 Antonio Casanova-Lizón1
Antonio Casanova-Lizón1 Agustín Manresa-Rocamora1,2
Agustín Manresa-Rocamora1,2 José Manuel Sarabia1,2
José Manuel Sarabia1,2 Diego Pastor1
Diego Pastor1 Alejandro Javaloyes1
Alejandro Javaloyes1 Iván Peña-González1
Iván Peña-González1 Manuel Moya-Ramón1,2*
Manuel Moya-Ramón1,2*
- 1Department of Sport Sciences, Sport Research Centre, Miguel Hernandez University, Elche, Spain
- 2Alicante Institute for Health and Biomedical Research (ISABIAL), Alicante, Spain
Introduction: Exercising at home is an accessible alternative to the gym, although it presents challenges such as low adherence, poor quality and difficulties in reaching set goals. Wearable technologies and the use of heart rate variability (HRV) make it possible to personalise workouts, optimise fitness and improve adherence. However, specific exercise recommendations based on these metrics are still lacking. This study evaluated the impact of HRV-based training using the Selftraining UMH app in an autonomous format versus a Personal Trainer-led approach.
Methods: Seventy sedentary adults were divided into three groups: Autonomous (n = 18), Personal Trainer (n = 23), and Control (n = 29). After a two-week baseline HRV assessment, participants underwent an 11-week intervention, with pre- and post-tests on peak oxygen uptake, aerobic power, total test time, strength, and HRV.
Results: Both intervention groups completed similar session numbers (23.3 vs. 24.5) and high-intensity workouts (13.7 vs. 14.6). Both groups improved significantly (p < 0.05) across all fitness metrics, except aerobic power in the Autonomous group. Effect sizes ranged from small to large (0.21–1.12 Autonomous; 0.23–1.63 Personal Trainer). Strength improvements were greater in the Personal Trainer group, and both outperformed the Control group (p < 0.05) on all variables except aerobic power in the Autonomous group.
Conclusions: The findings demonstrate that HRV-based training effectively enhances fitness in sedentary adults, with both delivery methods showing similar adherence and benefits. The Selftraining UMH app offers an accessible alternative for autonomous exercise, particularly in settings without professional supervision, promoting improved population health outcomes.
1 Introduction
Physical exercise is a cornerstone of overall health, offering benefits beyond muscle conditioning and disease prevention. Scientific evidence links physical inactivity to non-communicable diseases, such as stroke, hypertension, type 2 diabetes, obesity, coronary heart disease, certain cancers, dementia, mental health problems, and increased mortality rates, particularly from cardiovascular disease (1). Conversely, regular exercise not only helps combat these conditions but also improves cognitive function (2) and promotes well-being (3). Despite its benefits, modern society has experienced increasing levels of sedentary behaviour (4). In 2016, physical inactivity was more than twice as prevalent in high-income countries (36.8%) compared to low-income countries (16.2%), with an upward trend observed in wealthier nations between 2001 and 2016 (5).
Traditionally, exercise has been associated with gyms and sports facilities, but many individuals face barriers such as time constraints, financial limitations and accessibility issues (6). Recent research highlights the benefits of home exercise as a more convenient and accessible alternative (7), promoting well-being (8), cardiovascular (9) and mental health (10). However, lack of supervision in home exercise programmes can lead to challenges such as inconsistent adherence, poor exercise quality, and difficulty achieving fitness goals (11). Adherence, defined as following professional recommendations (12), is influenced by personal and environmental factors (13). In addition, there is no universal standard for assessing exercise adherence, complicating efforts to identify predictors of success (13).
The rise of digital technologies, especially wearable technologies (WTs), offers new solutions for objective measurement and guiding exercise (13). WTs, such as smartwatches and devices embedded in smartphones, enable real-time data collection and feedback (14). These devices have been shown to improve adherence by providing users with objective measurements and education (15). Increasing emphasis is being placed on a personalised approach to exercise, recognising the variability in individuals' physiological responses to training (16). Day-to-day training models dynamically adjust workouts based on personal data, optimising performance and reducing the risk of injury (17).
Heart rate variability (HRV) has emerged as a key tool for personalising training. HRV measures variations between consecutive heartbeats and reflects the balance between the sympathetic and parasympathetic branches of the autonomic nervous system (ANS) (18). HRV is sensitive to exercise response and fatigue levels (19, 20), making it a valuable indicator for adjusting training intensity. For example, normal values of HRV suggest readiness for intense exercise, while altered values indicate the need for lighter activity or rest (11). Validated applications such as HRV4Training (21) and Welltory (22), along with devices such as Elite HRV (23), offer accessible ways to measure HRV. However, these tools typically provide HRV values without specific exercise recommendations based on those metrics.
Due to the current challenges in accessing guided training, the efficacy of HRV as an exercise control tool, and the role of personal training in measuring this variable, the Miguel Hernández University of Elche has developed a mobile application called Selftraining UMH. This application employs a day-to-day guided model based on HRV. Therefore, the objective of this study was to analyse adherence and the effects of self-directed training prescribed using the Selftraining UMH app, as well as training led by a personal trainer.
2 Materials and methods
2.1 Participants
Participants were male and female adults, either sedentary or with at least three months of physical inactivity, willing to start a physical exercise programme in an autonomous or a personal trainer-led mode. Exclusion criteria included pre-existing medical conditions, age over 60, or being physically active (engaging in >150 min of moderate-intensity or >75 min of vigorous-intensity activity per week) (24). The information required to verify the inclusion and exclusion criteria was self-reported through an initial interview and the Physical Activity Readiness Questionnaire (PAR-Q) (25).
In the initial phase of the study, recruitment of participants was carried out through a multi-channel strategy. Various dissemination platforms were used, including project- and institution-specific social networks, information posters and leaflets distributed, as well as awareness-raising campaigns through local radio stations. In parallel, participation was promoted through informative talks given in university classrooms and educational centres.
Participants provided written informed consent, and ethical approval was granted by the university's Ethics Committee (CID.DPC.01.19), adhering to Good Clinical Practice and the Declaration of Helsinki.
2.2 Experimental design
The study spanned 16 weeks, divided into two periods: a 2-week control period (CP) for stabilisation and baseline HRV measurements, followed by an 11-week training period (TP). Assessments were conducted before (PRE-EV) and after the training period (POST-EV), with a familiarization week (FAM-EV) to minimize the learning effect. Participants who were not interested in the training programme were not randomised and, therefore, assigned to the control group (CG). The remaining participants were randomised into two groups: an autonomous HRV-guided group using the Selftraining UMH app (AUG) or a personal trainer-led HRV-guided group (PTG). HRV was used to prescribe daily training (Figure 1).

Figure 1. Experimental design. AUG, autonomous group; FAM-EV, familiarization evaluation; CP, control period; PRE-EV, evaluation conducted prior to the training period; PTG, personal training group; TP, training period; HRV, heart rate variability guided; POST-EV, evaluation after the training period.
2.3 Evaluation
2.3.1 Physical fitness variables
The evaluations were conducted in the Training Analysis and Optimization Laboratory of the Sport Research Centre of the Miguel Hernández University of Elche. Participants refrained from drinking or speaking during the test and avoided intense exercise 24 h prior. Tests included:
Aerobic Capacity: peak oxygen uptake (VO2 peak) was measured via an incremental treadmill test using the Bruce protocol (26), with gas exchange data collected using the Metalyzer 3B (Cortex GmbH, Germany).
Upper Body Strength: A one-minute Bench Press Test was performed using a Smith Machine with a standardised load (35 kg for men, 15 kg for women) (27). Proper execution required full elbow extension during the upward phase and allowing the bar to touch the chest during the downward phase.
Lower Body Strength: A squat test assessed maximum repetitions in one minute, ensuring proper form and a consistent depth (27). A brief warm-up was conducting before starting the test. During this phase, participants were instructed on proper squatting technique. A box was positioned to provide a consistent depth, ensuring 90 degrees of knee flexion at the bottom of each repetition (28). Participants received feedback on their technique throughout the test. Repetitions that performed incorrectly were excluded from the total count.
2.3.2 Assessment of heart rate and HRV
Heart rate (HR) and HRV were recorded using a Polar H10 chest strap and the Elite HRV app (29). During the subsequent 5 min, HR and HRV data were recorded while participants remained seated in a resting state. The final 2 min of the recording were earmarked for subsequent analysis (30) using Kubios HRV Premium software (v3.5.0) (31). The root mean square of successive differences (rMSSD) parameter was chosen due to its reliability (32), and ectopic beats were corrected using automated artefact correction in the Kubios software (33).
2.3.3 Adherence to exercise training
Adherence for the PTG was tracked via attendance records (34), and for the AUG, through app usage logs. HR monitors verified target HR zones. Across the 11 weeks, participants were scheduled for 33 sessions, with adherence monitored to ensure compliance.
Training zones were determined based on the percentage of maximum heart rate (HR max), following the classifications established by the American College of Sports Medicine (35). In this study, high-intensity exercise was defined as activity at ≥80% of HR max, moderate-intensity exercise ranged from 60% to 79% of HR max, and low-intensity exercise was classified as ≤59% of HR max.
2.3.4 SF-36 health survey
This self-administered questionnaire assessed eight health domains, scored on a 0–100 scale, with higher scores indicating better health-related quality of life (36, 37). The Spanish adaptation by Alonso et al. (38) was used in this study.
2.3.5 Psychological vitality and affective state
Psychological vitality was measured using the Subjective Vitality Questionnaire (39), with responses recorded on a 0–7 Likert scale. The Spanish adaptation by Molina-García et al. (40).
The Positive and Negative Affect Schedule (41, 42) measured emotional states before and after exercise sessions, using a nine-item questionnaire with a 1–7 Likert scale. The Spanish adaptation by López-Gómez et al. (43).
2.4 Physical exercise programme
The programme lasted 11 weeks, with a frequency of three sessions per week, each lasting 45–60 min, with 48–72 h of rest between sessions. Both the mobile app and the supervised programme included four levels of intensity, each offering four different session options. The first level included low-intensity sessions, and the remaining levels (level 2, level 3 and level 4) included high-intensity sessions (11). The training programme was gamified through the app to enhance motivation and participation. Participants earned stars for completing sessions within a level. Once a predetermined number of stars were accumulated, they progressed to the next level of intensity. Designed to span three months, the app provides a comprehensive, adaptable and user-friendly framework for people starting an exercise routine, ensuring sustained engagement and progressive development. This design ensured a gradual increase in intensity and workload, while maintaining a balance between challenge and adaptability to suit participants' abilities. Sessions included warm-up, strength and endurance exercises, as well as a cool-down phase.
In level 1, the main objective was to familiarise participants with the physical exercise programme and ensure proper technique. Strength exercises included squats, shoulder presses, lunges, push-ups and rowing. In addition, core-focused exercises such as front planks, side planks, dynamic and static back bridges, dead bugs, and bird dogs were introduced. Each exercise consisted of 15 repetitions, followed by one minute of rest. During rest, participants alternated between 20 s of core exercises (e.g., active planks) and 40 s of passive rest. Participants completed four sets of each exercise before moving on to the next, performing 4–5 exercises per session. A two-minute rest was provided between exercises (Supplementary Figure S1). In level 2, the intensity was increased by incorporating additional aerobic exercises alongside the strength exercises from level 1. Aerobic activities included mountain climbers, skipping, jumping jacks, burpees, side steps, and boxing. Each exercise was performed for 30 s, followed by a 30 s rest. Sessions consisted of 10–12 exercises per set, and participants completed two sets in total (Supplementary Figure S2). In level 3, the integration of aerobic and strength exercises was maintained while the training volume was increased. Participants performed three sets instead of two. The number of exercises per session started with 8 during the first weeks and increased to 10 in the following weeks. The duration of each exercise (30 s) and the rest period (30 s) remained unchanged. A two-minute rest interval was introduced between sets (Supplementary Figure S3). In level 4, the structure of level 3 was maintained, but the work-rest ratio was modified to increase the intensity. Each exercise was performed for 40 s, while the rest period was reduced to 20 s. The two-minute rest interval between sets remained unchanged, and the number of exercises and sets was consistent with that of level 3 (Supplementary Figure S4).
The programme started with low-intensity sessions in weeks 1 and 2 and progressed to two high-intensity and one low-intensity session per week. All sessions were designed so that they could be performed at home or outdoors, using minimal or low-cost equipment to ensure accessibility. The number of intervals increased gradually throughout the programme, following a linear periodisation approach. This strategy facilitated a progressive increase in high-intensity exercise, starting with a low volume to promote safe physiological adaptation. The periodisation plan and the evolution of training variables can be found in Supplementary Table S1. The exercise programme was developed based on fundamental training principles, including overload, progression, individualisation, periodisation and specificity (44).
2.5 HRV-guided training prescription
Participants recorded HRV daily using the Welltory smartphone app (22) and photoplethysmography (PPG) (45). Measurements, lasting two minutes, were taken in a supine position upon waking, with a consistent breathing pattern. HRV values were transformed into their natural logarithms (Ln-rMSSD) for parametric analysis (46). Training prescriptions were based on a seven-day rolling average (Ln-rMSSD7day−roll−avg) relative to the smallest worthwhile change (SWC), defined as the mean ± 0.5 × standard deviation (SD) (47).
Training intensity was guided by the Ln-rMSSD7day−roll−avg relative to the SWC. High-intensity sessions were prescribed when HRV was above or within the SWC, while low-intensity sessions were recommended if HRV was below the lower limit of the SWC (48, 49). A variation of the decision-making algorithm developed by Javaloyes et al. (48) was followed, which is a modification of the algorithm proposed by Kiviniemi et al. (49) (Figure 2). Supplementary Table S2, details how progress was made at different intensity levels throughout the training programme for both experimental groups, where HRV was within normal HRV values as determined by the SWC. Supplementary Table S3 presents the evolution of the training programme over several weeks, establishing a differentiation in the intensity levels and their distribution according to the PNS response measured through the HRV. The progression of intensity is implemented in a gradual and controlled manner, ensuring adequate physiological adaptation before progressing to higher levels. The adopted model contemplates three high-intensity levels, which require the completion of six sessions within the same level, with HRV values above or within the SWC before allowing progression to the next level.
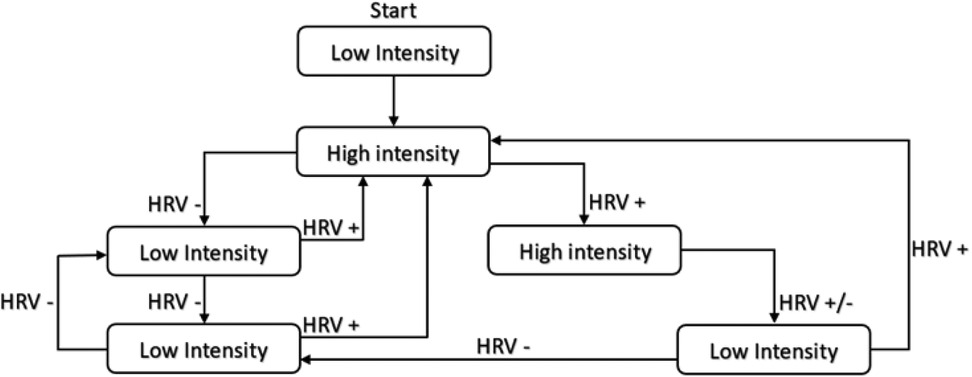
Figure 2. HRV-guided training decision algorithm.
2.5.1 Autonomous group guided by the Selftraining UMH app
The AUG followed the same programme remotely, using the Selftraining UMH app. Instructional videos provided guidance on app use and HRV measurement techniques (links can be found in the Supplementary Material). Weekly follow-ups via email or phone addressed technical issues and provided feedback on training adherence and execution.
2.5.2 Group guided by a personal trainer
Participants in the PTG trained in person under supervision of sports science professionals at the Sports Research Centre of Miguel Hernández University of Elche.
2.5.3 Control group
Prior to the study, and during short personal interviews, participants assigned to the CG were asked not to initiate any exercise programme throughout the study duration. Therefore, these participants maintained their previous physical activity levels. Afterwards, this information was confirmed during the final assessment. All the participants confirmed that they remained inactive during the full study period.
2.6 Structure and functionalities Selftraining UMH application
The Selftraining UMH mobile application is designed to prescribe physical training through the daily monitoring of HRV. The application is organised into three main sections. From the home screen, the user can access tools for monitoring their physiological state, including.
The application enables the manual recording of body weight, allowing for continuous monitoring of physical condition over time. This feature facilitates the assessment of weight fluctuations and their potential impact on overall health and fitness (Figure 3).

Figure 3. Manual recording of body weight.
HRV is recorded each morning, providing physiological insights and generating personalised recommendations based on the obtained values. The measurement process can be conducted through various methods. When using optical measurement via a smartphone camera, the user follows on-screen instructions, positioning a finger over the camera and flash. The measurement is initiated by pressing the “START” button, leading to a one-minute recording. An additional informational section (“+INFO”) provides guidance on the correct procedure, the optimal conditions for measurement, and the recommended user's state. For HRV measurement using an external HR monitor, a compatible device must be connected. If used for the first time or not automatically detected, the user must manually enter the monitor's identification number. The measurement begins upon selecting the “START” button and lasts for one minute, with an informational section (“+INFO”) available for further instructions on the correct measurement protocol. Alternatively, HRV can be recorded via integration with the Welltory application, which requires permission to access relevant data. Upon launching the Welltory app, the user has six seconds to position the index finger over the camera and flash. The measurement process takes between one and two minutes, depending on movement and sensor coverage. Once completed, selecting the red button returns the user to the Selftraining UMH application, where the recorded HRV data can be saved. Additionally, the system allows for manual data entry, enabling the incorporation of HRV values obtained from other devices or applications, ensuring broader compatibility with external monitoring systems (Figure 4).

Figure 4. Measurement HRV various methods.
The application includes a structured autonomous training programme designed based on physiological data. This programme spans three months and consists of three weekly training sessions, each lasting one hour. The intensity of each session is determined through a proprietary algorithm that analyses previously recorded HRV values, allowing for a personalised approach to training. A comprehensive library of pre-recorded video workouts is accessible within the application, offering users a variety of training options. Prior to each session, the user is provided with information regarding their physiological state and recommended intensity levels. While the application generates optimised workout suggestions, flexibility is offered through the option to select sessions of varying intensity. During training, real-time performance tracking is available, with functionalities that allow the user to pause, stop, or restart the session. If a compatible HR monitor is connected, HR data can be recorded, further enhancing the precision of training adaptation. Following each session, a post-exercise self-assessment tool enables the user to evaluate their subjective fatigue levels using a numerical scale from 1 to 10, contributing to a more comprehensive understanding of physiological responses to exercise (Figure 5).
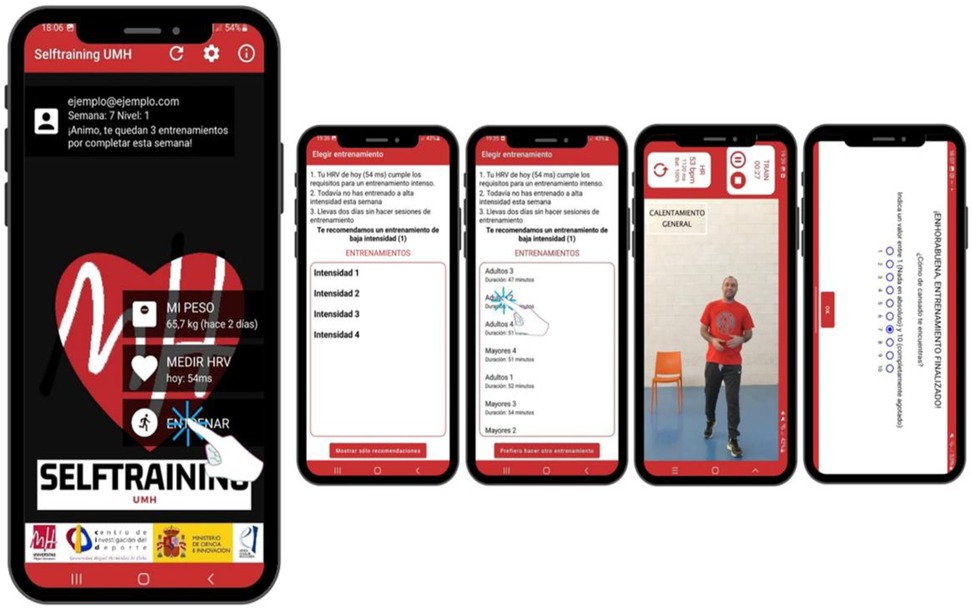
Figure 5. Training within the application.
2.7 Training load quantification
Training load was assessed using the Edwards Training Impulse (eTRIMP) method (50), modified to include Zone 0 (<50% HR maximum) combined with Zone 1. The internal load was measured via the Session Rating of Perceived Exertion (sRPE) scale (51).
2.8 Statistical analysis
A repeated measures analysis of variance (ANOVA) was performed to analyse changes in each of the groups and an independent measures ANOVA was performed to compare exercise adherence between the two experimental groups. Finally, an analysis of covariance (ANCOVA) was used to analyse differences between changes after the intervention taking into account pre-intervention values, to reduce error variance and improve statistical power (52). Effect sizes (ES) Cohen's d were calculated with 95% confidence intervals and significance was set at p < 0.05, with the following interpretations: trivial (≤0.19), small (0.20–0.49), moderate (0.50–0.79), and large (≥0.80) (53). The association between variables was assessed with Pearson's correlation coefficient (r) and interpreted as trivial (≤0.09), small (0.10–0.29), moderate (0.30–0.49), high (0.50–0.69), very high (0.70–0.89) and almost perfect (≥0.90) (54). Analyses were performed using Excel and JASP software (55).
3 Results
3.1 Participants
Ninety-three participants were recruited for the study. Three were excluded after the initial interview for not meeting the inclusion criteria (one for cardiovascular disease and two for being physically active), leaving 90 eligible subjects. These were randomly assigned to two experimental groups: AUG (n = 31) and PTG (n = 29), as the participants included in the CG (n = 30) were allocated by convenience. Four subjects did not start the assigned intervention: three from the AUG (9.7%, for work, family or technical reasons) and one from the PTG (3.4%, for work reasons). During the study period, 14 participants dropped out: nine from AUG (29%) and five from PTG (17.2%), mainly due to health problems, family, work or academic commitments. In addition, two participants did not attend the final evaluations: one from AUG (3.2%) and one from the CG (3.3%). In total, 70 subjects completed the 11-week programme: 18 in the AUG, 23 in the PTG and 29 in the CG. A detailed flow of participants' progress is presented in Figure 6 (56), and baseline descriptive characteristics are provided in Table 1.
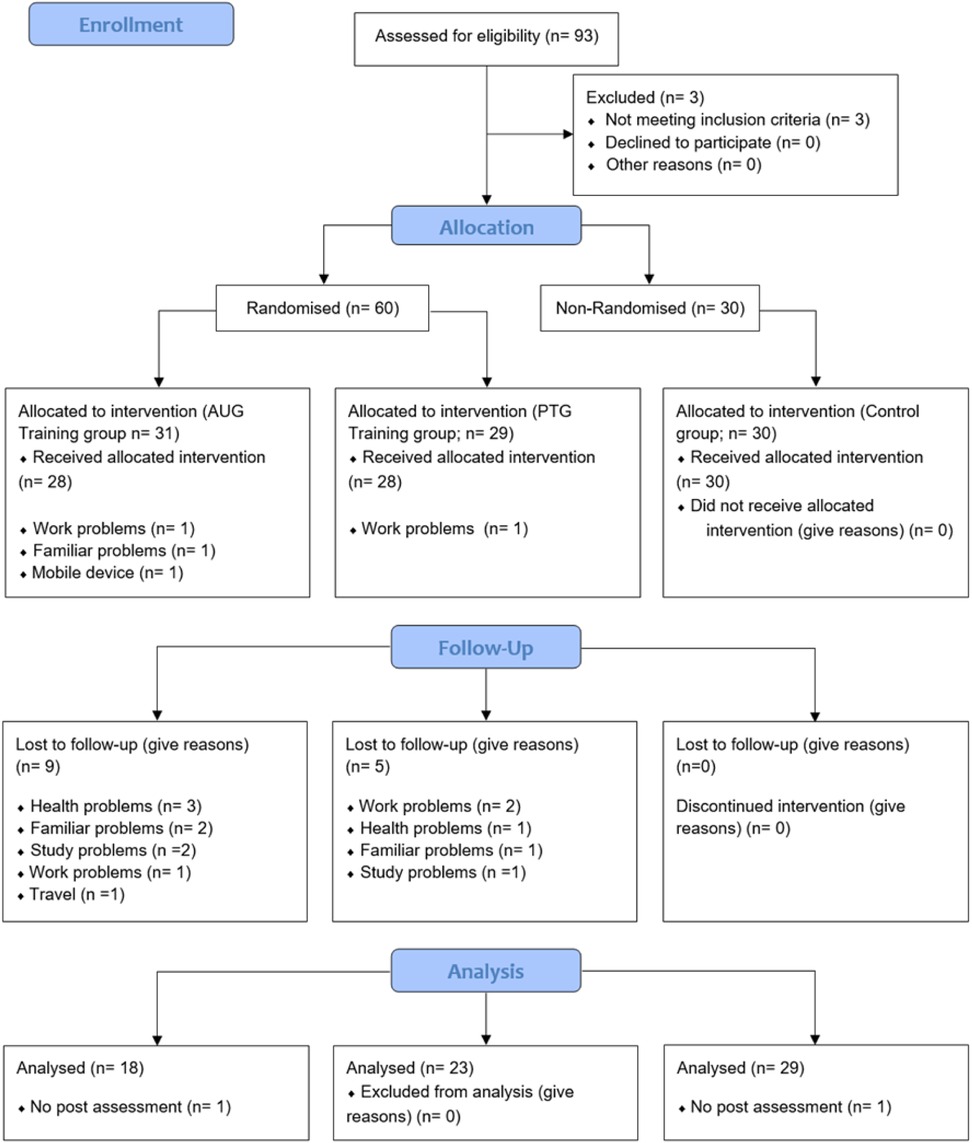
Figure 6. CONSORT 2010 flow diagram subjects. AUG, autonomous group; PTG, personal training group.
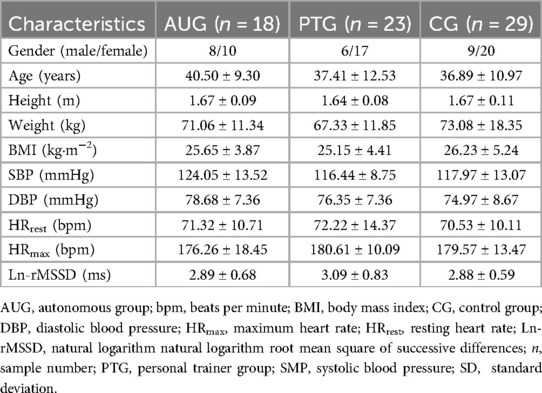
Table 1. Descriptive statistics of adult participants (mean ± SD).
3.2 Physical fitness variables and heart rate variability
The interaction between the two factors reached statistical significance for all the analysed variables (p < 0.01). Intra-group comparisons in both EG showed significant improvements in all fitness-related variables (p ≤ 0.04), except for maximal aerobic power in the AUG. ES based on Cohen's d ranged from trivial to large (d = 0.15 to d = 1.12) for the AUG and from small to large (d = 0.23 to d = 1.63) for the PTG. In contrast, the CG did not show statistically significant increases in any variable. A detailed summary of the results and comparisons for all groups is presented in Table 2.
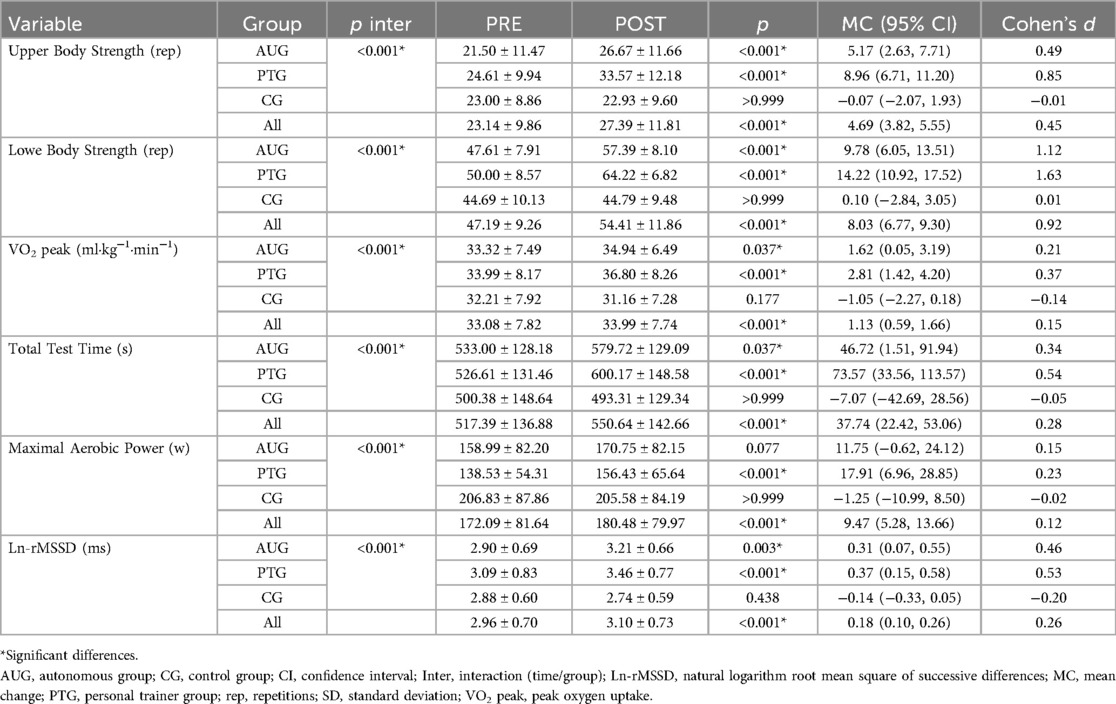
Table 2. Effect of exercise on fitness variables (mean ± SD).
As for the ANCOVA, the results reached statistical significance for all the variables analysed (p < 0.01). Concretely, statistically significant differences were found for the following variables (p ≤ 0.01) were found between AUG and PTG change in the number of repetitions in upper and lower body strength, with the magnitude of the ES being large (d = –1.03 and d = –1.06, respectively) in favour of PTG. Furthermore, although no statistically significant differences were found, a smaller change in VO2 peak was observed in AUG than in PTG, with the magnitude of ES being moderate (d = –0.60). Comparisons between AUG and CG changes showed significant differences in favour of AUG in all variables (p ≤ 0.01), except for maximal aerobic power (p = 0.06), with moderate to large ES (d = 0.72 to d = 2.19). When comparing PTG with CG, changes were statistically superior in PTG in all variables (p < 0.01), with large ES (d = 1.07 to d = 3.25). A detailed summary of the comparisons between all groups is provided in Table 3.
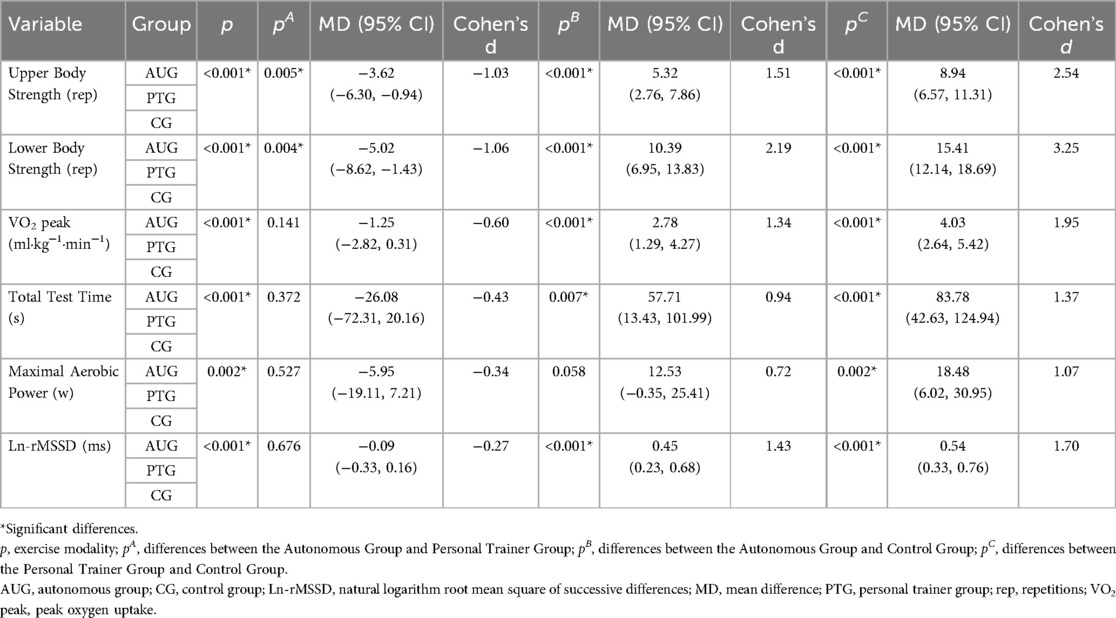
Table 3. Between-group comparisons of mean change in fitness variables.
Correlation analysis showed moderate (r = 0.36 to r = 0.45) and significant (p < 0.01) associations between changes in HRV and changes in fitness-related variables. A detailed summary of the correlation results is provided in Table 4.
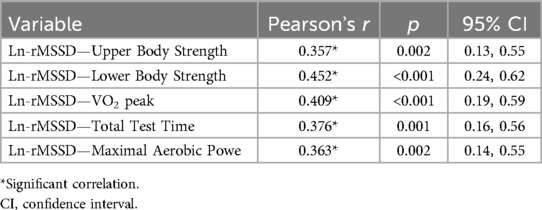
Table 4. Correlation of changes in HRV with improvement in physical fitness.
3.3 Adherence to physical exercise programme
No statistical differences were found between AUG and PTG in terms of total number of sessions, number of high-intensity sessions, number of low-intensity sessions or training frequency (p ≥ 0.25). (Supplementary Table S4).
However, in the high-intensity sessions, statistically significant differences were found between the experimental groups in the time spent within the low- and high-intensity zones (p < 0.01). In the AUG, a higher percentage of time was observed within the low intensity zone. In contrast, in the PTG, the percentage of time was higher in the high intensity zone. Data analysis showed a small ES magnitude in the moderate intensity zone (d = 0.23) and large ones in the low and high intensity zones (d = 1.84 and d = 3.07, respectively). In the low-intensity sessions, statistically significant differences were found between the experimental groups in time spent, within the zones rated as low, moderate and high intensity (p < 0.01). In the AUG, a higher percentage of time was observed in the low intensity zone, with the magnitude of the ES being large (d = 1.42). In the PTG group, the percentage of time was higher in the moderate and high intensity zone, with large ES (d = 1.30 and d = 0.97, respectively). The results of these comparisons are shown in Table 5.
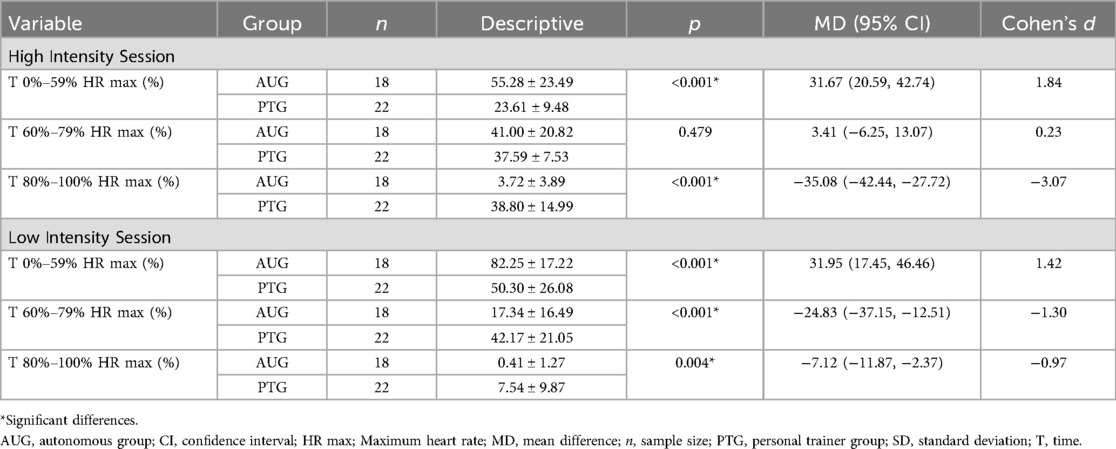
Table 5. Comparison time in each intensity zone during sessions (mean ± SD).
3.4 SF-36 health survey
The interaction between the two factors reached statistical significance for the dimensions of physical role, bodily pain, vitality, and health evolution (p ≤ 0.03). In the AUG, only the health evolution dimension of the SF-36 questionnaire showed a significant increase after the intervention (p < 0.01), with a trivial to large ES magnitude (d = 0.17 to d = 1.60). In PTG, significant improvements were identified in physical role, bodily pain, general health, vitality, mental health, and health evolution at the end of the training programme (p ≤ 0.03), with the magnitude of ES being between small and large (d = 0.35 to d = 1.76). No significant changes were found in CG. Regardless of the group, the results showed a statistically significant increase in the physical function, general health, social function, emotional role, and mental health (p ≤ 0.03), with ES ranging from d = 0.23 to d = 1.25 (Supplementary Table S5).
Between-group change differences did not reach statistical significance for physical and social functions (p > 0.05), so pairwise comparisons were not performed. In the remaining dimensions, statistically significant differences were found between AUG and PTG change only in the vitality dimension (p = 0.02), with a large ES magnitude (d = –0.86) in favour of PTG. Comparisons between AUG and CG changes showed significant differences in favour of AUG in vitality, emotional role, and health evolution (p ≤ 0.04), showing small to large ES magnitudes (d = 0.28 to d = 1.31). Finally, when comparing PTG with CG, changes were statistically superior in PTG in all quality of life dimensions (p ≤ 0.04), showing magnitudes of ES between small and large (d = 0.47 to d = 1.93). Full details are provided in Supplementary Table S6.
3.5 Psychological vitality and affective state
The interaction between the two factors reached statistical significance for psychological vitality and negative affective state (p ≤ 0.04). In the AUG, significant improvements were observed in psychological vitality and negative affective state (p ≤ 0.02), showing moderate ES magnitudes for positive affective state (d = 0.62) and large for vitality (d = 0.89) and negative affective state (d = 0.81). In the PTG, all variables improved significantly (p ≤ 0.03), with ES magnitudes being moderate for positive affective state (d = 0.62) and large for vitality (d = 0.81) and negative affective state (d = 1.00). In contrast, CG showed no significant changes. Regardless of the group, the results showed a statistically significant increase in the psychological vitality and negative affective state (p ≤ 0.04), with ES the d = 0.66 and d = –0.59, respectively (Supplementary Table S7).
The overall ANCOVA reached statistical significance for all variables analysed (p < 0.01). Specifically, no statistically significant differences were found in the change between AUG and PTG in any variable (p ≥ 0.99). Comparisons between AUG and CG changes showed significant differences in favour of AUG in vitality, positive affective state and negative affective state (p ≤ 0.02), showing large ES magnitudes (d = 0.82 to d = 1.09). Similarly, when comparing PTG with CG, changes were statistically greater in PTG on these same variables (p ≤ 0.01), with ES magnitudes being large (d = 0.83 to d = 1.21). Full results are presented in Supplementary Table S8.
3.6 Training load
When comparing the groups, statistically significant differences (p < 0.01) were found between the AUG and PTG in cumulative training load in all zones in favour of the PTG, except in zone 2 (p = 0.24). The magnitude of the ES varied between small for zone 2 (d = 0.38) and large for the rest of the zones and for the total training load (d = 1.27 to d = 2.79). Detailed results of these comparisons are presented in Table 6.
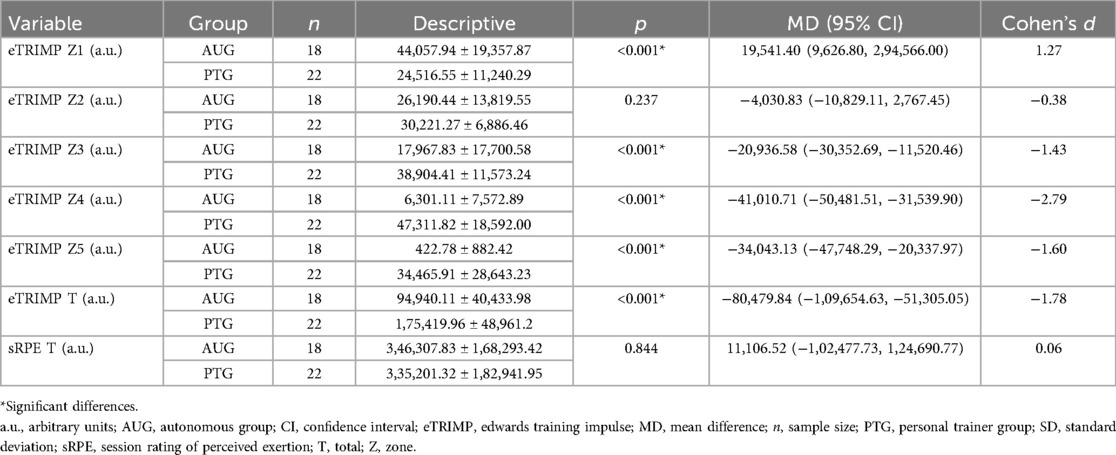
Table 6. Comparison of the training load during the programme (mean ± SD).
3.7 Adverse events
No adverse events directly related to the interventions were reported. Prior to the study, some participants faced technical problems or schedule changes. During the intervention, 14 participants dropped out due to work, family or academic commitments, health problems (such as minor surgeries or COVID-19) and holidays.
4 Discussion
The aim of this study was to evaluate adherence and the effects of Autonomous Training (AUG) via the Selftraining UMH app and face-to-face Personal Trainer-Led (PTG) training group, both guided by HRV, in sedentary adults. Both intervention groups showed significant improvements in upper and lower body strength, aerobic capacity (VO2 peak), total test time, and HRV. However, only the PTG achieved statistically significant improvements in maximal aerobic power. Adherence was similar between groups, but the PTG demonstrated greater consistency in session intensity and frequency of high-intensity activities.
In between-group comparisons, statistically significant differences in upper and lower body strength were found when comparing AUG with PTG. In addition, both intervention groups showed significant differences in strength, aerobic capacity and HRV compared to the CG. However, improvements in VO2 peak reached statistical significance only when comparing PTG with CG.
4.1 Selftraining UMH mobile app
Our results regarding the impact of the Selftraining UMH app on improving aerobic capacity (MD = 1.62 ml·kg−1·min−1 intra-group and MD = 2.78 ml·kg−1·min−1 vs. CG) are consistent with previous studies on exercise apps. For example, App-tivate improved VO2 peak by 1.4 ml·kg−1·min−1 intra-group and 2.0 ml·kg−1·min−1 vs. controls in people with metabolic disorders (57). The Harufit app, in patients recovering from acute myocardial infarction, increased VO2 peak by 3.18 ml·kg−1·min−1 in the intra-group comparisons (58). In young people, Clinic C, integrated with virtual reality and exercise bikes, also achieved an increase of 3.18 ml·kg−1·min−1 (59). Other apps, such as Strava, Pacer, MapMyWalk, and Pokémon Go, used for step monitoring in adolescents, reported increases that ranged from 1.18 and MD = 0.95 ml·kg−1·min−1 in intra-group analyses to 0.57 and 0.43 ml·kg−1·min−1 compared to CGs, although without structured programmes (60). In adults, Acupedo (walking), FMTK (bodyweight exercises at home), and LogMyFood (diet tracking via photographic records) reported improvements of up to 1.32 ml·kg−1·min−1 in six weeks and 1.07 ml·kg−1·min−1 at 12 weeks in intra-group analyses. Previous reviews support these results, highlighting significant improvements in different populations using apps that track daily steps (61, 62). Mobile apps can, therefore, achieve comparable physical adaptations to supervised programmes, provided that exercise prescriptions are equivalent (63) and adherence is adequate (64). Furthermore, a systematic review with meta-analysis suggests that the impact on VO2 peak is greater when mobile apps include features such as continuous monitoring (65) and automated feedback (66). Notably, improvements in aerobic capacity tend to be more consistent in short-term studies lasting less than 12 weeks (67).
The increased strength in both upper and lower body PTG (p < 0.01) can be attributed to technical adjustments by the trainer, which optimise muscle activation and motor unit recruitment. During the first 6–8 weeks of training, strength improvements are predominantly neurological, whereas in later weeks (12–26), they are due to myofibrillar hypertrophy and possible transitions between fast muscle fibres types IIa and IIx (68). Additionally, the higher workload in high-intensity zones (80%–100% HR max) in the PTG contributed to significant differences with respect to the AUG (69). Results on the use of mobile apps for strength development are varied and depend on the programme design and population. A recent study showed significant improvements in upper and lower body strength in active (p = 0.02 and p = 0.02, respectively) and inactive (p = 0.02 and p < 0.01, respectively) adolescents in the within-group analysis (60). However, only the active subjects showed differences in the lower body compared to the CG (p = 0.03), possibly due to their regular physical activity (60). In young adults (59), improvements in lower body strength (p = 0.01) were observed after using mobile technologies, but these were smaller compared to traditional interventions without the use of technology or supervised HIIT (70–73).
The PTG was the only one to show a significant improvement in maximal aerobic power (p < 0.01). The effect of training guided by heart rate variability in a supervised manner for the improvement of maximal power has been previously demonstrated in studies carried out with different populations (46, 48). However, although the change did not reach statistical significance in this study, we found an improvement in the AUG of power of a magnitude of 11.75 watts. Furthermore, our results show that the groups did not have the same power values before training, and when the changes are analysed, taking into account the values before the intervention, no differences are found in the improvement in this variable (p = 0.53).
These greater improvements may be attributed to greater exposure to high-intensity zones during training sessions. Evidence suggests that individuals participating in self-contained exercise programmes often do not reach the prescribed intensity during high-intensity sessions (74–78), despite completing the same total number of sessions, including both high- and low-intensity sessions. This difference is likely to be influenced by psychological, social and technical factors.
The improvements observed in both modalities are due to the use of periodisation techniques, which structure loading and recovery cycles. In addition, the manipulation of FITT principles (frequency, intensity, time, type) allowed for personalised adjustments, avoiding plateaus and injuries (79–81). The inclusion of HIIT, a time-efficient method, and resistance exercises favoured overall improvements in physical performance, mobility and functional independence, essential for quality of life (82, 83). This comprehensive approach maximises exercise adherence and ensures sustainable benefits (84).
4.2 HRV-based physical exercise programmes
The results are consistent with previous research that has demonstrated the efficacy of HRV-guided exercise programmes in optimising physical performance (85) and reducing the risk of overtraining (86). This approach allows for daily adjustments in exercise load according to individual physiological state. Previous studies have reported significant improvements in fitness parameters in diverse populations, including sedentary (87), recreational runners (49, 88), elite athletes (46, 48, 89) and patients with pathologies (90). In particular, HRV-guided training is superior to predefined programmes as it personalises the load to maximise physiological adaptations and minimise variability in individual responses (17, 91, 92).
In our study, both AUG and PTG showed increases in rMSSD, with mean differences (MD) of 0.45 milliseconds and 0.54 milliseconds, respectively, vs. CG. This highlights the positive effect of exercise on parasympathetic nervous system (PNS) modulation. Consistent with this, previous research has reported significant improvements in rMSSD in healthy sedentary people (93) and patients with various pathologies (94–96). Additionally, significant intra-group improvements were observed in our study, with pre and post-intervention MD increases of 0.31 milliseconds in the AUG and 0.37 milliseconds in the PTG. Similar findings were reported by Picard et al. (96), who observed a standard MD increase of 0.30 milliseconds in rMSSD in within-group analyses. The observed improvements reinforce the idea that physical exercise may be an effective non-pharmacological strategy to improve cardiac vagal modulation and reduce mortality risk (97–99).
Unlike other applications, the Selftraining UMH app integrates an HRV-based programme that measures, monitors exercise responses and prescribes daily routines tailored to individual needs. In addition, HRV can be monitored during activity to ensure that the target intensity is reached.
4.3 Adherence
Although there was no significant difference in the total number of sessions completed between AUG and PTG (MD = 23.28 vs. MD = 24.52), nor in number of low-intensity (MD = 9.56 vs. MD = 9.96) and high-intensity sessions (MD = 13.72 vs. MD = 14.57), the AUG adherence rate (70.56%) was notably higher than the average for online interventions (≈50%) (100). This can be attributed to the effective use of new technologies and the flexibility of the programme, which allowed participants to adjust the duration and frequency of sessions according to their needs, facilitating integration into their daily routines (101–104). Personalisation within a structured framework not only favours engagement but also the long-term sustainability of the programme.
Understanding the factors that influence adherence to physical exercise is essential for ensuring long-term commitment and success (105–107). Men are generally more motivated by challenges, competition, social recognition, and the desire to increase muscle size and strength. They also tend to prefer high-intensity, competitive exercises that focus on the upper body. In contrast, women are typically driven by goals related to enhancing their physical appearance, toning their muscles, and managing body weight. Additionally, they show a greater preference for supervised activities that target the lower body (108).
Sex-based differences in adaptation to training have a physiological basis. Variations have been identified in fatigue resistance (109–111), inflammatory response following eccentric exercise (112), recovery time (113), and muscle fibre composition (114, 115). While Wilmore (116) found that both sexes achieved similar relative gains in strength and lean body mass, subsequent studies have produced mixed results (117–122), depending on whether the data are presented in absolute or relative terms. A recent meta-analysis by Roberts et al. (123) found that men and women respond similarly in terms of strength and muscle size development in the lower body. However, women demonstrate greater relative strength gains in the upper body.
During endurance training, women utilise more fatty acids than men, which enhances carbohydrate conservation and reduces neuromuscular fatigue, with fewer peripheral alterations. It has been suggested that oestrogen may have a protective effect against damage caused by repetitive eccentric muscle actions (124). At the cardiac level, functional adaptations of the left ventricle to endurance training are less pronounced or even absent in women despite similar hypertrophic responses in both sexes (125). Furthermore, oxygen transport, constrained by the lower total haemoglobin mass in women (126, 127), limits their ability to achieve a higher VO2 peak (128). Their relatively lower blood volume also restricts the amount of blood available to active muscles without compromising supply to other tissues, potentially impacting aerobic performance (129).
4.4 Quality of life and well-being
The findings of this study highlight the significant impact of structured physical exercise programmes on health-related quality of life and psychological well-being, as evidenced by the improvements observed in both the AUG and PTG compared to the CG. These results reflect the complex interactions between the physiological benefits of exercise and participants' subjective perceptions, aligning with previous research.
In the PTG, significant improvements were noted across multiple SF-36 dimensions, including physical role (p = 0.02), bodily pain (p = 0.03), general health (p = 0.03), vitality (p < 0.01), mental health (p = 0.01), and health evolution (p < 0.01). These outcomes can be attributed to the structured, supervised nature of the programme, which ensured proper intensity, adherence, and consistent feedback (130). This approach likely optimised the physical and mental health benefits of exercise by promoting regional musculoskeletal adaptations and alleviating dysfunction, as well as through the progressive manipulation of training variables (131, 132). Conversely, the AUG showed significant improvements primarily in health evolution (p < 0.01), with moderate effect sizes observed in vitality (d = 0.62), emotional role (d = 0.57), and mental health (d = 0.50). These results demonstrate the effectiveness of self-directed exercise programmes, particularly in enhancing perceived energy and reducing fatigue, though the lack of professional feedback and social interaction may limit adherence and training intensity, which could lead to negligible effects in psychological assessments. Previous research has shown that combining resistance training with aerobic exercise yields greater benefits compared to aerobic exercise alone (133). In contrast, the CG did not experience significant changes in any of the SF-36 dimensions, underscoring the importance of regular exercise, whether supervised or self-directed, in improving quality of life and psychological well-being. These findings are consistent with previous studies highlighting exercise's role in alleviating physical and emotional limitations (134).
Psychological well-being outcomes further support the benefits of exercise. Intra-group analyses revealed significant improvements in vitality (MD = 1.08) and negative affective state (MD = 0.91) for the AUG, while the PTG showed improvements in vitality (MD = 0.98), positive affective state (MD = 0.79), and negative affective state (MD = 1.11). Between-group comparisons confirmed significant differences between the intervention groups and the CG in all variables (p < 0.05). These results can be attributed to the capacity of exercise to reduce stress, enhance emotional regulation, and foster positive psychological states (135). While both intervention groups achieved notable gains, the PTG demonstrated slightly greater improvements, likely due to the structured feedback and motivational environment provided by trainer-led sessions.
The absence of significant changes in social and physical function may be due to a ceiling effect, as these dimensions are less impacted in moderately active populations (136). Nonetheless, the differences in changes between groups due to exercise modality underscores the importance of programme design in maximising perceived benefits. Overall, these findings reinforce the multifaceted benefits of well-designed exercise programmes on health-related quality of life and psychological well-being.
4.5 Training load
Training load, as measured by eTRIMP, was significantly higher in the PTG (p < 0.01), while the sRPE method showed no difference in the subjective perception of load between groups. This suggests that while eTRIMP reflects a greater reliance on high-intensity sessions in the trained group (facilitated by the coach's technical guidance and group training dynamics), the perceived demand and appropriateness of the exercise load were comparable between groups. In the AUG group, this equivalence can be attributed to the use of tools such as HRV monitoring and autonomous decision-making based on these readings. However, the shorter cumulative time in high-intensity zones in the AUG (3.72% vs. 38.80%, p < 0.01) probably explains the smaller improvements in fitness variables. These results emphasise the need to optimise feedback strategies in self-directed programmes to ensure greater exposure to high-intensity training. On the other hand, AUG exhibited a greater emphasis on low-intensity sessions, which may be more appropriate for individuals with initial fitness limitations but less effective in driving significant physiological adaptations. Previous evidence indicates that self-selected intensity in exercise is often inferior to supervised sessions in promoting improvements in fitness (74–78), probably due to psychological, social and technical factors. Although the total tolerated load was equivalent between groups, the lack of differences in perceived load, despite substantial variations in intensity distribution, suggests that the presence of a coach may not be essential to induce adaptations in sedentary populations. In self-directed programmes, HRV emerges as a critical tool to guide decision-making and replicate the technical adjustments typically associated with direct supervision.
Group interaction in supervised programmes also plays a crucial role, enhancing performance through implicit competition, social pressure and motivational support (137–140). According to self-determination theory (141), group environments that promote a positive motivational climate reinforce connectedness, competence and autonomy, facilitating more intense and sustained effort over time.
4.6 Limitations
This study had several limitations. First, the final sample number of participants who completed the study in both experimental groups reduced statistical power, thereby limiting the applicability of the findings to the broader population. Second, the proportion of women was twice that of men. The low participation of men in structured physical exercise programmes may be influenced by a combination of psychological, social and cultural factors. Gender stereotypes play a significant role, as men often perceive such programmes as less appealing, associating them with lower intensity compared to activities like weightlifting (142). Furthermore, these programmes may not align with men's preferences for independence, competitiveness and self-direction, as they tend to prefer varying their routines according to personal interests and goals rather than adhering to a pre-defined structure (143–145). Some men also perceive these programmes as insufficiently challenging (146) or view them as socially accepted activities primarily targeted at women, which reinforces their lack of interest (147, 148). Lastly, the study did not include a post-intervention follow-up to assess whether participants who completed the programme-maintained adherence to physical exercise over time. Such follow-up data could provide valuable insights into the long-term effectiveness of the intervention.
4.7 Relevance for clinical practice and public health
The observed increases in VO2 peak 1.62 ml·kg−1·min−1 in the AUG and 2.81 ml·kg−1·min−1 in the PTG, may have significant long-term health implications. Research suggests that a 1 ml·kg−1·min−1 increase in VO2 peak is associated with a 9% reduction in the relative risk of all-cause mortality (149, 150), an impact comparable to a 10 cm decrease in waist circumference or a 10-mmHg reduction in systolic blood pressure (151). Importantly, aerobic capacity, like physical exercise, independently reduces mortality risk, emphasising the critical relevance of the improvements in VO2 peak observed in this study (152).
Technology-guided autonomous physical exercise programmes, such as the Selftraining UMH app, provide an accessible and flexible alternative, particularly in scenarios where face-to-face attendance is not feasible. While it is not intended to replace professionally supervised training, it can serve as an initial step toward online programmes, potentially encouraging participants to seek face-to-face guidance in the future. For sustained long-term benefits, a hybrid approach that combines technological autonomy with human supervision may be particularly effective (153). In this regard, the results highlight the relevance of maintaining constant user interaction with the app to maximise the intervention's success (154). This highlights the potential for mobile apps to bridge gaps in access to exercise programmes while complementing traditional supervised modalities, thereby enhancing public health outcomes.
4.8 Practical applications
For older adults, the application includes a library of video-based training sessions specifically designed for their age group. The updated version of the application, “Selftraining Health”, is aimed at enhancing emotional well-being and physical health in individuals with mental health conditions and addictions.
The Selftraining UMH application, based on HRV, could be implemented in rehabilitation programmes. Before its use for different clinical populations, it would be necessary to adapt the training sessions and validate them according to the specific needs of the target population.
The practical implementation of this application in digital health training enables users, regardless of their familiarity with technology, to access personalised exercise programmes that can be performed independently. Moreover, by integrating wearable technologies to track HRV, Selftraining UMH facilitates precise monitoring of the user's physical condition, promoting continuous education in the use of emerging health technologies. This combination of physical exercise and digital training significantly contributes to improving public health and quality of life while fostering digital literacy in the healthcare domain.
4.9 Future research
Future research involving the Selftraining UMH application could adopt a crossover design, allowing participants in the Self-Directed Training modality to switch to the Personal Trainer-Led Training modality and vice versa. This approach would enable a direct comparison of the results obtained across both training modalities. Additionally, future studies could explore the effectiveness of the programme in other age groups, such as younger adults and older adults, to evaluate its applicability and impact across a broader demographic spectrum.
5 Conclusions
In conclusion, the findings of this study demonstrated comparable levels of adherence and physical fitness in both experimental groups before and after the training period. Additionally, significant improvements were observed within both groups in fitness-related variables when comparing pre- and post-intervention assessments. When analysing changes between groups, both experimental groups showed significant differences compared to the CG in fitness-related variables. However, statistical differences between the AUG and the PTG were observed only in upper and lower body strength. These results suggest that autonomously guided physical exercise, prescribed through HRV monitoring via the Selftraining UMH application, is a practical and effective tool for individuals seeking to initiate a physical exercise programme but face barriers to accessing training centres or supervised sessions due to cost or time constraints. However, given the results, supervised HRV-guided training is more effective than autonomous HRV-guided training for improving strength levels. Therefore, to optimise improvements in physical fitness, it is recommended that physical exercise programmes are carried out under the supervision of qualified exercise and sports professionals.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Universidad Miguel Hernández de Elche (Ref: DPS.JSM.02.18). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AC-L: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. AM-R: Data curation, Formal analysis, Writing – review & editing. JS: Investigation, Methodology, Writing – original draft. DP: Investigation, Validation, Writing – original draft. AJ: Investigation, Methodology, Writing – original draft. IP-G: Investigation, Validation, Writing – original draft. MM-R: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This work was supported by the Ministerio de Ciencia e Innovación under Grant PID 2019-107721RB-I00; and Ministerio de Educación, Cultura y Deporte under Grant FPU19/01032.
Acknowledgments
The authors would like to thank the Graduates in Physical Activity and Sport Sciences Juan Arturo Ballester-Ferrer and Roberto Montón-Martínez for their help in the direction and supervision of the training sessions of the face-to-face group carried out at the Sports Research Centre of Miguel Hernández University of Elche. Sabina Baladzhaeva for her assistance in proofreading the English spelling.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2025.1578478/full#supplementary-material
References
1. Katzmarzyk PT, Friedenreich C, Shiroma EJ, Lee IM. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries. Br J Sports Med. (2022) 56(2):101–6. doi: 10.1136/bjsports-2020-103640
2. Erickson KI, Voss MW, Prakash RS, Basak C, Szabo A, Chaddock L, et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci U S A. (2011) 108(7):3017–22. doi: 10.1073/pnas.1015950108
3. O'Donovan G, Blazevich AJ, Boreham C, Cooper AR, Crank H, Ekelund U, et al. The ABC of physical activity for health: a consensus statement from the British association of sport and exercise sciences. J Sports Sci. (2010) 28(6):573–91. doi: 10.1080/02640411003671212
4. Organization WH. Global Action Plan on Physical Activity 2018-2030: More Active People for a Healthier World. Pennsylvania: Lippincott Williams & Wilkins (2023).
5. Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. (2018) 6(10):e1077–e86. doi: 10.1016/S2214-109X(18)30357-7
6. Hillsdon M, Foster C, Thorogood M. Interventions for the promotion of physical activity. Cochrane Database Syst Rev. (2001) (3):Cd003180. doi: 10.1002/14651858.CD003180
7. Wang Y, Liu X, Wang W, Shi Y, Ji X, Hu L, et al. Adherence, efficacy, and safety of wearable technology-assisted combined home-based exercise in Chinese patients with ankylosing spondylitis: randomized pilot controlled clinical trial. J Med Internet Res. (2022) 24(1):e29703. doi: 10.2196/29703
8. Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: the evidence. CMAJ. (2006) 174(6):801–9. doi: 10.1503/cmaj.051351
9. Buckingham SA, Taylor RS, Jolly K, Zawada A, Dean SG, Cowie A, et al. Home-based versus centre-based cardiac rehabilitation: abridged cochrane systematic review and meta-analysis. Open Heart. (2016) 3(2):e000463. doi: 10.1136/openhrt-2016-000463
10. Peluso MA, Guerra de Andrade LH. Physical activity and mental health: the association between exercise and mood. Clinics (Sao Paulo, Brazil). (2005) 60(1):61–70. doi: 10.1590/S1807-59322005000100012
11. Casanova-Lizón A, Sarabia JM, Pastor D, Javaloyes A, Peña-González I, Moya-Ramón M. Designing an app to promote physical exercise in sedentary people using a day-to-day algorithm to ensure a healthy self-programmed exercise training. Int J Environ Res Public Health. (2023) 20(2):1528. doi: 10.3390/ijerph20021528
12. Jones DL, Bhanegaonkar AJ, Billings AA, Kriska AM, Irrgang JJ, Crossett LS, et al. Differences between actual and expected leisure activities after total knee arthroplasty for osteoarthritis. J Arthroplasty. (2012) 27(7):1289–96. doi: 10.1016/j.arth.2011.10.030
13. Duong V, Dennis S, Ferreira ML, Heller G, Nicolson PJA, Robbins SR, et al. Predictors of adherence to a step count intervention following total knee replacement: an exploratory cohort study. J Orthop Sports Phys Ther. (2022) 52(9):620–9. doi: 10.2519/jospt.2022.11133
14. Solomon DH, Rudin RS. Digital health technologies: opportunities and challenges in rheumatology. Nat Rev Rheumatol. (2020) 16(9):525–35. doi: 10.1038/s41584-020-0461-x
15. Grunberg VA, Greenberg J, Mace RA, Bakhshaie J, Choi KW, Vranceanu AM. Fitbit activity, quota-based pacing, and physical and emotional functioning among adults with chronic pain. J Pain. (2022) 23(11):1933–44. doi: 10.1016/j.jpain.2022.07.003
16. Bouchard C, Rankinen T. Individual differences in response to regular physical activity. Med Sci Sports Exercise. (2001) 33(6 Suppl):S446–51. discussion S52–3. doi: 10.1097/00005768-200106001-00013
17. Aubert AE, Seps B, Beckers F. Heart rate variability in athletes. Sports Med. (2003) 33(12):889–919. doi: 10.2165/00007256-200333120-00003
18. Singh V, Gupta A, Sohal JS, Singh A. A unified non-linear approach based on recurrence quantification analysis and approximate entropy: application to the classification of heart rate variability of age-stratified subjects. Med Biol Eng Comput. (2019) 57(3):741–55. doi: 10.1007/s11517-018-1914-0
19. Bellenger CR, Fuller JT, Thomson RL, Davison K, Robertson EY, Buckley JD. Monitoring athletic training status through autonomic heart rate regulation: a systematic review and meta-analysis. Sports Med. (2016) 46(10):1461–86. doi: 10.1007/s40279-016-0484-2
20. Halson SL. Monitoring training load to understand fatigue in athletes. Sports Med. (2014) 44(Suppl 2):S139–47. doi: 10.1007/s40279-014-0253-z
21. Plews DJ, Scott B, Altini M, Wood M, Kilding AE, Laursen PB. Comparison of heart-rate-variability recording with smartphone photoplethysmography, Polar H7 chest strap, and electrocardiography. Int J Sports Physiol Perform. (2017) 12(10):1324–8. doi: 10.1123/ijspp.2016-0668
22. Moya-Ramon M, Mateo-March M, Peña-González I, Zabala M, Javaloyes A. Validity and reliability of different smartphones applications to measure HRV during short and ultra-short measurements in elite athletes. Comput Methods Programs Biomed. (2022) 217:106696. doi: 10.1016/j.cmpb.2022.106696
23. Perrotta AS, Jeklin AT, Hives BA, Meanwell LE, Warburton DER. Validity of the elite HRV smartphone application for examining heart rate variability in a field-based setting. J Strength Cond Res. (2017) 31(8):2296–302. doi: 10.1519/JSC.0000000000001841
24. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World health organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54(24):1451–62. doi: 10.1136/bjsports-2020-102955
25. Thomas S, Reading J, Shephard RJ. Revision of the physical activity readiness questionnaire (PAR-Q). Can J Sport Sci. (1992) 17(4):338–45.1330274
26. Bruce RA. Exercise testing of patients with coronary heart disease. Principles and normal standards for evaluation. Ann Clin Res. (1971) 3(6):323–32.5156892
27. Bayles MP. ACSM’s Exercise Testing and Prescription. Pennsylvania, USA: Lippincott Williams & Wilkins (2023).
28. Lorenzetti S, Ostermann M, Zeidler F, Zimmer P, Jentsch L, List R, et al. How to squat? Effects of various stance widths, foot placement angles and level of experience on knee, hip and trunk motion and loading. BMC Sports Sci Med Rehabil. (2018) 10:14. doi: 10.1186/s13102-018-0103-7
29. Speer KE, Semple S, Naumovski N, McKune AJ. Measuring heart rate variability using commercially available devices in healthy children: a validity and reliability study. Eur J Investig Health Psychol Educ. (2020) 10(1):390–404.34542492
30. Bourdillon N, Schmitt L, Yazdani S, Vesin JM, Millet GP. Minimal window duration for accurate HRV recording in athletes. Front Neurosci. (2017) 11:456. doi: 10.3389/fnins.2017.00456
31. Tarvainen MP, Niskanen JP, Lipponen JA, Ranta-Aho PO, Karjalainen PA. Kubios HRV–heart rate variability analysis software. Comput Methods Programs Biomed. (2014) 113(1):210–20. doi: 10.1016/j.cmpb.2013.07.024
32. Plews DJ, Laursen PB, Stanley J, Kilding AE, Buchheit M. Training adaptation and heart rate variability in elite endurance athletes: opening the door to effective monitoring. Sports Med. (2013) 43(9):773–81. doi: 10.1007/s40279-013-0071-8
33. Lipponen JA, Tarvainen MP. A robust algorithm for heart rate variability time series artefact correction using novel beat classification. J Med Eng Technol. (2019) 43(3):173–81. doi: 10.1080/03091902.2019.1640306
34. Ren Z, Zhu H, Zhang T, Hua H, Zhao K, Yang N, et al. Effects of a 12-week transtheoretical model-based exercise training program in Chinese postoperative bariatric patients: a randomized controlled trial. Obes Surg. (2021) 31(10):4436–51. doi: 10.1007/s11695-021-05607-3
35. Scheid JL, O’Donnell E. Revisiting heart rate target zones through the lens of wearable technology. ACSM’s Health Fit J. (2019) 23(3):21–6. doi: 10.1249/FIT.0000000000000477
36. Brazier JE, Harper R, Jones NM, O'Cathain A, Thomas KJ, Usherwood T, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ (Clinical Research ed). (1992) 305(6846):160–4. doi: 10.1136/bmj.305.6846.160
37. Ware JE, Snow KK, Kosinski M, Gandek B. SF-36 Health Survey. Manual and Interpretation Guide. Boston, MA: The Health Institute, New England Medical Center (1993).
38. Alonso J, Prieto L, Antó JM. The Spanish version of the SF-36 health survey (the SF-36 health questionnaire): an instrument for measuring clinical results. Med Clin (Barc). (1995) 104(20):771–6.7783470
39. Ryan RM, Frederick C. On energy, personality, and health: subjective vitality as a dynamic reflection of well-being. J Pers. (1997) 65(3):529–65. doi: 10.1111/j.1467-6494.1997.tb00326.x
40. Molina-García J, Castillo I, Pablos C. Bienestar psicológico y práctica deportiva en universitarios. Motricidad Eur J Hum Mov. (2007) 18:79–91.
41. Mackinnon A, Jorm AF, Christensen H, Korten AE, Jacomb PA, Rodgers B. A short form of the positive and negative affect schedule: evaluation of factorial validity and invariance across demographic variables in a community sample. Pers Individ Dif. (1999) 27(3):405–16. doi: 10.1016/S0191-8869(98)00251-7
42. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. (1988) 54(6):1063–70. doi: 10.1037/0022-3514.54.6.1063
43. López-Gómez I, Hervás G, Vázquez C. Adaptación de las “escalas de afecto positivo y negativo” (PANAS) en una muestra general española. Psicol Conduct. (2015) 23(3):529.
44. Kasper K. Sports training principles. Curr Sports Med Rep. (2019) 18(4):95–6. doi: 10.1249/JSR.0000000000000576
45. Singstad BJ, Azulay N, Bjurstedt A, Bjørndal SS, Drageseth MF, Engeset P, et al. Estimation of heart rate variability from finger photoplethysmography during rest, mild exercise and mild mental stress. J Electr Bioimpedance. (2021) 12(1):89–102. doi: 10.2478/joeb-2021-0012
46. Javaloyes A, Sarabia JM, Lamberts RP, Plews D, Moya-Ramon M. Training prescription guided by heart rate variability vs. Block periodization in well-trained cyclists. J Strength Cond Res. (2020) 34(6):1511–8. doi: 10.1519/JSC.0000000000003337
47. Plews DJ, Laursen PB, Kilding AE, Buchheit M. Heart rate variability in elite triathletes, is variation in variability the key to effective training? A case comparison. Eur J Appl Physiol. (2012) 112(11):3729–41. doi: 10.1007/s00421-012-2354-4
48. Javaloyes A, Sarabia JM, Lamberts RP, Moya-Ramon M. Training prescription guided by heart-rate variability in cycling. Int J Sports Physiol Perform. (2019) 14(1):23–32. doi: 10.1123/ijspp.2018-0122
49. Kiviniemi AM, Hautala AJ, Kinnunen H, Tulppo MP. Endurance training guided individually by daily heart rate variability measurements. Eur J Appl Physiol. (2007) 101(6):743–51. doi: 10.1007/s00421-007-0552-2
51. Borg G, Hassmén P, Lagerström M. Perceived exertion related to heart rate and blood lactate during arm and leg exercise. Eur J Appl Physiol Occup Physiol. (1987) 56(6):679–85. doi: 10.1007/BF00424810
52. Keselman HJ, Huberty CJ, Lix LM, Olejnik S, Cribbie RA, Donahue B, et al. Statistical practices of educational researchers: an analysis of their ANOVA, MANOVA, and ANCOVA analyses. Rev Educ Res. (1998) 68(3):350–86. doi: 10.3102/00346543068003350
53. Cohen J. Quantitative methods in psychology: a power primer. Psychol Bull. (1992) 112:155–9. doi: 10.1037/0033-2909.112.1.155
54. Schober P, Boer C, Schwarte LA. Correlation coefficients: appropriate use and interpretation. Anesth Analg. (2018) 126(5):1763–8. doi: 10.1213/ANE.0000000000002864
55. Love J, Selker R, Marsman M, Jamil T, Dropmann D, Verhagen J, et al. JASP: graphical statistical software for common statistical designs. J Stat Softw. (2019) 88:1–17. doi: 10.18637/jss.v088.i02
56. Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, et al. CONSORT 2010 Statement: extension to randomised pilot and feasibility trials. BMJ (Clinical Research ed). (2016) 355:i5239. doi: 10.1136/bmj.i5239
57. Cárcamo-Regla R, Carrasco-Marín F, Ochoa-Rosales C, Zapata-Lamana R, Rozas K, Martorell M, et al. Metabolic and cardiorespiratory fitness changes in women undergoing a physical exercise program assisted by a mobile application. A non-randomized controlled study. Rev Med Chil. (2023) 151(7):869–79. doi: 10.4067/s0034-98872023000700869
58. Jo HS, Kim HM, Go CH, Yu HY, Park HK, Han JY. Effectiveness of home-based cardiac rehabilitation with optimized exercise prescriptions using a mobile healthcare app in patients with acute myocardial infarction: a randomized controlled trial. Life (Basel, Switzerland). (2024) 14(9):1122. doi: 10.3390/life14091122
59. Nam JS, Kim HA, Kwak TJ, Cho KH, Jung IY, Moon CW. Feasibility of mobile health app-based home aerobic exercise for physical performance in healthy young adults. Ann Rehabil Med. (2024) 48(1):75–85. doi: 10.5535/arm.230023
60. Gómez-Cuesta N, Mateo-Orcajada A, Meroño L, Abenza-Cano L, Vaquero-Cristóbal R. A mobile app-based intervention improves anthropometry, body composition and fitness, regardless of previous active-inactive status: a randomized controlled trial. Front Public Health. (2024) 12:1380621. doi: 10.3389/fpubh.2024.1380621
61. Yerrakalva D, Yerrakalva D, Hajna S, Griffin S. Effects of mobile health app interventions on sedentary time, physical activity, and fitness in older adults: systematic review and meta-analysis. J Med Internet Res. (2019) 21(11):e14343. doi: 10.2196/14343
62. Gregory ME, Cao W, Rahurkar S, Haroun F, Stock JC, Ghazi SM, et al. Effectiveness of mobile health for exercise promotion on cardiorespiratory fitness after a cancer diagnosis: a systematic review and meta-analysis. Cancer Med. (2024) 13(17):e7079. doi: 10.1002/cam4.7079
63. Rospo G, Valsecchi V, Bonomi AG, Thomassen IW, van Dantzig S, La Torre A, et al. Cardiorespiratory improvements achieved by American college of sports medicine’s exercise prescription implemented on a mobile app. JMIR Mhealth Uhealth. (2016) 4(2):e77. doi: 10.2196/mhealth.5518
64. Mateo-Orcajada A, Vaquero-Cristóbal R, Abenza-Cano L. Importance of training volume through the use of step trackers apps promoted from the subject of physical education to change body composition, physical fitness and physical activity in adolescents and the influence of gender(✰,✰✰). Physiol Behav. (2024) 273:114402. doi: 10.1016/j.physbeh.2023.114402
65. Laranjo L, Ding D, Heleno B, Kocaballi B, Quiroz JC, Tong HL, et al. Do smartphone applications and activity trackers increase physical activity in adults? Systematic review, meta-analysis and metaregression. Br J Sports Med. (2021) 55(8):422–32. doi: 10.1136/bjsports-2020-102892
66. Bond DS, Thomas JG, Raynor HA, Moon J, Sieling J, Trautvetter J, et al. B-MOBILE–a smartphone-based intervention to reduce sedentary time in overweight/obese individuals: a within-subjects experimental trial. PLoS One. (2014) 9(6):e100821. doi: 10.1371/journal.pone.0100821
67. Romeo A, Edney S, Plotnikoff R, Curtis R, Ryan J, Sanders I, et al. Can smartphone apps increase physical activity? Systematic review and meta-analysis. J Med Internet Res. (2019) 21(3):e12053. doi: 10.2196/12053
68. Bird SP, Tarpenning KM, Marino FE. Designing resistance training programmes to enhance muscular fitness: a review of the acute programme variables. Sports Med. (2005) 35(10):841–51. doi: 10.2165/00007256-200535100-00002
69. Mazzetti SA, Kraemer WJ, Volek JS, Duncan ND, Ratamess NA, Gómez AL, et al. The influence of direct supervision of resistance training on strength performance. Med Sci Sports Exercise. (2000) 32(6):1175–84. doi: 10.1097/00005768-200006000-00023
70. Gourgoulis V, Aggeloussis N, Kasimatis P, Mavromatis G, Garas A. Effect of a submaximal half-squats warm-up program on vertical jumping ability. J Strength Cond Res. (2003) 17(2):342–4. doi: 10.1519/1533-4287(2003)017%3C0342:eoashw%3E2.0.co;2
71. Kim Y, White T, Wijndaele K, Sharp SJ, Wareham NJ, Brage S. Adiposity and grip strength as long-term predictors of objectively measured physical activity in 93,015 adults: the UK biobank study. Int J Obes. (2017) 41(9):1361–8. doi: 10.1038/ijo.2017.122
72. Kraemer WJ, Ratamess NA, French DN. Resistance training for health and performance. Curr Sports Med Rep. (2002) 1(3):165–71. doi: 10.1249/00149619-200206000-00007
73. Ryan AS, Treuth MS, Hunter GR, Elahi D. Resistive training maintains bone mineral density in postmenopausal women. Calcif Tissue Int. (1998) 62(4):295–9. doi: 10.1007/s002239900434
74. Dias MRC, Simão R, Saavedra FJF, Buzzachera CF, Fleck S. Self-selected training load and RPE during resistance and aerobic training among recreational exercisers. Percept Mot Skills. (2018) 125(4):769–87. doi: 10.1177/0031512518774461
75. Elsangedy HM, Krause MP, Krinski K, Alves RC, Hsin Nery Chao C, da Silva SG. Is the self-selected resistance exercise intensity by older women consistent with the American college of sports medicine guidelines to improve muscular fitness? J Strength Cond Res. (2013) 27(7):1877–84. doi: 10.1519/JSC.0b013e3182736cfa
76. Focht BC. Perceived exertion and training load during self-selected and imposed-intensity resistance exercise in untrained women. J Strength Cond Res. (2007) 21(1):183–7. doi: 10.1519/00124278-200702000-00033
77. Lacroix A, Hortobágyi T, Beurskens R, Granacher U. Effects of supervised vs. unsupervised training programs on balance and muscle strength in older adults: a systematic review and meta-analysis. Sports Med. (2017) 47(11):2341–61. doi: 10.1007/s40279-017-0747-6
78. Thiebaud RS, Funk MD, Abe T. Home-based resistance training for older adults: a systematic review. Geriatr Gerontol Int. (2014) 14(4):750–7. doi: 10.1111/ggi.12326
79. Campbell KL, Neil SE, Winters-Stone KM. Review of exercise studies in breast cancer survivors: attention to principles of exercise training. Br J Sports Med. (2012) 46(13):909–16. doi: 10.1136/bjsports-2010-082719
80. Dipla K. The FITT principle in individuals with type 2 diabetes: from cellular adaptations to individualized exercise prescription. Adv Med Med Res. (2017) 22:1–18. doi: 10.9734/JAMMR/2017/34927
81. Wagner P, Brehm W, Sygusch R. The seven-sequence intervention: sedentary adults on their way to fitness and health. Res Sports Med. (2004) 12(4):265–82. doi: 10.1080/15438620490887023
82. Wilke J, Kaiser S, Niederer D, Kalo K, Engeroff T, Morath C, et al. Effects of high-intensity functional circuit training on motor function and sport motivation in healthy, inactive adults. Scand J Med Sci Sports. (2019) 29(1):144–53. doi: 10.1111/sms.13313
83. Westcott WL. Resistance training is medicine: effects of strength training on health. Curr Sports Med Rep. (2012) 11(4):209–16. doi: 10.1249/JSR.0b013e31825dabb8
84. Lucini D, Pagani M. Exercise prescription to foster health and well-being: a behavioral approach to transform barriers into opportunities. Int J Environ Res Public Health. (2021) 18(3):968. doi: 10.3390/ijerph18030968
85. Medellin Ruiz JP, Rubio-Arias JÁ, Clemente-Suarez VJ, Ramos-Campo DJ. Effectiveness of training prescription guided by heart rate variability versus predefined training for physiological and aerobic performance improvements: a systematic review and meta-analysis. Appl Sci. (2020) 10(23):8532. doi: 10.3390/app10238532
86. Manresa-Rocamora A, Flatt AA, Casanova-Lizón A, Ballester-Ferrer JA, Sarabia JM, Vera-Garcia FJ, et al. Heart rate-based indices to detect parasympathetic hyperactivity in functionally overreached athletes. A meta-analysis. Scand J Med Sci Sports. (2021) 31(6):1164–82. doi: 10.1111/sms.13932
87. da Silva DF, Ferraro ZM, Adamo KB, Machado FA. Endurance running training individually guided by HRV in untrained women. J Strength Cond Res. (2019) 33(3):736–46. doi: 10.1519/JSC.0000000000002001
88. Vesterinen V, Nummela A, Heikura I, Laine T, Hynynen E, Botella J, et al. Individual endurance training prescription with heart rate variability. Med Sci Sports Exercise. (2016) 48(7):1347–54. doi: 10.1249/MSS.0000000000000910
89. Schmitt L, Willis SJ, Fardel A, Coulmy N, Millet GP. Live high-train low guided by daily heart rate variability in elite nordic-skiers. Eur J Appl Physiol. (2018) 118(2):419–28. doi: 10.1007/s00421-017-3784-9
90. Manresa-Rocamora A, Sarabia JM, Guillen-Garcia S, Pérez-Berbel P, Miralles-Vicedo B, Roche E, et al. Heart rate variability-guided training for improving mortality predictors in patients with coronary artery disease. Int J Environ Res Public Health. (2022) 19(17):10463. doi: 10.3390/ijerph191710463
91. Clemente-Suárez VJ. Periodized training achieves better autonomic modulation and aerobic performance than non-periodized training. J Sports Med Phys Fitness. (2018) 58(11):1559–64. doi: 10.23736/S0022-4707.17.07582-X
92. Yanlin C, Fei H, Shengjia X. Training variables and autonomic nervous system adaption. Chin J Tissue Eng Res. (2020) 24(2):312. doi: 10.3969/j.issn.2095-4344.1430
93. Casanova-Lizón A, Manresa-Rocamora A, Flatt AA, Sarabia JM, Moya-Ramón M. Does exercise training improve cardiac-parasympathetic nervous system activity in sedentary people? A systematic review with meta-analysis. Int J Environ Res Public Health. (2022) 19(21):13899. doi: 10.3390/ijerph192113899
94. Manresa-Rocamora A, Ribeiro F, Sarabia JM, Íbias J, Oliveira NL, Vera-García FJ, et al. Exercise-based cardiac rehabilitation and parasympathetic function in patients with coronary artery disease: a systematic review and meta-analysis. Clin Auton Res. (2021) 31(2):187–203. doi: 10.1007/s10286-020-00687-0
95. Pearson MJ, Smart NA. Exercise therapy and autonomic function in heart failure patients: a systematic review and meta-analysis. Heart Fail Rev. (2018) 23(1):91–108. doi: 10.1007/s10741-017-9662-z
96. Picard M, Tauveron I, Magdasy S, Benichou T, Bagheri R, Ugbolue UC, et al. Effect of exercise training on heart rate variability in type 2 diabetes mellitus patients: a systematic review and meta-analysis. PLoS One. (2021) 16(5):e0251863. doi: 10.1371/journal.pone.0251863
97. Brook RD, Julius S. Autonomic imbalance, hypertension, and cardiovascular risk. Am J Hypertens. (2000) 13(6 Pt 2):112s–22. doi: 10.1016/S0895-7061(00)00228-4
98. National Research Council Panel on Race E, Health in Later L. The national academies collection: reports funded by national institutes of health. In: Anderson NB, Bulatao RA, Cohen B, editors. Critical Perspectives on Racial and Ethnic Differences in Health in Late Life. Washington (DC): National Academies Press (US) Copyright © 2004, National Academy of Sciences (2004). doi: 10.17226/11086
99. Sandercock GR, Bromley PD, Brodie DA. Effects of exercise on heart rate variability: inferences from meta-analysis. Med Sci Sports Exercise. (2005) 37(3):433–9. doi: 10.1249/01.MSS.0000155388.39002.9D
100. Kelders SM, Kok RN, Ossebaard HC, Van Gemert-Pijnen JE. Persuasive system design does matter: a systematic review of adherence to web-based interventions. J Med Internet Res. (2012) 14(6):e152. doi: 10.2196/jmir.2104
101. Mehra S, van den Helder J, Kröse BJ, Engelbert RH, Weijs PJ, Visser B. The Use of a tablet to increase older adults' exercise adherence. In: Ali R, Lugrin B, Charles F, editors. International Conference on Persuasive Technology. Vol. 16. Cham: Springer (2021). p. 47–54. doi: 10.1007/978-3-030-79460-6_4
102. Valenzuela T, Okubo Y, Woodbury A, Lord SR, Delbaere K. Adherence to technology-based exercise programs in older adults: a systematic review. J Geriatr Phys Ther. (2018) 41(1):49–61. doi: 10.1519/JPT.0000000000000095
103. Geraedts HA, Zijlstra W, Zhang W, Bulstra S, Stevens M. Adherence to and effectiveness of an individually tailored home-based exercise program for frail older adults, driven by mobility monitoring: design of a prospective cohort study. BMC Public Health. (2014) 14:570. doi: 10.1186/1471-2458-14-570
104. Jungreitmayr S, Ring-Dimitriou S, Trukeschitz B, Eisenberg S, Schneider C. Effects of an information and communication technology-based fitness program on strength and balance in female home care service users. Int J Environ Res Public Health. (2021) 18(15):7955. doi: 10.3390/ijerph18157955
105. Kopcakova J, Veselska ZD, Geckova AM, Kalman M, van Dijk JP, Reijneveld SA. Do motives to undertake physical activity relate to physical activity in adolescent boys and girls? Int J Environ Res Public Health. (2015) 12(7):7656–66. doi: 10.3390/ijerph120707656
106. Sherwood NE, Jeffery RW. The behavioral determinants of exercise: implications for physical activity interventions. Annu Rev Nutr. (2000) 20:21–44. doi: 10.1146/annurev.nutr.20.1.21
107. Zamai CA, Bavoso D, Rodrigues AA, Barbosa JA. Motivos de adesão, manutenção e resultados alcançados através da prática de atividades físicas em academias. Rev Saúde Meio Ambiente. (2016) 3(2):13–22.
108. Nuzzo JL. Narrative review of sex differences in muscle strength, endurance, activation, size, fiber type, and strength training participation rates, preferences, motivations, injuries, and neuromuscular adaptations. J Strength Cond Res. (2023) 37(2):494–536. doi: 10.1519/JSC.0000000000004329
109. Hunter SK. Sex differences in fatigability of dynamic contractions. Exp Physiol. (2016) 101(2):250–5. doi: 10.1113/EP085370
110. Marshall PW, Metcalf E, Hagstrom AD, Cross R, Siegler JC, Enoka RM. Changes in fatigue are the same for trained men and women after resistance exercise. Med Sci Sports Exercise. (2020) 52(1):196–204. doi: 10.1249/MSS.0000000000002103
111. Metcalf E, Hagstrom AD, Marshall PW. Trained females exhibit less fatigability than trained males after a heavy knee extensor resistance exercise session. Eur J Appl Physiol. (2019) 119(1):181–90. doi: 10.1007/s00421-018-4013-x
112. Stupka N, Lowther S, Chorneyko K, Bourgeois JM, Hogben C, Tarnopolsky MA. Gender differences in muscle inflammation after eccentric exercise. J Appl Physiol. (2000) 89(6):2325–32. doi: 10.1152/jappl.2000.89.6.2325
113. Flores DF, Gentil P, Brown LE, Pinto RS, Carregaro RL, Bottaro M. Dissociated time course of recovery between genders after resistance exercise. J Strength Cond Res. (2011) 25(11):3039–44. doi: 10.1519/JSC.0b013e318212dea4
114. Haizlip KM, Harrison BC, Leinwand LA. Sex-based differences in skeletal muscle kinetics and fiber-type composition. Physiology (Bethesda, Md). (2015) 30(1):30–9. doi: 10.1152/physiol.00024.2014
115. Staron RS, Hagerman FC, Hikida RS, Murray TF, Hostler DP, Crill MT, et al. Fiber type composition of the vastus lateralis muscle of young men and women. J Histochem Cytochem. (2000) 48(5):623–9. doi: 10.1177/002215540004800506
116. Wilmore JH. Alterations in strength, body composition and anthropometric measurements consequent to a 10-week weight training program. Med Sci Sports. (1974) 6(2):133–8. doi: 10.1249/00005768-197400620-000254461973
117. Hunter GR, Bryan DR, Wetzstein CJ, Zuckerman PA, Bamman MM. Resistance training and intra-abdominal adipose tissue in older men and women. Med Sci Sports Exercise. (2002) 34(6):1023–8. doi: 10.1097/00005768-200206000-00019
118. Hurlbut DE, Lott ME, Ryan AS, Ferrell RE, Roth SM, Ivey FM, et al. Does age, sex, or ACE genotype affect glucose and insulin responses to strength training? J Appl Physiol. (2002) 92(2):643–50. doi: 10.1152/japplphysiol.00499.2001
119. Jozsi AC, Campbell WW, Joseph L, Davey SL, Evans WJ. Changes in power with resistance training in older and younger men and women. J Gerontol A Biol Sci Med Sci. (1999) 54(11):M591–6. doi: 10.1093/gerona/54.11.M591
120. Kell RT. The influence of periodized resistance training on strength changes in men and women. J Strength Cond Res. (2011) 25(3):735–44. doi: 10.1519/JSC.0b013e3181c69f22
121. Kosek DJ, Kim JS, Petrella JK, Cross JM, Bamman MM. Efficacy of 3 days/wk resistance training on myofiber hypertrophy and myogenic mechanisms in young vs. Older adults. J Appl Physiol. (2006) 101(2):531–44. doi: 10.1152/japplphysiol.01474.2005
122. Staron RS, Karapondo DL, Kraemer WJ, Fry AC, Gordon SE, Falkel JE, et al. Skeletal muscle adaptations during early phase of heavy-resistance training in men and women. J Appl Physiol. (1994) 76(3):1247–55. doi: 10.1152/jappl.1994.76.3.1247
123. Roberts BM, Nuckols G, Krieger JW. Sex differences in resistance training: a systematic review and meta-analysis. J Strength Cond Res. (2020) 34(5):1448–60. doi: 10.1519/JSC.0000000000003521
124. Besson T, Macchi R, Rossi J, Morio CYM, Kunimasa Y, Nicol C, et al. Sex differences in endurance running. Sports Med. (2022) 52(6):1235–57. doi: 10.1007/s40279-022-01651-w
125. Diaz-Canestro C, Montero D. The impact of sex on left ventricular cardiac adaptations to endurance training: a systematic review and meta-analysis. Sports Med. (2020) 50(8):1501–13. doi: 10.1007/s40279-020-01294-9
126. Murphy WG. The sex difference in haemoglobin levels in adults—mechanisms, causes, and consequences. Blood Rev. (2014) 28(2):41–7. doi: 10.1016/j.blre.2013.12.003
127. Schmidt W, Prommer N. Impact of alterations in total hemoglobin mass on VO2max. Exerc Sport Sci Rev. (2010) 38(2):68–75. doi: 10.1097/JES.0b013e3181d4957a
128. Santisteban KJ, Lovering AT, Halliwill JR, Minson CT. Sex differences in VO2max and the impact on endurance-exercise performance. Int J Environ Res Public Health. (2022) 19(9):4946. doi: 10.3390/ijerph19094946
129. Bassareo PP, Crisafulli A. Gender differences in hemodynamic regulation and cardiovascular adaptations to dynamic exercise. Curr Cardiol Rev. (2020) 16(1):65–72. doi: 10.2174/18756557OTc0bOTciTcVY
130. Penedo FJ, Dahn JR. Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Curr Opin Psychiatry. (2005) 18(2):189–93. doi: 10.1097/00001504-200503000-00013
131. Sluka KA, Frey-Law L, Hoeger Bement M. Exercise-induced pain and analgesia? Underlying mechanisms and clinical translation. Pain. (2018) 159(Suppl 1):S91–s7. doi: 10.1097/j.pain.0000000000001235
132. Price J, Rushton A, Tyros I, Tyros V, Heneghan NR. Effectiveness and optimal dosage of exercise training for chronic non-specific neck pain: a systematic review with a narrative synthesis. PLoS One. (2020) 15(6):e0234511. doi: 10.1371/journal.pone.0234511
133. Wender CLA, Manninen M, O'Connor PJ. The effect of chronic exercise on energy and fatigue states: a systematic review and meta-analysis of randomized trials. Front Psychol. (2022) 13:907637. doi: 10.3389/fpsyg.2022.907637
134. Rejeski WJ, Brawley LR, Shumaker SA. Physical activity and health-related quality of life. Exerc Sport Sci Rev. (1996) 24:71–108. doi: 10.1249/00003677-199600240-00005
135. Ekkekakis P, Parfitt G, Petruzzello SJ. The pleasure and displeasure people feel when they exercise at different intensities: decennial update and progress towards a tripartite rationale for exercise intensity prescription. Sports Med. (2011) 41(8):641–71. doi: 10.2165/11590680-000000000-00000
136. King AC, Pruitt LA, Phillips W, Oka R, Rodenburg A, Haskell WL. Comparative effects of two physical activity programs on measured and perceived physical functioning and other health-related quality of life outcomes in older adults. J Gerontol A Biol Sci Med Sci. (2000) 55(2):M74–83. doi: 10.1093/gerona/55.2.M74
137. Zajonc RB. Social facilitation. Science. (1965) 149(3681):269–74. doi: 10.1126/science.149.3681.269
138. Radel R, Sarrazin P, Legrain P, Wild TC. Social contagion of motivation between teacher and student: analyzing underlying processes. J Educ Psychol. (2010) 102(3):577. doi: 10.1037/a0019051
139. Coppack RJ, Kristensen J, Karageorghis CI. Use of a goal setting intervention to increase adherence to low back pain rehabilitation: a randomized controlled trial. Clin Rehabil. (2012) 26(11):1032–42. doi: 10.1177/0269215512436613
140. Ekkekakis P, Hartman ME, Ladwig MA. When studying affective responses to exercise, the definition of “intensity” must reference homeostatic perturbations: a retort to Vollaard et al. J Sport Exerc Psychol. (2024) 46(2):66–72. doi: 10.1123/jsep.2024-0064
141. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. (2000) 55(1):68–78. doi: 10.1037/0003-066X.55.1.68
142. Howe HS, Welsh TN, Sabiston CM. The association between gender role stereotypes, resistance training motivation, and participation. Psychol Sport Exerc. (2017) 33:123–30. doi: 10.1016/j.psychsport.2017.08.006
143. Geary DC. Male, Female: The Evolution of Human sex Differences. Washington, DC: American Psychological Association (1998).
144. Lever J. Sex Differences in the Complexity of Children’s Play and Games. Childhood Socialization: Routledge (2020). p. 325–43.
145. Rose AJ, Rudolph KD. A review of sex differences in peer relationship processes: potential trade-offs for the emotional and behavioral development of girls and boys. Psychol Bull. (2006) 132(1):98–131. doi: 10.1037/0033-2909.132.1.98
146. Teixeira PJ, Carraça EV, Markland D, Silva MN, Ryan RM. Exercise, physical activity, and self-determination theory: a systematic review. Int J Behav Nutr Phys Act. (2012) 9:78. doi: 10.1186/1479-5868-9-78
147. George BG. Forfeit: opportunity, choice, and discrimination theory under title IX. Yale J Law Fem. (2010) 22:1. http://hdl.handle.net/20.500.13051/7022
148. Sax LJ. The Gender Gap in College: Maximizing the Potential of Women and Men. San Francisco: Jossey-Bass (2008).
149. Kavanagh T, Mertens DJ, Hamm LF, Beyene J, Kennedy J, Corey P, et al. Prediction of long-term prognosis in 12 169 men referred for cardiac rehabilitation. Circulation. (2002) 106(6):666–71. doi: 10.1161/01.CIR.0000024413.15949.ED
150. Laukkanen JA, Zaccardi F, Khan H, Kurl S, Jae SY, Rauramaa R. Long-term change in cardiorespiratory fitness and all-cause mortality: a population-based follow-up study. Mayo Clin Proc. (2016) 91(9):1183–8. doi: 10.1016/j.mayocp.2016.05.014
151. Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. (2009) 301(19):2024–35. doi: 10.1001/jama.2009.681
152. Davidson T, Vainshelboim B, Kokkinos P, Myers J, Ross R. Cardiorespiratory fitness versus physical activity as predictors of all-cause mortality in men. Am Heart J. (2018) 196:156–62. doi: 10.1016/j.ahj.2017.08.022
153. Silva AG, Simões P, Queirós A, Rocha NP, Rodrigues M. Effectiveness of mobile applications running on smartphones to promote physical activity: a systematic review with meta-analysis. Int J Environ Res Public Health. (2020) 17(7):2251. doi: 10.3390/ijerph17072251
Keywords: app, healthy sedentary people, heart rate variability, physical exercise, physical fitness, wearable technologies
Citation: Casanova-Lizón A, Manresa-Rocamora A, Sarabia JM, Pastor D, Javaloyes A, Peña-González I and Moya-Ramón M (2025) Impact of heart rate variability-based exercise prescription: self-guided by technology and trainer-guided exercise in sedentary adults. Front. Sports Act. Living 7:1578478. doi: 10.3389/fspor.2025.1578478
Received: 17 February 2025; Accepted: 5 May 2025;
Published: 22 May 2025.
Edited by:
Pietro Picerno, University of Sassari, ItalyReviewed by:
Islem Bejaoui, University of Messina, ItalySniegina Poteliuniene, Vytautas Magnus University, Lithuania
Copyright: © 2025 Casanova-Lizón, Manresa-Rocamora, Sarabia, Pastor, Javaloyes, Peña-González and Moya-Ramón. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manuel Moya-Ramón, bW1veWFAdW1oLmVz