). Secondary trauma among caregivers who work with Mexican and central American refugees. Hisp. J. Behav. Sci.37, 257–273. doi: 10.1177/0739986315578842
44
Maresca G. Corallo F. Catanese G. Formica C. Lo Buono V. (2022). Coping strategies of healthcare professionals with burnout syndrome: A systematic review, vol. 58:327. Medicina (Kaunas, Lithuania: MDPI).
45
McCann I. L. Pearlman L. A. (1990). Vicarious traumatization: a framework for understanding the psychological effects of working with victims. J. Trauma. Stress.3, 131–149. doi: 10.1007/BF00975140
46
Ogińska-Bulik N. Gurowiec P. J. Michalska P. Kędra E. (2021). Prevalence and predictors of secondary traumatic stress symptoms in health care professionals working with trauma victims: a cross-sectional study. PLoS One16:e0247596. doi: 10.1371/journal.pone.0247596
47
Opie E. Brooks S. Greenberg N. Rubin G. J. (2020). The usefulness of pre-employment and pre-deployment psychological screening for disaster relief workers: a systematic review. BMC Psychiatry20:211. doi: 10.1186/s12888-020-02593-1
48
Ozcan O. Hoelterhoff M. Wylie E. (2021, 2021). Faith and spirituality as psychological coping mechanism among female aid workers: a qualitative study. J. Int. Humanit. Action16, 1–14. doi: 10.1186/s41018-021-00100-z
49
Posselt M. Baker A. Deans C. Procter N. (2020). Fostering mental health and well-being among workers who support refugees and asylum seekers in the Australian context. Health Soc. Care Community28, 1658–1670. doi: 10.1111/hsc.12991
50
Roberts F. Teague B. Lee J. Rushworth I. (2021). The prevalence of burnout and secondary traumatic stress in professionals and volunteers working with forcibly displaced people: a systematic review and two Meta-analyses. J. Trauma. Stress.34, 773–785. doi: 10.1002/jts.22659
51
Sagaltici E. Cetinkaya M. Nielsen S. Y. Sahin S. K. Gulen B. Altindag A. (2022). Identified predictors and levels of burnout among staff workers in a refugee camp of first immigrant group: a cross-sectional study. Medicine11, 135–141. doi: 10.5455/medscience.2021.08.272
52
Shah S. A. Garland E. Katz C. (2007). Secondary traumatic stress: prevalence in humanitarian aid workers in India. Traumatology (Tallahass Fla)13, 59–70. doi: 10.1177/1534765607299910
53
Shin H. Park Y. M. Ying J. Y. Kim B. Noh H. Lee S. M. (2014). Relationships between coping strategies and burnout symptoms: a meta-analytic approach. Prof Psychol Res Pr45, 44–56. doi: 10.1037/a0035220
54
Soliman H. H. (2017). Social work in the Middle East: Routledge.
55
Stamm B.H. (2009). Professional quality of life: compassion satisfaction and fatigue version 5 (ProQOL). Available at: https://proqol.org/ (Accessed December 23, 2023).
56
Stamm B.H. (2010). The concise ProQOL manual. Eastwoods: LLC.
57
Strohmeier H. Scholte W. F. (2015). Trauma-related mental health problems among national humanitarian staff: a systematic review of the literature. Eur. J. Psychotraumatol.6. doi: 10.3402/ejpt.v6.28541
58
Tekeli-Yesil S. Isik E. Unal Y. Almossa F. A. Unlu H. K. Aker A. T. (2018). Determinants of mental disorders in Syrian refugees in Turkey versus internally displaced persons in Syria. Am. J. Public Health108, 938–945. doi: 10.2105/AJPH.2018.304405
59
Tessitore F. Caffieri A. Parola A. Cozzolino M. Margherita G. (2023). The role of emotion regulation as a potential mediator between secondary traumatic stress, burnout, and compassion satisfaction in professionals working in the forced migration field. Int. J. Environ. Res. Public Health20:2266. doi: 10.3390/ijerph20032266
60
Theisen-Womersley G. (2021). Trauma and resilience among displaced populations: a sociocultural exploration, Cham: Springer. 1–305.
61
Thieleman K. Cacciatore J. (2014). Witness to suffering: mindfulness and compassion fatigue among traumatic bereavement volunteers and professionals. Social Work (United States)59, 34–41. doi: 10.1093/sw/swt044
62
Tosone C. (2011). The legacy of september 11: shared trauma, therapeutic intimacy, and professional posttraumatic growth. Traumatology (Tallahass Fla)17, 25–29. doi: 10.1177/1534765611421963
63
Tosone C. McTighe J. P. Bauwens J. (2015). Shared traumatic stress among social Workers in the Aftermath of hurricane Katrina. Br. J. Soc. Work.45, 1313–1329. doi: 10.1093/bjsw/bct194
64
Tosone C. Mctighe J. P. Bauwens J. Naturale A. (2011). Shared traumatic stress and the long-term impact of 9/11 on Manhattan clinicians. J. Trauma. Stress.24, 546–552. doi: 10.1002/jts.20686
65
UNHCR , (2023). Mid-Year Trends 2023 | UNHCR. Available online at: https://www.unhcr.org/mid-year-trends-report-2023 (Accessed 1. 27. 24).
66
UNHCR , (2024). Global Appeal 2024 | Global Focus. Available online at: https://reporting.unhcr.org/global-appeal-2024 (Accessed 1.28.24).
67
Walkup M. (1997). Policy dysfunction in humanitarian organizations: the role of coping strategies, institutions, and organizational culture. J. Refug. Stud.10, 37–60. doi: 10.1093/jrs/10.1.37
68
Wang X. L. Chan C. L. W. Shi Z. B. Wang B. (2013). Mental health risks in the local workforce engaged in disaster relief and reconstruction. Qual. Health Res.23, 207–217. doi: 10.1177/1049732312467706
69
WHO (2019). Burnout an “occupational phenomenon”: International Classification of Diseases. Geneva: World Health Organization. Available at: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases
70
Yeşil A. Polat Ş. (2023). Investigation of psychological factors related to compassion fatigue, burnout, and compassion satisfaction among nurses. BMC Nurs.22. doi: 10.1186/s12912-023-01174-3
71
Young T. Pakenham K. I. (2021). The mental health of aid workers: risk and protective factors in relation to job context, working conditions, and demographics. Disasters45, 501–526. doi: 10.1111/disa.12440
72
Young T. K. H. Pakenham K. I. Norwood M. F. (2018). Thematic analysis of aid workers’ stressors and coping strategies: work, psychological, lifestyle and social dimensions. J. Int. Humanit. Action3, 1–16. doi: 10.1186/s41018-018-0046-3
Summary
Keywords
burnout, compassion satisfaction, displacement, humanitarian aid work, shared trauma, secondary traumatic stress, Middle East
Citation
Adwi M, Abdellatif N, Sadek I and Elsheikh M (2025) Compassion satisfaction and compassion fatigue in humanitarian aid workers: the relationship with shared trauma and coping mechanisms. Front. Psychol. 16:1522092. doi: 10.3389/fpsyg.2025.1522092
Received
05 November 2024
Accepted
06 March 2025
Published
02 April 2025
Volume
16 - 2025
Edited by
Vasfiye Bayram Deger, Mardin Artuklu University, Türkiye
Reviewed by
Amaya Alexandra Ramos, Independent researcher, Washington, DC, United States
Wilis Srisayekti, Padjadjaran University, Indonesia
Hıdır Apak, Mardin Artuklu University, Türkiye
Updates
Copyright
© 2025 Adwi, Abdellatif, Sadek and Elsheikh.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohamed Adwi, mohamed.adwi.206@azhar.edu.eg
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.