 Emilia Pietiläinen
Emilia Pietiläinen Heikki Kyröläinen
Heikki Kyröläinen Kai Parkkola
Kai Parkkola Tiina Luukkaala5,6
Tiina Luukkaala5,6 Tommi Vasankari
Tommi Vasankari- 1Faculty of Medicine and Health Technology, Tampere University, Tampere, Finland
- 2Center for Military Medicine, Helsinki, Finland
- 3Faculty of Sport and Health Sciences, University of Jyväskylä, Jyväskylä, Finland
- 4Department of Leadership and Military Pedagogy, National Defence University, Helsinki, Finland
- 5Health Sciences, Faculty of Social Sciences, Tampere University, Tampere, Finland
- 6Research, Development and Innovation Center, Tampere University Hospital, Tampere, Finland
- 7UKK institute for Health Promotion Research, Tampere, Finland
Introduction: The primary objectives of the present individualized randomized controlled trial were to increase physical activity (PA) and improve physical fitness.
Materials and methods: 260 military employees around Finland participated. Two-thirds, (158), were randomized in the intervention and one-third, (101), in the control group. The intervention group used Exsed Movesense accelerometers linked to smartphones measuring PA and sleep for six months. They received feedback via a smartphone application, were encouraged to exercise during worktime for 2 hours/week, and participated in telephone counseling. The control group continued PA routines without the accelerometer or feedback. Measurements were taken at the baseline, 6-mo and 12-mo after the intervention. They included two-week RM 42-accelerometer measurements of PA, cardiometabolic biomarkers, body composition, physical fitness tests, and a questionnaire about stress and work ability for the intervention group at every point and for the control group at baseline and 12-mo. At the 6-mo, only PA was measured in the control group. Primary outcomes were changes in PA from baseline to 6-mo and 12-mo as well as changes in maximal oxygen uptake and fitness index from baseline to 12-mo. Secondary outcomes were changes in other parameters from baseline to 12-mo. The effect of the intervention on primary and secondary outcomes was analyzed using unadjusted generalised linear mixed model, accounting for a group-by-time interaction effect in all models.
Results: There was no statistically significant group-by-time interaction regarding the measured parameters. However, amount the intervention group daily standing time (mean increase 18 min/day, 95% confidence interval [CI] 6–29 min/day) and maximal oxygen uptake (mean increase 2.15 ml/kg/min 95% CI 0.56–3.74 ml/kg/min) tended to increase during twelve months.
Discussion: The intervention did not effectively change the primary outcomes, but showed encouraging trends and revealed the potential and challenges of the intervention developed to increase PA in a military workplace.
1 Introduction
Physical fitness and health are important aspects of performance and work ability (1–5). Physical activity (PA) improves physical fitness (4) and has a beneficial impact on cardiometabolic health (6–8) by improving glucose and lipid metabolism as well as reducing blood pressure (6–8). Optimal performance at work is only possible if cardiometabolic risk factors are at their lowest levels related to the workload (1). While PA has been shown to improve cardiometabolic health (6–8), it has also been shown to have a positive effect on work ability (9) and relieve stress by physiological mechanisms and by enhancing self-esteem, self-efficacy, and onés predisposition for social interactions (10). Therefore, a physically active lifestyle plays an important role in maintaining the performance of the working-age population.
The performance and work ability of military workers play an essential role in national defence, while physical fitness and health are important aspects of it (11). Soldierś daily tasks require good physical and mental performance, and professional soldiers working in the Finnish Defence Forces are obliged, according to the law, to maintain good physical fitness to meet their work requirements. While civil tasks contain mostly office or logistics work, for civilian employees, maintaining good physical fitness is optional. Still, good physical performance can be required in demanding tasks and peacekeeping operations (12).
However, PA has declined among the working-age population around the world during the last decades (13, 14). Additionally, surveys and accelerometer measurements carried out among the working-age population in Finland revealed that the volume of endurance training is not sufficient to sustain the health and fitness of the population (15, 16). Objective data recorded using accelerometers show that 76% of the day is passive time, mostly spent sitting (16). These issues challenging health and performance are seen among military personnel as well. A wide survey performed among military workers in Finland showed that only 51% of its participants exercise regularly, at least three times a week (17). Added to this, studies performed among US and German soldiers have shown a decline in performance as well as an increase in body fat over the years (18, 19).
These findings, showing the increasing inactivity of the working-age population in general (13, 14, 16) as well as of military personnel (17–19), elicit a need for interventions aimed at large populations to promote PA and thereby health and work ability (6–9). Health behavior change interventions teach their participants techniques to facilitate behavior change. Self-monitoring in combination with at least one self-regulation technique, such as goal-setting and review, have been shown to be associated with PA intervention effectiveness (20). Promising results to motivate and thus to increase PA have been gained from previous studies using tools as accelerometers combined with online feedback and smartphone techniques in adolescents and adult civilians (21–25). Furthermore, intervention utilizing smartphone-linked accelerometers serves as an opportunity for precise prevention, while the concept enables tailored, constant online feedback on the physical activity of the participants (26). Additionally, interventions taking advantage of telephone counseling combined with self-monitoring, and enabling physical activity to be performed during working hours, have been shown their effect in increasing physical activity (22, 23, 27, 28). Yet, a limited number of studies have been published utilizing smartphone-linked accelerometers in randomized controlled studies to decrease sedentary behavior (SB) or increase PA (25, 29, 30). Further, the advantages of an intervention combining smartphone-linked accelerometers, telephone counseling, and encouragement to exercise during working hours have not been investigated before among military employees.
The present study is one of the first studies that investigates the effects of long-term PA guidance on levels of PA and SB using health technology. The participants wear accelerometers and are able to monitor their PA and SB online. These types of studies using self-monitoring and goal-setting to increase PA are so far rare. Additionally, the present study aims to give new insight into this field by investigating the effects of an intervention combining an interactive accelerometer with personalized online feedback on physical activity via a smartphone application, telephone counseling, and the possibility of exercising for two hours a week during working hours among military employees. The primary objectives of the developed intervention are to increase PA and physical fitness. Additionally, the secondary objectives are to improve body composition, cardiometabolic health status, reduce stress, and improve work ability among military employees. The hypothesis is that the intervention will increase daily PA; decrease SB; and improve physical fitness.
2 Materials and methods
2.1 Intervention protocol
Permission to perform our study was granted by the local ethics committee of the Tampere University Hospital (R16189) and Defence Command Finland (AN8355, 1367/12.04.01/2015; AN8355, 2055/09.05/2022). The six-month intervention and its subsequent six-month follow-up protocol, as well as the timeline of the measurements performed in different phases of the study, are illustrated in Table 1. The intervention group started their intervention six months after the baseline measurements. The intervention concentrating on PA lasted six months, during which time the intervention group participants wore an interactive accelerometer (ExSed Movesense, Suunto, Finland) that was linked to a smartphone application (ExSed, UKK, Terveyspalvelut Oy, Tampere, Finland) and, further, to a cloud service. The accelerometers were checked to function similarly before giving them to the intervention group participants. The participants received information on their accumulated daily PA, SB, standing, and quality of sleep via the smartphone application. The accelerometer was downloaded with ExSed algorithms with a mean amplitude deviation and angle for posture estimation that were developed and validated at the UKK Institute (Tampere, Finland) (31–33). The accelerometer was worn on the hip during waking hours and on the wrist during sleep. It transmitted the PA and sleep data to the ExSed application via Bluetooth. The application provided constant feedback on PAs (light PA [LPA], moderate-to-vigorous PA [MVPA]), steps, standing, as well as on the quality of sleep (total sleep time, restless sleep time, restful sleep time). The recorded data was transmitted and saved to a cloud service (34). The application set daily goals for PA for each day, which were in line with the national recommendations (35, 34). The personal guidance and feedback were transmitted as illustrative histograms (graphical columns that illustrated participantś activity and achievement of their daily goals). Participants could observe online the accumulation and sufficiency of their daily PA by monitoring the ExSed application whenever most convenient (34). After this six-month intervention period, the intervention group participants returned the accelerometers to the UKK institute.
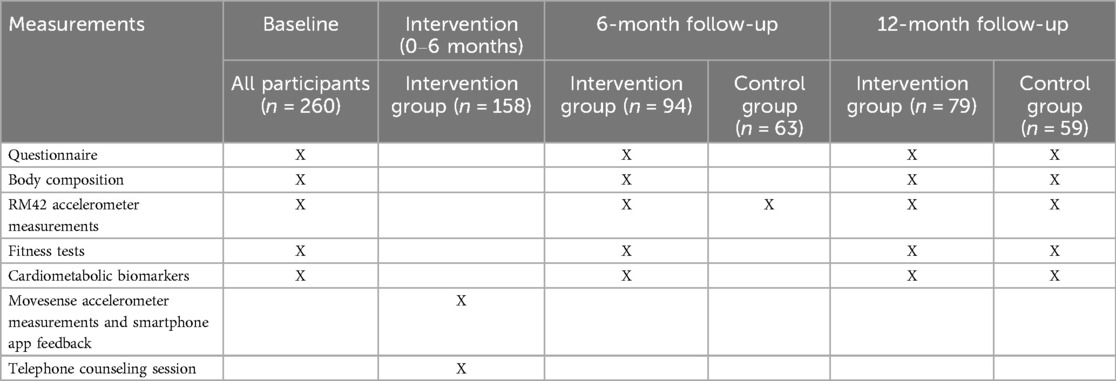
Table 1. The intervention protocol and the measurements performed in different phases of the study.
The intervention group participants also received telephone counseling about their PA and exercise habits once during the six-month intervention period. The counseling session could be scheduled earliest a month from the beginning of the intervention and, at the latest, a month before the end of the intervention. During the counseling session (lasting 10 minutes), the participants were interviewed about their PA habits and the factors hindering these habits. The physical education instructor gave individualized feedback to the participants and encouraged the participants to increase their PA and decrease their SB if the PA was not sufficient. If the participants’ PA was at a good level, they were encouraged to continue their exercise and PA routines as they had by far. The telephone counseling sessions were carried out by two physical education instructors and a research physician using a pre-planned interview sheet. Moreover, the participants of the intervention group were also encouraged to use the existing benefit to exercise for two hours a week during working hours from the beginning of the intervention.
The control group continued their normal exercise routines without an accelerometer or feedback, while the intervention was ongoing among the intervention group participants. This possibility to exercise during working hours is offered to all the employees working in the FDF under the existing FDF guidelines, therefore, the control group participants could use the possibility to exercise during working hours, but they were not separately encouraged to do so.
2.2 Sample size calculations
Before the intervention, the sample size was calculated using the participantś fitness indices. The calculations assumed that the fitness indices would increase by 0.14 for male soldiers; 0.45 for female soldiers; 0.34 for male civilian employees; and 0.24 for female civilian employees. For the evaluation of physical fitness, the appropriate number of study participants was approximately 175 soldiers and 99 civilian employees [G*Power 3.1.9.2, Wilcoxon signed-rank test (matched pairs), correlation between groups assumption r = 0.80] (36).
Drop-outs in different phases are presented in Figure 1. The reasons for dropping out included changing workplace to a new location, attending a crisis management mission, the loss of the accelerometer, the dysfunction of the accelerometer, personal reasons, the loss of motivation, health reasons, the lack of time, the long study duration, feeling uncomfortable using the accelerometer and not gaining any interesting information.

Figure 1. Dropout chart.
In the post hoc power analysis, the effect size was calculated using the means and standard deviations of PA and physical fitness test results at the twelve-month follow-up. Then, the mean and standard deviation of the fitness index would be 3.7 (SD 1.53) in the intervention group and 3.3 (SD 1.17) in the control group (Supplementary Table A), with an allocation ratio 2:1. The effect size would be d = 0.294 (small), and the sample size needed would be 275 participants in the intervention group and 137 participants in the control group (calculated using G*Power 3.1.9.7).
2.3 Randomization
After the baseline measurements, the participants were randomized into an intervention group and a control group using a randomization questionnaire. The intervention was implemented according to the intention-to-treat principle. Two-thirds of the participants were assigned to the intervention group and one-third to the control group. The randomization questionnaire asked for personal information to create homogenous groups according to age, gender, working status (civilian employee vs. soldier) and PA as during how many days a week they performed moderate-intensity physical activity (options were: 1 [“Not at all”], 2 [“Only light intensity physical activity at least on one day a week”], 3 [“Once a week”], 4 [“Twice a week”], 5 [“Three times a week”], 6 [“At least four times a week”]). The type of smartphone or other smart device that the participants used was asked about to confirm that the participants in the intervention group had a device that supported the application used in the intervention. The participants had an ID linked to their questionnaire information, which ensured that the results of the participant could not be identified with a certain individual. The data were expressed in numeric form: age (2 [ages 20–29], 3 [ages 30–39], 4 [ages 40–49], 5 [ages 50 and over]), gender (1 [man], 2 [woman]), and PA (1–6 according to the answer choice). The research physician gave the randomization questionnaires to the participants, collected the questionnaires, created their IDs, and exported the questionnaire information into the excel sheet. The results from the questionnaires, exported into the excel sheet, including participant IDs, were sent to the UKK institute and manually randomized by a separate researcher, ensuring during the process that the profile of both groups would appear similar. Finally, 158 of the participants were randomized to the intervention group and 101 to the control group.
2.4 Measurements
All participants were measured at three different time points during the study: at the baseline, after the intervention at the six-month follow-up, and at the twelve-month follow-up (six months from the end of the intervention). The performed measurements were similar for all participants at the baseline and twelve-month follow-up points, but only intervention group participants performed all the measurements at the six-month follow-up point. The control group participated only PA and SB measurements at six-month follow-up point. At the beginning of the study, all the participants participated in baseline measurements, which were carried out over a two-month period. The baseline measurements included measurements of PA with an RM42 accelerometer (UKK Terveyspalvelut Oy, Tampere, Finland) for two weeks, body composition measurements, blood samples for cardiometabolic biomarkers, fitness tests, and a questionnaire inquiring about experienced stress and working ability. The intervention group participants were measured again at the six-month and twelve-month follow-up points, as at the baseline. At the six-month follow-up point, the intervention had ended, and the intervention group had returned their Movesense accelerometers to the UKK institute. Between the six-month and twelve-month follow-up points, the intervention group continued their normal routines without the accelerometer or feedback.
At the six-month follow-up point, the control group only performed PA measurements using an RM42 accelerometer for two weeks to examine whether there were any changes in their PA as a result of participating in the study without participating in the intervention. The last measurements, to study the sustainability of the intervention, were performed at the twelve-month follow-up point and these measurements were the same as at the baseline for the control group participants, as they were for the intervention group participants.
The accelerometer (UKK RM42; UKK Terveyspalvelut Oy) measurements for two weeks were used to analyze the PA of the participants at the baseline, at the six-month follow-up, and at the twelve-month follow-up. The accelerometers were worn on a belt on the hip during waking hours. As the accelerometer is not water-resistant, it had to be taken off when showering and during water activities. After the two-week measurement period, the accelerometers were sent to the UKK Institute (Tampere, Finland), where the recorded data was analyzed. All participants received results and feedback from these accelerometer measurements from all time points only after the twelve-month follow-up measurements.
The device measured the acceleration in three orthogonal x, y, and z directions at a sampling rate of 100 Hz, and the resultant was established using these three components. Added to this, the mean amplitude deviation of the resultant was analyzed in 6 s epoch lengths (33). PA was categorized into light, moderate, and vigorous activity according to metabolic equivalents (METs). A resting metabolic rate of 1 MET corresponds to a 3.5 ml/kg/min oxygen consumption rate (32, 33). Time spent in a sitting and reclining position was considered as SB. SB has an energy expenditure of ≤1.5 MET, LPA has an energy expenditure of <3 MET, and MVPA has an energy expenditure of ≥3 MET. The oxygen cost of movement (ml/kg/min) was calculated for each stage as the ratio of measured oxygen consumption (ml/kg/min) to known speed (km/min) as described by Vähä-Ypyä et al. (32). Steps were identified using the magnitude of the horizontal component of the dynamic acceleration (37). Standing still could be separated from sitting or lying with 100% accuracy, and it was analyzed separately (32, 33, 31).
The daily step count, length of total LPA, MVPA, standing time, and SB were analyzed as well as accumulated PA bouts containing both LPA and MVPA, and stationary bouts. Stationary time was referred to as time spent lying, reclining, or sitting, while standing was analyzed separately (31, 38). The daily averages for total PA accumulated from bouts lasting 0–3 min, 3–10 min and longer than 10 min–as well as total stationary time accumulated from bouts lasting 0–20 min, 20–60 min and longer than 60 min–were also calculated for each participant. Participants having data of 10 hours from at least four days were included for further analyses. The group values were analyzed using the mean values for each participant.
The body composition of the participants was measured by using body mass, body height, body mass index (BMI), fat percentage (FAT%), and waist circumference. The measurements were performed in the morning after at least two hours of fasting. The segmental multifrequency bioimpedance analysis assessment (InBody 720, Biospace Co Ltd., Seoul, Korea) was used to measure body mass, BMI, and FAT%. A tape measure was used to measure the waist circumference in the midline between the lowest rib and iliac crest after exhaling.
Selected cardiometabolic biomarkers were used to evaluate the cardiometabolic health of the participants. The blood samples for the cardiometabolic biomarkers were collected after twelve hours of fasting. Serum fasting total cholesterol, low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), and triglycerides were analyzed to assess lipid metabolism. Fasting blood glucose (gluc), glycated hemoglobin (HbA1c), and insulin (INS) were analyzed to evaluate glucose metabolism.
HDL, triglycerides, gluc, and HbA1c were analyzed using a Konelab 20 XTi device (Thermo Electron Co., Vantaa, Finland), and an isolated LDL fraction was used for the direct measurement of LDL (the Enzymatic Colorimetric Determination of Serum Cholesterol method). The sensitivity for gluc and HbA1c are 0.1 mmol/L and 0.03 mmol/L, and the intra-assay coefficients of variance are 1.0% and 8.6% respectively. The ranges for the total cholesterol, triglyceride, HDL, and LDL assays vary from 0.1 to 15, from 0.09 to 11, from 0.04 to 2.84, and from 0.3 to 8.9 mmol/L, respectively. The intra-assay coefficients of variance are 1.1% for total cholesterol, 1.0% for triglycerides, 3.4% for LDL and 0.5% and for HDL. INS was analyzed using chemical luminescence techniques (Immulite 2000, Siemens Healthcare Diagnostics, Camberley, UK) with an assay sensitivity of 2 mIU/L and an inter-assay coefficient of variation of 5.1%.
Endurance and muscle fitness tests were used to evaluate the physical fitness of the participants. The endurance test assessed the aerobic capacity of the participants, and the participants performed a twelve-minute running test (39), or a cycle ergometer test (40), or a UKK 2-km walking test (41) as an endurance test. Every participant had to use the same test at every measurement point. Maximal oxygen uptake (VO2max) was used to express the maximal aerobic capacity. The muscle fitness test consisted of a maximal standing long jump (SLJ), evaluating the maximal power production of the lower extremities, as well as one minute of sit-ups, and one minute of push-ups, assessing the dynamic muscle endurance capacity of the trunk and upper extremities (42). According to the results of an endurance test and a muscle strength test, participantś endurance and muscle strength indices were determined using age-dependent reference values. The fitness index was calculated as an average of the endurance and muscle strength indices (12).
The work ability of the participants was analyzed with the statement and question “Work ability at the moment compared with work ability at its highest during onés career. It is assumed that your work ability gains 10 points at its highest. What score would you give your current work ability on a scale of 0–10 (a zero-score meaning “total inability to work”)?” The options ranged from 0 meaning the total inability to work, to 10, meaning work ability at its highest (43). This single question on work ability is widely used and validated in evaluating work ability. A high correlation has been detected between this single question on work ability and work ability index (44–46). Further, this single question on work ability has been shown to be as valid as the work ability index (47) in evaluating work ability of employees.
Experienced stress was evaluated with a statement and question from Occupational Stress Questionnaire “Stress is an emotional state where a person feels tense, restless, anxious, or nervous, and/or the person has difficulty sleeping because of troubling thoughts. Are you experiencing this kind of stress at the moment?” The answering options were 1 (“Not at all”), 2 (“I'm only experiencing this a little”), 3 (“I'm experiencing this somewhat”, 4 (“I'm experiencing this rather a lot”) and 5 (“I'm experiencing this a lot”) (48). The Occupational Stress Questionnaire is a widely used method in occupational health to assess characteristics and stress factors of work and stress reactions of employees in Finnish companies (49, 50). The questionnaire has been investigated in several research projects of the Finnish Institute of Occupational Health since 1977 (49). The validity of the stress question has been studied, and there is an association between psychological symptoms and mental resources (51).
2.5 Primary and secondary outcomes
The primary outcomes of the study were differences between the groups in changes in PA measured with the RM42 accelerometer from baseline to six-month and twelve-month follow-ups, as well as differences between the groups in changes in physical fitness from baseline to twelve-month follow-up. More specifically, these included MVPA, LPA, SB, standing, and daily step count from baseline to six- and twelve-month follow-ups, as well as changes in VO2max and fitness index from baseline to twelve-month follow-up.
Secondary outcomes of the study were differences between the groups in changes in body composition, cardiometabolic biomarkers, muscular fitness test results, experienced stress, and work ability from baseline to the twelve-month follow-up. These included changes in BMI, FAT%, waist circumference, total cholesterol, HDL, LDL, triglycerides, HbA1c, gluc, INS, push-ups, sit-ups, and SLJ from baseline to twelve-month follow-up. Further, secondary outcomes included differences between the groups in changes in PA accumulated from bouts lasting 0–3 min, 3–10 min, and longer than 10 min, as well as stationary time accumulated from bouts lasting 0–20 min, 20–60 min and longer than 60 min from baseline to the six-month- and twelve-month follow-ups (36).
2.6 Statistical analyses
Parameters of PA, body composition, cardiometabolic biomarkers, fitness test results, experienced stress, and work ability are described by mean with 95% confidence interval for mean. Two-sided p-values under 0.05 were considered as statistically significant. Statistical analyses were carried out with SPSS statistical software (SPSS, IBM, Armonk, New York, USA) versions 29.0.1.0. Unadjusted effects of the changes in the measured parameters were modelled as normally distributed, distributed over time (baseline, six-, and twelve- months) using Generalized Linear Mixed Models. Group-by-time interaction effect was included in all models. Participants created potential sources of variation, and therefore, this subject-specific effect was included as a random effect in the model (52). Explanatory factors were modelled as fixed effects. The Generalized Linear Mixed Model was applied with the R statistical software package (version 4.4.2, Ime4 function, R Core Team [2024]. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/).
3 Results
3.1 Participants
Participants were recruited from six military brigades around Finland by the research physician with help from brigadeś physical education officers. They were soldiers and civilian employees working in the Finnish Defence Forces (FDF). The participants had to be aged between 19 and 60 years old and eligible to perform the annual fitness tests of the FDF. An occupational physician determined if the health of the participant allowed her or him to perform the fitness tests (36). The participants were given information about the study, and they gave their written informed consent to participate.
Altogether, 260 military employees participated in the study. Characteristics of the participants are presented in Table 2. Altogether 108 (68%) of the 158 participants in the intervention group were soldiers, and 113 (72%) were men. In the control group, 77 (76%) of the participants were soldiers, and 81 (80%) were men.
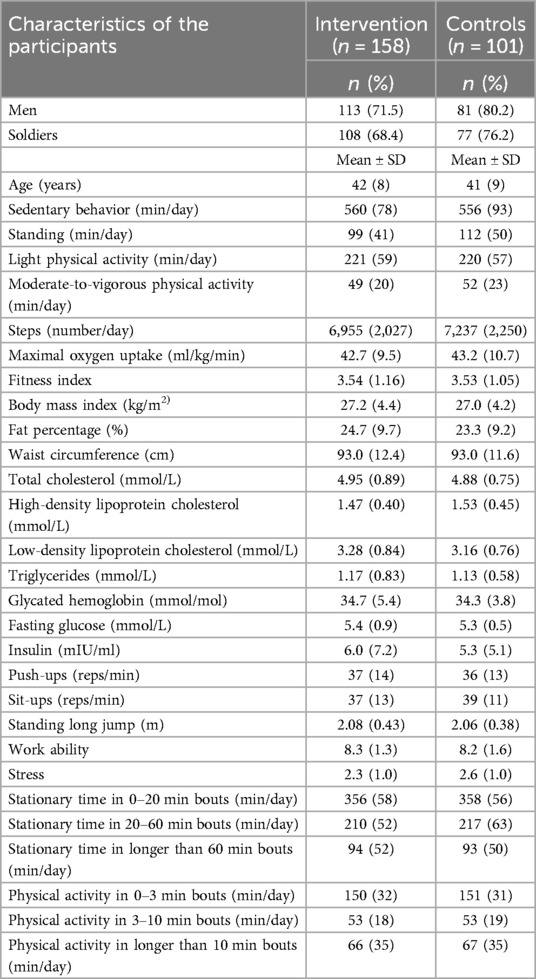
Table 2. Characteristics of the intervention and control group participants.
3.2 Physical activity (PA)
Changes in the PA measurements during the one-year follow-up are presented in Table 3. There was no statistically significant group-by-time interaction in the PA parameters. Only the standing time tended to increase (mean increase 18, 95% CI 6–29 min/day) among the intervention group participants during the twelve-month follow-up compared to the control group participants (mean decrease −4 95% CI −23–15 min/day), among whom the standing time decreased.
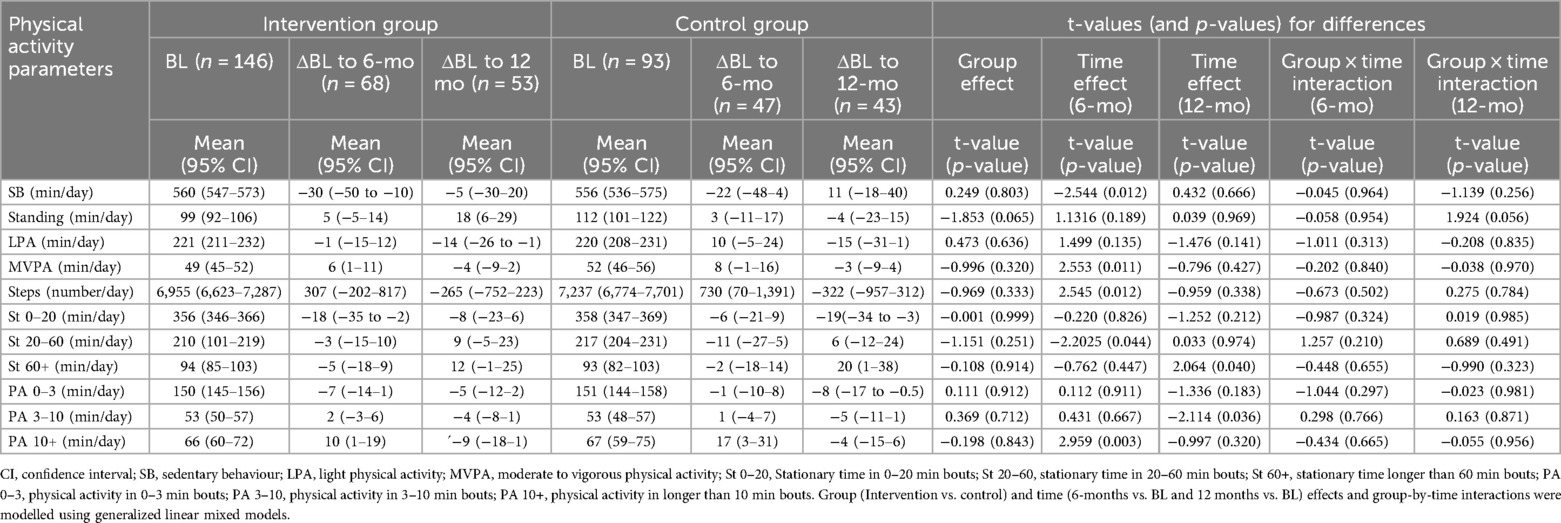
Table 3. Changes (Δ) in physical activity in measurements from baseline (BL) to six-month and twelve-month (mo) follow-ups.
SB decreased in the intervention group during the follow-up, but not in the control group. The overall effect of stationary time accumulated from bouts lasting 0–20 minutes and PA accumulated from bouts lasting 0–3 min/day was decreasing in both groups. The direction of other PA parameters varied during follow-up.
3.3 Body composition
Changes in body composition during the one-year follow-up are presented in Table 4. There was no group-by-time interaction in body composition between the intervention and control groups during the twelve-month follow-up. When observing changes in body composition over time, FAT% decreased from the baseline to the end of follow-up in both groups. Both BMI and waist circumference decreased in the intervention group but increased in the control group, but still without a statistically significant interaction effect. The magnitude of these changes is described in detail in Table 4.
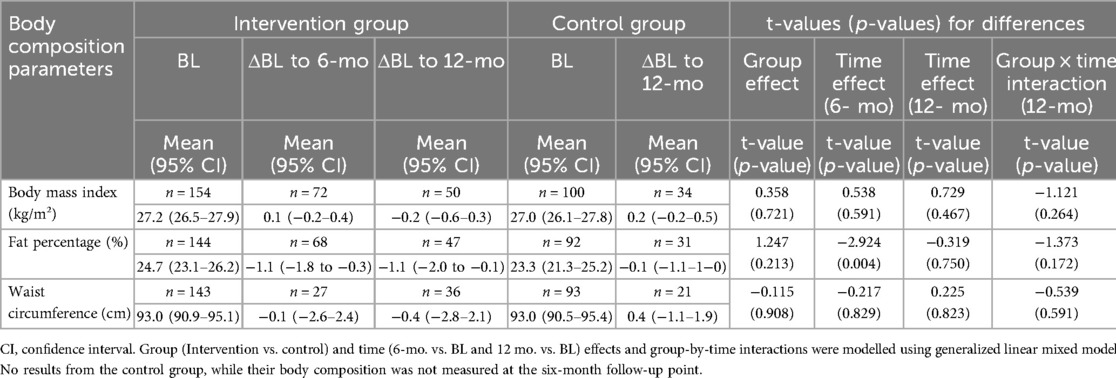
Table 4. Changes (Δ) in body composition from baseline (BL) to six-month and twelve-month (mo) follow-ups.
3.4 Cardiometabolic biomarkers
Changes in cardiometabolic biomarkers during the one-year follow-up are presented in Table 5. There was no group-by-time interaction in the cardiometabolic biomarkers between the intervention and control groups during the twelve-month follow-up. Still, total cholesterol and LDL decreased in the intervention group but increased in the control group. HDL tended to decrease and triglycerides increase in both groups. All results measuring glucose metabolism tended to increase in both intervention and control groups. The magnitude of these changed is described in detail in Table 5.

Table 5. Changes (Δ) in cardiometabolic biomarkers from baseline (BL) to six-month and twelve-month (mo) follow-ups.
3.5 Fitness tests
Changes in the fitness test results during the one-year follow-up are presented in Table 6. There was no statistically significant group-by-time interaction in the fitness test results between the intervention and control groups during the twelve-month follow-up. However, the VO2max tended to increase among the intervention group (mean increase 2.15 CI 95% 0.56–3.74 ml/kg/min) participants compared to those in the control group (mean decrease −0.71 CI 95% −3.880–2.37), but the group-by-time interaction did not reach full statistical significance (t = 2.009, p = 0.052). The trends in fitness index and push-ups results were increasing in both intervention and control groups, but the results of other studied parameters varied during the follow-up. The magnitude of these changes is described in detail in Table 6.
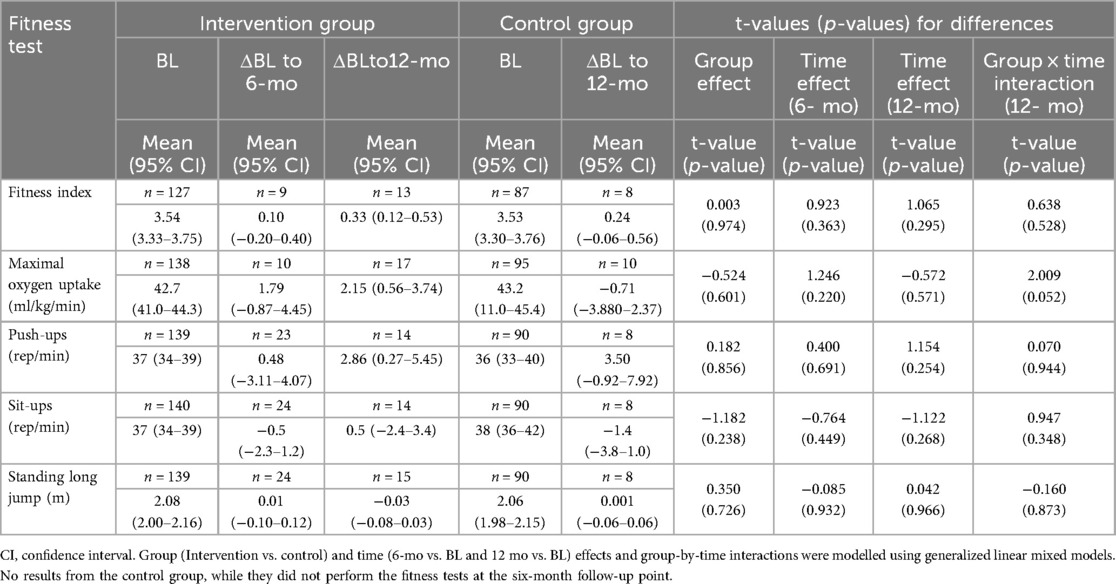
Table 6. Changes (Δ) in fitness test results from baseline (BL) to six-month and twelve-month (mo) follow-ups.
3.6 Stress and work ability
Changes in stress and work ability during the one-year follow-up are presented in Table 7. There was less stress among the intervention group than the control group. During the one-year follow-up, stress was perceived to be higher, and work ability lower in both the intervention and control groups. The magnitude of these changes is described in detail in Table 7.
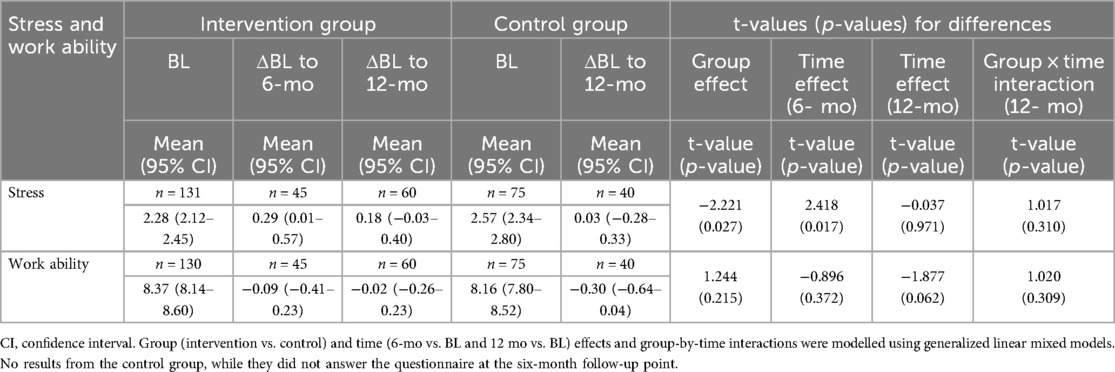
Table 7. Changes (Δ) in experience stress and work ability from baseline (BL) to six-month and twelve-month (mo) follow-ups.
4 Discussion
The implemented intervention tended to increase daily standing time among the intervention group in the long term, even though there was no intervention group interaction regarding the PA or SB from the baseline to the six-month or twelve-month follow-ups. Previously, interventions targeted to reduce SB have shown reductions in sitting time largely achieved by standing (53). However, during the time interval from the baseline to the twelve-month follow-up, there was a reduction in MVPA and LPA in addition to the reduction in SB among the intervention group. This might indicate that standing has replaced some of the time spent in LPA and MVPA. Replacing sitting or reclining with standing has been shown to improve glucose and lipid metabolism by increasing skeletal muscle activity (54), and standing more has been shown to be beneficially associated with hepatic insulin sensitivity (55), which shows the importance of standing behavior in health promotion. However, the change in daily standing time during the twelve-month follow-up among the intervention group was only 18 min/day, which is not supposed to cause major improvements in health parameters, while it also replaces some of the daily MVPA and LPA, which are associated positively with cardiometabolic health (53, 54).
Altogether, MVPA and daily step count increased, and SB decreased during the six-month follow-up in both the intervention and control groups. It seems that participation alone in the present study increased the daily PA among the studied participants. However, the increases in the daily PA were not permanent, as the daily PA had decreased back to the baseline level in both groups by the time of the twelve-month follow-up. The LPA even decreased from the baseline values among the intervention group. Previous studies of PA interventions have shown similar results: the reduction of the achieved PA improvements back to the baseline levels after active monitoring has ended, even when statistically significant improvements in PA had been attained (24).
In terms of body composition, there was no group-by-time interaction during the follow-up. However, fat percentage declined during the twelve-month follow-up in both groups. PA increased from baseline to the six-month follow-up, but the PA had decreased back to the baseline level by the end of the twelve-month follow-up. This might indicate that changes in fat percentage and improvements in body composition can be due to other factors, such as diet (56) or improved sleep (57), while the application used in the intervention also provided feedback on sleeping habits.
Moreover, there was no group-by-time interaction regarding cardiometabolic biomarkers. Still, there was an increase in HbA1c, gluc, and INS, and a decrease in HDL during the follow-up in both groups. These findings indicate negative changes in both glucose and lipid metabolism. Further, these changes seemed not to be related to the changes in PA, and thus, they were probably due to other factors. Employees in high-stress occupations, such as firefighters, military, and law enforcement personnel, are exposed to a variety of stressors, such as psychological, physiological, and environmental stressors (58–60). These stressors have been shown to increase the risk of cardiovascular disease to develop (61). Cardiovascular risk factors for coronary disease and metabolic syndrome have been shown to be common among firefighters and police officers despite their good physical fitness levels (62). During shift work, there may often occur abnormal eating patterns caused by circadian stress (63), which may lead to consuming sugars, sodium, and saturated fat, which increase the prevalence of obesity, hyperlipidemia, and metabolic syndrome (63–65). While the FAT% decreased during the follow-up period, indicating decreased adiposity, increases in HbA1c, INS, and gluc, and a decrease in HDL might still be due to the quality of food consumed (66, 67).
Additionally, the results showed no group-by-time interaction regarding physical fitness, but the VO2max tended to increase in the intervention group compared to the control group. Fitness index and push-up results tended to increase during the twelve-month follow-up in both groups. While the intervention did not separate the type of PA (e.g., muscle strength training from aerobic exercise training), the intervention group participants were encouraged to perform, and positive changes in muscle strength could be expected. Yet, the accelerometers did not accurately recognize the movements, which are only performed with the upper or lower extremities (e.g., gym exercise) (68), so the changes in muscle strength were not expected to be remarkable. However, the number of results from the physical fitness tests was sparse at the six-month and twelve-month follow-ups, distorting the results.
There was no group-by-time interaction regarding experienced stress or work ability. The intervention group participants experienced less stress than the control group participants, and stress tended to increase during the intervention among the intervention group participants. Yet, there is no data from the control group after the intervention with which to compare these results, and therefore, the meaning of these findings remains unexplained concerning the differences between the groups.
This study has several limitations. The drop-out rate was 47%, which might be affected by the mobile nature of the work of soldiers. Soldiers working for the Finnish Defence Forces can be commanded to work in different places around Finland and might serve on crisis management missions in other countries at some point in their careers. Changing workplace to one in a different part of the country can lower the threshold for dropping out of the study, and being commanded to go on a crisis management mission would prevent continuing participation in the study. Added to this, the participantś retention of PA interventions tend to vary between 31% at the lowest to 100% at the highest (69), indicating that the drop-out rate of the current study is not unusual. Furthermore, the accelerometer was not water-resistant, so water activities could not be recorded. Also, the accelerometer may not accurately recognize movements that are only performed with the upper or lower extremities (e.g., gym exercises) and movements performed in a supine position (e.g., Pilates) (68). Moreover, it took two months to perform the baseline measurements, and the intervention could be started only after six months from the baseline measurements due to working schedules concerning conscriptś educational tasks. During these six months between the baseline measurements and the beginning of the intervention might have occurred changes in measured parameters. Further, the limitations include the lack of dietary assessment and the use of general advice to reduce SB and increase PA, despite having access to monitored behavioral data that could have allowed even more personalized recommendations.
The strengths of the study include the sensor-based measurements of the PA, measurement method taking advantage of accelerometers (70), which are also able to record separately LPA, MVPA, SB, and standing. Moreover, the created intervention takes advantage of smartphone technology, making it accessible to large populations, while smartphones or smart devices are commonly owned in the Western world. Furthermore, during the intervention, participants received constant individualized online feedback on their physical activity and sleeping habits, which extended throughout their workday and leisure time. This serves as an opportunity for precision prevention at both the workplace and in free time (26). Additionally, the created intervention needs only a little timely investment from the provider, while the only additional requirements besides a smartphone for the implementation of the intervention would be an accelerometer and consultation with a PA instructor once during the six-month period, neither of which requires a big investment of human resources.
In conclusion, the present intervention, utilizing accelerometer–smartphone app technology combined with telephone counseling and encouragement to use the possibility to exercise during two working hours a week, did not succeed in increasing PA, but it showed potential in increasing daily standing in the long term. Again, when comparing the intervention and control groups, there were no group-by-time interactions regarding body composition, cardiometabolic biomarkers, physical fitness, or work ability. However, there was an increase in stress among the intervention group during the intervention, which was not observed between baseline and the twelve-month follow-up. Also, VO2max tended to increase during the twelve-month follow-up among the intervention group participants; however the dropout rate was high in aerobic fitness tests, which likely biased the results. The study reveals the potential and challenges of a light PA intervention for large populations needing low investment time-wise by the provider, in terms of increasing PA and decreasing SB among military employees. From a practical point of view, a certain number of accelerometers could be provided to the willing employees, and physical education officers could arrange one PA counseling session every six months for them without these arrangements adding them massive workload. However, the variability of the weekly work environments, working hours, and work tasks challenges the implementation of this kind of PA intervention in a military workplace. Further, low adherence has been shown in device-based physical activity monitoring in the long term, and some studies have shown better achievements when the physical activity goals have been targeted by minutes (24, 71, 72). In potential future physical activity interventions, creating pre-scheduled time slots for exercise, also for field training weeks, targeting the physical activity goals by minutes and pre-scheduling the baseline and follow-up measurements, as well as the start of the intervention for set dates for all employees working in the brigades, would help to receive more reliable results. The authority responsible for planning the yearly schedules for the brigades could arrange the timetable so that it would not disturb the education of the conscripts. Further studies with larger sample sizes should be conducted to assess the effects of the intervention used in this study setting and the generalisability of the current findings.
Data availability statement
The data used in this study are not publicly available. According to the research permit granted by the Finnish Defence Command, the raw data is owned by the Finnish Defence Command. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Tampere University Hospital (R16189). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. The Defence Command Finland granted permission for performing the study among the employees of the Finnish Defence Forces (AN8355,1367/12.04.01/2015; AN8355,2055/09.05/2022).
Author contributions
EP: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing. HK: Funding acquisition, Methodology, Project administration, Resources, Validation, Writing – review & editing. KP: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing. TL: Data curation, Formal analysis, Software, Writing – review & editing. TV: Methodology, Resources, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study was funded by the Finnish Defence Forces Centre for Military Medicine RD Executive Team (BM9746/6.12./29.9.2016), the Finnish Defence Command (AN20429, 16.11.2017), the Finnish Defence Forces Centre for Military Medicine (7000075612/23.11.2018), the Finnish Defence Forces Centre for Military Medicine (BR12768, 3813/01.03.00/2019), the National Defence Support Foundation of Finland (TELI/2020/2021) and the Finnish Medical Society Duodecim (TELI/2018).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2025.1549980/full#supplementary-material
References
1. Arthur A, Mensah-Asamoah A, Brown EKM, Ocansey AK, Moses MO. Work ability and anthropometric indices correlate with cardiovascular risk factors in public sector employees: cross-sectional study. Health Sci Rep. (2023) 6(11):e1728. doi: 10.1002/hsr2.1728
2. Bugajska J, Makowiec-Dabriwska T, Kostka T. Individual and Occupational Determinants: Work Ability in People with Health Problems. Taylor & Francis Group (2020). Available online at: https://ebookcentral.proquest.com/lib/tampere/detail.action?docID=6311170
3. Husu P, Tokola K, Vähä-Ypyä H, Sievänen H, Vansankari T. Accelerometer-measured physical behavior and cardiorespiratory fitness as indicators of work ability. Int J Environ Res Public Health. (2023) 20:5414. doi: 10.3390/ijerph20075414
4. Ługowska K, Kolanowski W, Trafialek J. Increasing physical activity at school improves physical fitness of early adolescents. Int J Environ Res Public Health. (2023) 20(3):2348. doi: 10.3390/ijerph20032348
5. Suorsa K, Mattila V-M, Leskinen T, Heinonen OJ, Pentti J, Vahtera J, et al. Work ability and physical fitness among aging workers: the Finnish retirement and aging study. Eur J Ageing. (2022) 19(4):1301–10. doi: 10.1007/s10433-022-00714-1
6. Lin X, Zhang X, Guo J, Roberts CK, McKenzie S, Wu X-C, et al. Effects of exercise training on cardiorespiratory fitness and biomarkers of cardiometabolic health: a systematic review and meta-analysis of randomized controlled trials. J Am Heart Assoc. (2015) 4(7):e002014. doi: 10.1161/JAHA.115.002014
7. Pengcheng H, Huanmiao X, Reilly KH, Yiguan W, Wei M, Bo X. Physical activity and risk of hypertension: a meta-analysis of prospective cohort studies. Hypertension. (2013) 62(6):1021–26. doi: 10.1161/HYPERTENSIONAHA.113.01965
9. Lusa S, Punakallio A, Mänttäri S, Korkiakangas E, Oksa J, Oksanen T, et al. Interventions to promote work ability by increasing sedentary workers’ physical activity at workplaces – A scoping review. Appl Ergon. (2020) 82:102962. doi: 10.1016/j.apergo.2019.102962
10. Wijndaele K, Matton L, Duvigneaud N, Lefevre J, De Bourdeaudhuij I, Duquet W, et al. Association between leisure time physical activity and stress, social support and coping: a cluster-analytical approach. Psychol Sport Exerc. (2007) 8(4):425–40. doi: 10.1016/j.psychsport.2006.08.001
12. Honkamaa S, Hyppönen H. PVHSM koulutusala 043-PEHENKOS palkatun henkilöstön kenttäkelpoisuus ja fyysinen työkyky (2014)
13. Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in sufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1-9 million participants. Lancet Global Health. (2018) 10(5):e1077–86. doi: 10.1016/S2214-109X(18)30357-7
14. Ng S, Popkin B. Time use and physical activity: a shift away from movement across the globe. Obes Rev. (2012) 13(8):659–80. doi: 10.1111/j.1467-789X.2011.00982.x
15. Peltonen M, Laatikainen T, Borodulin K, Wikström K, Jousilahti P, Jula A, et al. Prevalence of ideal cardiovascular health in an adult Finnish population: the national FINRISK 2007 study. Int Heart Vasc Dis J. (2014) 2(3):3–10. doi: 10.24412/2311-1623-2014-3-3-11
16. Husu P, Tokola K, Vähä-Ypyä H, Sievänen H. Physical activity, sedentary behavior and bedtime among Finnish adults measured 24/7 tri-axial accelerometery. J Meas Phys Behav. (2021) 4:163–73. doi: 10.1123/jmpb.2020-0056
17. Pihlainen K. Puolustusvoimien palkatun henkilöstön liikunta-aktiivisuuden yhteys terveyden riskitekijöihin ja suositukset palveluiden kehittämiseksi (2010).
18. Knapik JJ, Sharp MA, Steelman RA. Secular trends in the physical fitness of United States army recruits on entry to service 1975–2013. J Strength Cond Res. (2017) 31(7):2030–52. doi: 10.1519/JSC.0000000000001928
19. Leyk D, Witzki A, Willi G, Rohde U, Rüther T. Even one is too much: sole presence of one of the risk factors overweight, lack of exercise, and smoking reduces physical fitness of young soldiers. J Strength Cond Res. (2015) 29(Suppl 11):199–203. doi: 10.1519/JSC.000000000000106720
20. Hankonen N, Sutton S, Prevost AT, Simmons RK, Griffin SJ, Kinmonth AL, et al. Which behavior change techniques are associated with changes in physical activity, diet and body mass index in people with recently diagnosed diabetes? Ann Behav Med. (2015) 49(1):7–17. doi: 10.1007/s12160-014-9624-9
21. Bort-Roig J, Gilson ND, Puig-Ribera A, Contreras RS, Trost SG. Measuring and influencing physical activity with smartphone technology: a systematic review. Sports Med. (2014) 44(5):671–86. doi: 10.1007/s40279-014-0142-5
22. Goode AP, Hall KS, Batch BC, Huffman KM, Hastings SN, Allen KD, et al. The impact of interventions that integrate accelerometers on physical activity and weight loss: a systematic review. Ann Behav Med. (2017) 51(1):79–93. doi: 10.1007/s12160-016-9829-1
23. Guthrie N, Bradlyn A, Thompson SK, Yen S, Haritatos J, Dillon F, et al. Development of an accelerometer-linked online intervention system to promote physical activity in adolescents. PLoS One. (2015) 10(5):e0128639. doi: 10.1371/journal.pone.0128639
24. Hodkinson A, Kontopantelis E, Adeniji C, van Marwijk H, McMillan B, Bower P, et al. Accelerometer- and pedometer-based physical activity interventions among adults with cardiometabolic conditions: a systematic review and meta-analysis. JAMA Network Open. (2019) 2(10):e1912895. doi: 10.1001/jamanetworkopen.2019.12895
25. Sjöros T, Laine S, Garthwaite T, Vähä-Ypyä H, Löyttyniemi E, Koivumäki M, et al. Reducing sedentary time and whole-body insulin sensitivity in metabolic syndrome: a 6-month randomized controlled trial. Med Sci Sports Exerc. (2022) 55(3):342–53. doi: 10.1249/MSS.0000000000003054
26. Mess F, Blaschke S, Gebhard D, Friedrich J. Precision prevention in occupational health: a conceptual analysis and delelopment of a unified understanding and an integrative framework. Front Public Health. (2024) 12:1444521. doi: 10.3389/fpubh.2024.1444521
27. Sjøgaard G, Christensen JR, Justesen JB, Murray M, Dalager T, Fredslund GH, et al. Exercise is more than medicine: the working age population’s well-being and productivity. J Sport Health Sci. (2016) 5(2):159–65. doi: 10.1016/j.jshs.2016.04.004
28. Dalager T, Justesen J, Murray M, Boyle E, Sjøgaard G. Implementing intelligent physical exercise training at the workplace: health effects among office workers—a randomized controlled trial. Eur J Appl Physiol. (2016) 116(7):1433–42. doi: 10.1007/s00421-016-3397-8
29. Van Dijk-Huisman HC, Senden R, Smeets MHH, Marcellis RGJ, Magdelijns FJH, Lenssen AF. The effect of a smartphone app with an accelerometer on the physical activity behavior on hospitalized patients: a randomized controlled trial. Sensors (Basel). (2023) 23(21):8704. doi: 10.3390/s23218704
30. Bittel DC, Bittel AJ, Williams C, Elazzazi A. Improving exercise performance with an accelerometer-based smartphone app: a randomized controlled trial. Am J Phys Med Rehabil. (2017) 96(5):307–14. doi: 10.1097/PHM.0000000000000618
31. Vähä-Ypyä H, Husu P, Suni J, Vasankari T, Sievänen H. Reliable recognition of lyinf, sitting, and standing with a hip-worn accelerometer. Scand J Med Sci Sports. (2018) 28(3):1092–102. doi: 10.1111/sms.13017
32. Vähä-Ypyä H, Vasankari T, Husu P, Mänttäri A, Vuorimaa T, Suni J, et al. Validation of cut-points for evaluating the intensity of physical activity with accelerometry-based mean amplitude deviation (MAD). PLoS One. (2015) 10(8):e0134813. doi: 10.1371/journal.pone.0134813
33. Vähä-Ypyä H, Vasankari T, Husu P, Suni J, Sievänen H. A universal, accurate intensity-based classification of different physical activities using raw data of accelerometer. Clin Physiol Funct Imaging. (2015) 35(1):64–70. doi: 10.1111/cpf.12127
34. Vasankari V, Halonen J, Husu P, Vähä-Ypyä H, Tokola K, Suni J, et al. Personalised eHealth intervention to increase physical activity and reduce sedentary behaviour in rehabilitation after cardiac operations: study protocol for the PACO randomised controlled trial (NCT03470246). BMJ Open Sport Exerc Med. (2019) 5(1):e000539. doi: 10.1136/bmjsem-2019-000539
35. UKK Institute. Liikkumalla terveyttä-askel kerrallaan. Viikoittainen liikkumisen suositus 18- 64 -vuotiaille. (2019) Available online at: https://ukkinstituutti.fi/liikkuminen/liikkumisen-suositukset/aikuisten-liikkumisen-suositus/ (Accessed October 04, 2025).
36. Pietiläinen E, Kyröläinen H, Vasankari T, Santtila M, Luukkaala T, Parkkola KA. Randomized controlled trial protocol for using an accelerometer-smartphone application intervention to increase physical activity and improve health among employees in a military workplace. Methods Protoc. (2022) 5(1):1. doi: 10.3390/mps5010001
37. Mizell D. Using gravity to estimate accelerometer orientation. Seventh IEEE International Symposium on Wearable Computers, 2003 (2003). p. 252–53. doi: 10.1109/ISWC.2003.1241424
38. Tremblay MS, Aubert S, Barnes JD, Saunders TJ, Carson V, Latimer-Cheung AE, et al. Sedentary behavior research network (SBRN) – terminology consensus project process and outcome. Int J Behav Nutr Phys Act. (2017) 14(1):75. doi: 10.1186/s12966-017-0525-8
39. Cooper KH. A means of assessing maximal oxygen intake: correlation between field and treadmill testing. JAMA. (1968) 203(3):201–04. doi: 10.1001/jama.1968.03140030033008
40. Storer TW, Davis JA, Caiozzo VJ. Accurate prediction of VO2max in cycle ergometry. Med Sci Sports Exercise. (1990) 22(5):704–12. doi: 10.1249/00005768-199010000-0002
41. Suni J, Oja P, Laukkanen R, Millunpalo S, Pasanen M, Vartiainen TM, et al. Validity of UKK 2 km walking test: relations to physical activity and health. Med Sci Sports Exercise. (1995) 27(Supplement):S77. doi: 10.1249/00005768-199505001-00433
42. Pihlainen K, Santtila M, Häkkinen K, Kyröläinen H. Associations of physical fitness and body composition characteristics with simulated military task performance. J Strength Cond Res. (2018) 32(4):1089–98. doi: 10.1519/JSC.0000000000001921
43. Ilmarinen J. The work ability index (WAI). Occup Med (Chic Ill). (2007) 57(2):160. doi: 10.1093/occmed/kqm008
44. Radkiewicz P, Widerszal-Bazyl M. Psychometric properties of work ability index in the light of comparative survey study. Int Congr Ser. (2005) 1280:304–9. doi: 10.1016/j.ics.2005.02.089
45. Karttunen J, Rautiainen R. Work ability index among Finnish dairy farmers. J Agric Saf Health. (2009) 15(4):353–64. doi: 10.13031/2013.28889
46. Ahlström L, Grimby-Ekman A, Hagberg M, Delive L. The work ability index and single-item question: associations with sick leave, symptoms, and health - a prospective study of women on long-term sick leave. Scand J Work Environ Health. (2010) 36(5):404–12. doi: 10.5271/sjweh.2917
47. El Fassi M, Bocquet V, Majery N, Lair ML, Couffignal S, Mairiaux P. Work ability assessment in a worker population: comparison and determinants of work ability index and work ability score. BMC Public Health. (2013) 13:305. doi: 10.1186/1471-2458-13-305
48. Kettunen O, Vuorimaa T, Vasankari T. A 12-month exercise intervention decreased stress symptoms and increased mental resources among working adults – results perceived after a 12-month follow-up. Int J Occup Med Environ Health. (2015) 28(1):157–68. doi: 10.13075/ijomeh.1896.00263
49. Elo A-L, Leppänen A, Lindström K, Ropponen T. OSQ, Occupational Stress Questionnaire – Users Instructions. Reviews 19. Helsinki: Finnish Institute of Occupational Health (1992).
50. Elo A-L, Leppänen A, Sillanpää P. Applicability of survey feedback for an occupational health method in stress management. Occup Med. (1998) 48(3):181–8. doi: 10.1093/occmed/48.3.181
51. Elo A-L, Leppänen A, Jahkola A. Validity of a singleitem measure of stress symptoms. Scand J Work Environ Health. (2003) 29(6):444–51. doi: 10.5271/sjweh.752
52. Fitzmaurice GM, Laird NM, Ware JH. Applied Longitudinal Analysis. Hoboken, NJ: John Wiley & Sons Incorporated (2012).
53. Curran F, Blake C, Cunningham C, Perrotta C, van der Ploeg H, Matthews J, et al. Efficacy, charactreristics, behavioural models and behaviour change strategies, of non-workplace interventions specifically targeting sedentary behaviour; a systematic review and meta-analysis of ransomised control trials in healthy ambulatory adults. PLoS One. (2021) 16(9):e0256828. doi: 10.1371/journal.pone.0256828
54. Healy GN, Winkler EAH, Owen N, Anuradha S, Dunstan DW. Replacing sitting time with standing or stepping: associations with cardio-metabolic risk biomarkers. Eur Heart J. (2015) 36(39):2643–49. doi: 10.1093/eurheartj/ehv308
55. Laine S, Sjöros T, Garthwaite T, Honka M, Löyttyniemi E, Eskola O, et al. Daily standing time, dietary fiber, and intake of unsaturated fatty acids are beneficially associated with hepatic insulin sensitivity in adults with metabolic syndrome. Front Endocrinol (Lausanne). (2024) 15:1272886. doi: 10.3389/fendo.2024.1272886
56. Pérez-Escamilla R, Obbagy JE, Altman JM, Essery EV, McGrane MM, Wong YP, et al. Dietary energy density and body weight in adults and children: a systematic review. J Acad Nutr Diet. (2012) 112(5):671–84. doi: 10.1016/j.jand.2012.01.020
57. St-Onge M-P. Sleep-obesity relation: underlying mechanisms and consequences for treatment. Obes Rev. (2017) 18(S1):34–9. doi: 10.1111/obr.12499
58. Carey MG, Al-Zaiti SS, Dean GE, Sessanna L, Finnell DS. Sleep problems, depression, substance use, social bonding, and quality of life in professional firefighters. J Occup Environ Med. (2011) 53(8):928–33. doi: 10.1097/JOM.0b013e318225898f
59. Garbarino S, De Carli F, Nobili L, Mascialino B, Squarcia S, Penco MA, et al. Sleepiness and sleep disorders in shift workers: a study on a group of Italian police officers. Sleep. (2002) 25(6):648–53. doi: 10.1093/sleep/25.6.642
60. Hoge CW, Auchterlonie JL, Milliken CS. Mental health problems, use of metal health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. JAMA. (2006) 295(9):1023–32. doi: 10.1001/jama.295.9.1023
61. Huang C-J, Webb HE, Zourdos MC, Acevedo EO. Cardiovascular reactivity, stress and physical activity. Front Physiol. (2013) 4:314. doi: 10.3389/fphys.2013.00314
62. Leischik R, Foshag P, Strauβ M, Littwitz H, Garg P, Dworrak B, et al. Aerobic capacity, physical activity and metabolic risk factors in firefighters compared with police officers and sedentary clerks. PLoS One. (2015) 10(7):e0133113. doi: 10.1372/journal.pone.0133113
63. Lowden A, Moreno C, Holmbaeck U, Lennernaes M, Tucker P. Eating and shift work-effects on habits, metabolism, and performance. Scand J Work Environ Health. (2010) 36(2):150–62. doi: 10.5271/sjweh.2898
64. Faghri PD, Mignano C, Huendo-Medina TB, Cherniack M. Psychological health and overweight and obesity among high stressed work environments. Obesity. (2015) 1(1):10.16966/2380-5528.101. doi: 10.16966/2380-5528.101
65. Kivimäki M, Head J, Ferrie JE, Shipley MJ, Brunner E, Vahtera J, et al. Work stress, weight gain and weight loss: evidence for bidirectional effects of job strain on body mass index in the Whitehall II study. Int J Obes. (2006) 30(6):982–7. doi: 10.1038/sj.ijo.0803229
66. De Koning L, Chiuve SE, Fung TT, Willett WC, Rimm EB, Hu FB. Diet-quality scores and the risk of type 2 diabetes in men. Diabetes Care. (2011) 34(5):1150–6. doi: 10.2337/dc10-2352
67. Aronis K, Khan S, Mantzoros C. Effects of trans fatty acids on glucose homeostasis: a meta-analysis of randomized, placebo-controlled clinical trials. Am J Clin Nutr. (2012) 96(5):1093–9. doi: 10.3945/ajcn.112.040576
68. Strath SJ, Kaminsky LA, Ainsworth BE, Ekelund U, Freedson PS, Gary RA, et al. Guide to the assessment of physical activity: clinical and research applications: a scientific statement from the American Heart Association. Circulation. (2013) 128(20):2259–79. doi: 10.1161/01.cir.0000435708.67487.da
69. Carroll JK, Yancey AK, Spring B, Figueroa-Moseley C, Mohr DC, Mustian KM, et al. What are successful recruitment and retention strategies for underserved populations? Examining physical activity interventions in primary care and community setting. Transl Behav Med. (2011) 1(2):234–51. doi: 10.1007/s13142-011-0034-2
70. Westerterp KR. Assessment of physical activity: a critical appraisal. Eur J Appl Physiol. (2009) 105(6):823–8. doi: 10.1007/s00421-009-1000-2
71. Baker G, Mutrie N, Lowry R. Using pedometers as motivational tool: are goals set in steps more effective than goals set in minutes for increasing walking? Int J Health Promot Educ. (2008) 46(1):21–6. doi: 10.1080/14635240.2008.10708123
Keywords: physical activity, accelerometer, mobile applications, physical fitness, cardiometabolic health, sedentary behavior
Citation: Pietiläinen E, Kyröläinen H, Parkkola K, Luukkaala T and Vasankari T (2025) A randomized controlled trial utilizing an interactive accelerometer linked to a smartphone application for enhancing physical activity and health among military employees. Front. Sports Act. Living 7:1549980. doi: 10.3389/fspor.2025.1549980
Received: 22 December 2024; Accepted: 28 July 2025;
Published: 22 August 2025.
Edited by:
Iuliia Pavlova, Lviv State University of Physical Culture, UkraineReviewed by:
Arto J. Pesola, South-Eastern Finland University of Applied Sciences, FinlandTuija Leskinen, University of Turku, Finland
Copyright: © 2025 Pietiläinen, Kyröläinen, Parkkola, Luukkaala and Vasankari. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emilia Pietiläinen, ZW1pbGlhLnBpZXRpbGFpbmVuQHR1bmkuZmk=