 Dawei Wang1,2
Dawei Wang1,2 Yuheng Zhang
Yuheng Zhang Songtao Lu
Songtao Lu- 1School of Physical Education, Central China Normal University, Wuhan, China
- 2College of Physical Education, Hubei Minzu University, Enshi, China
- 3School of Sports, Wuhan University of Science and Technology, Wuhan, China
- 4School of Sports Health, Hubei University of Chinese Medicine, Wuhan, China
Background: Depression symptoms are commonly experienced by adults and older people; however, there is uncertainty concerning the associations of lifestyle with the risk of depression. This study systematically reviewed and meta-analyzed observational data to assess the link between instrumented sedentary behavior (i-SB) and physical activity (i-PA) measures and depression risk among adult and older populations.
Methods: A systematic review across four databases was performed up to July 27, 2024, targeting studies linking i-SB, i-PA, and depression. The review included a dose–response meta-analysis, presenting results as odds ratios (OR) and 95% confidence intervals (95% CI).
Results: Fifty-one studies, encompassing 1,318,687 participants, fulfilled the inclusion criteria. The comparison between the most and least sedentary groups yielded a pooled OR of 1.09 (95% CI 1.05–1.13). The comparison between the least and most active participant groups yielded pooled ORs of 0.96 (95% CI 0.93–0.98) for light activity (LPA), 0.91 (95% CI 0.86–0.96) for moderate-to-vigorous activity (MVPA), 0.93 (95% CI 0.90–0.96) for total physical activity (TPA), and 0.87 (95% CI 0.81–0.94) for steps per day. After adjusting i-PA, a lower OR for i-SB did not indicate a significant link to increased depression risk. Meta-regression analyses confirmed a dose–response relationship between SB, MVPA, daily steps, and depression.
Conclusion: The association between i-SB and the risk of depression was not consistent with the results of previous self-reported studies. MVPA linked to the risk of depression was independent of i-SB, whereas the link between i-SB and the risk of depression was not independent of i-PA.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=546666, identifier CRD42024546666.
1 Introduction
Mental health encompasses cognitive rationality, emotional equilibrium, behavioral suitability, interpersonal harmony, and adaptive flexibility, marking a state of well-being throughout an individual’s developmental trajectory. According to a 2017 survey conducted by the World Health Organization, nearly one billion individuals worldwide, a staggering figure, are grappling with various mental health challenges (World Health Organization, 2017). The 2020 WHO Guidelines highlight that regular physical activity in adults aged 18–64 yields substantial health benefits, including mental health improvements such as reduced anxiety and depression symptoms, along with enhanced cognitive function and better sleep quality, all of which collectively contribute to an individual’s overall well-being (World Health Organization, 2020). Physical activity (PA), defined as any bodily movement resulting from skeletal muscle contractions that lead to energy expenditure above basal levels (≥1.5 METs[Metabolic Equivalent of Task]), is associated with a multitude of benefits including physical fitness, mental health enhancement, and cognitive improvements (Ainsworth et al., 2011). PA can serve as a complementary or alternative strategy for mental health and behavioral function interventions (Murray et al., 2023). Sedentary behavior (SB), characterized by activities undertaken in a seated, reclined, or supine position during periods of wakefulness, involves an energy expenditure equivalent to or less than 1.5 metabolic equivalents (METs) (Ainsworth et al., 2011). This includes various everyday activities, such as viewing television, engaging with computers, and maintaining a seated posture while utilizing transportation (Tremblay et al., 2017). These behaviors typify a low level of energy expenditure, in contrast to the higher energy demands of PA.
Empirical evidence, as documented in prior investigations, has unequivocally established a link between distinct intensities of PA (Rautio and Seppänen, 2024) and SB (Siwa et al., 2023) and the prevalence and incidence of depressive symptoms. Precisely speaking, extant studies have firmly corroborated the notion that the reallocation of a mere 15-min duration of moderate-to-vigorous PA (MVPA) to SB precipitates a marked elevation in the intensity of depressive symptoms, quantifiable by an increment of 0.46 units on a relevant measurement scale (Murray et al., 2023). Interestingly, the aggregate duration of sedentary time exhibits a significant relationship with escalated depressive symptoms exclusively within the male population (Wemeck et al., 2022). These findings collectively underscore the intricate interplay between sedentary habits, PA patterns, and mental health, particularly in the context of depressive symptom management. Second, previous research has recognized PA as a potentially effective means of preventing mental health issues (Denche-Zamorano et al., 2023). Previous research has confirmed that an increase in PA is associated with a reduction in the risk of depression (B: −0.043, 95% confidence intervals-95% CI: −0.071 to −0.016) (Iob et al., 2023). Furthermore, in adults over the age of 65, depressive symptoms have been associated with a reduction in the total duration of PA at an intensity greater than 3 METs (Dhakal et al., 2023). In summary, PA has a positive causal effect on the prevention of depression, whereas excessive sedentary time may increase the risk of anxiety and diminish mental health status.
However, determining the precise amount of PA required to substantially reduce the risk of depression and, conversely, identifying the threshold of SB that significantly elevates exposure to the risk of depression remains a question worthy of contemplation and further investigation. Previous studies have shown that moderate-to-vigorous PA (MVPA) is significantly associated with a reduced likelihood of depression (pooled odds ratios, OR: 0.817, 95% CI: 0.678 to 0.985). Replacing 30 min of SB with 30 min of MVPA was linked to a decrease in the odds of depression (OR: 0.815, 95% CI: 0.669 to 0.992). Conversely, substituting 30 min of MVPA with 30 min of SB was associated with an increased risk of depression (OR: 1.227, 95% CI: 1.008 to 1.495) (Park et al., 2024). This suggests that converting 30 min of sitting time into an equivalent duration of MVPA can lower the probability of developing depression, whereas replacing 30 min of MVPA with sitting can increase the risk of depression (Park et al., 2024). This indicates that to prevent depression in the elderly, it is advisable to accumulate a greater amount of MVPA throughout the day rather than simply engaging in light PA (LPA) (Chen et al., 2023). This indicates that allocating a greater proportion of one’s daily PA profile to MVPA as opposed to SB or LPA is associated with a notable decrease in the risk of developing depressive disorders (Blodgett et al., 2023). Consequently, the exact delineation of the association between SB and PA concerning depression, in conjunction with a thorough comparative examination of the effect sizes, assumes crucial significance in the conception of potent intervention models geared toward the amelioration of depressive conditions. This knowledge will be instrumental in guiding personalized lifestyle modifications and public health policies designed to optimize mental health outcomes.
Due to the limitations of questionnaires in accurately capturing unstructured PA and the tendency of adults to overestimate PA while underestimating SB (Ryan et al., 2018; Dyrstad et al., 2014), previous meta-analyses and observational studies may have been compromised in their accuracy of estimating the risk of depression due to these subjective factors. Furthermore, self-reported measures tend to overestimate PA and underestimate SB (Ryan et al., 2018). A previous study reported that a total of 119 (76%) young-to-middle-aged adults and 72 (90%) older adults reported that they met the recommended Dutch PA guidelines, while I-PA (instrumented measures) indicated that 37 (24%) and 13 (16%) participants, respectively, objectively met these criteria (Rojer et al., 2020). Given that objective measurements can provide more accurate data, our study exclusively used objective measures of PA and SB, which is a key strength. In other words, using objective instruments such as accelerometers and pedometers, more researchers have quantified the actual association among SB, PA, and depression, effectively mitigating the influence of participants’ subjective factors on the precision of depression risk estimation. These approaches maximally utilize all available data and generate more robust and reliable statistical results.
The aim of this systematic review and meta-analysis is to quantify the link between instrument-assessed sedentary behavior (i-SB) and physical activity (i-PA) with depression. It involves assessing the measurable impacts of i-SB and i-PA and outlining the dose–response relationship with depressive symptoms. Our hypothesis posited that escalated i-SB coupled with diminished i-PA correlates with an augmented risk of depression, which can potentially be ameliorated by increased i-PA or reduced i-SB. The insight derived from this investigation reinforces the pivotal function of PA in curtailing the likelihood of depression and sustaining mental health integrity, concurrently accentuating the importance of judiciously managing sedentary intervals. The empirical evidence garnered herein offers a robust scientific rationale for formulating public health initiatives aimed at endorsing PA and discouraging protracted sedentary periods with the overarching goal of enhancing mental health resilience within the population.
2 Methods
2.1 Search strategy
The systematic review protocol is registered with PROSPERO under CRD42024546666. Following PRISMA guidelines, a rigorous search of PubMed, Scopus, PsycINFO, and SPORTDiscus (via EBSCO) was conducted to identify literature on the link between physical activity and depression, from inception to July 27, 2024. We conducted a search for articles using specific search terms such as “depression OR depressive symptoms,” “physical activity OR exercise OR physical training,” “sedentary behavior OR behavior,” “sedentary OR sedentary behaviors,” “sedentary lifestyle OR lifestyle,” “sedentary OR physical sedentary OR physical inactivity,” “adult OR older,” and “accelerometry OR accelerometer OR pedometer OR monitoring.” We focused on prospective studies. Furthermore, we systematically reviewed the reference lists of all included studies to identify additional eligible articles, without language restrictions. The comprehensive search methodology is detailed in Supplementary Tables S1–S4.
2.2 Study selection
Two of three reviewers (DW and ZG) conducted a comprehensive assessment of titles, abstracts, and full texts to ascertain study eligibility per predefined criteria, with disagreements resolved by a third reviewer (SL). The literature management was facilitated by EndNote (Version X8.2, Clarivate Analytics, Philadelphia, PA, USA). Studies were eligible if they were published in English or Chinese and met the following criteria: (1) observational cohort, cross-sectional, case–control, or Mendelian randomization studies assessing sedentary behavior (SB) or physical activity (PA) via pedometry or accelerometry; (2) included depression, depressive symptoms, or major depression as outcomes; (3) involved adults aged 18 or older; (4) targeted adults generally, not a specific disease group; and (5) reported ORs, RRs, HRs, and 95% CIs for the association between PA/SB and depression risk, or provided data to calculate these metrics. In cases of multiple studies on the same population, only those with longer follow-ups or larger sample sizes were included. Researchers independently identified eligible studies and collectively determined their inclusion based on the established criteria.
2.3 Statistical analyses
This meta-analysis was performed utilizing STATA software (v16.0), with all statistical tests being two-tailed. The analysis involved a two-step approach for categorical and continuous variables to assess the link between physical activity (PA) and depression risk. The results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). Studies were categorized as cohort, cross-sectional, or Mendelian randomization for pooled analysis. Random-effect models were applied to compute pooled ORs. Heterogeneity was assessed using the I2 statistic, with values of 25, 50, and 75% indicating low, moderate, and high heterogeneity, respectively (Higgins et al., 2019). The significance level for evaluating heterogeneity was established at 0.05. The tests conducted by Egger and Begg were employed to ascertain the presence of publication bias (Higgins et al., 2019). To perform sensitivity analysis, studies were sequentially omitted to evaluate their influence on the pooled effect of the remaining studies. Data were categorized into subgroups by study design, gender, age, research domain, study rigor, and control for confounders, followed by meta-analysis. Meta-regression was used to assess heterogeneity across studies.
To assess the relationship between dosage and response, we calculated weekly cumulative durations of physical activity (PA) and sedentary behavior (SB) for each effect value from the literature, assuming constant PA and SB durations over the follow-up period. The median was used to define the reference dose. Intervals below 0.5 were adjusted to 0.25, and when the upper open interval reached 1 or more, the difference between intermediate dose intervals was set at 0.25, resulting in an exposure value of 1.25 (Zhang et al., 2015).
The researchers utilized a robust error meta-regression technique, as outlined by Xu et al., to determine the slopes of the continuous dose–response relationship (nonlinear trends) and their corresponding 95% confidence intervals (Xu and Doi, 2018). This was done by analyzing the natural logarithms of the reported odds ratios (ORs) and confidence intervals (CIs) across several categories of physical activity (PA) and sedentary behavior (SB) measurements. This approach employs a single-stage method, treating each study as a sample cluster. It addresses within-study correlations using clustered robust standard errors. The Stata XBLC function was applied to derive a dose–response curve, based on the model’s goodness-of-fit assessment (Zhang et al., 2015).
2.4 Quality assessment
The Newcastle-Ottawa Scale (NOS) was utilized for quality assessment of the literature (Wells et al., 2000). Quality is directly proportional to the NOS score, with a maximum possible score of 9. Studies were categorized as low, moderate, or high quality based on NOS scores of 0–3, 4–6, and 7–9, respectively. Discrepancies in quality evaluation were resolved through group consensus to determine the final score.
3 Results
3.1 Description of included studies
Initially, we identified 6,939 articles, with 1977 remaining after deduplication. Following title and abstract screening, 234 articles underwent full-text eligibility assessment. An additional article was included post-reference check, culminating in a final analysis of 51 articles, encompassing 14 cohort studies (Blodgett et al., 2023; Chan et al., 2022; Chan et al., 2023; Herbolsheimer et al., 2018; Ho et al., 2022; Hsueh et al., 2020; Hussenoeder et al., 2023; King et al., 2022; Konopka et al., 2022; Ku et al., 2018; Okely et al., 2019; Mossavar-Rahmani et al., 2023; Siwa et al., 2023; Zhang et al., 2021), 33 cross-sectional studies (Araki et al., 2022; Asai et al., 2018; Del Pozo Cruz et al., 2020; Bae et al., 2023; Biddle et al., 2021; Bustamante et al., 2013; Casals et al., 2024; Chen et al., 2023; Dennison et al., 2021; Dhakal et al., 2023; Eriksson et al., 2020; Felez-Nobrega et al., 2023; Heinz et al., 2022; Hollands et al., 2020; Hsiao et al., 2022; Kirschner et al., 2022; Larisch et al., 2020; Lee et al., 2014; Li et al., 2022; Loprinzi, 2013; Loprinzi and Mahoney, 2014; Maher et al., 2018; McKercher et al., 2009; Michalak et al., 2022; Morres et al., 2019; Park et al., 2024; Rethorst et al., 2017; Song et al., 2012; Tully et al., 2020; Vallance et al., 2011; Wemeck et al., 2022; Yasunaga et al., 2018; Zhou et al., 2024) and 4 Mendelian randomization study (Ba et al., 2024; Casanova et al., 2023; Choi et al., 2019; Iob et al., 2023). A visualization of the article selection process is shown in Figure 1.
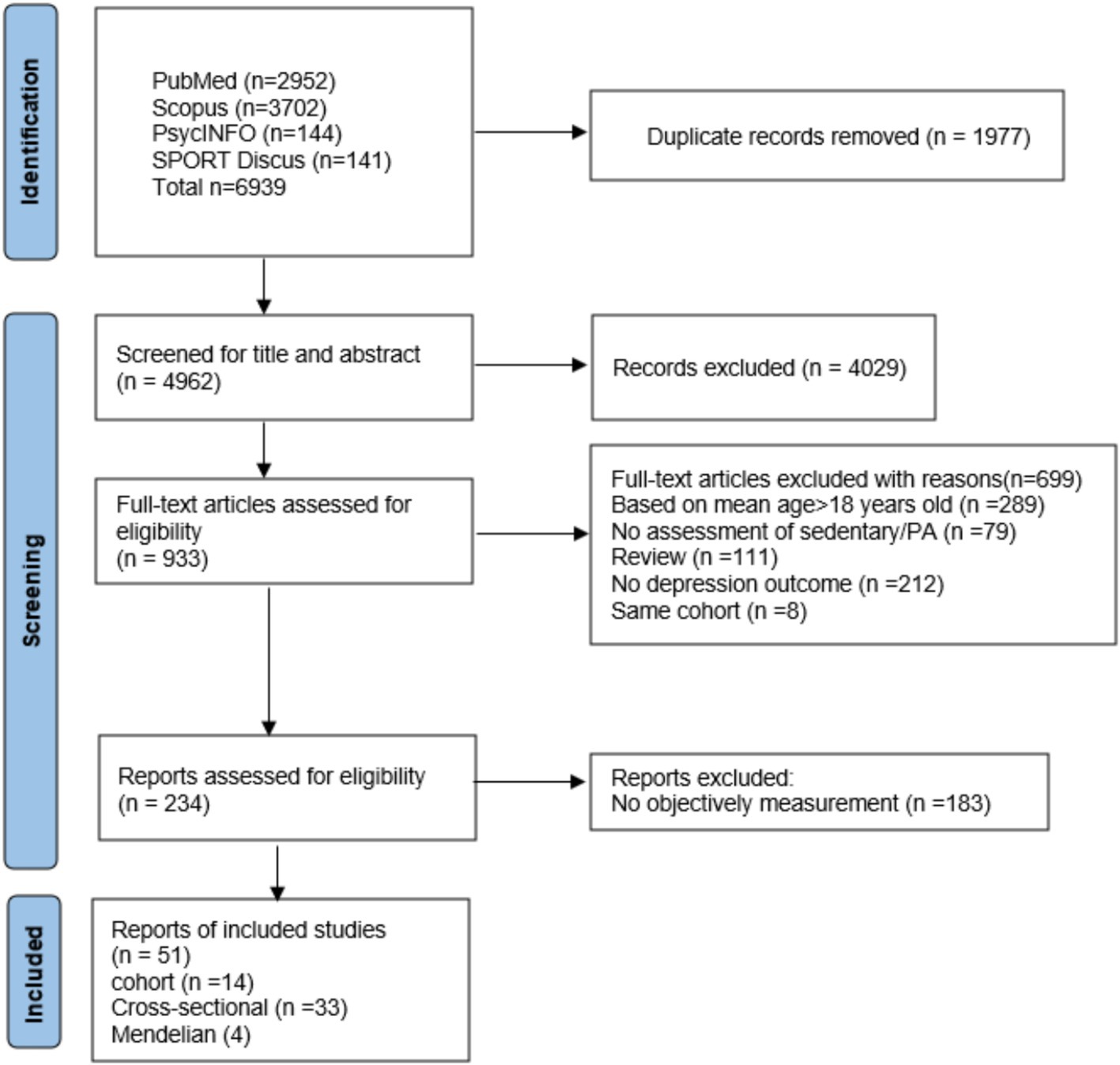
Figure 1. PRISMA flow diagram for the identification of included studies.
Supplementary Table S5 details the characteristics of 51 studies, encompassing 1,318,687 participants across 14 cohort studies (n = 134,047), 33 cross-sectional studies (n = 253,221), and Mendelian randomization studies (n = 812,245). These studies were conducted in Europe (n = 7: UK, Germany, Poland, Spain, Sweden, Greece), Asia (n = 4: Taiwan, China, South Korea, Japan), Oceania (n = 1: Australia), North America (n = 1: USA), and South America (n = 1: Brazil). Participants’ mean age spanned from 18.0 to 86 years, with female representation ranging from 0 to 81.4%. Depression rates across studies varied between 3.2 and 48.8% (Supplementary Table S6). The methodological quality of the studies is detailed in Supplementary Table S8, with 33 out of 51 studies classified as high quality and one study as low quality.
3.2 Measurement method
Supplementary Table S7 provides a summary of the measurement instruments utilized, encompassing accelerometers such as ActiGraph, MoveMonitor, Fitmit Charge, GENEActiv Original, StepWatch™, McRoberts, Actiwatch 2, GENEActiv, Active style ProHJA-350IT, Vitamove, and Yamax Digiwalker. The study employed five accelerometer types, four pedometer types, and three additional devices worn on the hip, wrist, thigh, and triceps. Various cut-off values were applied to evaluate i-SB and i-PA, with i-SB ranging from 1,040 to 2,689 CPM or 1.51 to 2.99 METs, and MVPA thresholds set at >1,040 and ≥ 2,690 CPM or ≥ 3.00 METs. Data collection spanned a minimum of four consecutive days, with the majority of studies extending this period to seven consecutive days.
3.3 Results for instrumented sedentary behavior and physical activity
3.3.1 Sedentary behavior and depression
Supplementary Table S6 presents an overview of the association between i-SB, i-PA, and depression. Figure 2 presents forest plots depicting the link between i-SB and depression risk across 21 studies. The highest i-SB category exhibited an OR of 1.09 (95% CI 1.05–1.13, p < 0.05, I2 = 93.8) relative to the lowest category, as determined by a pooled random-effects model. The OR for cross-sectional studies is 1.15 (95% CI 1.07–1.23), for cohort studies is 1.14 (95% CI 1.01–1.28), and for Mendelian randomization method studies is 1.01 (95% CI 0.99–1.04). The funnel plots (Supplementary Figure SA) indicated no statistically significant publication bias (Egger’s test p = 0.18). Tully et al. (2020) was excluded after sensitivity analysis.
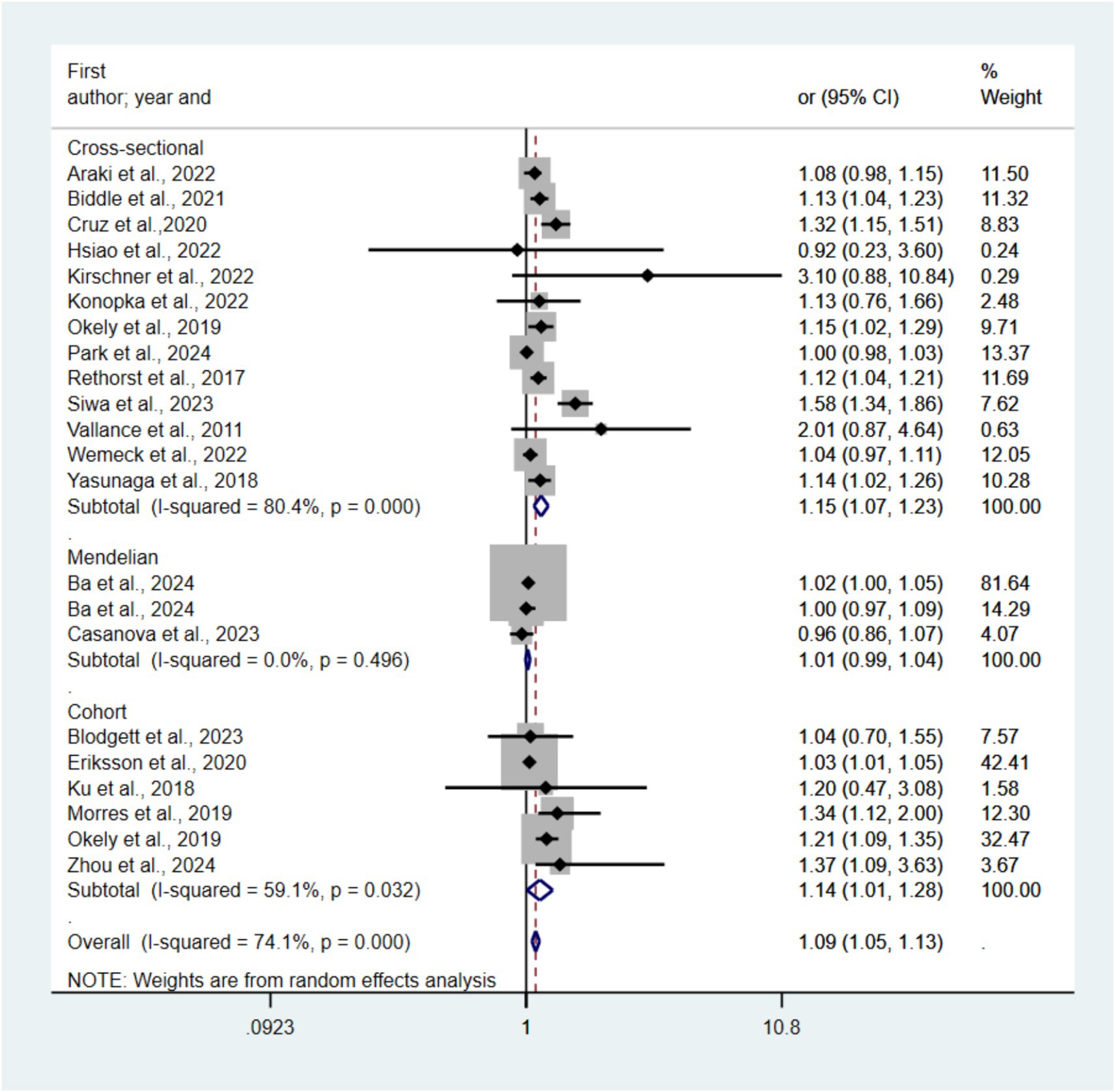
Figure 2. Forest plots of the association between i-SB and risk of depression.
3.3.2 Light physical activity and depression
Figure 3 presents forest plots depicting the correlation between LPA and depression risk across nineteen included studies. Compared with the lowest LPA category, the pooled random-effects model resulted in an OR of 0.96 (95% CI 0.93–0.98, p < 0.05, I2 = 81.2) for the highest category. The OR for cross-sectional studies is 0.97 (95% CI 0.95–0.99), and for cohort studies is 0.90 (95% CI 0.93–0.98). The funnel plots (see Supplementary Figure SB) indicated no statistically significant publication bias (Egger’s test p = 0.31). Sensitivity analysis showed that excluding any single study did not substantially alter the pooled effect estimates.
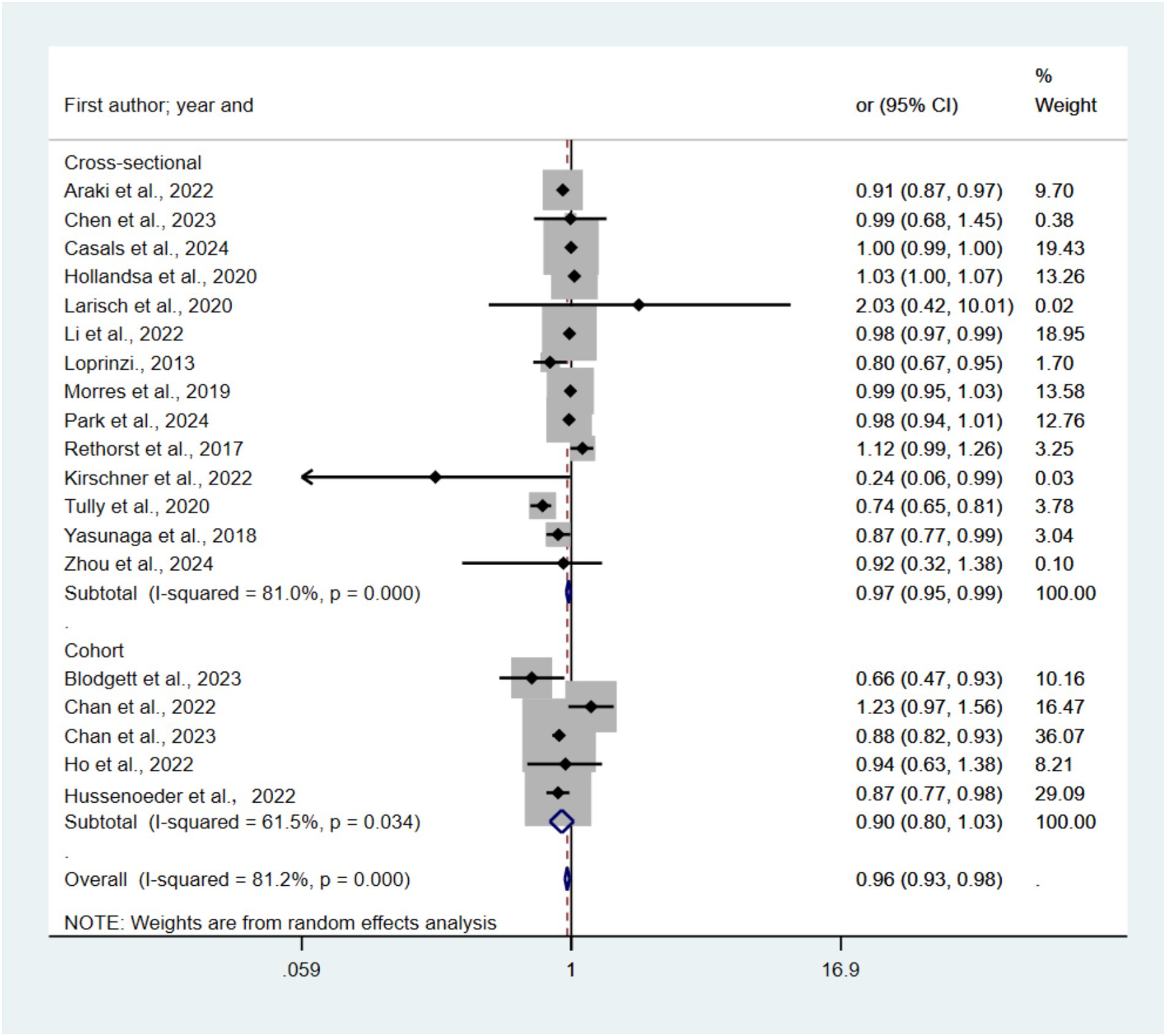
Figure 3. Forest plots of the association between LPA and risk of depression.
3.3.3 Moderate-to-vigorous physical activity and depression
Figure 4 presents forest plots depicting the link between MVPA and depression risk across 30 included studies. Compared with the lowest MVPA category, the pooled random-effects model resulted in an OR of 0.91 (95% CI 0.86–0.96, p < 0.05, I2 = 82.6) for the highest category. The OR for cross-sectional studies is 0.87 (95% CI 0.79–0.95), for cohort studies is 0.94 (95% CI 0.83–1.05), and for Mendelian randomization method studies is 0.96 (95% CI 0.92–1.01). The funnel plots (see Supplementary Figure SC) indicated no statistically significant publication bias (Egger’s test p = 0.40). Konopka et al. (2022) was excluded after sensitivity analysis.
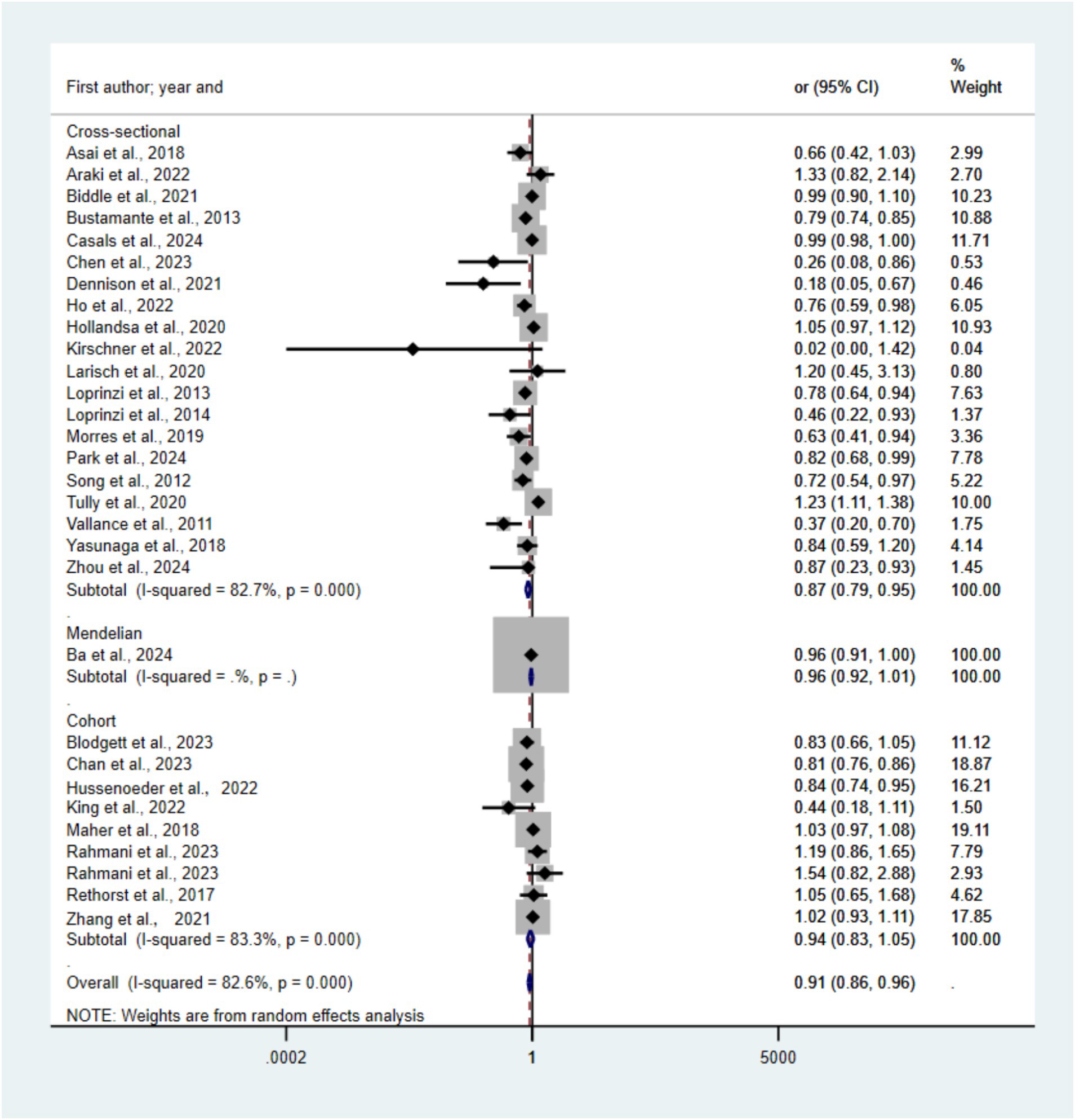
Figure 4. Forest plots of the association between MVPA and risk of depression.
3.3.4 Total physical activity and depression
Figure 5 presents forest plots depicting the relationship between TPA and depression risk across 30 studies. The pooled random-effects model revealed an OR of 0.93 (95% CI 0.90–0.96, p < 0.05, I2 = 86.0%) for the highest TPA category compared to the lowest. Subgroup analyses yielded ORs of 0.93 (95% CI 0.88–0.98) for cross-sectional studies, 0.90 (95% CI 0.82–0.98) for cohort studies, and 0.94 (95% CI 0.91–0.98) for Mendelian randomization studies. Statistically significant publication bias was detected via funnel plot and Egger’s test (p = 0.00). Sensitivity analysis, with individual study exclusion, showed no significant alterations in the combined effect size.
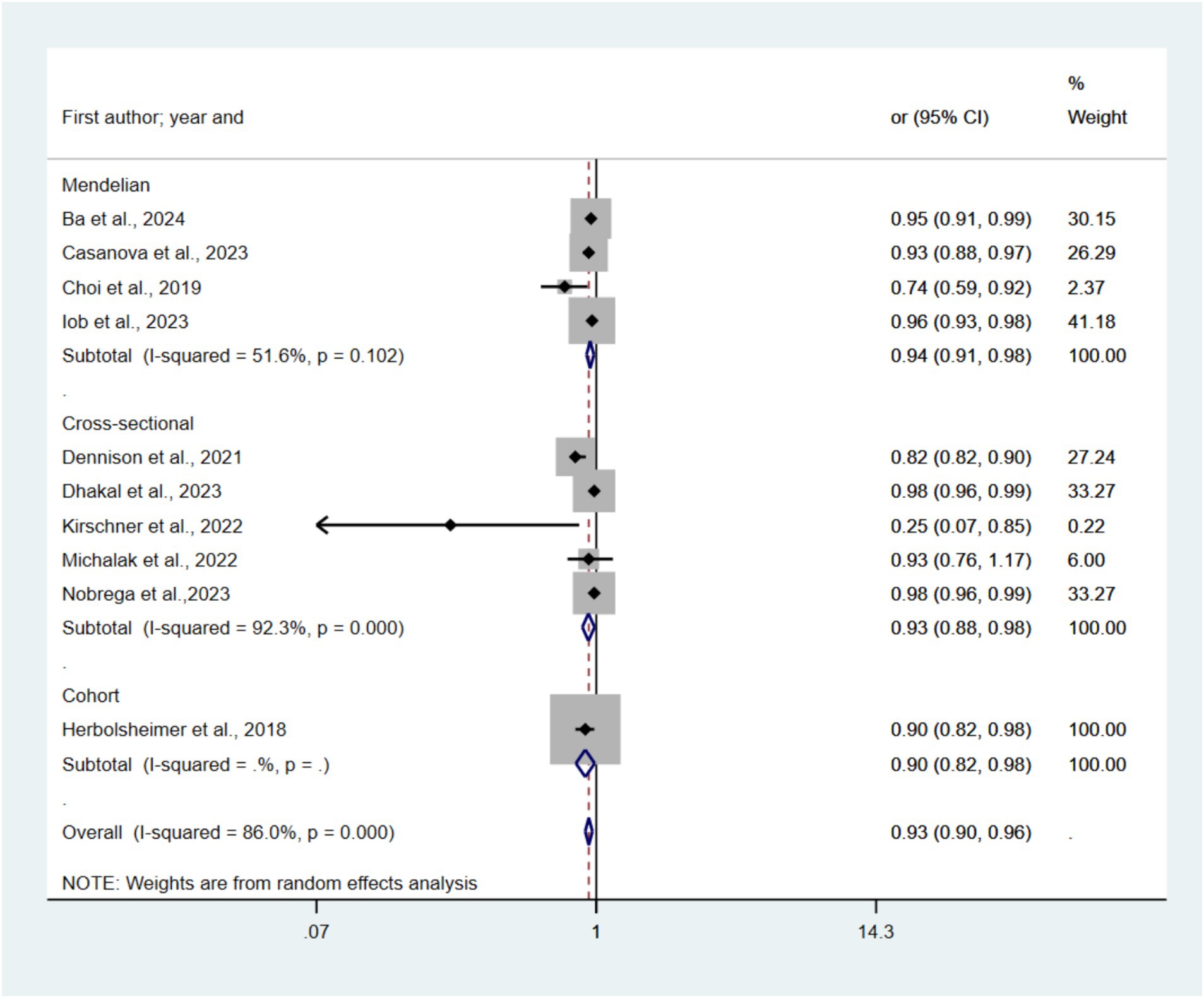
Figure 5. Forest plots of the association between TPA and risk of depression.
3.3.5 Step and depression
Figure 6 presents forest plots depicting the link between TPA and depression risk across nine studies. The pooled random-effects model indicated a significantly lower odds ratio (OR) of 0.87 (95% CI: 0.81–0.94, p < 0.05, I2 = 87.2%) for the highest TPA category compared to the lowest. The stratified analysis revealed ORs of 0.56 (95% CI: 0.28–1.13) for cross-sectional studies and 0.79 (95% CI, 0.68–0.93) for cohort studies. Statistically significant publication bias was detected using both funnel plot analysis (Supplementary Figure SE) and Egger’s test (p = 0.08). Sensitivity analysis, with individual study exclusion, showed no significant alterations in the combined effect size.
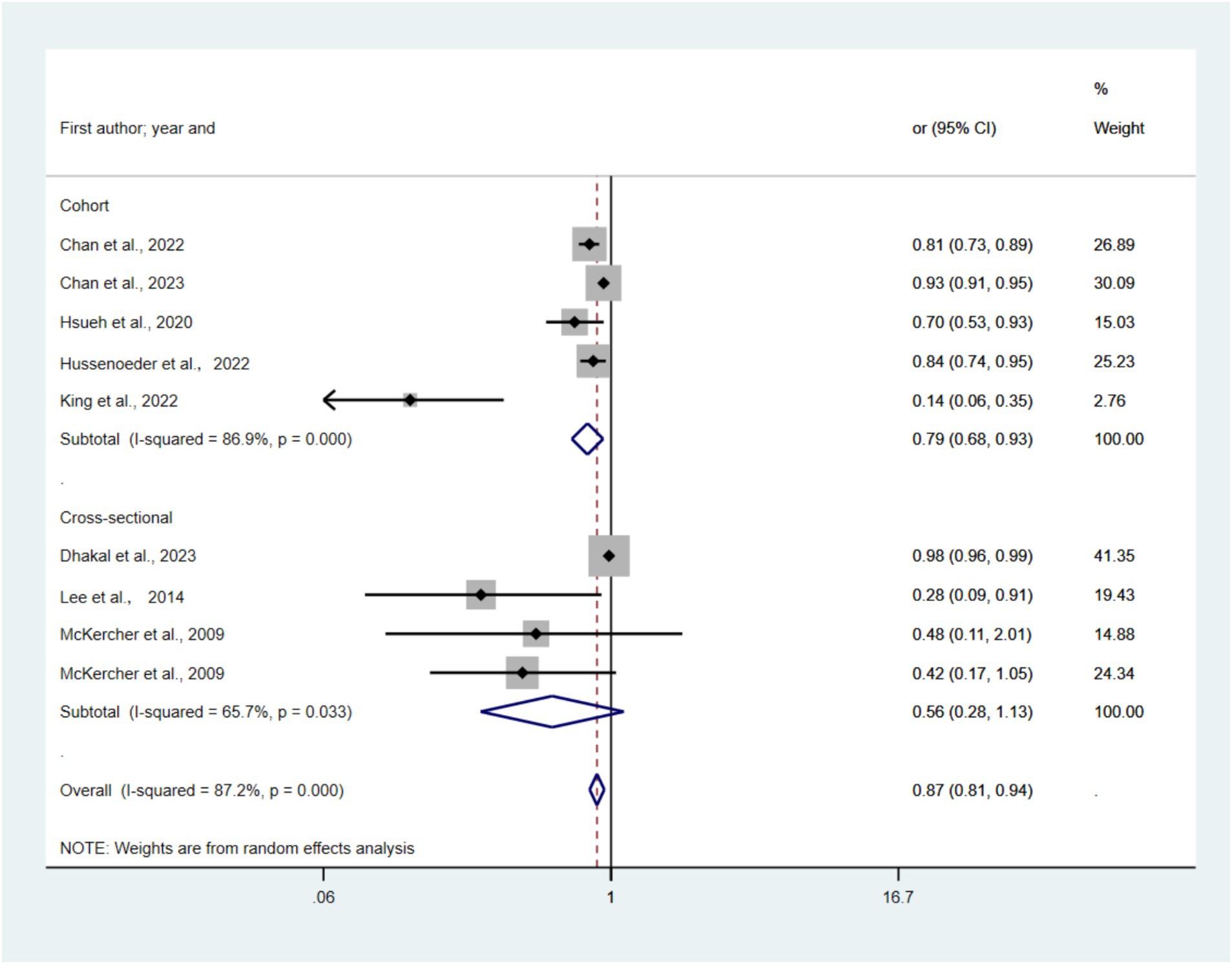
Figure 6. Forest plots of the association between Daily Step and risk of depression.
3.4 Subgroup analysis
Table 1 presents the outcomes of subgroup analyses, assessing the stability of pooled results and identifying potential heterogeneity sources. For MVPA, heterogeneity was significantly associated with study design and depression scales, suggesting their impact on pooled ORs. In the case of SB, heterogeneity was significantly linked to study design and BMI-related confounding factors, indicating their influence on pooled ORs.
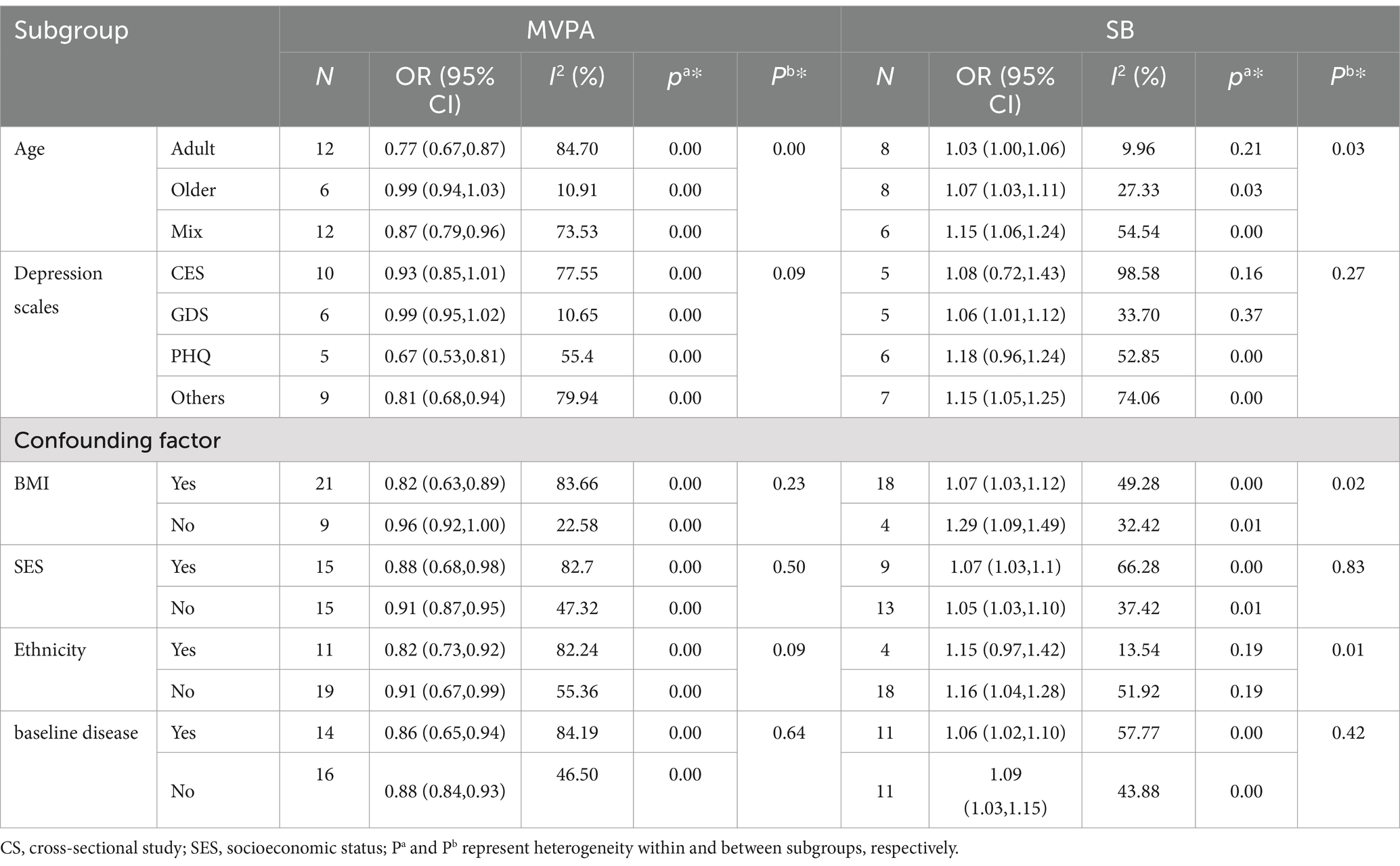
Table 1. Results of the subgroup analysis.
Significant within-subgroup heterogeneity in the studies on MVPA was found in all subgroups, indicating that between-group heterogeneity or other unknown factors may influence heterogeneity. Regarding i-SB, significant heterogeneity was also found in the SB subgroups, except for the Adult, CES, GDS, and Non-Adjusted Ethnicity groups. The findings indicate potential influences on the pooled odds ratios (ORs) of the subgroups by these factors. The relationship between i-PA, i-SB, and depression was inconsistent across most analyses. The high heterogeneity among the included studies may be attributed to the large number of included studies and disparities in the study design, depression ascertainment, and adjustment variables.
3.5 The impact of sedentary behavior and physical activity on depression after mutual adjustment
Regarding SB, seven articles adjusted for time spent in PA, and 14 articles with no adjustment for PA were identified. The pooled random-effects model resulted in an OR with adjusted PA of 1.02 (95% CI 1.00–1.04, p = 0.53 > 0.05, I2 = 0), while the OR for no PA adjusted was 1.20(95% CI 1.08–1.33, p = 0.00 < 0.05, I2 = 95.2%) (see Supplementary Figure SH). Regarding MVPA, four articles adjusted for time spent in SB, and 25 articles did not adjust for SB. The pooled random-effects model resulted in an OR with an adjusted SB of 0.63 (95% CI 0.44–0.89, p = 0.00 < 0.05, I2 = 92.1%), while the OR with no SB adjusted was 0.92 (95% CI 0.87–0.98, p = 0.00 < 0.05, I2 = 82.9%) (see Supplementary Figure SG).
3.6 Dose–response relationship
For SB, we found a linear association relationship between SB and the risk of depression (pnonlinearity = 0. 30) (Figure 7A). The risk of depression increased by 4% for every additional hour of SB per day SB (p < 0.01; OR = 1.04, 95% CI 0.90–1.19). For MVPA, we found a nonlinear association relationship between MVPA and depression (pnonlinearity = 0.0077) (Figure 7B). When MVPA was <35 min/day, the risk of depression decreased by 20% for every additional 5 min/day of MVPA (p < 0.01; OR = 0.80, 95% CI 0.60–0.94). When MVPA was >35 min/day, the risk of depression increased by 16% for every additional 5 min/day of MVPA (p < 0.01; OR = 1.16, 95% CI 0.92–1.56). For steps per day, we found a nonlinear association relationship between steps per day and depression (pnonlinearity = 0.0016) (Figure 7C). When steps per day was <4,000 steps/day, the risk of depression decreased by 9% for every additional 1,000 steps/day of MVPA (p < 0.01; OR = 0.91, 95% CI 0.81–0.99). When steps per day was >4,000 steps/day, the risk of depression decreased by 8% for every additional 1,000 steps/day of MVPA (p < 0.01; OR = 1.08, 95% CI 0.96–1.22).
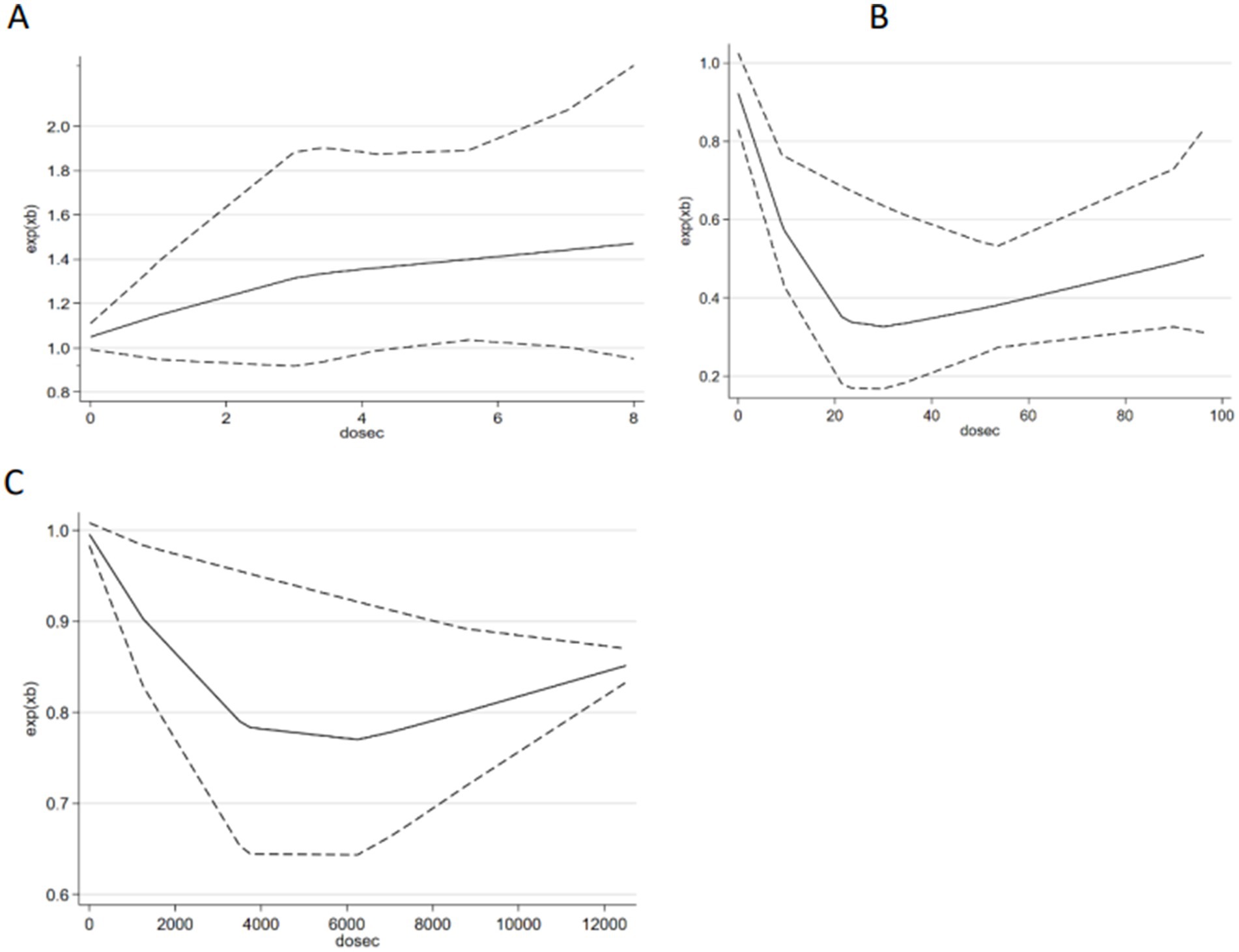
Figure 7. The dose–response relationship between i-SB, MVPA, daily step and depression risk.
4 Discussion
To the best of our knowledge, this is the first systematic review and dose–response meta-analysis of the association between instrumented measures of SB, PA, and depression among adult and older populations. This meta-analysis showed that both higher i-SB levels and lower i-PA levels were associated with a higher depression risk. For SB, LPA, MVPA, TPA, and step, the effect size OR values were 1.09 (95% CI 1.05–1.13), 0.96 (95% CI 0.93–0.98), 0.91 (95% CI 0.86–0.96), 0.93 (95% CI 0.90–0.96), and 0.87 (95% CI 0.81–0.94). The lowest OR was observed for the step group. The study also reported mutually adjusted ORs for PA and SB. Meta-regression analyses confirmed significant dose–response associations between SB, MVPA, daily steps, and depression risk.
The OR of 1.16 (95% CI 1.08–1.24) found in this study is lower than those reported in previous meta-analyses examining the link between self-reported sedentary behavior and depression [1.42, 95% CI: 1.22–1.67 (Zhou et al., 2023); 1.28, 95% CI 1.17–1.39 (Wang et al., 2019), 1.25, 95% CI 1.16–1.35 (Zhai et al., 2015)]. The OR for physical activity (PA) in this study, 0.87 (95% CI 0.81–0.94), closely aligns with prior meta-analyses examining the link between self-reported PA and depression, particularly when contrasting inactive with active adults and older populations [0.90, 95% CI: 0.83–0.98 (Schuch et al., 2019); 0.83, 95% CI: 0.78–0.98 (Guo et al., 2022)]. SB is often underestimated and PA is often overestimated when using self-reported measures (Ryan et al., 2018). Prior meta-analyses and observational studies may have been affected by this, potentially affecting the precision of the depression risk estimation. Recently, Gianfredi et al. (2020) conducted a meta-analysis of the associations between objectively measured PA and incident and prevalent depression, including 37,408 participants, with the overall effect size of depression for the highest vs. the lowest level of PA being −1.16 (95% CI −1.41 to −0.91). In contrast to the previous meta-analysis, which encompassed studies with chronic obstructive pulmonary disease or cancer patients and middle-aged to elderly populations, our analysis focused exclusively on healthy populations, excluding those with patient groups. Furthermore, our study utilized objective metrics for physical activity and sedentary behavior to assess depression risk, offering a more precise and targeted analysis. Furthermore, the ORs from Mendelian randomization studies based on a large sample were 1.01(0.99, 1.04) for i-SB and 0.94(0.91,0.98) for i-PA, which are both more negative than cohort and cross-sectional studies. Therefore, future research should cautiously interpret the association of PA and SB with depression.
Subgroup analysis revealed significant age-related heterogeneity, suggesting age moderates the relationship between physical activity, sedentary behavior and depression among adult and older populations. In elderly populations, these associations were non-significant, with higher ORs than adults, potentially indicating a weakening relationship with age. These findings contrast with Dishman et al. (2021), who found no age difference among the adult population. Gender stratification was limited due to insufficient sex-disaggregated data, and findings from the included study on gender moderation were inconsistent. Hsueh et al. (2020) and others reported reduced depression risk with increased physical activity only in men (OR: 0.75, 95% CI: 0.62–0.91), while Song et al. (2012) found a higher risk only in women (OR: 1.47, 95% CI: 1.12–1.93). Several studies reported non-significant differences in results for sex subgroups, including Hussenoeder et al. (2023). Wemeck et al. (2022) noted potential gender differences, opposing prior findings of stronger associations in women. Further research is needed to clarify these discrepancies and explore underlying mechanisms.
Another main finding in this study was that after adjusting for PA, i-SB did not significantly correlate with an increased risk of depression (1.02:95% CI 1.00–1.04, p = 0.53 > 0.05). The study indicates that PA could reduce the depressive risk associated with SB. Even after accounting for SB, MVPA with a lower OR remained significantly linked to a decreased risk of depression (OR = 0.63; 95% CI, 0.44–0.89; p < 0.05), suggesting that SB does not affect PA’s protective role against depression. These findings are consistent with those of a previous observational study on the risk of depression among adolescents (De Faria et al., 2022) and a meta-analysis on all-cause mortality risk (Rojer et al., 2020). In brief, the link between PA and the risk of depression was independent of SB, and the link between SB and the risk of depression was not independent of PA. The potential mechanism may be that PA promotes health holistically from physiological, psychological, and social perspectives. SB primarily impacts healthy lifestyles in the physiological dimension. A previous study indicated that sufficient PA is significantly associated with lower odds of depressive symptoms across low, moderate, and high levels of SB, suggesting that PA may play a protective role against depressive symptoms in adults even with prolonged SB (Liao et al., 2015). It should also be considered that PA for older adults yields benefits that extend beyond depression, such as the maintenance of functional independence, which might in turn contribute to a reduced likelihood of depression (Du et al., 2015).
The current research primarily employed two objective measurement tools: accelerometers and pedometers, irrespective of the specific models or wear locations. The overall heterogeneity may be attributed to improper installation of measurement components and a lack of standardization among various measurement devices. This problem has also been noted in previous studies, including one conducted by Gianfredi et al. (2020). Montoye et al. (2016) conducted a study that contrasted the accuracy of accelerometers placed on the hips, thighs, and wrists. These results suggest that wrist-worn devices are more sensitive and specific than hip-worn devices for assessing SB and LPA. The device worn on the thigh demonstrated maximum specificity and sensitivity. Therefore, To enable rigorous comparison across studies, it is imperative to use standardized methods and ensure the calibration of devices for evaluating i-SB and i-PA. The comparison of different studies is complicated by the absence of a standardized definition for the assessment of SB and PA, leading to the utilization of varying cut-off values and devices, which are significant sources of heterogeneity. Therefore, to facilitate the comparison of various studies, it is imperative to adopt standardized methodologies and ensure the calibration of different devices when evaluating SB and PA in future research.
Although the exact mechanisms underlying the impact of SB on the adult and older population’s mental health are not fully understood, various possibilities have been suggested. SB, when experienced in isolation, can evoke a sense of loneliness and hence have a detrimental effect on mental well-being (Hoare et al., 2016). Furthermore, the media’s transmission of cultural signals can influence other behaviors associated with mental health, such as eating disorders and aggressive conduct (Primack et al., 2009). Media overexposure is a common occurrence throughout the day and night. Throughout the day, engaging in screen-based activities may replace participation in more beneficial and/or physically active activities, including PA and face-to-face conversation (Ohannessian, 2009). Given this lack of information, research specifically examining the neurological underpinnings of these individuals is particularly intriguing.
Our research holds substantial implications for public mental health. It is imperative to quantify the relationship between internet-based sedentary behavior (i-SB) and internet-based physical activity (i-PA) with depression and to compare the effect sizes for i-SB and i-PA in this meta-analysis to facilitate optimal risk management of physical activity in adults and older populations. It is crucial to clarify this association because international standards for PA (150 min of moderate-intensity PA or 75 min of vigorous-intensity PA) are increasingly emphasizing the need to reduce sedentary time and screen use (WHO, 2020). Our findings underscore the significance of mitigating SB and enhancing PA for mental health. The meta-analysis indicates a bidirectional link between depressive symptoms and both PA and SB, implying that mental health surveillance and support could foster healthier lifestyle decisions. Incorporating structured PA into therapeutic regimens may prove advantageous for individuals experiencing depressive symptoms. Ultimately, while advocating for PA and curbing SB is essential for a balanced lifestyle across all age groups, these measures alone may not suffice to prevent depression. It is advisable to adopt a comprehensive approach that includes early intervention, tactics tailored to each gender, and integration with broader mental health assistance.
Our meta-analysis has several strengths. Primarily, the use of exclusively objective measures of PA and SB represents a strength of this review, as questionnaires may not capture unstructured PA, and adults and older populations are susceptible to overreporting PA and underreporting SB (Ryan et al., 2018; Dyrstad et al., 2014). This study included a large number of participants, with a total of 1,318,687. A key merit of this study is the precise measurement of the relationship between SB, PA, and depression, utilizing objective tools such as accelerometers and pedometers. The analyses, which incorporated cohort studies with diverse follow-up periods, suggest a minimal likelihood of reverse causation. This study incorporated Mendelian randomization research methods to further elucidate the causal relationships between related variables. Furthermore, we performed a conventional binary and dose–response meta-analysis to investigate the impact of these two factors on depression in adults and older populations. This technique effectively utilizes all available data and yields robust statistical results.
The study’s findings should be interpreted with caution due to several limitations. Firstly, the meta-analysis exhibited significant heterogeneity, likely attributable to the diverse studies included. Secondly, the absence of a standardized approach for evaluating i-SB and i-PA across studies hinders direct comparison, as it involves disparate cut-off values, measurement devices, wearing positions, durations, and analytical methods. Lastly, the 33 cross-sectional studies do not permit the establishment of causal inferences, as the relationships cannot be definitively determined. These studies are not equipped to ascertain causal relationships. Consequently, these findings necessitate cautious interpretation. To explore the interplay between PA, SB, and depression risk in adults and older populations, further longitudinal and interventional research is imperative.
5 Conclusion
The association between i-SB and the risk of depression was not consistent with the results of previous self-reported studies. The link between MVPA and the risk of depression was independent of i-SB, whereas the link between i-SB and the risk of depression was not independent of i-PA. We found a linear relationship between SB and the risk of depression and a nonlinear relationship between MVPA or steps per day and depression. The study underscores the necessity of advocating physical activity and curtailing sedentary behavior in forthcoming healthy lifestyle recommendations for adult and older populations.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Author contributions
DW: Conceptualization, Data curation, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing. YZ: Conceptualization, Data curation, Formal analysis, Visualization, Writing – original draft. ZG: Conceptualization, Formal analysis, Methodology, Validation, Writing – review & editing. SL: Conceptualization, Data curation, Formal analysis, Investigation, Project administration, Resources, Software, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the Fundamental Research Funds for the Central Universities of China (CCNU24ZZ117).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2025.1542340/full#supplementary-material
References
Ainsworth, B. E., Haskell, W. L., Herrmann, S. D., Meckes, N., Bassett, D. R., Tudor-Locke, C., et al. (2011). 2011 compendium of physical activities: a second update of codes and MET values. Med. Sci. Sports Exerc. 43, 1575–1581. doi: 10.1249/MSS.0b013e31821ece12
Araki, K., Yasunaga, A., Shibata, A., Hattori, K., Honma, R., Sato, N., et al. (2022). Cross-sectional associations between replacing sedentary behavior with physical activity by accelerometer-measured and depression in frail older adults: an Isotemporal substitution approach. Jpn. J. Phys. Fitness Sports Med. 71, 185–192. doi: 10.7600/JSPFSM.71.185
Asai, Y., Obayashi, K., Oume, M., Ogura, M., Takeuchi, K., Yamagami, Y., et al. (2018). Farming habit, light exposure, physical activity, and depressive symptoms. A cross-sectional study of the HEIJO-KYO cohort. J. Affect. Disord. 241, 235–240. doi: 10.1016/j.jad.2018.08.003
Ba, H., Zhang, L., Peng, H., He, X., and Wang, Y. (2024). Causal links between sedentary behavior, physical activity, and psychiatric disorders: a Mendelian randomization study. Ann. General Psychiatry 23:9. doi: 10.1186/s12991-024-00495-0
Bae, S., Jang, M., Kim, G. M., Yang, J. G., Thapa, N., Park, H. J., et al. (2023). Nonlinear associations between physical function, physical activity, sleep, and depressive symptoms in older adults. J. Clin. Med. 12, 6009–6021. doi: 10.3390/jcm12186009
Biddle, S. J. H., Henson, J., Davies, M. J., Khunti, K., Sutton, S., Yates, T., et al. (2021). Device-assessed total and prolonged sitting time: associations with anxiety, depression, and health-related quality of life in adults. J. Affect. Disord. 287, 107–114. doi: 10.1016/j.jad.2021.03.037
Blodgett, J. M., Mitchell, J. J., Stamatakis, E., Chastin, S., and Hamer, M. (2023). Associations between the composition of daily time spent in physical activity, sedentary behaviour and sleep and risk of depression: compositional data analyses of the 1970 British cohort study. J. Affect. Disord. 320, 616–620. doi: 10.1016/j.jad.2022.09.110
Bustamante, E. E., Wilbur, J., Marquez, D. X., Fogg, L., Staffileno, B. A., and Manning, A. (2013). Physical activity characteristics and depressive symptoms in older Latino adults. Ment. Health Phys. Act. 6, 69–77. doi: 10.1016/j.mhpa.2013.05.001
Casals, C., Corral-Pérez, J., Ávila-Cabeza-de-Vaca, L., González-Mariscal, A., Carrión-Velasco, Y., Rodríguez-Martínez, M. C., et al. (2024). Exploring the interplay of frailty, physical function, physical activity, nutritional status, and their association with quality of life and depressive symptoms in older adults with the frailty phenotype. Int. J. Geriatr. Psychiatry 39, e6078–e6014. doi: 10.1002/gps.6078
Casanova, F., O'Loughlin, J., Karageorgiou, V., Beaumont, R. N., Bowden, J., Wood, A. R., et al. (2023). Effects of physical activity and sedentary time on depression, anxiety and well-being: a bidirectional Mendelian randomisation study. BMC Med. 21:501. doi: 10.1186/s12916-023-03211-z
Chan, L. L. Y., Brodie, M. A., and Lord, S. R. (2023). Prediction of incident depression in middle-aged and older adults using digital gait biomarkers extracted from large-scale wrist sensor data. J. Am. Med. Dir. Assoc. 24, 1106–1113.e11. doi: 10.1016/j.jamda.2023.04.008
Chan, L. L. Y., van Schooten, K. S., Lord, S. R., Delbaere, K., and Brodie, M. (2022). Short daily-life walking bouts and poor self-reported health predict the onset of depression in community-dwelling older people: a 2-year longitudinal cohort study. J. Am. Med. Dir. Assoc. 23, 1242–1247.e3. doi: 10.1016/j.jamda.2021.12.042
Chen, J., Lai, T. F., Lin, L. J., Park, J. H., and Liao, Y. (2023). Is overall and timing-specific physical activity associated with depression in older adults? Front. Public Health 11:1241170. doi: 10.3389/fpubh.2023.1241170
Choi, K. W., Chen, C. Y., Stein, M. B., Klimentidis, Y. C., Wang, M. J., Koenen, K. C., et al. (2019). Assessment of bidirectional relationships between physical activity and depression among adults: a 2-sample Mendelian randomization study. JAMA Psychiatry 76, 399–408. doi: 10.1001/jamapsychiatry.2018.4175
De Faria, F. R., Barbosa, D., Howe, C. A., Canabrava, K. L. R., Sasaki, J. E., and Dos Santos Amorim, P. R. (2022). Time-use movement behaviors are associated with scores of depression/anxiety among adolescents: A compositional data analysis. Mendeley Data 17:e0279401. doi: 10.1016/j.jpeds.2016.08.104
Del Pozo Cruz, B., Alfonso-Rosa, R. M., McGregor, D., Chastin, S. F., Palarea-Albaladejo, J., and Del Pozo Cruz, J. (2020). Sedentary behaviour is associated with depression symptoms: compositional data analysis from a representative sample of 3233 US adults and older adults assessed with accelerometers. J. Affect. Disord. 265, 59–62. doi: 10.1016/j.jad.2020.01.023
Denche-Zamorano, A., Rodriguez-Redondo, Y., Barrios-Fernandez, S., Mendoza-Munoz, M., Rojo-Ramos, J., Garcia-Gordillo, M. A., et al. (2023). Depression, anxiety and antidepressants and anxiolytics use in Spanish informal caregivers according to the physical activity frequency: EHSS 2014-2020. Healthcare (Basel) 11, 990–1002. doi: 10.3390/healthcare11070990
Dennison, C. A., Legge, S. E., Bracher-Smith, M., Menzies, G., Escott-Price, V., Smith, D. J., et al. (2021). Association of genetic liability for psychiatric disorders with accelerometer-assessed physical activity in the UK biobank. PLoS One 16, 1–14. doi: 10.1371/journal.pone.0249189
Dhakal, A., Kurisu, K., Park, S., and Yoshiuchi, K. (2023). Association of psychosocial factors with physical activity among Japanese adults aged 65 and older: a 6-year repeated cross-sectional study from the Nakanojo Study. BioPsychoSocial Medicine. 17, 32. doi: 10.1186/s13030-023-00289-y
Dishman, R. K., McDowell, C. P., and Herring, M. P. (2021). Customary physical activity and odds of depression: a systematic review and meta-analysis of 111 prospective cohort studies. Br. J. Sports Med. 55, 926–934. doi: 10.1136/bjsports-2020-103140
Du, W.-J., Tan, J.-P., Yi, F., Zou, Y.-M., Gao, Y., Zhao, Y.-M., et al. (2015). Physical activity as a protective factor against depressive symptoms in older Chinese veterans in the community: result from a national cross-sectional study. Neuropsychiatr. Dis. Treat. 11, 803–813. doi: 10.2147/NDT.S80295
Dyrstad, S., Hansen, B., Holme, I., and Anderssen, S. (2014). Comparison of self-reported versus accelerometer-measured physical activity. Med. Sci. Sports Exerc. 46, 99–106. doi: 10.1249/MSS.0b013e3182a0595f
Eriksson, M., Naas, S., Berginstrom, N., Nordstrom, P., Hansson, P., and Nordstrom, A. (2020). Sedentary behavior as a potential risk factor for depression among 70-year-olds. J. Affect. Disord. 263, 605–608. doi: 10.1016/j.jad.2019.11.035
Felez-Nobrega, M., Werneck, A. O., El Fatouhi, D., de Luca, K., Islam, S. M. S., and Franzese, F. (2023). Device-based physical activity and late-life depressive symptoms: an analysis of influential factors using share data. J. Affect. Disord. 322, 267–272. doi: 10.1016/j.jad.2022.11.006
Gianfredi, V., Blandi, L., Cacitti, S., Minelli, M., Signorelli, C., Amerio, A., et al. (2020). Depression and objectively measured physical activity: a systematic review and Meta-analysis. Int. J. Environ. Res. Public Health. 17, 3738–3758. doi: 10.3390/ijerph17103738
Guo, Z., Li, R., and Lu, S. (2022). Leisure-time physical activity and risk of depression: a dose-response meta-analysis of prospective cohort studies. Medicine (Baltimore) 101:e29917. doi: 10.1097/MD.0000000000029917
Heinz, M. V., Price, G. D., Ruan, F., Klein, R. J., Nemesure, M., Lopez, A., et al. (2022). Association of selective serotonin reuptake inhibitor use with abnormal physical movement patterns as detected using a piezoelectric accelerometer and deep learning in a nationally representative sample of noninstitutionalized persons in the US. JAMA Netw. Open 5, –e225403. doi: 10.1001/jamanetworkopen.2022.5403
Herbolsheimer, F., Ungar, N., and Peter, R. (2018). Why is social isolation among older adults associated with depressive symptoms? The mediating role of out-of-home physical activity. Int. J. Behav. Med. 25, 649–657. doi: 10.1007/s12529-018-9752-x
Higgins, J. P., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M. J., et al. (2019). Cochrane handbook for systematic reviews of interventions. JohnWeiley & Sons: Chichester, UK.
Ho, F. K., Petermann-Rocha, F., Parra-Soto, S., Boonpor, J., Gill, J. M. R., Gray, S. R., et al. (2022). Device-measured physical activity and incident affective disorders. BMC Med. 20:290. doi: 10.1186/s12916-022-02484-0
Hoare, E., Milton, K., Foster, C., and Allender, S. (2016). The associations between sedentary behaviour and mental health among adolescents: a systematic review. Int. J. Behav. Nutr. Phys. Act. 13:108. doi: 10.1186/s12966-016-0432-4
Hollands, L., Lambert, J., Price, L., Powell, D., and Greaves, C. (2020). Ecological momentary assessment of mood and physical activity in people with depression. J. Affect. Disord. 271, 293–299. doi: 10.1016/j.jad.2020.03.085
Hsiao, C., Hsueh, M. C., and Liao, Y. (2022). Associations between objectively measured sedentary behavior patterns and depressive symptoms in older adults: a cross sectional study. Ment. Health Phys. Act. 23:100471. doi: 10.1016/j.mhpa.2022.100471
Hsueh, M. C., Stubbs, B., Lai, Y. J., Sun, C. K., Chen, L. J., and Ku, P. W. (2020). A dose response relationship between accelerometer assessed daily steps and depressive symptoms in older adults: a two-year cohort study. Age Ageing 50, 519–526. doi: 10.1093/ageing/afaa162
Hussenoeder, F. S., Conrad, I., Pabst, A., Engel, C., Zachariae, S., Zeynalova, S., et al. (2023). Physical activity and mental health: the connection between step count and depression, anxiety and quality of sleep. Psychol. Health Med. 28, 2419–2429. doi: 10.1080/13548506.2022.2159453
Iob, E., Pingault, J.-B., Munafò, M. R., Stubbs, B., Gilthorpe, M. S., Maihofer, A. X., et al. (2023). Testing the causal relationships of physical activity and sedentary behaviour with mental health and substance use disorders: a Mendelian randomisation study. Mol. Psychiatry 28, 3429–3443. doi: 10.1038/s41380-023-02133-9
King, W. C., Hinerman, A. S., White, G. E., Courcoulas, A. P., and Belle, S. H. (2022). Associations between physical activity and changes in depressive symptoms and health-related quality of life across 7 years after roux-en-Y gastric bypass surgery: a multicenter prospective cohort study. Ann. Surg. 276, e777–e783. doi: 10.1097/sla.0000000000004652
Kirschner, M., Golsteijn, R. H. J., van der Wurff, I. S. M., Savelberg, H. H. C. M., and de Groot, R. H. M. (2022). The role of physical activity behavior in the mental wellbeing of vocational education and training students: the PHIT2LEARN study. Front. Educ. 7:839848. doi: 10.3389/feduc.2022.839848
Konopka, M. J., Köhler, S., Stehouwer, C. D. A., Schaper, N. C., Henry, R. M. A., van der Kallen, C. J. H., et al. (2022). Accelerometer-derived sedentary time and physical activity and the incidence of depressive symptoms – the Maastricht study. Psychol. Med. 52, 2786–2793. doi: 10.1017/S0033291720004924
Ku, P. W., Steptoe, A., Liao, Y., Sun, W. J., and Chen, L. J. (2018). Prospective relationship between objectively measured light physical activity and depressive symptoms in later life. Int. J. Geriatr. Psychiatry 33, 58–65. doi: 10.1002/gps.4672
Larisch, L. M., Kallings, L. V., Hagströmer, M., Desai, M., Rosen, P. V., and Blom, V. (2020). Associations between 24 h movement behavior and mental health in office workers. Int. J. Environ. Res. Public Health 17, 1–20. doi: 10.3390/ijerph17176214
Lee, H., Lee, J. A., Brar, J. S., Rush, E. B., and Jolley, C. J. (2014). Physical activity and depressive symptoms in older adults. Geriatr. Nurs. 35, 37–41. doi: 10.1016/j.gerinurse.2013.09.005
Li, Y. M., Konstabel, K., Mottus, R., and Lemola, S. (2022). Temporal associations between objectively measured physical activity and depressive symptoms: an experience sampling study. Front. Psych. 13:920580. doi: 10.3389/fpsyt.2022.920580
Liao, Y., Shibata, A., Ishii, K., and Oka, K. (2015). Independent and combined associations of physical activity and sedentary behavior with depressive symptoms among Japanese adults. Int. J. Behav. Med. 23, 402–409. doi: 10.1007/s12529-015-9484-0
Loprinzi, P. D. (2013). Objectively measured light and moderate-to-vigorous physical activity is associated with lower depression levels among older US adults. Aging Ment. Health 17, 801–805. doi: 10.1080/13607863.2013.801066
Loprinzi, P. D., and Mahoney, S. (2014). Concurrent occurrence of multiple positive lifestyle behaviors and depression among adults in the United States. J. Affect. Disord. 165, 126–130. doi: 10.1016/j.jad.2014.04.073
Maher, J. P., Huh, J., Intille, S., Hedeker, D., and Dunton, G. F. (2018). Greater variability in daily physical activity is associated with poorer mental health profiles among obese adults. Ment. Health Phys. Act. 14, 74–81. doi: 10.1016/j.mhpa.2018.02.004
McKercher, C. M., Schmidt, M. D., Sanderson, K. A., Patton, G. C., Dwyer, T., and Venn, A. J. (2009). Physical activity and depression in young adults. Am. J. Prev. Med. 36, 161–164. doi: 10.1016/j.amepre.2008.09.036
Michalak, J., Niemeyer, H., Tschacher, W., Baumann, N., Chi Zhang, X., and Adolph, D. (2022). Subjective and objective measures of activity in depressed and non-depressed individuals in everyday life. Journal of experimental. Psychopathology 13, 1–8. doi: 10.1177/20438087221092582
Montoye, A. H. K., Pivarnik, J. M., Mudd, L. M., Biswas, S., and Pfeiffer, K. A. (2016). Validation and comparison of accelerometers worn on the hip, thigh, and wrists for measuring physical activity and sedentary behavior. AIMS Public Health 3, 298–312. doi: 10.3934/publichealth.2016.2.298
Morres, I. D., Hatzigeorgiadis, A., Krommidas, C., Comoutos, N., Sideri, E., Ploumpidis, D., et al. (2019). Objectively measured physical activity and depressive symptoms in adult outpatients diagnosed with major depression. Clin. Perspect. Psychiatry Res 280:112489. doi: 10.1016/j.psychres.2019.112489
Mossavar-Rahmani, Y., Lin, J., Pan, S., Song, R. J., Xue, X., Spartano, N. L., et al. (2023). Characterizing longitudinal change in accelerometry-based moderate-to-vigorous physical activity in the Hispanic community health study/study of Latinos and the Framingham heart study. BMC Public Health 23:1614. doi: 10.1186/s12889-023-16442-9
Murray, R. M., Dore, I., Sabiston, C. M., Michael, F., and O'Loughlin, J. L. (2023). A time compositional analysis of the association between movement behaviors and indicators of mental health in young adults. Scand. J. Med. Sci. Sports 33, 2598–2607. doi: 10.1111/sms.14471
Ohannessian, C. M. (2009). Media use and adolescent psychological adjustment: an examination of gender differences. J. Child Fam. Stud. 18, 582–593. doi: 10.1007/s10826-009-9261-2
Okely, J. A., Cukic, I., Shaw, R. J., Chastin, S. F., Dall, P. M., Deary, I. J., et al. (2019). Positive and negative well-being and objectively measured sedentary behaviour in older adults: evidence from three cohorts. BMC Geriatr. 19:28. doi: 10.1186/s12877-019-1026-1
Park, J., Nam, H. K., and Cho, S. I. (2024). Association between accelerometer-derived physical activity and depression: a cross-sectional study using isotemporal substitution analysis. BMJ Open 14:e078199. doi: 10.1136/bmjopen-2023-078199
Primack, B. A., Swanier, B., Georgiopoulos, A. M., Land, S. R., and Fine, M. J. (2009). Association between media use in adolescence and depression in young adulthood: a longitudinal study. Arch. Gen. Psychiatry 66, 181–188. doi: 10.1001/archgenpsychiatry.2008.532
Rautio, N., and Seppänen, M. (2024). Associations between neighbourhood characteristics, physical activity and depressive symptoms: the Northern Finland Birth Cohort 1966 Study. European Journal of Public Health. 34, 114–120. doi: 10.1093/eurpub/ckad215
Rethorst, C. D., Moncrieft, A. E., Gellman, M. D., Arredondo, E. M., Buelna, C., Castañeda, S. F., et al. (2017). Isotemporal analysis of the Association of Objectively Measured Physical Activity with Depressive Symptoms: results from Hispanic community health study/study of Latinos (HCHS/SOL). J. Phys. Act. Health 14, 733–739. doi: 10.1123/jpah.2016-0648
Rojer, A. G. M., Ramsey, K. A., Trappenburg, M. C., van Rijssen, N. M., Otten, R. H. J., Heymans, M. W., et al. (2020). Instrumented measures of sedentary behaviour and physical activity are associated with mortality in community-dwelling older adults: a systematic review, meta-analysis and meta-regression analysis. Ageing Res. Rev. 61:101061. doi: 10.1016/j.arr.2020.101061
Ryan, D. J., Wullems, J. A., Stebbings, G. K., Morse, C. I., Stewart, C. E., and Onambele-Pearson, G. L. (2018). Reliability and validity of the international physical activity questionnaire compared to calibrated accelerometer cut-off points in the quantification of sedentary behaviour and physical activity in older adults. PLoS One 13:e0195712. doi: 10.1371/journal.pone.0195712
Schuch, F. B., Stubbs, B., Meyer, J., Heissel, A., Zech, P., Vancampfort, D., et al. (2019). Physical activity protects from incident anxiety: a meta-analysis of prospective cohort studies. Depress. Anxiety 36, 846–858. doi: 10.1002/da.22915
Siwa, M., Kulis, E., Banik, A., Szczuka, Z., Boberska, M., Wietrzykowska, D., et al. (2023). Associations between depressive symptoms and sedentary behaviors in dyads: longitudinal crossover effects. Ment. Health Phys. Act. 24:100501. doi: 10.1016/j.mhpa.2022.100501
Song, M. R., Lee, Y. S., Baek, J. D., and Miller, M. (2012). Physical activity status in adults with depression in the National Health and nutrition examination survey, 2005-2006. Public Health Nurs. 29, 208–217. doi: 10.1111/j.1525-1446.2011.00986.x
Tremblay, M. S., Aubert, S., Barnes, J. D., Saunders, T. J., Carson, V., Latimer-Cheung, A. E., et al. (2017). Sedentary behavior research network (SBRN) – terminology consensus project process and outcome. Int. J. Behav. Nutr. Phys. Act. 14:75. doi: 10.1186/s12966-017-0525-8
Tully, M. A., McMullan, I., and Blackburn, N. E. (2020). Sedentary behavior, physical activity, and mental health in older adults: An isotemporal substitution model. Scand. J. Med. Sci. Sports. 265, 538–544. doi: 10.1016/j.jad.2019.11.088
Vallance, J. K., Winkler, E. A. H., Gardiner, P. A., Healy, G. N., Lynch, B. M., and Owen, N. (2011). Associations of objectively-assessed physical activity and sedentary time with depression: NHANES (2005–2006). Prev. Med. 53, 284–288. doi: 10.1016/j.ypmed.2011.07.013
Wang, X., Li, Y., and Fan, H. (2019). The associations between screen time-based sedentary behavior and depression: a systematic review and meta-analysis. BMC Public Health 19:1524. doi: 10.1186/s12889-019-7904-9
Wells, G.A., Shea, B., O’Connell, D., Peterson, J., Welch, V., Losos, M., et al. (2000). The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. Available online at: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (Accessed July 22, 2024).
Wemeck, A. O., Kandola, A., Tebar, W. R., Silva, D. R., Stubbs, B., and Christofaro, D. G. D. (2022). Does physical activity moderate the association between device-measured sedentary time patterns and depressive symptoms in adults? Brazil. J. Psychiatry 44, 584–589. doi: 10.47626/1516-4446-2022-2533
World Health Organization., (2017). Depression and other common mental disorders: global health estimates. Available online at: https://www.who.int/publications/i/item/depression-global-health-estimates (Accessed July 15, 2024)
World Health Organization., (2020). Global recommendations on physical activity for health. Available online at: https://www.who.int/publications/i/item/9789241599979 (Accessed July 15, 2024).
Xu, C., and Doi, S. A. R. (2018). The robust error meta-regression method for dose-response meta-analysis. Int. J. Evid. Based Healthc. 16, 138–144. doi: 10.1097/xeb.0000000000000132
Yasunaga, A., Shibata, A., Ishii, K., Koohsari, M. J., and Oka, K. (2018). Cross-sectional associations of sedentary behaviour and physical activity on depression in Japanese older adults: an isotemporal substitution approach. BMJ Open 8:e022282. doi: 10.1136/bmjopen-2018-022282
Zhai, L., Zhang, Y., and Zhang, D. (2015). Sedentary behaviour and the risk of depression: a meta-analysis. Br. J. Sports Med. 49, 705–709. doi: 10.1136/bjsports-2014-093613
Zhang, T., Dong, S., and Zhou, Z. (2015). The advanced meta-analysis method-based on stata. Shanghai: Fudan University Press, 220–232.
Zhang, D., Pettee Gabriel, K., Sidney, S., Sternfeld, B., Jacobs, D. Jr., and Whitaker, K. M. (2021). Longitudinal bidirectional associations of physical activity and depressive symptoms: the CARDIA study. Prev. Med. Rep. 23:101489. doi: 10.1016/j.pmedr.2021.101489
Zhou, Q., Guo, C., Yang, X., and He, N. (2023). Dose-response association of total sedentary behaviour and television watching with risk of depression in adults: a systematic review and meta-analysis. J. Affect. Disord. 324, 652–659. doi: 10.1016/j.jad.2022.12.098
Keywords: sedentary behavior, physical activity, accelerometry, depression, adults, older populations
Citation: Wang D, Zhang Y, Guo Z and Lu S (2025) Sedentary behavior and physical activity are associated with risk of depression among adult and older populations: a systematic review and dose–response meta-analysis. Front. Psychol. 16:1542340. doi: 10.3389/fpsyg.2025.1542340
Edited by:
Diogo Monteiro, Politécnico de Leiria, PortugalCopyright © 2025 Wang, Zhang, Guo and Lu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Songtao Lu, THVzb25ndGFvQHd1c3QuZWR1LmNu