 V. Schöffl
V. Schöffl X. Iruretagoiena
X. Iruretagoiena T. Nelson
T. Nelson Paulo Miro
Paulo Miro- 1Department of Orthopedic and Trauma Surgery, Klinikum Bamberg, Bamberg, Germany
- 2Department of Trauma Surgery, Friedrich Alexander University of Erlangen–Nuremberg, Erlangen, Germany
- 3Section of Wilderness Medicine, Department of Emergency Medicine, University of Colorado School of Medicine, Denver, CO, United States
- 4School of Clinical and Applied Sciences, Leeds Becket University, Leeds, United Kingdom
- 5Division of Exercise Physiology and Metabolism, Department of Sport Science, University of Bayreuth, Bayreuth, Germany
- 6Deusto Physical TherapIker, Physical Therapy Department, Faculty of Health Sciences, University of Deusto, San Sebastian, Spain
- 7Camp4 Human Performance, Salt Lake City, UT, United States
- 8Department of Radiology and Imaging Sciences, School of Medicine, The University of Utah, Salt Lake City, UT, United States
Introduction: Primary Periphyseal Stress Injuries (PPSI) of the hand and fingers are relatively uncommon but are most frequently seen in adolescent rock climbers. A major limitation in the current literature on PPSIs is the lack of a standardized nomenclature and radiological classification. This gap complicates the accurate diagnosis, treatment, and comparison of outcomes across studies.
Methods: We conducted a comprehensive structured literature review of the relevant PPSI literature in climbers using Pubmed, SPORTDiscus, and Web of Science to identify the relevant studies on PPSI in adolescent rock climbers. Based on the findings from existing research and our own data, we propose a new classification system for these injuries.
Results: A five-grade classification system, with subgroups, has been developed based on both clinical and radiographic data. The classification is presented in a table, along with figures illustrating examples of the various injury types.
Conclusion: Additional research is required to assess the reliability and reproducibility of this classification system. We plan to conduct these evaluations in future studies.
Introduction
Primary Periphyseal Stress Injuries (PPSI) of the hand and fingers are relatively rare but are most commonly observed in adolescent rock climbers (1–3). In fact, they are the most common sport-specific injury in young climbers (2, 4) These injuries are rarely the result of a single traumatic event; rather, they are considered chronic injuries (stress fractures) cause by the repetitive, often supra-physiologic stress applied to the fingers during climbing (5). Although PPSIs are by far most commonly associated with rock climbing, they have also been reported, albeit infrequently, in other athletes such as gymnasts, baseball players, and pianists (4).
Physeal stress injuries generally occur when the extremity is subjected to repetitive loading without adequate rest periods to allow for structural adaptation (6–8). Physeal stress injuries affecting the epiphyseal growth plate complex are referred as (1, 4, 8, 9) primary periphyseal stress injuries (6). A recent framework proposed by Caine et al. (6) provides a novel understanding of the pathophysiological mechanisms and outcomes of PPSIs. Diagnosing these injuries in climbers' fingers can be particularly challenging, as they are often not visible on radiographs (9, 10). Additionally, MRI diagnosis can be difficult because of the need for thin-slice, angulated imaging planes (9, 11). Diagnostic and therapeutic guidelines have recently been proposed to address these challenges (10).
One persistent issue highlighted in the literature on PPSIs, both in general and specifically among climbers, is the lack of standardized nomenclature and radiological classification (1, 6, 8, 9). In a recent publication, Caine et al. (6) noted significant inconsistencies and imprecision in the terminology used to describe these injuries. Existing classification systems, such as the Salter-Harris (12) and Aitkens (13) classifications, are widely recognized but lack specificity regarding the pathophysiology of PPSIs (8). The Salter-Harris classification, originally designed for classifying acute fractures involving the growth plate, has been applied to categorize metaphyseal stress injuries in young athletes (6), including climbers' fingers injuries (4, 8, 9). However, while the radiographic appearance of some of these injuries may resemble Salter–Harris type I fractures, the pathology and mechanism of these injuries differ substantially (6, 8). Early-stage stress fractures, which may not show a distinct fracture line on radiographs but exhibit edema on MRI are not represented in the existing classifications for acute fractures. Additionally, dorsal physeal widening seen in stress fractures (radiographic sign 1) is completely different from epiphysiolysis described in Salter-Harris 1. Moreover, the extent of sclerosis in PPSIs cannot be observed in acute fractures and cannot be classified using Salter-Harris or Aitkins. Given these limitations, there is a clear need for the development and validation of a more precise imaging-based classification system for PPSIs in general, as well as one specifically tailored to finger injuries in climbers. Such a system would improve diagnostic consistency and provide better guidance for treatment.
Methods
Our primary area of research and expertise focuses on climbing-related injuries, including their diagnosis and classification. To inform our study, we performed a structured literature review using Pubmed, SPORTDiscus, and Web of Science–with the final search on March 1st, 2025. This search was supplemented by manually reviewing the reference lists of selected articles to identify additional relevant studies. We employed a combination of MeSH terms and tailored search keywords, including “epiphyseal fractures”, “adolescent climbers”, “finger injuries”, and “youth climbers”.
We reviewed the extracted studies on PPSIs in climbers' fingers (1–5, 9–11, 14–38) and developed a new classification system. This system integrates clinical presentation (4, 5, 10, 16), biomechanics (5, 14), imaging findings (9, 11, 15), and elements from previously established frameworks such as Salter-Harris (12) and Aitkens (13). Additionally, the extent of sclerosis in the fracture line, as observed in CT scans, was considered, as this is a critical variable in the decision algorithm of Schöffl et al. (10) to determine whether surgical spot drilling should be recommended.
Results
A total of 50 important publications were gathered, and the injuries were analysed with a focus on their classification. Most of what is known about PPSIs among climbers arises from case reports and case series (8). Caine et al. (1) reported in 2021 that overall, there were 11 published case reports and series describing a total of 80 patients, including 65 males and 15 females, between ages 11 and 17, with PPSIs involving the hand and fingers (5, 11, 20–24, 39–43). With newer reports from Schöffl et al. (10), who reported an additional 37 digital PPSIs in 27 patients (19 male, 8 female), there are presently 107 (84 males, 23 females) published cases, making the fingers the most frequent anatomical site for published case reports of PPSIs.
Overall, physeal stress injuries occur when repetitive loading of the extremity is imposed without sufficient interval of rest to allow for structural adaptation (6–8). Physeal stress injuries involving the epiphyseal growth plate complex have been referred as primary periphyseal stress injuries (PPSIs) (1, 6). The most frequent digital PPSI reported were Salter-Harris type III involving the dorsal aspect of the middle phalanx, but Salter-Harris type I, II and V have also been reported (3, 5, 8, 11, 16–24, 39–41, 43, 44).
Conventional radiography serves as the primary imaging modality for assessing PPSIs of the fingers, due to its accessibility and cost-effectiveness (9). The most common radiographic manifestation of finger PPSIs is a Salter Harris type III fracture of the dorsal long finger middle phalanx (9, 10). It is recommended to obtain a minimum of two orthogonal views, typically anteroposterior (AP) and lateral views (9). Computed Tomography (CT) provides a more comprehensive assessment of the physis and adjacent osseous structures compared to radiographs (9). CT may reveal radiographically occult periphyseal sclerosis or osteopenia and premature physeal closure (9, 16). Magnetic Resonance Imaging (MRI) presents numerous clinically significant advantages over radiography and CT (4, 9). The most common presentation in MRI is a Salter Harris III fracture, characterized by physeal widening with a fracture through the physeal hyaline cartilage extending to the epiphysis, manifesting as increased T2 or short inversion time inversion-recovery (STIR) signal in these regions (9, 13). Also Salter Harris II and I injuries are reported in MRI (1, 4, 9, 10). Overuse injuries without associated fracture demonstrate similar widening of the physis, but without fracture of the hyaline cartilage, allowing differentiation from Salter-Harris I fractures (16).
In a recent publication Caine et al. (6) discussed inconsistencies and imprecision in the nomenclature used to describe primary periphyseal stress injuries. The use of the Salter-Harris (12) and Aitkens classifications (13, 45), in particular, seem not very specific to the pathophysiology. Initially intended for classifying direct or acute fractures involving the growth plate, the Salter-Harris classification has often been applied in an attempt to categorize metaphyseal stress injuries in young athletes (6, 24, 41, 42). However, while the radiographic appearance of these injuries may appear similar to Salter–Harris type I fractures, the nature and mechanism of the injury are actually quite different (8, 29). The authors conclude that given the short-comings of the Salter–Harris classification for describing these injuries, it follows that there is a need for the future development and testing of a more precise imaging-based classification to grade PPSIs that can be used to guide appropriate treatment (8, 29).
The first author has extensively studied the pathophysiology and therapy of these PPSI injuries and the Sportsmedical Center of the Klinikum Bamberg, Bamberg, Germany serves as an international refferal center for these injuries. Thus, based on the analysis of 50 relevant publications, along with our clinical and scientific experience with these fractures, we propose the following classification. The aim of this classification is to combine clinical symptoms with radiological presentations in conventional radiographs, CT scans or MRIs (Figures 1–3). It is important to differentiate between fractures with and without sclerosis on a CT scan, as the presence of sclerosis is an indication for surgery in the Schöffl et al. algorithm (10).

Figure 1. Radiographic sign 1. Dorsal widening of the dorsal middle phalangeal physis with irregularity, fragmentation, and periphyseal osteopenia (4, 8, 9). Physeal widening correlates with hypertrophied chondrocytes extending into the metaphysis, a consequence of disrupted metaphyseal vascular supply (46). Physeal irregularity and fragmentation result, in part, from damage and effacement of the zone of provisional calcification (47). (14 y old girl, right middle finger).
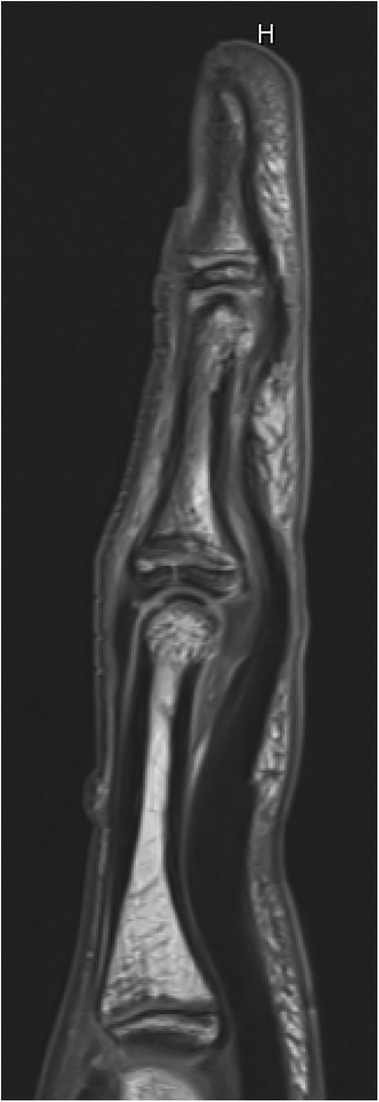
Figure 2. Radiographic sign 2. Non-displaced dorsal fracture of the epiphyseal-metaphyseal-complex (EPM) of the middle phalanx base (5, 9). (13 y old boy, left middle finger).

Figure 3. Radiographic sign 3. Displaced dorsal fracture of the epiphyseal-metaphyseal-complex (EPM) of the middle phalanx base (15 y old boy, right middle finger).
Proposed classification
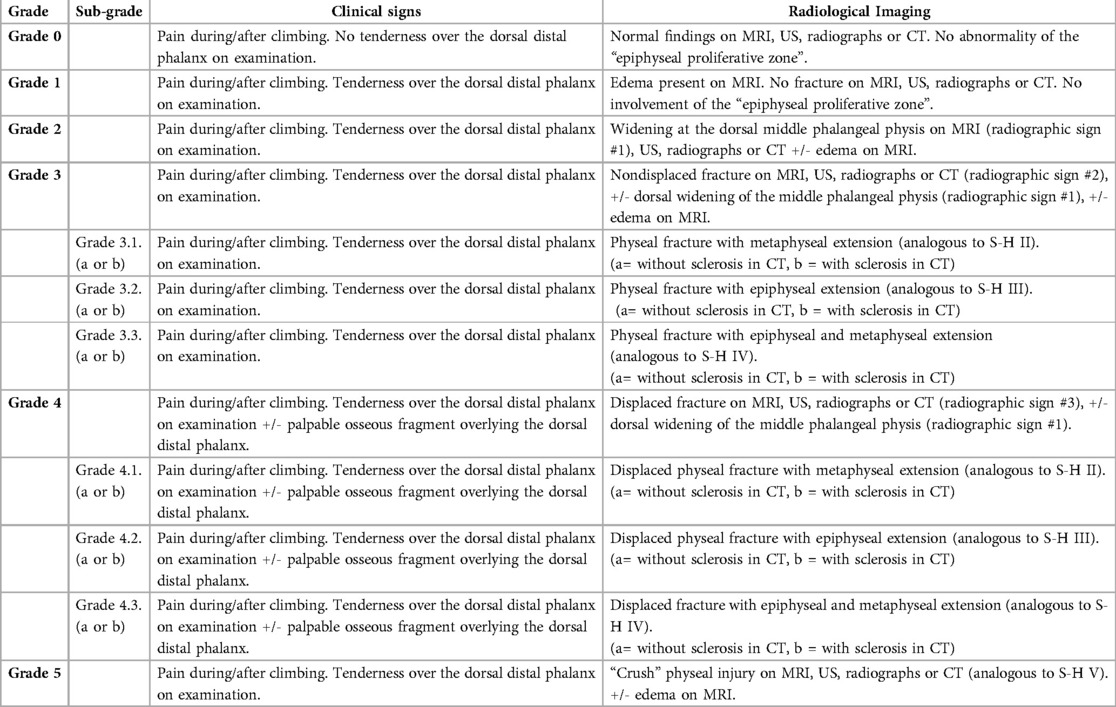
Clinical and radiological classification of primary periphyseal stress injuries in adolescent rock climbers
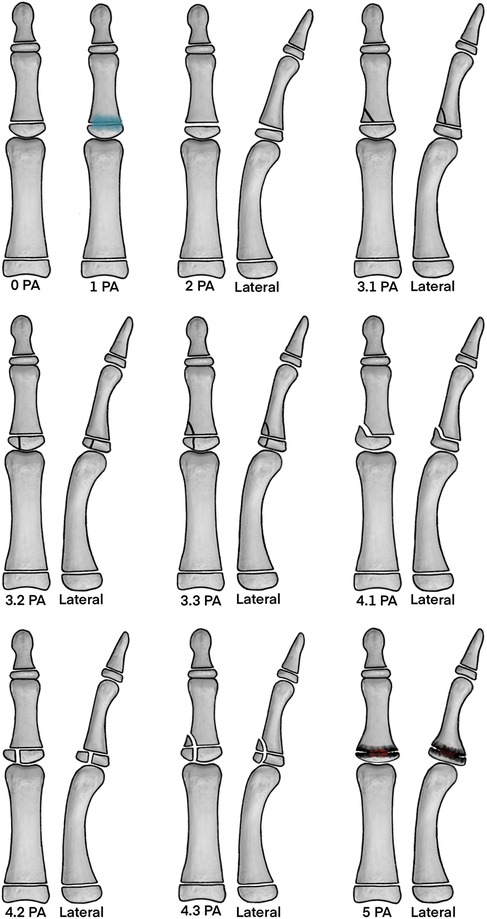
Figure 4. Proposed classification. The illustrations demonstrate the main findings in either x-ray, MRI or CT-scan of the proposed classification. Note that edema may also be present in all higher graded injuries and adjunct to these images the possible condition of sclerosis is defined with an “a” or “b” (a = without sclerosis in CT, b = with sclerosis in CT) (Figure by Nelson T, DC, MS, CSCS, Camp4 Human Performance).
Conclusion
The classification presented is to be considered a proposal pending further evaluation. It is based on scientific analysis, but also personal experience, thus a certain level of bias is possible. Nevertheless, we tried to minimize this by including a radiologist with extensive experience of these injuries, as well as another clinician, in the research team.
Further research is necessary to evaluate the reliability of this classification system and its inter-observer agreement, which we plan to address in future studies.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: xray analysis from former studies were included these studies are published. Requests to access these datasets should be directed todm9sa2VyLnNjaG9lZmZsQG1lLmNvbQ==.
Ethics statement
The studies involving humans were approved by Friedrich Alexander University Erlangen-Nuremberg. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
VS: Writing – review & editing, Writing – original draft. XI: Project administration, Validation, Methodology, Investigation, Writing – original draft, Conceptualization, Writing – review & editing, Supervision. TN: Writing – review & editing, Supervision, Validation, Visualization, Conceptualization. PM: Investigation, Software, Writing – review & editing, Writing – original draft, Methodology, Validation, Visualization, Supervision, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
Author TN was employed by Camp4 Human Performance.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Caine D, Meyers R, Nguyen J, Schöffl V, Maffulli N. Primary periphyseal stress injuries in young athletes: a systematic review. Sports Med. (2022) 52(4):741–72. doi: 10.1007/s40279-021-01511-z
2. Schöffl V, Schöffl I, Jones G, Klinder A, Küpper T, Gunselmann L, et al. Prospective analysis of injury demographics, distribution, severity and risk factors in adolescent climbers. BMJ Open Exerc Med. (2025) 11(1):e002212. doi: 10.1136/bmjsem-2024-002212
3. Jones G, Johnson R, Schöffl V, Schöffl I, Lutter C, Johnson MI, et al. Primary periphyseal stress injuries of the fingers in adolescent climbers: a critical review. Curr Sports Med Rep. (2022) 21(12):436–42. doi: 10.1249/JSR.0000000000001016
4. Schöffl V, Moser O, Küpper T. Stress fractures of the growth plates in the fingers of adolescent rock climbers. Unfallchirurgie (Heidelb). (2024) 127(11):824–31. doi: 10.1007/s00113-024-01482-6
5. Schöffl I, Schöffl V. Epiphyseal stress fractures in the fingers of adolescents: biomechanics, pathomechanism, and risk factors. Eur J Sports Med. (2015) 3(1):27–37.
6. Caine D, Maffulli N, Meyers RN, Schöffl V, Nguyen J. Inconsistencies and imprecision in the nomenclature used to describe primary periphyseal stress injuries: towards a better understanding. Sports Med. (2022) 52(4):685–707. doi: 10.1007/s40279-022-01648-5
7. DiFiori JP, Benjamin HJ, Brenner JS, Gregory A, Jayanthi N, Landry GL. Overuse injuries and burnout in youth sports: a position statement from the American medical society for sports medicine. Ckin j Sport Med. (2014) 24:3–20. doi: 10.1136/bjsports-2013-093299
8. Schöffl V, Iruretagoiena X. Physeal stress injuries of the hand and fingers. In: Caine D, Nguyen J, Grady M, editors. Physeal Stress Injuries Physeal Stress Injuries in Young Athletes: Diagnosis, Treatment and Prevention. Contemporary Pediatric and Adolescent Sports Medicine. Heidelberg, New York: Springer (2024). p. 119–40.
9. Miro P, Crawford A, Mills M, Schöffl V. Imaging of primary periphyseal finger stress injuries in climbers. Skeletal Radiol. (2024) 54:1215–24. doi: 10.1007/s00256-024-04832-y
10. Schöffl V, Schöffl I, Flohe S, El-Sheikh Y, Lutter C. Evaluation of a diagnostic-therapeutic algorithm for epiphyseal growth plate stress injuries in adolescent climbers. Am J Sports Med. (2021) 50(1):229–37. doi: 10.1177/03635465211056956
11. Bayer T, Schöffl VR, Lenhart M, Herold T. Epiphyseal stress fractures of finger phalanges in adolescent climbing athletes: a 3.0-tesla magnetic resonance imaging evaluation. Skeletal Radiol. (2013) 42(11):1521–5. doi: 10.1007/s00256-013-1694-4
12. Salter RB, Harris WR. Injuries involving the epiphyseal plate. J Bone Joint Surg Am. (1963) 45(3):587–622. doi: 10.2106/00004623-196345030-00019
13. Aitken AP. The end results of the fractured distal tibial epiphysis. J Bone Joint Surg Am. (1936) 18:685–91.
14. Bärtschi N, Scheibler AG, Schweizer A. Palmar shift of the proximal interphalangeal joint in different grip positions as a potential risk factor for periphyseal injuries in adolescent climbers. Wilderness Environ Med. (2023) 34(4):451–6. doi: 10.1016/j.wem.2023.06.008
15. Miro P, Miro E, Ho T, Feuerborn M, Crawford A, Schöffl V. Rock climbing-related injuries: a clinical and imaging overview. Cur Sports Med Rep. (2024) 23(11):381–91. doi: 10.1249/JSR.0000000000001209
16. Bärtschi N, Scheibler A, Schweizer A. Symptomatic epiphyseal sprains and stress fractures of the finger phalanges in adolescent sport climbers. Hand Surg Rehabil. (2019) 38(4):251–6. doi: 10.1016/j.hansur.2019.05.003
17. Meyers RN, Schöffl VR, Mei-Dan O, Provance AJ. Returning to climb after epiphyseal finger stress fracture. Curr Sports Med Rep. (2020) 19(11):457–62. doi: 10.1249/JSR.0000000000000770
18. Meyers RN, Howell DR, Provance AJ. The association of finger growth plate injury history and speed climbing in youth competition climbers. Wilderness Environ Med. (2020) 31(4):394–9. doi: 10.1016/j.wem.2020.06.008
19. Halsey T, Johnson M, Jones G. Epiphyseal stress fractures of the fingers in an adolescent climber: a potential “maslow’s hammer” in terms of clinical reasoning. Curr Sports Med Rep. (2019) 18:431–3. doi: 10.1249/JSR.0000000000000658
20. Schöffl V, Lutter C, Woollings K, Schöffl I. Pediatric and adolescent injury in rock climbing. Res Sports Med. (2018) 26(sup1):91–113. doi: 10.1080/15438627.2018.1438278
21. Desaldeleer AS, Le Nen D. Bilateral fracture of the base of the middle phalanx in a climber: literature review and a case report. Orthop Traumatol Surg Res. (2016) 102(3):409–11. doi: 10.1016/j.otsr.2016.01.016
22. Schöffl V, Popp D, Küpper T, Schöffl I. Injury trends in rock climbers: evaluation of a case series of 911 injuries between 2009 and 2012. Wilderness Environ Med. (2015) 26(1):62–7. doi: 10.1016/j.wem.2014.08.013
23. Schöffl VR, Schöffl I. Finger pain in rock climbers: reaching the right differential diagnosis and therapy. J Sports Med Phys Fitness. (2007) 47(1):70–8.
24. Hochholzer T, Schöffl VR. Epiphyseal fractures of the finger middle joints in young sport climbers. Wilderness Environ Med. (2005) 16(3):139–42. doi: 10.1580/PR15-04.1
25. Jones G, Johnson M. A critical review of the incidence and risk factors for finger injuries in rock climbing. Curr Sports Med Rep. (2016) 15(6):400–9. doi: 10.1249/JSR.0000000000000304
26. Jones G, Asghar A, Llewellyn DJ. The epidemiology of rock climbing injuries. Br J Sports Med. (2007) 42(9):773–8. doi: 10.1136/bjsm.2007.037978
27. Barille AM, Feng S-Y, Neasiama J-A, Huang C. Injury rates, patterns, mechanisms, and risk factors among competitive youth climbers in the United States. Wilderness Environ Med. (2022) 33(1):25–32. doi: 10.1016/j.wem.2021.09.005
28. Chen DL, Meyers RN, Provance AJ, Zynda AJ, Wagner KJ 3rd, Siegel SR, et al. Early sport specialization and past injury in competitive youth rock climbers. Wilderness Environ Med. (2022) 33(2):179–86. doi: 10.1016/j.wem.2022.03.002
29. Meyers RN, Hobbs SL, Howell DR, Provance AJ. Are adolescent climbers aware of the most common youth climbing injury and safe training practices? Int J Environ Res Public Health. (2020) 167:812–22. doi: 10.3390/ijerph17030812
30. Schöffl VR, Hoffmann PM, Imhoff A, Küpper T, Schöffl I, Hochholzer T, et al. Long-term radiographic adaptations to stress of high-level and recreational rock climbing in former adolescent athletes: an 11-year prospective longitudinal study. Orthop J Sports Med. (2018) 6(9):2325967118792847. doi: 10.1177/2325967118792847
31. Siegel SR, Fryer SM. Rock climbing for promoting physical activity in youth. Am J Lifestyle Med. (2017) 11(3):243–51. doi: 10.1177/1559827615592345
32. Watts PB, Joubert LM, Lish AK, Mast JD, Wilkins B. Anthropometry of young competitive sport rock climbers. Br J Sports Med. (2003) 37(5):420–4. doi: 10.1136/bjsm.37.5.420
33. Miro P, Schöffl VR. Prevention of primary periphyseal stress injuries in skeletally immature climbers. Br J Sports Med. (2024) 58(15):883–4. doi: 10.1136/bjsports-2023-107774
34. Rugg C, Tiefenthaler L, Rauch S, Gatterer H, Paal P, Strohle M. Rock climbing emergencies in the Austrian Alps: injury patterns, risk analysis and preventive measures. Int J Environ Res Public Health. (2020) 17(20):7596. doi: 10.3390/ijerph17207596
35. Ting JWC, Jacomel T, Lindau TR, O’estrich KL. “Osgood schlatter of the finger”—a case report of apophysitis of the proximal inter-phalangeal joint of the finger and review of injuries in adolescent climbers. Actta Sci Orthop. (2020) 3(1):137–42.
36. Garcia K, Jaramillo D, Rubesova E. Ultrasound evaluation of stress injuries and physiological adaptations in the fingers of adolescent competitive rock climbers. Pediatr Radiol. (2017) 48(3):366–73. doi: 10.1007/s00247-017-4033-4
37. Woollings KY, McKay CD, Kang J, Meeuwisse WH, Emery CA. Incidence, mechanism and risk factors for injury in youth rock climbers. Br J Sports Med. (2015) 49(1):44–50. doi: 10.1136/bjsports-2014-094067
38. Schlegel C, Buechler U, Kriemler S. Finger injuries of young elite rock climbers. Schweiz Z Sportmed Sporttraumatol. (2012) 50(1):7–10.
39. Schöffl I, Schöffl V. Pediatric aspects in young rock climbers. In: Schöffl V, Schöffl I, Lutter C, Hochholzer T, editors. Climbing Medicine: A Practical Guide. Cham: Springer International Publishing (2022). p. 201–6.
40. El-Sheikh Y, Lutter C, Schöffl I, Schöffl V, Flohe S. Surgical management of proximal interphalangeal joint repetitive stress epiphyseal fracture nonunion in elite sport climbers. J Hand Surg (Am). (2018) 43(6):572.e1–.e5. doi: 10.1016/j.jhsa.2017.10.009
41. Hochholzer T, Schöffl V, Bischof B. [Epiphyseal fractures of the middle phalanx in sportclimbers] epiphysenfrakturen der fingermittelgelenke bei sportkletterern. Sport Ortho Trauma. (2002) 18:87–92.
42. Hochholzer T, Schöffl V, Krause R. Finger-Epiphysenverletzungen jugendlicher sportkletterer. Sport Ortho Trauma. (1997) 13(2):100–3.
43. Morrison AB, Schöffl VR. Physiological responses to rock climbing in young climbers. Br J Sports Med. (2007) 45(3):657–79. doi: 10.1136/bjsm.2007.034827
44. Schöffl V, Simon M, Lutter C. Finger and shoulder injuries in rock climbing. Orthopade. (2019) 48(12):1005–12. doi: 10.1007/s00132-019-03825-3
45. Aitken AP. Fractures of the epiphyses. Clin Orthop Relat Res. (1965) 41:19–23. doi: 10.1097/00003086-196500410-00002
46. Laor T, Wall EJ, Vu LP. Physeal widening in the knee due to stress injury in child athletes. Am J Roentgenol. (2006) 186:1260–64. doi: 10.2214/AJR.04.1606
Keywords: rock climbing, epiphyseal fractures, finger injury, fracture classification, periphyseal fractures
Citation: Schöffl V, Iruretagoiena X, Nelson T and Miro P (2025) Proposal of a specific classification of primary periphyseal stress injuries in adolescent rock climbers. Front. Sports Act. Living 7:1596624. doi: 10.3389/fspor.2025.1596624
Received: 19 March 2025; Accepted: 14 July 2025;
Published: 14 August 2025.
Edited by:
Michael Cassel, University of Potsdam, GermanyReviewed by:
Phil Newman, University of Canberra, AustraliaJames Walker, Sheffield Climbing Clinic, United Kingdom
Copyright: © 2025 Schöffl, Iruretagoiena, Nelson and Miro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: V. Schöffl, dm9sa2VyLnNjaG9lZmZsQG1lLmNvbQ==