Abstract
This research examines the effects of music therapy participation on mental health among Chinese university students, focusing on the mediating role of self-evaluation and the moderating role of gender. A moderated mediation model was proposed to explain how and for whom music therapy exerts its benefits. A cross-sectional survey was conducted with 1,000 students recruited through multi-stage random sampling from four universities across China. Participants completed the Music Therapy Participation Scale (MTPS), the Self-Evaluation Scale (SES), and the Mental Health Status Questionnaire (MHS-Q). Data were analyzed using structural equation modeling (SEM). Results indicated that higher music therapy participation was significantly associated with better mental health (β = −0.30, p < 0.001). Self-evaluation partially mediated this relationship (indirect effect β = −0.11, 95% CI [−0.14, −0.07]). Gender moderated the direct path, with a stronger effect observed for female students (interaction β = 0.09, p = 0.002). The findings suggest that music therapy improves mental health both directly and through enhanced self-evaluation, with gender shaping the strength of the direct benefit. These insights support the integration of tailored, gender-sensitive music therapy programs into university mental health services to promote student well-being.
1 Introduction
Mental health disorders are an essential issue in the world as the prevalence has been on the increase among the youths and young adult population (World Health Organization [WHO], 2022). A university student population is one of the most vulnerable groups that must manage academic stress, shifts in social spheres, and identity formation (Auerbach et al., 2018). Epidemiological surveys indicate that the problem is widespread among students, ranging from 14% to 22% in the West, and therefore the issue should be approached in its context (Stallman, 2010; Cuijpers et al., 2019).
The problem of mental health among university students is a burning issue in China. As stated, the issue rate was rather average a few years ago (Chen et al., 2013). However, the final surveys show an upward movement with a significant change. According to some of the studies, even in China, as many as 38% of the population of university students have mental health problems, and the percentage of the female population is even higher (Li et al., 2021). Such inconsistencies between studies can be explained by differences in measurement instruments and sampling, as well as by changes in the socio-academic environment over time (Liu et al., 2022). This rising trend demands viable, available, and effective intervention measures.
Music therapy, which is considered the use of musical interventions to achieve therapeutic objectives through clinical and evidence-based practices, has been deemed a safe and effective non-pharmacological methodology (Shultis and Schreibman, 2020). It can help reduce symptoms of anxiety and depression and enhance the overall quality of life across diverse populations, and meta-analytic reviews support these assertions (Aalbers et al., 2017; Leubner and Hinterberger, 2017; de Witte et al., 2020). Nevertheless, the process by which music therapy operates, primarily in the Chinese cultural and educational context, remains unexplored. In addition, as in the case of sustainable and inclusive interventions presented in other sources devoted to the topic, individualization and situational appropriateness of the specified programs, whether in the context of the educational environment (Roldan-Canovas et al., 2024) or the city’s well-being (Ortiz Diaz and Abbas, 2024), are the determinants of the success of any interventions.
The research presents a theoretical framework and applies it to hypothesis testing to understand how and to whom music therapy enhances mental health. Based on existing theories, we assume that self-evaluation, an essential part of self-concept, is the primary psychological process (mediator) that transforms musical engagement into improved mental health (Fancourt and Finn, 2019). At the same time, we test the question of whether gender should be influential (moderate) on the effectiveness of the direct action of music therapy, taking into consideration possible biological, psychosocial, and cultural conditions that can determine the difference in responses (Chen and Zhou, 2022; Tran et al., 2024). Elucidating these pathways, the research is expected to inform the design of more specific and compelling mental health promotion methods for Chinese university students.
2 Theoretical framework and hypotheses
2.1 Music therapy and mental health: a multi-theoretical perspective
2.1.1 Neurobiological theory
Music engages a broad bilateral network of brain areas associated with emotion, memory, and rewards, and can regulate autonomic functions (Koelsch, 2014; Zatorre, 2018). Such neural activity can promote neural plasticity, balance stress hormone levels (e.g., cortisol), and improve heart rate variability, thereby decreasing physiological arousal and increasing emotional well-being (Bernardi et al., 2006; Chanda and Levitin, 2013; Trost and Frühholz, 2021).
2.1.2 Psychological theory
Music can be considered one of the best means of emotional manipulation and expression (Juslin and Västfjäll, 2008; Carlson et al., 2021). The negative affective states, anxiety and sadness, are reduced because of listening to music and the music involvement. It is possible to enhance mental health through mechanisms such as mood congruence, cognitive distraction, and the evocation of positive affect.
2.1.3 Sociological theory
Music is commonly communal. Music-making in the group may result in social bonding, loneliness, social anxiety, and perceived social support, all of which are vital toward the preservation of mental health (Pearce et al., 2015; Williams et al., 2021). It aligns with studies highlighting the importance of social connectedness and supportive conditions in reducing stress and burnout (Tran et al., 2024).
2.2 The mediating role of self-evaluation
Self-evaluation, which includes constructs such as self-esteem and self-efficacy, is the subjective assessment of personal value and potential (Rosenberg, 1965). It is a strong predictor of mental health, in which low self-evaluation is a predictive risk factor of depression and anxiety (Sowislo and Orth, 2013; Orth and Robins, 2022). We suggest that music therapy improves self-assessment in a variety of ways: (a) learning musical skills will help in developing a sense of competence and self-efficacy (Geeves et al., 2020); (b) aesthetic engagement and expressing artistic ideas can increase self-worth; and (c) positive feedback in a therapeutic or group context will validate the individual (MacDonald et al., 2021). Such enhanced self-assessment then leads to improved mental health. Therefore, self-evaluation is theorized to serve as an intermediary.
2.3 The moderating role of gender
The prevalence and response of mental health to interventions vary between genders. Psychological distress is frequently reported among female university students in China, which may be explained by the combination of biological factors, gender-specific social norms, and peculiarities of stressors (Li et al., 2021; Chen and Zhou, 2022). Also, studies indicate that women might also be more emotionally responsive and receptive to aesthetic and interpersonal stimuli, such as those found in music (Linnemann et al., 2015; Park et al., 2021). Thus, we also hypothesize that the effect of gender would mediate the association between music therapy and mental health, with a stronger association among female students.
2.4 Research hypotheses
H1: Mental health is positively linked to music therapy participation.
H2: Self-assessment has a positive relationship with mental health.
H3: Self-assessment mediates the connection between engagement in music therapy and mental well-being.
H4: There is a moderator effect by gender on the direct association between music therapy attendance and mental health, whereby the correlation is higher amongst female students.
3 Research methods
3.1 Participants and procedure
A cross-sectional study was done in September 2025. Participants were recruited using the multi-stage random sampling method (Kish, 1965). First, four universities in the various geographical regions of China (East, South, West, North) were randomly selected from a national list. Second, across each university, academic departments were randomly selected. Finally, based on the student rosters of assigned departments, individual students were randomly invited to participate. This strategy aimed to improve representativeness while accounting for the practical limitations of a nationwide random sample (Babbie, 2020).
The first web survey produced 1020 responses. Twenty responses were excluded: 12 for completing the study for less than 1/3 of the median time (indicating inattentive responding), and 8 for identical responses to all of the items. The final sample was 1,000 valid responses (98.04% retention rate). A priori power analysis in G*Power 3.1 with a linear multiple regression (fixed model, R2 increase), effect size, f2 = 0.05, α = 0.05, and the power of 1 −β = 0.95 showed a total sample size of 758 (Faul et al., 2009). Our final sample was above this requirement. All participants gave electronic informed consent. This study was approved by the Ethics Committee of Hanshan Normal University (Approval No. 2025111901).
3.2 Measures
All the instruments were Chinese versions that had been validated and were reliable among the required populations.
3.2.1 There will be participation in music therapy (independent variable)
Participation in music therapy will be assessed using a 12-item Music Therapy Participation Scale (MTPS), which was developed specifically for the present study in accordance with AMTA guidelines (2020). Items assessed frequency and depth of engagement in structured music-based activities with therapeutic intent over the past 6 months (e.g., “I have participated in group music therapy sessions,” “I use prescribed music listening for relaxation”). Responses were on a 5-point Likert scale (1 = Never, 5 = Very Often). Higher scores indicated greater participation. The scale demonstrated excellent internal consistency in this sample (Cronbach’s α = 0.92).
3.2.2 Self-evaluation (mediator)
Measured using the 10-item Self-Evaluation Scale (SES), a widely used Chinese adaptation of the Rosenberg Self-Esteem Scale (Wang and Zhang, 2011). Items (e.g., “On the whole, I am satisfied with myself”) are rated on a 4-point Likert scale (1 = Strongly Disagree, 4 = Strongly Agree). Higher scores indicate more positive self-evaluation. Cronbach’s α was 0.86.
3.2.3 Mental health (dependent variable)
Evaluated based on 12 questions on the Mental Health Status Questionnaire (MHS-Q), a screening instrument that is validated to be used on Chinese young adults (Chen and Zheng, 2021). They will include the past 2 weeks with the symptoms of depression, anxiety, and stress. Responses will be on a 4-point Likert scale (1 = Never, 4 = Almost Always). Primary analysis was performed using a continuous total score, with higher scores indicating poorer mental health (i.e., more symptoms). A cut-off score of ≥24 (including the study in the validation sample) and above (which falls in the top quartile of the score range) was adopted for descriptive purposes to determine the “probable cases” (Chanda and Levitin, 2013; Chen and Zheng, 2021). This yielded a case prevalence of 25.5% in our sample, which is similar to recent epidemiological estimates. Cronbach’s α was 0.88.
3.2.4 Demographic variables
Information regarding gender (male/female), age, annual family income (categorized as Low: <¥50,000; Medium: ¥50,000–150,000; High: >¥150,000), and parents’ marital status (married/not married) was collected.
3.3 Data analysis
Data were analyzed using the software SPSS 27.0 and AMOS 27.0. First, descriptive statistics and bivariate Pearson correlations were calculated. To test H1 and H2, an initial linear regression analysis was performed. To examine the fitted integrated moderated mediation model (H3 and H4), we used SEMs with the maximum likelihood estimation (Kline, 2023). The model incorporated music therapy as a predictor variable, self-evaluation as a mediator variable, mental health (continuous score) as an outcome variable, and gender as a moderator of the direct relationship of music therapy to mental health. Model fit was assessed using the χ2/df ratio (<3), CFI (>0.95), TLI (>0.95), and RMSEA (<0.06) (Hu and Bentler, 1999). The significance of the indirect effect (mediation) was tested using bias-corrected bootstrap confidence intervals (5,000 samples) (Hayes, 2022). A significant interaction term (Music Therapy × Gender) would indicate moderation, followed by a simple slope analysis to probe the effect at each gender level.
4 Results
4.1 Descriptive statistics and sample characteristics
A cross-sectional survey was administered to a final sample of 1,000 Chinese university students, recruited via a multi-stage random sampling procedure. First, four universities were randomly selected from different geographical regions of China (East, South, West, North). At each university, several academic departments were chosen at random, and then individual students were randomly selected from the lists of those departments. There were 1,020 respondents in the first pool. Ten responses were dropped: 12 because their time spent in completing those responses was less than a third of the median time (indicating that they were not paying attention), and 8 because they gave the same response to all items (suggesting that they were patterned responding). This left a final valid sample of 1,000 participants (retention rate: 98.04%).
As seen in Table 1, the mean age of the sample was 20.02 years (SD = 1.05), and the gender distribution was nearly equal (51.4% female). The probable mental health problems were determined based on the MHS-Q cutoff score (≥24) and affected 25.5% of cases (n = 255). The chi-square tests demonstrated significant correlations of the status of the mental health problems with several key variables including gender (χ2 = 11.89, *p* < 0.001, with more women having the issues), level of music therapy participation (χ2 = 55.35, *p* < 0.001), level of self-evaluation (χ2 = 19.58, *p* = 0.036) and the category of family income (χ2 = 6.64, *p* = 0.036). Parental marital status and age had no significant correlation with the status of mental health problems in this analysis.
TABLE 1
| Item | Category | All participants (n = 1000) n (%) | No probable MH problems (n = 745) n (%) | Probable MH problems (n = 255) n (%) | χ2 | *p* |
|---|---|---|---|---|---|---|
| Gender | Male | 486 (48.6) | 385 (51.7) | 101 (39.6) | 11.892 | 0.001 |
| Female | 514 (51.4) | 360 (48.3) | 154 (60.4) | |||
| Age group | 18–20 years | 721 (72.1) | 531 (71.3) | 190 (74.5) | 10.832 | 0.093 |
| 21–26 years | 279 (27.9) | 214 (28.7) | 65 (25.5) | |||
| Mean age (SD) | 20.02 (1.05) | 20.06 (1.04) | 19.89 (1.07) | – | – | |
| Family income | Low (<¥50k/year) | 442 (44.2) | 321 (43.1) | 121 (47.5) | 6.642 | 0.036* |
| Medium (¥50–150k/year) | 460 (46.0) | 357 (47.9) | 103 (40.4) | |||
| High (>¥150k/year) | 98 (9.8) | 67 (9.0) | 31 (12.2) | |||
| Parents’ marital status | Married | 935 (93.5) | 700 (94.0) | 235 (92.2) | 1.223 | 0.269 |
| Not married | 65 (6.5) | 45 (6.0) | 20 (7.8) | |||
| Music therapy participation | Low (Quartile 1) | 250 (25.0) | 220 (29.5) | 30 (11.8) | 55.350 | <0.001 |
| Moderate (Q2 & Q3) | 500 (50.0) | 367 (49.3) | 133 (52.2) | |||
| High (Quartile 4) | 250 (25.0) | 158 (21.2) | 92 (36.1) | |||
| Self-evaluation level | Low (Quartile 1) | 250 (25.0) | 202 (27.1) | 48 (18.8) | 19.584 | <0.001 |
| Moderate (Q2 & Q3) | 500 (50.0) | 377 (50.6) | 123 (48.2) | |||
| High (Quartile 4) | 250 (25.0) | 166 (22.3) | 84 (32.9) |
Sample demographic characteristics (N = 1000).
*p < 0.05. Bold values indicate statistically significant differences or coefficients (p < 0.05).
4.2 Reliability and validity
All measurement instruments demonstrated good to excellent reliability and structural validity in the current sample (Table 2). Factor loadings for all items exceeded 0.60, Cronbach’s α values were above 0.70, and KMO values surpassed 0.75, indicating the suitability of the data for factor analysis and subsequent modeling.
TABLE 2
| Variable | Item | Factor loading | Cronbach’s α | KMO |
|---|---|---|---|---|
| Music therapy (MTPS) | MT1 | 0.72 | 0.92 | 0.91 |
| MT2 | 0.78 | |||
| MT3 | 0.81 | |||
| MT4 | 0.84 | |||
| MT5 | 0.86 | |||
| MT6 | 0.85 | |||
| MT7 | 0.82 | |||
| MT8 | 0.79 | |||
| Self-evaluation (SES) | SE1 | 0.69 | 0.86 | 0.80 |
| SE2 | 0.75 | |||
| SE3 | 0.73 | |||
| SE4 | 0.80 | |||
| SE5 | 0.82 | |||
| SE6 | 0.83 | |||
| SE7 | 0.64 | |||
| SE8 | 0.69 | |||
| SE9 | 0.84 | |||
| SE10 | 0.71 | |||
| Mental health (MHS-Q) | MH1 | 0.63 | 0.88 | 0.76 |
| MH2 | 0.73 | |||
| MH3 | 0.91 | |||
| MH4 | 0.76 | |||
| MH5 | 0.59 |
Reliability and validity of measurement scales (N = 1000).
4.3 Correlation analysis
Bivariate Pearson correlations among the key continuous variables are presented in Table 3. As hypothesized, music therapy participation was significantly and negatively correlated with mental health problems (*r* = −0.31, *p* < 0.001), indicating that higher involvement was associated with fewer reported symptoms. Self-evaluation was also significantly and negatively correlated with mental health problems (*r* = −0.37, *p* < 0.001). Furthermore, participation in music therapy was positively correlated with self-evaluation (*r* = 0.42, *p* < 0.001). These preliminary correlations provided support for testing the proposed mediation model.
TABLE 3
| Variable | M | SD | 1 | 2 | 3 |
|---|---|---|---|---|---|
| 1. Music therapy | 2.98 | 0.89 | – | – | – |
| 2. Self-evaluation | 2.85 | 0.54 | 0.42*** (p < 0.001) | – | – |
| 3. Mental health problems | 22.70 | 6.72 | −0.31* (p = 0.018) | −0.37* (p = 0.008) | – |
Pearson correlations among key continuous variables (N = 1000).
*p < 0.05, ***p < 0.001.
4.4 Testing the moderated mediation model
To test the hypothesized model–where self-evaluation mediates the link between music therapy and mental health, and gender moderates the direct path–we employed structural equation modeling (SEM) using maximum likelihood estimation.
4.4.1 Model fit
The proposed model demonstrated an acceptable to good fit to the data: χ2/df = 2.89, Comparative Fit Index (CFI) = 0.96, Tucker-Lewis Index (TLI) = 0.94, Root Mean Square Error of Approximation (RMSEA) = 0.05 (90% CI [0.04, 0.06]), Standardized Root Mean Square Residual (SRMR) = 0.04. These indices suggest that the model adequately represents the observed relationships in the data.
4.4.2 Path coefficients and hypotheses testing
The standardized path coefficients are illustrated in Figure 1 and detailed in Table 4.
FIGURE 1
![Diagram illustrating the relationship between music therapy, self-evaluation, gender, and mental health problems. Music therapy is directly linked to self-evaluation (β = 0.42) and mental health problems (β = -0.19). Self-evaluation also affects mental health problems (β = -0.25). Gender has a small effect on self-evaluation (β = 0.09), and an indirect effect of β = -0.11 on mental health problems within a 95% confidence interval [-0.14, -0.07]. Solid and dashed arrows indicate the strength and direction of influence.](https://www.frontiersin.org/files/Articles/1746614/xml-images/fpsyg-16-1746614-g001.webp)
Final moderated mediation model with standardized path coefficients. **p < 0.01, ***p < 0.001. Dashed line indicates moderation path.
TABLE 4
| Path (relationship) | β (std. coeff.) | S.E. | Z-value | *p* | 95% BC Boot CI |
|---|---|---|---|---|---|
| Direct effects | |||||
| Music therapy → self-evaluation | 0.42 | 0.03 | 12.81 | <0.001 | [0.36, 0.48] |
| Self-evaluation → mental health problems | −0.25 | 0.04 | −6.92 | <0.001 | [−0.32, −0.18] |
| Music therapy → mental health problems (direct effect) | −0.19 | 0.04 | −5.12 | <0.001 | [−0.26, −0.12] |
| Interaction effect | |||||
| Music therapy × gender → mental health problems | 0.09 | 0.03 | 3.08 | 0.002 | [0.03, 0.15] |
| Indirect effect | |||||
| Music therapy → self-evaluation → mental health problems | −0.11 | 0.02 | – | <0.001 | [−0.14, −0.07] |
Structural equation modeling (SEM) results for the moderated mediation model.
*Bold values indicate statistically significant differences or coefficients (p < 0.05).
4.4.3 Direct and mediating effects
Music therapy participation significantly predicted higher self-evaluation (β = 0.42, p < 0.001). Self-evaluation, in turn, significantly predicted lower levels of mental health problems (β = −0.25, *p* < 0.001). The direct effect of music therapy on mental health problems, after accounting for the mediator, remained significant and negative (β = −0.19, *p* < 0.001). The indirect effect of music therapy on mental health problems through self-evaluation was statistically significant (β = −0.11, 95% Bias-Corrected Bootstrap CI [−0.14, −0.07]). This confirms that self-evaluation partially mediates the relationship between music therapy and mental health, supporting H3. The total effect of music therapy on mental health problems was β = −0.30 (*p* < 0.001), supporting H1. The positive association between self-evaluation and mental health (fewer problems) supports H2.
4.4.4 Moderating effect of gender
The interaction term between music therapy and gender on mental health problems was significant (β = 0.09, *p* = 0.002). Simple slope analysis (Figure 2) revealed that the adverse effect of music therapy on mental health problems was significant for both males (β = −0.12, *p* = 0.001) and females (β = −0.26, *p* < 0.001), but the effect was significantly more substantial for female students. This finding supports H4, indicating that gender moderates the direct path.
FIGURE 2
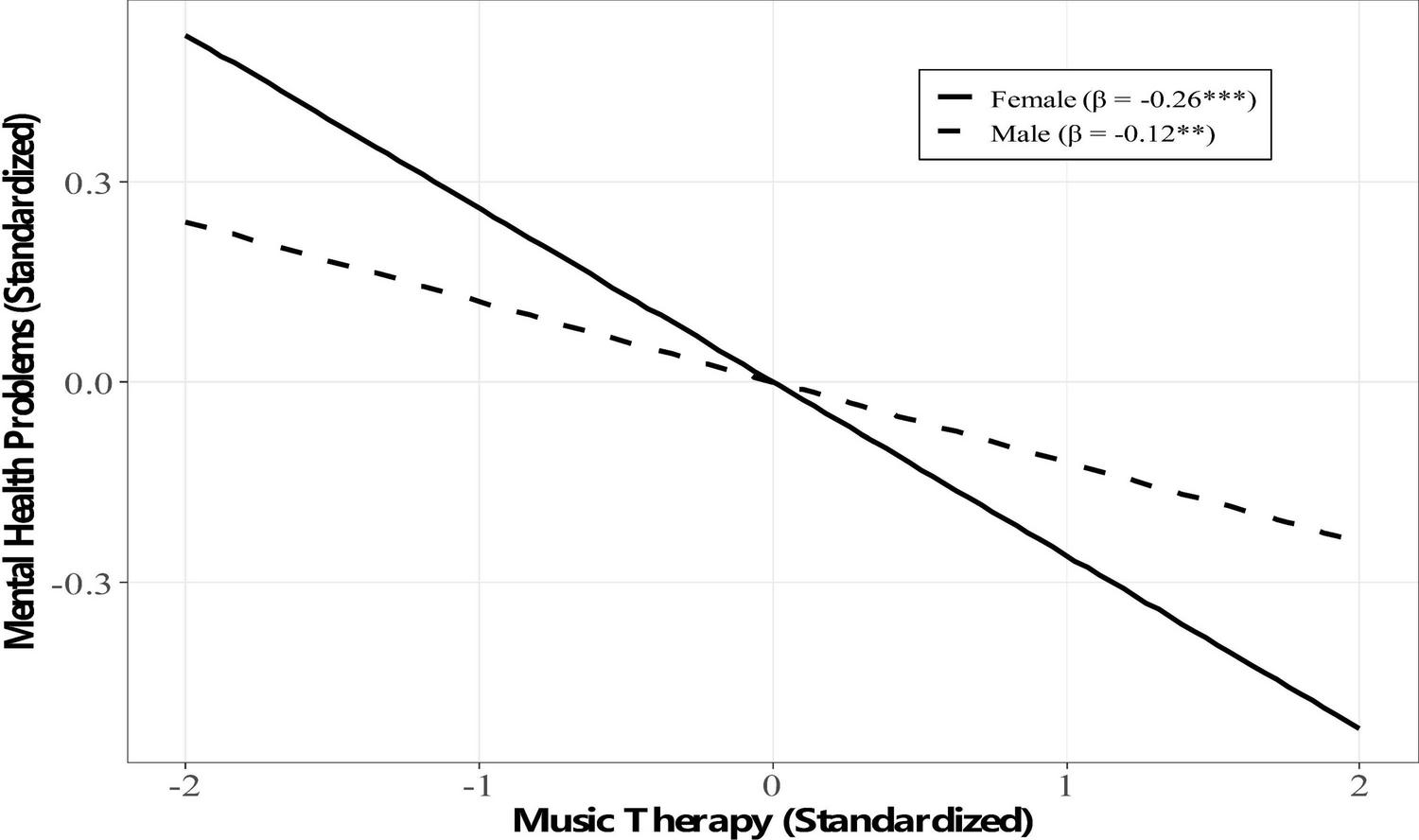
Simple slopes for the moderating effect of gender on the direct path. *p < 0.05, ***p < 0.001.
4.5 Ancillary analysis: family income and mental health
An exploratory analysis of variance (ANOVA) was conducted to further examine the unexpected relationship between family income and mental health problem status identified in the chi-square test (see Table 5). Results indicated a significant main effect of income category on mental health problem scores, F(2, 997) = 3.58, *p* = 0.028. Post hoc comparisons using Tukey’s HSD revealed that the Medium-income group reported significantly fewer mental health problems than the Low-income group (*p* = 0.045). The high-income group was no different from the Low or Medium groups. It is non-linear, indicating that moderate economic resources, in the case of Chinese university students, are associated with minimal mental health risk, which could be explained by the absence of sufficient support and excessive performance-related pressure, as in the high-income group.
TABLE 5
| Family income category | n | Mental health problem score M (SD) |
95% confidence interval | Tukey HSD post hoc comparisons |
|---|---|---|---|---|
| Low | 442 | 23.10 (1.20) | [22.98, 23.22] | vs. Medium: *p* = 0.045 |
| Medium | 460 | 21.45 (1.10) | [21.33, 21.57] | vs. Low: *p* = 0.045 |
| High | 98 | 22.13 (1.30) | [21.87, 22.39] | vs. Low: *p* = 0.471 vs. Medium: *p* = 0.682 |
One-way ANOVA and post hoc comparisons for mental health problems by family income category.
*p < 0.05.
5 Discussion
This research examined a mediated mediation model linking music therapy participation and mental health among Chinese university students. The results are a solid argument for the proposed framework. First, as hypothesized, greater involvement in music therapy was associated with improved mental health (fewer reported symptoms). Second, self-evaluation also enhanced this relationship and was confirmed as a mediating mechanism. Third, the direct effect of music therapy was moderated by gender, and female students obtained a more direct mental health benefit as a result of participation.
5.1 The mediating pathway: enhancing the self
The substantial intermediary effect of self-evaluation aligns with psychological assumptions that therapeutic practices promote mastery and self-esteem (Sowislo and Orth, 2013). With competence, creativity, and positive reinforcement in a therapeutic environment, music therapy is likely to offer powerful experiences of competence and validation (Fancourt and Finn, 2019; Geeves et al., 2020). Such improved self-assessment is then mobilized as an internal strength that shields against stress and negative affect, thereby increasing mental health (Orth and Robins, 2022). This process highlights the importance of the fact that the positive effects of music therapy are not limited to the short-term mood improvement but extend to a more enduring cognitive-affective shift.
5.2 Gender as a moderator: cultural and psychological nuances
The biological and psychosocial viewpoints are combined in the observation that the direct mental health benefits of music therapy were more pronounced in women. We found that women reported more mental health issues as baseline, which is also in line with the national trends (Li et al., 2021). It would render them more accepting of the emotional and communal essence of the music therapy due to their vulnerability to emotional and relational stimuli (Linnemann et al., 2015; Park et al., 2021). Moreover, within the Chinese set-up where women can feel the stress of society, music therapy can serve as a safe and viable means of emotional and stress discharge, which women can readily sympathize with, rather than with their male counterparts (Chen and Zhou, 2022).
5.3 Unexpected pattern of family income
The negative conclusion about family income is worth viewing with caution. Although riches tend to generate protective factors, in high-performing settings, wealth may also be associated with enormous pressures to perform, which may offset its advantages (Luthar et al., 2020). It may be that the “moderate” income group can be financially safe enough without the high-stress, status-seeking demand that leads to anxiety. Here, the link between socioeconomic elements and mental well-being in competitive societies is multi-dimensional as well, and reflects contemporary literature on sustainability by vindicating the need to address well-being holistically and take into account contextual stressors (Ortiz Diaz and Abbas, 2024).
5.4 Implications for practice
5.4.1 University mental health programming
Music therapy-related interventions (e.g., group drumming, therapeutic choirs, guided music listening) should be considered among the options in university student wellness programs because they are non-stigmatizing and engaging (de Witte et al., 2020).
5.4.2 Gender-sensitive intervention
Practitioners are advised to be mindful of the potentially greater direct efficacy of the music therapy process for female students and to accommodate their needs by designing or promoting groups, and by evaluating how to engage male students (MacDonald et al., 2021).
5.4.3 Focus on self-development
Interventions aimed at developing self-assessment should explicitly enhance it through musical exercises and structured positive feedback based on success, and capitalize on this central process to bring about permanent change (Geeves et al., 2020).
5.5 Limitations and future directions
This research is limited in several ways. First, its cross-sectional nature does not allow for making definitive causal conclusions. Although our model is conceptually motivated, longitudinal or experimental research is required to establish the direction of effects and to rule out reverse causality (e.g., better mental health leading to increased therapy participation). Second, the self-report scale is prone to biases. Future study may include behavioral observations, physiological indicators, or clinician ratings. Third, the sampling, however, was not entirely nationally representative. More comprehensive random sampling frames should be used in future research. Fourth, we have not quantified the particular forms or “doses” of music therapy; the effectiveness of the various modalities remains a significant future question (de Witte et al., 2022). Lastly, music preference was initially intended to be measured, but was then dropped due to measurement limitations. The development and inclusion of this variable in future work should also be rigorously tested to assess whether it moderates the efficacy of the intervention (Carlson et al., 2021).
6 Conclusion
This research contributes to expanding knowledge about the mechanisms of music therapy and the people it directly affects in the Chinese university environment. The findings go beyond merely establishing a relationship between a variable (self-evaluation) and another (gender) by determining that self-evaluation is a fundamental psychological process and that gender is the primary moderating variable. Although cross-sectional data have limitations, the findings strongly indicate that music therapy is a potential field for positively influencing mental health among students (Aalbers et al., 2017; de Witte et al., 2020). The fact that it has two practical purposes, a direct emotional rewards and a means of enhancing the self, makes it a valuable tool. It is advised that universities and mental health professionals create and apply music-based interventions, considering gender differences and students’ emphasis on self-evaluation as a long-term tool for well-being.
Statements
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Author contributions
WW: Writing – original draft, Conceptualization, Writing – review & editing, Methodology.
Funding
The author(s) declared that financial support was not received for this work and/or its publication.
Acknowledgments
I would like to thank the students who participated in this study for their time and honesty. Gratitude is also extended to the School of Music at Hanshan Normal University for logistical support during data collection.
Conflict of interest
The author(s) declared that this work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declared that generative AI was not used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1
Aalbers S. Fusar-Poli L. Freeman R. E. Spreen M. Ket J. C. Vink A. C. et al (2017). Music therapy for depression.Cochrane Database Syst. Rev.2017:CD004517. 10.1002/14651858.CD004517.pub3
2
Auerbach R. P. Mortier P. Bruffaerts R. Alonso J. Benjet C. Cuijpers P. et al (2018). WHO world mental health surveys international college student project: Prevalence and distribution of mental disorders.J. Abnormal Psychol.127623–638. 10.1037/abn0000362
3
Babbie E. R. (2020). The practice of social research, 15th Edn. Boston, MA.: Cengage Learning.
4
Bernardi L. Porta C. Sleight P. (2006). Cardiovascular, cerebrovascular, and respiratory changes induced by different types of music.Heart92445–452. 10.1136/hrt.2005.064600
5
Carlson E. Saarikallio S. Toiviainen P. Bogert B. Kliuchko M. Brattico E. (2021). Maladaptive and adaptive emotion regulation through music: A behavioral and neuroimaging study of males and females.Front. Hum. Neurosci.15:726039. 10.3389/fnhum.2021.726039
6
Chanda M. L. Levitin D. J. (2013). The neurochemistry of music.Trends Cogn. Sci.17179–193. 10.1016/j.tics.2013.02.007
7
Chen J. Zheng X. (2021). Psychometric evaluation of the Mental Health Status Questionnaire (MHS-Q) among Chinese university students: A validation study.J. Affect. Disord.292476–483. 10.1016/j.jad.2021.05.086
8
Chen L. Wang L. Qiu X. H. Yang X. X. Qiao Z. X. Yang Y. J. et al (2013). Depression among Chinese university students: Prevalence and socio-demographic correlates.PLoS One8:e58379. 10.1371/journal.pone.0058379
9
Chen X. Zhou X. (2022). Gender differences in mental health and responses to psychological interventions among Chinese college students: A meta-analysis.Curr. Psychol.41, 1234–1245. 10.1007/s12144-022-03021-1
10
Cuijpers P. Auerbach R. P. Benjet C. Bruffaerts R. Ebert D. Karyotaki E. et al (2019). The World Health Organization world mental health international college student initiative: An overview.Intern. J. Methods Psychiatric Res.28:e1761. 10.1002/mpr.1761
11
de Witte M. da Silva, Pinho A. Stams G. J. Moonen X. Bos A. E. et al (2020). Music therapy for stress reduction: A systematic review and meta-analysis.Health Psychol. Rev.14294–324. 10.1080/17437199.2020.1846580
12
de Witte M. Spruit A. van Hooren S. Moonen X. Stams G. J. (2022). Effects of music interventions on stress-related outcomes: A systematic review and two meta-analyses.Health Psychol. Rev.16134–159. 10.1080/17437199.2020.1846580
13
Fancourt D. Finn S. (2019). What is the evidence on the role of the arts in improving health and well-being? A scoping review.Geneva: World Health Organization.
14
Faul F. Erdfelder E. Buchner A. Lang A.-G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses.Behav. Res. Methods411149–1160. 10.3758/BRM.41.4.1149
15
Geeves A. McIlwain D. J. Sutton J. (2020). “The sense of agency in music making: Learning, performing, and listening,” in The Routledge companion to music cognition, (Milton Park: Routledge), 419–430.
16
Hayes A. F. (2022). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach, 3rd Edn. New York, NY: Guilford Press.
17
Hu L. Bentler P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives.Struct. Equat. Model.61–55. 10.1080/10705519909540118
18
Juslin P. N. Västfjäll D. (2008). Emotional responses to music: The need to consider underlying mechanisms.Behav. Brain Sci.31559–621. 10.1017/S0140525X08005293
19
Kish L. (1965). Survey sampling.Hoboken, NJ: John Wiley & Sons.
20
Kline R. B. (2023). Principles and practice of structural equation modeling, 5th Edn. New York, NY: Guilford Press.
21
Koelsch S. (2014). Brain correlates of music-evoked emotions.Nat. Rev. Neurosci.15170–180. 10.1038/nrn3666
22
Leubner D. Hinterberger T. (2017). Reviewing the effectiveness of music interventions in treating depression.Front. Psychol.8:1109. 10.3389/fpsyg.2017.01109
23
Li W. Dorstyn D. S. Jarmon E. Guo Y. (2021). Prevalence of mental health problems among Chinese college students: A systematic review and meta-analysis.J. Affect. Disord.287293–300. 10.1016/j.jad.2021.03.044
24
Linnemann A. Ditzen B. Strahler J. Doerr J. M. Nater U. M. (2015). Listening to music as a means of stress reduction in daily life.Psychoneuroendocrinology6082–90. 10.1016/j.psyneuen.2015.06.008
25
Liu X. Ping S. Gao W. (2022). Changes in undergraduate students’ psychological well-being as they experience university life: A longitudinal study in China.Intern. J. Environ. Res. Public Health19:1274. 10.3390/ijerph19031274
26
Luthar S. S. Kumar N. L. Zillmer N. (2020). High-achieving schools pose risks to adolescents: Documented problems, implicated processes, and directions for interventions.Am. Psychol.75983–995. 10.1037/amp0000556
27
MacDonald R. Kreutz G. Mitchell L. (2021). Music, health, and wellbeing.Oxford: Oxford University Press.
28
Orth U. Robins R. W. (2022). Is high self-esteem beneficial? Revisiting a classic question.Am. Psychol.775–17. 10.1037/amp0000922
29
Ortiz Diaz J. K. Abbas E. W. (2024). Urban green spaces and quality of life among young adults: Moderating effects of loneliness.J. Environ. Psychol.95:102345
30
Park M. Hennig-Fast K. Bao Y. Carl P. Mölbert S. C. (2021). Gender differences in the neural correlates of music-evoked emotion.Soc. Cogn. Affect. Neurosci.161160–1172. 10.1093/scan/nsab072
31
Pearce E. Launay J. Dunbar R. I. M. (2015). The icebreaker effect: Singing fosters rapid social bonding.R. Soc. Open Sci.2:150221. 10.1098/rsos.150221
32
Roldan-Canovas C. Chacón-Castro M. Jadán-Guerrero J. Salvador-Ullauri L. Acosta-Vargas P. (2024). Music education with artificial intelligence for inclusive and sustainable early childhood learning.Sustainability16:1234.
33
Rosenberg M. (1965). Society and the adolescent self-image.Princeton NJ: Princeton University Press.
34
Shultis C. L. Schreibman J. (2020). AMTA and aspirational ethics. Music Ther. Perspect.38, 7–8. 10.1093/mtp/miaa004
35
Sowislo J. F. Orth U. (2013). Does low self-esteem predict depression and anxiety? A meta-analysis of longitudinal studies.Psychol. Bull.139213–240. 10.1037/a0028931
36
Stallman H. M. (2010). Psychological distress in university students: A comparison with general population data.Aus. Psychol.45249–257. 10.1080/00050067.2010.482109
37
Tran A. V. Van Tran H. Luong T. T. Nguyen T. N. (2024). Exploring the relationship between stress, burnout, and occupational accidents in civil construction.Safety Sci.180:106543. 10.1016/j.ssci.2024.106543
38
Trost W. Frühholz S. (2021). The neuroaesthetics of music: A research agenda coming of age.Brain Sci.11:734. 10.3390/brainsci11060734
39
Wang C.-K. J. Zhang L. (2011). The reliability and validity of the Chinese version of the rosenberg self-esteem scale in university students.Chin. J. Clin. Psychol.19457–459
40
Williams E. Dingle G. A. Clift S. (2021). A systematic review of mental health and well-being outcomes of group singing for adults with a mental health condition.Eur. J. Public Health31164–172. 10.1093/eurpub/ckaa125
41
World Health Organization [WHO] (2022). World mental health report: Transforming mental health for all.Geneva: WHO.
42
Zatorre R. J. (2018). Musical pleasure and reward: Mechanisms and dysfunction.Ann. N. Y. Acad. Sci.142390–99. 10.1111/nyas.13684
Summary
Keywords
gender, mental health, music therapy, self-evaluation, university students
Citation
Wang W (2026) The association between music therapy and mental health in Chinese university students: a moderated mediation model of self-evaluation and gender. Front. Psychol. 16:1746614. doi: 10.3389/fpsyg.2025.1746614
Received
14 November 2025
Revised
24 December 2025
Accepted
29 December 2025
Published
04 February 2026
Volume
16 - 2025
Edited by
Yoon Fah Lay, Universiti Malaysia Sabah, Malaysia
Reviewed by
Y. Chen, Jining Medical University, China
Xin Shan, Sangmyung University, Republic of Korea
Updates
Copyright
© 2026 Wang.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wei Wang, 20250069@hstc.edu.cn
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.