 Jessica E. Bourne
Jessica E. Bourne Sam Leary2
Sam Leary2- 1Centre for Exercise, Nutrition and Health Sciences, School of Policy Studies, University of Bristol, Bristol, United Kingdom
- 2NIHR Bristol Biomedical Research Centre, University Hospitals Bristol and Weston NHS Foundation Trust and University of Bristol, Bristol, United Kingdom
- 3Population Health Sciences, University of Bristol, Bristol, United Kingdom
Background: Physical activity (PA) is a key component in the management of type 2 diabetes. However, this population have low rates of PA engagement. Electrically assisted cycling has been identified as a means through which to increase PA by incorporating activity into daily life, while overcoming some of the barriers to conventional cycling. The determinants of e-cycling among people living with chronic disease are largely unknown. The aim of this research was to explore the determinants of e-cycling among individuals with type 2 diabetes using the Theoretical Domains Framework (TDF) and the Capability, Opportunity and Motivation for Behaviour change model (COM-B). This information is important for determining the suitability of future e-cycling initiatives and, if appropriate, inform future e-cycling interventions.
Method: One-to-one semi structured interviews were conducted with 16 participants from the e-cycling arm of a pilot randomised controlled trial between September 2019 and April 2020. The TDF was used to develop the interview guide. The framework method of analysis was used, incorporating both deductive and inductive reasoning. A conceptual model of the factors that influence e-cycling in this population was created.
Results: The most commonly reported TDF domains were skills, knowledge, belief about capabilities, belief about consequences and environmental context and resources. Specifically, e-bike training facilitated e-cycling engagement by providing participants with the skills, knowledge, and confidence needed to ride the e-bike and ride on the road. In addition, the enjoyment of e-cycling was a key facilitator to engagement. Participants engaged in e-cycling to improve their health rather than for environmental reasons. Most barriers to e-cycling related to the natural or physical environment.
Conclusion: This study provides insight into the personal, social, and environmental factors associated with e-cycling in this population. The findings of this study can be used to develop a more refined e-cycling intervention targeting the factors identified as influencing e-cycling engagement. In addition, this information will help in the selection of mechanistic outcome measures for evaluation.
1. Introduction
Type 2 diabetes is a metabolic disease that negatively impacts an individual's physical and mental health (1–6). By 2040, it is estimated that approximately 642 million individuals worldwide will be diagnosed with diabetes, of which 90% will be type 2 diabetes (7). The cost of ongoing treatment and management of type 2 diabetes and its associated complications places considerable strain on health services (8).
Physical activity (PA) is an important lifestyle factor in the prevention and treatment of type 2 diabetes (9–13). However, individuals with type 2 diabetes are less physically active than those without type 2 diabetes and many fail to meet the recommendation of 150-min of moderate to vigorous physical activity (MVPA) per week (14–16). Interventions aimed at increasing PA in this population often require significant contact time and expertise, thereby limiting their scalability (17). Furthermore, individuals often return to prior PA levels when left to self-manage their activity (17–19). As such, there is a need to develop PA interventions that are less labour intensive and that are effective at promoting behaviour change beyond the intervention period.
Active travel is widely recognised nationally and internationally as a means of increasing PA. As such, encouraging active travel is endorsed by the National Institute of Health and Care Excellence (20) and the World Health Organization (21). Among individuals with type 2 diabetes active commuting is associated with increased PA and lower body mass index (22). Despite widespread endorsement, rates of engagement in active travel in the UK and around the world are low (23–25), especially among individuals living with type 2 diabetes (22). Community-based initiatives can serve to increase cycling behaviour (26–29), however it is rarely maintained over time (30, 31). Furthermore, there are several barriers to conventional cycling that could discourage engagement including physical constraints associated with hilly terrain and poor physical fitness, as well as a lack of time and the distance people have to travel (32). These barriers may be accentuated in individuals with type 2 diabetes given their overall lower levels of PA.
Electrically-assisted bicycles (e-bikes; also known as pedelecs) have been identified as an alternative form of active travel that can positively impact health (33) while overcoming some of the commonly reported barriers to conventional cycling. While e-bikes have many similarities with conventional bicycles, the electrical assistance requires less physical effort and leads to greater riding distance and frequency (34–36). Therefore, it is likely that some determinants of conventional cycling are less relevant to e-cycling. Despite the electrical assistance evidence suggests that e-cycling is performed at at least a moderate intensity and leads to similar or slightly lower physical markers of intensity than conventional cycling (33). However, given that individuals report e-cycling for longer and more frequently than they do a conventional bicycle, e-cycling is often associated with greater weekly energy expenditure than a conventional bicycle (35, 37).
Research conducted with e-bike owners and those who have been provided with an e-bike as part of an intervention reveals that the ability to ride further, faster, on hillier terrain and to ride with friends and family are common facilitators to e-cycling engagement. Conversely, bad weather, poor infrastructure and theft concerns are common barriers to engagement (34, 36, 38–40). To date, few studies have explored the factors associated with e-cycling among people living with chronic disease for whom engagement in active travel is low (22). People living with chronic conditions may experience e-cycling interventions differently and be impacted by different contextual factors than a healthy adult population. Two studies have specifically explored factors associated with e-bike engagement in people living with chronic disease. Boland and colleagues (41) examined the use of adapted e-bikes in three individuals recovering from a stroke. The level of social support, motivation for riding, level of physical impairment all impacted riding. Among individuals with type 2 diabetes, Searle and colleagues (42) reported that e-cycling was perceived as enjoyable and enabled individuals to cycle with friends and family. However, they did not conduct a comprehensive evaluation of the data to explore the determinants of e-bike use, rather the researchers were interested in understanding how e-cycling impacted participants management of their diabetes. E-cycling may offer an alternative to structured lifestyle interventions for individuals with type 2 diabetes, enabling exercise to be completed outside and incorporated into daily life which may lead to sustained physical activity behaviour.
Understanding how participants experience e-cycling, particularly the barriers and facilitators to riding, will enable the development of a conceptual understanding of the factors that are most influential on e-cycling engagement in this population. The use of behaviour-change theory and models can help in this understanding and identify key intervention components required to bring about change. The Medical Research Council guidance for developing complex interventions outlines that researchers need to have a theoretical understanding of the potential processes of change (43). When little is known about the target behaviour in the population of interest qualitative research is useful to develop a theoretical understanding of the behaviour (44). The Behaviour Change Wheel is a practical intervention design tool which transparently guides researchers through intervention design and delivery. At the core of the BCW is the COM-B model which can be used to determine what needs to change for the desired behaviour to occur (45). The COM-B model proposes that human behaviour is a result of the interaction between capability, opportunity and motivation. Specifically, for a behaviour to occur a person must have the psychological and physical capability to perform the behaviour; the physical and social opportunity to engage in it; and they must have the motivation, either conscious or automatic, to engage. COM-B has been found to be an effective model in explaining physical activity behaviours (46).
The Theoretical Domains Framework (TDF) was designed to understand behaviour theoretically by establishing which processes of change should be targeted (47). The TDF consists of 14 theoretical domains that consider the environmental, social, cognitive and affective influences on behaviour (48). The TDF maps directly onto the COM-B components, enabling expansion of each of these components and assisting in identification of the potential determinants of behaviour. Once identified, this information can be used to guide the selection of quantitative measures to examine potential moderating and mediating effects as part of a full-scale evaluation and/or to inform target areas for intervention in future e-cycling initiatives among individuals living with chronic disease. The primary objective of the study was to explore the factors associated with e-cycling engagement among individuals with type 2 diabetes following trialling an e-bike using the TDF and COM-B model, and to develop a conceptual model of the behaviour.
2. Methods
2.1. Participants and procedures
One-to-one semi-structured interviews were conducted with individuals who were randomised to the intervention arm of a parallel two-arm pilot randomised controlled trial. The trial compared an e-cycling intervention against a standard-care waitlist control in adults with type 2 diabetes (49). Eligibility for the study included having a clinical diagnosis of type 2 diabetes and being between 30 and 70-years of age. Individuals were ineligible if they self-reported engagement in ≥150-min of MVPA per week (50); took exogenous insulin; had a myocardial infarction or stroke in the past six months or had evidence of end-stage renal failure or liver disease; had uncontrolled hypertension; had any other contraindications to exercise; were not cleared to engage in PA by their GP and/or were unable to read and communicate in English. This single centre study was conducted in the city of Bristol, England. Individuals in the intervention arm received e-bike training consisting of two one-to-one training sessions followed by a 12-week e-bike loan in which they were instructed to use the e-bike as they desired (i.e., no riding goals stipulated). During the e-bike loan participants were offered two further training sessions. Twenty individuals were allocated to the intervention arm. Four participants discontinued with the intervention (reasons included: personal situation [n = 2], purchased an e-bike [n = 1], undisclosed [n = 1]). Seventeen individuals were invited to take part in the interviews of which 16 participated. Interviews were conducted by JEB over the telephone between September 2019 and April 2020, within two weeks of finishing the e-bike trial. The interviews were digitally recorded using encrypted recording devices. The recordings were transcribed verbatim by Transcription UK and stored using NVivo data management software (NVivo10, QSR International, 2012). The transcripts were checked against the original recordings to ensure reliability. Interviews ranged between 33mins and 50mins in length. Ethical approval was obtained from the NHS Health Research Authority Southwest/Central Bristol Research Ethics Committee (Ref: 18/SW/0164) and was sponsored by the University of Bristol.
2.2. Interview questions
The interview topic guide was developed using the Theoretical Domains Framework (TDF) (48) and based on guidance by Atkins and colleagues (51). The interview guide included at least one question for each theoretical domain to comprehensively consider the possible influences on e-cycling. The interview guide is provided in the Supplementary Material. Follow-up probes or prompts were included to delve more deeply into each domain (51). The order in which questions were asked was flexible to enable flow during the interview.
2.3. Qualitative data analysis
Interview data were analysed using the Framework method (52) and guided by Gale and colleagues seven-stage analysis process (53). The Framework method sits within the family of analyses methods known as ‘thematic analysis” (53, 54) and is suited to research that has specific questions and a pre-defined sample (55). Framework analysis does not require adherence to either inductive or deductive analysis approaches and is therefore appropriate in the current theory-based study. In addition, it does not prescribe to a single epistemological or ontological framework thereby providing a degree of flexibility regarding how data analyses is approached (54). Table 1 outlines the steps involved in analysing the data. JEB created the e-cycling intervention as part of her PhD research. She had training in qualitative research methods, developed the interview guide and conducted the interviews. JEB analysed the data with in-depth discussions with AS. In the current study a critical realist ontology and constructionist epistemology was adopted regarding the data.

Table 1. The seven stages of the framework method of qualitative analysis and how they were applied to the research question.
3. Results
3.1. Participants characteristics
Of the 16 participants interviewed, there was an equal split between men and women and a mean age of 59.75 years (Standard Deviation = 6.85). Ten participants were working either full or part time. Fourteen participants had some degree of cycling experience prior to the trial. Overall 56.25% of participants completed three or more cycling lessons with the instructors. Fifteen participants had at least one private vehicle at their residence. The distances travelled on the e-bike during the loan period by the 13 participants with available data ranged from 9 km to 1,878 km (Median = 144.4; IQR: 117.0, 307.0), with a median of 22 journeys (IQR: 13, 33) over the loan period based on travel log books. Table 2 provides the demographic characteristics of participants.
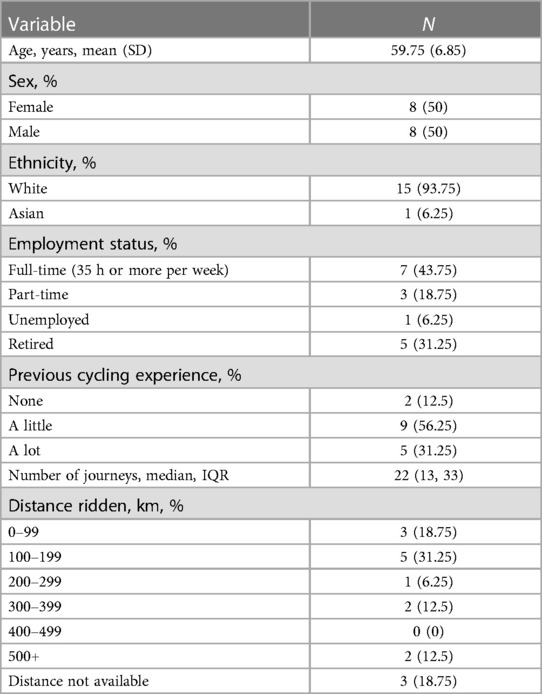
Table 2. Demographic characteristics.
3.2. Summary of the TDF and COM-B model
The transcripts provided data that represent all the fourteen domains of the TDF and all components of the COM-B model. Table 3 presents a summary of COM-B constructs, TDF domains and frequency counts, themes and example quotes. Whether the theme was identified as a barrier or facilitator to e-cycling engagement is reported. The COM-B constructs, TDF domains and how they relate to one another are summarised narratively and a conceptual model proposed (Figure 1).
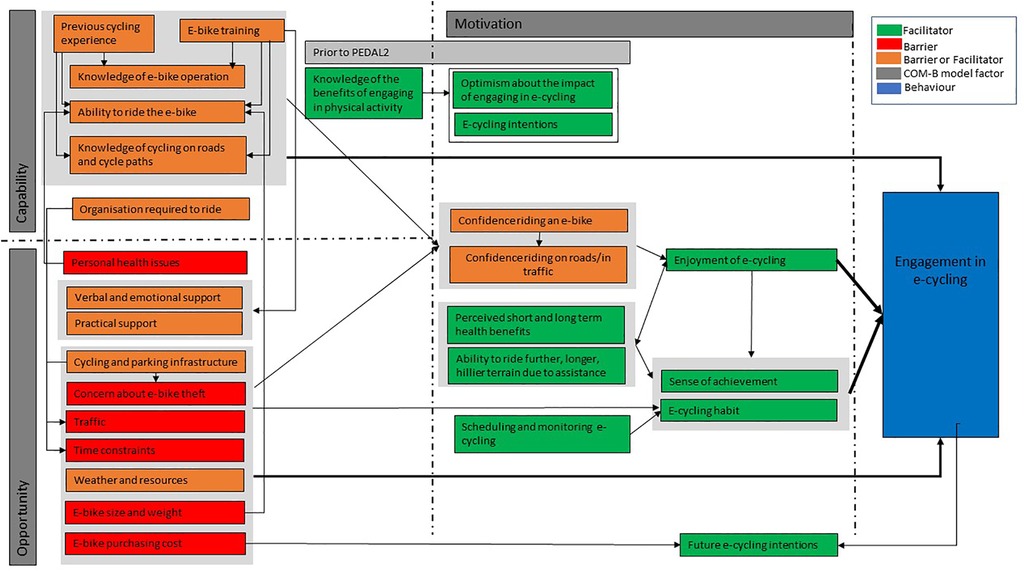
Figure 1. Conceptual model of e-cycling in adults with type 2 diabetes.
The most commonly reported domains were skills, knowledge, beliefs about consequences, belief about capabilities and environmental context/resources, and the least commonly reported domains were optimism, goals and behavioural regulation.
3.2.1. Capability
Physical capability: skills
Fifteen participants were able to ride the e-bike by the end of the training period. Of these 15, 14 had some degree of previous cycling experience. Participants with more recent cycling or motorcycling experience (two to three years) reported greater ability to ride the e-bike than those with no experience or who had not ridden for a long time (Table 3.1.a.iii). While several participants engaged in frequent cycling at a younger age, and reported confidence riding a bicycle, many were surprised at how different e-cycling was to conventional cycling. This was attributed to the devices themselves, the poor conditions of the roads and the amount of traffic compared to when they used to cycle. As such, some participants felt their previous riding skills did not translate to e-cycling in the present day.
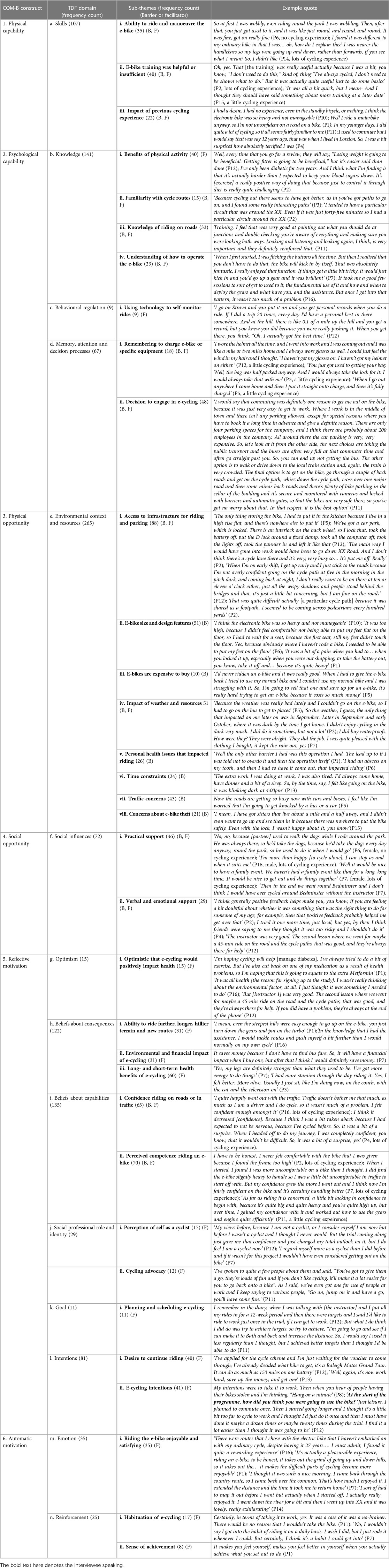
Table 3. COM-B constructs, TDF domains, sub-themes and example quotes.
Before starting the e-bike training participants with previous cycling experience felt that the training was going to be unnecessary. However, all participants reported learning new skills, specifically how to handle the e-bike and use the electrical assistance, and how to ride safely on roads and in traffic (Table 3.1.a.i/ii). The training conducting during the loan period enabled participants to practice their skills.
Psychological capability
Knowledge
The majority of participants were aware of the benefits of engaging in PA, in general, and for diabetes management (Table 3.2.b.i). Several participants felt that engaging in PA was an easier way of managing their diabetes than dieting. This knowledge impacted their desire to sign up for the trial and engage in e-cycling.
The e-bike training provided participants with sufficient knowledge on how to use the e-bike. Over time, with practice, participants became more efficient at using the gears and electrical assistance (Table 3.2.b.iv). In addition, the training taught participants how to safely ride on the road and where to find safe cycle paths (Table 3.2.b.ii/iii). When choosing where to ride some participants reported sticking to familiar routes, for which they knew the cycling infrastructure and/or traffic levels. While others enjoyed using the cycling maps to plan rides and explore new bike paths (Table 3.2.b.ii).
Behavioural regulation
Although infrequently discussed, some participants reported that monitoring their behaviour using tools such as Strava or a GPS watch encouraged them to engage in e-cycling.
Memory, attention and decision making processes
Participants reported evaluating the pros and cons of cycling vs. using a different mode of transport (Table 3.2.d.ii). As such, the decision to engage in e-cycling was often carefully considered. In general participants felt that utilitarian journeys required more organisation than recreational journeys. However, participants who had cycled regularly in the past reported having strategies to ensure they would remember all the required equipment, such as prepacking bags or running through mental checklists before leaving to ensure they had all their equipment (Table 3.2.d.i).
3.2.2. Opportunity
Physical opportunity: environmental context and resources
Barriers relating to the physical opportunity were the most commonly reported by participants in this study and included:.
Cycling infrastructure, parking facilities and traffic
Participants were concerned that the e-bike could be stolen if left in a public space, especially when the parking facilities were deemed inadequate (Table 3.3.e.viii). Theft anxiety was exacerbated as the e-bike was on loan and participants were unclear of the financial implications for themselves if the e-bike was stolen. Participants reported that they would have been less anxious about locking the e-bike up in public spaces if it belonged to them. Having good parking facilities at a destination facilitated e-cycling, particularly for utilitarian purposes, while poor parking facilities inhibited e-bike use (Table 3.3.e.i). Having limited e-bike storage at home also inhibited e-cycling. Several participants had to keep the e-bike indoors which meant getting in and out the house required considerable effort (Table 3.3.e.i).
Regarding riding, participants were reluctant to ride on roads with no cycling infrastructure, primarily due to traffic concerns (Table 3.3.e.vii). Participants who felt they were close to segregated cycle paths were willing to cycle short distances on the road to reach these paths. Participants’ level of confidence riding the e-bike and riding on roads impacted the degree to which segregated cycling infrastructure was deemed a necessity. For those with limited confidence riding on roads, not having easy access to segregated paths negatively impacted their e-cycling. For participants with high levels of confidence riding on the road the absence of cycling infrastructure, while not enjoyable, did not stop them from engaging in that specific ride. There was concern regarding the volume of traffic on cycle paths and the complications of mixing cyclists and pedestrians due to travelling at variable speeds. In addition, a few participants reported that in the dark the cycle paths felt isolated, and they felt vulnerable (Table 3.3.e.i).
Time and weather constraints
Work and personal caring responsibilities inhibited e-cycling for some participants, particularly those in full-time employment who felt they had limited time (Table 3.3.e.vi). Heavy rain and darkness were the two weather related barriers frequently reported by participants (Table 3.3.e.iv). For some participants having wet weather gear and good lights helped to overcome these issues, while others actively chose not to cycle in these conditions despite access to equipment.
E-bike specific issues
The weight of the e-bike was noticeable to all participants and in some cases made the e-bike hard to manoeuvre (Table 3.3.e.ii). In addition, for some the e-bike frame was perceived as being too large, leading to feelings of discomfort. Many participants, potentially due to the weight of the bike, wanted to be able to comfortably put their feet on the ground when stationary. Issues with the perceived size and weight of the frame impacted participants confidence both riding the e-bike and riding on the road. In addition, participants found the battery itself to be inconvenient and heavy to carry around.
Several participants commented that they would like to continue cycling after the trial but that the cost of the bike meant they were unable to do so. For some participants this meant changing to conventional cycling, while for others this meant not engaging in cycling until they had saved sufficient money to purchase an e-bike (Table 3.3.e.iii).
Personal health issues
During the study personal health issues impacted cycling for several participants. These were both acute and chronic in nature. The chronic conditions occurred in participants over 60-years of age, while acute conditions occurred in younger participants. Four participants reported having pre-existing additional health conditions. For two participants this negatively impacted riding (arthritis in hand and difficulty lifting their arm to signal due to cancer treatment) while the other two were able to develop strategies to deal with the health condition (blind in one eye and hearing loss in one ear) (Table 3.3.g.v).
Social opportunity
When instructors were perceived as engaged in the training, participants reported feeling practically and emotionally supported. These instructors delivered more training sessions and participants felt that they practiced riding in areas that they may not have previously considered. However, instructors perceived as being disengaged conducted less training sessions and participants did not feel supported through the training (Table 3.4.f.i/ii).
Outside of the e-bike training, the amount of practical support received and/or desired ranged greatly between participants. Participants with no previous cycling experience desired more practical support to enable or motivate them to ride than those who knew how to cycle (Table 3.4.f.i). Several participants reported cycling with friends and family which was enjoyable and motivational (Table 3.4.f.i). There appeared to be a gender difference with men being content to cycle alone and women desiring greater practical riding support.
Similarly, some participants found verbal support to be encouraging, while others felt their decision to ride was not influenced by others. For individuals who were unsure about whether e-cycling was appropriate for them the feedback from others was impactful, either encouraging them to continue e-cycling or confirming their decision to stop. For one participant, who was struggling with e-cycling, the feedback from their friends impacted their decision to stop riding (Table 3.4.f.ii). There were no apparent differences in the perception of verbal support based on gender.
3.2.3. Motivation
Reflective motivation
Optimism
Participants primary motivation for signing up for the study and engaging in e-cycling was to have a positive impact on their health rather than due to environmental concerns (Table 3.5.g.i). Given their knowledge of the benefits of PA, participants reported being optimistic that e-cycling would positively impact their health (Table 3.5.g.i).
Belief about capabilities
For the majority of participants the e-bike training positively impacted their perceived competence to ride the e-bike and over time, with increased practice, this confidence grew (Table 3.5.g.ii). Participants with recent cycling experience (two to three years) were more confident riding an e-bike on roads and in traffic compared to those that hadn't ridden for a while (Table 3.5.g.i). However, for some participants, even previous cyclists, the unanticipated differences between conventional cycling and e-cycling, as well as the poor conditions of the road negatively impacted their riding confidence (Table 3.5.g.i).
The weight and size of the e-bike negatively impacted confidence riding the e-bike for some participants (Table 3.5.g.ii). Participants reported how the instructors made a series of alterations to the seat height or provided a smaller size e-bike to increase their comfort and ability to ride. With practice, and alterations to the equipment, participants’ felt they were able to ride the bike and became more confident (Table 3.5.g.i/ii).
Overall participants’ degree of confidence riding the e-bike impacted their confidence riding on the road. Specifically, participants who were more confident riding the e-bike were also more confident riding on the road with traffic. While those who were uncomfortable on the e-bike reported greater anxiety riding on the roads due to not being able to respond to changing situations and interactions with cars.
Belief about consequences
Beliefs about the consequences of engaging in e-cycling were the most commonly reported facilitators to engagement. Specifically, both men and women felt that e-cycling positively impacted a variety of health outcomes including a) diabetes management, through notable decreases in blood sugar levels, b) improved mental health and c) increased fitness (Table 3.5.i.iii). By comparison, few participants felt that e-cycling had significant financial or environmental implications for themselves.
One of the most commonly reported facilitators to e-cycling was the electrical assistance which enabled participants to travel further, faster and on hillier terrain in comparison to a conventional bicycle (Table 3.5.i.i). This contributed to e-cycling engagement and enabled participants to try out routes that they would not have considered tackling on a conventional bicycle.
Social identity
Using an e-bike regularly for three months enabled some participants to feel more like a cyclist. However, the degree to which participants identified as a cyclist varied greatly. Specifically, participants who reported a stronger e-cycling habit, and greater distances travelled, saw themselves more as cyclists than those who did not get in the habit of cycling regularly and travelled less distance (Table 3.5.j.i). Three participants shared how they would advocate e-cycling to others, while another three reported having specific discussions around the benefits of e-cycling and saw themselves as role models for e-cycling (Table 3.5.j.ii).
Goals
Participants who rode a greater distance over the trial period discussed setting a range of e-cycling goals including riding to a certain location, using less assistance or completing a route in a faster time (Table 3.5.k.i).
Intentions
Prior to the study participants planned to use the e-bike for both recreational and utilitarian purposes. However, for those that intended to make utilitarian journeys via e-bike, and replace other transport modes, they discussed how they were unable to achieve this intention due to a range of environmental barriers identified above (Table 3.5.l.ii). Though one participant, who planned to use the e-bike purely for leisure, used it primarily for commuting (Table 3.5.l.ii). This individual felt able to commute on the e-bike due to access to safe parking infrastructure at their place of work.
At the end of the study, 12 participants wanted to continue riding an e-bike, with five actively seeking out e-bike purchasing options and one purchasing an e-bike part way through the study (Table 3.5.l.i). Two participants wanted to continue riding on a conventional bicycle following the study. Of those seeking out e-bikes half reported that an e-bike was out of their price range and expressed a need to save up or wait for a change of circumstances (e.g., retirement).
Automatic motivation
Emotion
The enjoyment associated with e-cycling was a key facilitator to engagement. Specifically, the ability to ride new and longer routes meant e-cycling led to feelings of enjoyment (Table 3.6.m.i). Part of the enjoyment of e-cycling came from being in the fresh air and nature and having the ability to explore new routes. Cyclically, the enjoyment associated with riding led participants to ride further and more frequently than they had anticipated.
Reinforcement
Participants reported experiencing a sense of achievement once a ride was complete (Table 3.6.n.ii). This achievement, along with the enjoyment, led to increased riding and some participants commented how this helped e-cycling to become a habit for them (Table 3.6.n.i).
4. Discussion
This theory-based qualitative study examined the factors associated with engagement in e-cycling among individuals with type 2 diabetes, with a particular focus on identifying barriers and facilitators to engagement. In addition, the study sought to develop a conceptual understanding of how these factors relate to one another to impact behaviour. This information can be used to refine the current intervention (57) and/or guide future initiatives aimed at increasing e-cycling in people living with chronic disease. The key findings of this study are discussed below.
4.1. The importance of e-bike training to build actual and perceived capability
The results of this study highlight that regardless of previous cycling experience e-bike training is beneficial, providing participants with riding skills, knowledge of how to safely ride on roads and where and how to access segregated cycling infrastructure. Consequently, participants reported increased confidence when riding the e-bike, riding on the road and exploring new cycling routes. The increase in confidence was greatest among individuals who had not cycled for a considerable period of time. Similar increases in confidence have been reported among older adults in the UK following e-bike training (58). Furthermore, a recent review of conventional bike skills training programmes concluded that training led to increased riding confidence, and was positively associated with increased cycling frequency (29). These findings highlight the importance of training to target key individual level predictors of e-cycling, namely skills, knowledge, and confidence.
Despite the apparent positive impact of training on cycling behaviour, e-bike interventions rarely report the details of training provided. This maybe because no formal training is conducted, training is minimal, or researchers do not consider the impact of the e-bike training on behaviour. Lack of reporting of intervention content and duration is a similar problem in conventional cycling studies (29). An understanding of what is delivered as part of an e-cycling intervention is important to determine what is most likely to facilitate e-cycling. E-bike training is of particular importance to older adults or people living with chronic disease who may have pre-existing health concerns that require adaptations to the e-bike, riding style or riding location. These issues can be addressed and overcome with support from an instructor, as was the case in the current trial. It is important to note that in the current trial three participants, (two with a little cycling experience and one with no experience) required more than the specified four training sessions, highlighting the need to tailor e-bike training.
In addition, more support was desired for women who had less cycling experience than men when entering the study, a finding echoed in other e-bike trials (59). In the current trial men completed higher levels of skills training (National Cycling Skills levels two and three) than women prior to taking the e-bike home and cycled further, on average, than women during the trial. Previous cycling research has shown that higher levels of national skills cycle training completed is associated with more riding (60). As such, women should be supported to reach these higher levels of skills training prior to an e-bike loan.
Instructor led cycling sessions conducted during the e-bike loan made participants feel supported and offered an informal setting in which to discuss e-cycling and practice riding. Furthermore, participants that attended these sessions rode further than those that did not. Serali and colleagues (29) found that cycling frequency decreased over time following training and recommend that training should be followed up by post training support to ensure that participants consolidate the skills and confidence gained during training. This recommendation is supported by the findings of the current study and suggest that the additional support provided in the current study, above and beyond delivering skills training, is important to practice skills and maintain confidence. Conversely, when participants reported instructors to be disengaged in the training this negatively impacted confidence. As such, instructors need to be comprehensively trained, not only on the skills component, for which they were confident (49), but also on how to offer support and effectively engage with a population who may require more support than the instructors are used to providing.
4.2. E-bike size and weight concerns
Despite comprehensive training several participants reported that the e-bike was too large making it difficult to manoeuvre, leading to decreased confidence riding the e-bike in general and in traffic. While the e-bikes provided were an appropriate size based on participants’ height, participants wanted to be able to fully place their feet on the ground. E-bike size concerns are not a commonly reported barrier to e-cycling and could be due to the characteristics of this sample. Specifically, the current sample were classified as obese and had extremely low fitness levels which could have negatively impacted balance (49). In addition, a type 2 diabetes diagnosis is associated with reduced balance (61–63). This reduced balance and low fitness could have meant participants found it hard to manage the weight of the e-bike when stopping and starting. In the current study the provision of a smaller frame size, which enabled the participant to fully plant their feet on the ground, was associated with increased confidence riding the e-bike and riding on roads. As such, the provision of smaller e-bike frames than is standard would likely increase riding confidence and engagement in e-cycling in this population.
4.3. Motivational factors that impact e-cycling
Participants were motivated to engage in e-cycling to improve their health as opposed to impacting the environment. This optimism regarding health was largely met, with participants perceiving improvements in fitness, mental health and diabetes management, findings echoed in previous e-cycling research (42). Engaging in e-cycling was perceived as an easier way of managing their diabetes than diet or other types of exercise, largely due to the enjoyment of riding. Enjoyment came from the ability to ride a bike comfortably due to less physical exertion than a conventional bicycle and the ability to ride further, faster and on hillier terrain than previously possible. These benefits are consistently reported in the e-cycling literature (34). A substantive body of literature now demonstrates that positive enjoyment during exercise is associated with greater future engagement (64) and is a unique aspect of e-cycling over other forms of active travel. High levels of enjoyment appeared to increase the habit of e-cycling in the current sample, with participants who felt e-cycling had become habit accumulating greater kilometres ridden than those who did not.
4.4. The need for social support
In the current sample, the degree to which support was required, or desired, varied based on level of experience and gender. Specifically, individuals with low levels of cycling experience, who were primarily women, required and desired more practical support from both the instructor and friends and family. One participant attributed their inability to become an independent cyclist on a lack of social support in their personal life. In addition, women reported wanting to ride with friends or family to a greater extent than men. Conversely, men reported that e-cycling alone was relaxing and enjoyable. This has been reported in other e-cycling studies among older adults (58, 65). In the current study verbal support was less influential than practical support. This may be due to the higher-than-average rates of cycling in Bristol and potentially a community acceptance of cycling in general (66).
4.5. The impact of the natural and built environment
Access to safe parking infrastructure was a commonly reported barrier to utility e-cycling. Specifically, a lack of safe parking facilities and fear of theft negatively impacted riding. While these are commonly reported barriers to cycling (34, 67) these fears were exacerbated in the current study due to the e-bike not being owned by the participant and concerns over the financial implications of e-bike theft. While there is scant evidence of the impact of bicycle parking in cities on cycling behaviour, Heinen and colleagues report that the supply and quality of parking can impact cycling behaviour (68).
Home parking facilities were also a concern for some participants. Specifically, participants reported having to park the e-bike in the house and the effort required to get the bike in and out negatively impacted riding. Very little research has explored the impact of home parking facilities on cycling behaviour. This concern maybe more pertinent to e-bikes which are heavier and bulkier than conventional bicycles (69). In the current study two participants reported regularly commuting to work. These individuals reported having access to safe bicycle storage and showers and in one case the company had restricted car parking making e-cycling more attractive. Workplace facilities and polices such as these have been found to be positively associated with cycle commuting (70–73).
The cycling infrastructure to which an individual had access also impact riding. Specifically, participants were more willing to cycle when they had access to a segregated cycling path close to their home. Providing infrastructure that supports the needs of cyclists is recognised as a key strategy to encourage more cycling in cities (74–76). Two recent systematic reviews show that cycling behaviour increased following the introduction of new infrastructure or upgrading existing infrastructure (77, 78), however evaluation of environmental interventions is complex and findings vary based on the method of evaluation used (79).
Overall factors associated with the natural and built environment were instrumental in participants decision to engage in e-cycling or take an alternative mode of transport. In some cases, participants removed any notion of utility cycling and stuck to recreational rides due to these barriers, this was particularly relevant for individuals with no or little previous riding experience. While participants were encouraged to engage in problem solving and action planning to overcome such barriers, the extent to which individuals engaged in these activities at appropriate times is unknown.
4.6. The financial cost of e-bikes
Trialling an e-bike led to 12 of the 16 participants wanting to purchase an e-bike to continue riding, largely due to the high level of enjoyment. This is in line with other research which has reported that the desire to purchase an e-bike substantially increases following a e-bike trial and is associated with enjoyment, positive attitudes towards e-bikes and perceived benefits (59, 80). While many individuals are willing to pay the large expense of an e-bike (59, 80, 81) others, including individuals in this study, although willing, do not have the financial security to be able to purchase an e-bike (59). Following completion of a trial period, purchasing an e-bike has been reported to be an independent predictor of e-bike use over time (59) and is associated with reducing an individual's habitual use of the car (82). As such, ways of helping participants to view e-bikes as a financially viable option is of upmost importance.
4.7. Strengths and limitations
A strength of this research is the use of the TDF and COM-B to examine experiences of e-cycling in this population. To the authors’ knowledge this is the first time this framework and model have been used to explore peoples understanding and perception of e-cycling. Their use allow for the exploration of factors beyond skills and knowledge-based considerations and for the development of an understanding of the impact of context on e-cycling engagement. This information can be used to develop a programme theory, identifying hypothesised causal pathways, which can be tested in future trials. However, there are several limitations. Firstly, using the thematic approach means that data are combined and summarised, so that individual level detail maybe lost (83). In the current analysis the aim was to bring forward unique cases into the matrix and report these in the results. Secondly, thematic analysis focuses primarily on what the data show, thus failing to consider potential areas that are not discussed. While this is hard to avoid, use of the TDF ensured that a wide range of topics were covered. Thirdly, telephone interviews have been suggested to be inferior to face-to-face interviews due to a lack of visual cues, however, there is limited evidence to support this statement (84). Rather, telephone interviews may enable participants to share information more openly than face-to-face interviews, and participants maybe more relaxed when talking from the comfort of their own home (84). Fourthly, the role of the researcher may have impacted the data obtained, the analysis and the findings. The prior relationship that the researcher, who conducted the pilot RCT, had with participants may have impacted how participants responded to questions. To try and overcome this a distinction was made between the e-bike training and the study, to help the participant view them as different components to encourage honest opinions to be shared. Participants were asked to give frank answers to enable intervention improvements. In addition, the researchers who conducted the analysis were commuting cyclists at the time of the study. This may have influenced interpretation of the data. However, interpretations made by the researchers and reviewed by the participants showed consistency, therefore increasing the trustworthiness of the findings. Fifthly, 94% of the sample identified as White. As such, these findings cannot be generalised to other ethnicities. However, a strength of the study is the equal inclusion of men and women. Sixthly, 14 of the 16 participants had some degree of cycling experience, which may bias the identified barriers and facilitators to e-cycling reported and therefore the current findings cannot be generalised to individuals new to cycling. Individuals who had recent cycling experience (i.e., in the last two or three years) had greater perceived capability and confidence than those with little or no cycling experience. While one individual who had never previously cycled was unable to e-cycle following instruction. However, the degree to which previous cycling experience impacted current e-cycling behaviour depended largely on the individual and additional contextual factors.
4.8. Implications for future research
Using the information obtained from this analysis, researchers should refine the intervention to address some of the highlighted concerns using the Behaviour Change Wheel. Following refinement, a programme theory should be developed to generate hypotheses about how the intervention impacts cycling in this population. This can be used to guide the selection of quantitative mechanistic outcomes and contextual variables that should be examined in a future trial. Further research should be conducted to differentially examine the impact of such e-cycling interventions on individuals new to cycling or who have not ridden for a considerable amount of time, as the degree of training required appears to be different to those who are confident with cycling. In addition, such an intervention should be trialled in different populations to allow comparison of experiences.
While training is important, it needs to be part of a multifaceted approach including improving infrastructure and introducing policy to encourage e-cycling engagement. Future research should involve working with stakeholders to establish how to address some of the contextual barriers to e-cycling, specifically cycling and parking infrastructure and traffic concerns, and the impact that addressing these components has on e-cycling engagement. In addition, means through which to address the financial cost of initiating e-cycling should be explored. Examining the relative impact of these micro-environmental, social and individual factors, and their associated costs, will provide guidance on how best to promote e-cycling in the future and highlight the potential for scalability.
5. Conclusion
Findings from this study provide insight into the personal, social and environmental factors that individuals with type 2 diabetes report as barriers and facilitators to e-cycling. Using the TDF and COM-B model is a starting point to understanding e-cycling in the current context and identifying what needs to change to modify the behaviour. This can inform the development of a conceptual framework which hypothesizes how these factors impact one another to influence e-cycling behaviour. This is the first step in developing an understanding of the mechanisms through which the e-bike training impacts individual capability and motivation, and identifying the importance of different environmental and social factors on e-cycling engagement. The findings of this study can be used to improve the quality of bicycle skills training currently being offered and to guide the selection of mechanistic outcome measures for future evaluation, guide scale-up to other locations and inform policymakers of what further actions need to be taken to enable people to adopt bicycling.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by NHS Health Research Authority Southwest/Central Bristol Research Ethics Committee (Ref: 18/SW/0164). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JB designed the study. SL, CE and AS contributed to the design of the study. JB collected the data. JB and AS analysed the data. JB drafted the full manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the NIHR Biomedical Research Centre at University Hospitals Bristol and Weston NHS Foundation Trust and the University of Bristol. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2023.1150724/full#supplementary-material
References
1. Almdal T, Scharling H, Jensen J, Vestergaard H. The independent effect of type 2 diabetes mellitus on ischemic heart disease, stroke, and death: a population-based study of 13 000 men and women with 20 years of follow-up. Arch Intern Med. (2004) 164(13):1422–6. doi: 10.1001/archinte.164.13.1422
2. Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. (1998) 339(4):229–34. doi: 10.1056/NEJM199807233390404
3. The Emerging Risk Factors Collaboration. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. (2010) 375(9733):2215–22. doi: 10.1016/S0140-6736(10)60484-9
4. Trikkalinou A, Papazafiropoulou AK, Melidonis A. Type 2 diabetes and quality of life. World J Diabetes. (2017) 8(4):120–9. doi: 10.4239/wjd.v8.i4.120
5. Mommersteeg PMC, Herr R, Pouwer F, Holt RIG, Loerbroks A. The association between diabetes and an episode of depressive symptoms in the 2002 world health survey: an analysis of 231 797 individuals from 47 countries. Diabetic Med. (2013) 30(6):e208–e14. doi: 10.1111/dme.12193
6. Adler AI, Stevens RJ, Manley SE, Bilous RW, Cull CA, Holman RR, et al. Development and progression of nephropathy in type 2 diabetes: the United Kingdom prospective diabetes study (UKPDS 64). Kidney Int. (2003) 63(1):225–32. doi: 10.1046/j.1523-1755.2003.00712.x
7. Ogurtsova K, Fernandes JD dR, Huang Y, Linnenkamp U, Guariguata L, Cho NH, et al. IDF diabetes atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. (2017) 128(Suppl C):40–50. doi: 10.1016/j.diabres.2017.03.024
8. Hex N, Bartlett C, Wright D, Taylor M, Varley D. Estimating the current and future costs of type 1 and type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs. Diabetic Med. (2012) 29(7):855–62. doi: 10.1111/j.1464-5491.2012.03698.x
9. Knowler WC, Barrett-Connor E, Fowler SE, DPPR Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. (2002) 346(6):393–403. doi: 10.1056/NEJMoa012512
10. Orchard TJ, Temprosa M, Barrett-Connor E, Fowler S, Goldberg R, Mather K, et al. Long-term effects of the diabetes prevention program interventions on cardiovascular risk factors: a report from the DPP outcomes study. Diabetic Med. (2013) 30(1):46–55. doi: 10.1111/j.1464-5491.2012.03750.x
11. Lindström J, Louheranta A, Mannelin M, Rastas M, Salminen V, Eriksson J, et al. The Finnish diabetes prevention study (DPS). Diabetes Care. (2003) 26(12):3230. doi: 10.2337/diacare.26.12.3230
12. Colberg SR, Sigal RJ, Yardley JE, Riddell MC, Dunstan DW, Dempsey PC, et al. Physical activity/exercise and diabetes: a position statement of the American diabetes association. Diabetes Care. (2016) 39(11):2065–79. doi: 10.2337/dc16-1728
13. Umpierre D, Ribeiro PA, Kramer CK, Leitao CB, Zucatti AT, Azevedo MJ, et al. Physical activity advice only or structured exercise training and association with HbA1c levels in type 2 diabetes: a systematic review and meta-analysis. JAMA. (2011) 305(17):1790–9. doi: 10.1001/jama.2011.576
14. Morrato EH, Hill JO, Wyatt HR, Ghushchyan V, Sullivan PW. Physical activity in U.S. adults with diabetes and at risk for developing diabetes, 2003. Diabetes Care. (2007) 30(2):203–9. doi: 10.2337/dc06-1128
15. Brawner CA, Churilla JR, Keteyian SJ. Prevalence of physical activity is lower among individuals with chronic disease. Med Sci Sports Exerc. (2016) 48(6):1062–7. doi: 10.1249/MSS.0000000000000861
16. Steeves JA, Murphy RA, Crainiceanu CM, Zipunnikov V, Van Domelen DR, Harris TB. Daily patterns of physical activity by type 2 diabetes definition: comparing diabetes, prediabetes, and participants with normal glucose levels in NHANES 2003–2006. Prev Med Rep. (2015) 2:152–7. doi: 10.1016/j.pmedr.2015.02.007
17. Haghighi M M, Mavros Y, Fiatarone Singh MA. The effects of structured exercise or lifestyle behavior interventions on long-term physical activity level and health outcomes in individuals with type 2 diabetes: a systematic review, meta-analysis, and meta-regression. J Phys Act Health. (2018) 15:1–11. doi: 10.1123/jpah.2017-0589
18. Wing RR, Bahnson JL, Bray GA, Clark JM, Coday M, Egan C, et al. Long-term effects of a lifestyle intervention on weight and cardiovascular risk factors in individuals with type 2 diabetes mellitus: four-year results of the look AHEAD trial. Arch Intern Med. (2010) 170(17):1566–75. doi: 10.1001/archinternmed.2010.334
19. Hobbs N, Godfrey A, Lara J, Errington L, Meyer TD, Rochester L, et al. Are behavioral interventions effective in increasing physical activity at 12 to 36 months in adults aged 55 to 70 years? A systematic review and meta-analysis. BMC Med. (2013) 11(1):75. doi: 10.1186/1741-7015-11-75
20. National Institute for Health and Care Excellence. Physical activity: Walking and cycling. London, UK: National Institute for Health and Care Excellence (2012).
21. World Health Organization. Global action plan on physical activity 2018–2030: more active people for a healthier world. Geneva, Switerland: World Health Organization (2018).
22. Falconer CL, Cooper AR, Flint E. Patterns and correlates of active commuting in adults with type 2 diabetes: cross-sectional evidence from UK biobank. BMJ Open. (2017) 7:e017132. doi: 10.1136/bmjopen-2017-017132
23. Department for Transport. Walking and cycling statistics, England: 2019. London, UK: Department for Transport (2020).
24. Ministry of Transport. New Zealand household travel survey 2015−2017. Wellington, New Zealand: Minstry of Transport (2017).
25. Cooper J, Corcoran J. Census of population and housing: commuting to work—more stories from the census, 2016. Canberra, Australia: Australian Bureau of Statistics (2018).
26. Rissel CE, New C, Wen LM, Merom D, Bauman AE, Garrard J. The effectiveness of community-based cycling promotion: findings from the cycling connecting communitiesproject in Sydney, Australia. Int J Behav Nutr Phys Act. (2010) 7(1):8. doi: 10.1186/1479-5868-7-8
27. Transport for London. Adult cycle training monitoring final report financial year 2014/15. London, UK: Transport for London (2016).
28. Yang L, Sahlqvist S, McMinn A, Griffin SJ, Ogilvie D. Interventions to promote cycling: systematic review. Br Med J. (2010) 341:c5293. doi: 10.1136/bmj.c5293
29. Sersli S, DeVries D, Gislason M, Scott N, Winters M. Changes in bicycling frequency in children and adults after bicycle skills training: a scoping review. Transp Res Part A Policy Pract. (2019) 123:170–87. doi: 10.1016/j.tra.2018.07.012
30. Rissel C, Watkins G. Impact on cycling behavior and weight loss of a national cycling skills program (AustCycle) in Australia 2010–2013. J Transp Health. (2014) 1(2):134–40. doi: 10.1016/j.jth.2014.01.002
31. Jones CHD, Ogilvie D. Motivations for active commuting: a qualitative investigation of the period of home or work relocation. Int J Behav Nutr Phys Act. (2012) 9(1):109. doi: 10.1186/1479-5868-9-109
32. de Geus B, Hendriksen I. Cycling for transport, physical activity and health: what about pedelecs? In: Gerike R, Parkin J, editors. Cycling futures: from research into practice. 1st ed Farnham: Routledge (2015):17–31.
33. Bourne JE, Sauchelli S, Perry R, Page A, Leary S, England C, et al. Health benefits of electrically-assisted cycling: a systematic review. Int J Behav Nutr Phys Act. (2018) 15(116):1–15. doi: 10.1186/s12966-018-0751-8
34. Bourne JE, Cooper AR, Kelly P, Kinnear FJ, England C, Leary S, et al. The impact of e-cycling on travel behaviour: a scoping review. J Transp Health. (2020) 19:100910. doi: 10.1016/j.jth.2020.100910
35. Castro A, Gaupp-Berhausen M, Dons E, Standaert A, Laeremans M, Clark A, et al. Physical activity of electric bicycle users compared to conventional bicycle users and non-cyclists: insights based on health and transport data from an online survey in seven European cities. Transp Res Interdiscip Perspect. (2019) 1:1–10. doi: 10.1016/j.trip.2019.100017
36. Söderberg f.k.a. Andersson A, Adell E, Winslott Hiselius L. What is the substitution effect of e-bikes? A randomised controlled trial. Transp Res D Transp Environ. (2021) 90:102648. doi: 10.1016/j.trd.2020.102648
37. Stenner HT, Boyen J, Hein M, Protte G, Kück M, Finkel A, et al. Everyday pedelec use and its effect on meeting physical activity guidelines. Int J Environ Res Public Health. (2020) 17(13):1–9. doi: 10.3390/ijerph17134807
38. MacArthur J, Cherry C, Harpool M, Scheppke D. A north american survey of electric bicycle owners. NITC-RR-1041. Portland, OR: Transportation Research and Education Center (TREC) (2018). doi: 10.15760/trec.197
39. Popovich N, Gordon E, Shao Z, Xing Y, Wang Y, Handy S. Experiences of electric bicycle users in the Sacramento, California area. Travel Behav Soc. (2014) 1(2):37–44. doi: 10.1016/j.tbs.2013.10.006
40. Jones T, Harms L, Heinen E. Motives, perceptions and experiences of electric bicycle owners and implications for health, wellbeing and mobility. J Transp Geogr. (2016) 53:41–9. doi: 10.1016/j.jtrangeo.2016.04.006
41. Boland P, Connell L, Thetford C, Janssen J. Exploring the factors influencing the use of electrically assisted bikes (e-bikes) by stroke survivors: a mixed methods multiple case study. Disabil Rehabil. (2020) 44:1–10. doi: 10.1080/09638288.2020.1817986
42. Searle A, Ranger E, Zahra J, Tibbitts B, Page A, Cooper A. Engagement in e-cycling and the self-management of type 2 diabetes: a qualitative study in primary care. BJGP Open. (2019) 3(2):1–9. doi: 10.3399/bjgpopen18X101638
43. Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of medical research council guidance. Br Med J. (2021) 374:n2061. doi: 10.1136/bmj.n2061
44. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new medical research council guidance. Br Med J. (2008) 337:a1655. doi: 10.1136/bmj.a1655
45. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. (2011) 6:42. doi: 10.1186/1748-5908-6-42
46. Howlett N, Trivedi D, Troop NA, Chater AM. Are physical activity interventions for healthy inactive adults effective in promoting behavior change and maintenance, and which behavior change techniques are effective? A systematic review and meta-analysis. Transl Behav Med. (2019) 9(1):147–57. doi: 10.1093/tbm/iby010
47. Michie S, Johnston M, Abraham C, Lawton R, Parker D, Walker A. Psychological theory group. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care. (2005) 14(1):26–33. doi: 10.1136/qshc.2004.011155
48. Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. (2012) 7(37):1–17. doi: 10.1186/1748-5908-7-37
49. Bourne JE, Leary S, Page A, Searle A, England C, Thompson D, et al. Electrically assisted cycling for individuals with type 2 diabetes mellitus: a pilot randomized controlled trial. Pilot Feasibility Stud. (2023) 9:1–19. doi: 10.1186/s40814-023-01283-5
50. Canadian Society of Exercise Physiology. Get active questionnaire. Canada: Canadian Society of Exercise Physiology (2017). Available at: https://www.csep.ca/CMFiles/GAQ_CSEPPATHReadinessForm_2pages.pdf
51. Atkins L, Francis J, Islam R, O'Connor D, Patey A, Ivers N, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implement Sci. (2017) 12:77. doi: 10.1186/s13012-017-0605-9
52. Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Burgess A, editors. Analysing qualitative data. London: Routledge (1994). p. 173–94.
53. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. (2013) 13(1):117. doi: 10.1186/1471-2288-13-117
54. Spencer L, Ritchie J, Ormston R, O'Connor W, Barnard M. Analysis: principles and processes. In Qualitative research practice. A guide for social science students & researchers. Ritchie J, Lewis J, McNaughton Nicholls C, Ormston R (Editors). 2nd ed London, UK: Sage (2014).
55. Smith J, Firth J. Qualitative data analysis: the framework approach. Nurse Res. (2011) 18(2):52–62. doi: 10.7748/nr2011.01.18.2.52.c8284
56. Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. (2005) 15(9):1277–88. doi: 10.1177/1049732305276687
57. Bourne JE, Page A, Leary S, Andrews RC, England C, Cooper AR. Electrically assisted cycling for individuals with type 2 diabetes mellitus: protocol for a pilot randomized controlled trial. Pilot Feasibility Stud. (2019) 5(1):136. doi: 10.1186/s40814-019-0508-4
58. Spencer B, Jones T, Leyland L-A, van Reekum CM, Beale N. ‘Instead of “closing down” at our ages … we’re thinking of exciting and challenging things to do’: older people's Microadventures outdoors on (e-)bikes. J Adventure Educ Outdoor Learn. (2019) 19(2):124–39. doi: 10.1080/14729679.2018.1558080
59. Ton D, Duives D. Understanding long-term changes in commuter mode use of a pilot featuring free e-bike trials. Transp Policy (Oxf). (2021) 105:134–44. doi: 10.1016/j.tranpol.2021.03.010
60. Johnson R, Margolis S. A review of the effectiveness of adult cycle training in tower hamlets, London. Transp Policy (Oxf). (2013) 30:254–61. doi: 10.1016/j.tranpol.2013.09.005
61. Schwartz AV, Vittinghoff E, Sellmeyer DE, Feingold KR, Rekeneire ND, Strotmeyer ES, et al. Diabetes-related complications, glycemic control, and falls in older adults. Diabetes Care. (2008) 31(3):391. doi: 10.2337/dc07-1152
62. D'Silva LJ, Lin J, Staecker H, Whitney SL, Kluding PM. Impact of diabetic complications on balance and falls: contribution of the vestibular system. Phys Ther. (2016) 96(3):400–9. doi: 10.2522/ptj.20140604
63. Morrison S, Colberg SR, Parson HK, Vinik AI. Relation between risk of falling and postural sway complexity in diabetes. Gait Posture. (2012) 35(4):662–8. doi: 10.1016/j.gaitpost.2011.12.021
64. Rhodes RE, Kates A. Can the affective response to exercise predict future motives and physical activity behavior? A systematic review of published evidence. Ann Behav Med. (2015) 49(5):715–31. doi: 10.1007/s12160-015-9704-5
65. Van Cauwenberg J, De Bourdeaudhuij I, Clarys P, de Geus B, Deforche B. E-bikes among older adults: benefits, disadvantages, usage and crash characteristics. Transportation (Amst). (2018) 46:2151–72. doi: 10.1007/s11116-018-9919-y
67. Heinen E, van Wee B, Maat K. Commuting by bicycle: an overview of the literature. Transport Reviews. (2010) 30(1):59–96. doi: 10.1080/01441640903187001
68. Heinen E, Buehler R. Bicycle parking: a systematic review of scientific literature on parking behaviour, parking preferences, and their influence on cycling and travel behaviour. Transport Reviews. (2019) 39(5):630–56. doi: 10.1080/01441647.2019.1590477
69. Fishman E, Cherry C. E-bikes in the mainstream: reviewing a decade of research. Transport Reviews. (2016) 36(1):72–91. doi: 10.1080/01441647.2015.1069907
70. Porter AK, Kohl HW, Salvo D. Dose-response association of workplace facilities and policies with commuter bicycling among adults. J Transp Health. (2019) 14:100603. doi: 10.1016/j.jth.2019.100603
71. Heinen E, Maat K, van Wee B. The effect of work-related factors on the bicycle commute mode choice in The Netherlands. Transportation (Amst). (2013) 40(1):23–43. doi: 10.1007/s11116-012-9399-4
72. Hipp JA, Dodson EA, Lee JA, Marx CM, Yang L, Tabak RG, et al. Mixed methods analysis of eighteen worksite policies, programs, and environments for physical activity. Int J Behav Nutr Phys Act. (2017) 14(1):79. doi: 10.1186/s12966-017-0533-8
73. Knott CS, Sharp SJ, Mytton OT, Ogilvie D, Panter J. Changes in workplace car parking and commute mode: a natural experimental study. J Epidemiol Community Health. (2019) 73(1):42. doi: 10.1136/jech-2018-210983
74. Dill J. Bicycling for transportation and health: the role of infrastructure. J Public Health Policy. (2009) 30:S95–110. doi: 10.1057/jphp.2008.56
75. Garrard J, Rose G, Lo SK. Promoting transportation cycling for women: the role of bicycle infrastructure. Prev Med. (2008) 46(1):55–9. doi: 10.1016/j.ypmed.2007.07.010
76. Pucher J, Buehler R. Making cycling irresistible: lessons from The Netherlands, Denmark and Germany. Transport Reviews. (2008) 28(4):495–528. doi: 10.1080/01441640701806612
77. Stappers NEH, Van Kann DHH, Ettema D, De Vries NK, Kremers SPJ. The effect of infrastructural changes in the built environment on physical activity, active transportation and sedentary behavior—a systematic review. Health Place. (2018) 53:135–49. doi: 10.1016/j.healthplace.2018.08.002
78. Panter J, Guell C, Humphreys D, Ogilvie D. Can changing the physical environment promote walking and cycling? A systematic review of what works and how. Health Place. (2019) 58:102161. doi: 10.1016/j.healthplace.2019.102161
79. Mölenberg FJM, Panter J, Burdorf A, van Lenthe FJ. A systematic review of the effect of infrastructural interventions to promote cycling: strengthening causal inference from observational data. Int J Behav Nutr Phys Act. (2019) 16(1):93. doi: 10.1186/s12966-019-0850-1
80. Simsekoglu Ö, Klöckner C. Factors related to the intention to buy an e-bike: a survey study from Norway. Transp Res F: Traffic Psychol. (2019) 60:573–81. doi: 10.1016/j.trf.2018.11.008
81. Fyhri A, Heinen E, Fearnley N, Sundfør HB. A push to cycling—exploring the e-bike’s Role in overcoming barriers to bicycle use with a survey and an intervention study. Int J Sustain Transp. (2017) 11(9):681–95. doi: 10.1080/15568318.2017.1302526
82. Moser C, Yann B, Hille S. E-bike trials’ potential to promote sustained changes in car owners’ mobility habits. Environ Res Lett. (2018) 13:1–6. doi: 10.1088/1748-9326/aaad73
83. Creswell JW. Research design: qualitative, quantitative, and mixed methods approaches. 3rd ed Thousand Oaks, CA, US: Sage Publications, Inc (2009).
Keywords: e-cycling, perceptions, physical activity, type 2 diabetes, qualitative
Citation: Bourne JE, Leary S, England C and Searle A (2023) ‘‘I felt marvellous e-cycling. If I had long hair I would have flicked it”: a qualitative investigation of the factors associated with e-cycling engagement among adults with type 2 diabetes. Front. Sports Act. Living 5:1150724. doi: 10.3389/fspor.2023.1150724
Received: 24 January 2023; Accepted: 11 September 2023;
Published: 29 September 2023.
Edited by:
Jenna McVicar, Deakin University, AustraliaReviewed by:
Annika Frahsa, University of Bern, SwitzerlandMatthew Ahmadi, The University of Sydney, Australia
© 2023 Bourne, Leary, England and Searle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jessica E. Bourne SmVzc2ljYS5ib3VybmVAYnJpc3RvbC5hYy51aw==