 Daniel C. Ogrezeanu1
Daniel C. Ogrezeanu1 Andrea Tur-Boned2Nicholas Rolnick3,4
Andrea Tur-Boned2Nicholas Rolnick3,4 Juan J. Carrasco5,6
Juan J. Carrasco5,6 Carlos Cruz-Montecinos5,7
Carlos Cruz-Montecinos5,7 Joaquín Calatayud1*
Joaquín Calatayud1* Santiago Bonanad8
Santiago Bonanad8 Sofía Pérez-Alenda5
Sofía Pérez-Alenda5
- 1Exercise Intervention for Health Research Group (EXINH-RG), Department of Physiotherapy, University of Valencia, Valencia, Spain
- 2Department of Physiotherapy, University of Valencia, Valencia, Spain
- 3The Human Performance Mechanic, New York, NY, United States
- 4Department of Exercise Sciences and Recreation, Lehman College, Bronx, NY, United States
- 5Physiotherapy in Motion Multispeciality Research Group (PTinMOTION), Department of Physiotherapy, University of Valencia, Valencia, Spain
- 6Intelligent Data Analysis Laboratory, University of Valencia, Valencia, Spain
- 7Laboratory of Clinical Biomechanics, Department of Physical Therapy, Faculty of Medicine, University of Chile, Santiago, Chile
- 8Haemostasis and Thrombosis Unit, Universitary and Polytechnic Hospital La Fe, Valencia, Spain
Introduction: Low-load resistance training with concurrent blood flow restriction (BFR) provides strength and hypertrophy benefits to healthy individuals and some clinical populations. This is the first study assessing safety and physiological responses of autoregulated (AUTO) and non-autoregulated (NAUTO) BFR protocols in people with hemophilia (PWH). Therefore, this study aimed to evaluate the acute safety, cardiovascular, neuromuscular and perceptual responses during AUTO and NAUTO BFR training in PWH.
Methods: Eleven severe PWH under prophylaxis performed two sessions of elbow flexion and extension using elastic bands at 50% of the limb occlusion pressure (LOP) with different BFR settings (AUTO vs. NAUTO). Safety, cardiovascular parameters, rating of perceived exertion, elbow pain and pressure algometry were assessed at different timepoints. High-density surface electromyography activity and its spatial distribution were determined for biceps and triceps brachii.
Results: Both BFR conditions were safe in PWH. AUTO provided a hypotensive and hypoalgesic acute response, albeit without between-group differences. Triceps brachii showed differences in spatial distribution, and greater activity with AUTO in the last 3 cycles of the first 3 sets. Although no major differences were found between both conditions in perceptual responses, AUTO condition increased VAS scores during both exercises. No adverse events were observed.
Conclusions: BFR at 50%LOP during arm exercise with either AUTO or NAUTO appears to be equally safe in PWH, but AUTO showed trends for improved cardiovascular and neuromuscular responses. AUTO produced a hypotensive and hypoalgesic acute post-exercise response, albeit without between-group differences, a greater activation in triceps brachii, and higher values of pain. No serious adverse events were observed.
1 Introduction
Hemophilia is an X-linked congenital bleeding disorder caused by a deficiency of the clotting factors VIII or IX (1). A bleeding tendency is characteristic in severe cases, most commonly in synovial joints like the elbows (1). A single bleed or recurrent bleeds may cause hemophilic arthropathy, causing joint destruction with irreversible changes in the cartilage and bone tissue, leading patients to experience pain and limitation in daily activities (2).
Exercise programmes are usually designed and implemented to help manage the recovery after a bleed or to prevent bleeding episodes (3). To improve muscle strength, regular heavy-load resistance training with external loads of 60%–90% of one-repetition maximum (1RM) is recommended (4). However, some studies have demonstrated similar gains in strength (5) and hypertrophy (6) between high-load training and low-load training (20%–30% 1RM) with blood flow restriction (BFR). BFR training (BFRT) consists in applying an external pressure to the most proximal region of the limb, causing a full restriction of venous outflow while maintaining arterial inflow of blood distal to the cuff (7). This is thought to induce a hypoxic environment leading to increased levels of metabolic stress, a rise in type II muscle fibre recruitment, and the accumulation of metabolites (8). BFRT may be appropriate in patients who may not be able to tolerate heavy-loads (9) such as people with hemophilia (PWH), where a nuanced equilibrium between improving strength and risk of joint injury exists (3). This complex equilibrium impacts prescription of exercise regimens. In addition, BFRT enables shorter training sessions, which, together with the low intensity used, could help manage kinesiophobia and catastrophism that is usually present in PWH (10).
To reduce the potential for excessive stress on the cardiovascular system (e.g., blood pressure increase), the use of personalized limb occlusion pressures (LOP) is recommended (7). Nevertheless, LOP is statically determined at rest and does not account for muscle contractions. Previous studies have shown an increase in intramuscular pressure with reduced blood flow during contractions (11, 12). This happens with non-autoregulated (NAUTO) BFR devices in which the pressure applied to the limb is not adapted to the phase of muscular contraction, leading to variable levels of vascular occlusion (13, 14). Conversely, autoregulated (AUTO) devices avoid variability in applied pressure to the limb by monitoring for pressure changes and adjusting pressure dynamically, partially deflating when surpassing the target percentage of LOP and reinflating when pressure goes below the desired level, rapidly compensating the higher than desired occlusion levels that occur during muscle contractions (14). Theoretically, AUTO should be better tolerated than NAUTO, resulting in improved clinical outcomes. However, only a few number of studies (15, 16) thus far have examined the acute differences between AUTO and NAUTO, all conducted in healthy people and reporting no major differences in cardiovascular outcomes (e.g., brachial blood pressures). In one study (15), AUTO appeared to reduce the risk for adverse events, muscle soreness after 24 h and was perceived to be significantly less uncomfortable; however, the other study found no differences in perceptual experiences or differences in mitigating adverse responses as both conditions did not induce any adverse events (16). In addition, no previous studies have investigated the neuromuscular differences between NAUTO and AUTO in clinical population, which could provide useful information for clinical decision-making. This underscores the necessity for further studies to be conducted wherein BFR pressure application settings are applied among populations with musculoskeletal conditions that stand to derive the greatest benefit from them. Thus far, only two studies have implemented BFR resistance training in PWH (17, 18). One demonstrated safety, albeit within a small number of repetitions (17), while the other implemented a full standard BFR session (18). However, both only used a traditional NAUTO device and only during one exercise in the lower body (17, 18). Hence, the purpose of this study was to examine the acute safety, cardiovascular, neuromuscular and perceptual responses during AUTO and NAUTO BFRT in the upper body in PWH.
2 Methods
2.1 Participants
Candidates were adult PWH A or B (moderate or severe), 18–60 years old and undergoing prophylaxis. Participants were excluded if they (1) had surgical procedures performed 6 months prior to the exercise program; (2) participated in any other form of exercise, not previously done, during the study; (3) had any changes in medication during the study; (4) had a major bleeding episode that posed a risk or prevented exercise 6 weeks prior to or during the study; (5) had another hemostatic defect; (6) had history of stroke, brain surgery, major depression, or any self-perceived cognitive alterations that could affect the performance of study tasks. Participants were duly informed and gave written informed consent. The study conformed to the Declaration of Helsinki, was approved by the local Ethics Committee, and adheres to STROBE guidelines.
2.2 Procedures
Demographics and clinical data were collected from recent medical records and interviews. Participants were asked to not consume any nourishment, alcohol, or stimulants in the 2 h prior to the sessions. They were asked to not engage in any form of physical activity more intense than basic activities in the 24 h before the sessions nor use any analgesics, and they were also recommended to sleep a minimum of 7–8 h the night before.
Participants attended two sessions separated by approximately one week (mean 9.6 days; SD 4.1). Each session, an intervention was assigned in a counterbalanced manner, including elbow extensions and flexions, speed and external resistance matched, but with a different BFR protocol: (1) occlusion at 50% LOP with non-autoregulated pressure setting (NAUTO); (2) occlusion at 50% LOP with autoregulated pressure setting (AUTO). On the first day, the following baseline assessments were collected: elbow pain intensity was assessed using the 100 mm visual analogue scale (VAS) while kinesiophobia was assessed using the Tampa Scale for Kinesiophobia (TSK-11). Leisure-time physical activity and resistance training experience were also assessed.
Then, with the participants seated, measures of cardiovascular stress [systolic blood pressure (SBP), diastolic blood pressure (DBP) and heart rate (HR)] were evaluated in the dominant arm using an automatic tensiometer (M3 Comfort, OMRON Healthcare, Japan). Three measurements were taken (separated by 2 min) and averaged at each timepoint: preexercise (pre), immediate postexercise (post), and 10 min after exercise (post 10 min). Also, the mean arterial pressure (MAP), taking into account DBP, HR and pulse pressure (PP; which is the difference between SBP and DBP), was calculated with the formula: MAP = DBP + [0.01 × EXP(4.14–40.74/HR) × (PP)]. Afterwards, pressure pain thresholds (PPT) were evaluated using a digital pressure algometer (NOD, OT Bioelettronica, Italy), 3 cm distal to the dominant arm lateral epicondyle, in the extensor digitorum muscle tendon. Three PPT measurements were taken (separated by 30 s) and averaged at each timepoint.
Subsequently, as a baseline safety precaution measure, an ultrasound scan (LOGIQ C5 Premium, GE Healthcare, USA) of the exercising arm (the dominant one) was performed to exclude subclinical active bleeding in the biceps and triceps brachii. Next, active elbow extension/flexion range of motion (ROM) was measured using a goniometer, with the participants standing. Three measurements were taken for each movement and their mean registered.
Exercise intensity was identified using elastic bands (TheraBand CLX, Performance Health, USA) progressively from lowest to highest resistance (yellow color to red, green, blue, black, silver or gold). Participants performed 2–3 sets of 2 reps with 60 s rests until they rated a 2 on Borg's CR10 Scale (corresponds to 30% 1RM) (19). A 5 min rest was then taken during which, with the participants standing, the high-density surface electromyography (HDsEMG) protocol began with skin marking in the biceps brachii and triceps brachii muscles (20). After the skin was shaved and abraded to remove dead skin cells and cleaned with cotton wool dipped in alcohol, the electrode grids were positioned, with the electrode columns oriented along the muscle fibers. The reference electrodes were placed at the wrist. Specifically, HDsEMG was recorded in monopolar derivation with semi-disposable adhesive matrices (GR10MM0804, OT Bioelettronica, Italy) of 32 (8 × 4) equally spaced electrodes (with an inter-electrode distance of 10 mm). HDsEMG signals were sampled at 2,000 Hz and converted to digital data by a 16-bit analogue to digital converter (Sessantaquattro, 64-channel HDsEMG, OT Bioelettronica, Italy).
Before the training and after a submaximal practice trial, participants performed two maximum voluntary isometric contractions (MVIC) for each muscle (with 30 s rest) to normalize HDsEMG (to the highest MVIC or the highest in session amplitude, if higher), and to measure maximum isometric elbow flexion and extension strength by performing the MVICs against a fixed hand-held dynamometer (NOD, OT Bioelettronica, Italy). Participants sat with erect posture and no back support at 90° of elbow flexion. In this position, participants performed a 2 s progressive ramp contraction and then maintained a maximum contraction effort for the next 3 s. Participants were verbally encouraged to reach their maximal effort.
After a 5 min rest, the LOP of the exercising upper limb was determined with the participants standing while the pneumatic cuff (SmartCuffs PRO 3, Smart Tools Plus, USA) was placed on the most proximal portion of their arm (cuff width, 6.35 cm). The inflation procedure was automated and based on an in-device algorithm validated against the current Doppler ultrasound gold standard (21). Once LOP was determined, the cuff was deflated, and the participants rested quietly for 5 min before training. For safety, a pulse oximeter (CMS50D, Contec Medical Systems Co., China) was used on the thumb throughout the session.
The exercise protocol followed the standard BFRT structure of four sets (30, 15, 15, 15 reps; 30 s rests) with continuous BFR (5 min break between exercises for reperfusion). The elastic bands were pre-stretched (adding about 25% of the initial length) and a metronome was used to ensure a cadence of 1.5 s per movement phase. After performing each set, HR and oxygen saturation (SaO2) were assessed with the pulse oximeter and participants were asked to rate their rating of perceived exertion (RPE) on the Borg CR10 scale, their pain intensity in the exercising arm with the VAS, and degree of perceived tolerability using a five-point scale (i.e., very well tolerated = 5, tolerated = 4, neutral = 3, not well tolerated = 2 and not tolerated = 1). Moreover, after finishing the two exercises, SBP, DBP, HR, VAS and PPTs were reassessed immediately and at 10 min after. Subsequently, participants completed a global change scale about the potential change in their fear of practicing BFRT (very much improved, much improved, minimally improved, no change, minimally worse, much worse, very much worse). Finally, 24, 48 and 72 h after each session, participants were interviewed about delayed onset muscle soreness (DOMS), joint pain, and stiffness using an 11-point scale after palpating the arm and moving from full flexion to full extension. They were also asked about any suspicion of muscle or joint bleeds, or any possible adverse effects, and instructed to report any they might feel during the week after.
2.3 HDsEMG data analysis
The HDsEMG signals were processed offline using custom-made algorithms implemented in MATLAB software (The MathWorks Inc., Natick, Massachusetts, USA, version R2018b). All raw signals were amplified to obtain the EMG data in microvolts. Next, a differentiation of the 32-monopolar HDsEMG channels was carried out along the fibers direction (columns of the grid) to obtain arrays of 7 columns × 4 rows of bipolar signals, i.e., 28 RMS signals on each electrode array. A Butterworth fourth-order zero-lag band-pass filter (20–400 Hz) was then applied to each signal to eliminate low and high-frequency noise. Subsequently, a visual inspection was carried out to discard signals with excess noise. A moving root-mean-squared (RMS) smoothing filter was applied to the HDsEMG signals, implemented with a 1,000 ms window (500 ms backward and 500 ms forward) for each signal sample.
Once the signals were filtered, an automatic segmentation of the contractions was carried out from the maximum and minimum peaks of each signal. This methodology allows us to delimit the period of muscle activity, but not to distinguish the concentric and eccentric phases of muscle contractions. However, it has been used before in many previously published studies (17, 18, 22). While it is true that contraction mode can affect EMG amplitude, and many studies synchronize EMG with other types of additional external signals to be able to do this (video recording, motion capture, and accelerometer data) (23, 24), we chose to analyze the exercise sets with no differentiation between the concentric and eccentric components, as patients normally complete both components together during their rehabilitation programmes.
In each of the contractions, the mean RMS activation percentage (amplitude) was obtained by normalizing the result to the highest RMS activation value reached by the participant during the session (including MVIC). After obtaining these normalized variables in each signal of the map (7 × 4 matrix signals), the average nRMS values were obtained, as well as the coordinates of the HDsEMG nRMS map centroid (x- and y-axis coordinates for the medial-lateral and cranial-caudal direction, respectively) and the modified entropy. The average nRMS HDsEMG from all channels on the matrix was used as a parameter of muscle activation, while the displacement of the centroid and variations in the modified entropy were used to assess HDsEMG activity spatial distribution. A higher modified entropy (from a maximum possible value of 4.81 in the case of our matrices of 28 RMS signals) represents less heterogeneity in the spatial distribution of nRMS values within the electrode matrix, ergo higher homogeneity, whilst a decrease in entropy indicates a decrease of homogeneity. Coefficient of variation (CoV) was defined as the standard deviation (SD) of the 28 RMS values divided by the average of the 28 RMS values. When SD is small relative to the mean, this results in a smaller CoV. Therefore, when channel signals are more uniform, there will be a smaller CoV to also indicate increased homogeneity (reduced heterogeneity). To allow statistical analysis, the repetitions of each set were averaged in successive cycles. In the case of set 1 (30 reps), each cycle consists of the average of 6 reps. In sets 2–4 (15 reps), each cycle is the result of averaging 3 reps. In all cases, 5 cycles were obtained.
2.4 Statistical analysis
An a priori power analysis was conducted (G∗Power; Düsseldorf, Germany) to calculate the required sample size. With the present study design, assuming a medium effect size (f = 0.30), a 5% alpha risk (α = 0.05) and 20% beta risk (β = 0.2; power = 0.80), and a correlation between repeated measures of 0.6, a total of 11 participants were sufficient.
The statistical analysis was performed with SPSS v26 (IBM Corp, USA). The normality of the data was verified with the Shapiro–Wilk test. Descriptive results are shown as mean (SD), median [25th−75th percentiles] or n (percentages) as appropriate.
The differences between conditions (AUTO, NAUTO) and times (pre, post, post 10 min) for SBP, DBP, HR, MAP, VAS and PPT were evaluated using linear mixed models. The conditions and times were entered into the model as repeated measures with fixed effects.
RPE, VAS, tolerability and HR were evaluated using linear mixed models to analyze differences between conditions and sets (1–4). The conditions and sets were configured as repeated measures with fixed effects.
The differences between conditions, sets and cycles (1–5) for nRMS, CoV, modified entropy and centroid were evaluated using linear mixed models. The conditions, sets and cycles were considered as repeated measures with fixed effects. In all mixed models, subject was entered as random effect and the restricted maximum likelihood estimation method was used with the Satterwait approximation. When the main effects indicated significant differences, the Bonferroni correction was applied to avoid Type I error caused by multiple comparisons. Data were statistically significant when p < 0.05.
3 Results
3.1 Participants
Eleven adults with hemophilia A participated in the study. Demographic and clinical data are shown in Table 1. About half (54.55%) of the participants had a history of resistance training and were involved in physical activity for at least 1 day·week–1. No serious adverse effects were reported during the sessions, with none of the reported events impeding the completion of the exercises.
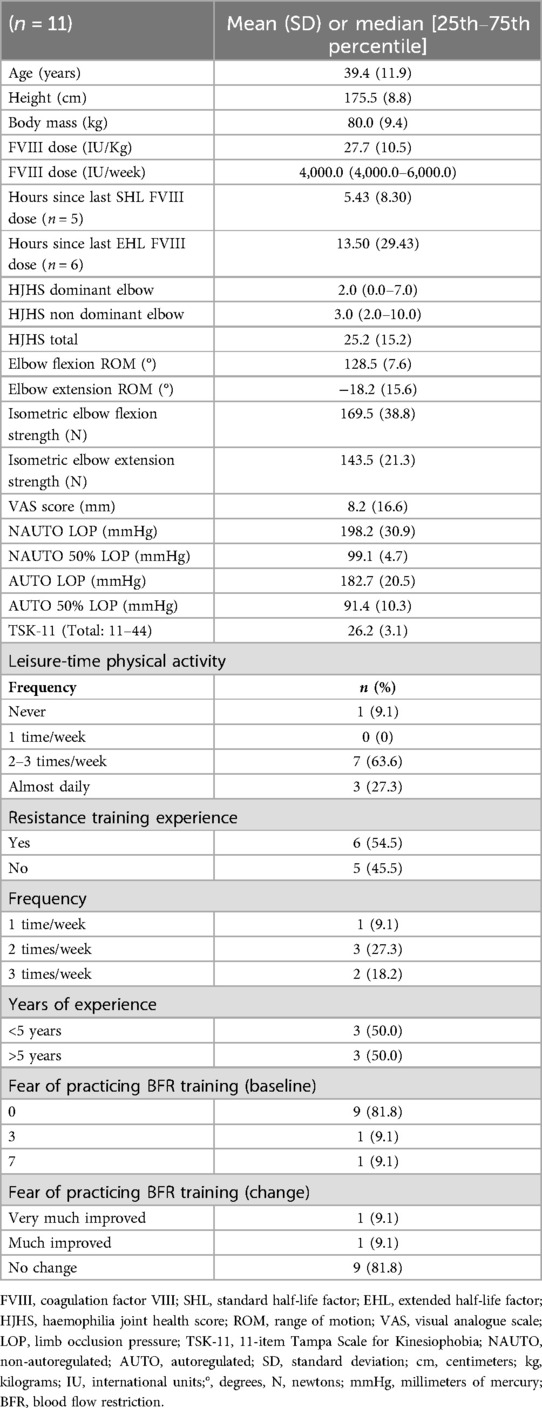
Table 1. Demographic and clinical data.
3.2 Cardiovascular and hypoalgesic responses
The acute cardiovascular and hypoalgesic responses to NAUTO and AUTO BFRT are shown in Table 2. The AUTO condition was the only one that produced a hypotensive and hypoalgesic acute response, albeit there were no between-group differences.
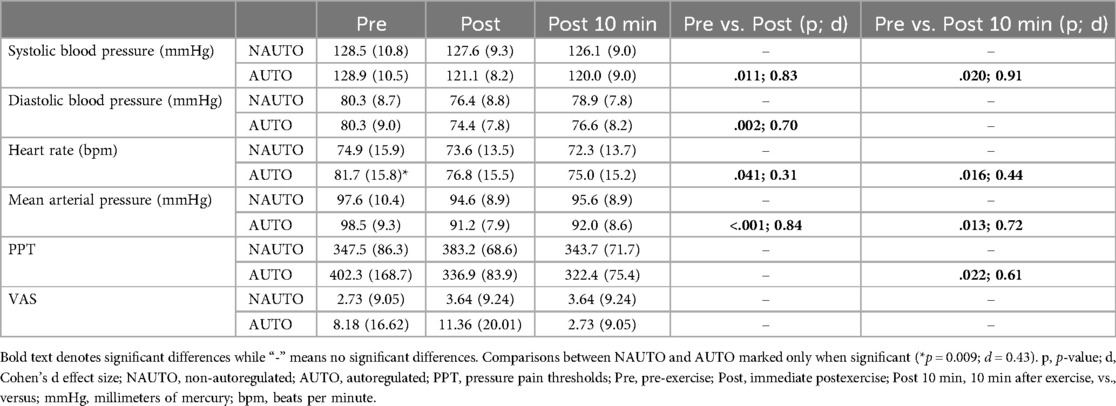
Table 2. Acute cardiovascular and hypoalgesic responses before and after the blood flow restriction resistance training session.
3.3 High-density surface EMG
Neuromuscular activity (mean %nRMS for biceps and triceps brachii muscles) during both BFR conditions is shown in Figure 1. While biceps brachii had no difference between both conditions, triceps brachii showed a greater activation with the AUTO condition in the last 3 cycles of the first 3 sets.
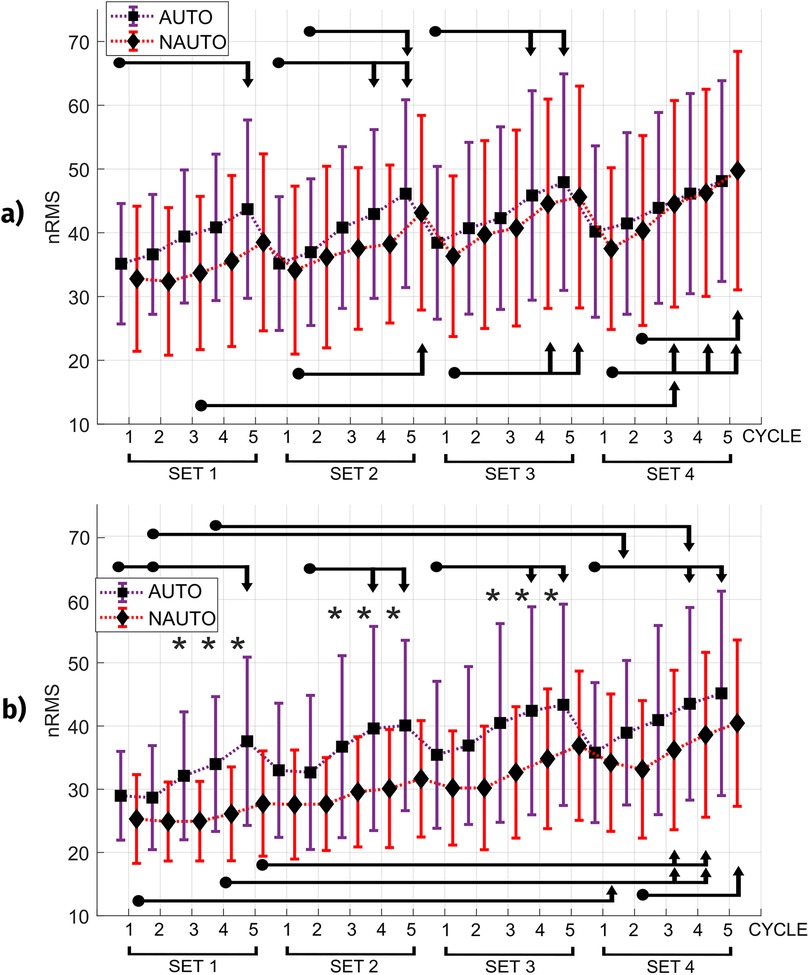
Figure 1. Normalized values of electromyographic amplitude (nRMS) for each condition. (a) Biceps brachii (b) Triceps brachii. *Indicates a difference between the two blood flow restriction conditions (AUTO and NAUTO). The start and end of the arrow indicate the compared intervals. Those at the top of the figure represent the AUTO condition, while those at the bottom represent the NAUTO condition. AUTO, autoregulated; NAUTO, non-autoregulated; nRMS, normalized root-mean-square.
The mean locations for the nRMS map centroid in the biceps and triceps brachii obtained in each BFR condition are represented in Figure 2. The biceps brachii showed no statistically significant differences between both pressure settings in spatial distribution. Regarding the displacement of the map centroid in the triceps brachii, differences between both conditions (p < 0.05) were found in both axes, with NAUTO exhibiting a cranial migration in y-axis and a lateral migration in x-axis. In addition, the modified entropy did not change.
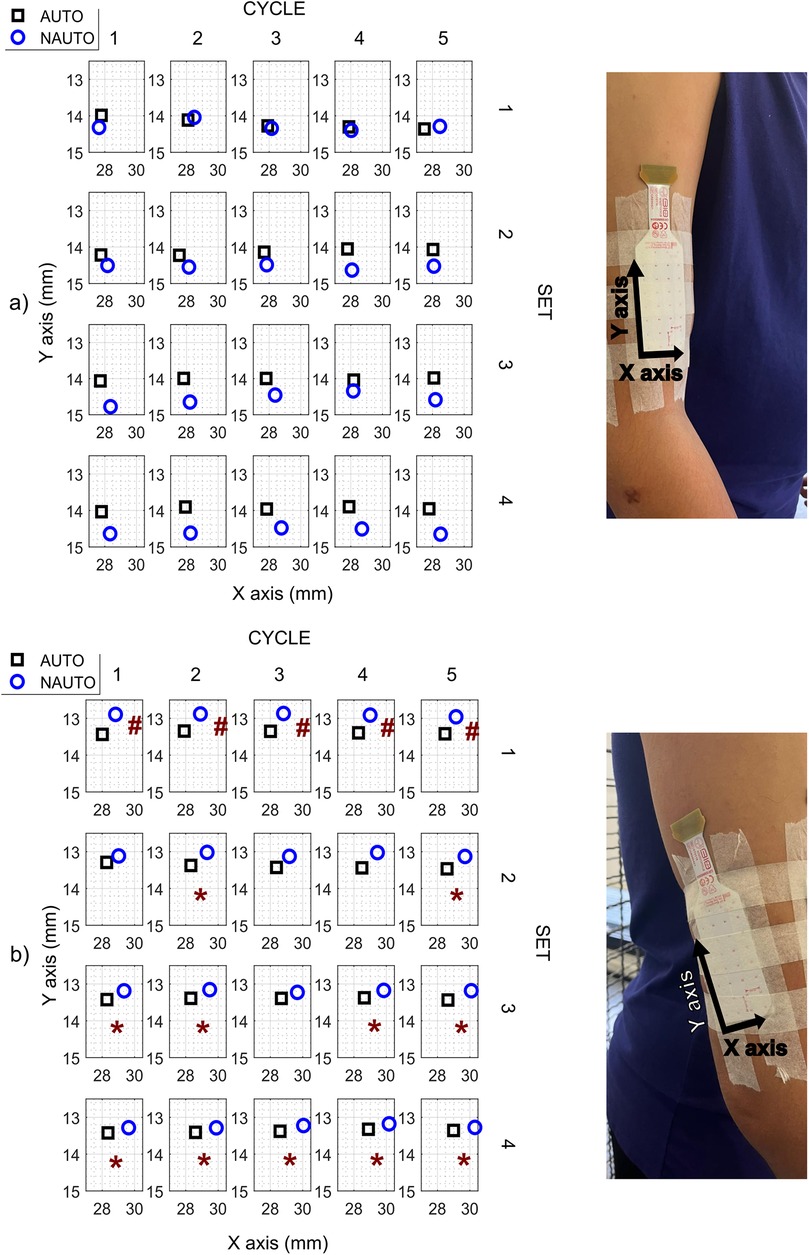
Figure 2. Mean values of normalized values of electromyographic amplitude (nRMS) maps centroid in each condition and placement of the high-density surface electromyography electrodes. (a) Biceps brachii (b) Triceps brachii. *Indicates differences on the x-axis (medial-lateral direction), while the # indicates differences on the y-axis (cranial-caudal direction) in each of the 5 cycles of each one of the 4 exercise sets. AUTO, autoregulated; NAUTO, non-autoregulated; mm, millimeters.
3.4 Perceptual responses, heart rate and oxygen saturation
The acute perceptual responses, HR and SaO2 after each exercise set of BFRT are shown in Table 3. Overall, there were no major differences between both types of BFR pressure application setting. However, compared to NAUTO, the AUTO condition increased VAS scores during each set of exercise with elbow flexion and during sets 2–4 with elbow extension. Both BFR types were equally tolerable and safe, without great increases in RPE or high pain levels.
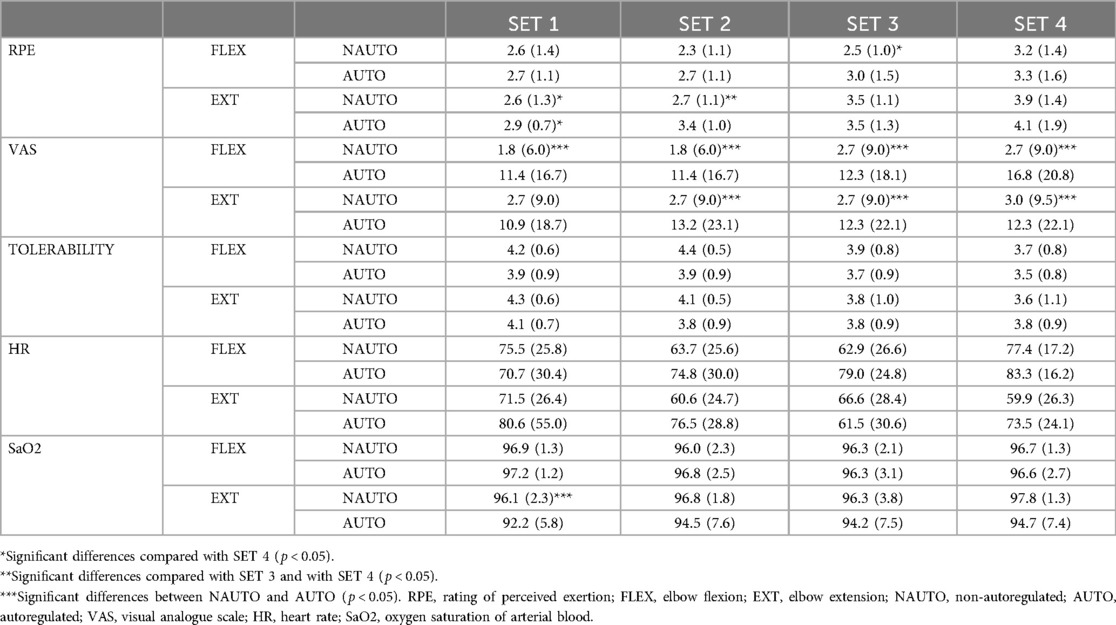
Table 3. Acute perceptual and cardiovascular responses after each set of blood flow restriction resistance training.
3.5 Adverse events
To better contextualize the safety profile of BFRT in severe PWH, adverse events as they relate to BFRT and the characteristics of PWH were considered as: (a) minor and/or expected due to BFR application (tightness in arm, itchy hand/forearm, finger congestion); (b) minor and/or expected due to resistance exercise and PWH fitness (DOMS, stiffness); (c) minor and/or expected due to the characteristics of PWH and their arthropathy status (elbow or shoulder crepitation); (d) clinically relevant concerns due to the characteristics of PWH and their arthropathy status (superficial hematoma from BFR cuff; elbow or shoulder pain; elbow or shoulder stiffness; elbow or shoulder joint bleeds; muscle bleeds). Most reports (Table 4) consisted of feeling tightness in the arm (4 NAUTO vs. 3 AUTO), with two reports from the same participant in NAUTO, two more from another in AUTO, and one in each condition from the same participant. Additionally, one participant reported tightness and elbow crepitation (due to arthropathy) in the NAUTO condition, while another one reported finger congestion in the AUTO condition. One participant reported feeling a light shoulder pain during elbow flexion exercise in AUTO. Another participant reported feeling itchiness in the hand and forearm in both conditions. Also, one participant presented a slight superficial hematoma caused by the BFR cuff (NAUTO), and another one unexpectedly suffered an insignificant superficial skin abrasion caused by the sharp edge of the EMG matrix in the elbow crease (NAUTO). Additionally, participants reported their levels of DOMS, joint pain, and stiffness after 24, 48 and 72 h. The most reported were DOMS at 24 and 48 h, especially in AUTO. Only one participant reported a slight exacerbation of his elbow extension joint pain (to a 4 on the VAS, from a baseline level of 2). Another participant reported feeling elbow stiffness (without pain) 24 h post AUTO.
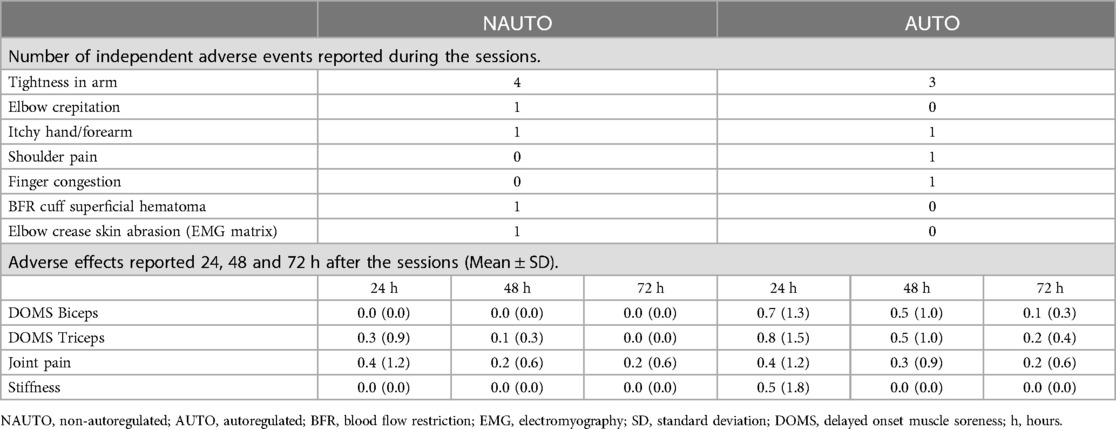
Table 4. Adverse events within 11 participants who completed all sessions.
4 Discussion
This is the first study to examine the acute safety, cardiovascular, neuromuscular and perceptual responses during AUTO and NAUTO BFRT in PWH. The main and novel findings were: (1) the AUTO condition was the only one providing a hypotensive and hypoalgesic acute response, albeit no between-group differences were found; (2) the AUTO condition induced greater triceps brachii activation in the last 3 cycles of the first 3 sets; (3) compared to NAUTO, the AUTO condition showed higher VAS scores during each set of elbow flexion exercise and during the last 3 sets of elbow extension; (4) both BFR types were equally tolerable and safe, without great increases in RPE or high pain levels; (5) no serious adverse events were reported during the experimental sessions and during the first week.
Our results support the idea that exercise can provide an acute post-exercise hypotensive response. However, this result was only evident after the AUTO condition, albeit no differences were found between conditions. A recent meta-analysis demonstrated a decrease in DBP when applying intermittent BFR with low-load upper limb training in healthy people (25). Regrettably, no previous studies evaluate pre and post exercise cardiovascular outcomes with different BFR types. Furthermore, Jacobs et al. (15) found an increase of cardiovascular outcomes (SBP, DBP, HR, MAP) during a fixed protocol with both BFR conditions in healthy individuals, albeit differences between AUTO and NAUTO were not significant. These higher cardiovascular results while training could be explained by an increase in sympathetic nervous system activity maintained and augmented via feedback from baroreceptors located in the aorta and carotid artery, as well as by stimulation of mechanically and metabolically sensitive receptors in skeletal muscle (26). Then, the acute hypotensive response produced after exercise could be explained by a reactivation of parasympathetic nervous system (26) and by reactive hyperemia (vasodilator substances increase) following cuff removal (27).
Our nRMS results show no differences between both BFR conditions in biceps brachii, but a greater activation of triceps brachii with the AUTO condition in the last 3 cycles of the first 3 sets. Partly in line, Bordessa et al. (28) found no significant differences between both BFR conditions in peak or average quadriceps EMG activity, albeit among healthy people and using different devices. Concerning the muscle activity increase, two studies (17, 28) demonstrated differences in neuromuscular activation depending on the external load, not on the cuff occlusion. However, both biceps and triceps brachii muscle activation increased progressively across the four sets conducted in our study, in accordance with previous findings evaluating a BFRT session with low-load elastic resistance (29). Unfortunately, no previous studies were conducted on PWH comparing both BFR types. We also observed shifts in the nRMS map of the triceps brachii, specifically the cranial and lateral migrations in the NAUTO condition. These shifts suggest acute adaptive responses in redistribution of activity similar to effects seen in endurance tasks in other muscle groups, such as the trapezius (30) and back muscles (31). It is thought that this redistribution of activity likely prevents localized muscle fatigue (32). However, there were no differences in entropy, indicating that the overall homogeneity in the spatial distribution of nRMS values within the electrode matrix was similar between conditions.
Concerning the acute perceptual responses, there were no major differences between both types of BFR pressure application. However, in general, we found higher RPE values during elbow extension than during elbow flexion and higher RPE during the last set, concurring with our nRMS results. A previous study performed in healthy individuals, found higher values during leg extension training with AUTO than with NAUTO (28). Furthermore, Jacobs et al. (15) found higher RPE values over time in the NAUTO device among healthy individuals in a leg extension BFR fixed protocol. Conversely, another recent study showed no differences in perceptual responses between NAUTO and AUTO in multi-joint lower body failure exercise using the Delfi device (16). Therefore, the perceptual responses elicited with AUTO/NAUTO may be device specific, region specific (e.g., upper versus lower limb), or protocol specific (e.g., fixed versus failure) and likely requires some consideration during the implementation process. Partly in line with our VAS results, Bordessa et al. (28) found higher values of pain in the AUTO condition among healthy individuals in a leg extension training protocol. However, concerns were made regarding the comparisons given the cuff design differences between conditions (33). However, our VAS values with both conditions were low, with most participants reporting no pain, which could be explained by a greater tolerance to pain in PWH, potentially due to their habituation to recurrent painful episodes associated with the condition, or by substantial variability in individual pain perception. Nevertheless, both BFR conditions were equally well tolerated. In fact, only 8 adverse events occurred during the NAUTO session, while 6 adverse events appeared during the AUTO session, none of them impeding the completion of the exercises. Some of the reported events happened in the same participants and could be explained due to the restriction of blood flow distal to the cuff location. Slightly in line with these results, Jacobs et al. (15) also found a higher number of adverse events (presyncopal symptoms, numbness in leg and exercise intolerance) during NAUTO training sessions, with presyncopal symptoms as the most common event. However, in our study, the adverse events did not impede participants to complete the session, while in the Jacobs et al. (15) study 10 participants stopped exercising due to presyncopal symptoms during sessions. After all, no bleeding events were reported during our study nor in the first week post sessions, which is the most important finding in terms of safety for PWH. All in all, our findings infer that both types of BFR can be used, potentially informing clinical decision-making in hemophilia care, physiotherapy or exercise prescription contexts. However, specialists should consider using AUTO to increase triceps activation and when cardiovascular responses are relevant to patients. Additionally, the EMG activity spatial distribution variability seen with NAUTO seems to reflect a necessity to compensate a superior accumulation of metabolic stress and peripheral fatigue possibly due to impaired contractile function because of the higher pressures applied to the limb.
Our study is not without limitations. The number of participants was small, although HDsEMG has high reliability, and measurements were conducted among patients with a rare disease. In addition, differentiating concentric and eccentric phases could provide deeper insights into task-specific neuromuscular control. However, in our rehabilitation context, we prioritized the magnitude of the EMG activity. Given the modest sample size and the use of a medium effect size in our power analysis, there remains a risk of Type II error. Consequently, null findings should be interpreted with caution, as the study may not have been sufficiently powered to detect smaller, yet potentially meaningful, effects. Albeit BFRT is safe among PWH during a small number of sessions, specialists should carefully consider tailored prophylaxis for individual participation. The current findings reflect the acute responses of two sessions of BFRT. Future studies should evaluate the long-term adaptations to BFRT in PWH, as cardiovascular, neuromuscular, and perceptual effects may differ after repeated sessions due to adaptation, sensitization, or cumulative effects (e.g., joint stress in hemophilia).
5 Conclusions
AUTO and NAUTO conditions at 50% LOP appear to be equally tolerable and safe in severe PWH, under prophylaxis treatment, during an upper limb standard BFRT protocol, without great increases in RPE or pain. However AUTO showed trends for improved cardiovascular and neuromuscular responses. AUTO condition induced a hypotensive and hypoalgesic acute response, albeit no between-group differences were found. The AUTO condition resulted in increased muscular activation in the triceps brachii during the final cycles of the first sets, as well as higher VAS scores. The current findings reflect the acute responses to BFRT and long-term responses in PWH may differ due to adaptation, sensitization, or cumulative effects.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study involving humans was approved by The Ethics Committee of Research in Humans of the Ethics Commission in Experimental Research of University of Valencia (reference: UV-INV_ETICA-2334229). The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DCO: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft. AT-B: Data curation, Investigation, Writing – original draft. NR: Methodology, Writing – review & editing. JJC: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft. CC-M: Methodology, Writing – review & editing. JC: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft. SB: Resources, Writing – review & editing. SP-A: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The authors declare that this study received funding from Pfizer, under a research grant (75061703), paid to the institution. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Acknowledgments
The authors thank all the patients who participated in this research for their contribution. An unrestricted clinical research grant was provided by Pfizer for the conduct of the study, paid to the institution. Pfizer had no input on the content of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Srivastava A, Santagostino E, Dougall A, Kitchen S, Sutherland M, Pipe SW, et al. WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia. (2020) 26(S6):1–158. doi: 10.1111/hae.14046
2. Gualtierotti R, Solimeno LP, Peyvandi F. Hemophilic arthropathy: current knowledge and future perspectives. J Thromb Haemost. (2021) 19(9):2112–21. doi: 10.1111/jth.15444
3. Blamey G, Forsyth A, Zourikian N, Short L, Jankovic N, De Kleijn P, et al. Comprehensive elements of a physiotherapy exercise programme in haemophilia–a global perspective. Haemoph Off J World Fed Hemoph. (2010) 16(Suppl 5):136–45. doi: 10.1111/j.1365-2516.2010.02312.x
4. Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. (2011) 43(7):1334–59. doi: 10.1249/MSS.0b013e318213fefb
5. Grønfeldt BM, Lindberg Nielsen J, Mieritz RM, Lund H, Aagaard P. Effect of blood-flow restricted vs heavy-load strength training on muscle strength: systematic review and meta-analysis. Scand J Med Sci Sports. (2020) 30(5):837–48. doi: 10.1111/sms.13632
6. Lixandrão ME, Ugrinowitsch C, Berton R, Vechin FC, Conceição MS, Damas F, et al. Magnitude of muscle strength and mass adaptations between high-load resistance training versus low-load resistance training associated with blood-flow restriction: a systematic review and meta-analysis. Sports Med Auckl NZ. (2018) 48(2):361–78. doi: 10.1007/s40279-017-0795-y
7. Patterson SD, Hughes L, Warmington S, Burr J, Scott BR, Owens J, et al. Blood flow restriction exercise: considerations of methodology, application, and safety. Front Physiol. (2019) 10:533. doi: 10.3389/fphys.2019.00533
8. Pearson SJ, Hussain SR. A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy. Sports Med Auckl NZ. (2015) 45(2):187–200. doi: 10.1007/s40279-014-0264-9
9. Perera E, Zhu XM, Horner NS, Bedi A, Ayeni OR, Khan M. Effects of blood flow restriction therapy for muscular strength, hypertrophy, and endurance in healthy and special populations: a systematic review and meta-analysis. Clin J Sport Med Off J Can Acad Sport Med. (2022) 32(5):531–45. doi: 10.1097/JSM.0000000000000991
10. Ucero-Lozano R, López-Pina JA, Ortiz-Pérez A, Cuesta-Barriuso R. The relationship between chronic pain and psychosocial aspects in patients with haemophilic arthropathy. A cross-sectional study. Haemoph Off J World Fed Hemoph. (2022) 28(1):176–82. doi: 10.1111/hae.14469
11. Hoelting BD, Scheuermann BW, Barstow TJ. Effect of contraction frequency on leg blood flow during knee extension exercise in humans. J Appl Physiol. (2001) 91(2):671–9. doi: 10.1152/jappl.2001.91.2.671
12. Lutjemeier BJ, Miura A, Scheuermann BW, Koga S, Townsend DK, Barstow TJ. Muscle contraction-blood flow interactions during upright knee extension exercise in humans. J Appl Physiol. (2005) 98(4):1575–83. doi: 10.1152/japplphysiol.00219.2004
13. Hughes L, Rosenblatt B, Gissane C, Paton B, Patterson SD. Interface pressure, perceptual, and mean arterial pressure responses to different blood flow restriction systems. Scand J Med Sci Sports. (2018) 28(7):1757–65. doi: 10.1111/sms.13092
14. Hughes L, Swain PM, Lai T, McEwen JA. It’s time to regulate—the importance of accurate surgical-grade tourniquet autoregulation in blood flow restriction exercise applications. Phys Ther Sport. (2024) 67:41–6. doi: 10.1016/j.ptsp.2024.02.001
15. Jacobs E, Rolnick N, Wezenbeek E, Stroobant L, Capelleman R, Arnout N, et al. Investigating the autoregulation of applied blood flow restriction training pressures in healthy, physically active adults: an intervention study evaluating acute training responses and safety. Br J Sports Med. (2023) 57(14):914–20. doi: 10.1136/bjsports-2022-106069
16. Rolnick N, Licameli N, Moghaddam M, Marquette L, Walter J, Fedorko B, et al. Autoregulated and non-autoregulated blood flow restriction on acute arterial stiffness. Int J Sports Med. (2024) 45(1):23–32. doi: 10.1055/a-2152-0015
17. Calatayud J, Ogrezeanu DC, Carrasco JJ, Martinez-Valdes E, Pérez-Alenda S, Cruz-Montecinos C, et al. Safety, feasibility, and neuromuscular activity of acute low-load resistance exercise with or without blood flow restriction in patients with severe hemophilia. Eur J Haematol. (2023) 111(1):47–56. doi: 10.1111/ejh.13965
18. Ogrezeanu DC, Calatayud J, Rodríguez S, Carrasco JJ, Martinez-Valdes E, Casaña J, et al. Acute neuromuscular and perceptual responses to blood flow restriction exercise in adults with severe haemophilia: a pilot study. Haemophilia. (2024) 30(5):1193–202. doi: 10.1111/hae.15084
19. Buckley JP, Borg GAV. Borg’s scales in strength training; from theory to practice in young and older adults. Appl Physiol Nutr Metab Physiol Appl Nutr Metab. (2011) 36(5):682–92. doi: 10.1139/h11-078
20. Barbero M, Merletti R, Rainoldi A. Atlas of Muscle Innervation Zones. Milano: Springer Milan (2012). Available online at: http://link.springer.com/10.1007/978-88-470-2463-2 (Accessed April 15, 2021).
21. Abbas MJ, Dancy ME, Marigi EM, Khalil LS, Jildeh TR, Buckley PJ, et al. An automated technique for the measurement of limb occlusion pressure during blood flow restriction therapy is equivalent to previous gold standard. Arthrosc Sports Med Rehabil. (2022) 4(3):e1127–32. doi: 10.1016/j.asmr.2022.04.002
22. Sundstrup E, Jakobsen MD, Andersen CH, Zebis MK, Mortensen OS, Andersen LL. Muscle activation strategies during strength training with heavy loading vs. repetitions to failure. J Strength Cond Res. (2012) 26(7):1897–903. doi: 10.1519/JSC.0b013e318239c38e
23. Marri K, Swaminathan R. Analysis of concentric and eccentric contractions in biceps brachii muscles using surface electromyography signals and multifractal analysis. Proc Inst Mech Eng. (2016) 230(9):829–39. doi: 10.1177/0954411916654198
24. Moore D, Semciw AI, McClelland J, Wajswelner H, Pizzari T. Rehabilitation exercises for the gluteus Minimus muscle segments: an electromyography study. J Sport Rehabil. (2019) 28(6):544–51. doi: 10.1123/jsr.2017-0262
25. Lemos LK, Toledo Teixeira Filho CA, Biral TM, de Souza Cavina AP, Junior EP, Oliveira Damasceno Sd, et al. Acute effects of resistance exercise with blood flow restriction on cardiovascular response: a meta-analysis. J Comp Eff Res. (2022) 11(11):829–42. doi: 10.2217/cer-2021-0272
26. Fu Q, Levine BD. Exercise and the autonomic nervous system. Handb Clin Neurol. (2013) 117:147–60. doi: 10.1016/B978-0-444-53491-0.00013-4
27. Tschakovsky ME, Rogers AM, Pyke KE, Saunders NR, Glenn N, Lee SJ, et al. Immediate exercise hyperemia in humans is contraction intensity dependent: evidence for rapid vasodilation. J Appl Physiol. (2004) 96(2):639–44. doi: 10.1152/japplphysiol.00769.2003
28. Bordessa JM, Hearn MC, Reinfeldt AE, Smith TA, Baweja HS, Levy SS, et al. Comparison of blood flow restriction devices and their effect on quadriceps muscle activation. Phys Ther Sport. (2021) 49:90–7. doi: 10.1016/j.ptsp.2021.02.005
29. Yasuda T, Fukumura K, Fukuda T, Iida H, Imuta H, Sato Y, et al. Effects of low-intensity, elastic band resistance exercise combined with blood flow restriction on muscle activation. Scand J Med Sci Sports. (2014) 24(1):55–61. doi: 10.1111/j.1600-0838.2012.01489.x
30. Farina D, Leclerc F, Arendt-Nielsen L, Buttelli O, Madeleine P. The change in spatial distribution of upper trapezius muscle activity is correlated to contraction duration. J Electromyogr Kinesiol. (2008) 18(1):16–25. doi: 10.1016/j.jelekin.2006.08.005
31. Sanderson A, Martinez-Valdes E, Heneghan NR, Murillo C, Rushton A, Falla D. Variation in the spatial distribution of erector spinae activity during a lumbar endurance task in people with low back pain. J Anat. (2019) 234(4):532–42. doi: 10.1111/joa.12935
32. Falla D, Gizzi L, Tschapek M, Erlenwein J, Petzke F. Reduced task-induced variations in the distribution of activity across back muscle regions in individuals with low back pain. Pain. (2014) 155(5):944–53. doi: 10.1016/j.pain.2014.01.027
Keywords: electromyography, resistance training, ischemic preconditioning, hemarthrosis, hemophilia A
Citation: Ogrezeanu DC, Tur-Boned A, Rolnick N, Carrasco JJ, Cruz-Montecinos C, Calatayud J, Bonanad S and Pérez-Alenda S (2025) Acute safety, cardiovascular, perceptual and neuromuscular responses to autoregulated and non-autoregulated blood flow restriction training during elbow rehabilitation in people with hemophilia. Front. Sports Act. Living 7:1587615. doi: 10.3389/fspor.2025.1587615
Received: 4 March 2025; Accepted: 14 July 2025;
Published: 31 July 2025.
Edited by:
Giuseppe D'Antona, University of Pavia, ItalyReviewed by:
Cleiton Augusto Libardi, Federal University of São Carlos, BrazilMarta Sevilla-Sanchez, University of A Coruña, Spain
Copyright: © 2025 Ogrezeanu, Tur-Boned, Rolnick, Carrasco, Cruz-Montecinos, Calatayud, Bonanad and Pérez-Alenda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joaquín Calatayud, am9hcXVpbi5jYWxhdGF5dWRAdXYuZXM=