 Stian Langgård Jørgensen1,2,3,4*
Stian Langgård Jørgensen1,2,3,4* Signe Kierkegaard2,3,4
Signe Kierkegaard2,3,4 Marie Bagger Bohn2,3,4
Marie Bagger Bohn2,3,4 Per Aagaard5Inger Mechlenburg4,6
Per Aagaard5Inger Mechlenburg4,6- 1Department of Occupational and Physical Therapy, Horsens Regional Hospital, Horsens, Denmark
- 2Horsens Research Centre - Hip Training & Preservation Surgery (H-HIP), Department of Occupational and Physical Therapy, Horsens Regional Hospital, Horsens, Denmark
- 3Department of Orthopedic Surgery, Horsens Regional Hospital, Horsens, Denmark
- 4Department of Clinical Medicine, Aarhus University, Aarhus, Denmark
- 5Department of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, Denmark
- 6Department of Orthopedic Surgery, Aarhus University Hospital, Aarhus, Denmark
Objective: To evaluate the effectiveness of pre-operative resistance training in patients allocated to TJR surgery on selected post-operative outcomes, via a meta-analysis of studies using exercise modalities and loading intensities objectively known to promote gains in muscle size and strength in adults of young-to-old age.
Design: A systematic review and meta-analysis.
Literature Search: Cochrane Central, MEDLINE, EMBASE, and PEDro were searched on August 4th 2021.
Study Selection: Randomized Controlled Trials (RCTs) were included if (i) they compared pre-operative lower-limb-exercises before elective TJR with standard care, (ii) explicitly reported the exercise intensity, and (iii) reported data on functional performance.
Data Synthesis: This systematic review and meta-analysis is reported in accordance with the PRISMA reporting guidelines. A random effects model with an adjustment to the confidence interval was performed for pooling the data.
Results: One thousand studies were identified. After applying exclusion criteria, five RCTs were located including 256 participants (mean age ranged from 61 to 72 years, 54% women). Moderate-to-large improvements in functional performance and maximal knee extensor strength were observed at 3 months after surgery along with small-to-moderate effects 12 months post-operatively. For patient-reported outcomes, small-to-moderate improvements were observed at 3 months post-operatively with no-to-small improvements at 12 months.
Conclusion: Prehabilitation efforts involving progressive resistance training provides an effective means to improve post-operative outcomes related to functional performance, knee extensor strength and patient-reported outcome in patients undergoing TJR. Due to large methodological diversity between studies, an optimal loading intensity remains unknown.
Systematic Review Registration: Prospero ID: CRD42021264796.
Introduction
Total knee or hip replacement surgery (TJR) is typically offered to patients to reduce joint pain and increase quality of life (Skoffer et al., 2015; Moyer et al., 2017). However, up to 20% of the patients report a non-optimal outcome after surgery due to insufficient pain relief and/or persistent deficits in functional capacity (Moyer et al., 2017; Franz et al., 2018). In fact, functional performance and muscle strength have been observed to remain below levels of healthy age-matched adults even years after surgery (Mizner et al., 2005; Bade et al., 2010).
The prevalence of TJR procedures is increasing internationally (Moyer et al., 2017; Odgaard et al., 2020a,b) with an projected growth of 174% THR- and 673% TKR-procedures from 2005 to 2030 in the United States alone (Kurtz et al., 2007). Thus, efficient and safe treatment paradigms seem highly warranted.
Preoperative exercise-based training (prehabilitation) has been suggested as an essential component, attributing to a fast recovery after TJR (Franz et al., 2018; Ghosh and Chatterji, 2018; Lim and Thahir, 2021). However, often with limited pre-operative time from accepting surgery to the day-of-surgery (i.e., 4–12 weeks), it is reasonable to address impairments expected to have significant impact on the post-operative outcome, such as lower limb muscle mass and strength. In support of this notion, both pre-operative functional performance and lower limb muscle strength have each been positively associated with post-operative functional performance up to 2 years post-operatively in patients receiving TJR (Fortin et al., 1999; Bade et al., 2010; Zeni and Snyder-Mackler, 2010; Holstege et al., 2011; Nankaku et al., 2013; Skoffer et al., 2015). Thus, despite involving different surgical procedures and affecting different muscle groups, both patient populations (TKR, THR) are likely to benefit from exercise interventions that aim at increasing lower limb muscle strength and improving functional performance.
Progressive resistance training (PRT) is commonly referred to as the Gold Standard intervention modality for promoting consistent gains in mechanical muscle function in healthy individuals (Garber et al., 2011). Also, PRT is often applied in older adults and selected orthopedic populations using loading intensities ranging from ~60–85% 1 repetition maximum (1 RM), typically leading to substantial improvements in functional performance, muscle strength and muscle hypertrophy (Suetta, 2004; Aagaard et al., 2010; Steib et al., 2010; Borde et al., 2015; Csapo and Alegre, 2016; Skoffer et al., 2016; Ferraz et al., 2018; Hughes et al., 2019). Notably, novel training approaches using lower exercise loads and concurrent restriction of blood flow to the exercising limb such as low-load blood flow restricted exercise appear effective also regarding increasing skeletal muscle strength and improving functional performance in patients suffering from knee OA (Segal N. A. et al., 2015; Segal N. et al., 2015; Bryk et al., 2016; Ferraz et al., 2018).
Previous systematic reviews and meta-analyses have generally observed no-to-little evidence in favor of prehabilitation after TJR surgery (Kwok et al., 2015; Wang et al., 2016; Chesham and Shanmugam, 2017; Husted et al., 2020) with the overall evidence of moderate-to-low methodological quality (Kwok et al., 2015; Skoffer et al., 2015; Chesham and Shanmugam, 2017; Moyer et al., 2017). However, no restrictions on the specific loading/exercise intensity (%1 RM) employed in these reviews (Kwok et al., 2015; Skoffer et al., 2015; Wang et al., 2016; Chesham and Shanmugam, 2017; Moyer et al., 2017; Husted et al., 2020). To remove the noise from exercise interventions of insufficient (i.e., too low) exercise intensities, the present systematic review and meta-analysis aimed to evaluate the effectiveness of pre-operative training in patients scheduled for elective TJR using exercise modalities and loading intensities objectively known to promote gains in muscle size and strength in the spectrum of healthy populations of young-to-old age.
Methods
The review was conducted in accordance with PRISMA statement guidelines (Moher et al., 2015) and was registered at the International Prospective Register of Systematic Reviews (PROSPERO): CRD42021264796.
Search Strategy
A literature search was conducted at the Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, and the Physiotherapy Evidence Database on August 4th 2021. As our institutions did not hold the rights to complete searches in The Allied and Complementary Database, it was not possible to accommodate this element of the PROSPERO protocol.
Search terms are presented in Supplementary File 1.
Two authors (SLJ, SK) independently screened titles and abstracts to identify potentially eligible trials based on predetermined criteria. The full text of potentially eligible papers was retrieved and independently assessed by the same two authors to determine eligibility. Any disagreements were resolved via consensus or by consulting a third author (IM) when necessary.
Eligibility Criteria
Studies were eligible for inclusion in the present meta-analysis if fulfilling the following criteria: (i) involving a randomized controlled trial (RCT) design, (ii) written in English, (iii) comparing the post-operative effect of pre-operative lower-limb PRT exercise performed prior to TJR to usual care or control interventions, (iv) containing specific information about the exercise intensity, and (v) including data on functional performance. Trials were excluded if: not designed as a RCT, including participants scheduled for TJR for other reasons than OA (i.e., rheumatoid arthritis or trauma), or if not reporting exercise intensity for the intervention group(s).
Inclusion Exclusion Criteria
Inclusion criteria were trials that used exercise paradigms designed and implemented to increase lower limb muscle strength and promote skeletal muscle hypertrophy (Steib et al., 2010; Borde et al., 2015; Patterson et al., 2019). Before initiating the literature search, we specified the original criteria outlined in our PROSPERO registration protocol to comprise studies utilizing (i) resistance exercises with loading intensities ≥60% 1 RM, (ii) resistance training employing moderate-to-low load intensities (<60% 1 RM) performed to concentric contraction failure in at least the final exercise set in each exercise, or (iii) exercising with low loads and concurrent blood flow restriction for the exercising limb (Kim et al., 2017).
Co-interventions, including patient education, mobilization, manipulation, massage therapies, glucocorticoid injection, analgesia, balance training, knee and hip joint mobility exercises were allowed, except if dose/exposure was distributed unequally between the intervention and control groups, in which case studies were excluded from the analysis.
Comparator Groups
Included studies were allowed to use control groups allocated to usual care or control interventions.
Outcome Measures
To assess the effectiveness of the pre-operative intervention procedures, the present meta-analysis included the following functional performance tests: (i) Sit-to-stand tests, (ii) Ambulatory function assessed by the Timed Up & Go test (Alghadir et al., 2015), (iii) Stair climbing test, (iv) habitual horizontal walking speed, and (v) maximal isometric voluntary knee extensor muscle strength assessed either using isokinetic dynamometry or hand held dynamometry (Aagaard et al., 2002; Koblbauer et al., 2011).
Duration of time to follow-up was characterized as medium-term (2–4 months) or long-term (10–12 months or longer). If a study reported both medium-term and long-term outcome data, data from both time points were extracted. If the same RCT divided the reporting of medium-term and long-term follow-up data into separate publications, the results were used separately in the relevant meta-analysis. Further, functional tests measuring time required to perform a pre-set number of repetitions (i.e., 5 times sit-to-stand test) were converted into repetitions per second to allow a standardized analysis, with increasing values representing enhanced test performance in all cases. The specific conversion was performed using the following equation on the raw dataset [online Supplementary Material (Holsgaard-Larsen et al., 2020)]: .
Quality Assessment
Risk of Bias (RoB) assessments (Figure 1) were performed using the Cochrane Collaboration's tool for assessing RoB, as described in detail previously (Higgins et al., 2019). The RoB assessment scores on the reporting of judgement items were: (i) Adequate (Bias, if present, is unlikely to alter the results seriously), (ii) Unclear (A risk of bias that raises some doubt about the results), and (iii) Inadequate (Bias may alter the results seriously), corresponding with (i) low, (ii), unclear, and (iii) high risk of bias, respectively (Grønfeldt et al., 2020).
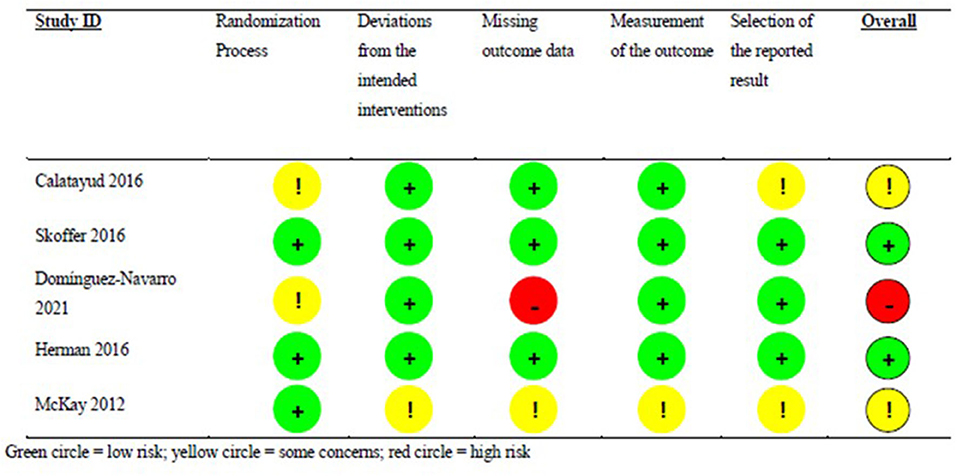
Figure 1. Risk of Bias Assessment for each individual study. Green circle, low risk; yellow circle, some concerns; red circle, high risk.
The RoB analysis included five distinct aspects of reporting: the randomization process, deviations from the intended intervention, missing outcome data, measurement of the outcome variables, and selected reporting of the obtained results.
RoB was performed independently by two reviewers (SJ, IM) and discrepancies were resolved through discussion until reaching consensus. As IM coauthored Skoffer et al. (2016, 2020), the RoB assessment was performed by SJ and PA.
The Grades of Recommendation, Assessment, Development and Evaluation (GRADE) scheme (Atkins et al., 2004; Guyatt et al., 2008) was used to assess the quality of evidence in the performed meta-analyses. The overall GRADE certainty ratings include “very low,” “low,” “moderate,” and “high” (Brignardello-Petersen et al., 2018).
Data Extraction, Synthesis, and Analysis
Two authors (SJ, SK) both extracted data from each study by following a predefined scheme. Data were cross-checked for differences in data-extraction and discrepancies were resolved through discussion until agreement was reached. Otherwise, a third author was consulted until consensus was reached (MB).
The following data were extracted from each study:
1. Trial characteristics (sample size, first author name, year of publication, type of trial, country, source of funding, trial registration status, reported sources of bias/conflicts of interest).
2. Participant characteristics (inclusion and exclusion criteria, age, sex, body mass).
3. Intervention procedures, including exercise.
4. Comparator/control group intervention, exercise characteristics if applicable.
5. Co-interventions, if any, reported for each group.
6. Outcomes variables reported, including time of assessment.
Due to the small number of included trials, the meta-analyses were performed using a random effects model with an adjustment to the confidence interval proposed by IntHout et al. (2014) computing the effect size (Hedges' g) of the included prehabilitation intervention protocols compared with their respective control group (Higgins et al., 2019). Results were extracted in form of post-intervention group mean data, standard deviation (SD) and sample size as inputs for the meta-analyses. In case of incomplete data, means and SDs were extrapolated from article graphs (WebPlotDigitizer 4.5).
As we assume outcome variables to be in collected in different units across studies, data are presented as standardized mean difference (SMD) along with their respective 95% confidence intervals (CI). For interpretation of the SMD, the following definitions were adopted: >0.2 small effect, >0.5 moderate effect, >0.8 large effect (Cohen, 2013).
Heterogeneity between the included studies was assessed using the I2 statistics and interpreted as low (I2 = 0–30%), moderate (I2 = 30–60%) and high (I2 ≥ 60%) heterogeneity (Higgins et al., 2003, 2019). All statistical analyses were conducted in Stata 17.0 (StataCorp, TX, USA).
Results
Summary of Findings
We identified 1,000 hits from the literature search performed on August 4th 2021. After removing duplicates, 672 potentially eligible trials were identified (Figure 2). Following title and abstract screening, 605 records were excluded while 66 records remained for full-text reading. A total of 59 records were excluded for not meeting the inclusion criteria, leaving a total of seven studies to be included in the present analysis. Four trials reported baseline and short-term follow-up data on patients scheduled for TKR: McKay et al. (2012), Calatayud et al. (2016), Skoffer et al. (2016), and (Domínguez-Navarro et al. 2021) and a single study reported baseline and short-term follow-up data on patients scheduled for THR: Hermann et al. (2015). In addition, two articles reported long-term follow-up data based on the above studies, namely: Skoffer et al. (2020) [follow-up data based on Skoffer et al. (2016)] and Holsgaard-Larsen et al. (2020) [follow-up data based on Hermann et al. (2015)]. Ultimately, seven papers were deemed eligible in the present meta-analyses. However, since each study trial only could be counted once in each seperate analysis, a maximum of five trials per analysis was possible. Data from Hermann et al. (2015) and Holsgaard-Larsen et al. (2020) were extracted from available Supplementary Spread Sheet Files (Holsgaard-Larsen et al., 2020).
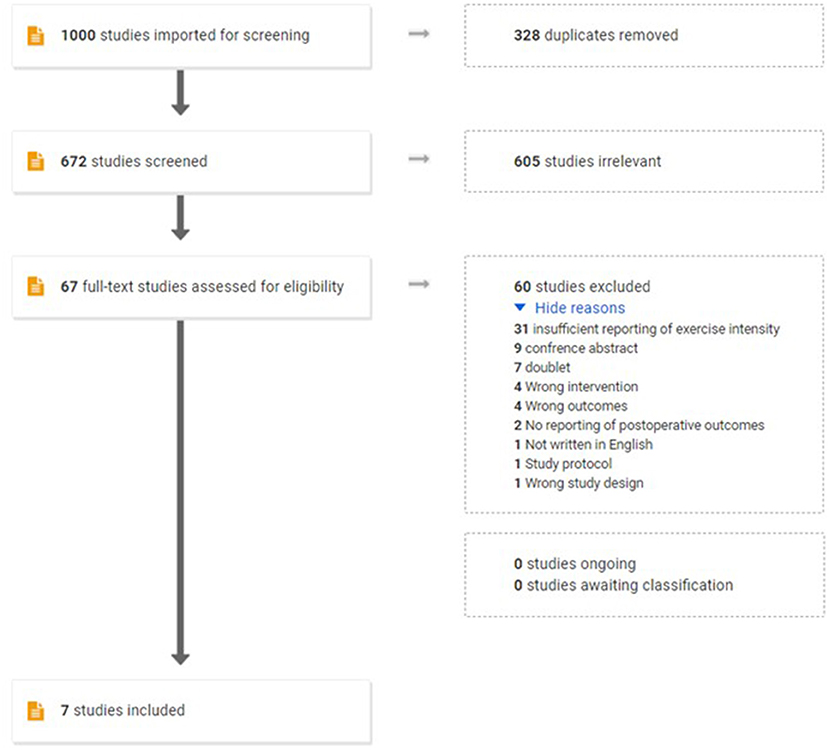
Figure 2. Flow chart of the study selection process.
According to our preregistered Prospero protocol (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=264796), it was the explicit study aim to investigate the effect of pre-operative resistance training (PRT) on the post-operative recovery following total knee replacement (TKR) as well as hip replacement (THR). To adhere to the Prospero protocol, we have retained the single trial on THR in our analysis.
Trial, Participants, and Intervention Characteristics
Individual study characteristics are summarized in Table 1. A total of 256 patients scheduled for TJR were included in the meta-analysis (176 TKR/80 THR). Mean age was 61–72 years and 54% of the participants were women. Four trials provided usual care (Hermann et al., 2015; Calatayud et al., 2016; Skoffer et al., 2016; Domínguez-Navarro et al., 2021) while one trial involved control intervention (McKay et al., 2012) in the control group. Two trials utilized a percentage of 1 RM to quantify training load intensity (McKay et al., 2012; Domínguez-Navarro et al., 2021), while three trials controlled loading intensity by adjusting exercise loads to target a certain number of repetitions when performed to contraction failure (Hermann et al., 2015; Calatayud et al., 2016; Skoffer et al., 2016). Training periods ranged from 4 to 10 weeks 2–3 times per week. All exercise sessions were supervised in all trials. Baseline, 3- and 12-month follow-up assessments for all included studies are reported in Table 2. As all medium-term data were collected at 3 months post-operatively and all long-term data were collected at 12, 3, and 12 months were used in the following sections as temporal terms to denote “medium-term” and “long-term” effects, respectively. Only Holsgaard-Larsen et al. (2020) reported findings 5–7 months post-operatively. Therefore, we decided to exclude this intermediate time point from the present analysis. Also, stair climbing performance, knee flexor strength, and hip extensor and flexor strength were reported by a single study only at 12 months post-operatively. Therefore, these time points for these particular outcome variables were excluded from the present long-term (12 month) analysis. None of the studies assessed markers related to skeletal muscle mass.

Table 1. Trial characteristics of the five included randomized controlled trials.
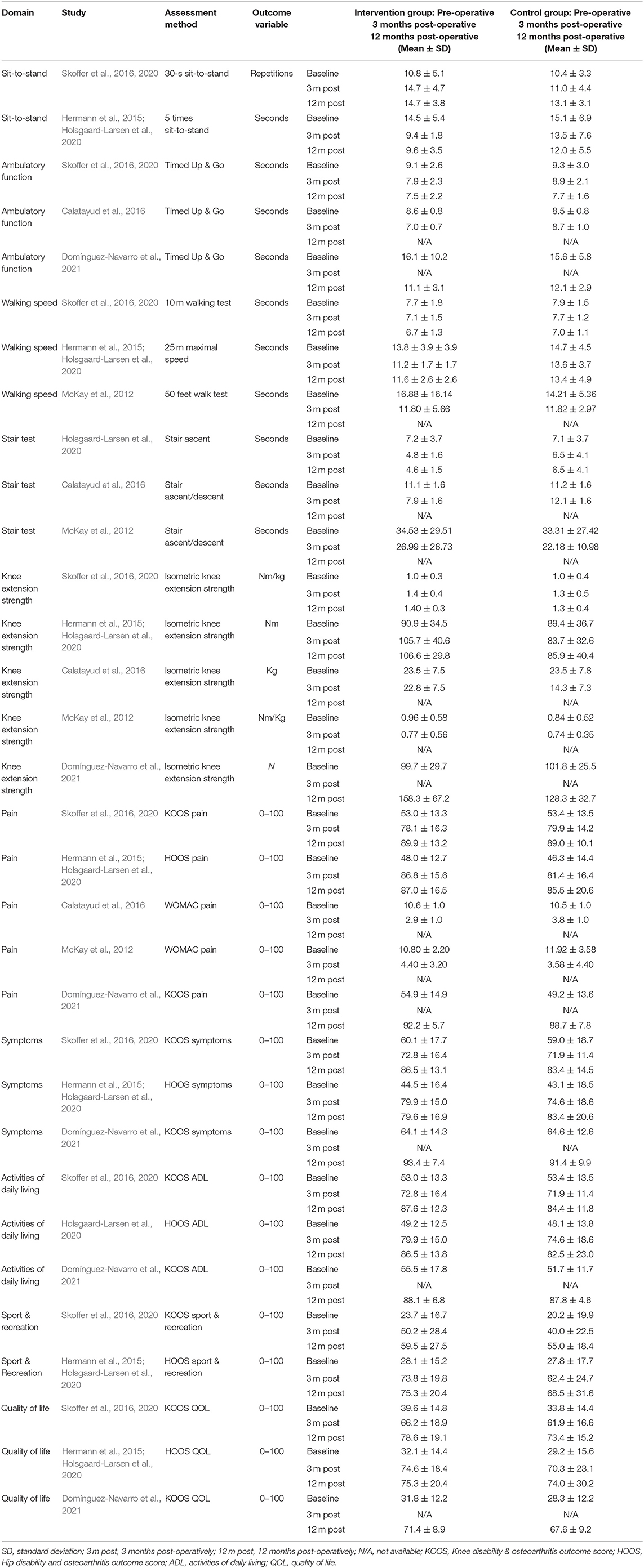
Table 2. Outcome variables from each individual trial.
Risk of Bias Assessement and Grade Assessment
RoB assessments for all included trials are presented in Figure 1. RoB was judged low for Hermann et al. (2015) and Skoffer et al. (2016). Some concerns were noted with regard to the randomization process, the selection of reported results, and missing information on pre-registration in Calatayud et al. (2016). Likewise, concerns regarding the randomization process was noted for (Domínguez-Navarro et al. 2021), along with high risk of bias with regard to missing outcome data. Finally, concerns with regards to deviations from the intended intervention procedures, missing outcome data, measurements of outcome variables, and selection of reported results were noted for McKay et al. (2012).
The level of certainty in evidence was rated low-to-very low for all outcome variables, mainly due to moderate-to-high risks of bias (Table 3).
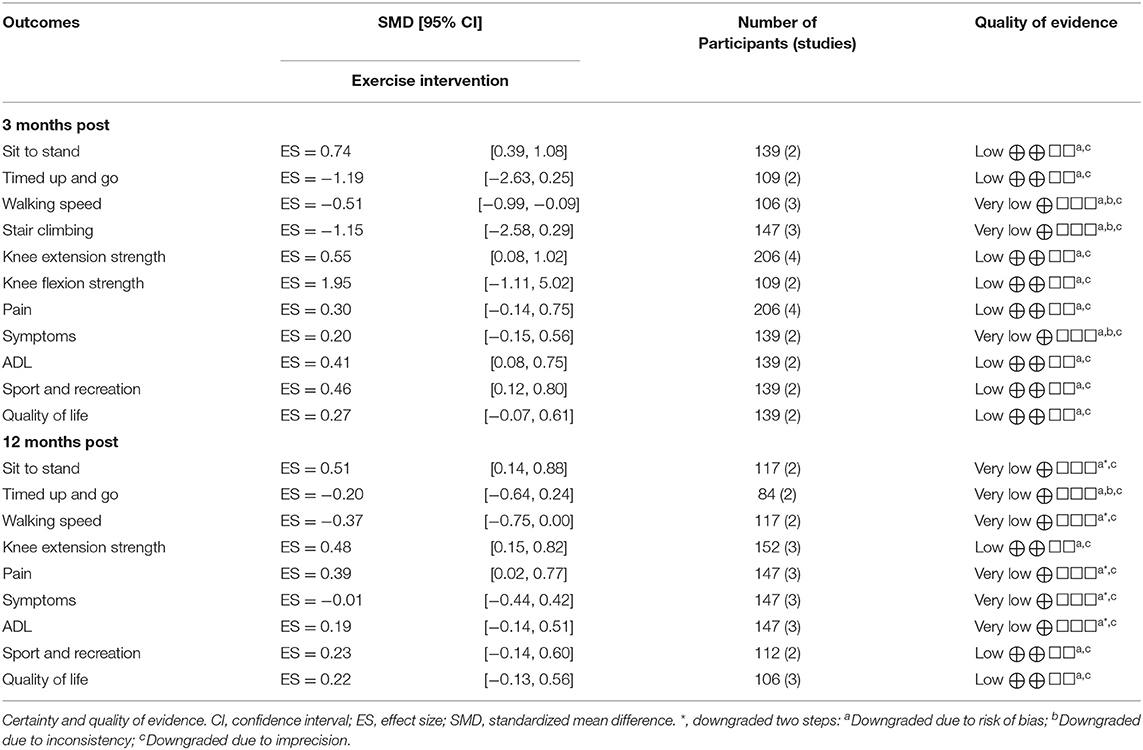
Table 3. Meta-analysis results.
Effects of Prehabilitation vs. Standard Care or Control Intervention on Functional Performance, Knee Extensor and Flexor Strength, and Patient-Reported Outcomes
A total of 6 studies were included in the meta-analyses. We conducted seven meta-analyses comparing prehabilitation with usual care or control intervention 3 months post-operative on sit-to-stand performance (Skoffer et al., 2016; Holsgaard-Larsen et al., 2020), Timed Up&Go (Calatayud et al., 2016; Skoffer et al., 2016), walking speed (McKay et al., 2012; Skoffer et al., 2016; Holsgaard-Larsen et al., 2020), stair climbing (McKay et al., 2012; Calatayud et al., 2016; Holsgaard-Larsen et al., 2020), and 12 months post-operative for sit-to-stand performance (Holsgaard-Larsen et al., 2020; Skoffer et al., 2020), Timed Up & Go (Skoffer et al., 2020; Domínguez-Navarro et al., 2021), and walking speed (Holsgaard-Larsen et al., 2020; Skoffer et al., 2020). We conducted three meta-analyses comparing the effect of prehabilitation with usual care or control intervention on knee extensor 3 months post-operatively (McKay et al., 2012; Calatayud et al., 2016; Skoffer et al., 2016; Holsgaard-Larsen et al., 2020), knee flexor strength 3 months post-operatively (Calatayud et al., 2016; Skoffer et al., 2016), and knee extensor strength 12 months post-operatively (Holsgaard-Larsen et al., 2020; Skoffer et al., 2020; Domínguez-Navarro et al., 2021); and ten meta-analyses on pain assessed at 3 months (McKay et al., 2012; Calatayud et al., 2016; Skoffer et al., 2016) and 12 months post-operatively (Holsgaard-Larsen et al., 2020; Skoffer et al., 2020; Domínguez-Navarro et al., 2021), symptoms 3 months (Skoffer et al., 2016; Holsgaard-Larsen et al., 2020) and 12 months post-operatively (Holsgaard-Larsen et al., 2020; Skoffer et al., 2020; Domínguez-Navarro et al., 2021), activities of daily living 3 months (Skoffer et al., 2016; Holsgaard-Larsen et al., 2020) and 12 months post-operatively (Holsgaard-Larsen et al., 2020; Skoffer et al., 2020; Domínguez-Navarro et al., 2021), Sport & Recreation 3 months post-operatively (Skoffer et al., 2016; Holsgaard-Larsen et al., 2020), and quality of life 3 months (Skoffer et al., 2016) and 12 months post-operatively (Holsgaard-Larsen et al., 2020; Skoffer et al., 2020; Domínguez-Navarro et al., 2021).
There was a significant effect in favor of prehabilitation on sit-to-stand performance 3 and 12 months post-operatively, on walking speed 3 and 12 months post-operatively, while no significant effect favoring prehabilitation for Timed Up & Go and stair climbing or stair climbing performance (Figure 3) (Holsgaard-Larsen et al., 2020; Skoffer et al., 2020; Domínguez-Navarro et al., 2021). Furthermore, a significant effect in favor of prehabilitation on maximal knee extensor strength emerged 3 and 12 months post-operatively, whereas no significant effect in favor of prehabilitation was observed for knee flexor strength 3 months post-operatively (Figure 4). Lastly, a significant effect in favor of prehabilitation was observed for ADL 3 months post-operatively, Sport & Recreation 3 months post-operatively, and pain 12 months post-operatively. No effect in favor of prehabilitation was found for the remaining patient-reported outcomes (Figure 5).

Figure 3. Forrest plots on post-operative functional performance 3 and 12 months post-operatively. Forest plots of the results of a random-effects meta-analysis shown as standardized mean differences with 95% CIs on functional performance 3 and 12 months post-operatively. For each study, the blue square represents the point estimate of the intervention effect. The horizontal line joins the lower and upper limits of the 95% CI of this effect. The red diamonds represent the pooled mean difference for each outcome.
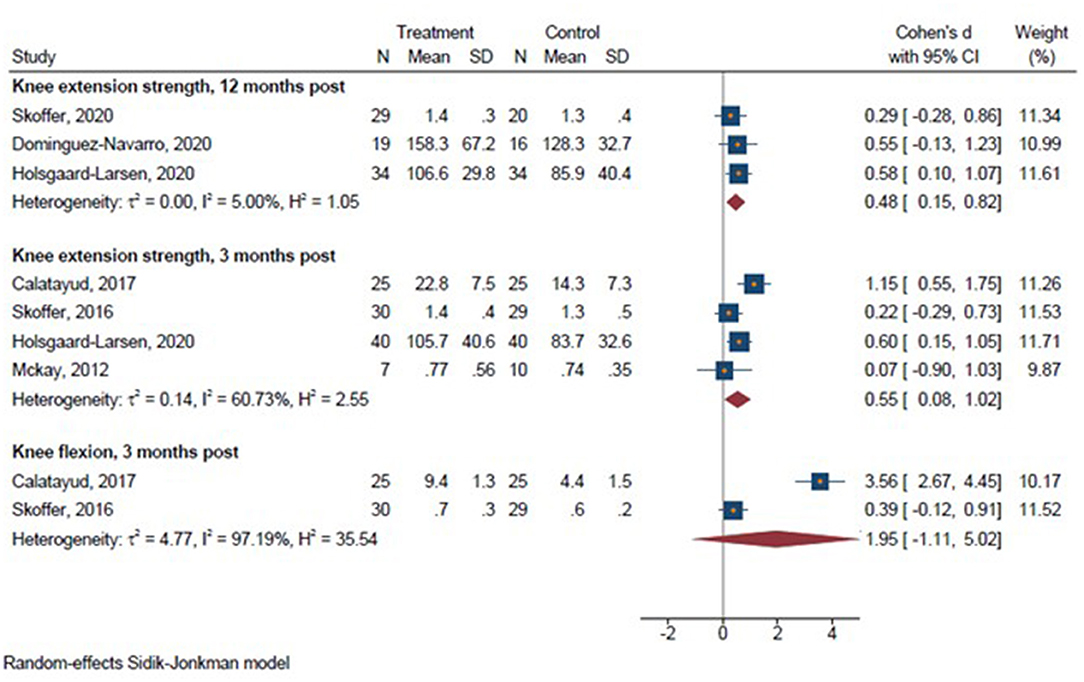
Figure 4. Forrest plots on lower limb strength 3 and 12 months post-operatively. Forest plots of the results of a random-effects meta-analysis shown as standardized mean differences with 95% CIs on lower limb strength 3 and 12 months post-operatively. For each study, the blue square represents the point estimate of the intervention effect. The horizontal line joins the lower and upper limits of the 95% CI of this effect. The red diamonds represent the pooled mean difference for each outcome.

Figure 5. Forrest plots on patient-reported outcomes 3 and 12 months post-operatively. Forest plots of the results of a random-effects meta-analysis shown as standardized mean differences with 95% CIs on patient-reported outcomes 3 and 12 months post-operatively. For each study, the blue square represents the point estimate of the intervention effect. The horizontal line joins the lower and upper limits of the 95% CI of this effect. The green diamonds represent the pooled mean difference for each outcome.
Discussion
The main finding of the present meta-analysis was that pre-operative prehabilitation training involving progressive resistance training (PRT) prior to TJR was indeed effective in producing enhanced medium-term and long-term gains in sit-to-stand performance, horizontal gait speed, and maximal knee extensor muscle strength compared to usual are or control intervention. Also, accentuated improvements in patient-reported outcomes representing the perceived ability to engage in activities of daily living, sport and recreational activities, along with larger reductions in pain were observed with PRT-based prehabilitation training up to 12 months post-operatively. However, not all functional performance measures or patient-reported outcomes were favored by PRT prior to TJR. The heterogeneous observations between different studies may in part rely on differences in total training volume and/or loading intensity (cf. Table 3). Thus, a pronounced degree of methodological diversity appears to exist between study specific exercise protocols, which may help to explain the marked differences in effects sizes observed across studies (cf. Figure 3). Specifically, McKay et al. (2012) showed no difference between groups for functional performance 3 months after surgery while Calatayud et al. (2016) and Holsgaard-Larsen et al. (2020) demonstrated significant differences between groups for the same outcomes (Figure 3). Thus, it may appear that mirroring a training protocol to Calatayud et al. (2016) or Hermann et al. (2015) would result in higher post-operative gains in functional performance and lower limb strength.
Thus, interpreting the singular results in i.e., Figure 3 from a clinical perspective, it appears that adopting a training protocol similar to Calatayud et al. (2016) or Hermann et al. (2015) may result in more pronounced post-operative gains in functional performance and lower limb muscle strength, respectively.
No previous systematic review has been able to identify any long-term effects of prehabilitation on various measures of objective functional performance or maximal knee extensor strength after TJR. This lack of identifiable effects may, at least in part, be ascribed to the inclusion of intervention protocols that are suboptimal for improving skeletal muscle strength. Thus, the inclusion of study trials utilizing unknown-to-low loading intensities and/or total training volumes and/or submaximal exercise protocols may have contributed to dilute the sensitivity of the overall meta-analysis to document the true effect of prehabilitation activities based on more optimized resistance training paradigms with documented anabolic (Aagaard et al., 2001) and neuro-facilitating (Aagaard et al., 2002) effects.
In the present meta-analysis, patient-reported ADL and Sport & Recreation were positively affected by prehabilitation exercise training when assessed 3 months after surgery (moderate effect). Furthermore, a small effect favoring prehabilitation was found for patient-reported pain 12 months after surgery. Hence, the present meta-analysis points to positive effects in both objectively measured function and patient reported function up to 12 months after surgery, in contrast to previous meta-analyses (Moyer et al., 2017).
The effect of prehabilitation on patient reported outcomes was small yet clearly evident in the present meta-analysis. The attenuated effect on patient reported outcomes may be explained by patients undergoing TJR achieve a very large perceived improvement from the surgical procedure (illustrated in Table 2). Hence, the range of subjectively perceived improvements imposed by exercise may be limited in such patients. Nonetheless, we were able to demonstrate a facilitating effect of prehabilitation training on this parameter in the present meta-analysis, which is a notable finding given the relatively small overall sample size (n = 256).
All of the included trials as well as one ongoing trials (Jørgensen et al., 2020) utilized fully supervised exercise session throughout the entire intervention period. Future studies should be conducted to examine if exercise protocols involving less extensive 1:1 supervision will be able to ensure a high adherence to training as well as a sufficient (i.e., effective) quality of exercise. This would likely facilitate the implementation of pre-operative training into the healthcare systems and offer more patients the opportunity to improve key outcome parameters (i.e., lower-limb strength and functional performance) associated with a higher post-operative functional performance-level in a “better in, better out”-manner.
Strengths and Limitations
In terms of methodological strengths, the present study adhered to the guidelines outlined by the Cochrane Handbook for Systematic Reviews of Interventions [version 6.2 (updated February 2021)] and the PRISMA statement (Moher et al., 2015). Specifically, inclusion and exclusion criteria were stated a priori, while study populations were comparable across trials and a majority of the functional performance tests remained similar across trials. As an additional strength of the present study, all included trials reported data on the specific exercise intensity, to ensure that sufficient exercise intensity and volume were employed in all studies included in the analyses.
A number of limitations may exist with the present meta-analysis. Firstly, the low number of studies (n = 7) included in the present systematic review may be considered a limitation, especially since comprising only five independent trials. However, as only RCT studies with relatively similar populations were included, and a random effects model with an adjustment to the confidence interval due few eligible studies (IntHout et al., 2014) was applied, we consider the results of the present analyses robust and valid. Despite being unable to perform our preplanned search in the The Allied and Complementary Database, we deem that the present literature search was effective of capturing all relevant studies.
Secondly, only a single study investigated the effect of pre-operative PRT in patients scheduled for THR, thus limiting the generalizability of the involved sub-analysis to patients suffering from end-stage hip OA. However, despite that TKR and THR are inherently different surgeries with differing effects on muscle and functional performance, and with different trajectories of recovery, it has been proposed that both patient populations may benefit from improving functional performance and lower-limb muscle strength prior to surgery (Bade et al., 2010; Zeni and Snyder-Mackler, 2010; Holstege et al., 2011; Nankaku et al., 2013; Skoffer et al., 2015). Therefore, before any firm conclusions can be drawn on the benefits of pre-operative PRT for patients scheduled for THR on post-operative functional performance, lower limb strength, and patient-reported outcomes, more research on this particular patient population is warranted.
Thirdly, despite exclusively including studies using exercise modalities and loading intensities objectively known to increase muscle strength and mass, intervention protocols were found to differ markedly between studies in terms of duration, total training volume and loading intensity. Consequently, optimal prehabilitation exercise dosage in terms of loading intensity and total duration remains to be investigated in patients scheduled for TJR surgery.
Fourthly, only very few studies have examined the long-term effects of strength-based prehabilitation in TJR patients (Holsgaard-Larsen et al., 2020; Skoffer et al., 2020; Domínguez-Navarro et al., 2021), underlining the need for more research to confirm the conclusions of the present meta-analysis. Furthermore, due to relatively high dropout rates from baseline to 12-month follow-up (Holsgaard-Larsen et al., 2020; Skoffer et al., 2020; Domínguez-Navarro et al., 2021), it appears important to ensure that future RCTs are sufficiently powered to detect long-term effects (≥12 months).
Lastly, low-to-very-low quality evidence formed all the comparisons in this systematic review. Our certainty of evidence was downgraded due to limitations in the randomization process, mainly due to deviations from the intended intervention procedures, missing data, and selection of the reported results. However, due to the nature of RCTs involving an exercise intervention group vs. usual care or control intervention group, in nature preventing from achieving full blinding of all participants and observers, it seems impossible to achieve high-level evidence when applying the GRADE assessment tool.
Conclusions
The present meta-analyses demonstrates that prehabilitation training involving progressive resistance exercise prior to TJR effectively induce long-lasting improvements in functional performance, maximal knee extensor muscle strength, and pain scoring, respectively. However, due to large methodological heterogeneity between the exercise protocols applied in the present studies, optimal choices about loading intensities, duration and total training volume remains unknown.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
SJ and SK organized the database and selected the appropriate studies. MB and SJ performed the data exctraction. SJ performed the statistical analysis and wrote the first draft of the manuscript. All authors contributed to conception, design of the study, participated in the data extraction, quality assessment, manuscript revision, read, and approved the submitted version.
Funding
This study was funded by the Nis Hanssens Mindeslegat 464000 dkr, Aase & Ejnar Danielsens Foundation 250000 dkr, Central Denmark Regional Health Science Foundation 99568 dkr, The Association for Danish Physiotherapists Foundation for research 131600 dkr, Hede Nielsens Foundation 58199 dkr, Hartmann's Foundation 94049 dkr.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2022.924307/full#supplementary-material
References
Aagaard, P., Andersen, J. L., Dyhre-Poulsen, P., Leffers, A. M., Wagner, A., Peter Magnusson, S., et al. (2001). A mechanism for increased contractile strength of human pennate muscle in response to strength training: changes in muscle architecture. J. Physiol. 534, 613–623. doi: 10.1111/j.1469-7793.2001.t01-1-00613.x
Aagaard, P., Simonsen, E. B., Andersen, J. L., Magnusson, P., and Dyhre-Poulsen, P. (2002). Increased rate of force development and neural drive of human skeletal muscle following resistance training. J. Appl. Physiol. 93, 1318–1326. doi: 10.1152/japplphysiol.00283.2002
Aagaard, P., Suetta, C., Caserotti, P., Magnusson, S. P., and Kjaer, M. (2010). Role of the nervous system in sarcopenia and muscle atrophy with aging: strength training as a countermeasure. Scand. J. Med. Sci. Sports 20, 49–64. doi: 10.1111/j.1600-0838.2009.01084.x
Alghadir, A., Anwer, S., and Brismée, J.-M. (2015). The reliability and minimal detectable change of Timed Up and Go test in individuals with grade 1-3 knee osteoarthritis. BMC Musculoskelet. Disord. 16, 174. doi: 10.1186/s12891-015-0637-8
Atkins, D., Best, D., Briss, P. A., Eccles, M., Falck-Ytter, Y., Flottorp, S., et al. (2004). Grading quality of evidence and strength of recommendations. BMJ 328, 1490. doi: 10.1136/bmj.328.7454.1490
Bade, M. J., Kohrt, W. M., and Stevens-Lapsley, J. (2010). Outcomes before and after total knee arthroplasty compared to healthy adults. J. Orthop. Sports Phys. Ther. 40, 559–567. doi: 10.2519/jospt.2010.3317
Borde, R., Hortobágyi, T., and Granacher, U. (2015). Dose-Response relationships of resistance training in healthy old adults: a systematic review and meta-analysis. Sports Med. 45, 1693–1720. doi: 10.1007/s40279-015-0385-9
Brignardello-Petersen, R., Bonner, A., Alexander, P. E., Siemieniuk, R. A., Furukawa, T. A., Rochwerg, B., et al. (2018). Advances in the GRADE approach to rate the certainty in estimates from a network meta-analysis. J. Clin. Epidemiol. 93, 36–44. doi: 10.1016/j.jclinepi.2017.10.005
Bryk, F. F., dos Reis, A. C., Fingerhut, D., Araujo, T., Schutzer, M., Cury, R. P. L., et al. (2016). Exercises with partial vascular occlusion in patients with knee osteoarthritis: a randomized clinical trial. Knee Surg. Sports Traumatol. Arthrosc. 24, 1580–1586. doi: 10.1007/s00167-016-4064-7
Calatayud, J., Casaña, J., Ezzatvar, Y., Jakobsen, M. D., Sundstrup, E., Andersen, L. L., et al. (2016). High-intensity preoperative training improves physical and functional recovery in the early post-operative periods after total knee arthroplasty: a randomized controlled trial. Knee Surg. Sports Traumatol. Arthrosc. 25, 2864–2872. doi: 10.1007/s00167-016-3985-5
Chesham, R. A., and Shanmugam, S. (2017). Does preoperative physiotherapy improve postoperative, patient-based outcomes in older adults who have undergone total knee arthroplasty? A systematic review. Physiother. Theory Pract. 33, 9–30. doi: 10.1080/09593985.2016.1230660
Cohen, J. (2013). Statistical Power Analysis for the Behavioral Sciences. 2nd ed. New York, NY: Routledge. doi: 10.4324/9780203771587
Csapo, R., and Alegre, L. M. (2016). Effects of resistance training with moderate vs heavy loads on muscle mass and strength in the elderly: a meta-analysis. Scand. J. Med. Sci. Sports 26, 995–1006. doi: 10.1111/sms.12536
Domínguez-Navarro, F., Silvestre-Muñoz, A., Igual-Camacho, C., Díaz-Díaz, B., Torrella, J. V., Rodrigo, J., et al. (2021). A randomized controlled trial assessing the effects of preoperative strengthening plus balance training on balance and functional outcome up to 1 year following total knee replacement. Knee Surg. Sports Traumatol. Arthrosc. 29, 838–848. doi: 10.1007/s00167-020-06029-x
Ferraz, R. B., Gualano, B., Rodrigues, R., Kurimori, C. O., Fuller, R., Lima, F. R., et al. (2018). Benefits of resistance training with blood flow restriction in knee osteoarthritis. Med. Sci. Sports Exerc. 68, 1239–1251. doi: 10.1249/MSS.0000000000001530
Fortin, P. R., Clarke, A. E., Joseph, L., Liang, M. H., Tanzer, M., Ferland, D., et al. (1999). Outcomes of total hip and knee replacement: preoperative functional status predicts outcomes at six months after surgery. Arthritis Rheum. 42, 1722–1728. doi: 10.1002/1529-0131(199908)42:8<1722::AID-ANR22>3.0.CO;2-R
Franz, A., Queitsch, F. P., Behringer, M., Mayer, C., Krauspe, R., Zilkens, C., et al. (2018). Blood flow restriction training as a prehabilitation concept in total knee arthroplasty: a narrative review about current preoperative interventions and the potential impact of BFR. Med. Hypotheses. 110, 53–59. doi: 10.1016/j.mehy.2017.10.029
Garber, C. E., Blissmer, B., Deschenes, M. R., Franklin, B. A., Lamonte, M. J., Lee, I. M., et al. (2011). Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med. Sci. Sports Exerc. 43, 1334–1359. doi: 10.1249/MSS.0b013e318213fefb
Ghosh, A., and Chatterji, U. (2018). An evidence-based review of enhanced recovery after surgery in total knee replacement surgery. J. Perioper. Pract. 29, 281–290. doi: 10.1177/1750458918791121
Grønfeldt, B. M., Lindberg Nielsen, J., Mieritz, R. M., Lund, H., and Aagaard, P. (2020). Effect of blood-flow restricted vs heavy-load strength training on muscle strength: systematic review and meta-analysis. Scand. J. Med. Sci. Sports 30, 837–848. doi: 10.1111/sms.13632
Guyatt, G. H., Oxman, A. D., Kunz, R., Vist, G. E., Falck-Ytter, Y., Schunemann, H. J., et al. (2008). What is “quality of evidence” and why is it important to clinicians? BMJ 336, 995–998. doi: 10.1136/bmj.39490.551019.BE
Hermann, A., Holsgaard-Larsen, A., Zerahn, B., Mejdahl, S., and Overgaard, S. (2015). Preoperative progressive explosive-type resistance training is feasible and effective in patients with hip osteoarthritis scheduled for total hip arthroplasty - a randomized controlled trial. Osteoarthr. Cartil. 24, 1–8. doi: 10.1016/j.joca.2015.07.030
Higgins, J. P., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M. J., et al. (2019). Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons. doi: 10.1002/9781119536604
Higgins, J. P. T., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ 327, 557–560. doi: 10.1136/bmj.327.7414.557
Holsgaard-Larsen, A., Hermann, A., Zerahn, B., Mejdahl, S., and Overgaard, S. (2020). Effects of progressive resistance training prior to total HIP arthroplasty & a secondary analysis of a randomized controlled trial. Osteoarthr. Cartil. 28, 1038–1045. doi: 10.1016/j.joca.2020.04.010
Holstege, M. S., Lindeboom, R., and Lucas, C. (2011). Preoperative quadriceps strength as a predictor for short-term functional outcome after total hip replacement. Arch. Phys. Med. Rehabil. 92, 236–241. doi: 10.1016/j.apmr.2010.10.015
Hughes, L., Rosenblatt, B., Haddad, F., Gissane, C., McCarthy, D., Clarke, T., et al. (2019). Comparing the effectiveness of blood flow restriction and traditional heavy load resistance training in the post-surgery rehabilitation of anterior cruciate ligament reconstruction patients: a UK national health service randomised controlled trial. Sports Med. 49, 1787–1805. doi: 10.1007/s40279-019-01137-2
Husted, R. S., Juhl, C., Troelsen, A., Thorborg, K., Kallemose, T., Rathleff, M. S., et al. (2020). The relationship between prescribed pre-operative knee-extensor exercise dosage and effect on knee-extensor strength prior to and following total knee arthroplasty: a systematic review and meta-regression analysis of randomized controlled trials. Osteoarthr. Cartil. 28, 1412–1426. doi: 10.1016/j.joca.2020.08.011
IntHout, J., Ioannidis, J. P. A., and Borm, G. F. (2014). The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med. Res. Methodol. 14, 25. doi: 10.1186/1471-2288-14-25
Jørgensen, S. L., Bohn, M. B., Aagaard, P., and Mechlenburg, I. (2020). Efficacy of low-load blood flow restricted resistance EXercise in patients with Knee osteoarthritis scheduled for total knee replacement (EXKnee): protocol for a multicentre randomised controlled trial. BMJ Open 10, e034376. doi: 10.1136/bmjopen-2019-034376
Kim, D., Loenneke, J. P., Ye, X., Bemben, D. A., Beck, T. W., Larson, R. D., et al. (2017). Low-load resistance training with low relative pressure produces muscular changes similar to high-load resistance training. Muscle Nerve. 56, E126–E33. doi: 10.1002/mus.25626
Koblbauer, I. F. H., Lambrecht, Y., Van, D. H., Neeter, C., Engelbert, R. H. H., Poolman, R. W., et al. (2011). Reliability of maximal isometric knee strength testing with modified hand-held dynamometry in patients awaiting total knee arthroplasty: useful in research and individual patient settings? A reliability study. BMC Musculoskelet. Disord. 12, 249. doi: 10.1186/1471-2474-12-249
Kurtz, S., Ong, K., Lau, E., Mowat, F., and Halpern, M. (2007). Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Joint Surg. 89, 780–785. doi: 10.2106/00004623-200704000-00012
Kwok, I. H., Paton, B., and Haddad, F. S. (2015). Does pre-operative physiotherapy improve outcomes in primary total knee arthroplasty?—A systematic review. J. Arthroplasty 30, 1657–1663. doi: 10.1016/j.arth.2015.04.013
Lim, J. A., and Thahir, A. (2021). Perioperative management of elderly patients with osteoarthritis requiring total knee arthroplasty. J. Perioper. Pract. 31, 209–214. doi: 10.1177/1750458920936940
McKay, C., Prapavessis, H., and Doherty, T. (2012). The effect of a prehabilitation exercise program on quadriceps strength for patients undergoing total knee arthroplasty: a randomized controlled pilot study. PM R 4, 647–656. doi: 10.1016/j.pmrj.2012.04.012
Mizner, R. L., Petterson, S. C., and Snyder-Mackler, L. (2005). Quadriceps strength and the time course of functional recovery after total knee arthroplasty. J. Orthop. Sports Phys. Ther. 35, 426–436. doi: 10.2519/jospt.2005.35.7.424
Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., et al. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 4, 1. doi: 10.1186/2046-4053-4-1
Moyer, R., Ikert, K., Long, K., and Marsh, J. (2017). The value of preoperative exercise and education for patients undergoing total hip and knee arthroplasty: a systematic review and meta-analysis. JBJS Rev. 5, e2. doi: 10.2106/JBJS.RVW.17.00015
Nankaku, M., Tsuboyama, T., Akiyama, H., Kakinoki, R., Fujita, Y., Nishimura, J., et al. (2013). Preoperative prediction of ambulatory status at 6 months after total hip arthroplasty. Phys. Ther. 93, 88–93. doi: 10.2522/ptj.20120016
Odgaard, A., Lindberg-Larsen, M., Schrøder, H., Madsen, H. Ø. F., and Troelsen, A. (2020a). The Danish Hip Arthroplasty Register (DHR), 2020. National Annual Report. Available online at: http://www.dhr.dk
Odgaard, A., Østergaard, S. E., Lindberg-Larsen M, Schrøder, H., and Madsen, F. (2020b). Dansk Knæalloplastikregister Årsrapport. Regionernes Kliniske Kvalitetsudviklingsprogram (RKKP). Available online at: https://www.sundhed.dk/content/cms/99/4699_dkr-arsrapport-2020_offentliggorelse.pdf (accessed December 31, 2019).
Patterson, S. D., Hughes, L., Warmington, S., Burr, J., Scott, B. R., Owens, J., et al. (2019). Blood flow restriction exercise position stand: considerations of methodology, application, and safety. Front. Physiol. 10, 533. doi: 10.3389/fphys.2019.00533
Segal, N., Davis, M. D., and Mikesky, A. E. (2015). Efficacy of blood flow-restricted low-load resistance training for quadriceps strengthening in men at risk of symptomatic knee osteoarthritis. Geriatr. Orthop. Surg. Rehabil. 6, 160–167. doi: 10.1177/2151458515583088
Segal, N. A., Williams, G. N., Davis, M. C., Wallace, R. B., and Mikesky, A. E. (2015). Efficacy of blood flow-restricted, low-load resistance training in women with risk factors for symptomatic knee osteoarthritis. PM R 7, 376–384. doi: 10.1016/j.pmrj.2014.09.014
Skoffer, B., Dalgas, U., and Mechlenburg, I. (2015). Progressive resistance training before and after total hip and knee arthroplasty: a systematic review. Clin. Rehabil. 15, 14–29. doi: 10.1177/0269215514537093
Skoffer, B., Maribo, T., Mechlenburg, I., Hansen, P. M., Søballe, K., Dalgas, U., et al. (2016). Efficacy of preoperative progressive resistance training on postoperative outcomes in patients undergoing total knee arthroplasty. Arthritis Care Res. 68, 1239–1251. doi: 10.1002/acr.22825
Skoffer, B., Maribo, T., Mechlenburg, I., Korsgaard, C. G., Søballe, K., Dalgas, U., et al. (2020). Efficacy of preoperative progressive resistance training in patients undergoing total knee arthroplasty: 12-month follow-up data from a randomized controlled trial. Clin. Rehabil. 34, 82–90. doi: 10.1177/0269215519883420
Steib, S., Schoene, D., and Pfeifer, K. (2010). Dose-response relationship of resistance training in older adults: a meta-analysis. Med. Sci. Sports Exerc. 42, 902–914. doi: 10.1249/MSS.0b013e3181c34465
Suetta, C. (2004). Training-induced changes in muscle CSA, muscle strength, EMG, and rate of force development in elderly subjects after long-term unilateral disuse. J. Appl. Physiol. 97, 1954–1961. doi: 10.1152/japplphysiol.01307.2003
Wang, L., Lee, M., Zhang, Z., Moodie, J., Cheng, D., Martin, J., et al. (2016). Does preoperative rehabilitation for patients planning to undergo joint replacement surgery improve outcomes? A systematic review and meta-analysis of randomised controlled trials. BMJ Open 6, e009857. doi: 10.1136/bmjopen-2015-009857
Keywords: prehabilitation, functional performance, muscle strength, orthopedics, patient reported outcomes
Citation: Jørgensen SL, Kierkegaard S, Bohn MB, Aagaard P and Mechlenburg I (2022) Effects of Resistance Training Prior to Total Hip or Knee Replacement on Post-operative Recovery in Functional Performance: A Systematic Review and Meta-Analysis. Front. Sports Act. Living 4:924307. doi: 10.3389/fspor.2022.924307
Received: 20 April 2022; Accepted: 22 June 2022;
Published: 14 July 2022.
Edited by:
Abbey Thomas, University of North Carolina at Charlotte, United StatesReviewed by:
Dana Judd, University of Colorado Anschutz Medical Campus, United StatesSuzanne Broadbent, University of the Sunshine Coast, Australia
Copyright © 2022 Jørgensen, Kierkegaard, Bohn, Aagaard and Mechlenburg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stian Langgård Jørgensen, c3RpYWpvQHJtLmRr