 Salma Verenice Cristerna-Huerta1
Salma Verenice Cristerna-Huerta1 Melissa Vega-Burgueño1
Melissa Vega-Burgueño1 Marcela de Jesús Vergara-Jiménez1
Marcela de Jesús Vergara-Jiménez1 Erika Martínez-López2
Erika Martínez-López2 Elisa Barrón-Cabrera1*
Elisa Barrón-Cabrera1*
- 1Facultad de Ciencias de la Nutrición y Gastronomía, Universidad Autónoma de Sinaloa, Culiacán, México
- 2Instituto de Nutrigenética y Nutrigenómica Traslacional, Departamento de Biología Molecular y Genómica, Centro Universitario en Ciencias de la Salud, Universidad de Guadalajara, Guadalajara, México
Background: The NLRP3 inflammasome is a molecular structure involved in inflammation and innate immune response, its overexpression has been associated with the development of several diseases. Physical exercise plays an important role in regulating systemic inflammation, however different types of exercise seem to have a different effect in the regulation of the NLRP3 inflammasome.
Objective: To provide updated information related to the effect of different types and training durations of exercise on NLRP3 inflammasome complex, IL-1β—IL-18 cytokines quantification in adults with different metabolic conditions.
Methods: The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology for manuscript research and preparation was followed using PubMed, Science Direct, SpringerLink, Scopus and Google Scholar databases for literature review. Out of 1,514 articles identified, only 11 articles fulfilled the inclusion criteria.
Results: Moderate-intensity aerobic exercise and moderate resistance exercise seems to significantly decreased concentrations of the cytokine IL-1β, NLRP3 protein and caspase-1, as well as ASC and NLRP3 gene expression. High-intensity aerobic exercise exerted the opposite effects by increasing NLRP3 gene expression and the cytokines IL-1β and IL-18.
Conclusion: Resistance, aerobic and combined exercise (≥8 weeks) were linked to downregulated key NLRP3 inflammasome components across diverse populations. These results support exercise as a safe and effective strategy to modulate NLRP3-driven inflammation. Notably, evidence suggest that resistance and combined modalities showed superior efficacy in reducing both gene and cytokine levels. This positions structured exercise as a valuable tool in managing chronic low-grade inflammation.
Introduction
NLRP3 inflammasome formation is initiated by the nucleotide oligomerization domain (NOD)-like receptors (NLR), which are key in the regulation of the innate immune system and the recognition of diverse intracellular pathogens such as the damage-associated molecular patterns (DAMPs), pathogen-associated molecular patterns (PAMPs), danger signals, caspase-1 activity, and the secretion of IL-18 and IL-1β cytokines (1).
The NLRs are classified according to the protein binding domains located in their amino-terminal region: (1) NOD composed of 6 members, (2) IPAF or NLRC consisting of 2 members, and (3) Nucleotide-binding oligomerization domain, Leucine rich Repeat and Pyrin domain Containing (NLRP), for which currently 14 members are recognized. The NRLPs are associated with the formation of inflammasomes, which are molecular complexes that serve as sensors and mediators of systemic inflammation (2).
There are diverse isoforms of NLRP, including NLRP1 to NLRP14. However, NLRP3, also known as cryopyrin, is the most studied and characterized cause their close relationship with chronic diseases (3). NLRP3 inflammasome has three components: (1) The NLRP3 protein which contains a central nucleotide-binding oligomerization, (2) an ASC adaptor protein and (3) the procaspase-1 (4).
The activation of the NLRP3 inflammasome requires two independent signals (5). The first signal is considered priming and promotes the transcription of NLRP3, pro-IL-1β, and pro-IL-18 proteins form. The second signal is activation and this results in the oligomerization and assembly of the NLRP3 inflammasome, promoting the cleavage of caspase-1, which, in turn, cleaves pro-IL-1β and pro-IL-18 cytokines into their mature forms.
The activation of NLRP3 inflammasome-dependent caspase-1 is also implicated in a form of inflammatory cell death known as pyroptosis (1). Pyroptosis is characterized by cellular inflammation, plasma membrane rupture due to water influx, and the release of proinflammatory cellular contents (6).
NLRP3 inflammasome serves as the central axis of innate immunity, regulating the secretion of proinflammatory cytokines and playing an indispensable role in modulating inflammatory responses (7). Inflammation stands as a key characteristic influencing the development and progression of numerous diseases (8). The NLRP3 inflammasome can act both as a sensor and contributor in the pathogenesis of obesity (9), certain types of cancer, metabolic diseases such as diabetes (10), atherosclerosis, cardiovascular diseases (11), and neurodegenerative diseases (12). Unlike other inflammasomes, NLRP3 inflammasome response to numerous stimuli, including environmental factors like diet and physical exercise (13).
On the other hand, the majority of individuals affected by chronic diseases and conditions related to uncontrolled inflammasome activation share similar lifestyle behaviors, such as being overweight or obese, unhealthy dietary habits, and physical inactivity (14). These behaviors are major contributors to diseases causing significant mortality worldwide. Physical inactivity alone contributes to 9% of global deaths (15), despite the well-known benefits of exercise in disease related to inflammatory pathways (16).
A study conducted by Abd El-Kader & Al-Ahreef demonstrated that exercise has an anti-inflammatory effect by reducing proinflammatory markers such as TNF-α, IL-6, and CRP, accompanied by an increase in IL-10 in blood samples from older adults (17). Furthermore, scientific evidence suggests that exercise may regulate inflammation through the NLRP3 inflammasome (18). However, the optimal intensity, frequency, and duration of training to achieve the best benefits in inflammation indicators associated with the NLRP3 inflammasome are still unknown.
Therefore, the aim of this systematic review is to provide updated information related to the effect of different types and training durations of exercise on the NLRP3 inflammasome complex, quantification of cytokines IL-1β—IL-18 in adults with different metabolic conditions to provide specific recommendations on which type of exercise contributes to a significant reduction in NLRP3 inflammasome levels.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines, as per its latest update (19).
Search strategy
PubMed, Science Direct, SpringerLink, Scopus and Google Scholar were employed for a systematic literature search that were published between January 1st, 2020 to January 31th, 2025. For the Google Scholar database, Publish or Perish software was used to optimize the search. The search was restricted to studies published in English. The following search filters were used: clinical trial, human species, adults aged 18 years or older. The search terms used, either individually or in combination, were selected based on PubMed MeSH terms: “physical exercise”, “exercise training”, “inflammasome”, “NLRP3 inflammasome”, “adults”, “metabolic diseases”, “NLRP3”, “ASC”, “caspase-1”, “pro-caspase-1”, “IL-1β”, and “IL-18”. A manual search of the reference lists of selected original articles was conducted to identify additional studies.
Inclusion and exclusion criteria
Inclusion criteria: Randomized clinical trials, case-control studies, published in the last 5 years, written in English, include data on the physical exercise program (duration, intensity, frequency), quantitatively assess at least one of the NLRP3 inflammasome-associated components (NLRP3, ASC, CASPASE-1, IL-1β and IL-18).
Exclusion criteria: reviews, studies based on animal models or in vitro cellular models, studies without exercise intervention (this refers to unstructured exercise with weekly sessions, defined intensity, and a duration of at least 4 weeks), studies without a structured physical exercise program, single-session interventions, marathons, competitions, races, incomplete data on the variables of interest and studies with a population sample under 18 years of age.
Data are shown following the population, intervention, comparison, outcome, and study design (PICOS) approach:
• Population: Adults aged ≥18 years old, without restrictions on gender or health conditions.
• Intervention: Various types of exercise, including isometric grip, resistance exercise, aerobic exercise, combined aerobic and resistance exercise, with a a frequency of at least two sessions per week, with a minimum duration of 20 min per session, exercise intensity between 30% and 100% of maximum heart rate, minimum duration of 4 weeks of intervention.
• Comparison: Control group without exercise compared to an exercise group, under the same habitual conditions.
• Outcome: Indicators related to the gene expression and protein concentrations of the NLRP3 inflammasome, including concentrations of NLRP3, ASC, pro-caspase-1, caspase-1, IL-18, and IL-1β, measured in peripheral blood (plasma, serum, or peripheral blood mononuclear cells).
• Study Design: Randomized controlled trials (RCTs), cohort and case-control studies published in English language.
Titles and abstracts of identified articles were independently reviewed. Following preliminary screening, full-text articles were examined according to the selection criteria. For this systematic review, studies were grouped according to the type of exercise performed: aerobic exercise, resistance exercise, and combination of aerobic and resistance exercise, as well as training duration exercise (≤12 weeks or ≥13 weeks).
Data extraction
The following characteristics of the selected studies were extracted: Author, publication year, country where the study was conducted, health status, age, population characteristics, biological sample, pharmacological and/or dietary treatment, and exercise intervention details (type, method, intensity, frequency, duration). Means and standard deviations of indicators associated with inflammasome activation (NLRP3, ASC, caspase-1, IL-1β, IL-18) were also extracted.
Risk of bias assessment
The methodological quality of the selected studies was assessed using the “Cochrane Tool for Risk of Bias” (20). This tool evaluates seven aspects of potencial bias: (1) random sequence generation (selection bias); (2) allocation concealment (selection bias); (3) blinding of participants and personnel (performance bias); (4) blinding of outcome assessment (detection bias); (5) incomplete outcome data (attrition bias); (6) selective reporting (reporting bias); (7) other potencial sources biases.
Each aspect was rated as “low risk”, “high risk”, or “unclear risk” of bias, according to the criteria described in the Cochrane tool. For scoring purposes, only domains rated as “low risk” were assigned one point; aspects rated as “high” or “unclear” received zero points. Thus, the maximum possible score per study was 7. Based on the total score, each study could be classified as high quality (5–7 points), moderate quality (3–4 points), or low quality (0–2 points) (20).
To ensure consistency, the risk of bias was independently evaluated by two reviewers. Discrepancies between reviewers were resolved through discussion and consensus; if agreement could not be reached, a third reviewer was consulted to make the final decision.
Results
Study selection
A total of 1,514 studies were identified by searching PubMed, Science Direct, SpringerLink, Scopus and Google Scholar databases. 32 duplicate articles were removed. After reviewing titles and abstracts, 71 articles were excluded, leaving 165 articles for full-text screening, A study was added from the references list of an article. Finally, 155 articles were excluded because they were systematic reviews or meta-analyses, cell lines or murine, did not comply as structured exercise, did not have physical activity or did not describe the details of the physical activity program. A total of 11 studies were included for this systematic review (21–31). These results are described qualitatively. The flowchart of the selection process is shown in Figure 1.
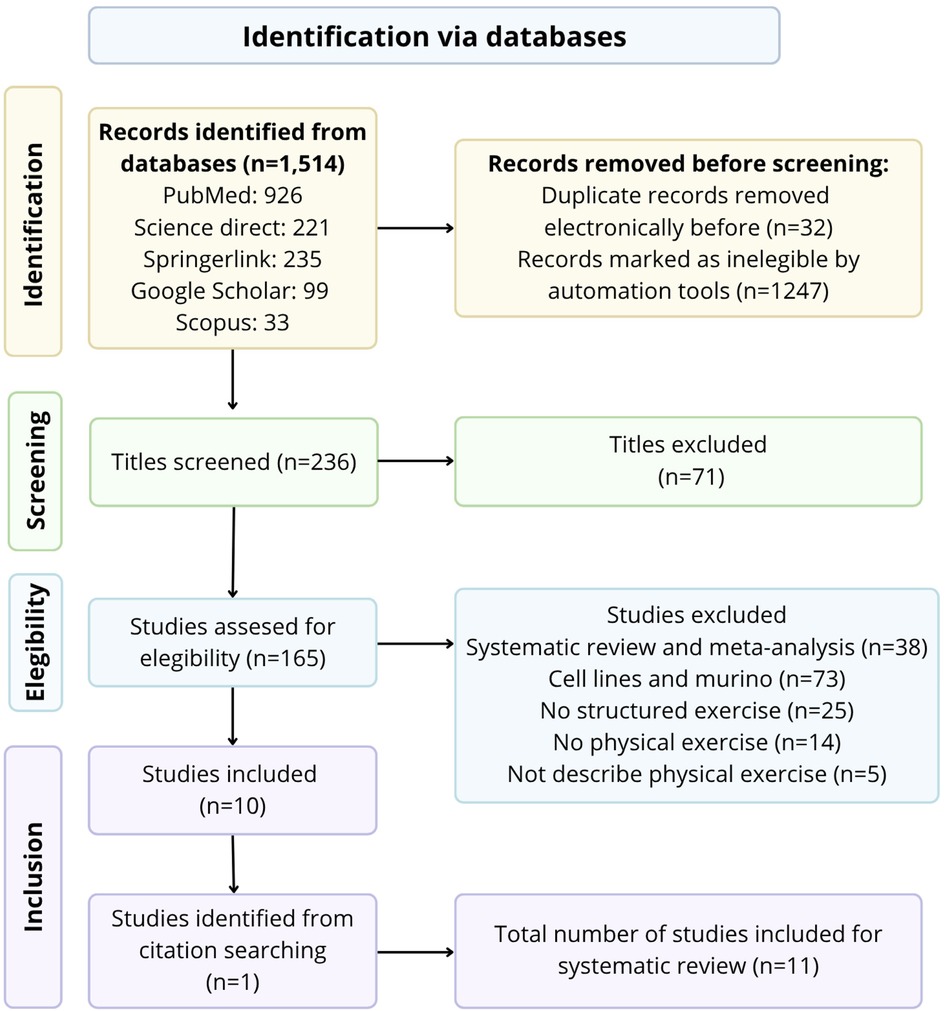
Figure 1. PRISMA flowchart for systematic reviews.
Study characteristics
We included 11 clinical trials conducted in various countries, including Mexico, Brazil, Canada, Italy Iran, Spain, and China. Among these studies, 5 analyzed NLRP3 levels (21, 25, 26, 30, 31), 1 analyzed ASC levels (22), 1 analyzed Caspase-1 levels (31), 9 analyzed IL-1β levels (22–24, 26–31) and 2 studies analyzed IL-18 levels (24, 26). The results were derived from 593 participants (200 in the control group and 393 in the exercise group). Age ranged between 23 and 78 years old. Participants in 2 of the studies were healthy, while participants in the remaining studies reported comorbidities such as type 2 diabetes, overweight or obesity, prediabetes, hypertension, coronary artery disease and among others. Out of the 11 studies, 4 had two groups, 2 studies had three groups, 2 studies had four groups, 1 study had four groups and 2 studies had six groups. Table 1 provides a summary of the study characteristics.
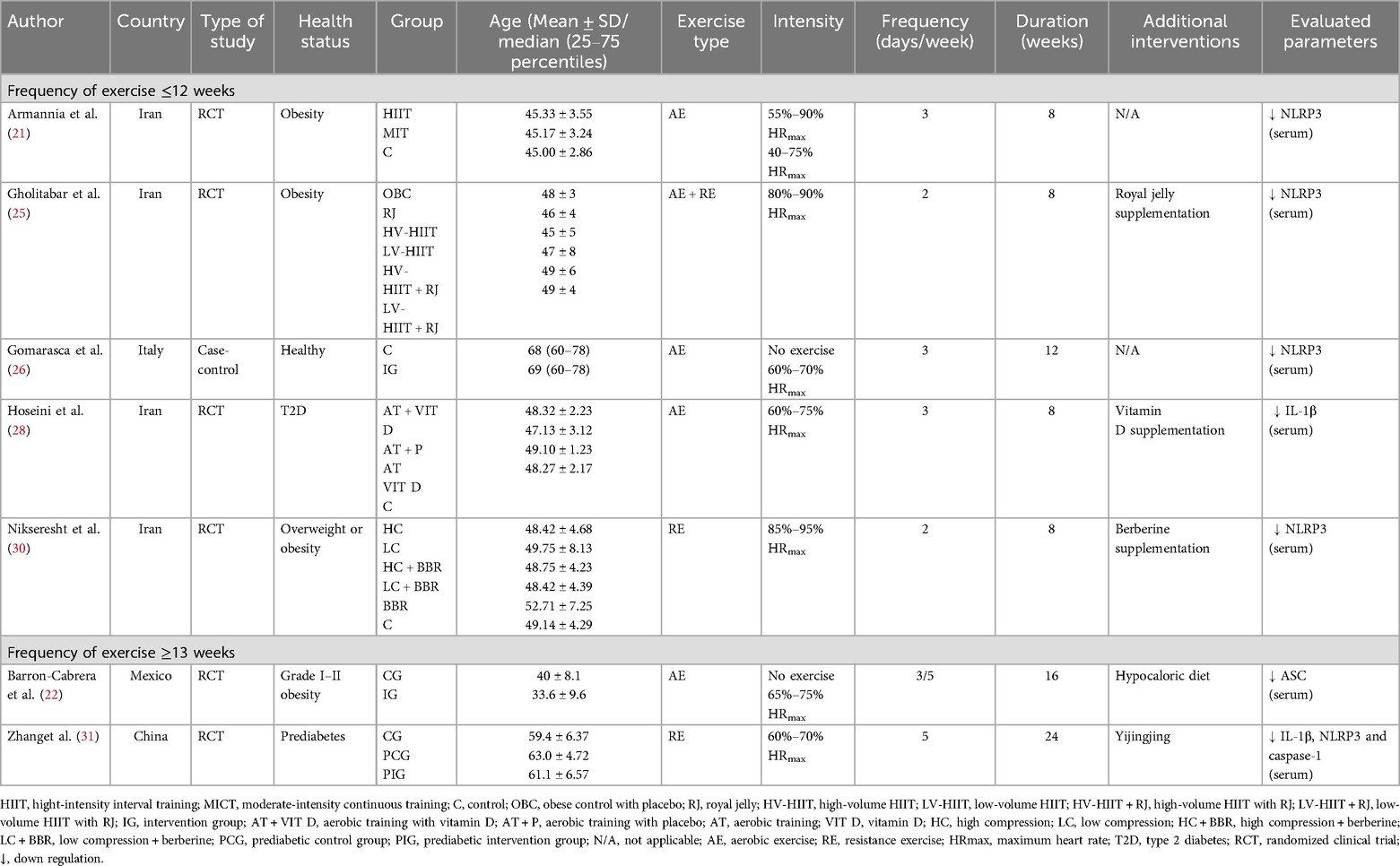
Table 1. The effects of different types of exercise on the expression of genes involved in the NLRP3 inflammasome in adults with some metabolic conditions.
The detailed characteristics of training for each study are presented in Tables 1, 2. The exercise intervention mainly included three types: aerobic exercise (AE), resistance exercise (RE), combined aerobic and resistance exercise (AE + RE), and isometric grip strength. Aerobic exercise included activities like walking, jogging, standard Nordic walking, cycling and, in some cases, treadmill and/or cycle ergometer use. Resistance exercise aimed to increase muscle strength through exercises such as transverse plane pushing, frontal plane pulling, squat jump, abdominal crunches, leg press, bicep curls, pectoral deck, jumping jack, sometimes using dumbbells and/or resistance bands. Isometric grip exercise involved isometric contractions using a handgrip dynamometer. The training frequency ranged from 2 to 5 sessions per week with durations ranging from 8 to 24 weeks. In all control groups, no exercise intervention was applied, and participants were instructed to continue their daily routines. In 6 out of 11 studies, participants received pharmacological, supplementation or dietary interventions to manage specific diseases.
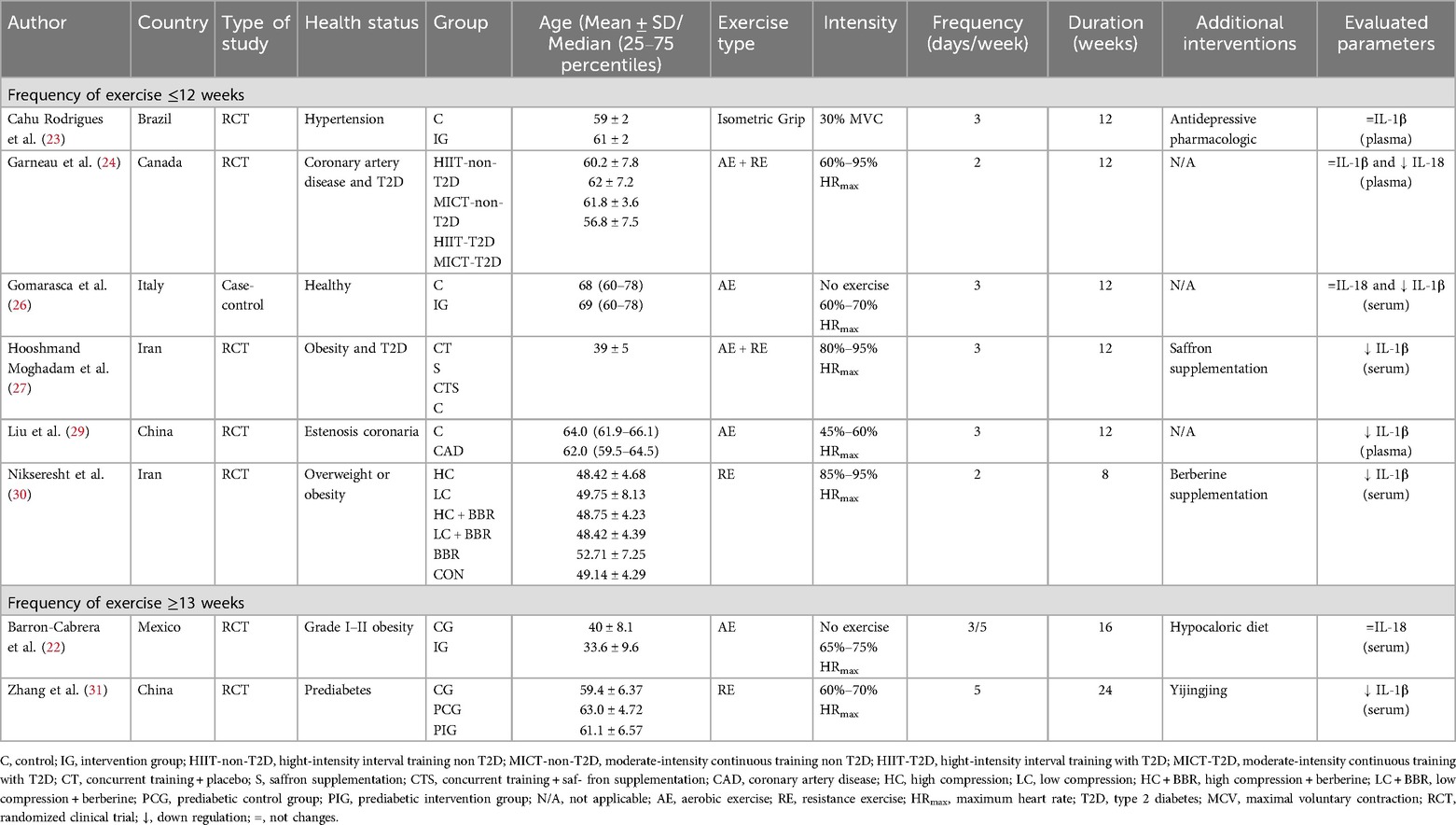
Table 2. The effects of different types of exercise on cytokines involved in the NLRP3 inflammasome in adults with some metabolic conditions.
Risk of bias of selected studies
The “Cochrane Tool for Risk of Bias” (20) was employed to assess the quality of the included studies (Figure 2). Two studies did not clearly describe how the random sequence was generated. Ten studies showed a high risk of bias in participant and personnel blinding due to the nature of the exercise intervention. Nine studies did not mention details of outcome assessment blinding, while two studies had incomplete outcome data. No study had a high risk of other bias or selective reporting. According to the Cochrane tool, two studies were of medium quality (score of 3–4), and nine studies were of high quality (score of 5–7).
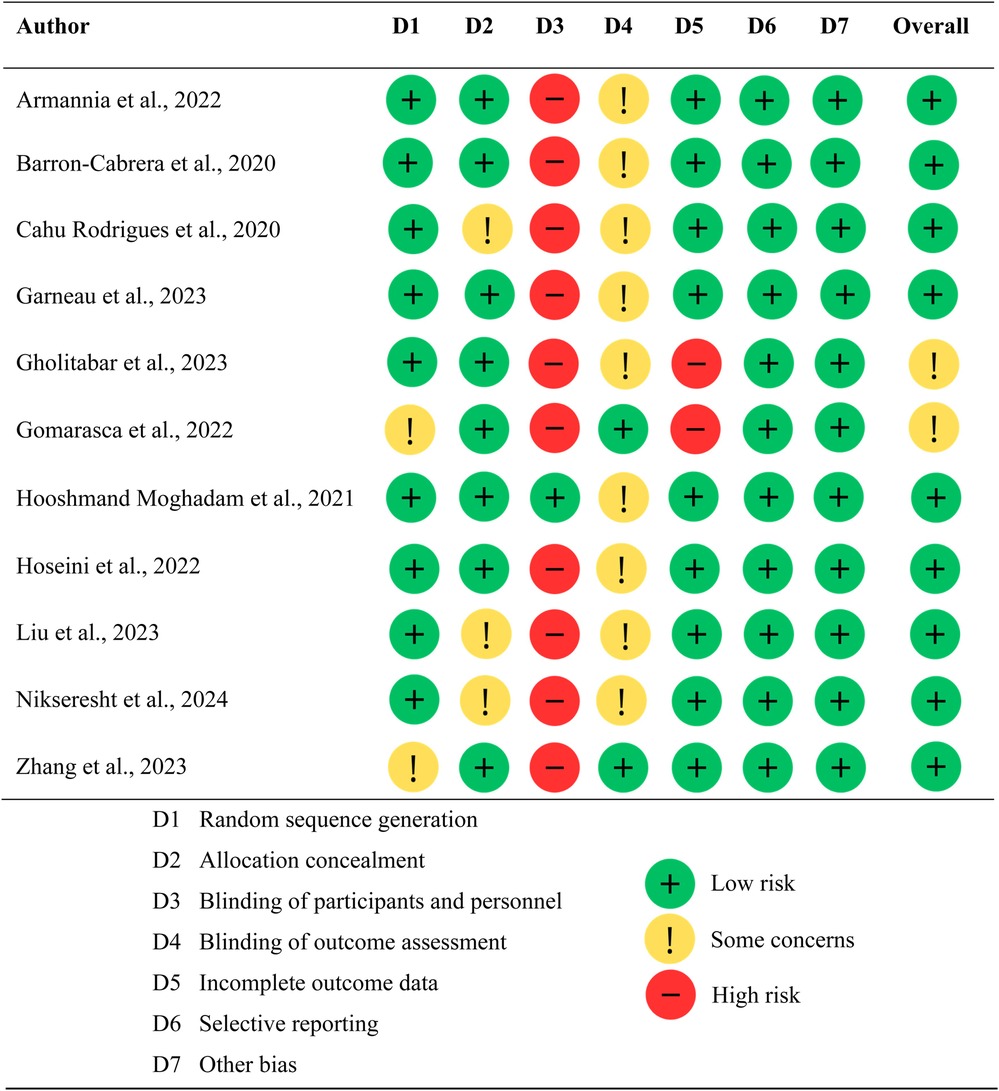
Figure 2. Quality assessment of studies using the cochrane risk of bias tool.
Effects of physical exercise on NLRP3 inflammasome
Aerobic exercise
Frequency ≤12 weeks
Four studies assessed the effect of aerobic exercise on at least one key molecule related to the NLRP3 inflammasome. In a study conducted in elderly women, assessing the impact of moderate aerobic exercise through Nordic walking over a 12-week period on the main components of the inflammasome in blood sample. A total of 58 elderly women were randomly assigned an experimental group, which participated in a Nordic walking training program, and a control group, which did not undergo any additional activity and was instructed to maintain their usual lifestyle habits. Additionally, subgroups were created based on participants' body mass index (BMI), classifying them as normal weight and overweight/obese. The training program implemented by the experimental group consisted of three sessions per week, each lasting 60 min, comprising a 10-min warm-up, 40 min of Nordic walking, and a 10-min cool-down. Standard Nordic walking poles were used during the sessions, and the activity was supervised by a team of assistants and trainers. Nordic walking was performed at an intensity of 60%–70% of maximum heart rate. Blood samples were collected from the antecubital vein in the experimental group at different time points: baseline, before (T1-pre) and after (T2-post) the first Nordic walking session, just before the last exercise session, after 12 weeks of training (T2-pre), and immediately after the last training session (T2-post). For the control group, blood samples were collected at the beginning and end of the study. Total RNA was extracted from these blood samples and subjected to reverse transcription for subsequent real-time PCR of the NLRP3 gene, using the 2-ΔΔCq relative quantification method. Furthermore, concentrations of cytokines IL-18 and IL-1β were quantified in the blood serum. The experimental group showed a significant decrease in NLRP3 gene expression at T2-pre compared to T1-pre. When comparing subgroups of normal weight and overweight/obesity within the experimental group, no significant differences were observed. However, the normal weight subgroup exhibited a significant increase in NLRP3 gene expression (T1-pre vs. T1-post). Nevertheless, subsequently at 12 weeks and before starting the training session, a significant decrease in NLRP3 expression (T1-pre vs. T2-pre) was observed in this same group. IL-18 concentrations remained unchanged in the experimental group, with no significant differences between the experimental and control groups or between normal weight and overweight/obesity subgroups. On the other hand, IL-1β cytokine experienced a decrease at the beginning of training (T1-pre vs. T1-post), increased after the first exercise period, decreased after 12 weeks of training, and increased again in the last exercise session. The main findings indicate that participation in a Nordic walking training program is associated with a reduction in inflammasome expression at rest, as well as the acquisition of a post-exercise proinflammatory response after completing the Nordic walking program. When categorizing participants based on their body mass index, it is observed that the NLRP3 gene response is more pronounced in individuals with normal weight compared to those with obesity (26).
A study conducted in adults with obesity aimed to assess the effects of two aerobic training strategies: high-intensity interval training (HIIT) and moderate-intensity continuous training (MICT). Participants were randomly assigned to one of three groups: HIIT, MICT, or a control group. The exercise groups underwent training three times per week for a period of 8 weeks. The HIIT protocol was performed at an intensity ranging from 55% to 90% of maximum heart rate (HRmax), while the MICT protocol ranged from 40% to 75% of HRmax. Each session lasted a total of 35 min and included a 5-min warm-up and a 5-min cool-down. Gene expression analysis of NLRP3 revealed a significant downregulation in both exercise groups compared to the control group (21).
A randomized study was conducted to evaluate the combined effects of vitamin D supplementation and aerobic exercise in individuals with obesity. Participants were allocated into four groups: aerobic training plus vitamin D (AT + Vit D), aerobic training plus placebo (AT + placebo), vitamin D alone (Vit D), and control with placebo (C). The AT + Vit D and Vit D groups received a weekly dose of 50,000 IU of vitamin D, while the AT and control groups were administered a placebo identical in color, taste, and form. The aerobic exercise protocol, assigned to the AT + Vit D and AT + placebo groups, was home-based and performed three times per week over 8 weeks. Each session began with 10 min of warm-up and ended with 10 min of cool-down. The main exercise component started at 20 min per session at 60% of maximum heart rate and progressively increased to 40 min at 75% of maximum heart rate. Gene expression of IL-1β was assessed as the primary outcome. The findings indicated that eight weeks of aerobic exercise combined with vitamin D supplementation significantly downregulated IL-1β gene expression compared to the control group (28).
A study investigated the role of meteorin-like protein (Metrnl) in mitigating vascular inflammation in CAD patients post-exercise. CAD patients who underwent a 12-week moderate-intensity continuous training (MICT) regimen exhibited decreased inflammatory cytokine expression, particularly IL-1β. In fact, plasma Metrnl levels, were inversely associated with, IL-1β and CAD severity. These decreased cytokine levels were most likely due to NLRP3 inflammasome down-regulation (29).
Frequency ≥13 weeks
In a study of adults with obesity grade I and II were randomized into two groups. The first group underwent a nutritional program, consisting of a hypocaloric diet with a 20% reduction in total energy expenditure, calculated using the Mifflin St. Jeor formula adjusted to current weight, and a macronutrient distribution of 50% carbohydrates, 30% fats, and 20% proteins. The second group combined the hypocaloric diet with progressive moderate-intensity aerobic exercise. The main exercises focused on improving aerobic capacity through walking and jogging, functional exercise circuits, and short sprints to enhance speed. Dumbbells weighing less than 5 kg were also incorporated to promote endurance. Analysis of ASC gene mRNA expression from leukocytes in peripheral blood was performed using the relative quantification method 2-ΔΔcq. At baseline, no significant differences were found between the two study groups. At the final time point, a significant decrease in ASC gene mRNA expression was observed in the group combining diet and exercise compared to the group that only underwent dietary intervention. Additionally, a significant decrease in ASC gene mRNA expression was found from baseline to final time in the group that performed both diet and exercise compared to the group that only implemented the hypocaloric diet. IL-18 and IL-1β cytokines were quantified in serum; however, no significant differences were observed in their levels over time in this study (22).
Current evidence suggests that regular aerobic exercise (three times per week), performed at an intensity ranging from 40% to 90% of maximum heart rate, can exert significant anti-inflammatory effects. These effects are mediated by the downregulation of key genes associated with the NLRP3 inflammasome, particularly ASC, NLRP3, and IL-1β. However, these transcriptional changes are not reflected in the circulating levels of the cytokines IL-18 and IL-1β. These findings indicate that such a physical intervention constitutes an effective strategy for mitigating low-grade chronic inflammation commonly associated with metabolic diseases such as obesity and type 2 diabetes through the downregulation of the NLRP3 inflammasome. Notably, similar effects have also been observed in metabolically healthy individuals.
Resistance exercise
Frequency ≤12 weeks
Two studies evaluated the effects of resistance exercise on the NLRP3, IL-1β and caspase-1 genes, and the cytokine IL-1β. In a study conducted on elderly individuals with prediabetes, the impacts of combined Yijinjing and resistance training were investigated to determine whether a direct correlation between the NLRP3 inflammasome and symptoms associated to insulin resistance and liver damage exist. A randomized clinical trial was performed, where participants were randomly assigned to one of three following groups: a healthy control group, a prediabetes control group, and a prediabetes exercise group. The prediabetes exercise group participated in combined Yijinjing and resistance training sessions for 6 months with 5 sessions per week. The resistance part of the training involved exercises with elastic bands for 8 min, with an intensity ranging between 60% and 70% of the maximum heart rate. Each session comprised 5 min of warm-up, Yijinjing training, elastic band training, and 5 min of cooling down, with a total duration of 47–76 min per session. Concentrations of the cytokine IL-1β in serum were determined using ELISA kits. To assess NLRP3 inflammasome activity, protein expressions of the inflammasome signaling cascade, including NLRP3, IL-1β, and caspase-1, were detected in peripheral blood mononuclear cells by western blot analysis. A significant overactivation of the inflammasome was observed in the prediabetes control group compared to healthy control subjects, as indicated by the results obtained through NLRP3, caspase-1, and IL-1β protein concentrations. The serum IL-1β concentration was higher in the prediabetes control group than in control subjects. On the other hand, the gene expression of NLRP3, CASPASE-1, and IL-1β, as well as the serum IL-1β concentration, decreased significantly in the prediabetes exercise group after 6 months of combined Yijinjing and resistance training (31).
Frequency ≥13 weeks
In another study conducted in middle-aged overweight or obese men with prediabetes, they evaluated the effect of a low-volume HIIT training program with different levels of compression, with or without berberine supplementation, on the upregulation of NLRP3 and IL-1β non-coding RNA. Study participants were assigned to one of the following groups: high compression HIIT (HC), low compression HIIT (LC), high compression HIIT with berberine supplementation (HC + BBR), low compression HIIT with berberine supplementation (LC + BBR), exclusive berberine supplementation (BBR) and a control group (CON). The training groups performed a home HIIT protocol twice a week for 8 weeks, while the control and BBR groups maintained a sedentary lifestyle. The high-compression HIIT protocol consisted of 2–4 sets of 8 20-s sequences of physical activity, interspersed with 10 s of rest, with a 1-min rest between sets. In contrast, the low compression HIIT protocol included 20 s of rest between sequences. Participants in the HC + BBR, LC + BBR, and BBR groups received supplementation of 1,000 mg berberine in capsules daily. The results indicated that the low compression (LC) HIIT group presented a significant decrease in NLRP3 expression at the end of the intervention. In addition, all exercise groups, regardless of berberine supplementation, showed a reduction in IL-1β levels, suggesting a beneficial effect of HIIT on systemic inflammation in this population (30).
Several studies have demonstrated that progressive resistance training elicits anti-inflammatory effects by downregulating inflammasome-related gene expression, particularly NLRP3, CASPASE-1, and IL-1β. These effects are especially notable in older adults and individuals with prediabetes, overweight, or obesity. The observed molecular changes reflect a reduction in low-grade chronic inflammation, which is commonly associated with metabolic disorders and aging. A progressive resistance training program is therefore recommended as an effective strategy to modulate inflammation via the NLRP3 inflammasome pathway. Such programs should be performed 2–5 times per week for a minimum of 12 weeks, at an intensity ranging between 60% and 95% of maximum heart rate.
Combined aerobic and resistance exercise
Frequency ≤12 weeks
In a study in subjects with obesity they analyzed the effects of a high-intensity interval training (HIIT) program (TABATA) at a high and low volume, in conjunction with royal jelly supplementation. Participants were allocated into five experimental groups, a control group, and a placebo group. The training protocols were administered twice weekly over an 8-week period, while the supplementation groups received 1,000 mg of royal jelly daily for the same time. The relative expression of the NLRP3 gene was quantified using real-time polymerase chain reaction (RT-PCR). The findings indicated a significant reduction in NLRP3 expression across all intervention groups following the 8-week period, with the most pronounced decrease observed in the high-volume HIIT group receiving royal jelly supplementation (25).
Another study involving men with obesity and type 2 diabetes mellitus examined the effects of saffron supplementation combined with concurrent training (aerobic and resistance exercise). Participants were randomly assigned to one of four groups: concurrent training plus placebo (CT), saffron supplementation only (S), concurrent training combined with saffron supplementation (CTS), or a control group (CON). The training protocol consisted of four components per session: a 10-min warm-up, a resistance training (RT) circuit, an aerobic training (AT) circuit, and a 10-min cool-down. The RT component included exercises such as leg press, bench press, leg extension, lat pulldown, lying leg curl, and shoulder press. The AT protocol involved 10 1-min high-intensity intervals on a treadmill at 80%–95% of maximum heart rate (HRmax), interspersed with 1-min active recovery periods at 40%–60% of HRmax. Training intensity began at 80% HRmax in the first week and was progressively increased to 95% HRmax by the final week. Participants in the CTS group received a 100 mg capsule of pure saffron immediately after each training session and at the same time on non-training days. Those in the S group took the same daily dose of saffron at a consistent time, while participants in the CT group received an identical placebo daily. The study measured levels of the pro-inflammatory cytokine IL-1β. Results demonstrated that all three intervention groups—CT, S, and CTS—experienced a significant reduction in IL-1β concentrations compared to the control group (27).
Other study examined the effects of two types of exercise training [moderate-to-vigorous intensity continuous training (MICT) and high-intensity interval training (HIIT)] on circulating cytokines in male patients with coronary artery disease (CAD), with and without type 2 diabetes. Over 12 weeks, both MICT and HIIT led to significant reductions on IL-18, regardless of the presence of T2D or exercise modality. No significant effects were observed for IL-1β. Overall, both HIIT and MICT were effective in attenuating systemic low-grade inflammation in CAD patients, particularly those with T2D (24).
It has been demonstrated that combining aerobic and resistance exercise, as well as high-intensity interval training (HIIT), effectively reduces the expression of the NLRP3 gene and the proinflammatory cytokine IL-1β in individuals with obesity and type 2 diabetes. These anti-inflammatory effects have been observed even with a low training frequency of just two sessions per week over a period of 8–12 weeks, and were further enhanced when exercise was combined with adjunct interventions such as saffron or royal jelly supplementation. These findings suggest that implementing a combined aerobic and resistance exercise program, or a low-frequency HIIT protocol performed at least twice weekly for a minimum of 6–8 weeks, constitutes an effective strategy to reduce systemic inflammation mediated by the NLRP3 inflammasome and IL-1β, particularly in individuals with obesity and type 2 diabetes mellitus.
Isometric grip
Frequency ≤12 weeks
A randomized clinical trial aimed to determine if isometric grip reduces arterial stiffness and, in turn, reduces blood pressure. Patients with hypertension were recruited and stratified by sex and systolic blood pressure into three different groups: home isometric grip training, supervised isometric grip training, and a control group. Isometric grip training consisted of 3 sessions per week for 12 weeks. Each session involved four sets of 2-min isometric contractions with alternating hands, using a grip dynamometer at 30% of the maximum voluntary contraction, with a 60-s rest period. Participants in the control group were asked to continue with their normal dietary and physical activity habits; however, at the end of the study, they were provided with the isometric exercise program. The concentration of the cytokine IL-1β in plasma was evaluated using the Invitrogen kit. No statistically significant changes in IL-1β concentrations were found in any group (23).
The isometric training in patients with hypertension have shown that this form of exercise can confer notable cardiovascular benefits, including reductions in blood pressure and arterial stiffness. However, after 12 weeks of intervention, no significant changes were observed in plasma levels of the proinflammatory cytokine IL-1β. These findings suggest that, unlike other exercise modalities—such as aerobic, resistance, or high-intensity interval training (HIIT)—isometric handgrip training does not exert a demonstrable direct effect on NLRP3 inflammasome modulation or on systemic inflammation as measured by circulating IL-1β levels. However, further research employing this type of training is needed to enhance the robustness of the findings.
Discussion
The findings of this systematic review indicate that physical exercise, in its various modalities, constitutes an effective intervention to downregulate inflammatory activity mediated by the NLRP3 inflammasome. This effect is primarily achieved through the reduction of gene and/or protein expression of key inflammasome components such as NLRP3, ASC, and caspase-1, as well as through decreased circulating levels of the proinflammatory cytokines IL-1β and IL-18.
A key finding of this review was the modality-specific effect of exercise on inflammation. While moderate aerobic exercise consistently reduced gene expression of inflammasome-related targets, it did not consistently lower circulating IL-1β or IL-18 levels. In contrast, progressive resistance training and combined aerobic-resistance programs proved more effective in reducing both gene expression and systemic cytokine levels, with benefits evident from as early as 8 weeks of intervention (Figure 3). This discrepancy may be explained by the biphasic mechanism of inflammasome activation. The first signal (Signal 1), triggered by PAMPs and DAMPs, activates NF-κB and upregulates the transcription of NLRP3, pro-IL-1β, and pro-IL-18. However, these precursors are biologically inactive. A second signal (Signal 2) dependent on intracellular events such as oxidative stress, mitochondrial dysfunction, or ionic imbalance is required for inflammasome assembly, caspase-1 activation, and cytokine maturation. Therefore, exercise protocols that primarily affect transcriptional pathways, as seen with moderate aerobic training, may reduce gene expression without significantly affecting systemic cytokine levels, which are harder to detect due to their short half-life and localized release.
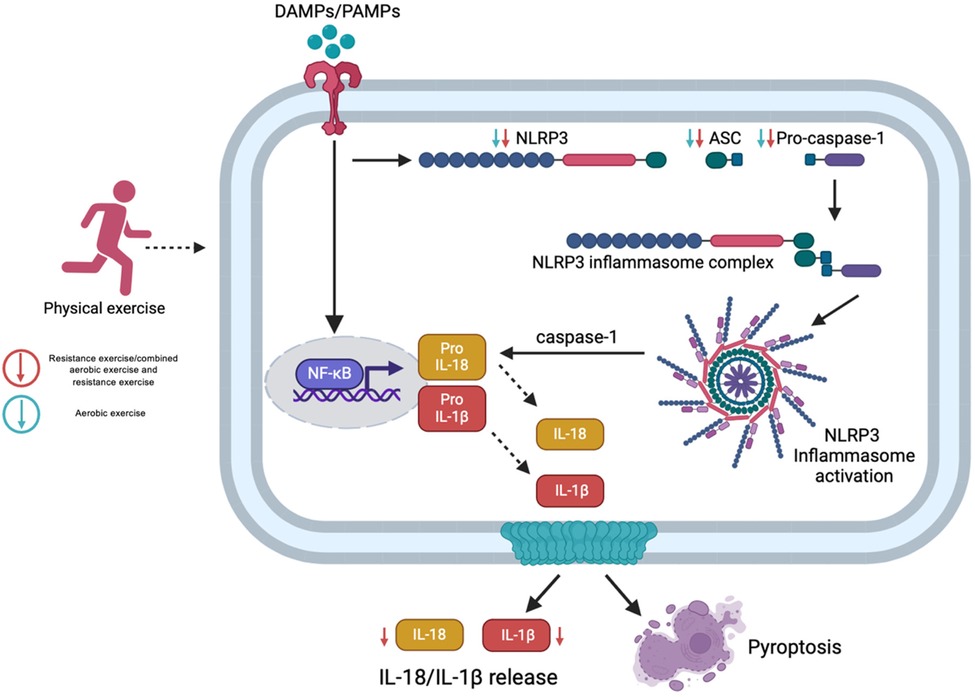
Figure 3. Molecular responses to NLRP3 inflammasome activation following different exercise modalities. Exercise exerts modality-specific effects on inflammation. Moderate aerobic exercise reduces NLRP3 inflammasome gene expression but shows limited impact on systemic IL-1β and IL-18. In contrast, resistance and combined training more effectively lower both gene expression and circulating cytokines, with measurable benefits within 8 weeks. Created with BioRender.com.
Conversely, resistance and combined training modalities induce both metabolic and mechanical stimuli, capable of simultaneously modulating Signal 1 and Signal 2, resulting in a more comprehensive suppression of inflammasome activation. This dual modulation translates into greater effectiveness in reducing both transcript and protein levels of key inflammatory mediators. Moreover, several included studies reported sustained anti-inflammatory benefits between 8 and 24 weeks of training, suggesting that structured and consistent exercise regimens can drive meaningful molecular adaptations, even in populations with elevated baseline inflammation due to metabolic conditions. In contrast, isometric handgrip exercise, while beneficial for blood pressure control, has not demonstrated significant effects on IL-1β levels, suggesting a limited capacity to modulate inflammasome-mediated inflammatory activity.
While certain limitations should be acknowledged, they do not significantly detract from the relevance and contribution of the present study. One such limitation is the heterogeneity among the included trials, which can be attributed to the relatively recent development of research exploring the effects of exercise on inflammasome activation. Consequently, the available evidence is not yet sufficient to enable a standardized comparison across different exercise modalities, metabolic conditions, and combined interventions. The inclusion of studies involving combined interventions may also enhance the effects of exercise, potentially influencing the interpretation of results and contributing to the observed variability. Additionally, some studies report only gene expression data without corresponding protein concentration measurements, which may limit the depth of interpretation. Nonetheless, despite these challenges, the study provides valuable insights and highlights important directions for future research in this emerging field.
Future research should prioritize the design and implementation of randomized controlled trials (RCTs) with robust methodological frameworks. These studies should employ standardized and supervised exercise protocols (carefully controlling for intensity, duration, and type of activity) to allow for more accurate comparisons across populations and metabolic conditions. Moreover, integrating both gene expression analyses and cytokine quantification in these trials will be essential to elucidate the upstream and downstream effects of exercise on the NLRP3 inflammasome complex and its related inflammatory mediators.
Conclusion
Despite methodological heterogeneity among studies in terms of participant populations, intervention duration, exercise protocols, and biomarker assessments, consistent patterns emerged. Aerobic exercise, resistance exercise, and the combination of both, when performed regularly (≥8 weeks, 3 sessions per week), seems to demostrate an anti-inflammatory effect by down-regulating NLRP3, ASC, CASPASE-1, IL-1β, and IL-18, independently in individuals with disease and in healthy individuals.
Altogether, these findings underscore the role of physical exercise as a safe, non-pharmacological, and personalized strategy to counteract chronic low-grade inflammation via the NLRP3 inflammasome pathway. Resistance and combined training modalities appear particularly effective in clinical contexts where inflammation plays a central role.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
SC-H: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. MV-B: Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. MV-J: Investigation, Resources, Writing – review & editing. EM-L: Methodology, Supervision, Writing – review & editing. EB-C: Conceptualization, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Camell C, Goldberg E, Dixit VD. Regulation of NLRP3 inflammasome by dietary metabolites. Semin Immunol. (2015) 27(5):334–42. doi: 10.1016/j.smim.2015.10.004
2. Montaño Estrada LF, Fortoul Van der Goes TI, Rendón Huerta EP, Montaño Estrada LF, Fortoul Van der Goes TI, Rendón Huerta EP. ¿Qué son los inflamosomas? El NLRP3 como por ejemplo. Rev Fac Med (Méx). (2017) 60(1):42–9.
3. Ziehr BK, MacDonald JA. Regulation of NLRPs by reactive oxygen species: a story of crosstalk. Biochim Biophys Acta (BBA) Mol Cell Res. (2024) 1871(8):119823. doi: 10.1016/j.bbamcr.2024.119823
4. Lamkanfi M. Emerging inflammasome effector mechanisms. Nat Rev Immunol. (2011) 11(3):213–20. doi: 10.1038/nri2936
5. Bauernfeind F, Bartok E, Rieger A, Franchi L, Núñez G, Hornung V. Cutting edge: reactive oxygen species inhibitors block priming, but not activation, of the NLRP3 inflammasome. J Immunol. (2011) 187(2):613–7. doi: 10.4049/jimmunol.1100613
6. Fink SL, Cookson BT. Caspase-1-dependent pore formation during pyroptosis leads to osmotic lysis of infected host macrophages. Cell Microbiol. (2006) 8(11):1812–25. doi: 10.1111/j.1462-5822.2006.00751.x
7. Dupaul-Chicoine J, Arabzadeh A, Dagenais M, Douglas T, Champagne C, Morizot A, et al. The NLRP3 inflammasome suppresses colorectal cancer metastatic growth in the liver by promoting natural killer cell tumoricidal activity. Immunity. (2015) 43(4):751–63. doi: 10.1016/j.immuni.2015.08.013
8. Ridker PM, Hennekens CH, Buring JE, Rifai N. C-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in women. N Engl J Med. (2000) 342(12):836–43. doi: 10.1056/NEJM200003233421202
9. Stienstra R, van Diepen JA, Tack CJ, Zaki MH, van de Veerdonk FL, Perera D, et al. Inflammasome is a central player in the induction of obesity and insulin resistance. Proc Natl Acad Sci U S A. (2011) 108(37):15324–9. doi: 10.1073/pnas.1100255108
10. Stienstra R, Joosten LAB, Koenen T, Tits B van, Diepen JA van, Berg SAA, et al. The inflammasome-mediated caspase-1 activation controls adipocyte differentiation and insulin sensitivity. Cell Metab. (2010) 12(6):593–605. doi: 10.1016/j.cmet.2010.11.011
11. Duewell P, Kono H, Rayner KJ, Sirois CM, Vladimer G, Bauernfeind FG, et al. NLRP3 inflamasomes are required for atherogenesis and activated by cholesterol crystals that form early in disease. Nature. (2010) 464(7293):1357–61. doi: 10.1038/nature08938
12. Halle A, Hornung V, Petzold GC, Stewart CR, Monks BG, Reinheckel T, et al. The NALP3 inflammasome is involved in the innate immune response to amyloid-β. Nat Immunol. (2008) 9(8):857–65. doi: 10.1038/ni.1636
13. Sakhon OS, Victor KA, Choy A, Tsuchiya T, Eulgem T, Pedra JHF. NSD1 mitigates caspase-1 activation by listeriolysin O in macrophages. PLoS One. (2013) 8(9):e75911. doi: 10.1371/journal.pone.0075911
14. Haileamlak A. Physical inactivity: the major risk factor for non-communicable diseases. Ethiop J Health Sci. (2019) 29(1):810. doi: 10.4314/ejhs.v29i1.1
15. Lee I-M, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Impact of physical inactivity on the world’s major non-communicable diseases. Lancet. (2012) 380(9838):219–29. doi: 10.1016/S0140-6736(12)61031-9
16. You T, Arsenis NC, Disanzo BL, LaMonte MJ. Effects of exercise training on chronic inflammation in obesity: current evidence and potential mechanisms. Sports Med. (2013) 43(4):243–56. doi: 10.1007/s40279-013-0023-3
17. Abd El-Kader SM, Al-Shreef FM. Inflammatory cytokines and immune system modulation by aerobic versus resisted exercise training for elderly. Afr Health Sci. (2018) 18(1):120–31. doi: 10.4314/ahs.v18i1.16
18. Mejías-Peña Y, Estébanez B, Rodriguez-Miguelez P, Fernandez-Gonzalo R, Almar M, de Paz JA, et al. Impact of resistance training on the autophagy-inflammation-apoptosis crosstalk in elderly subjects. Aging (Albany NY). (2017) 9(2):408–18. doi: 10.18632/aging.101167
19. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. Declaración PRISMA 2020: una guía actualizada para la publicación de revisiones sistemáticas. Rev Esp Cardiol (Engl Ed). (2021) 74(9):790–9. doi: 10.1016/j.recesp.2021.06.016
20. Higgins JP, Green S. Manual Cochrane de revisiones sistemáticas de intervenciones Version 5.1.0. London: The Cochrane Collaboration (2011). p. 1–639. Available online at: http://handbook.cochrane.org/
21. Armannia F, Ghazalian F, Shadnoush M, Keyvani H, Gholami M. Effects of high-intensity interval vs. moderate-intensity continuous training on body composition and gene expression of ACE2, NLRP3, and FNDC5 in obese adults: a randomized controlled trial. Med J Islam Repub Iran. (2022) 36:161. doi: 10.47176/mjiri.36.161
22. Barrón-Cabrera E, González-Becerra K, Rosales-Chávez G, Mora-Jiménez A, Hernández-Cañaveral I, Martínez-López E. Low-grade chronic inflammation is attenuated by exercise training in obese adults through down-regulation of ASC gene in peripheral blood: a pilot study. Genes Nutr. (2020) 15(1):15. doi: 10.1186/s12263-020-00674-0
23. Rodrigues C, Farah SL, Silva BQ, Correia G, Pedrosa M, Vianna R, et al. Vascular effects of isometric handgrip training in hypertensives. Clin Exp Hypertens. (2020) 42(1):24–30. doi: 10.1080/10641963.2018.1557683
24. Garneau L, Terada T, Mistura M, Mulvihill EE, Reed JL, Aguer C. Exercise training reduces circulating cytokines in male patients with coronary artery disease and type 2 diabetes: a pilot study. Physiol Rep. (2023) 11(5):e15634. doi: 10.14814/phy2.15634
25. Gholitabar S, Dabidi Roshan V, Fallah M. Effects of TABATA exercise volume and royal jelly supplementation on NLRP3 inflammasome and lncRNA-H19 expression in obese men. Asian J Sports Med. (2024) 15(4):1–11. doi: 10.5812/asjsm-151873
26. Gomarasca M, Micielska K, Faraldi M, Flis M, Perego S, Banfi G, et al. Impact of 12-week moderate-intensity aerobic training on inflammasome complex activation in elderly women. Front Physiol. (2022) 13:792859. doi: 10.3389/fphys.2022.792859
27. Hooshmand Moghadam B, Rashidlamir A, Attarzadeh Hosseini SR, Gaeini AA, Kaviani M. The effects of saffron (Crocus sativus L.) in conjunction with concurrent training on body composition, glycaemic status, and inflammatory markers in obese men with type 2 diabetes mellitus: a randomized double-blind clinical trial. Br J Clin Pharmacol. (2022) 88(7):3256–71. doi: 10.1111/bcp.15222
28. Hoseini R, Rahim HA, Ahmed JK. Concurrent alteration in inflammatory biomarker gene expression and oxidative stress: how aerobic training and vitamin D improve T2DM. BMC Complement Med Ther. (2022) 22:165. doi: 10.1186/s12906-022-03645-7
29. Liu J, Diao L, Xia W, Zeng X, Li W, Zou J, et al. Meteorin-like protein elevation post-exercise improved vascular inflammation among coronary artery disease patients by downregulating NLRP3 inflammasome activity. Aging. (2023) 15(24):14720–32. doi: 10.18632/aging.205268
30. Nikseresht M, Dabidi Roshan V, Nasiri K. Inflammatory markers and noncoding-RNAs responses to low and high compressions of HIIT with or without berberine supplementation in middle-aged men with prediabetes. Physiol Rep. (2024) 12(15):e16146. doi: 10.14814/phy2.16146
Keywords: ASC, caspase-1, exercise training, NLRP3 inflammasome, NLRP3 physical activity
Citation: Cristerna-Huerta SV, Vega-Burgueño M, Vergara-Jiménez MdJ, Martínez-López E and Barrón-Cabrera E (2025) Assembly and activation of the NLRP3 inflammasome and cytokine quantification in response to exercise in adults with different metabolic conditions: a systematic review. Front. Sports Act. Living 7:1602208. doi: 10.3389/fspor.2025.1602208
Received: 29 March 2025; Accepted: 7 July 2025;
Published: 21 July 2025.
Edited by:
Zhiwen Luo, Fudan University, ChinaReviewed by:
Gerardo Pavel Espino-Solis, Autonomous University of Chihuahua, MexicoLijing Gong, Beijing Sport University, China
Copyright: © 2025 Cristerna-Huerta, Vega-Burgueño, Vergara-Jiménez, Martínez-López and Barrón-Cabrera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elisa Barrón-Cabrera, ZWxpc2FiYXJyb25AdWFzLmVkdS5teA==