 Sheila Geiger1,2*
Sheila Geiger1,2* Julia Aufderlandwehr1,2
Julia Aufderlandwehr1,2 Anna Julia Esser1,2
Anna Julia Esser1,2 Theresa Schadendorf1,2
Theresa Schadendorf1,2 Thomas Muehlbauer3
Thomas Muehlbauer3 Eva-Maria Skoda1,2
Eva-Maria Skoda1,2 Martin Teufel1,2
Martin Teufel1,2 Alexander Bäuerle1,2
Alexander Bäuerle1,2
- 1Clinic for Psychosomatic Medicine and Psychotherapy, LVR-University Hospital Essen, University of Duisburg-Essen, Essen, Germany
- 2Center for Translational Neuro- and Behavioral Sciences (C-TNBS), University of Duisburg-Essen, Essen, Germany
- 3Division of Movement and Training Sciences/Biomechanics of Sport, University of Duisburg-Essen, Essen, Germany
Background: Elite athletes are exposed to many different sport-specific stressors that may put them at particular risk for mental health symptoms and disorders. E-mental health interventions could be a feasible option to support elite athletes in need. The aim of the present study was to assess the acceptance of e-mental health interventions among elite athletes and explore its underlying drivers and barriers.
Materials and methods: A cross-sectional study was conducted with N = 382 elite athletes. Of these, N = 275 (71.99%, 167 females) were included in the statistical analyses. The impact of various sociodemographic, sport-related and medical characteristics on acceptance was assessed. EHealth-related data and acceptance of e-mental health interventions were examined using a modified assessment based on the Unified Theory of Acceptance and Use of Technology (UTAUT).
Results: Overall, the acceptance of e-mental health interventions in elite athletes can be classified as high (M = 3.69 SD = 0.97). In the UTAUT regression model sex, financial situation, depression symptoms, digital confidence, digital overload as well as the UTAUT predictors performance expectancy, effort expectancy, and social influence predicted acceptance significantly.
Conclusions: The UTAUT model has proven to be a valuable instrument in predicting of acceptance of e-mental health interventions in elite athletes. Given the strong association between acceptance and future use, new interventions should focus on the explored factors to establish effective e-mental health interventions for elite athletes.
1 Introduction
Participation in elite sports requires rigorous training, physical fitness, and mental toughness. Alongside these demanding requirements, elite athletes often experience significant psychological distress, including anxiety, depression, and sleep disturbance (1). Sport-specific stressors, such as high levels of competition, injury, and pressure to perform might influence an elite athlete's career (2). According to a systematic review and meta-analysis (1) the prevalence of mental health symptoms and disorders may be slightly higher among current and former elite athletes when compared to the general population. Specifically, the prevalence ranged from 19% for alcohol misuse to 34% for anxiety and depression among active elite athletes, and from 16% for distress to 26% for anxiety and depression among former elite athletes (1). This variance reflects the different types of mental health challenges faced by athletes, emphasizing the need for effective psychological support to address these issues comprehensively. Moreover, the heterogeneity of existing studies highlights the need for further high-quality research in this field to better understand and address the mental health needs of elite athletes.
However, elite athletes, despite experiencing risk factors and mental health symptoms, are less inclined to seek professional help compared to the general population (3). This reluctance can be attributed to factors like fear of stigmatization, potential impact on performance and career, the perception of seeking help as a sign of weakness, and a lack of understanding of mental health (4, 5). Apart from the effects of stigma, there could be additional obstacles that contribute to the challenges of receiving psychotherapeutic treatment. These barriers encompass individual factors like limited awareness of treatment choices or motivational issues arising from extended waiting periods to start treatment. Structural barriers, such as inadequate cross-sector coordination, limited availability of care options in specific regions, and prolonged waiting periods for psychotherapy appointments, also contribute to the issue (6).
To overcome these barriers and improve access to mental health care, innovative e-mental health solutions have emerged as a promising strategy. The term “eHealth” broadly encompasses the use of electronic devices such as cell phones and computers to enhance medical care (7). EHealth interventions can be divided between self-help methods, computer-assisted treatments, and telehealth services. Self-help methods involve self-guided efforts to cope with (mental) health issues, often through self-help books or online programs (8, 9). Computer-assisted treatments use computer programs to deliver aspects of psychotherapy directly to patients (10, 11). Telehealth services, as defined by the WHO (12), involve the delivery of health care services where patients and providers are separated by distance, using information and communication technology for diagnosis, treatment, and consultation. E-mental health interventions, i.e., the provision of mental health services via digital technologies, offer flexible, cost-effective, and accessible support, overcoming structural barriers and reaching a larger number of individuals compared to traditional face-to-face counselling (13, 14). Multiple studies investigating the efficacy of e-mental health interventions in treating various mental disorders and health-related outcomes have demonstrated outcomes similar to those achieved through in-person therapy (14–17). This study focuses on e-mental health interventions that fall under the category of telehealth.
Thus, e-mental health interventions have proven to be useful, but are not yet integrated into everyday life, as the utilization of specific e-mental interventions continues to be minimal (18–20). A key consideration regarding technology use is understanding individuals’ motivations for adopting it. The most important factor in this regard is the degree to which a technology is accepted. Previous studies show that the acceptance of e-mental health interventions is generally rather low (21–23) whereasore recent studies suggest that the acceptance of e-mental health interventions is generally rather moderate to high (24–28).
Hence, assessing the acceptance of e-mental health interventions as well as influencing factors among elite athletes is crucial. Until now, no research has been conducted using validated measurement methods to evaluate the acceptance of e-mental health interventions and its predictors among elite athletes. Consequently, the current study employs the Unified Theory of Acceptance and Use of Technology [UTAUT; (29)]. The UTAUT has been found to be a valuable framework for evaluating the acceptance of eHealth-interventions in a number of studies (22, 23, 30, 31). The UTAUT model identifies three key factors that contribute to an individual's acceptance (or behavioral intention) of any technology: performance expectancy, effort expectancy, and social influence. Performance expectancy refers to the extent to which a person believes they will benefit from using the technology, while effort expectancy measures the ease of use associated with the technology, and social influence reflects the degree to which important others, such as family or friends, believe the person should use the technology.
Based on previous research that has explored acceptance in other populations, this study aims to fill the gap by setting forth the following objectives: The first objective is to assess the level of acceptance of e-mental health interventions in elite athletes. The second objective is to evaluate whether acceptance levels of e-mental health interventions vary among elite athletes based on sociodemographic, eHealth, or sport-related factors. The third objective is to explore the factors that influence the acceptance of e-mental health interventions among elite athletes.
2 Materials and methods
2.1 Study design and participants
The study was carried out as a web-based, cross-sectional survey among German adult (aged ≥18 years) elite athletes from December 2021 to December 2022. The criteria for elite athletes were determined, in part, by the International Olympic Committee's consensus statement and included (1) alignment of life to sports, (2) striving for excellence, and (3) participation in professional or Olympic competitions (32–34). Participants were recruited through regional and national sport clubs and associations, social media and coaches. The participation was anonymous and voluntary and there was no financial or material incentive offered. Furthermore, before starting the survey, electronic informed consent was obtained. The setup of the study was developed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Faculty of Medicine of the University of Duisburg-Essen (19-8947-BO). The survey was answered by 382 participants, but 29 (7.59%) of them were under 18 years old and 78 (20.42%) did not meet the criteria of elite athletes, resulting in their exclusion at the start of the survey. Therefore, the final sample size for data analysis comprised 275 participants.
2.2 Measures
2.2.1 Sociodemographic and sport-related data
In this study, sociodemographic data was collected through self-reported measures, including chronological age, sex, level of education and living as well as family and employment status. Financial situation was assessed on a 10-point-Likert scale (0 = “I barely get by”, 10 = “I don't have to restrict myself in any way”). Moreover, sport-related variables, including type of sport, years in elite sport, days at home during the last month as well as earning a living through sport, were assessed.
2.2.2 Psychometric data
The Patient Health Questionnaire-8 (PHQ-8) was used to assess depression symptoms (35). This questionnaire comprises eight items, and participants responded using a four-point Likert scale (0 = never to 3 = almost every day). The internal consistency of the PHQ-8 in this study was found to be high (Cronbach's α = 0.85). The Generalized Anxiety Disorder Scale-7 (GAD-7) is a validated (36) instrument to assess symptom severity and probability of GAD. It contains seven items, each scored from 0 to 3, indicating the frequency of symptoms experienced over the past 2 weeks. A score of 0 means the symptom has not been experienced at all while a score of 3 stands for a daily occurrence of the symptom. Cronbach's α in our study was high (α = 0.85).
2.2.3 eHealth-related data
To assess eHealth-related data, participants rated three items regarding their digital confidence (use of digital media, online platforms, and digital devices) on a five-point Likert scale (1 = not confident at all, 5 = very confident). The internal consistency of this scale was found to be excellent (Cronbach's α = 0.90). Moreover, three self-generated items were utilized to measure internet anxiety, which is defined as the fear or apprehension that individuals experience when using the internet (37). Participants provided responses on a five-point Likert scale (e.g., “I have concerns about using the internet”, 1 = does not apply to me, 5 = does apply to me). The internal consistency of this scale was found to be high (Cronbach's α = 0.80). Additionally, we used three self-generated items with a five-point Likert scale to assess digital overload, defined as the stress and burden felt due to the constant accessibility and constant use of digital devices (e.g., “I feel burdened by the constant accessibility via cell phone or mail”, 1 = does not apply to me, 5 = does apply to me). Cronbach's α was sufficient [α = 0.73; (38)]. All scales used in the study have been well-established through their application in prior research studies (24–26, 39).
2.2.4 Acceptance and UTAUT predictors
To measure the acceptance towards e-mental health interventions a modified questionnaire based on the UTAUT was applied (40). The modified UTAUT questionnaire comprises 14 items that are rated on a five-point Likert scale (0 = strongly disagree, 4 = strongly agree). The dependent variable in this study is acceptance, operationalized as behavioural intention (e.g., “I would like to try a psychological online intervention”), which was assessed using four items. The internal consistency of acceptance (behavioural intention) was found to be excellent (Cronbach's α = 0.90). The two UTAUT predictors, effort expectancy (e.g., “Using a psychological online intervention would not be an additional burden for me”) and social influence (e.g., “My coach would approve the use of a psychological online intervention”), were each measured using three items and demonstrated the following internal consistencies: Cronbach's α = 0.63 for effort expectancy and α = 0.85 for social influence. While the Cronbach's α for effort expectancy is relatively low, which may indicate questionable internal consistency, this finding contrasts with previous studies where the scale has shown adequate reliability (31). Performance expectancy (e.g., “A psychological online intervention could help me improve my mental health”) was assessed using four items and exhibited excellent internal consistency (Cronbach's α = 0.91).
2.3 Statistical analysis
The statistical analyses were performed using version 26 of SPSS Statistics by IBM in New York, NY, USA and RStudio version 4.0.2 by RStudio PBC in Boston, MA, USA. Firstly, the internal consistencies of various psychometric questionnaires were determined, and descriptive statistics were calculated. Additionally, in accordance with prior research, acceptance (BI) was classified into low (1.00–2.34), moderate (2.35–3.67), and high (3.68–5.00) categories (23, 26–28). The sum scores for the GAD-7 and PHQ-8 scales were computed. Mean acceptance (BI) differences between groups based on sociodemographic, sport- and eHealth-related data were examined using t-tests and ANOVAs, with the latter being used for variables with multiple categories. The level of significance was established at α = 0.05 (two-sided test). Post-hoc tests were conducted following the mean comparisons, and α correction was implemented using the Bonferroni method. Considering the present sample size (N = 275), normal distribution in the variables was assumed [see central limit theorem; (41)]; hence, parametric tests were used. We conducted a hierarchical regression analysis, following approaches in comparable literature, to maintain consistency and comparability of results (23, 25, 26, 39, 40, 42). The blocks were structured as follows: (1) sociodemographic and sport-related variables to control for baseline characteristics, (2) mental health variables to account for psychological factors, (3) eHealth-related variables to capture digital engagement, and (4) UTAUT predictors to assess technology acceptance factors.
3 Results
3.1 Sample characteristics
The participants (N = 275; 167 females) were M = 23.65 years old (SD = 6.29), while three quarters of the sample were 18–25 years old. 42.5% of the athletes rated their financial situation as okay or better (M = 6.95; SD = 2.09). Regarding the type of sports, 133 participants were active in team sports, while 190 did individual sports and 47 athletes participated in both. On average, the athletes were active in elite sport for 9.69 years (SD = 5.25) and spent an average of 21.79 (SD = 7.42) days at home in the last month. The participants reported high digital confidence (M = 4.12; SD = 0.73) and low internet anxiety (M = 1.84; SD = 0.80), while their digital overload was moderate (M = 2.71; SD = 0.96). See Table 1 for a full description of the study population.
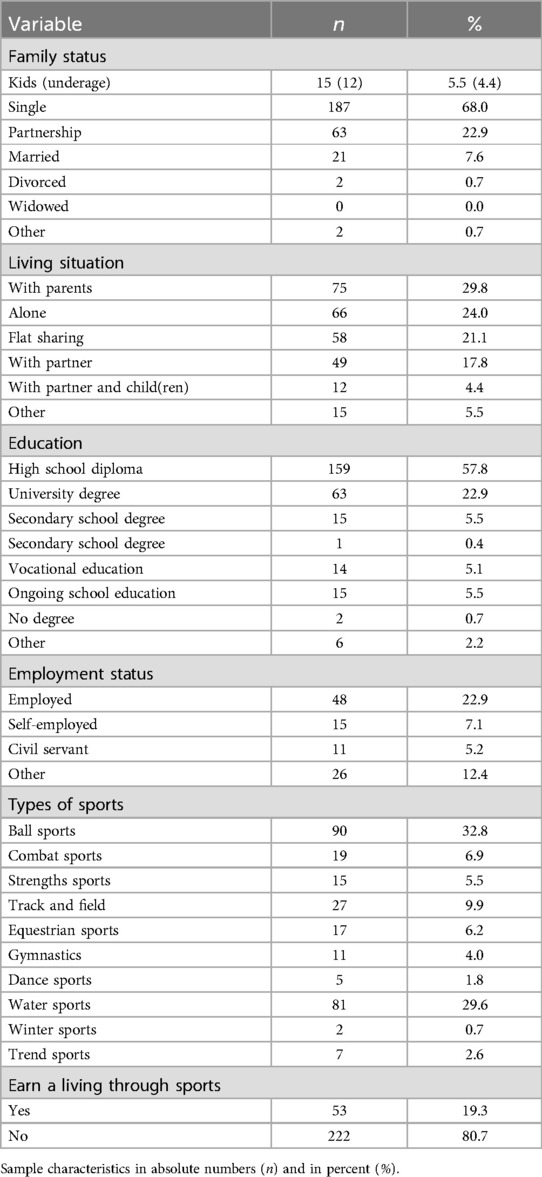
Table 1. Description of the study sample (N = 275).
3.2 Research objective 1 and 2: acceptance of eHealth-interventions and influencing factors
The general acceptance of e-mental health interventions was high (M = 3.69 SD = 0.97). Regarding the degree of acceptance, the sample of 275 participants was categorized into groups as follows: 35 (12.7%) participants showed low, 65 (23.6%) showed moderate, and 175 (63.6%) showed high acceptance.
There was a significant difference in acceptance between female and male participants (t189.07 = −2.48; p = .014), with females showing higher acceptance than males. In addition, elite athletes in individual sports were found to have significantly higher acceptance scores compared to those who participate in team sports (F2,272 = 3.47; p = .032). However, acceptance did not differ between living situations. A report summarizing the results regarding differences in acceptance is presented in Supplementary Table S1.
3.3 Research objective 3: predictors of acceptance
In the multiple hierarchical regression analysis, it was shown that sociodemographic predictors explained 7.3% of the variance in acceptance in the first step (R2 = 0.073; F6,268 = 3.512; p = 0.002). Of the sociodemographic predictors sex (β = 0.144; p = 0.017) and financial situation predicted acceptance significantly (β = −0.210; p < 0.001). In the second step, mental health variables explained another 6.8% of the variance in acceptance (Δ R² = 0.068; F8,266 = 5.453; p < 0.001). In detail, depression symptoms significantly predicted acceptance (β = 0.261; p = 0.013), whereas presence of generalized anxiety symptoms was no significant predictor of acceptance (p = 0.818). In the third step, eHealth-related variables were included and explained another 4.9% of variance (Δ R² = 0.049; F11,263 = 5.592; p = 0.002). Digital overload (β = 0.149; p = 0.024) and digital confidence (β = 0.145; p = 0.013) predicted acceptance significantly, whereas internet anxiety was no significant predictor of acceptance (p = 0.127). In the last step, UTAUT predictors explained 47.4% (Δ R² = 0474; F14,260 = 36.702; p < 0.001) of the variance resulting in a total explained variance in acceptance of 66.4%. Of the variables included in step four, performance expectancy (β = 0.477; p < 0.001), effort expectancy (β = 0.192; p < 0.001), and social influence (β = 0.203; p < 0.001) significantly predicted acceptance. Table 2 displays the parameters of the hierarchical regression model of acceptance.
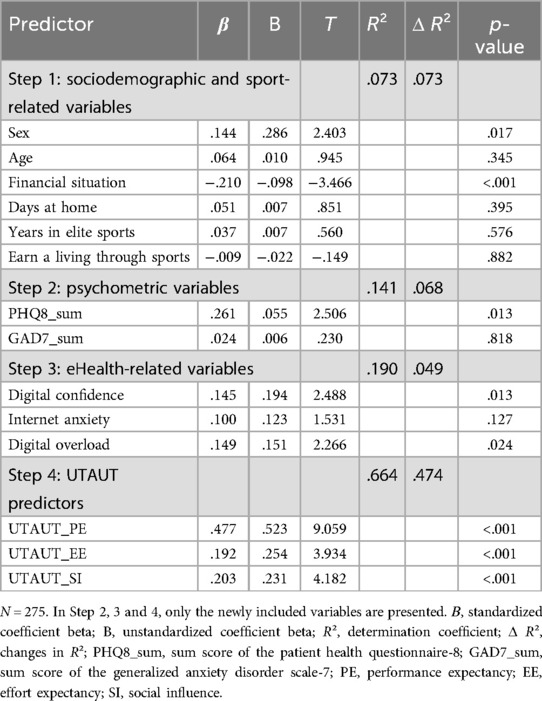
Table 2. Hierarchical regression model of acceptance.
4 Discussion
4.1 Principal findings
E-mental health interventions are an effective alternative to personal therapy that combats stigma and ensures accessibility. Assessing the acceptance and predictors of these interventions is critical to future utilization and implementation. This study is the first to investigate this among elite athletes. General acceptance of e-mental health interventions among elite athletes was high, with 23.6% showing moderate and 63.6% showing high acceptance. Acceptance was associated with sex and being engaged in team or individual sports. In the multiple hierarchical regression analysis, sex, financial situation, depression symptoms, digital confidence, and digital overload were significant predictors of acceptance. Of the UTAUT predictors, performance expectancy, effort expectancy and social influence were significant predictors of acceptance and explained a high percentage of variance. The overall model provided 66.4% of explained variance in acceptance of e-mental health interventions.
Overall, acceptance levels in this study exceeded or were as high as those observed in previous studies similarly examining the acceptance of e-mental health interventions among various populations (24, 25–28, 39, 43), which can be a good prerequisite for the implementation and actual use of such interventions in elite sports. Especially for elite athletes who travel a lot, it can be beneficial to use treatment alternatives that are independent of location and time. An additional advantage is that the usage of mental health interventions can reduce fear of stigmatization. In line with this, Klein et al. (44) found that high levels of stigma were associated with a preference for e-mental health interventions.
4.2 Predictors of acceptance
Several predictors of acceptance have already been identified in various studies exploring the acceptance of e-mental health interventions among different samples. These predictors include sex (45, 46) and internet anxiety (47). The results of the present study also suggest that sex is a predictor for acceptance. Female athletes showed significantly higher acceptance than male athletes. There are studies that yield consistent results (24, 25), while others demonstrate no difference between sex (31, 48). The results can be explained by the observation that women have a more positive attitude towards seeking professional psychological help than their male counterparts (49). Moreover, our results align with research indicating that female elite athletes tend to report higher levels of psychological burden compared to their male counterparts (50, 51). Therefore, one could expect that psychologically burdened individuals would be particularly receptive to embracing new digital healthcare options. Interestingly, age did not emerge as a significant predictor in this study, which may be attributed to the relatively young average age of the sample, resulting in a more homogenous group with similar familiarity and comfort with digital technology. Also the sport-related variables (number of days spent at home, years in elite sports, and earning a living through sports) did not emerge as significant predictors of acceptance. This could be because these factors may not have a direct impact on the acceptance of e-mental health interventions. Athletes in different stages of their careers or with varying financial situations could experience similar needs and barriers regarding mental health interventions, leading to insufficient variation in these variables to produce significant results.
Digital confidence and digital overload emerged as further significant predictors of acceptance. Similarly, a potential explanation in this context could be that increased digital overload contributes to heightened psychological burden, consequently resulting in a greater willingness to accept e-mental health interventions. Moreover, individuals who are more confident in using digital media seem to accept them more. Conversely, individuals who lack digital confidence or have limited experience with digital media encounter significant barriers when accessing innovative e-mental health services. This may be because those more aware of their digital habits are also more receptive to solutions that can help manage their digital interactions. During the development of new e-mental health interventions, these varying capabilities should be taken into account. In contrast to previous research (47), internet anxiety was not found to be a significant predictor in this study. This might be because digital technologies have become increasingly commonplace, even in elite sports. The majority of athletes may possess sufficient digital competence, allowing them to overcome moderate internet anxiety when considering e-mental health interventions.
Another significant predictor of acceptance is the financial situation as assessed by the elite athletes. One possible reason for this observation could be that elite athletes who perceived their financial situation negatively experienced greater psychological burden. Consequently and in line with the other findings, they displayed a greater inclination towards accepting eHealth-interventions. Notably, the financial situation was found to be highly significant with a negative correlation coefficient, indicating that the worse the financial situation, the higher the acceptance of e-mental health interventions. This finding underscores the possibility that greater financial strain leads to increased psychological stress, thereby heightening acceptance. Consistent with this, depressive symptoms were also found to be an additional predictor of acceptance. Similar findings were also evident in other studies (24, 25, 46). In line with this, elite athletes showed significantly lower acceptance if they were engaged in team sports compared to individual sports. This fits with research showing that team athletes are less likely to suffer from anxiety or depression than individual athletes (52). Another plausible explanation could be that individual athletes spend significantly more time alone than team athletes and are therefore more receptive to e-mental-health interventions. Additionally, individual athletes may perceive higher levels of anonymity when using e-mental-health interventions, as there are fewer people who could potentially find out about their participation compared to those in team sports.
Regarding the UTAUT model, the results of this study provide strong support for the validity in measuring the acceptance of e-mental health interventions, supporting prior research outcomes (25, 53–56). Specifically, the key predictors, social influence, effort expectancy, and performance expectancy accounted for 66.4% of the variance in acceptance, demonstrating a high and comparable level of explained variance to the original UTAUT validation study (70%) conducted by Venkatesh, Morris (40). Moreover, performance expectancy emerged as the most important predictor of acceptance, with negative outcome expectations predicting lower intention to use, which is consistent with previous research findings (23, 25, 57, 58). Furthermore, this observation is consistent with literature indicating that performance expectancy is a predictor of treatment outcome in psychotherapy (59). The strong relationship between performance expectancy and the acceptance of e-mental health interventions (β 03D; 0.477; p < 0.001) emphasizes the necessity for transparent eHealth education that openly deals with misunderstandings or unrealistic expectations.
Social intention includes a person's belief that important people in his or her life, e.g., family or friends, would endorse the use of e-mental health interventions (40). This highlights the systemic dimension of person-environment interaction in the context of elite sport. Promoting acceptance can be facilitated by the positive attitudes of significant individuals toward e-mental health interventions and the willingness of physicians to recommend these programs. Specifically, general practitioners can play a vital role as key influencers in encouraging the adoption of eHealth solutions (60–62). A study by Van Voorhees, Hsiung (62) demonstrated that uptake of an e-mental health intervention increased when clinicians offered client-centered information which aimed to strengthen intrinsic motivation. Therefore, facilitation of acceptance needs to include relevant parties of health care (e.g., practitioners, clinicians, administrators) as important mediators of eHealth implementation.
In addition, it is critical to emphasize that consideration of the influencing factors of effort expectancy, performance expectancy, and social influence during the development and implementation phases is essential to improving acceptance. While these three key predictors are of utmost importance within the UTAUT model, our findings highlight the need to consider additional factors for a comprehensive understanding of acceptance and how to maximize it. Here, so-called acceptance facilitating interventions can be used to reduce people's fears and misconceptions about e-health interventions and thus increase acceptance (21, 22, 30).
The high acceptance of e-mental health interventions among elite athletes underscores their practical value. Coaches, sports staff, and medical professionals should integrate these tools into athletes’ routines and support their effective use. Addressing the identified significant predictors, such as digital confidence and depressive symptoms, is crucial when developing and implementing these interventions for this target group. Considering athletes’ travel schedules, it is essential that e-mental health solutions are accessible from any location. Emphasizing early detection, self-management skills, and support from key stakeholders can enhance the impact of these interventions (63). By implementing these strategies, e-mental health tools can more effectively address the mental health needs of elite athletes.
4.3 Limitations
Interpretation of our results should regard the following limitations. Firstly, our study design was a web-based cross-sectional study. The cross-sectional study design does not display any change over time and no statement to causality can be made. Longitudinal studies could address this limitation by tracking changes in acceptance and predictors over time. Because internet access was inevitable for participation, the sample of elite athletes who took part in our study might be more open minded about eHealth-interventions than the average elite athlete. As the sample was primarily made up of young people and the group of elite athletes tends to be younger and to have internet access, we do not really assume any bias here. Furthermore, it is likely that elite athletes who do not have much psychological support at this point in time are more interested in e-mental health interventions and show higher levels of acceptance than others. Another relevant factor might be that the study was conducted during different stages of the COVID-19 pandemic, a period marked by a rapid establishment and acceptance of digital patient care approaches (64). The pandemic highlighted the need for accessible psychological care as rates of depression, anxiety, and stress increased (65, 66). Additionally, high satisfaction with telemedicine during this time (67) suggests that the pandemic may have contributed to the observed higher acceptance of e-mental health interventions.
Since all data was self-reported, they are of limited reliability. For the evaluation of mental health, we used validated and established measures (GAD-7, PHQ-8), but it should be considered that all of these are symptom-based measures and therefore have a limited diagnostic accuracy. Another limitation is the low internal consistency of the effort expectancy scale (Cronbach's α = 0.63), which may affect its reliability. This was unexpected given its prior validation (31). Future research should revise or add items to improve the scale's reliability and ensure accurate measurement of effort expectancy in e-mental health interventions. As an operationalization of acceptance, we used behavioral intention. A prediction to actual use cannot be made because the intention to use does not always lead to actual use, known as the intention-behavior-gap (68). Further longitudinal research will be needed to assess how acceptance relates to actual behavior. We suggest measuring uptake rates and explore further barriers and incentives to use e-mental health interventions for elite athletes.
4.4 Conclusions
The results of this study support the assumption that elite athletes readily accept e-mental health interventions, providing a solid foundation for the integration of novel e-mental health interventions. Core predictors of acceptance included factors such as performance expectancy, effort expectancy, and social influence as well as depressive symptoms, digital confidence, and digital overload. Understanding these influencing factors is crucial for tailoring e-mental health interventions and encouraging their actual use in situations where in-person treatment is scarce, e-mental health interventions present a viable option. Stakeholders should consider the specific expectations, needs, and digital skills of elite athletes to enhance the effectiveness and adoption of these interventions. Future research should focus on longitudinal studies to explore how acceptance evolves over time and its impact on actual behavior. Additionally, improving the reliability of measurement tools and understanding the intention-behavior gap will strengthen the evidence base for e-mental health interventions. Finally, this study emphasizes the necessity of considering participants’ expectations, needs, and capabilities in the development and implementation of innovative treatment approaches. Addressing these aspects will contribute to better support for elite athletes and the optimization of mental health care in this population.
Data availability statement
The raw data supporting the conclusions of this article will be made available upon reasonable request to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethik-Kommission Universität Duisburg-Essen. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SG: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. JA: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. AE: Investigation, Project administration, Supervision, Writing – original draft, Writing – review & editing. TS: Investigation, Project administration, Supervision, Writing – original draft, Writing – review & editing. TM: Project administration, Supervision, Writing – original draft, Writing – review & editing, Investigation. E-MS: Conceptualization, Investigation, Project administration, Supervision, Writing – original draft, Writing – review & editing. MT: Conceptualization, Investigation, Project administration, Supervision, Writing – original draft, Writing – review & editing. AB: Conceptualization, Investigation, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. We thank the Open Access Fund of the University of Duisburg-Essen for supporting the publication of the manuscript.
Acknowledgments
We are thankful to our colleagues who provided expertise that greatly assisted the research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2024.1416045/full#supplementary-material
References
1. Gouttebarge V, Castaldelli-Maia JM, Gorczynski P, Hainline B, Hitchcock ME, Kerkhoffs GM, et al. Occurrence of mental health symptoms and disorders in current and former elite athletes: a systematic review and meta-analysis. Br J Sports Med. (2019) 53(11):700–6. doi: 10.1136/bjsports-2019-100671
2. Arnold R, Fletcher D. A research synthesis and taxonomic classification of the organizational stressors encountered by sport performers. J Sport Exerc Psychol. (2012) 34(3):397–429. doi: 10.1123/jsep.34.3.397
3. Watson JC. College student-athletes’ attitudes toward help-seeking behavior and expectations of counseling services. J Coll Stud Dev. (2005) 46(4):442–9. doi: 10.1353/csd.2005.0044
4. Gulliver A, Griffiths KM, Christensen H. Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry. (2010) 10:113. doi: 10.1186/1471-244X-10-113
5. Gulliver A, Griffiths KM, Christensen H. Barriers and facilitators to mental health help-seeking for young elite athletes: a qualitative study. BMC Psychiatry (2012) 12:157. doi: 10.1186/1471-244x-12-157
6. Radisch J, Büchtemann D, Kästner D, Kopke K, Moock J, Rössler W, et al. A literature- and expert-based analysis of the outpatient treatment of depressive ill people in Germany. Psychiatr Prax. (2013) 40(5):252–8. doi: 10.1055/s-0032-1332917
7. Oh H, Rizo C, Enkin M, Jadad A. What is eHealth (3): a systematic review of published definitions. J Med Internet Res. (2005) 7(1):e1. doi: 10.2196/jmir.7.1.e1
8. Van't Hof E, Cuijpers P, Stein DJ. Self-help and Internet-guided interventions in depression and anxiety disorders: a systematic review of meta-analyses. CNS Spectr. (2009) 14(2 Suppl 3):34–40. doi: 10.1017/s1092852900027279
9. VandenBos GR. APA Dictionary of Psychology. Washington: American Psychological Association (2007). Available online at: https://dictionary.apa.org/self-help (08/13/2024).
10. Carroll KM, Rounsaville BJ. Computer-assisted therapy in psychiatry: be brave—it’s a new world. Curr Psychiatry Rep. (2010) 12(5):426–32. doi: 10.1007/s11920-010-0146-2
11. Wright JH, Owen JJ, Richards D, Eells TD, Richardson T, Brown GK, et al. Computer-assisted cognitive-behavior therapy for depression: a systematic review and meta-analysis. J Clin Psychiatry (2019) 80(2):3573. doi: 10.4088/JCP.18r12188
12. World Health Organization. Telemedicine: opportunities and developments in member states: report on the second global survey on eHealth 2009 (global observatory for eHealth series, volume 2). Healthc Inform Res. (2012) 18(2):153–5. doi: 10.4258/hir.2012.18.2.153
13. Ebert DD, Van Daele T, Nordgreen T, Karekla M, Compare A, Zarbo C, et al. Internet- and mobile-based psychological interventions: applications, efficacy, and potential for improving mental health: a report of the Efpa E-Health taskforce. Eur Psychol. (2018) 23(2):167–87. doi: 10.1027/1016-9040/a000318
14. Hedman E, Andersson E, Ljótsson B, Andersson G, Rück C, Lindefors N. Cost-effectiveness of internet-based cognitive behavior therapy vs. cognitive behavioral group therapy for social anxiety disorder: results from a randomized controlled trial. Behav Res Ther. (2011) 49(11):729–36. doi: 10.1016/j.brat.2011.07.009
15. Andersson G, Cuijpers P, Carlbring P, Riper H, Hedman E. Guided internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: a systematic review and meta-analysis. World Psychiatry. (2014) 13(3):288–95. doi: 10.1002/wps.20151
16. Andrews G, Basu A, Cuijpers P, Craske MG, McEvoy P, English CL, et al. Computer therapy for the anxiety and depression disorders is effective, acceptable and practical health care: an updated meta-analysis. J Anxiety Disord. (2018) 55:70–8. doi: 10.1016/j.janxdis.2018.01.001
17. Heber E, Ebert DD, Lehr D, Cuijpers P, Berking M, Nobis S, et al. The benefit of web- and computer-based interventions for stress: a systematic review and meta-analysis. J Med Internet Res. (2017) 19(2):e32. doi: 10.2196/jmir.5774
18. Apolinário-Hagen J, Harrer M, Kählke F, Fritsche L, Salewski C, Ebert DD. Public attitudes toward guided internet-based therapies: web-based survey study. JMIR Ment Health. (2018) 5(2):e10735. doi: 10.2196/10735
19. Nunes A, Limpo T, Castro SL. Acceptance of mobile health applications: examining key determinants and moderators. Front Psychol. (2019) 10:2791. doi: 10.3389/fpsyg.2019.02791
20. Torous J, Nicholas J, Larsen ME, Firth J, Christensen H. Clinical review of user engagement with mental health smartphone apps: evidence theory and improvements. Evidence Based Mental Health. (2018) 21(3):116–9. doi: 10.1136/eb-2018-102891
21. Baumeister H, Nowoczin L, Lin J, Seifferth H, Seufert J, Laubner K, et al. Impact of an acceptance facilitating intervention on diabetes patients’ acceptance of internet-based interventions for depression: a randomized controlled trial. Diabetes Res Clin Pract. (2014) 105(1):30–9. doi: 10.1016/j.diabres.2014.04.031
22. Baumeister H, Seifferth H, Lin J, Nowoczin L, Lüking M, Ebert D. Impact of an acceptance facilitating intervention on patients’ acceptance of internet-based pain interventions: a randomized controlled trial. Clin J Pain. (2015) 31(6):528–35. doi: 10.1097/ajp.0000000000000118
23. Hennemann S, Beutel ME, Zwerenz R. Drivers and barriers to acceptance of web-based aftercare of patients in inpatient routine care: a cross-sectional survey. J Med Internet Res. (2016) 18(12):e337. doi: 10.2196/jmir.6003
24. Damerau M, Teufel M, Musche V, Dinse H, Schweda A, Beckord J, et al. Determining acceptance of e-mental health interventions in digital psychodiabetology using a quantitative web-based survey: cross-sectional study. JMIR Form Res. (2021) 5(7):e27436. doi: 10.2196/27436
25. Rentrop V, Damerau M, Schweda A, Steinbach J, Schüren LC, Niedergethmann M, et al. Predicting acceptance of e-mental health interventions in patients with obesity by using an extended unified theory of acceptance model: cross-sectional study. JMIR Form Res. (2022) 6(3):e31229. doi: 10.2196/31229
26. Bäuerle A, Mallien C, Rassaf T, Jahre L, Rammos C, Skoda EM, et al. Determining the acceptance of digital cardiac rehabilitation and its influencing factors among patients affected by cardiac diseases. J Cardiovasc Dev Dis (2023) 10(4):174. doi: 10.3390/jcdd10040174
27. Stoppok P, Teufel M, Jahre L, Rometsch C, Müßgens D, Bingel U, et al. Determining the influencing factors on acceptance of ehealth pain management interventions among patients with chronic pain using the unified theory of acceptance and use of technology: cross-sectional study. JMIR Form Res. (2022) 6(8):e37682. doi: 10.2196/37682
28. Esber A, Teufel M, Jahre L, In der Schmitten J, Skoda EM, Bäuerle A. Predictors of patients’ acceptance of video consultation in general practice during the coronavirus disease 2019 pandemic applying the unified theory of acceptance and use of technology model. Digit Health (2023) 9:20552076221149317. doi: 10.1177/20552076221149317
29. Davis FD. Perceived usefulness. Perceived ease of use, and user acceptance of information technology. MIS Q. (1989) 13(3):319–40. doi: 10.2307/249008
30. Ebert DD, Berking M, Cuijpers P, Lehr D, Pörtner M, Baumeister H. Increasing the acceptance of internet-based mental health interventions in primary care patients with depressive symptoms. A randomized controlled trial. J Affect Disord. (2015) 176:9–17. doi: 10.1016/j.jad.2015.01.056
31. Philippi P, Baumeister H, Apolinário-Hagen J, Ebert DD, Hennemann S, Kott L, et al. Acceptance towards digital health interventions—model validation and further development of the unified theory of acceptance and use of technology. Internet Interv. (2021) 26:100459. doi: 10.1016/j.invent.2021.100459
32. Lämmle L. Theoretische Konzeption, Diagnostik Und Bedeutung Von Motivation Und Selbstregulation Im (Hoch-) Leistungssport. In: Dresel M, Lämmle MDL, editors. Motivation, Selbstregulation Und Leistungsexzellenz. Münster: LIT (2011). p. 91–112.
34. Reardon CL, Hainline B, Aron CM, Baron D, Baum AL, Bindra A, et al. Mental health in elite athletes: international olympic committee consensus statement (2019). Br J Sports Med. (2019) 53(11):667–99. doi: 10.1136/bjsports-2019-100715
35. Kroenke K, Strine TW, Spitzer RL, Williams JB, Berry JT, Mokdad AH. The phq-8 as a measure of current depression in the general population. J Affect Disord. (2008) 114(1–3):163–73. doi: 10.1016/j.jad.2008.06.026
36. Löwe B, Decker O, Muller S, Brahler E, Schellberg D, Herzog W, et al. Validation and standardization of the generalized anxiety disorder screener (gad-7) in the general population. Med Care. (2008) 46(3):266–74. doi: 10.1097/MLR.0b013e318160d093
37. Presno C. Taking the byte out of internet anxiety: instructional techniques that reduce computer/internet anxiety in the classroom. J Educ Computing Res. (1998) 18(2):147. doi: 10.2190/UY72-5TG8-0LT5-AU4l
38. Prasad A, Quinones A. Digital overload warnings-“the right amount of shame”? In: Human-Computer Interaction. Human Values and Quality of Life: Thematic Area, HCI 2020, Held as Part of the 22nd International Conference, HCII 2020; Copenhagen, Denmark; July 19–24, 2020. Proceedings, Part III 22. Cham: Springer International Publishing (2020). p. 117–34.
39. Bäuerle A, Frewer AL, Rentrop V, Schüren LC, Niedergethmann M, Lortz J, et al. Determinants of acceptance of weight management applications in overweight and obese individuals: using an extended unified theory of acceptance and use of technology model. Nutrients. (2022) 14(9):1968. doi: 10.3390/nu14091968
40. Venkatesh V, Morris MG, Davis GB, Davis FD. User acceptance of information technology: toward a unified view. Inst Transit Econ Microecon Issues E-J. (2003) 27(3):425–78. doi: 10.2307/30036540
41. Filmus Y. Two proofs of the central limit theorem. (2010). Available online at: http://www.cs.toronto.edu/yuvalf/CLT.pdf (Accessed August 13, 2024).
42. Hennemann S, Beutel ME, Zwerenz R. Ready for eHealth? Health professionals’ acceptance and adoption of eHealth interventions in inpatient routine care. J Health Commun. (2017) 22(3):274–84. doi: 10.1080/10810730.2017.1284286
43. Schröder J, Bäuerle A, Jahre LM, Skoda EM, Stettner M, Kleinschnitz C, et al. Acceptance, drivers, and barriers to use eHealth interventions in patients with post-COVID-19 syndrome for management of post-COVID-19 symptoms: a cross-sectional study. Ther Adv Neurol Disord. (2023) 16:17562864231175730. doi: 10.1177/17562864231175730
44. Klein B, Cook S. Preferences for e-mental health services amongst an online Australian sample. J Appl Psychol. (2012) 6(1):28–39. doi: 10.7790/ejap.v6i1.184
45. Cimperman M, Makovec Brenčič M, Trkman P. Analyzing older users’ home telehealth services acceptance behavior-applying an extended UTAUT model. Int J Med Inform. (2016) 90:22–31. doi: 10.1016/j.ijmedinf.2016.03.002
46. Crisp DA, Griffiths KM. Participating in online mental health interventions: who is most likely to sign up and why? Depress Res Treat (2014) 2014:790457. doi: 10.1155/2014/790457
47. Lin J, Faust B, Ebert DD, Krämer L, Baumeister H. A web-based acceptance-facilitating intervention for identifying patients’ acceptance, uptake, and adherence of internet- and mobile-based pain interventions: randomized controlled trial. J Med Internet Res. (2018) 20(8):447–55. doi: 10.3109/09638288.2014.923529
48. Breil B, Kremer L, Hennemann S, Apolinário-Hagen J. Acceptance of mHealth apps for self-management among people with hypertension. Stud Health Technol Inform. (2019) 267:282–8. doi: 10.3233/shti190839
49. Nam SK, Chu HJ, Lee MK, Lee JH, Kim N, Lee SM. A meta-analysis of gender differences in attitudes toward seeking professional psychological help. J Am Coll Health. (2010) 59(2):110–6. doi: 10.1080/07448481.2010.483714
50. Abrahamsen FE, Roberts GC, Pensgaard AM. Achievement goals and gender effects on multidimensional anxiety in national elite sport. Psychol Sport Exerc. (2008) 9(4):449–64. doi: 10.1016/j.psychsport.2007.06.005
51. Gorczynski PF, Coyle M, Gibson K. Depressive symptoms in high-performance athletes and non-athletes: a comparative meta-analysis. Br J Sports Med. (2017) 51(18):1348–54. doi: 10.1136/bjsports-2016-096455
52. Pluhar E, McCracken C, Griffith KL, Christino MA, Sugimoto D, Meehan WP 3rd. Team sport athletes may be less likely to suffer anxiety or depression than individual sport athletes. J Sports Sci Med. (2019) 18(3):490–6.31427871
53. de Veer AJ, Peeters JM, Brabers AE, Schellevis FG, Rademakers JJ, Francke AL. Determinants of the intention to use e-health by community dwelling older people. BMC Health Serv Res. (2015) 15:103. doi: 10.1186/s12913-015-0765-8
54. Huygens MW, Vermeulen J, Friele RD, van Schayck OC, de Jong JD, de Witte LP. Internet services for communicating with the general practice: barely noticed and used by patients. Interact J Med Res. (2015) 4(4):e4245. doi: 10.2196/ijmr.4245
55. Quaosar G, Hoque MR, Bao Y. Investigating factors affecting elderly’s intention to use m-health services: an empirical study. Telemed J E Health. (2018) 24(4):309–14. doi: 10.1089/tmj.2017.0111
56. van Houwelingen CT, Ettema RG, Antonietti MG, Kort HS. Understanding older people’s readiness for receiving telehealth: mixed-method study. J Med Internet Res. (2018) 20(4):e123. doi: 10.2196/jmir.8407
57. Liu L, Miguel Cruz A, Rios Rincon A, Buttar V, Ranson Q, Goertzen D. What factors determine therapists’ acceptance of new technologies for rehabilitation—a study using the unified theory of acceptance and use of technology (UTAUT). Disabil Rehabil. (2015) 37(5):447–55. doi: 10.3109/09638288.2014.923529
58. Taiwo AA, Downe AG. The theory of user acceptance and use of technology (UTAUT): a meta-analytic review of empirical findings. J Theor Appl Inf Technol. (2013) 49(1):48–58.
59. Constantino MJ, Arnkoff DB, Glass CR, Ametrano RM, Smith JZ. Expectations. J Clin Psychol. (2011) 67(2):184–92. doi: 10.1002/jclp.20754
60. Geiger S, Steinbach J, Skoda EM, Jahre L, Rentrop V, Kocol D, et al. Needs and demands for e-mental health interventions in individuals with overweight and obesity: user-centred design approach. Obes Facts. (2023) 16(2):173–83. doi: 10.1159/000527914
61. Lillevoll KR, Wilhelmsen M, Kolstrup N, Høifødt RS, Waterloo K, Eisemann M, et al. Patients’ experiences of helpfulness in guided internet-based treatment for depression: qualitative study of integrated therapeutic dimensions. J Med Internet Res. (2013) 15(6):e126. doi: 10.2196/jmir.2531
62. Van Voorhees BW, Hsiung RC, Marko-Holguin M, Houston TK, Fogel J, Lee R, et al. Internal versus external motivation in referral of primary care patients with depression to an internet support group: randomized controlled trial. J Med Internet Res. (2013) 15(3):e42. doi: 10.2196/jmir.2197
63. Purcell R, Gwyther K, Rice SM. Mental health in elite athletes: increased awareness requires an early intervention framework to respond to athlete needs. Sports Med Open. (2019) 5(1):46. doi: 10.1186/s40798-019-0220-1
64. Bäuerle A, Jahre L, Teufel M, Jansen C, Musche V, Schweda A, et al. Evaluation of the e-mental health mindfulness-based and skills-based “cope it” intervention to reduce psychological distress in times of COVID-19: results of a bicentre longitudinal study. Front Psychiatry. (2021) 12:768132. doi: 10.3389/fpsyt.2021.768132
65. Bäuerle A, Teufel M, Musche V, Weismüller B, Kohler H, Hetkamp M, et al. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: a cross-sectional study in Germany. J Public Health (Oxf). (2020) 42(4):672–8. doi: 10.1093/pubmed/fdaa106
66. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. (2020) 288:112954. doi: 10.1016/j.psychres.2020.112954
67. Mann DM, Chen J, Chunara R, Testa PA, Nov O. COVID-19 transforms health care through telemedicine: evidence from the field. J Am Med Inform Assoc. (2020) 27(7):1132–5. doi: 10.1093/jamia/ocaa072
Keywords: eHealth, UTAUT, sports, internet, survey
Citation: Geiger S, Aufderlandwehr J, Esser AJ, Schadendorf T, Muehlbauer T, Skoda E-M, Teufel M and Bäuerle A (2024) Determining the acceptance of e-mental health interventions in elite athletes using the unified theory of acceptance and use of technology. Front. Sports Act. Living 6:1416045. doi: 10.3389/fspor.2024.1416045
Received: 11 April 2024; Accepted: 10 September 2024;
Published: 1 October 2024.
Edited by:
Jose Luis Pastrana-Brincones, University of St. Thomas, United StatesReviewed by:
Matt Mishkind, University of Colorado Anschutz Medical Campus, United StatesDominika Wilczyńska, Gdansk University of Physical Education and Sport, Poland
Copyright: © 2024 Geiger, Aufderlandwehr, Esser, Schadendorf, Muehlbauer, Skoda, Teufel and Bäuerle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sheila Geiger, c2hlaWxhLmdlaWdlckB1bmktZHVlLmRl