 Brice Picot1,2*
Brice Picot1,2* Alexandre Maricot3
Alexandre Maricot3 François Fourchet2,4
François Fourchet2,4 Alli Gokeler5,6
Alli Gokeler5,6 Bruno Tassignon3,7
Bruno Tassignon3,7 Ronny Lopes8
Ronny Lopes8 Alexandre Hardy9
Alexandre Hardy9
- 1Inter-University Laboratory of Human Movement Biology (LIBM), Savoie Mont-Blanc University, Chambéry, France
- 2French Society of Sports Physical Therapy (SFMKS Lab), Pierrefitte-sur-Seine, France
- 3Human Physiology and Sports Physiotherapy Research Group, Faculty of Physical Education and Physiotherapy, Vrije Universiteit Brussel, Brussels, Belgium
- 4Department of Physiotherapy, La Tour Hospital, Meyrin, Switzerland
- 5Exercise Science and Neuroscience, Department of Exercise & Health, Paderborn University, Paderborn, Germany
- 6Faculty of Health, Amsterdam University of Applied Science, Amsterdam, Netherlands
- 7REVAL Rehabilitation Research Center, Faculty of Rehabilitation Sciences, Hasselt University, Diepenbeek, Belgium
- 8Centre Orthopédique Santy, Hôpital Privé Jean Mermoz, Lyon, France
- 9Clinique du Sport, Paris, France
Lateral ankle sprain (LAS) is the most common traumatic injury, with a high recurrence rate and chronic ankle instability (CAI) developing in ∼40% of cases. LAS leads to patho-mechanical, sensory-perceptual and motor-behavioral deficits. Poor management of the return-to-sport (RTS) is now considered a major cause of re-injury and development of CAI, particularly due to the lack of validated tests and the failure of existing ones to account for those central deficits. The first part of this topic aimed to clarify concepts of cognitive constructs and sensory reweighting and their association with CAI. We also aimed to identify objective RTS criteria and discuss their limits regarding their ability to encompass central impairments. Motor-cognitive deficits have been identified using computerized cognitive tasks and dual-task paradigms. More specifically, deficits in visual memory, processing speed or inhibitory control and attentional resource allocation have demonstrated reduced performance in CAI populations. In addition, altered sensory reweighting process towards visual input has also been observed. While objective criteria are crucial to prevent re-injury, current evaluations remain largely subjective and central impairments are unaccounted for in conventional RTS testing. The Ankle-GOTM score was recently developed to guide clinicians in decision making process. To date, it is the first validated score that could help to identify patients who will RTS at the same level, those at risk of recurrence and those who are more likely to become copers. Unfortunately, it does not target cognitive or sensory reweighting alterations, that are both relevant in sport to manage gameplay demands.
1 Introduction
Lateral Ankle Sprain (LAS) is the most common injury in sports (1), and up to 40% of patients will develop chronic ankle instability (CAI) (2). This condition is characterized by a history of LAS resulting in a feeling of ankle instability, episodes of giving way and/or recurrent sprains as well as loss of function reported during daily activities and sports (3, 4). Ultimately, LAS has substantial consequences on patients, ranging from socio-economic impact to a diminished quality of life, often associated with the early onset of ankle osteoarthritis (5).
CAI is characterised by a spectrum of symptoms related to the ankle itself. According to the integrative model proposed by Hertel and Corbett (4), pathomechanical impairments represent a key component contributing to the development and perpetuation of chronic ankle instability (CAI). These impairments encompass structural and mechanical alterations that disrupt normal joint function. Notably, recurrent ankle sprains may lead to ligamentous laxity, altered arthrokinematics, and insufficient passive restraint, which in turn compromise joint congruency and load distribution. Additionally, deficits in dorsiflexion range of motion and postural alignment changes can modify movement patterns and increase stress on adjacent structures. Together, these mechanical disruptions establish a maladaptive foundation that predisposes individuals to persistent symptoms and recurrent injury.
Other factors that are not physically identifiable during routine examinations may also be present. Hertel and Corbett (4) emphasize that sensory-perceptual impairments play a central role in the CAI continuum. These deficits primarily reflect disrupted afferent input from peripheral mechanoreceptors following LAS. Diminished somatosensory feedback, particularly from the ligaments and surrounding soft tissues, can alter joint position sense and impair proprioception (6). Such changes compromise the central nervous system's ability to accurately perceive limb orientation and movement, thereby reducing sensorimotor control. As a result, individuals with CAI often exhibit delayed or inappropriate neuromuscular responses during dynamic tasks, further increasing the risk of reinjury and perpetuating functional limitations.
The same authors (4) highlight these motor-behavioral impairments as a critical component influencing long-term functional outcomes. They refer to maladaptive changes in motor planning and execution that emerge as a consequence of repeated injury and altered sensory input. During dynamic tasks, CAI patients often develop compensatory movement strategies, such as reduced joint excursions, increased co-contraction, or altered muscle recruitment patterns (7, 8). These protective behaviors are driven by fear of reinjury or reduced confidence in the ankle's stability. Altered motor pattern becomes progressively ingrained, contributing to performance deficits and perpetuating the cycle of instability.
This establishes the concept of a neurosignature unique to each patient, functioning as a form of individual and multifactorial identity profile (4). This interaction is particularly relevant because it enables us to interact with our environment accordingly. The brain sits between this interaction and influences this feedback loop constantly and brain neuroplasticity is frequently observed following LAS (9). The set of brain changes associated with CAI (=a neurosignature involving structural and functional adaptations) may affect not only how individuals respond to external stimuli, but also higher-order cognitive processes such as attention, working memory, and inhibition (10). Lastly, recent evidence suggests alterations in the sensory reweighting process (11–13), with an increased visual reliance among patients suffering from CAI (14, 15). One of the main reasons for the burden of LAS, particularly the high recurrence rate and the development of CAI, is poor management of the return-to-sport (RTS) (16). Conventional RTS assessments do not take these recent data into account and therefore do not target the central deficits that may be present among patients.
The overall objective of this two-part article (mini-review and perspective) is to summarize current knowledge on the central deficits associated with CAI, as well as existing RTS criteria. We will also propose a new tool for assessing cognitive deficits and sensory reweighting alteration in CAI patients to assist clinicians in their decision-making process, based on recent data.
In the first part, we present a synthesis of scientific literature addressing cognitive impairments and alterations in sensory reweighting associated with CAI. We also summarize the current literature regarding objective RTS criteria and discuss their limitations. Furthermore, we outline potential approaches for improving the assessment of central deficits through the implementation of dual-task paradigms.
In the second part (Targeting Visual-Sensory and Cognitive Impairments Following Lateral Ankle Sprains: A Practical Framework for Functional Assessment Across the Return-to-Sport Continuum. Part 2: From theory to practice: recommendations for optimizing Return To Sport after lateral ankle sprains using cognitive and visual-sensory assessments, Frontiers in Sports and Active Living, [under review]), we propose a β “brain” extension of the Ankle-GO™ score, which currently represents the only objective RTS criterion. This extension integrates dual-task conditions into each functional item of the score, in order to capture potential cognitive and sensory reweighting deficits in patients. In addition, we describe a framework for quantifying cognitive cost under dual-task conditions (DTC), thereby enabling clinicians to more effectively interpret the outcomes of this β “brain” extension.
2 Understanding central mechanisms and their implications in dynamic tasks
Too often, the field of cognition and its implications in dynamic tasks are haphazardly conflated or even confused—with topics related to sensory/visual reweighting. Given their potential importance in the context of LAS, we will clearly define what cognition and sensory reweighting process precisely are in the next paragraphs.
Human motor control emerges from an integrated network of cortical and subcortical regions. The primary motor cortex executes voluntary actions, while the premotor and supplementary motor areas coordinate planning and sequencing (17, 18). Higher-order cognitive control is provided by the prefrontal cortex, while the basal ganglia and cerebellum regulate movement initiation, learning, and fine-tuning (19, 20). Sensory integration is mediated by the posterior parietal cortex, which combines visual and proprioceptive information, with the cerebellum and vestibular pathways (17, 21). Then the superior parietal and association cortex further weight feedback to enhance motor control (13).
2.1 Cognition
According to Diamond (22), cognition is the study of cognitive processes or functioning in connection with the particular neural mechanisms that underlie them in the brain and any impairment of these mechanisms. In many sports situations that require focus, coordination, and control to override internal or external stimuli, higher-level cognitive functions, also known as “executive functions”, are crucial. As a collection of adaptive behaviors that enable athletes to successfully navigate the environment by shifting and adapting to changing environmental cues and needs, executive functions are defined as the capacity to coordinate cognitive, emotional, and motor processes (22). It is possible to distinguish between three primary executive functions: cognitive flexibility, working memory, and inhibition. The ability to regulate one's thoughts, behavior, attention, and/or emotions to overcome a strong internal inclination to act or an outside distraction is known as inhibition, or inhibitory control (22). Working memory, which describes a person's capacity to retain and hold information in an active, readily retrievable state while blocking out distractions and interference, is closely related to inhibitory control (22, 23). Cognitive flexibility is the ability to modify cognitive processing techniques in response to novel situations (22). For instance, processing speed (such as reaction time), visual attention, and dual tasking are examples of lower-level cognitive abilities. Information processing speed is the rate at which an athlete processes new information and the amount of time needed to retrieve previously stored information from memory. Information processing speed is a fundamental cognitive function required for more complex functions like working memory. It characterizes an athlete's capacity to perceive, process, and react to a sensory stimulus. A common metric for evaluating an athlete's ability to react quickly to a given stimulus is reaction time. The attempt to complete two or more tasks at the same time is known as dual tasking or multitasking (24). It is believed that training cognitive functions can be used to enhance one or more facets of sports performance by better understanding the distinct cognitive functions that underpin sports performance, both domain-general and domain-specific (25). This approach has been criticized, though, because it might not be sport-specific given the complexity of athletic settings (24). While domain-specific cognitive skill training is thought to have a higher transfer to sports performance because of its higher ecological validity, domain-general cognitive skill training is argued to not necessarily transfer to sports performance (25, 26).
2.2 Sensory reweighting
Sensory reweighting refers to the central nervous system's (CNS) ability to dynamically adjust the relative importance (or “weight”) of different sensory inputs (i.e visual, vestibular, and somatosensory/proprioceptive) to maintain balance and posture (27–29). This process allows individuals to adapt to changing environmental conditions in order to maintain optimal postural control. The relative weight of each sensory system depends on factors such as task complexity, environmental conditions, and the accuracy of sensory input. For example, when standing on firm surfaces, the CNS primarily relies on proprioception and vision to maintain balance. However, when standing on an unstable surface, the CNS reduces reliance on somatosensory input and shifts to more reliable sources, such as visual cues if available. In eyes-closed (EC) conditions, an increased reliance on somatosensory cues is observed (21).
There are different ways to identify visual contribution during postural control. Recently, the development of strobe glasses allows patients to perform dynamic tasks under perturbed vision, whereas full EC conditions only permit static tasks (14, 30). By constraining visual input (i.e stroboscopic vision) during dynamic activities such as hopping or jumping, clinicians can assess sensory reweighting towards vision. A significant decrease in performance under SV conditions, particularly in comparison to the uninjured limb or healthy individuals, may indicate increased reliance on visual input.
To summarize, successful performance in dynamic tasks relies on the integrated function of both lower- and higher-order cognitive processes. Lower-order cognition involves the fundamental, often automatic, processing of sensory input, while higher-order cognition encompasses the complex mechanisms of attention, memory, decision-making, and executive control (31). Together, these processes shape how information is interpreted and acted upon by integrating incoming sensory data with prior knowledge and task goals to guide behavior. In parallel, sensory reweighting is an adaptive process where the central nervous system dynamically shifts its reliance among sensory modalities (e.g., vision, proprioception, vestibular) based on environmental conditions and task demands. A key distinction is that while cognition governs the interpretation of information and subsequent decision-making, sensory reweighting adjusts the input signals themselves to optimize sensorimotor control.
A decline in either cognitive function (affecting interpretation and decision-making) or sensory reweighting abilities (disrupting the quality of sensory input) can reduce motor performance. This creates a potential sensorimotor mismatch, where the brain's commands and the body's feedback are misaligned, increasing the risk of injury (Figure 1). These alterations are commonly described in patients with CAI and may explain the high rate of recurrence in this population.
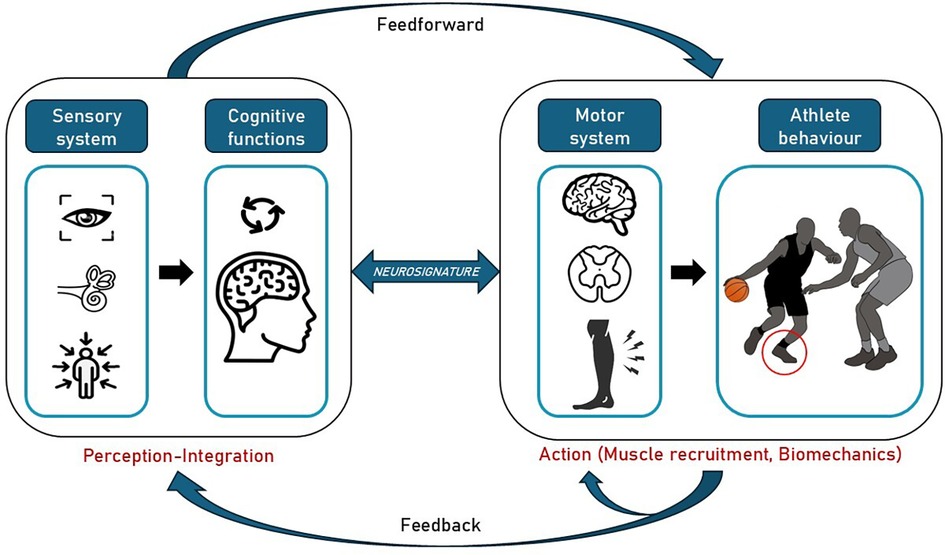
Figure 1. Motor control model driving specific athlete behaviour in a game situation with high risk of lateral ankle sprain. This involves perception of the environment (sensory informations), rapid and effective integration of these cues (cognitive functions), resulting in the production of afferents (motor system) leading to specific athlete biomechanics (action) to the game situation (Neurosignature).
3 Central alterations and RTS management following LAS
In the context of ankle impairments and drawing on Hertel's model (4)—particularly the sensorimotor loop—numerous clinical and practical applications can be identified.
3.1 Cognitive functions
Recent studies have identified subtle cognitive impairments in CAI mostly assessed using computerised cognitive tasks (CNT) and dual-task paradigms (10). The most commonly used paradigms to assess cognitive deficits were the number generation or digit span task and the serial subtraction performed during single-leg stance or gait (10).
Seated CNT have revealed deficits in visual memory (32), while evidence for impairments in attention (32–34) and processing speed is mixed (32, 34–38). Dual-task assessments have provided additional evidence for compromised cognitive-motor integration in CAI (39–44). Specifically, dual-task paradigms that tested inhibitory control and attentional resource allocation have demonstrated reduced performance in CAI populations compared to healthy controls (45, 46). This is particularly relevant given the functional overlap between perception–action coupling and executive control: many sport-specific or daily tasks require cognitive regulation of movement, especially when there is time pressure, adaptability is required. Understanding this interplay offers important insight into the central mechanisms that may underpin persistent functional deficits in CAI.
Indeed, CAI patients often exhibit longer reaction times, reduced spatial perception, and impaired memory (32, 38, 42, 47, 48). These deficits result in a reduced ability to respond to a dynamic and unpredictable environment, which is particularly common in sport, thereby increasing the likelihood of sensorimotor mismatch.
It should be noted that all mentioned studies relied relatively small patient samples (n < 30) and presented heterogeneity in the inclusion criteria for CAI, which may account for result variability (10, 39). Differences in dual-task outcomes could also reflect task difficulty and heterogeneity within CAI groups. Despite the accumulation of scientific data, the level of evidence remains limited and additional high-quality studies are needed to better understand, identify, and target cognitive deficits in patients with LAS/CAI.
3.2 Sensory reweighting
An increased reliance on visual information has been identified in CAI patients compared to healthy individuals during single-leg stance (13–15). While inconsistent results have been observed in eyes-open conditions, CAI patients almost consistently exhibit postural control impairments during eyes-closed conditions. Inadequate sensory reweighting may contribute to the functional deficits observed in CAI, caused by over- or under-reliance (beyond or under utilising what's optimal) on specific types of sensory input. For instance, while increased reliance on visual input may help maintain balance during traditional rehabilitation exercises, this strategy often breaks down in more complex, sport-specific environments. In such setting visual resources are already heavily engaged in managing gameplay demands such as tracking opponents, anticipating ball trajectories, and responding to unpredictable events.
The exact cause of this mechanism among CAI patients remains unclear. Since somatosensory receptors, such as articular receptors or muscle spindles, are frequently disrupted following LAS, loss of proprioception is frequently observed (6, 49). It could be argued that the CNS is enabled to overcome this loss of proprioceptive signals and shift to compensate for its reliance on visual information. Recent results (13) revealed that CAI patients show stronger but less stable functional connectivity between the superior parietal cortex and visual cortices, as well as greater variability in connectivity with the spinocerebellum, which correlates with increased visual reliance. Overall results align with Freeman's articular deafferentation theory (50).
Increased visual reliance is therefore considered as a compensatory mechanism that could partially explain postural control impairments and functional deficits observed following LAS and the high rate of recurrences. Therefore, it is crucial to identify individuals who rely excessively on vision for balance and implement rehabilitation strategies to restore appropriate sensory reweighting following injury.
Overall results confirm that central deficits occurred following LAS and could exist among CAI patients. However, it should be noted that there are significant discrepancies regarding inclusion criteria and the definition of CAI patients across studies. We recommend that authors follow the IAC guidelines when including CAI patients (3). More specifically, patient should (i) have suffered a history of at least one significant ankle sprain at least 12 months prior to the study enrolment, (ii) reported ankle joint “giving way”, and/or recurrent sprain and/or “feelings of instability” on the same ankle and (iii) reported diminished self-reported function.
Poor management of RTS is a key contributor to high recurrence rates and the development of CAI. Given recent data, it therefore seems essential to target central alterations throughout the RTS phase, particularly in sports patients performing dual-task situations. The following section reviews the current management of RTS, existing validated objective criteria and identifies their potential limitations in this regard.
3.3 Management of RTS
Return-to-Sport decisions are critical at the end of rehabilitation, particularly in populations such as individuals with CAI, where the risk of re-injury remains high. While physical recovery (e.g., restoration of range of motion, strength, and balance) is necessary, it is not sufficient to ensure safe and sustained RTS (51). A systematic review highlighted the lack of objective criteria to safely guide return-to-sport decisions (52). To date, there is no consensus on the specific criteria to be used, and decisions are still largely based on time-based guidelines (16).
Research shows that nearly half of athletes resume their sports activities the day after the injury, and within a week, up to 80% have returned to play (53, 54). However, most athletes do so without having fully recovered from the impairments caused by the sprain—such as deficits in postural control and joint range of motion (55, 56).
An expert consensus conducted by the International Ankle Consortium (IAC) emphasized the importance of evaluating five key domains before clearing an athlete to return to sport (57). The authors proposed a new “PAASS” framework to evaluate Pain, Ankle-specific impairments, Athlete perception (including kinesiophobia and psychological readiness), Sensorimotor control, and Sport-specific functional performance to guide clinicians in assessing readiness. Unfortunately, it does not specify how clinicians should assess these items.
3.4 The Ankle-GO™ score
This tool is a cluster of six items selected on their relevance for monitoring LAS patients (58, 59) and the recommendation of PAASS framework (57). All items and threshold values were selected based on their ability to distinguish between healthy individuals, copers, and patients with CAI. Finally, they were selected if they demonstrated sufficient reliability and validity and did not require specific or expensive equipment. The total duration of the Ankle-GO™ test does not exceed 30 min.
It has been recently developed and validated among patients suffering from CAI and could help to identify patients who will RTS at the same level of play (58), those who will suffer reinjury (60), and those who are more likely to become coper (61). The total score is 25 points (Table 1) spread over two self-reported questionnaires as well as four functional tests.
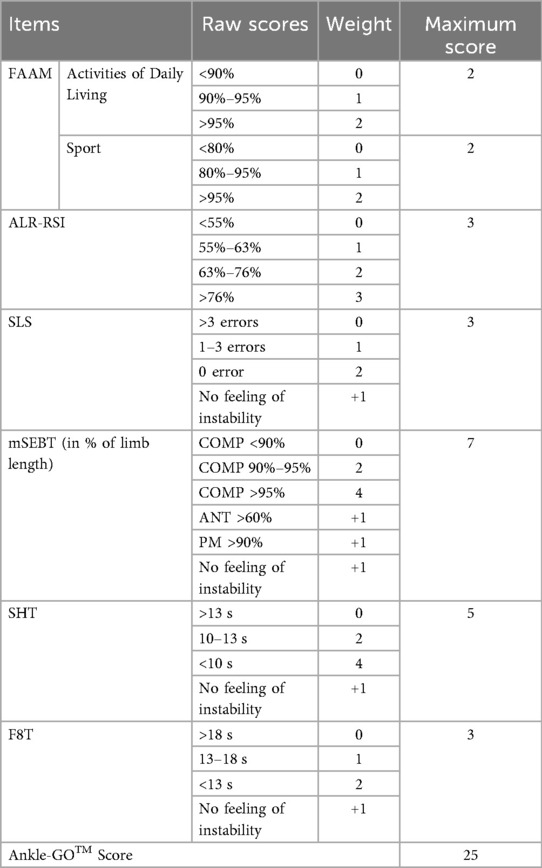
Table 1. Ankle-GO scoring system [adapted from (58)].
Ankle ligament reconstruction–return to sport after injury (ALR-RSI)
The ALR-RSI questionnaire assesses the psychological readiness of athletes to RTS following an ankle sprain (62–65). It includes 12 items rated from 0 (no confidence) to 10 (full confidence), with the total score converted to a percentage. Based on the original ACL-RSI and adapted for ankle injuries, the tool reflects the athlete's confidence and emotions, a higher score indicating better psychological readiness. LAS patients scoring above 46% two months after injury were more likely to return to preinjury level of sport or higher at 4 months (62).
Foot and ankle ability measure (FAAM)
The FAAM is a patient-reported outcome measure composed of two subscales: the Activities of Daily Living (FAAM-ADL, 21 items) and the Sports subscale (FAAM-Sport, 8 items) (66). Each item is rated on a 5-point Likert scale from 0 (unable to perform) to 4 (no difficulty). Scores are converted into percentages for each subscale, providing an overview of functional limitations. The FAAM is validated for CAI (67), higher scores indicate better self-reported function. Cut-off scores of 90% and 80% in ADL and Sports subscales, respectively, are used to identify patients with CAI (3). In addition, individuals are commonly considered copers if they score greater than 95% on both subscales (4).
Single-leg stance test (SLS)
The SLS test evaluates static postural control. The subject stands barefoot on one leg, eyes closed, with hands on hips and a slightly flexed knee (10°) for 20 s (68, 69). Examiner reports the number of balance errors during the tests: lifting hands-off iliac crest, opening eyes, stepping, stumbling or falling, moving hip into more than 30° of flexion or abduction, lifting forefoot or heel and remaining out of the test position more than 5 s (Table 1). A low number of errors indicates good static postural control. A proposed 3-error cut-off score is commonly used to identify CAI patients (68).
Modified star excursion balance test (mSEBT)
The mSEBT assesses dynamic postural control across three directions: anterior (ANT), posteromedial (PM), and posterolateral (PL) (70, 71). Standing barefoot on one leg, the patient reaches with the other leg in each direction and returns to the initial position without losing balance. The trial is canceled if the subject lifts any part of the stance foot, removes his/her hands from the hips or transfers weight to the other limb. The distance is recorded (in cm) and evaluated in relation to the limb length (from the anterior and superior iliac spine to the medial malleolus). A composite score (COMP) is calculated as the average of the three directions. After 4 learning trials in each direction for each leg, 3 trials are recorded and averaged (Table 1). Lower reaching distance indicates poorer dynamic postural control. Individuals scoring below 94% and 89.1% in the COMP score are more likely to get injured, and a cut-off score of 91% in the PM direction is described to identify CAI patients (68, 72, 73).
Side hop test (SHT)
The SHT evaluates lateral agility and neuromuscular control (74, 75). The patient hops side-to-side across two lines spaced 30 cm apart, completing 10 cycles as quickly as possible. The first hop is directed outward. Only valid hops (i.e without touching the lines) are counted. Completion time is recorded (Table 1). A cut-off score of 12.9 s has been calculated to identify CAI patients (68), with values below 10 s observed in the uninjured limb or healthy patients (74).
Figure-of-8 test (F8T)
The F8T is an agility test where the patient hops on one limb in a figure of 8 pattern as fast as possible between two cones 5 meters apart. The patient has to perform two consecutive laps, for a total distance of 20 m) (74). The time taken to complete the exercise is recorded, with a longer time reflecting poorer single-limb hopping performance. A cut-off score of 17.4 s was calculated to identify CAI patients (68), with values below 12 s observed in the uninjured limb or healthy patients (74).
An additional point is awarded for each of the four functional tests (SLS, mSEBT, SHT, F8T) if the subject does not report any feeling of instability during the activity (Table 1). This subjective measure accounts for perceived stability of the ankle, which is a key factor in chronic ankle instability (74).
Recent results revealed that following LAS, patients who score below 8 pts on the Ankle-GO™ score are less likely to RTS at the same level of play and 9 times more likely to suffer a reinjury within 2 two years (58, 60). In addition, those who score above 11 pts are 12 times more likely to become LAS copers (61). Lastly, after lateral ankle reconstruction for CAI patients, a cut-off score of 6 points allows to identify those who will return to sports (odd ratio = 18) (76).
The Ankle-GO™ score demonstrates good construct validity and internal consistency (Cronbach's α of 0.79) and excellent test–retest reliability (ICC = 0.99, with a minimal detectable change of 1.2 points), but these findings are based on a relatively small and homogeneous sample (64 LAS patients and 30 controls) (58). The tool was validated exclusively in physically active patients, limiting generalizability to elite athletes, adolescents, and older adults. Moreover, although discriminant and predictive validity were supported with Area under the Receiver Operating Characteristic Curve (AUC) = 0.77 for predicting RTS at 4 months, AUC = 0.75 for predicting reinjury over 2 years and AUC = 0.7 for predicting copers, these figures fall in the “fair to good” range, indicating that this score cannot be used as a standalone test for RTS.
4 Discussion
Despite very promising results, the Ankle-GO™ score is not perfect, particularly because it does not encompass dual-task situations or visual constraints that could highlight central deficits in patients. Yet, emerging theories suggest that central factors also play a pivotal role in ensuring a safe RTS, particularly in sports requiring cognitive constraints with dual tasks situations where visual attention is dedicated to the management of a ball or an opponent (Figure 1). Unfortunately, only few RTS evaluations involved cognitive constraints (47, 77). Thus, there is an urgent need to develop functional performance tests that incorporate cognitive and visual perturbations in patients with CAI (10, 32, 78, 79).
For example, during a hopping test, it is possible to add a secondary (cognitive) task such as counting backwards, memorizing and repeating a sequence of numbers, or reacting to a stimulus (color, sound, word). Performance can be evaluated by comparing the results of the motor test alone (distance, stability, contact time…) with those obtained under dual-task conditions. In parallel, cognitive errors and reaction time can be analyzed. Any deterioration in performance or cognition may indicate which task is being prioritized by the patient. This approach makes it possible to assess an individual's ability to maintain motor control while attention is divided, which more closely reflects the demands of real sporting activities. Yet, the impact of motor-cognitive interference can be quantified using Dual-Task Cost (DTC) (80).
Separate DTC values for motor and cognitive domains help identify which system is compromised and how task prioritization may influence performance.
Incorporating motor-cognitive testing and analyzing task prioritization strategies during RTS evaluation after LAS provides a more ecologically valid measure of functional recovery. These assessments can reveal persistent deficits in neuromotor control or cognitive flexibility that traditional tests miss. Ultimately, a dual-task framework enhances the clinician's ability to make informed, individualized RTS decisions that reduce reinjury risk and support long-term athletic performance. These aspects will be largely discussed in the part 2 of this article (Targeting Visual-Sensory and Cognitive Impairments Following Lateral Ankle Sprains: A Practical Framework for Functional Assessment Across the Return-to-Sport Continuum. Part 2: From theory to practice: recommendations for optimizing Return To Sport after lateral ankle sprains using cognitive and visual-sensory assessments, Frontiers in Sports and Active Living, [under review]).
4.1 Clinical implications for rehabilitation
Athletes recovering from CAI often revert to novice-like motor patterns, necessitating the relearning of previously automatic skills. This regression stems from the adoption of maladaptive movement strategies that increase reliance on cognitive resources and visual input, thereby reducing motor efficiency. Due to compromised sensorimotor pathways, these individuals typically engage in more conscious control of movement, which places greater demands on attentional capacity and slows reaction time. Athletes with CAI may exhibit increased attention directed toward their injured ankle, as they consciously monitor movement patterns and joint stability (81–83). This self-attentional focus is further reinforced during rehabilitation, when rehabilitation specialists frequently provide internal focus instructions—directing the athlete's attention to specific body mechanics, such as knee alignment or muscle activation (84). These cues may inadvertently contribute to excessive cognitive load. This adaptation reduces cognitive resources available for other tasks (85, 86). To restore automaticity, an external focus of attention—such as concentrating on the outcome of movement rather than its mechanics—can help free up cognitive resources. This shift enables enhanced cerebellar involvement in sensorimotor control, fostering improved internal modeling for predictive adjustments and real-time motor corrections.
According to Gibson's ecological theory of perception, movement and sensory information are inherently linked in a continuous feedback loop (87). Movement generates sensory information by interacting with the environment, while sensory input, in turn, guides and refines movement. This bidirectional relationship allows individuals to adapt their actions based on real-time environmental cues. In the context of sports, athletes rely on this dynamic interplay to adjust their positioning, timing, and force production in response to rapidly changing game conditions. This interplay between movement and sensory information highlights the need for rehabilitation programs that incorporate enriched environments to facilitate optimal recovery. By exposing patients to practice variability and/or different situational conditions, they can actively explore and refine movement patterns in response to real-time sensory input.
This framework applies particularly to athletic populations of patients with LAS/CAI, especially those who participate in sports involving dual tasks or risky movements, such as jumping, landing, and cutting movement. It also applies to athletes whose vision is focused on managing their environment (movements and positioning of opponents and teammates) or tracking the trajectory of a ball, for example.
A recent meta-analysis reveals that dual-task training may be effective in improving static and dynamic postural stability among CAI patients but confirms the need for more high-quality studies to confirm the short and long-term effectiveness (43). This applies regardless of age, level of practice or severity of injury. It also seems important to introduce dual-task situations and neurocognitive exercises, as well as assessments targeting these elements, with the aim of primary injury prevention among these athletes.
In the second part of this topic (Targeting Visual-Sensory and Cognitive Impairments Following Lateral Ankle Sprains: A Practical Framework for Functional Assessment Across the Return-to-Sport Continuum. Part 2: From theory to practice: recommendations for optimizing Return To Sport after lateral ankle sprains using cognitive and visual-sensory assessments, Frontiers in Sports and Active Living, [under review]), we will propose a “β(rain)” extension of the Ankle-GO™ score that could help clinicians to target sensory-visual and cognitive deficits among patients following LAS in the RTS continuum.
5 Conclusion
LAS are not solely peripheral injuries but lead to neuroplastic changes affecting sensory integration and cognition. These central alterations can undermine traditional rehabilitation and RTS decision-making. Unfortunately, objective RTS criteria are lacking and the only predictive tool currently available does not include visual perturbation or cognitive constraints. We encourage the International Ankle Consortium (IAC) to promote the inclusion of tools that assess central function in future consensus statements on decision-making regarding return to sport. Clinicians must adopt a neuromotor and neurocognitive approach to fully restore athletic function and reduce recurrence risk.
Author contributions
BP: Conceptualization, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AM: Validation, Writing – original draft, Writing – review & editing. FF: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing. AG: Writing – original draft, Writing – review & editing. BT: Writing – original draft, Writing – review & editing. RL: Writing – original draft, Writing – review & editing. AH: Resources, Supervision, Writing – original draft, Writing – review & editing, Funding acquisition.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fong DT-P, Hong Y, Chan L-K, Yung PS-H, Chan K-M. A systematic review on ankle injury and ankle sprain in sports. Sports Med. (2007) 37:73–94. doi: 10.2165/00007256-200737010-00006
2. Gribble PA, Bleakley CM, Caulfield BM, Docherty CL, Fourchet F, Fong DT-P, et al. 2016 Consensus statement of the international ankle consortium: prevalence, impact and long-term consequences of lateral ankle sprains. Br J Sports Med. (2016) 50:1493–5. doi: 10.1136/bjsports-2016-096188
3. Gribble PA, Delahunt E, Bleakley C, Caulfield B, Docherty C, Fourchet F, et al. Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the international ankle consortium. Br J Sports Med. (2014) 48:1014–8. doi: 10.1136/bjsports-2013-093175
4. Hertel J, Corbett RO. An updated model of chronic ankle instability. J Athl Train. (2019) 54:572–88. doi: 10.4085/1062-6050-344-18
5. Hong CC, Calder J. The burden of the “Simple Ankle Sprains”: a review of the epidemiology and long-term impact. Foot ankle clin. Complex Involving Ankle Sprain. (2023) 28:187–200. doi: 10.1016/j.fcl.2022.12.002
6. Xue X, Ma T, Li Q, Song Y, Hua Y. Chronic ankle instability is associated with proprioception deficits: a systematic review and meta-analysis. J Sport Health Sci. (2021) 10:182–91. doi: 10.1016/j.jshs.2020.09.014
7. Kim H, Son SJ, Seeley MK, Hopkins JT. Altered movement biomechanics in chronic ankle instability, coper, and control groups: energy absorption and distribution implications. J Athl Train. (2019) 54:708–17. doi: 10.4085/1062-6050-483-17
8. Kim H, Son SJ, Seeley MK, Hopkins JT. Kinetic compensations due to chronic ankle instability during landing and jumping. Med Sci Sports Exerc. (2018) 50:308–17. doi: 10.1249/MSS.0000000000001442
9. Maricot A, Dick E, Walravens A, Pluym B, Lathouwers E, De Pauw K, et al. Brain neuroplasticity related to lateral ankle ligamentous injuries: a systematic review. Sports Med. (2023) 53:1423–43. doi: 10.1007/s40279-023-01834-z
10. Burcal CJ, Needle AR, Custer L, Rosen AB. The effects of cognitive loading on motor behavior in injured individuals: a systematic review. Sports Med. (2019) 49:1233–53. doi: 10.1007/s40279-019-01116-7
11. Sagnard T, Picot B, Forestier N. Proprioceptive acuity, proprioceptive weighting and balance in individuals with chronic ankle instability. Gait Posture. (2025) 119:178–84. doi: 10.1016/j.gaitpost.2025.03.006
12. Sugimoto YA, McKeon PO, Rhea CK, Schmitz RJ, Henson R, Mattacola CG, et al. Sensory reweighting system differences on vestibular feedback with increased task constraints in individuals with and without chronic ankle instability. J Athl Train. (2024) 59:713–23. doi: 10.4085/1062-6050-0246.22
13. Xue X, Zheng S, Wang Z, Chen Y, Chang L, Wang Z, et al. Sensory reweighting revealed by superior parietal Cortex-based functional connectivity in chronic ankle instability: a resting-state fMRI study. Med Sci Sports Exerc. (2025) 57:2216–2226. doi: 10.1249/MSS.0000000000003762
14. Kim K-M. Higher visual reliance during single-leg balance bilaterally occurring following acute lateral ankle sprain: a potential central mechanism of bilateral sensorimotor deficits. Gait Posture. (2020) 78:26–9. doi: 10.1016/j.gaitpost.2020.03.003
15. Song K, Burcal CJ, Hertel J, Wikstrom EA. Increased visual use in chronic ankle instability: a meta-analysis. Med Sci Sports Exerc. (2016) 48:2046–56. doi: 10.1249/MSS.0000000000000992
16. Wikstrom EA, Mueller C, Cain MS. Lack of consensus on return-to-sport criteria following lateral ankle sprain: a systematic review of expert opinions. J Sport Rehabil. (2020) 29:231–7. doi: 10.1123/jsr.2019-0038
17. Kandel ER, Schwartz JH, Jessell TM, Siegelbaum SA, Hudspeth AJ. Principles of Neural Science. 5th ed. Columbus, OH: McGraw Hill Professional (2012).
18. Nachev P, Kennard C, Husain M. Functional role of the supplementary and pre-supplementary motor areas. Nat Rev Neurosci. (2008) 9:856–69. doi: 10.1038/nrn2478
19. Hikosaka O, Takikawa Y, Kawagoe R. Role of the basal ganglia in the control of purposive saccadic eye movements. Physiol Rev. (2000) 80:953–78. doi: 10.1152/physrev.2000.80.3.953
20. Manto M, Bower JM, Conforto AB, Delgado-García JM, da Guarda SNF, Gerwig M, et al. Consensus paper: roles of the cerebellum in motor control—the diversity of ideas on cerebellar involvement in movement. Cerebellum. (2012) 11:457–87. doi: 10.1007/s12311-011-0331-9
21. Peterka RJ. Chapter 2 - sensory integration for human balance control. In: Day BL, Lord SR, editors. Handbook of Clinical Neurology, Balance, Gait, and Falls. Amsterdam: Elsevier (2018). p. 27–42. doi: 10.1016/B978-0-444-63916-5.00002-1
22. Diamond A. Executive functions. Annu Rev Psychol. (2013) 64:135–68. doi: 10.1146/annurev-psych-113011-143750
23. Baddeley AD, Hitch G. Working memory. In: Bower GH, editor. Psychology of Learning and Motivation. New York, NY: Academic Press (1974). p. 47–89. doi: 10.1016/S0079-7421(08)60452-1
24. Herold F, Hamacher D, Schega L, Müller NG. Thinking while moving or moving while thinking – concepts of motor-cognitive training for cognitive performance enhancement. Front. Aging Neurosci. (2018) 10:228. doi: 10.3389/fnagi.2018.00228
25. Voss MW, Kramer AF, Basak C, Prakash RS, Roberts B. Are expert athletes ‘expert’ in the cognitive laboratory? A meta-analytic review of cognition and sport expertise. Appl Cogn Psychol. (2010) 24:812–26. doi: 10.1002/acp.1588
26. Broadbent DP, Causer J, Williams AM, Ford PR. Perceptual-cognitive skill training and its transfer to expert performance in the field: future research directions. Eur J Sport Sci. (2015) 15:322–31. doi: 10.1080/17461391.2014.957727
27. Assländer L., Peterka R.J., 2016. Sensory reweighting dynamics following removal and addition of visual and proprioceptive cues. J Neurophysiol 116, 272–85. doi: 10.1152/jn.01145.2015
28. Horak FB. Postural orientation and equilibrium: what do we need to know about neural control of balance to prevent falls? Age Ageing. (2006) 35(2):ii7–ii11. doi: 10.1093/ageing/afl077
29. Peterka RJ, Loughlin PJ. Dynamic regulation of sensorimotor integration in human postural control. J. Neurophysiol. (2004) 91:410–23. doi: 10.1152/jn.00516.2003
30. Kim KS, Kim J-S, Grooms DR. Stroboscopic vision to induce sensory reweighting during postural control. J Sport Rehabil. (2017) 26. doi: 10.1123/jsr.2017-0035
31. König P, Kühnberger K-U, Kietzmann TC. A unifying approach to high- and low-level cognition. In: Gähde U, Hartmann S, Wolf JH, editors. Models, Simulations, and the Reduction of Complexity. Berlin: De Gruyter (2013). p. 117–40. doi: 10.1515/9783110313680.117/pdf
32. Rosen AB, McGrath ML, Maerlender AL. Males with chronic ankle instability demonstrate deficits in neurocognitive function compared to control and copers. Res Sports Med. (2021) 29:116–28. doi: 10.1080/15438627.2020.1723099
33. Dury J, Sagawa Y, Michel F, Ravier G. Neuromuscular fatigue and cognitive constraints independently modify lower extremity landing biomechanics in healthy and chronic ankle instability individuals. J Sports Sci. (2024) 42:1341–54. doi: 10.1080/02640414.2024.2391209
34. Peri M, Gottlieb U, Finestone AS, Springer S. Does acute exercise stress affect postural stability and cognitive function in subjects with chronic ankle instability? Brain Sci. (2021) 11:788. doi: 10.3390/brainsci11060788
35. Bain KA, Baez S, Kosik KB, Hoch MC, Hoch JM, Johnson NF, et al. The relationship between health-related quality of life and lower-extremity visuomotor reaction time in young adult women following ankle sprain. J Sport Rehabil. (2023) 32:433–9. doi: 10.1123/jsr.2022-0199
36. Choi JY, Vogel C, Burcal CJ, Remski LE, Knarr BA, Rosen AB. Neurocognitive hop performance in patients with chronic ankle instability. Int J Athl Ther Train. (2023) 29:101–5. doi: 10.1123/ijatt.2023-0045
37. Mohammadi N, Hadian MR, Olyaei G. Information processing speed and accuracy in basketball players with and without functional ankle instability. J Mod Rehabil. (2019) 13:179–84. doi: 10.32598/JMR.13.3.179
38. Song K, Hoch JM, Quintana C, Heebner NR, Hoch MC. Slower visuomotor reaction time in division-I collegiate athletes with a history of ankle sprain. Res Sports Med. (2023) 31:473–81. doi: 10.1080/15438627.2021.1996361
39. Choi JY, Yoo T, Burcal CJ, Rosen AB. Dual-task differences in individuals with chronic ankle instability: a systematic review with meta-analysis. Gait Posture. (2023) 106:28–33. doi: 10.1016/j.gaitpost.2023.08.013
40. Hung Y, Miller J. Extrinsic visual feedback and additional cognitive/physical demands affect single-limb balance control in individuals with ankle instability. World J Orthop. (2016) 7:801–7. doi: 10.5312/wjo.v7.i12.801
41. Rahnama L, Salavati M, Akhbari B, Mazaheri M. Attentional demands and postural control in athletes with and without functional ankle instability. J Orthop Sports Phys Ther. (2010) 40:180–7. doi: 10.2519/jospt.2010.3188
42. Tavakoli S, Forghany S, Nester C. The effect of dual tasking on foot kinematics in people with functional ankle instability. Gait Posture. (2016) 49:364–70. doi: 10.1016/j.gaitpost.2016.07.302
43. Wang L, Yu G, Chen Y. Effects of dual-task training on chronic ankle instability: a systematic review and meta-analysis. BMC Musculoskelet Disord. (2023) 24:814. doi: 10.1186/s12891-023-06944-3
44. Zhong C, Luo X, Gao H, Zhang T, Zhu X, Huang X, et al. Effects of dual-task paradigm on the injury potential during landing among individuals with chronic ankle instability. Front Physiol. (2024) 15:1473844. doi: 10.3389/fphys.2024.1473844
45. Shiravi Z, Talebian Moghadam S, Hadian MR, Olyaei G. Effect of cognitive task on postural control of the patients with chronic ankle instability during single and double leg standing. J Bodyw Mov Ther. (2017) 21:58–62. doi: 10.1016/j.jbmt.2016.05.001
46. Springer S, Gottlieb U. Effects of dual-task and walking speed on gait variability in people with chronic ankle instability: a cross-sectional study. BMC Musculoskelet Disord. (2017) 18:316. doi: 10.1186/s12891-017-1675-1
47. Maricot A, Corlùy H, De Pauw K, Lathouwers E, Meeusen R, Roelands B, et al. Deficits in neurocognitive performance in patients with chronic ankle instability during a neurocognitive balance task – A retrospective case-control study. Phys Ther Sport. (2024) 66:1–8. doi: 10.1016/j.ptsp.2023.12.009
48. Mohamadi S, Ebrahimi I, Salavati M, Dadgoo M, Jafarpisheh AS, Rezaeian ZS. Attentional demands of postural control in chronic ankle instability, copers and healthy controls: a controlled cross-sectional study. Gait Posture. (2020) 79:183–8. doi: 10.1016/j.gaitpost.2020.03.007
49. Xue X, Chen Z, Xuan W, Tao W, Jin Z, Hua Y. Force sense deficits in chronic ankle instability: a systematic review and meta-analysis. PM R. (2023) 15:780–9. doi: 10.1002/pmrj.12833
50. Freeman MA. Instability of the foot after injuries to the lateral ligament of the ankle. J Bone Joint Surg Br. (1965) 47:669–77. doi: 10.1302/0301-620X.47B4.669
51. McCann RS, Welch Bacon CE, Suttmiller AMB, Gribble PA, Cavallario JM. Assessments used by athletic trainers to decide return-to-activity readiness in patients with an ankle sprain. J Athl Train. (2024) 59:182–200. doi: 10.4085/1062-6050-0037.22
52. Tassignon B, Verschueren J, Delahunt E, Smith M, Vicenzino B, Verhagen E, et al. Criteria-based return to sport decision-making following lateral ankle sprain injury: a systematic review and narrative synthesis. Sports Med. (2019) 49:601–19. doi: 10.1007/s40279-019-01071-3
53. McKeon JMM, Bush HM, Reed A, Whittington A, Uhl TL, McKeon PO. Return-to-play probabilities following new versus recurrent ankle sprains in high school athletes. J Sci Med Sport. (2014) 17:23–8. doi: 10.1016/j.jsams.2013.04.006
54. Roos KG, Kerr ZY, Mauntel TC, Djoko A, Dompier TP, Wikstrom EA. The epidemiology of lateral ligament complex ankle sprains in national collegiate athletic association sports. Am J Sports Med. (2017) 45:201–9. doi: 10.1177/0363546516660980
55. Lam KC, Marshall AN, Bay RC, Wikstrom EA. Patient-reported outcomes at return to sport after lateral ankle sprain injuries: a report from the athletic training practice-based research network. J Athl Train. (2023) 58:627–34. doi: 10.4085/1062-6050-0111.22
56. McCann R, Kosik K, Terada M, Gribble P. Residual impairments and activity limitations at return to play from a lateral ankle sprain. Int J Athl Ther Train. (2018) 23:83–8. doi: 10.1123/ijatt.2017-0058
57. Smith MD, Vicenzino B, Bahr R, Bandholm T, Cooke R, Mendonça LDM, et al. Return to sport decisions after an acute lateral ankle sprain injury: introducing the PAASS framework-an international multidisciplinary consensus. Br J Sports Med. (2021):2021–104087. doi: 10.1136/bjsports-2021-104087
58. Picot B, Lopes R, Rauline G, Fourchet F, Hardy A. Development and validation of the ankle-GO score for discriminating and predicting return-to-sport outcomes after lateral ankle sprain. Sports Health. (2024) 16:47–57. doi: 10.1177/19417381231183647
59. Picot B, Hardy A, Terrier R, Tassignon B, Lopes R, Fourchet F. Which functional tests and self-reported questionnaires can help clinicians make valid return to sport decisions in patients with chronic ankle instability? A narrative review and expert opinion. Front Sports Act Living. (2022) 4:902886. doi: 10.3389/fspor.2022.902886
60. Picot B, Fourchet F, Lopes R, Rauline G, Freiha K, D’hooghe P, et al. Low ankle-GO score while returning to sport after lateral ankle sprain leads to a 9-fold increased risk of recurrence: a two-year prospective cohort study. Sports Med Open. (2024) 10:23. doi: 10.1186/s40798-024-00693-w
61. Picot B, Fourchet F, Rauline G, Freiha K, Wikstrom E, Lopes R, et al. Ankle-GO score is associated with the probability of becoming coper after lateral ankle sprain: a 1-year prospective cohort study. Br J Sports Med. (2024) 58(19):1115–22. doi: 10.1136/bjsports-2024-108361
62. Picot B, Grimaud O, Rauline G, Haidar I, Moussa MK, Hardy A. Validity and reproducibility of the ARL-RSI score to assess psychological readiness before returning to sport after lateral ankle sprain. J Exp Orthop. (2024) 11:e12073. doi: 10.1002/jeo2.12073
63. Pioger C, Guillo S, Bouché P-A, Sigonney F, Elkaïm M, Bauer T, et al. The ALR-RSI score is a valid and reproducible scale to assess psychological readiness before returning to sport after modified Broström-Gould procedure. Knee Surg Sports Traumatol Arthrosc. (2022) 30(7):2470–5. doi: 10.1007/s00167-022-06895-7
64. Sigonney F, Lopes R, Bouché P-A, Kierszbaum E, Moslemi A, Anract P, et al. The ankle ligament reconstruction-return to sport after injury (ALR-RSI) is a valid and reproducible scale to quantify psychological readiness before returning to sport after ankle ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. (2020) 28:4003–10. doi: 10.1007/s00167-020-06020-6
65. Wang Y, Hinz M, Buchalter WH, Drumm AH, Eren E, Thomas Haytmanek C, et al. Ankle ligament reconstruction-return to sport after injury scale and return to sports after ankle ligament reconstruction or repair-A systematic review. J Exp Orthop. (2024) 11:e12077. doi: 10.1002/jeo2.12077
66. Martin RL, Irrgang JJ, Burdett RG, Conti SF, Van Swearingen JM. Evidence of validity for the foot and ankle ability measure (FAAM). Foot Ankle Int. (2005) 26:968–83. doi: 10.1177/107110070502601113
67. Carcia CR, Martin RL, Drouin JM. Validity of the foot and ankle ability measure in athletes with chronic ankle instability. J Athl Train. (2008) 43:179–83. doi: 10.4085/1062-6050-43.2.179
68. Linens SW, Ross SE, Arnold BL, Gayle R, Pidcoe P. Postural-stability tests that identify individuals with chronic ankle instability. J Athl Train. (2014) 49:15–23. doi: 10.4085/1062-6050-48.6.09
69. Riemann B, Caggiano A, M N, Lephart S. Examination of a clinical method of assessing postural control during a functional performance task. J Sport Rehabil. (1999) 8:171–83. doi: 10.1123/jsr.8.3.171
70. Gribble PA, Hertel J, Plisky P. Using the star excursion balance test to assess dynamic postural-control deficits and outcomes in lower extremity injury: a literature and systematic review. J Athl Train. (2012) 47:339–57. doi: 10.4085/1062-6050-47.3.08
71. Picot B, Terrier R, Forestier N, Fourchet F, McKeon PO. The star excursion balance test: an update review and practical guidelines. Int J Athl Ther Train. (2021) 1:1–9. doi: 10.1123/ijatt.2020-0106
72. Butler RJ, Lehr ME, Fink ML, Kiesel KB, Plisky PJ. Dynamic balance performance and noncontact lower extremity injury in college football players: an initial study. Sports Health. (2013) 5:417–22. doi: 10.1177/1941738113498703
73. Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star excursion balance test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther. (2006) 36:911–9. doi: 10.2519/jospt.2006.2244
74. Caffrey E, Docherty CL, Schrader J, Klossnner J. The ability of 4 single-limb hopping tests to detect functional performance deficits in individuals with functional ankle instability. J Orthop Sports Phys Ther. (2009) 39:799–806. doi: 10.2519/jospt.2009.3042
75. Docherty CL, Arnold BL, Gansneder BM, Hurwitz S, Gieck J. Functional-performance deficits in volunteers with functional ankle instability. J Athl Train. (2005) 40:30–4. PMCID: PMC1088342
76. Hardy A, Freiha K, Moussa MK, Valentin E, Rauline G, Alvino K, et al. Use of ankle-GO to assess and predict return to sport after lateral ankle reconstruction for chronic ankle instability. Orthop J Sports Med. (2025) 13:23259671251322903. doi: 10.1177/23259671251322903
77. Rosen AB, Choi JY, Anderson K, Remski LE, Knarr BA. Development, validity, and test-retest reliability of a new neurocognitive functional performance test: the choice-reaction hop test. Phys Ther Sport. (2023) 59:80–4. doi: 10.1016/j.ptsp.2022.12.003
78. Miao Y, Ge Y, Wang D, Mao D, Song Q, Wu R. Effects of visual disruption on static and dynamic postural control in people with and without chronic ankle instability. Front Bioeng Biotechnol. (2024) 12:1499684. doi: 10.3389/fbioe.2024.1499684
79. Mohammadi-Rad S, Salavati M, Ebrahimi-Takamjani I, Akhbari B, Sherafat S, Negahban H, et al. Dual-tasking effects on dynamic postural stability in athletes with and without anterior cruciate ligament reconstruction. J Sport Rehabil. (2016) 25:324–9. doi: 10.1123/jsr.2015-0012
80. Veldkamp R, Romberg A, Hämäläinen P, Giffroy X, Moumdjian L, Leone C, et al. Test-retest reliability of cognitive-motor interference assessments in walking with Various task complexities in persons with multiple sclerosis. Neurorehabil Neural Repair. (2019) 33:623–34. doi: 10.1177/1545968319856897
81. Gray R. Differences in attentional focus associated with recovery from sports injury: does injury induce an internal focus? J Sport Exerc Psychol. (2015) 37:607–16. doi: 10.1123/jsep.2015-0156
82. Grooms D, Appelbaum G, Onate J. Neuroplasticity following anterior cruciate ligament injury: a framework for visual-motor training approaches in rehabilitation. J Orthop Sports Phys Ther. (2015) 45:381–93. doi: 10.2519/jospt.2015.5549
83. Han S, Lee H, Son SJ, Hopkins JT. The effects of visual feedback disruption on postural control with chronic ankle instability. J Sci Med Sport. (2022) 25:53–7. doi: 10.1016/j.jsams.2021.07.014
84. Risberg MA, Holm I. The long-term effect of 2 postoperative rehabilitation programs after anterior cruciate ligament reconstruction: a randomized controlled clinical trial with 2 years of follow-up. Am J Sports Med. (2009) 37:1958–66. doi: 10.1177/0363546509335196
85. Gokeler A, Neuhaus D, Benjaminse A, Grooms DR, Baumeister J. Principles of motor learning to support neuroplasticity after ACL injury: implications for optimizing performance and reducing risk of second ACL injury. Sports Med. (2019) 49:853–65. doi: 10.1007/s40279-019-01058-0
86. Grooms DR, Page SJ, Nichols-Larsen DS, Chaudhari AMW, White SE, Onate JA. Neuroplasticity associated with anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. (2017) 47(3):180–9. doi: 10.2519/jospt.2017.7003
Keywords: lateral ankle sprains, chronic instability, cognition, sensory reweighting, return to sport
Citation: Picot B, Maricot A, Fourchet F, Gokeler A, Tassignon B, Lopes R and Hardy A (2025) Targeting visual-sensory and cognitive impairments following lateral ankle sprains: a practical framework for functional assessment across the return-to-sport continuum—Part 1. Sensory reweighting and cognitive impairments: what are we really talking about and why clinicians should consider central alterations in return to sport criteria. Front. Sports Act. Living 7:1668224. doi: 10.3389/fspor.2025.1668224
Received: 17 July 2025; Accepted: 1 October 2025;
Published: 23 October 2025.
Edited by:
Jia Han, Shanghai University of Medicine and Health Sciences, ChinaCopyright: © 2025 Picot, Maricot, Fourchet, Gokeler, Tassignon, Lopes and Hardy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Brice Picot, YnJpY2UucGljb3RAdW5pdi1zbWIuZnI=